 Shi Yi Chua
Shi Yi Chua Fairuz Nazri Abd Rahman
Fairuz Nazri Abd Rahman Selvasingam Ratnasingam2
Selvasingam Ratnasingam2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 30 October 2023
Sec. Autism
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1244164
This article is part of the Research Topic Wellbeing in Parents of Neurodivergent Children View all 8 articles
Objective: Caregivers of children with Autism Spectrum Disorder (ASD) often experience emotional and psychological distress, as well as disruptions to family life and employment due to the challenges of caring for children with ASD. This study examines the relationship between problem behaviours and caregiver burden among children with ASD.
Method: A cross-sectional study using convenience sampling recruited 230 caregivers of children with ASD aged 4 to 18 years from selected autism centres in Kuching, Sarawak. The caregivers completed the Aberrant Behaviour Checklist-2 and the Zarit Burden Interview.
Results: Univariate analysis revealed a significant difference in caregiver burden for children with ASD receiving medications (p = 0.013), registered with the Social Welfare Department (p = 0.036), and having siblings with ASD (p = 0.046). About 40% of the children exhibited at least one domain of problem behaviour. More than half of the caregivers (53.9%) experienced burden, with the majority experiencing mild burden. Positive associations were seen between irritability (r = 0.458, p < 0.01), social withdrawal (r = 0.439, p < 0.01), stereotypic behaviour (r = 0.392, p < 0.01), hyperactivity/non-compliance (r = 0.467, p < 0.01), and caregiver burden. Child factors, including the duration of problem behaviour (r = 0.182, p = 0.007), medication use (eta = 0.187, p = 0.005), Social Welfare Department registration (eta = 0.138, p = 0.036), and the presence of siblings with ASD (eta = 0.130, p = 0.046) were associated with caregiver burden. Multiple linear regression showed that hyperactivity/noncompliance significantly predicted caregiver burden.
Conclusion: Specific problem behaviours in children with ASD were associated with caregiver burden. These results highlight the need for interventions for the child with ASD and their caregivers.
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder which is characterized by persistent deficits in social communication and social interaction as well as restricted, repetitive patterns of behaviour, interests or activities which causes clinically significant impairment in social, occupational, and other important areas of functioning (1). A feasibility study on the use of Modified Checklist for Autism in toddlers (M-CHAT) among children of 18 to 36 months of age in child health clinics by Ministry of Health Malaysia in 2006 showed that the prevalence of ASD in Malaysia was approximately 1.6 in 1000 (2).
Individuals with ASD experience a variety of emotional and behavioural problems that include externalizing and internalizing behaviours such as anxiety, depression, somatization, rule-breaking, aggression, self-harm, inattention, hyperactivity, impulsivity, and abnormal thought. Moreover, these symptoms change as the child grows and vary in severity (3). The prevalence of problem behaviour in children with ASD was found to range from around 71 to 94.0% (4–6). These figures are at least three times higher compared to an earlier study conducted in Malaysia, where the reported prevalence was considerably lower, at 24.2% (7). While problem behaviour was found to be independent of age and gender (6), several factors have been linked to problem behaviours in ASD, including having comorbid intellectual disability, impaired adaptive functioning, language impairment, as well as medical comorbidities such as seizures, gastrointestinal and sleep disorders (8–12). Moreover, except for hyperactivity, these behaviour problems tend to persist from adolescence through adulthood, indicating their chronic nature (11).
Problem behaviours affect both the child with ASD and their family members. Severe behaviour problems hamper the child’s development, learning, expression of adaptive behaviour and effectiveness of early intervention. It also results in more intensive use of medications (13) and an increased risk of hospitalization (14). In addition, problem behaviours adversely affect caregivers financially, psychologically, and physically (15–19). Prior research has demonstrated that siblings of children with ASD often undergo emotional distress due to problem behaviours, affecting their upbringing and their relationship with their siblings with ASD (20, 21).
Providing care for individuals with disabilities is associated with a variety of negative experiences (22). It is reported that caregiving for children with ASD is more stressful and challenging than parenting children with typical development and children with other developmental disabilities (23, 24). These challenges include behavioural problems, financial difficulties, stigma and the lack of awareness in the community (25). Problem behaviour has been one of the most widely reported predictors of caregiver stress and burden (3, 26–29). Other predictors of caregiver burden include the severity of ASD symptoms, lower levels of perceived social support, low financial status, caregiver parenting skills and caregivers having medical comorbidities (18, 30–32). There are several studies that attempt to examine the bidirectional relationship between child behaviour and caregiver stress within families of children with ASD. These studies suggest that child behaviour can exacerbate parental stress, and parental stress likewise exacerbates child behavioural problems (3, 33). Moreover, parent–child transactions were found to vary with different life phases and with different domains of behaviour problems (34).
Previous research has consistently demonstrated the significant impact of cultural differences on individuals’ perceptions of illness and their coping strategies during times of stress (35, 36). The majority of investigations examining the relationship between behavioural issues and caregiver burden have been conducted in Western and European countries (28, 37). These countries tend to embrace individualistic values, in contrast to Asian countries, that emphasize collectivism, where group interdependence and norms hold significance (38). In such collectivistic cultures, children with ASD displaying problem behaviours might be seen as devaluating the family’s reputation, leading to stigmatization within the family. Malaysia, particularly in Sarawak, boasts a diverse population consisting of Malay, Iban, Chinese, and Bidayuh ethnicities (39). Each of these ethnic groups maintains distinct cultural and spiritual beliefs that influence their perception of illnesses, health seeking behaviour and coping skills (40). Having a child with ASD may be associated with mystic beliefs or sometimes linked to ancestral past transgression, leading caregivers to seek spiritual treatment instead (41). The varying religious practices and teachings within Malaysia may also exert an influence on how caregivers navigate challenges (41–43). Consequently, this interplay between cultural beliefs, stigma, religious practices, and values can lead to differing perceptions of caregiver burden and stress when compared to other nations.
This study is aimed to examine the relationship between problem behaviours in children with ASD, sociodemographic variables, and caregiver burden in Sarawak, Malaysia. This would facilitate the delivery of locally tailored interventions for children with ASD and their caregivers. We hypothesize that there is a significant association between problem behaviours and caregiver burden in this population.
This is a cross-sectional study involving caregivers of children with ASD in the child & adolescent Psychiatric clinic and the child developmental clinic in Sarawak General Hospital, the Kuching Autism Association (KAA) headquarters and the One Stop Early Intervention Centre (OSEIC) in Kuching, Sarawak. Sarawak is geographically the largest state in Malaysia. It lies in East Malaysia and shares the island of Borneo with the eastern state of Sabah, Indonesian Kalimantan, and Brunei. It differs from other states in Malaysia in terms of socio-demographics particularly ethnicity, culture, religion, and socio-economic status. The child & adolescent Psychiatry clinic and the child developmental Clinic in Sarawak General Hospital cater mainly to children with autism in Kuching city. The Kuching Autism Association is a non-governmental organization which was established since 1998. The association runs an educational and pre-vocational training centre for children with ASD aged 3 to 17 years and a sheltered workshop for adults with ASD. The One Stop Early Intervention Centre (OSEIC) in Kuching is an early intervention centre which offers interventions for children with developmental or learning disabilities including ASD, Down Syndrome, and Intellectual Disability. It provides early intervention services which include physiotherapy, occupational therapy or speech therapy to infants and children up to the age of 6 years.
The recruitment of caregivers of children with ASD was done through convenient sampling. The data collection period was from 1st December 2021 to 31st March 2022. The inclusion criteria for the caregiver were those aged 18 years and above who provided unpaid care to the children for at least 12 months, have working knowledge of Malay or English, and were able to give consent for the study. Exclusion criteria were caregivers who took care of the children with ASD for less than 12 months and caregivers who were receiving any form of payment for their services. Inclusion criteria for the children are children who were aged between 4 to 18 years and diagnosed with ASD by a paediatrician or a psychiatrist based on the diagnostic criteria of DSM 5 or the International Classification of Disease 10 (ICD-10) and were taken care of by caregivers in the family context.
The study population consisted of 230 caregivers of children with ASD visiting the above-mentioned centres in Kuching during the recruitment study period who fulfilled the inclusion criteria. All caregivers were briefed regarding the purpose of the study before consenting to participate in this study. Those who did not consent to the study were excluded from the study. Caregivers who agreed were requested to sign a consent before being enrolled in the study.
Each caregiver was given a set of 4 self-rating questionnaires which required about 20–25 min to complete. The caregivers were given explanations about the important instructions in each section of the questionnaires. The questionnaires were in English and Malay language. Caregivers were allowed to choose between the English or Malay-translated version of the questionnaires. The investigator was present to clarify any questions the caregivers had. Confidentiality was guaranteed to all participants. A coding system was used to organize the completed questionnaires. Caregivers and patients are not directly identifiable from the forms for the sake of confidentiality.
Permission from the original authors for the questionnaires Aberrant Behaviour Checklist-2 (ABC-2) and Zarit Burden Interview (ZBI) was obtained prior to commencing this study.
Information about the caregivers, including age, gender, ethnic group, the highest level of education, occupation, marital status, relationship with the patient, number of households, total household income (in Ringgit Malaysia), duration of caregiving and total contact hours were obtained. Patients’ socio-demographic data included age, gender, ethnic group, current or the highest level of education, types of specific intervention received (occupational therapy, speech therapy and/or applied behaviour therapy), the age and duration of these specific interventions received, other psychiatric illness, other medical illness, and the number of hospitalization due to problem behaviour, registration with the Social Welfare Department (Person with Disability status), benefits received from the Social Welfare Department or any other entity, and the presence of other family members with ASD were also gathered.
The ABC-2 (44) is a 58-item symptom checklist for rating inappropriate and maladaptive behaviours of school-age children or adults with mental disabilities. Scores on the 58 items resolve into five subscales: (1) irritability, agitation (e.g., disruptive behaviour), (2) lethargy, social withdrawal (e.g., isolation or inactivity), (3) stereotypic behaviour (e.g., repetitive purposeless movements), (4) hyperactivity, non-compliance (e.g., disobedient, overactive), and (5) inappropriate speech (e.g., repetitive talking). Each item is rated 0 to 3, with higher scores indicating greater severity. The authors report that domain scores falling above the 80th percentile can be defined as clinically significant. Numerous studies have been published supporting the reliability and validity of the ABC (45–47). The ABC has also been validated for Autism Spectrum Disorder (48). Kaat et al.’s study (48) also supported the standard factor structure of the ABC and the ABC’s construct validity in toddlers. The ABC-2 had been translated into multiple languages including Bahasa Malaysia. As the Malay ABC-2 is not validated in our local setting, a pilot test was carried out on 69 independent respondents. In this study, the Malay version of ABC-2 showed good internal consistency with the Cronbach’s α coefficient of at least 0.7 and above (see Supplementary Material).
The ZBI (49) was used to assess the level of subjective burden experienced by the caregivers of children and adolescents with ASD. It is a 22-item instrument used for measuring the caregiver’s perceived burden of providing family care. It was developed for use with caregivers of persons with dementia, but it had been used to assess many different types of caregivers, including those caring for persons with chronic health problems, mental health problems, and parents of children with health problems or behavioural and developmental problems. The 22 items are assessed on a 5-point Likert scale, ranging from 0 = “never” to 4 = “nearly always.” Item scores are added up to give a total score ranging from 0 to 88, with higher scores indicating a higher subjective burden. A total score of 0–20 indicates little or no burden, 21–40 indicates mild to moderate burden, 41–60 indicates moderate to severe burden, and 61–88 indicates severe burden. The questions focus on major areas such as burden in the relationship, emotional well-being, social and family life, finances, and loss of control over one’s life. It is available in English and Malay. It has recently been validated in the Malay language (50). The internal consistency of the Malay version of ZBI is good with a high Cronbach’s alpha coefficient of 0.898 and split-half correlation coefficient of 0.912. A score of 22 was selected as the suitable cut-off score for the Malay ZBI scale in the local population based on the ROC curve with the area under the curve of 0.786 (CI 0.658–0.914, p = 0.001). The Malay ZBI’s sensitivity and specificity were 70.8 percent and 69.2 percent, with a score of 22. In this study, the ZBI showed good internal consistency with Cronbach’s α coefficient of 0.91.
Statistical software, IBM-SPSS 26.0 (Armonk 2019), licensed to UKM, was used to complete the data analysis to answer the research questions of this study. Data was checked and cleaned. Preliminary data screening was done for missing values or possible wrong data entry. Normality assessment was also done for the data before proceeding to the analysis. The skewness values for all variables indicate that the distribution was normal since the values lay between −1 and 1.
Descriptive analysis was conducted for all the sociodemographic characteristics. Frequency and valid percentages were used to demonstrate categorical data. Means and standard deviation were used to demonstrate continuous variables. The mean caregiver total burden scores between children and caregiver sociodemographic variables were also compared using Independent t-test and one-way Analysis of Variance (ANOVA). Descriptive analysis was done for the five subscales of the ABC-2 (irritability, social withdrawal, stereotypic behaviour, hyperactivity, and inappropriate speech) and the total scores of the ZBI. Correlation analysis was done to assess the relationship between problem behaviour in children with ASD and caregiver burden. Simple linear regression analysis was done to determine if problem behaviour would predict caregiver burden. The association between child and caregiver variables and total burden scores was calculated using Eta correlation analysis for categorical variables. Pearson correlation analysis was used for continuous variables. A multiple linear regression analysis was also carried out to study the impact of the variables on caregiver burden.
This research was approved by the UKM research ethics committee (UKM PPI/111/8/JEP-2021-527). It was also registered under the National Medical Research Register Malaysia (NMRR-21-1179-59667). Approval was also obtained from Kuching Autism Association and One Stop Early Intervention Centre.
The caregivers with severe caregiver burden who were depressed or anxious during the interview were offered a referral to the adult psychiatric outpatient clinic with their consent. Additionally, they were advised about facilities where they could get assistance.
In this study, a total of 250 caregivers were approached. There was a total of 170 (73.9%) caregivers from the clinical group and 60 (23.1%) caregivers from the non-clinical group. 20 caregivers did not consent for the study (8 caregivers from the clinical group and 12 caregivers from the non-clinical group). We do not have information about the clinical features of the children and parents who did not participate. About 15.2% were female and 84.8% were male children with ASD (see Table 1). The mean age of the patients was 8.37 years, indicating patients involved in this study were, on average, around 8 years old. Most of the patients were Malay, 45.2%. The mean duration of problem behaviour among children having ASD was 4.23 years. More than half (67.0%) of the children did not have any other psychiatric disorders. Most children with ASD, i.e., 91.7%, did not have any other medical conditions. More than half of the children, 65.2%, were registered with the Social Welfare Department. In addition, there were only 4.3% of children with ASD who had other siblings with the disorder.
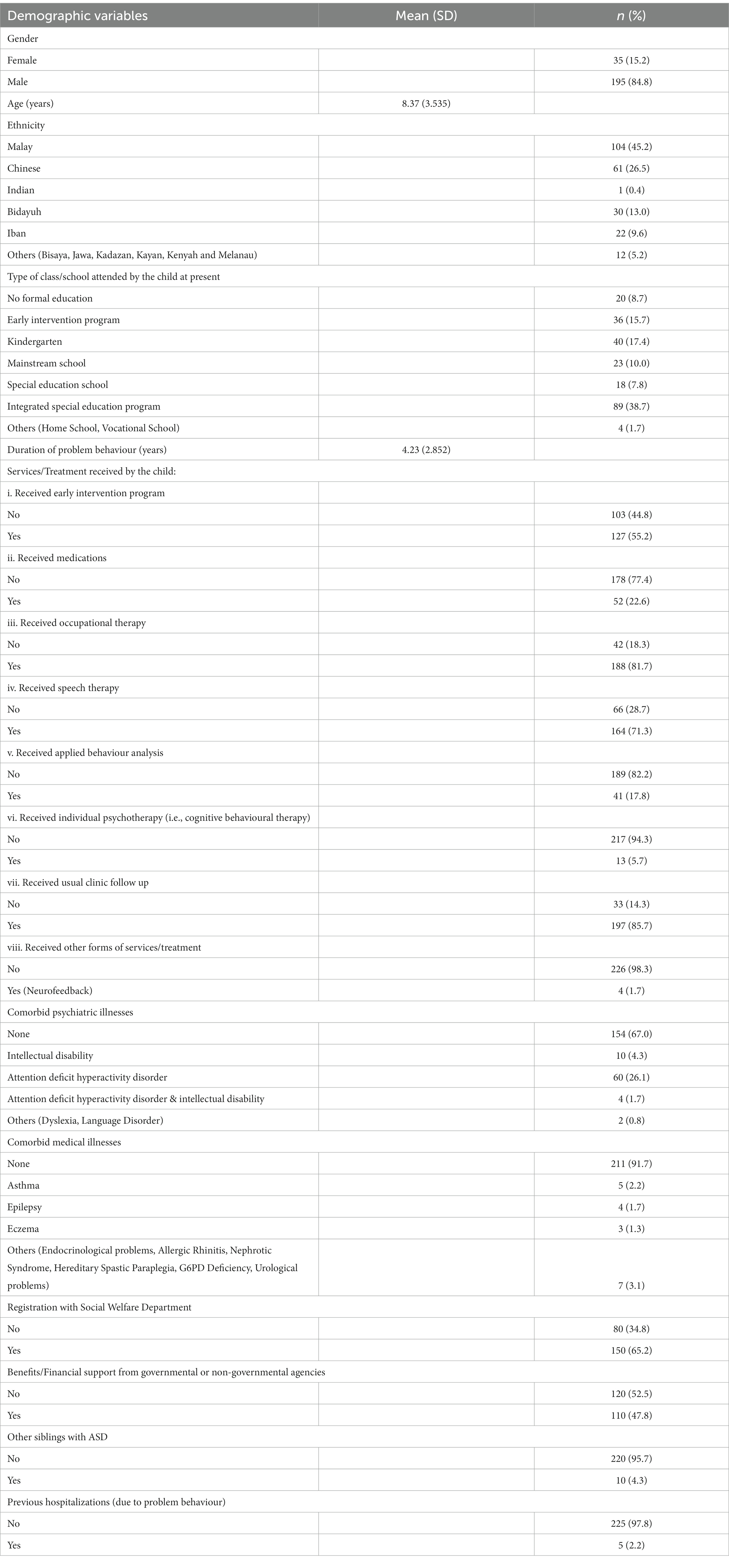
Table 1. Demographics of children and adolescents with ASD.
Children demographic data are summarized in Table 1.
Approximately 79.6% of carers were female, and 20.4% were male, as shown in Table 2. The mean age of the caregiver was 39.16 years, indicating that they were, on average, approximately 39 years old. In terms of ethnicity, 43.0% of the caregivers were Malay and around half of the caregivers (52.2%) had a tertiary education. Around half of the caregivers (52.2%) of caregivers held full-time employment. In terms of the marital status of caregivers, 93.9% were married. The majority of the caregivers (75.5%) were the patients’ mothers. According to the Department of Statistics Malaysia (51), household income is classified into 3 different income classifications – B40, M40, and T20. B40 represents the bottom 40% (household income is below RM 4,850 per month), M40 represents the middle 40% (household income between RM 4,851 per to RM 10,960 per month), and T20 represents the top 20% of Malaysian household income (household income exceeds RM 10,960 a month). Many caregivers had monthly household incomes below RM 4,850 (44.3%).
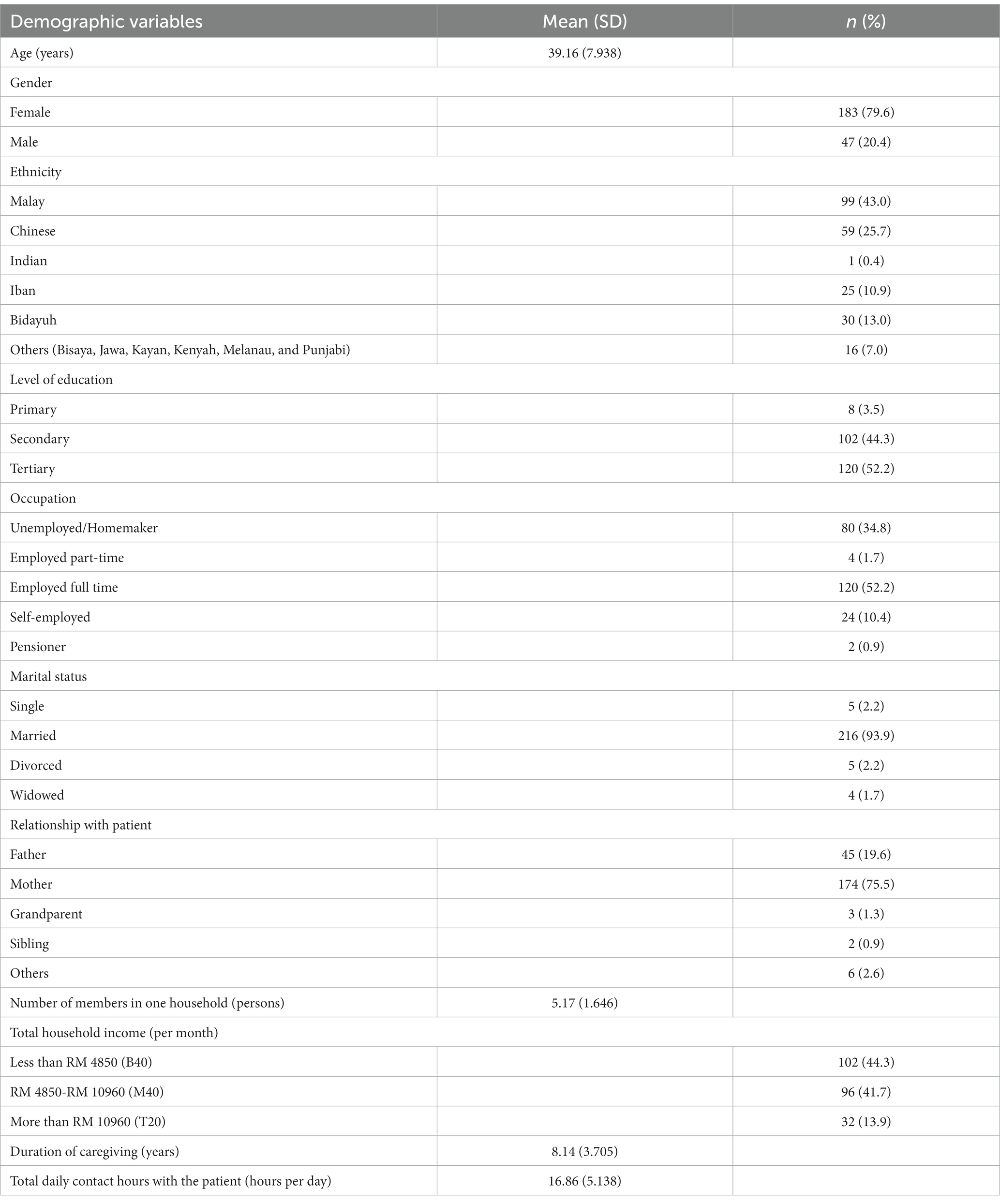
Table 2. Demographics of caregivers of children and adolescents with ASD.
Caregiver demographic data are summarized in Table 2.
Independent t-test and One-way ANOVA were conducted to compare the mean caregiver total burden score of the children’s sociodemographic variables (see Table 3). Caregivers of children with ASD who received medications had higher burden scores (M = 30.08, SD = 15.68) compared to those who did not receive medications (M = 24.00, SD = 12.75); t (71.841) = −2.559, p = 0.013. Similarly, caregivers of children with ASD registered with the Social Welfare Department had higher burden scores (M = 26.75, SD = 13.95) compared to those not registered (M = 22.79, SD = 12.821); t (228) = −2.111, p = 0.036. Caregivers of children with ASD who had siblings with ASD also showed higher burden scores (M = 33.80, SD = 19.932) compared to those without siblings with ASD (M = 24.99, SD = 13.257); t (228) = 2.006, p = 0.046.
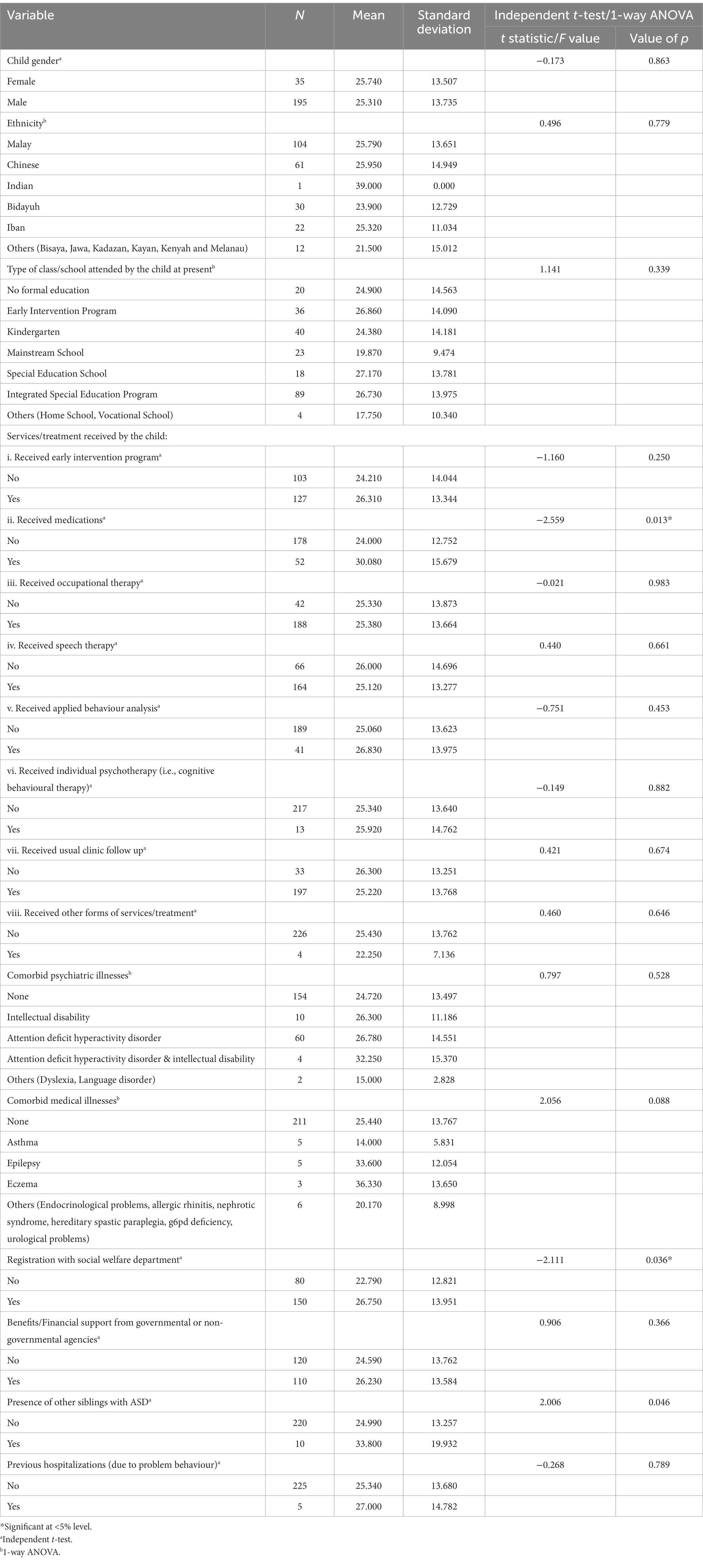
Table 3. Comparison of mean total burden score between child’s demographic variables.
There were no significant difference in the mean total burden scores for the other children sociodemographic variables and caregivers’ sociodemographic variables.
In this sample, almost half (40.4%) of the children had at least one form of problem behaviour domain which had total scores above the 80th percentile (see Table 4). Around one-third (27.8%) had concerning levels of social withdrawal, followed by 22.2% of children having concerning levels of stereotypic behaviour, 18.3% of children having concerning levels of irritability, 13.9% of children having concerning levels of hyperactivity/non-compliance and 13.9% of children having concerning levels of inappropriate speech.

Table 4. Children with ASD with problem behaviour.
The mean and standard deviation for the ABC-2 subscales are shown in Table 5.

Table 5. Mean and standard deviation for ABC-2 subscales.
The majority of the caregivers, 46.1%, were classified as having little or no burden, followed by 39.6% who were categorized as having mild to moderate level of burden, 13.5% who were classified as having moderate to severe burden and 0.9% with severe burden. Based on the results, the computed mean for the total ZBI score is 25.37 with a standard deviation of 13.672.
Pearson’s correlation analysis showed a significant positive correlation between the ABC-2 irritability, social withdrawal, stereotypic behaviour, and hyperactivity/noncompliance subscales with the total ZBI score. The irritability subscale showed a moderately positive correlation with the total ZBI score (r = 0.458, p < 0.01) (52). The Social Withdrawal subscale showed a moderately positive correlation with the total ZBI score (r = 0.439, p < 0.01). The Stereotypic Behaviour subscale showed a positive but weak correlation with the total ZBI score (r = 0.392, p < 0.01). The Hyperactivity/noncompliance subscale showed a positive moderate correlation with the total ZBI score (r = 0.467, p < 0.01). However, there was no association between the ABC-2 inappropriate speech subscale and the total ZBI score.
Correlation analysis showed a statistically significant association between the use of medication and total burden score (p < 0.05, eta = 0.187), indicating that there is a weak association between these two variables. In addition, the association between the duration of problem behaviour and total burden score was statistically significant (p < 0.05, r = 0.182), indicating that there is a weak association. There was also a statistically significant association between those registered with the Social Welfare Department and total burden score (p < 0.05, eta = 0.138), indicating a weak association between these two variables. Similarly, the association between the presence of other siblings with ASD and the total burden score was statistically significant (p < 0.05, eta = 0.130), indicating a weak association between the two variables. No other significant relationships were found with demographic variables.
For Model 1 (as shown in Table 6), there is a significant positive relationship between Irritability and caregiver burden (value of p < 0.05, B = 0.688), with a 0.688 unit increase in caregiver burden for every unit increase of irritability. Similarly, for Model 2, there is a significant positive relationship between social withdrawal and caregiver burden (value of p < 0.05, B = 0.740), with a 0.740 unit increase in caregiver burden for every unit increase of social withdrawal. For Model 3, stereotypic behaviour significantly has a positive influence on caregiver burden (value of p < 0.05, B = 1.114). This indicates that every 1 level increase in stereotypic behaviour increases 1.114 caregiver burden. For Model 4, hyperactivity/non-compliance significantly has a positive influence on caregiver burden (value of p < 0.05, B = 0.628). This indicates that every 1 level increase in hyperactivity/non-compliance increases 0.628 caregiver burden. For Model 5, the findings reveal that there is no significant effect between inappropriate speech on caregiver burden (value of p > 0.05, B = 0.553).
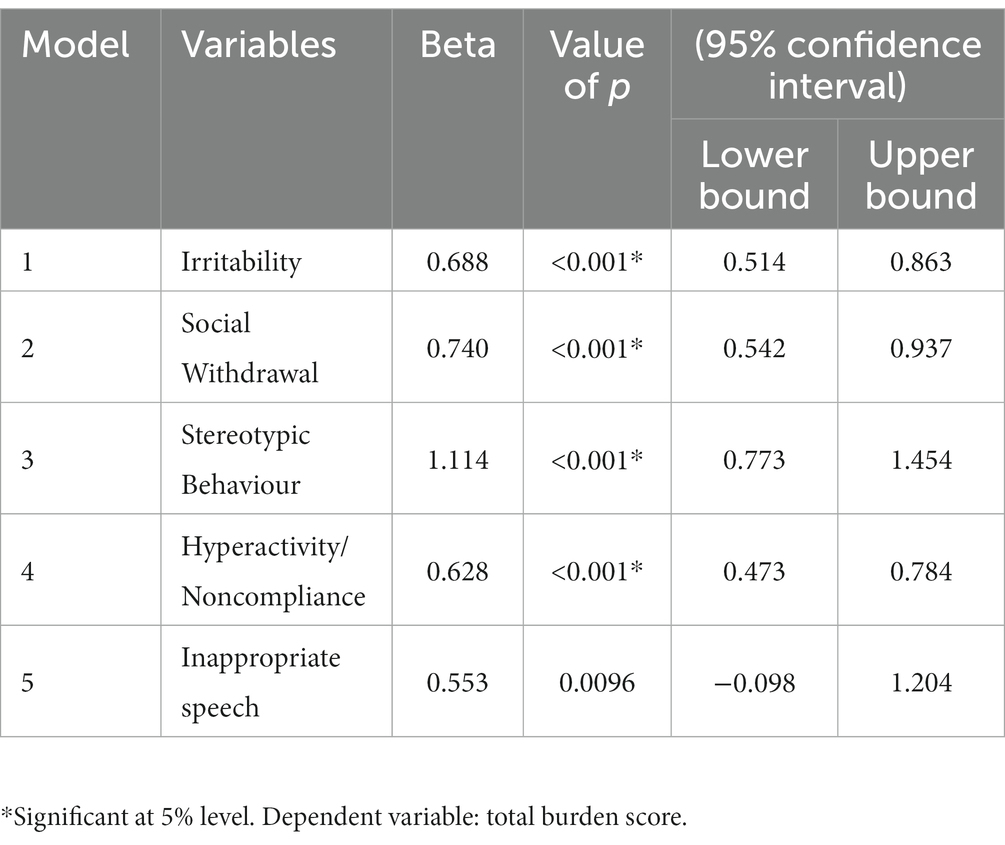
Table 6. Simple linear regression analysis.
Multiple linear regression for all five ABC-2 variables showed that only hyperactivity/ noncompliance subscale significantly predicts ZBI score. Every one score increase in the hyperactivity/noncompliance increases ZBI by 0.294 unit. Model 1 accounts for 22.3% of the variation in caregiver burden. In Model 2, the hyperactive/noncompliance domain remained a significant predictor for ZBI after further adjusted for confounders such as duration of problem behaviour, use of medications, registration with social welfare department and presence of other siblings with ASD. Every one score increase in hyperactive domain increases ZBI by 0.383 unit. Model 2 accounts for 25.6% of the variation in caregiver burden. No multicollinearity issue was detected as the VIF values for all predictors were <5.0. The results of the multiple linear regression are shown in Table 7.
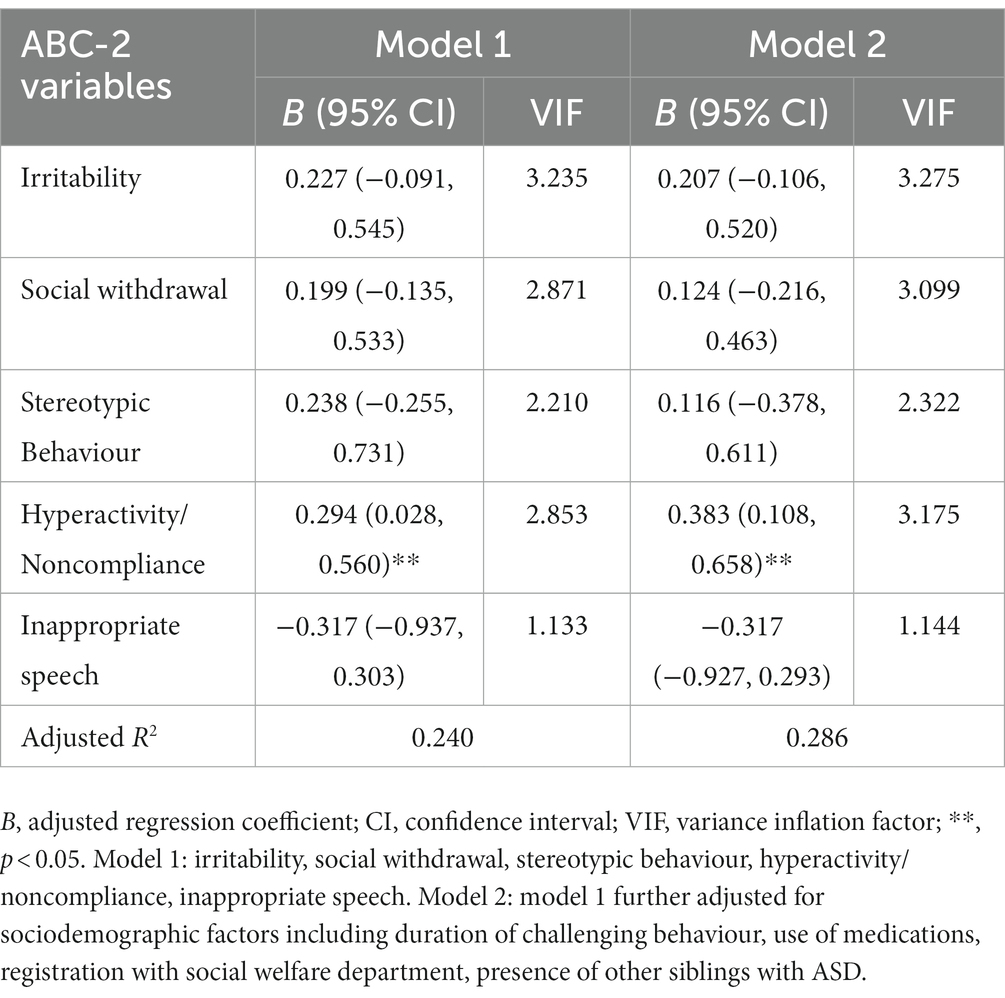
Table 7. Multiple linear regression on ABC-2 scores in relation to ZBI scores among caregiver.
This study aimed to examine the relationship between problem behaviour and caregiver burden. The result showed that nearly half of the children with ASD had at least one form of problem behaviour. More than half of the caregivers experienced caregiver burden, with the majority experiencing mild burden. Additionally, there were significant positive correlations between problem behaviour subscales (irritability, social withdrawal, stereotypic behaviour, and hyperactivity/noncompliance) and caregiver burden. Child variables such as duration of problem behaviour, use of medications, registration with the Social Welfare Department, and the presence of other siblings with ASD were associated with caregiver burden. Additionally, results from the multiple linear regression demonstrated that the hyperactivity/noncompliance subscale significantly predicted caregiver burden.
In this study, the mean age of the caregivers was 39 years. This is consistent with other previous studies done where the mean age of caregivers ranges from 38.91 to 42.5 (53–55). The latest demographic report for Malaysia shows that Malays comprise 57.9% of the population. In our study, 43% of the caregivers were Malay, which is lower than the national figure. This difference may be due to the significant presence of indigenous ethnic groups in Sarawak (56). Most of the caregivers were mothers of the child with ASD. This is consistent with other studies (54, 57). The male-to-female ratio in our study was found to be slightly higher at 5.5:1 as compared to the global estimate of 4.2:1 (58). Additionally, this study found a lower rate of psychiatric comorbidity compared to other studies previously done. Possible reasons include the low levels of mental health literacy and stigmatizing attitudes towards mental health problems among the public in Malaysia (59, 60). The stigma associated with psychiatric and neurodevelopmental disorders may possibly compel individuals to refrain from labeling their afflicted family members with disorders and under-reporting the severity of behavioural issues.
In our study, a higher prevalence of problem behaviour (40.4%) was found compared to Rzepecka et al.’s study (28%) (61). The higher prevalence found in our study could be due to the higher proportion of children with ASD in our sample compared to Rzepecka’s sample which consist of children with ASD and/or ID. Individuals with autism were found to have significantly higher levels of psychopathology than individuals with intellectual disability (62). The prevalence we found was lower compared to other studies (ranging from 72 to 93.7%) in children with ASD (4, 6, 63). This difference may be due to higher stigma and limited awareness about ASD and mental illness in Malaysia (59, 60, 64), causing caregivers to report fewer symptoms their child might be having.
Previous studies have shown that participants in clinical settings had higher ABC scores between subscales compared to those in non-clinical settings (26, 65–68). In this study, the majority of our participants were recruited from clinical settings (73.9%), with 23.1% originating from non-clinical settings. Mean scores obtained in our study differed from those in previous research on behavioural problems. Sannar et al. reported higher mean scores, likely because their study focused on children with Autism in a specialized inpatient psychiatric unit (66), who may have more severe behavioural issues than our participants who were drawn from outpatient clinics and the community. In contrast, our study found higher mean ABC-2 scores compared to a study by Kang et al. in Singapore (65). Kang et al. recruited their participants from an outpatient child developmental unit in a tertiary hospital, similar to our study. This difference could be because Singapore offers more accessible intervention services than Malaysia, resulting in fewer behavioural problems (69). In a Malaysian study examining the association between Vitamin D deficiency and behavioural symptoms in children with ASD, mean ABC-2 scores closely resembled our findings (70) with slightly elevated scores observed in irritability, social withdrawal, and hyperactivity/noncompliance subscales when compared to the group without Vitamin D deficiency at baseline. This may be due to the more similar demographic and cultural backgrounds of the participants in both studies.
In this study, most of the caregivers were found to have little or no burden. This is followed by caregivers who had mild to moderate burden. This suggests that the level of burden experienced by caregivers of children with ASD in this population was low. This is inconsistent with prior studies which found that perceived stress is moderate to high among caregivers of children with ASD (17, 23, 71–73). In Malaysia, cultural beliefs attribute having a child with ASD to past wrongdoings, and problem behaviours are perceived as bad parenting (36, 41, 64). Furthermore, individuals may view mental illness or stress as signs of weakness and incapacity (74). These prevailing beliefs and the associated stigma surrounding ASD and mental health issues can deter individuals from reporting symptoms due to the fear of judgment by others (64, 75). There are additional factors that could contribute to the lower reported burden in this study. Many studies have demonstrated the role of religious coping in dealing with stressful situations, physical and mental health challenges (35, 42, 76). In Malaysia, the major religions practiced are Islam, Christianity, and Buddhism, and their religious beliefs appear to play a significant role in helping caregivers interpret and cope positively with their child’s disability (41, 43, 64, 76). Their religious beliefs have made it easier for them to reach a stage of acceptance, giving them a sense of meaning while caring for their child with ASD (41, 76–78). However, further research is necessary to ascertain the extent to which these factors contribute to the lower perceived burden in this region.
A significant positive correlation was found between problem behaviours (irritability, social withdrawal, stereotypic behaviour and hyperactivity/non-compliance) and caregiver burden, indicating a higher level of these problem behaviours are associated with a higher caregiver burden. The results from this study are consistent with previous studies (79–83). Tomanik et al. found that mothers of children with autism reported the greatest stress when their children were more irritable, lethargic/socially withdrawn, hyperactive/non-compliant, unable to take care of themselves, and unable to communicate or interact with others (26). Similar to this study, the study failed to show a significant relationship between inappropriate speech and maternal stress. Multiple linear regression analysis showed that the hyperactivity/noncompliance domain remained a significant predictor for ZBI after further adjusted for covariates such as duration of problem behaviour, use of medications, registration with social welfare department and presence of other siblings with ASD. This supports previous research suggesting hyperactivity, noncompliance, aggression, and disruptive behaviours are significant predictors of parenting stress in children with ASD (27, 82, 84–86). Hyperactivity and disruptive behaviour are more likely to increase caregiver burden as these behaviours are more socially inappropriate. Aside from that, inappropriate speech was found to have no significant correlation with caregiver burden. Compared to externalizing behaviours, inappropriate speech may be socially less distressing and less disruptive.
A significant association was found between children with ASD receiving medications and caregiver burden. Those who receive medications are associated with greater age, more severe autism, more severe intellectual disability and increased scores in ABC (61, 87). In addition, children with ASD were reported to have higher levels of health care office visits and prescription drug use compared with children without ASD (88). It is probable that the usage of medicine indicates more severe behavioural issues, which would explain the higher burden scores and correlation between caregiver burden and medication use.
In addition, there was a significant association between the presence of other siblings with ASD in the family and caregiver burden. This is consistent with the findings of Orsmond et al., who reported that mothers caring for another child with a disability (in addition to the child with ASD) had greater levels of depression and anxiety symptoms (89). Having more than two children with chronic illness was also associated with caregivers’ burnout (90). The presence of another family member with developmental disabilities requiring specialized care will incur additional financial costs, and necessitate greater physical, emotional, and psychological support. This may possibly explain the significant association between these two variables.
This study found a significant association between the duration of problem behaviour in children with ASD and caregiver burden. There is no research that examines the association between the duration of problem behaviour and caregiver burden in children with ASD. However, a few studies showed a similar association between caregiver burden and duration of illness in other chronic illnesses in children (91–93). Previous studies also demonstrated a bidirectional relationship between behavioural problems and family stress, showing that it covaries across time (3, 33, 94–96). Ultimately, this relationship perpetuates both problem behaviour and caregiver burden.
There was a significant association between Social Welfare Department registration and total burden score. There are no previous studies that found a similar relationship between these two variables. Those registered with the Social Welfare Department are eligible for several services, including a monthly allowance, discounts on public transportation, fee waivers for medical services in government facilities and assistance with admission to special education schools. These services may alleviate the financial and psychological burdens experienced by caregivers. Caregivers are strongly encouraged to register their child with the Social Welfare Department to benefit from the services provided by the government. It is probable that those children with Social Welfare Department registration come from a lower socio-economic background. They may not have the privilege and access to early intervention programs, which may cause their symptoms to worsen. Consequently, they may require more interventional services, medical care, and admission to special education schools in comparison to individuals with less debilitating symptoms. Therefore, this could explain the significant difference and association between having Social Welfare Department registration and caregiver burden.
The present study has several limitations. The first limitation of this study is that the causal relationship between problem behaviour and caregiver burden could not be determined due to the cross-sectional nature of this study. Longitudinal studies should be done to assess the causal relationship between behavioural problems and caregivers. Another limitation of this study is the sampling method used. Convenience sampling may give rise to sampling bias. The use of convenience sampling may result in sampling bias. Caregivers who volunteered for the study might have better awareness about ASD and have less burden, making them more likely to participate than those who declined. Those who did not participate may have children with more severe behaviour problems and higher burden. Additionally, this study did not assess several crucial factors. These include caregiver medical illnesses, psychiatric comorbidities, perceived social support, religious beliefs, and coping skills, all of which could potentially influence caregiver burden. This study also did not investigate sex distribution among caregivers and its effect on the caregiving burden. As most of the caregivers in this study were mothers of children with ASD, the results may not be generalized to fathers or other family members who are caregivers. Aside from that, this study also did not assess the severity of ASD which may also affect the caregiver burden. Assessment tools to assess the severity of ASD symptoms include Autism Diagnosis Interview-Revised (ADI-R), Autism Diagnostic Observation Schedule (ADOS), and Childhood Autism Rating Scale (CARS). These assessment tools require training for administration and a longer assessment time. As a result of these factors and time limitations, the severity of ASD symptoms was not evaluated. In addition, both problem behaviour and caregiver burden were assessed using self-reported questionnaires, which is another limitation of this study. There may be bias in this study’s findings due to inaccurate reporting by the caregivers. Also, the ABC-2 tool was not validated in this context. Hence, results should be interpreted with caution and further studies are needed to evaluate its validity.
One of the strengths of this study is achieving an adequate sample size of 230. This improved the power of the study. The use of validated questionnaire such as the Zarit Burden Interview was an additional strength of the study.
In conclusion, the current study found that there was a positive association between problem behaviours (irritability, social withdrawal, stereotypic behaviour, and hyperactivity/noncompliance) and caregiver burden. Inappropriate speech was not associated with caregiver burden. Other factors that were also found to be associated with caregiver burden in this sample included the duration of problem behaviour, use of medications, the presence of other siblings with ASD in the family and being registered with the Social Welfare Department. These results underline the significance of locally tailored interventions for both the child with ASD and their caregivers. Future research should investigate the efficacy of interventions developed to assist both the child and the caregiver.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by University Kebangsaan Malaysia Research Ethics Committee and the National Medical Research Register Malaysia. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
SC, FA, and SR contributed to conception and design of the study. SC organized the database, performed the statistical analysis, and wrote the first draft of the manuscript. All authors contributed to the article and approved the submitted version.
This research received its funding from Geran Fundamental Fakulti Perubatan (FF-2021-417), UKM Research Ethics Committee, Malaysia. The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1244164/full#supplementary-material
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, D.C.: American Psychiatric Publishing. (2013).
2. Ministry of Health Malaysia (MOH). Clinical practice guidelines management of autism spectrum disorder in children and adolescents. (2014); Available at: https://www.moh.gov.my/index.php/pages/view/3962
3. Neece, CL, Green, SA, and Baker, BL. Parenting stress and child behaviour problems: a transactional relationship across time. Am J Intellect Dev Disabil. (2012) 117:48–66. doi: 10.1352/1944-7558-117.1.48
4. Chandler, S, Howlin, P, Simonoff, E, O'Sullivan, T, Tseng, E, Kennedy, J, et al. Emotional and behavioural problems in young children with autism spectrum disorder. Dev Med Child Neurol. (2016) 58:202–8. doi: 10.1111/dmcn.12830
5. Jang, J, Dixon, DR, Tarbox, J, and Granpeesheh, D. Symptom severity and challenging behaviour in children with ASD. Res Autism Spectr Disord. (2011) 5:1028–32. doi: 10.1016/j.rasd.2010.11.008
6. McTiernan, A, Leader, G, Healy, O, and Mannion, A. Analysis of risk factors and early predictors of challenging behaviour for children with autism spectrum disorder. Res Autism Spectr Disord. (2011) 5:1215–22. doi: 10.1016/j.rasd.2011.01.009
7. Ramachandram, S. Clinical characteristics and demographic profile of children with autism spectrum disorder (ASD) at child development clinic (CDC), Penang hospital. Med J Malaysia. (2019) 74:5.
8. Hartley-McAndrew, M, and Weinstock, A. Autism spectrum disorder: correlation between aberrant behaviours, EEG abnormalities and seizures. Neurol Int. (2010) 2:e10. doi: 10.4081/ni.2010.e10
9. Lundqvist, LO. Prevalence and risk markers of behaviour problems among adults with intellectual disabilities: a total population study in Örebro county. Sweden Res Dev Disabil. (2013) 34:1346–56. doi: 10.1016/j.ridd.2013.01.010
10. Nicholls, G, Hastings, R, and Grindle, C. Prevalence and correlates of challenging behaviour in children and young people in a special school setting. Eur J Spec Needs Educ. (2019) 35:1–15. doi: 10.1080/08856257.2019.1607659
11. Rattaz, C, Michelon, C, Munir, K, and Baghdadli, A. Challenging behaviours at early adulthood in autism spectrum disorders: topography, risk factors and evolution. J Intellect Disabil Res. (2018) 62:637–49. doi: 10.1111/jir.12503
12. Esteves, J, Perry, A, Spiegel, R, and Weiss, JA. Occurrence and predictors of challenging behaviour in youth with intellectual disability with or without autism. J Ment Health Res Intellect Disabil. (2021) 14:189–201. doi: 10.1080/19315864.2021.1874577
13. Tureck, K, Matson, JL, Turygin, N, and Macmillan, K. Rates of psychotropic medication use in children with ASD compared to presence and severity of problem behaviours. Res Autism Spectr Disord. (2013) 7:1377–82. doi: 10.1016/j.rasd.2013.08.003
14. Mandell, DS. Psychiatric hospitalization among children with autism spectrum disorders. J Autism Dev Disord. (2008) 38:1059–65. doi: 10.1007/s10803-007-0481-2
15. Allik, H, Larsson, JO, and Smedje, H. Health-related quality of life in parents of school-age children with asperger syndrome or high-functioning autism. Health Qual Life Outcomes. (2006) 4:1. doi: 10.1186/1477-7525-4-1
16. Kamaralzaman, S, Toran, H, Mohamed, S, and Abdullah, NB. The economic burden of families with autism spectrum disorders (ASD) children in Malaysia. J ICSAR. (2018) 2:71–7. doi: 10.17977/um005v2i12018p071
17. Alnazly, EK, and Abojedi, A. Psychological distress and perceived burden in caregivers of persons with autism spectrum disorder. Perspect Psychiatr Care. (2019) 55:501–8. doi: 10.1111/ppc.12356
18. Patel, AD, Arya, A, Agarwal, V, Gupta, PK, and Agarwal, M. Burden of care and quality of life in caregivers of children and adolescents with autism spectrum disorder. Asian J Psychiatry. (2022) 70:103030. doi: 10.1016/j.ajp.2022.103030
19. Weiss, JA, Cappadocia, MC, MacMullin, JA, Viecili, M, and Lunsky, Y. The impact of child problem behaviours of children with ASD on parent mental health: the mediating role of acceptance and empowerment. Autism. (2012) 16:261–74. doi: 10.1177/1362361311422708
20. Yacoub, E, Dowd, M, McCann, L, and Burke, L. Impact of challenging behaviour on siblings of people with autism. Adv Ment Health Intellect Disabil. (2018) 12:145–52. doi: 10.1108/AMHID-01-2018-0001
21. Chu, SY, Binti, KSNZ, Gan, CH, Fierro, V, CMH, C, and Hersh, D. “Sometimes I feel grateful…”: experiences of the adolescent siblings of children with autism spectrum disorder in Malaysia. J Autism Dev Disord. (2023) 53:795–807. doi: 10.1007/s10803-021-05184-5
22. Fazree, SDM, Zakaria, SM, and Mokhtar, DMM. Penjagaan anak kurang upaya di Klang, Selangor: pengalaman hidup dan krisis yang dialami ibu. E-BANGI J Sains Sos Dan Kemanus. (2021) 18:210–22.
23. Pandey, S, and Sharma, C. Perceived burden in caregivers of children with autism spectrum disorder. J Nepal Health Res Counc. (2018) 16:184–9. doi: 10.33314/jnhrc.v16i2.896
24. Valicenti-McDermott, M, Lawson, K, Hottinger, K, Seijo, R, Schechtman, M, Shulman, L, et al. Parental stress in families of children with autism and other developmental disabilities. J Child Neurol. (2015) 30:1728–35. doi: 10.1177/0883073815579705
25. Zakaria, SM, and NSM, Tauhaid. CABARAN MEMBESARKAN ANAK-ANAK AUTISME DARIPADA PERSPEKTIF IBU (the challenges of nurturing autistic children from the MOTHER’S perspective). J Psikol Malays (2018) (Cited April 4, 2023); 32. Available at: https://spaj.ukm.my/ppppm/jpm/article/view/319
26. Tomanik, S, Harris, GE, and Hawkins, J. The relationship between behaviours exhibited by children with autism and maternal stress. J Intellect Develop Disabil. (2004) 29:16–26. doi: 10.1080/13668250410001662892
27. McStay, RL, Dissanayake, C, Scheeren, A, Koot, HM, and Begeer, S. Parenting stress and autism: the role of age, autism severity, quality of life and problem behaviour of children and adolescents with autism. Autism Int J Res Pract. (2014) 18:502–10. doi: 10.1177/1362361313485163
28. Postorino, V, Gillespie, S, Lecavalier, L, Smith, T, Johnson, C, Swiezy, N, et al. Clinical correlates of parenting stress in children with autism Spectrum disorder and serious behavioural problems. J Child Fam Stud. (2019) 28:2069–77. doi: 10.1007/s10826-019-01423-7
29. Marsack-Topolewski, CN, and Maragakis, A. Relationship between symptom severity and caregiver burden experienced by parents of adults with autism. Focus Autism Dev Disabil. (2021) 36:57–65. doi: 10.1177/1088357620956927
30. Athari, P, Ghaedi, L, Kosnin, A, and Binti, M. Mothers’ depression and stress, severity of autism among children and family income. Int J Psychol Res. (2013) 6:98–106. doi: 10.21500/20112084.691
31. Vogan, V, Lake, JK, Weiss, JA, Robinson, S, Tint, A, and Lunsky, Y. Factors associated with caregiver burden among parents of individuals with ASD: differences across intellectual functioning. Fam Relat. (2014) 63:554–67. doi: 10.1111/fare.12081
32. Mohamad, MS, and Rosdi, NNA. Hubungan antara Tingkah laku Keibubapaan, Tekanan Psikologikal dengan Tahap Kesihatan Mental dalam kalangan Penjaga Kanak-Kanak Autisme (Relationship between Parenting Skills, Psychological Distress with Mental Health Level among Caregivers of Autism Children). J Psikol Malays. (2018), (Cited April 4, 2023); 32. Available at: https://spaj.ukm.my/ppppm/jpm/article/view/431
33. Baker, BL, McIntyre, LL, Blacher, J, Crnic, K, Edelbrock, C, and Low, C. Pre-school children with and without developmental delay: behaviour problems and parenting stress over time. J Intellect Disabil Res. (2003) 47:217–30. doi: 10.1046/j.1365-2788.2003.00484.x
34. Woodman, AC, Mawdsley, HP, and Hauser-Cram, P. Parenting stress and child behaviour problems within families of children with developmental disabilities: transactional relations across 15 years. Res Dev Disabil. (2015) 36C:264–76. doi: 10.1016/j.ridd.2014.10.011
35. Ilias, K, Cornish, K, Kummar, AS, Park, MSA, and Golden, KJ. Parenting stress and resilience in parents of children with autism spectrum disorder (ASD) in Southeast Asia: a systematic review. Front Psychol. (2018) 9:280. doi: 10.3389/fpsyg.2018.00280
36. Shorey, S, Ng, ED, Haugan, G, and Law, E. The parenting experiences and needs of Asian primary caregivers of children with autism: a meta-synthesis. Autism. (2020) 24:591–604. doi: 10.1177/1362361319886513
37. Giovagnoli, G, Postorino, V, Fatta, LM, Sanges, V, de Peppo, L, Vassena, L, et al. Behavioural and emotional profile and parental stress in preschool children with autism spectrum disorder. Res Dev Disabil. (2015) 45–46:411–21. doi: 10.1016/j.ridd.2015.08.006
38. Kramer, EJ, Kwong, K, Lee, E, and Chung, H. Cultural factors influencing the mental health of Asian Americans. West J Med. (2002) 176:227–31.
39. Department of the Premier of Sarawak. Sarawak Facts And Figures (2022). 2022. Available at: https://sarawak.gov.my/web/home/article_view/413/353/?id=382#353
40. Ravindran, N, and Myers, BJ. Cultural influences on perceptions of health, illness, and disability: a review and focus on autism. J Child Fam Stud. (2012) 21:311–9. doi: 10.1007/s10826-011-9477-9
41. Ilias, K, Cornish, K, Park, MSA, Toran, H, and Golden, KJ. Risk and resilience among mothers and fathers of primary school age children with ASD in Malaysia: a qualitative constructive grounded theory approach. Front Psychol. (2019) 9:2275. doi: 10.3389/fpsyg.2018.02275
42. Luthfi, NII, Alias, IA, and Mohamad, M. Religious coping of Malaysian Muslims with high sensory-processing sensitivity in facing the loss of loved one(s). Simulacra. (2023) 6:109–23. doi: 10.21107/sml.v6i1.19864
43. Mohamad, SP, Yusoff, MYZM, Adli, DSH, and Golden, KJ. Mental health studies on the coping strategies of Muslim parents of children with autism spectrum disorder in Malaysia (a narrative review). Malays J Med Health Sci. (2019) 15:168–77.
44. Aman, MG, and Singh, NN. Aberrant Behaviour checklist. 2nd ed. New York, USA: Slosson Educational Publication (ABC-2) (2017).
45. Frye, RE, Tippett, M, Delhey, L, and Slattery, J. Test–retest reliability and validity of the autism symptoms questionnaire. North Am J Med Sci (2016) (Cited June 16, 2022); 8. Available at: https://www.najms.com/index.php/najms/article/view/74
46. Rojahn, J, Schroeder, SR, Mayo-Ortega, L, Oyama-Ganiko, R, LeBlanc, J, Marquis, J, et al. Validity and reliability of the behaviour problems inventory, the aberrant behaviour checklist, and the repetitive behaviour scale-revised among infants and toddlers at risk for intellectual or developmental disabilities: a multi-method assessment approach. Res Dev Disabil. (2013) 34:1804–14. doi: 10.1016/j.ridd.2013.02.024
47. Norris, M, Aman, MG, Mazurek, MO, Scherr, JF, and Butter, EM. Psychometric characteristics of the aberrant behaviour checklist in a well-defined sample of youth with autism Spectrum disorder. Res Autism Spectr Disord. (2019) 62:1–9. doi: 10.1016/j.rasd.2019.02.001
48. Kaat, AJ, Lecavalier, L, and Aman, MG. Validity of the aberrant behaviour checklist in children with autism spectrum disorder. J Autism Dev Disord. (2014) 44:1103–16. doi: 10.1007/s10803-013-1970-0
49. Zarit, SH. The hidden victims of Alzheimer’s disease: families under stress. New York: New York University Press (1985).
50. Shim, VK, Drahman, I, and Ng, CG. Validation of the Malay version of Zarit burden interview (MZBI). Malays J Psychiatry, (2017), (Cited Feb 8, 2021); 26. Available at: http://mymedr.afpm.org.my/publications/60528
51. Household Income Survey Report 2022. (2022). Available at: https://www.dosm.gov.my/portal-main/release-content/household-income-survey-report--malaysia--states
52. Mukaka, M. A guide to appropriate use of correlation coefficient in medical research. Malawi Med J J Med Assoc Malawi. (2012) 24:69–71.
53. Ibrahim, MI, Bakar, RS, Sukeri, S, Rahman, AA, Othman, A, Rostenberghe, HV, et al. The unmet needs among parents of disabled children at support institutions in Kelantan, Malaysia. Malays J Med Health Sci. (2019) (Cited July 14, 2022); 15. Available at: http://mymedr.afpm.org.my/publications/80534
54. Nik Adib, NA, Ibrahim, MI, Ab Rahman, A, Bakar, RS, Yahaya, NA, Hussin, S, et al. Perceived stress among caregivers of children with autism spectrum disorder: a state-wide study. Int J Environ Res Public Health. (2019) 16:E1468. doi: 10.3390/ijerph16081468
55. Picardi, A, Gigantesco, A, Tarolla, E, Stoppioni, V, Cerbo, R, Cremonte, M, et al. Parental burden and its correlates in families of children with autism spectrum disorder: a multicentre study with two comparison groups. Clin Pract Epidemiol Ment Health. (2018) 14:143–76. doi: 10.2174/1745017901814010143
56. Ministry of Economy. Media statement for the report of demographic statistics Malaysia, second quarter 2023. Department of Statistics Malaysia; (2023). Available at: https://www.dosm.gov.my/uploads/release-content/file_20230809104845.pdf
57. ten Hoopen, LW, de Nijs, PFA, Duvekot, J, Greaves-Lord, K, Hillegers, MHJ, Brouwer, WBF, et al. Children with an autism spectrum disorder and their caregivers: capturing health-related and care-related quality of life. J Autism Dev Disord. (2020) 50:263–77. doi: 10.1007/s10803-019-04249-w
58. Zeidan, J, Fombonne, E, Scorah, J, Ibrahim, A, Durkin, MS, Saxena, S, et al. Global prevalence of autism: a systematic review update. Autism Res. (2022) 15:778–90. doi: 10.1002/aur.2696
59. Munawar, K, Mukhtar, F, Choudhry, FR, and Ng, ALO. Mental health literacy: a systematic review of knowledge and beliefs about mental disorders in Malaysia. Asia-Pac Psychiatry. (2022) 14:e12475. doi: 10.1111/appy.12475
60. Low, HM, Lee, LW, Ahmad, AC, Ghazali, EE, Tan, PK, and Lee, ASS. A survey of lay knowledge of autism spectrum disorder in Malaysia. J Sains Kesihat Malays. (2021) 19:49–57. doi: 10.17576/jskm-2021-1901-06
61. Rzepecka, H, McKenzie, K, McClure, I, and Murphy, S. Sleep, anxiety and challenging behaviour in children with intellectual disability and/or autism spectrum disorder. Res Dev Disabil. (2011) 32:2758–66. doi: 10.1016/j.ridd.2011.05.034
62. Brereton, AV, Tonge, BJ, and Einfeld, SL. Psychopathology in children and adolescents with autism compared to young people with intellectual disability. J Autism Dev Disord. (2006) 36:863–70. doi: 10.1007/s10803-006-0125-y
63. Ooi, YP, Tan, ZJ, Lim, CX, Goh, TJ, and Sung, M. Prevalence of behavioural and emotional problems in children with high-functioning autism spectrum disorders. Aust N Z J Psychiatry. (2011) 45:370–5. doi: 10.3109/00048674.2010.534071
64. Teo, JX, and Lau, B. Parental perceptions, attitudes and involvement interventions for autism spectrum disorders in Sarawak, Malaysia. Disabil CBR Incl Dev. (2018) 1:26–46. doi: 10.5463/dcid.v1i1.664
65. Kang, YQ, Teo, CM, Tan, MLN, Aw, MM, Chan, YH, and Chong, SC. Feeding difficulties in Asian children with autism spectrum disorder. Pediatr Neonatol. (2022) 63:48–56. doi: 10.1016/j.pedneo.2021.06.015
66. For the Autism and Developmental Disorders Inpatient Research Collaborative (ADDIRC)Sannar, EM, Palka, T, Beresford, C, Peura, C, Kaplan, D, et al. Sleep problems and their relationship to maladaptive behaviour severity in psychiatrically hospitalized children with autism Spectrum disorder (ASD). J Autism Dev Disord. (2018) 48:3720–6. doi: 10.1007/s10803-017-3362-3
67. Ferguson, SJ. Quality of life and aberrant behaviours in youth on the autism spectrum. San Francisco State University; (2021) (Cited Aug 20, 2023). Available at: http://hdl.handle.net/20.500.12680/4x51hq598
68. Griffin, ZAM, Boulton, KA, Thapa, R, DeMayo, MM, Ambarchi, Z, Thomas, E, et al. Atypical sensory processing features in children with autism, and their relationships with maladaptive behaviours and caregiver strain. Autism Res Off J Int Soc Autism Res. (2022) 15:1120–9. doi: 10.1002/aur.2700
69. Han, E, Tan, MMJ, Crane, L, and Legido-Quigley, H. A qualitative study of autism services and supports in Singapore: perspectives of service providers, autistic adults and caregivers. Autism. (2021) 25:2279–90. doi: 10.1177/13623613211016112
70. Jayanath, S, Fong, CY, and Sarvananthan, R. Autism spectrum disorder and vitamin D status: a cross-sectional study of children in a developing country in Southeast Asia. Res Autism Spectr Disord. (2021) 84:101786. doi: 10.1016/j.rasd.2021.101786
71. Baykal, S, Karakurt, MN, Çakır, M, and Karabekiroğlu, K. An examination of the relations between symptom distributions in children diagnosed with autism and caregiver burden, anxiety and depression levels. Community Ment Health J. (2019) 55:311–7. doi: 10.1007/s10597-018-0343-8
72. Cetinbakis, G, Bastug, G, and Ozel-Kizil, ET. Factors contributing to higher caregiving burden in Turkish mothers of children with autism spectrum disorders. Int J Dev Disabil. (2020) 66:46–53. doi: 10.1080/20473869.2018.1478630
73. Abdul Manan, AI, Amit, N, Said, Z, and Ahmad, M. The influences of parenting stress, children behavioural problems and children quality of life on depression symptoms among parents of children with autism: preliminary findings. J Sains Kesihat Malays. (2018) 16:137–43. doi: 10.17576/jskm-2018-16si-19
74. Ong, WJ, Shahwan, S, Goh, CMJ, Tan, GTH, Chong, SA, and Subramaniam, M. Daily encounters of mental illness stigma and individual strategies to reduce stigma – perspectives of people with mental illness. Front Psychol. (2020) 11:590844. doi: 10.3389/fpsyg.2020.590844
75. Chung, KM, Ebesutani, C, Bang, HM, Kim, J, Chorpita, BF, Weisz, JR, et al. Parenting stress and child behaviour problems among clinic-referred youth: cross-cultural differences across the US and Korea. Child Psychiatry Hum Dev. (2013) 44:460–8. doi: 10.1007/s10578-012-0340-z
76. Yaacob, WNW, Yaacob, LH, Zulkifli, MM, and Muhamad, R. A journey towards resilience: coping strategies adopted by parents with children having autism Spectrum disorder in Northeast Malaysia. Int J Environ Res Public Health. (2022) 19:2458. doi: 10.3390/ijerph19042458
77. Ilias, K, Liaw, JHJ, Cornish, K, Park, MSA, and Golden, KJ. Wellbeing of mothers of children with “A-U-T-I-S-M” in Malaysia: an interpretative phenomenological analysis study. J Intellect Develop Disabil. (2017) 42:74–89. doi: 10.3109/13668250.2016.1196657
78. Ting, SH, and Chuah, HK. Parents’ recognition of autistic behaviour and their coping strategies: a case study at Sarawak autistic association. 7, 52-65. Malays J Soc Policy Soc. (2010) 7:52–65.
79. Siu, QKY, Yi, H, Chan, RCH, Chio, FHN, Chan, DFY, and Mak, WWS. The role of child problem behaviours in autism spectrum symptoms and parenting stress: a primary school-based study. J Autism Dev Disord. (2019) 49:857–70. doi: 10.1007/s10803-018-3791-7
80. Hall, HR, and Graff, JC. Maladaptive behaviours of children with autism: parent support, stress, and coping. Issues Compr Pediatr Nurs. (2012) 35:194–214. doi: 10.3109/01460862.2012.734210
81. Firth, I, and Dryer, R. The predictors of distress in parents of children with autism spectrum disorder. J Intellect Develop Disabil. (2013) 38:163–71. doi: 10.3109/13668250.2013.773964
82. Barroso, NE, Mendez, L, Graziano, PA, and Bagner, DM. Parenting stress through the lens of different clinical groups: a systematic review & meta-analysis. J Abnorm Child Psychol. (2018) 46:449–61. doi: 10.1007/s10802-017-0313-6
83. Bradshaw, J, Gillespie, S, McCracken, C, King, BH, McCracken, JT, Johnson, CR, et al. Predictors of caregiver strain for parents of children with autism spectrum disorder. J Autism Dev Disord. (2021) 51:3039–49. doi: 10.1007/s10803-020-04625-x
84. Lecavalier, L, Leone, S, and Wiltz, J. The impact of behaviour problems on caregiver stress in young people with autism spectrum disorders. J Intellect Disabil Res JIDR. (2006) 50:172–83. doi: 10.1111/j.1365-2788.2005.00732.x
85. Huang, CY, Yen, HC, Tseng, MH, Tung, LC, Chen, YD, and Chen, KL. Impacts of autistic behaviours, emotional and behavioural problems on parenting stress in caregivers of children with autism. J Autism Dev Disord. (2014) 44:1383–90. doi: 10.1007/s10803-013-2000-y
86. Olson, L, Chen, B, Ibarra, C, Wang, T, Mash, L, Linke, A, et al. Externalizing behaviours are associated with increased parenting stress in caregivers of young children with autism. J Autism Dev Disord. (2022) 52:975–86. doi: 10.1007/s10803-021-04995-w
87. Aman, MG, Lam, KSL, and Collier-Crespin, A. Prevalence and patterns of use of psychoactive medicines among individuals with autism in the autism Society of Ohio. J Autism Dev Disord. (2003) 33:527–34. doi: 10.1023/A:1025883612879
88. Lavelle, TA, Weinstein, MC, Newhouse, JP, Munir, K, Kuhlthau, KA, and Prosser, LA. Economic burden of childhood autism spectrum disorders. Pediatrics. (2014) 133:e520–9. doi: 10.1542/peds.2013-0763
89. Orsmond, GI, Lin, LY, and Seltzer, MM. Mothers of adolescents and adults with autism: parenting multiple children with disabilities. Intellect Dev Disabil. (2007) 45:257–70. doi: 10.1352/1934-9556(2007)45[257:MOAAAW]2.0.CO;2
90. Ahmadi, B, Sabery, M, and Adib-Hajbaghery, M. Burnout in the primary caregivers of children with chronic conditions and its related factors. J Client-Centered Nurs Care. (2021) 7:139–48. doi: 10.32598/JCCNC.7.2.360.1
91. Cousino, MK, and Hazen, RA. Parenting stress among caregivers of children with chronic illness: a systematic review. J Pediatr Psychol. (2013) 38:809–28. doi: 10.1093/jpepsy/jst049
92. Piran, P, Khademi, Z, Tayari, N, and Mansouri, N. Caregiving burden of children with chronic diseases. Electron Physician. (2017) 9:5380–7. doi: 10.19082/5380
93. Pinquart, M. Parenting stress in caregivers of children with chronic physical condition-a meta-analysis. Stress Health J Int Soc Investig Stress. (2018) 34:197–207. doi: 10.1002/smi.2780
94. Osborne, LA, and Reed, P. The relationship between parenting stress and behaviour problems of children with autistic spectrum disorders. Except Child. (2009) 76:54–73. doi: 10.1177/001440290907600103
95. The Pathways in ASD Study TeamZaidman-Zait, A, Mirenda, P, Duku, E, Szatmari, P, Georgiades, S, et al. Examination of bidirectional relationships between parent stress and two types of problem behaviour in children with autism Spectrum disorder. J Autism Dev Disord. (2014) 44:1908–17. doi: 10.1007/s10803-014-2064-3
Keywords: problem behaviours, caregiver burden, children, autism, cross-sectional study, Sarawak (Malaysia)
Citation: Chua SY, Abd Rahman FN and Ratnasingam S (2023) Problem behaviours and caregiver burden among children with Autism Spectrum Disorder in Kuching, Sarawak. Front. Psychiatry. 14:1244164. doi: 10.3389/fpsyt.2023.1244164
Edited by:
Nicolás Ruiz Robledillo, University of Alicante, SpainReviewed by:
Ayşe Kılınçaslan, Istanbul University, TürkiyeCopyright © 2023 Chua, Abd Rahman and Ratnasingam. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fairuz Nazri Abd Rahman, ZmFpcnV6bkBwcHVrbS51a20uZWR1Lm15
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.