
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 04 August 2023
Sec. Public Mental Health
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1224551
 Kevin F. Boehnke1,2,3*
Kevin F. Boehnke1,2,3* Kasey Cox1Cody Weston4Moss Herberholz5
Kasey Cox1Cody Weston4Moss Herberholz5 Nicolas Glynos1,3
Nicolas Glynos1,3 Nicholas Kolbman1,3
Nicholas Kolbman1,3 Christopher W. Fields1,3Julie Barron6,7,8Daniel J. Kruger1,3,9
Christopher W. Fields1,3Julie Barron6,7,8Daniel J. Kruger1,3,9Introduction: There is substantial public interest in psychedelics as potential treatments for psychiatric conditions. However, most psychedelics are criminalized under federal law in the USA, so it is unclear whether use occurs with clinical support. Our objective was to assess whether naturalistic psychedelic use occurs with clinical support, interactions between those using psychedelics and healthcare providers (psychiatrist, therapist, or primary physicians), and use characteristics.
Methods: We conducted an online, anonymous, confidential, cross-sectional survey of adults reporting psychedelic use (N = 1221) through a psychedelics advocacy event and social media between 9/18/2022 and 11/5/2022. We assessed participant disclosure of psychedelic use with their psychiatric care provider (PsyCP) and/or primary care provider (PCP), desire for provider support, access to support, and rate of taking prescribed psychoactive medications alongside psychedelics.
Results: Among participants with such care providers, 22% disclosed psychedelic use to their PCP vs. 58% to their PsyCP. Participants were less confident in PCP vs. PsyCP ability to integrate psychedelics into treatment. Common reasons for nondisclosure included stigma, inadequate provider knowledge, and legal concerns. 23% reported taking psychedelics on the same day as potentially interacting psychiatric medications (e.g., anxiolytics, antidepressants). Despite 81% of participants desiring therapist support during psychedelic experiences, only 15% had received such support.
Discussion: Our results show that psychedelic use is generally disconnected from primary and psychiatric clinical care. This disconnection may result in safety issues, including inadequate screening for contraindicated conditions, lack of support during emergent adverse events, and drug interactions. Enhanced clinical education and orienting drug policy towards known harms and benefits of psychedelics is needed.
The field of psychedelic research has grown rapidly in the past decade, in part because of a changing political landscape and an overall desire for effective, alternative pharmacologic therapies for psychiatric conditions (1). Clinical trials have demonstrated a promising future for psychedelic-assisted psychotherapy, and both healthcare providers and the general public demonstrate an interest in the potential of these therapies (2, 3). Indeed, psilocybin administration, in concert with professional therapeutic support, has shown promising preliminary results for the treatment of major depression and treatment resistant depression (4–6), depression and anxiety in patients with life-threatening cancer (7–9), as well as alcohol and tobacco dependence (10–12). Antidepressant and anxiolytic effects as well as improvements in post-traumatic stress disorder symptoms have also been reported following use of other psychedelics including MDMA (3,4-methylenedioxymethamphetamine) (13, 14), the N,N-Dimethyltryptamine (DMT)-containing beverage ayahuasca (15, 16), ketamine (17), and lysergic acid diethylamide (LSD) (18). However, these compounds are not without risks: despite possible systematic underreporting of adverse events in clinical trials, there have been several known cases of serious adverse events such as suicidal ideation (5). Further, the psychological vulnerability and suggestibility elicited by psychedelics requires thoughtful care and support when used in the context of therapeutic relationships, as displayed by documented cases of abuse by psychedelic therapists, even in clinical trial settings (19, 20).
New legislation in Oregon, Colorado, and numerous municipalities in the U.S. has begun to decriminalize use of psychedelics, and national trends show an uptick in self-administered naturalistic psychedelic use (1, 21). These laws typically remove criminal penalties for possession of psychedelics but do not explicitly enable a commercial marketplace. While Oregon and Colorado legislation included provisions to allow psilocybin-assisted therapy treatment centers under providers with specific training, Oregon’s program just opened and Colorado’s is still under development. Elsewhere, naturalistic use typically occurs without healthcare provider oversight and is often for mental health reasons. For example, we recently conducted an online survey of 1,435 individuals, over half of whom used psychedelics for psychiatric conditions, most commonly anxiety and depression. In this survey, over 70% of participants never discussed their psychedelic use with their primary healthcare professional, although ~80% of participants said they would be very or extremely likely to seek support from a therapeutic provider for their psychedelic experience if one were legal and available (22). The main reasons for not disclosing use were due to stigma, legal concerns, and perceptions that their healthcare providers would be unable to successfully integrate psychedelics into their treatment. Although understandable in the current legal climate, this lack of communication raises concerns as there are several potential risks of unmonitored use, especially in individuals with conditions such as psychotic or bipolar disorders, post-traumatic stress disorder, or valvular heart disease, as well as among those taking medications that may interact with psychedelics, such as antidepressants or anxiolytics (23, 24).
Many individuals in this previous report also used psychedelics for psychiatric conditions – most commonly anxiety and depression (22). Unfortunately, there is minimal literature on the interactions between mental health providers and patients using psychedelics naturalistically. A recent survey of US-based clinical psychologists reported that nearly ⅔ of respondents did not have a clear understanding of psychedelic effects and would need to seek additional support to work with patients using psychedelics (2). Similarly, a 2021 survey of psychiatrists highlighted concerns about the lack of trained providers available for implementing psychedelic-based treatments (3). However, we are unaware of any reports documenting the other side of the therapeutic relationship – i.e., patient perspectives on interactions with psychiatric health providers about psychedelics.
Thus, in this report we explore the perceptions and preferences of individuals regarding psychedelic use in the context of their own general and mental healthcare. Specifically, we explore participants’ overall desire for provider support, access to support, preferences for professional versus underground settings, and their decisions to disclose psychedelic use with their psychiatric care providers (PsyCP) and/or primary care provider (PCP). We also investigated patient-reported combinations of taking prescribed psychoactive medications alongside psychedelics. As most therapeutic psychedelic research has explored effects on mental health conditions, we hypothesized that individuals would be more likely to discuss naturalistic use of psychedelics in the setting of psychiatric care when compared to primary care. We anticipate, however, that patients have low confidence in their providers’ knowledge about and ability to integrate psychedelics into their treatment, even though there is an overall desire for the support of trained providers.
We recruited respondents for this survey study via a confidential, anonymous survey link (Qualtrics, Provo, UT) that was open from September 18th to November 5th, 2022. Study recruitment occurred in two venues: (1) in person and via posted advertisements at a psychedelic advocacy event in Ann Arbor, MI and (2) online via email listservs and social media platforms such as Facebook and Reddit. We enabled the “Prevent Ballot Box Stuffing” setting in Qualtrics to prevent duplicate responses. To participate, individuals needed to be >18 years, report past psychedelic use, and live in the United States.
As described previously, we developed this survey collaboratively with input from various stakeholders, including therapists, psychedelic advocacy groups, and academics experienced in survey design and psychedelic research (25). The current study reports on components of this survey that investigated psychedelic use patterns as well as interactions related to psychedelics with healthcare providers, including PCPs and PsyCPs. We collected sociodemographic information and any past medical diagnoses of physical (e.g., cancer, diabetes) or mental health conditions (e.g., depression, anxiety, addiction), as well as information on psychedelic consumption (frequency of consumption, types of psychedelics consumed).
In addition to domains described above, we assessed how participants interacted with their PCP about psychedelic use. These included questions about whether participants had disclosed psychedelic use to their PCP, and their confidence in their PCP’s ability to integrate psychedelics into a treatment plan. Confidence level was assessed via a 5-point Likert scale, which ranged from “Not at all” to “Completely” confident. Those who did not disclose psychedelic use to their PCP were asked for rationale of non-disclosure, with options including privacy, legal concerns, stigma, and other choices.
Given that most naturalistic use of psychedelics was for mental health reasons (22), we asked participants about their interactions with PsyCPs. We used a similar battery of questions to those described above, with further questions about whether and what kind of psychiatric medications participants took or had taken on the same day as using psychedelics, as some medications may be contraindicated due to safety concerns and/or may blunt psychedelic effects (e.g., benzodiazepines, SSRIs) (26, 27). Participants who disclosed taking psychiatric medications on the same day as psychedelics were asked whether they believed there were any risks of combining these medications with psychedelics.
We asked participants about whether they had preparatory support before, during, and/or after psychedelic experiences, their likelihood of using psychedelics with a therapeutic provider (licensed or underground) and whether they had consumed psychedelics with a trained therapist or healthcare professional. Finally, participants were asked whether they thought that therapists and healthcare providers needed to experience psychedelics themselves in order to guide others, with responses on 5-point Likert scale questions ranging from “strongly disagree” to “strongly agree.”
A full list of the survey questions is provided in the appendix.
We characterized the study sample using descriptive statistics. Categorical variables are reported as n (%), and continuous variables are reported as mean ± SD and range. Measures with Likert scales (e.g., how confident participants were in their healthcare provider’s ability to integrate cannabis into treatment) were analyzed continuously. Using independent sample t-tests (effect sizes calculated using Cohen’s d statistic), we assessed whether participants who had disclosed psychedelic use to their PCP or PsyCP reported differences in their perceptions of whether they had adequate preparation for, support during, and support following psychedelic experiences. All analyses were conducted via SPSS version 27 (IBM Corp. 2020).
All surveys and procedures were approved by University of Michigan Health and Behavioral Sciences Institutional Review Board under the protocol HUM00205639 prior to data collection. Participants could withdraw at any time and were not compensated. Snacks were available at the advocacy event recruitment table to attract participant attention and interest.
Overall, 1,287 of 2,151 initiated surveys were completed (59.8% completion). Of these, n = 66 participants reported never taking psychedelics, leaving a final study sample of N = 1,221 individuals. These participants were 48% women, largely white (85%), 39 ± 12 years old on average, and 59% had a bachelor’s degree or higher level of education (Table 1). Only n = 17 (1.4%) lived in Oregon, the only state with decriminalized psychedelics at the time the survey was live. Most (67.2%) participants used psychedelics twice a year or more frequently, 23.7% used psychedelics once a month or more often. About one-fifth (18.2%) of participants had only used psychedelics once or had not used psychedelics in the past 5 years. The most used psychedelics were psilocybin mushrooms (93.4%), LSD (66.6%), and MDMA/MDA (57.0%). Smaller proportions of participants had used substances such as Ketamine (32.0%), DMT (30.5%), Salvia divinorum or salvinorin A (25.3%), mescaline (19.5%), other synthetic phenethylamines (14.1%), or ayahuasca (13.7%). Participants used an average of three different psychedelics (SD = 3), and 23.9% had used six or more different psychedelics. Most (85.7%) had used moderate or high doses of psychedelics while 14.3% had only used microdoses.
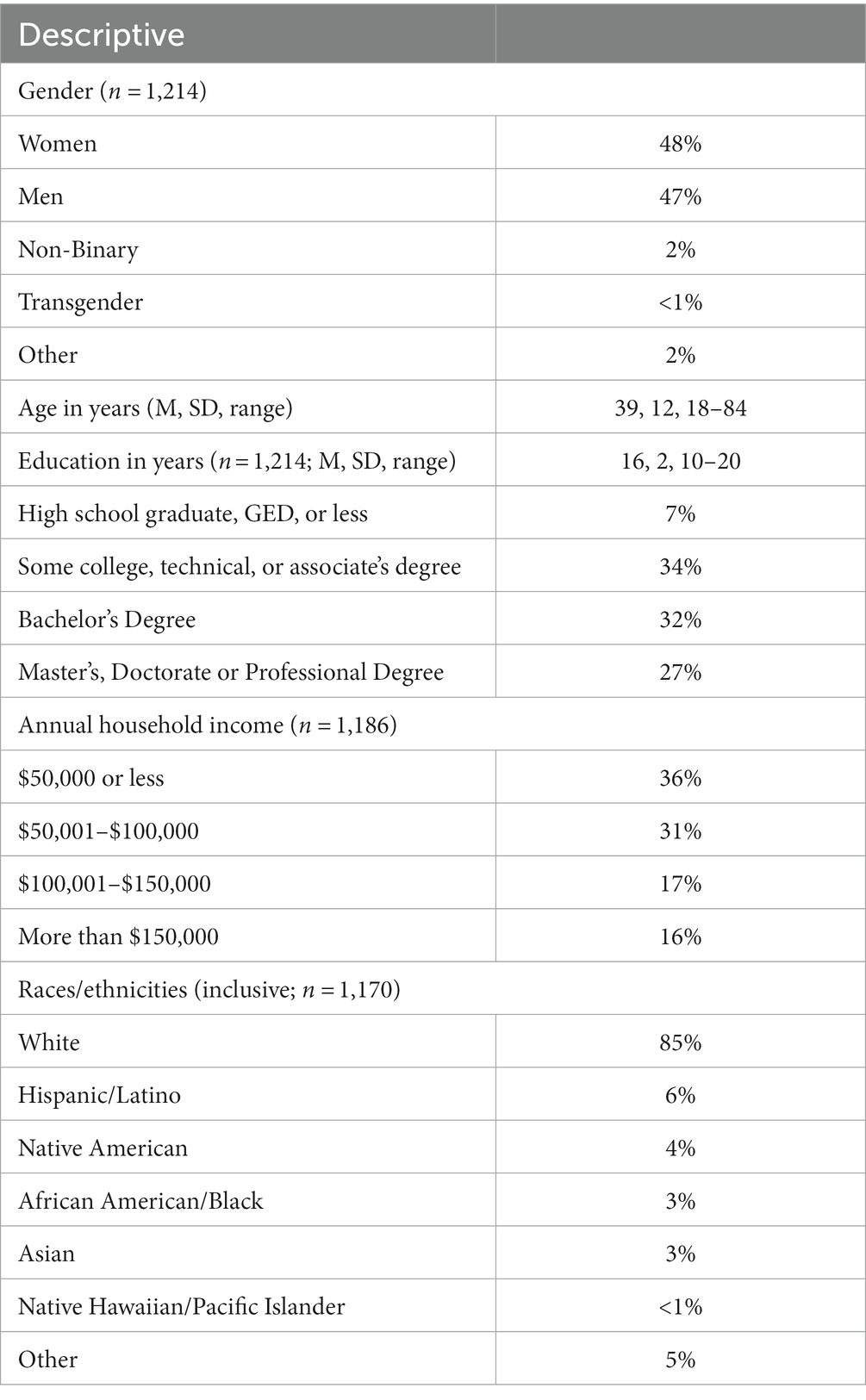
Table 1. Participant sociodemographics.
The most common past diagnoses cited by participants were depression (62%), anxiety (52%), and attention deficit hyperactivity disorder (ADHD, 27%). Overall, 22% of participants had discussed their psychedelic use with their PCP, while among the subset of n = 274 participants who reported having a PsyCP, 58% had discussed their psychedelic use with this PsyCP (Table 2). Compared to PCPs, participants were significantly more confident in their PsyCP’s ability to integrate psychedelics into treatment (mean difference = 0.66, 95% CI: 0.46–0.87, p < 0.001). The most common rationale for not disclosing psychedelic use to either PCPs or PsyCPs was stigma (59% for PCP and 70% for PsyCP).
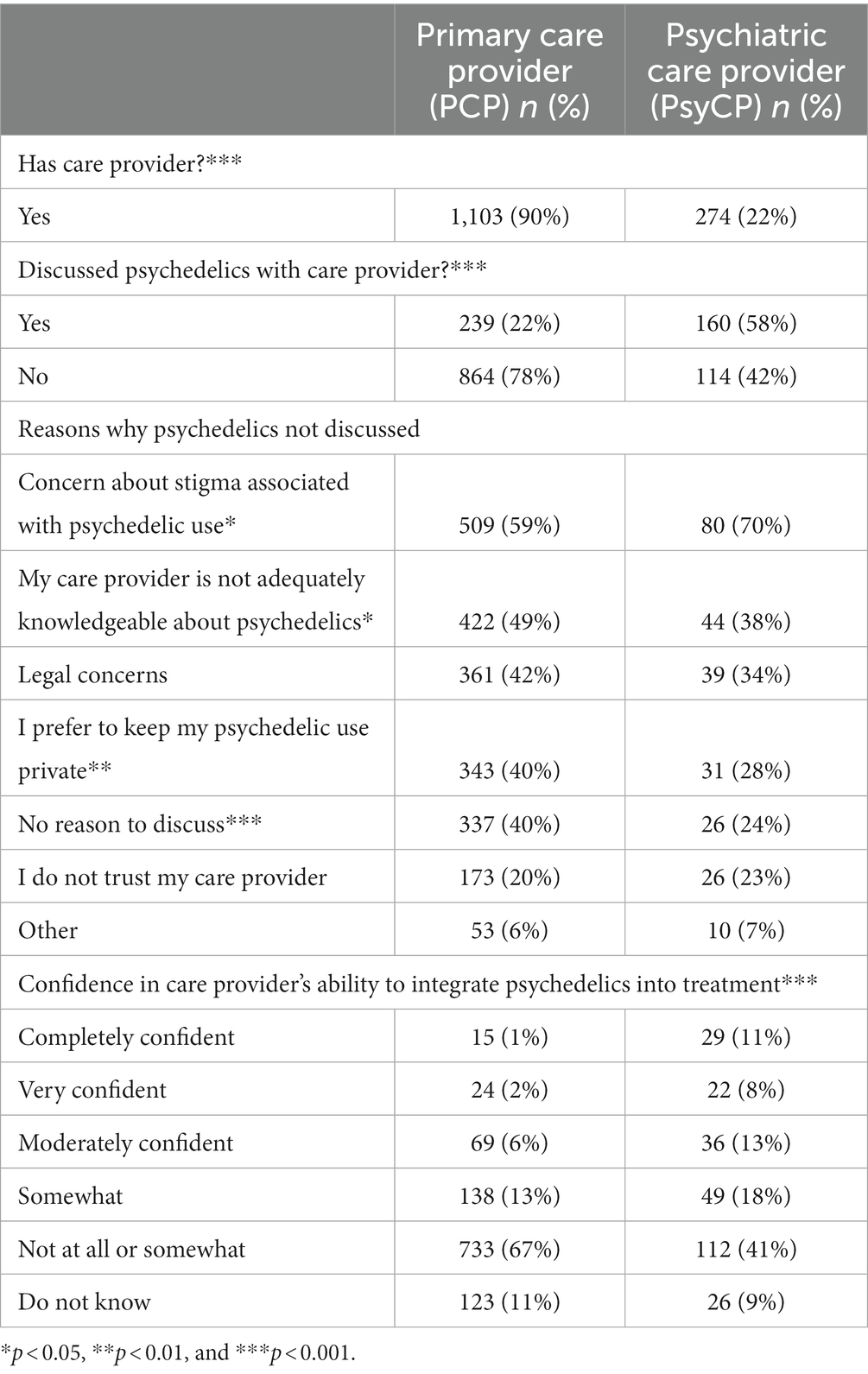
Table 2. Interactions with healthcare providers.
Overall, 23% of participants reported taking psychiatric medications on the day of their psychedelic experience (Table 3), including antidepressants (71%), stimulants (19%), and anxiolytics (13%). Fifty-four percent of those who did so reported that combining medications with psychedelics had risks. Although most participants believed that the presence of a trained therapist or healthcare professional was important to a successful psychedelic experience, only 15% of participants reported having used psychedelics under such settings (Table 4). Most participants also indicated that they would use psychedelics with the support of either a legal (81%) or underground (71%) therapist if one were available. The most common reasons for not seeking out a healthcare provider in this context were being uncertain of where to find that support (51%) or lack of affordability (28%). Notably, 75%–85% of participants agreed or strongly agreed that therapists or healthcare providers who were offering support during psychedelic experiences should have experience using psychedelics themselves.
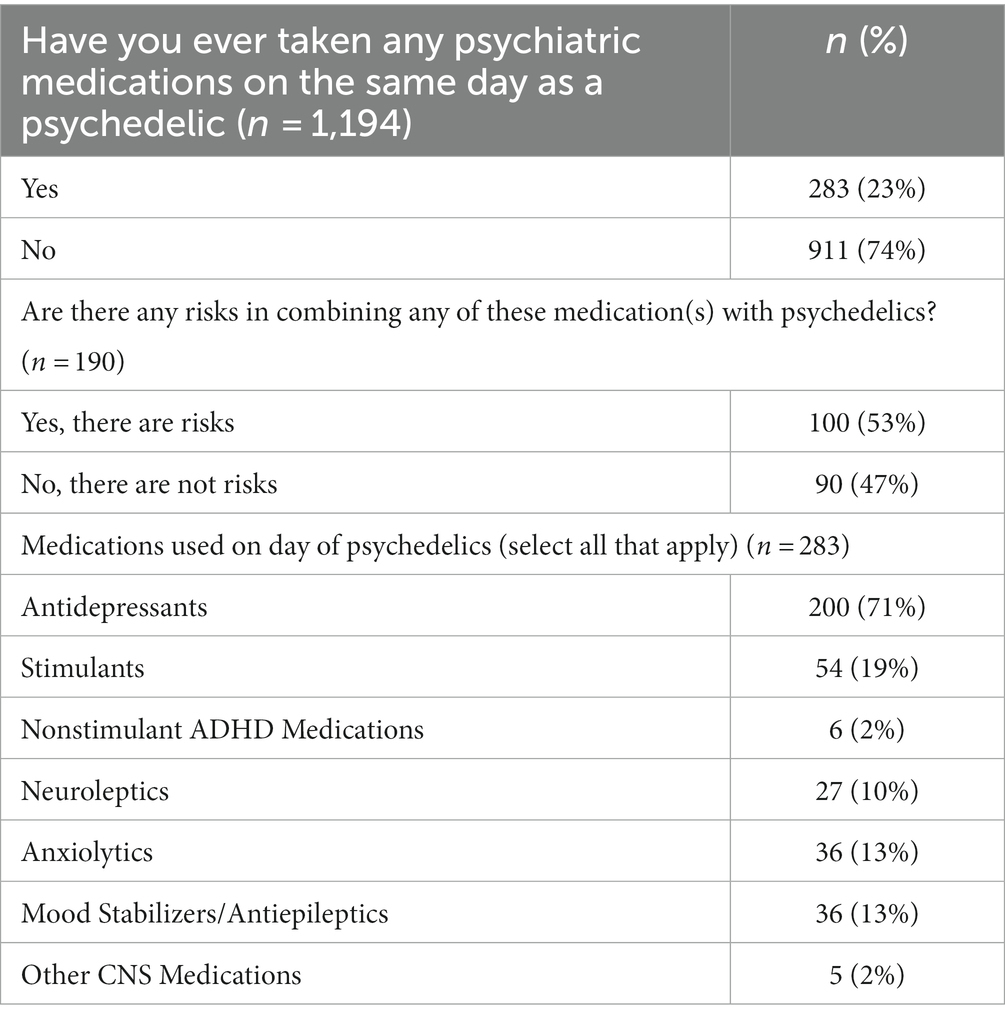
Table 3. Psychiatric medication use with psychedelics.
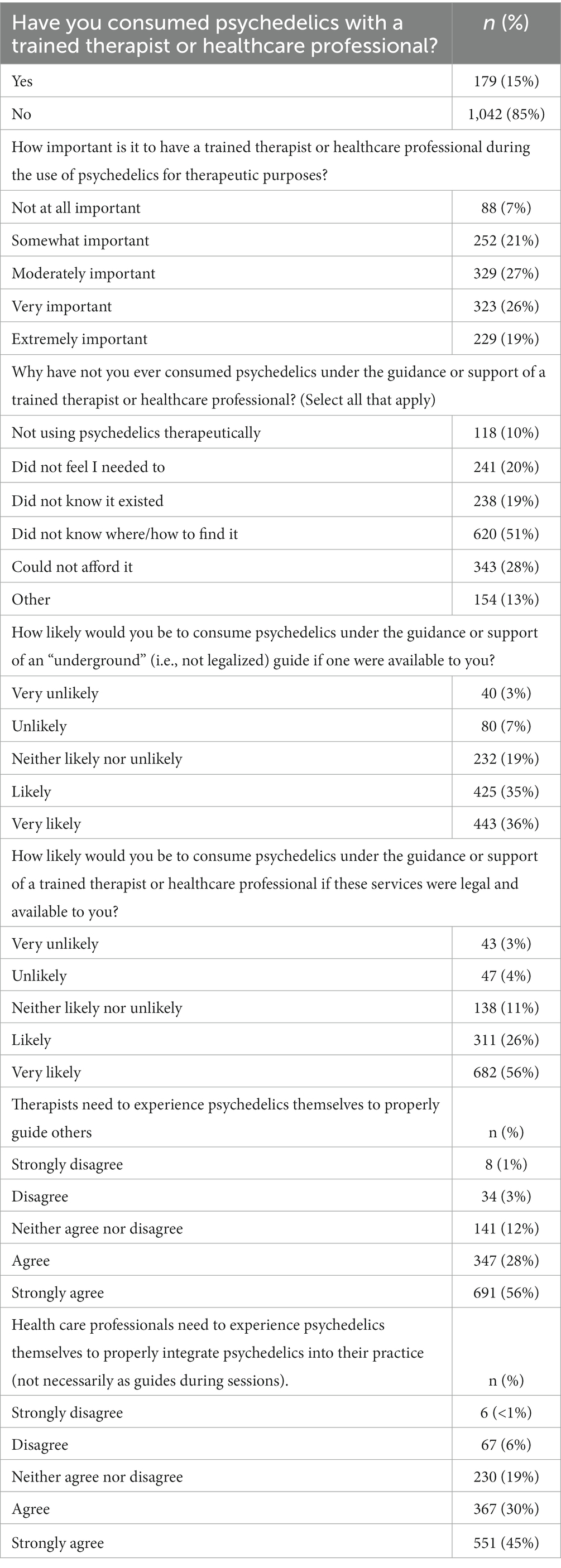
Table 4. Experiences with and attitudes toward taking psychedelics therapeutically.
Finally, 70% of participants reported always or often having adequate preparation for a psychedelic experience, 51% reported always or often having adequate support during psychedelic experiences, and 48% reported always or often having adequate support after a psychedelic experience (Table 5). The most common reason people reported not having adequate preparation or support was because they did not need it (35%), were not using psychedelics therapeutically (28%), or did not know where or how to find that support (28%). Those who discussed psychedelics with their primary healthcare provider were more likely to believe that they had adequate preparation for a psychedelic experience (t(1096) = 3.65, p < 0.001, d = 0.27), support during a psychedelic experience (t(1095) = 2.89, p = 0.002, d = 0.21), and support after a psychedelic experience (t(1095) = 3.74, p < 0.001, d = 0.27). There were no differences in perceived preparation adequacy (t(272) = 1.55, p = 0.001, d = 0.19), support during a psychedelic experience (t(272) = 0.41, p = 0.679, d = 0.05), or support after a psychedelic experience (t(272) = 0.96, p = 0.340, d = 0.12), by whether participants with a PsyCP disclosed their psychedelic use.

Table 5. Participant perceptions of support surrounding the psychedelic experience.
To the best of our knowledge, this is the first survey to explore participants’ interactions with their PsyCP around psychedelics. Consistent with our hypothesis, a considerably higher percentage of participants reported discussing psychedelics with their PsyCP compared to their PCP, and participants reported greater confidence in their PsyCP’s ability to integrate psychedelics into clinical care vs. their PCP. However, this confidence was still quite low, and over 20% of participants reported taking potentially interacting psychiatric medications with psychedelics on the same day. Our findings also uncover that while many people desire access to a therapist or guide for their psychedelic experiences, half or more of participants reported adequate preparation before, support during, and integration of their psychedelic experiences. Lastly, we report desired characteristics of healthcare providers who work with patients using psychedelics, which include personal experience with psychedelics and competence in the domain of psychedelic knowledge. Taken together, these findings highlight key areas for future research and policy efforts to enhance safety and provide additional supports for clinicians interacting with patients who use psychedelics.
Disclosure of psychedelics use to PsyCPs was higher than toward PCPs, perhaps afforded by the narrowed scope on mental health and often longer appointments. Still, respondents reported barriers to disclosure, including stigma and legal concerns. This concern is valid as prescription of controlled substances might reasonably be withheld by providers due to concerns about misuse of an illegal drug (i.e., psychedelics). Participants also felt that their care providers were not adequately knowledgeable about psychedelics, which aligns with a 2022 survey that examined psychiatrists’ knowledge of psychedelics and found that the average score was 4.2 ± 1.8 out of a possible 8 points (3). At that time, their most pronounced knowledge gaps were in an overestimation of the prevalence of hallucinogen use disorder and a limited awareness of the current status of psychedelic research.
This low rate of disclosure may affect the safety of psychedelic experiences. Indeed, despite many participants believing there were risks associated with mixing psychedelics and psychiatric medications, 23% of participants reported using psychiatric medications on the same day as a psychedelic, most commonly antidepressants, stimulants, and benzodiazepines. Many medications, especially antidepressants, likely interact with classical psychedelics (26). From a safety standpoint, this is most concerning because of the risk of serotonin syndrome, a potentially serious side effect in which heightened serotonergic activity leads to autonomic instability, neuromuscular changes, and mental status change (27). MDMA has the highest risk of serotonin syndrome among common psychedelic substances (28). Although recent studies show that the risk of serotonin syndrome with psilocybin is relatively low at the usual doses seen with recreational and therapeutic use (27), future research is needed to understand appropriate use of psychedelics in the context of concomitant medications. Indeed, a large systematic review showed numerous potential interactions between MDMA and alpha-2 adrenoceptor agonists, antipsychotics, and antidepressants, and between psilocybin and antipsychotics and anxiolytics (26). Outcomes of interactions may include blunting of psychedelic effects, increased risk of serotonin syndrome, as well as pharmacokinetic and/or pharmacodynamic changes. Taken together, these findings suggest that a nuanced discussion with a provider would provide opportunities to reduce risk and appropriately account for these interactions among people using psychedelics.
Although many respondents endorsed the importance of support from a trained therapist or healthcare professional when using psychedelics for therapeutic purposes, only 15% had consumed psychedelics with such support, largely because they did not know how to find these resources and due to affordability. Most participants agreed or strongly agreed that therapists offering psychedelic-assisted therapy should have personal experience with psychedelics. This poses an interesting challenge to the field, as there are currently legal barriers and professional consequences to providers using psychedelics in the United States, and the personal experience of any therapeutic drug’s effects is generally not part of provider training. However, many psychedelic therapists in clinical trials do report personal use of psychedelics, demonstrated by a survey of psychotherapists associated with Usona Institute’s Phase II clinical trial in which 28 of the 32 (88%) of respondents reported personal experience with at least one serotonergic psychedelic (29).
Notably, whereas 81% reported being likely or very likely to consume psychedelics with a trained therapist or guide, 71% were also open to using an “underground” guide if one were available, indicating substantial comfort with proceeding without sanctioned medical or mental health oversight. However, despite most participants not having support from a trained therapist for their psychedelic experiences, many reported having adequate preparation, support during, and integration after their experience. This suggests that individuals within this population are obtaining relevant information on how to use these substances as well as support from friends and other trusted adults to fill this gap. Compared to those who did not disclose, participants who disclosed psychedelic use to their primary care provider reported small but statistically significantly higher degrees of preparation, support during, and support after their psychedelic experience, suggesting that communication with healthcare providers may be important for creating appropriate set and setting for the psychedelic experience. Given the widespread interest in psychedelics but considerable gaps in availability and accessibility of trained healthcare providers (30), future research should focus on understanding what level of support is needed for people using psychedelics for various medical conditions, as well as patient factors (e.g., co-morbidities) that might require extra support.
A recent study projected that over half of US States will legalize psychedelics by 2034 to 2037 (1). With this rapidly changing landscape, we believe that psychiatrists, therapists, and PCPs have a critical role to play in facilitating safe use of psychedelics in healthcare. To make best use of therapeutic encounters with patients using psychedelics, providers need access to unbiased and thoughtful education about how to work with patients using these substances. This is especially important for psychotherapists, who will likely be doing the bulk of the clinical work in this area and will be on the front lines of working with patients in the suggestible, vulnerable state elicited by these compounds (19). More research is needed to help properly inform the clinical space, as there remains much uncertainty about what clinical factors predict a therapeutic vs. negative psychedelic experience, what kind of care is necessary prior to and after such experiences, and what therapeutic modalities should be employed to help maximize therapeutic outcomes.
We also believe it critical that providers have sufficient training to develop a trusting therapeutic alliance around psychedelic use, inquire about substance use using nonjudgmental language, and present risks, particularly interaction risks, clearly and at a patient-appropriate level of understanding. A lack of trust for their PsyCP was cited as a barrier to psychedelics discussion for 23% of respondents. Assuming this lack of trust is not limited to divulging information about illegal activities, this is alarming as a poor therapeutic alliance is likely to negatively impact the patient’s care more broadly (31).
A key legal barrier to appropriately addressing psychedelics in healthcare remains the Schedule I status of virtually all psychedelics, excepting ketamine. Given the active study and promising results throughout the peer-reviewed literature, that legal status does not align with the known safety profile and clinical potential of these substances. Accordingly, the expeditious revision of regulations and recommendations that are incongruent with our best understanding of medical reality should be a paramount priority (32).
The present study is limited by the convenience sampling strategy, which recruited via a psychedelics advocacy event and online forums. Further, our findings may not generalize to other populations as the participants were largely White, had an average age of 39, and included many psychedelic enthusiasts and advocates. We also acknowledge that our approach is rooted in a western academic tradition and does not address the indigenous traditions associated with psychedelics, which may provide support and integration in ways that were not interrogated by our questionnaire. We would also expect to see different trends in data with greater ethnic, racial, and socioeconomic diversity based on cultural factors. Finally, we did not investigate provider viewpoints on interactions with people using psychedelics nor did we investigate factors (e.g., diagnoses, psychedelics used) associated with feeling adequately supported during a psychedelic experience—both of which are fruitful areas for future research. These limitations are offset by several strengths, including our large sample size and questions that gauge previously unexamined aspects of naturalistic psychedelic use, including interactions with PCPs and PsyCP, desire for therapist support, and investigation of medications taken concomitantly with psychedelics.
In this large survey study of individuals using psychedelics naturalistically, we show that participants generally used psychedelics for managing mental health issues and desired more support from therapists or mental health professionals while using psychedelics. Participants engaged with PsyCP more frequently than with PCPs about psychedelic use, although confidence was low in both PsyCP and PCP ability to integrate psychedelics into current treatment. Many participants reported using psychiatric medications on the same day as psychedelics, including medications that may increase risk of side effects or potentially attenuate psychedelic effects (e.g., benzodiazepines, SSRIs). There were significant gaps in access and knowledge around finding either an underground or licensed therapist for such support. As psychedelics become more widely available through rapidly advancing liberalization efforts, our results demonstrate the continued need for healthcare provider education around psychedelics, as well as policies supporting training and harm reduction for those using these substances.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Institutional Review Board University of Michigan Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
KB, JB, CF, MH, NG, NK, and DK helped to conceive of the study and designed the survey. JB, CF, MH, NG, NK, and DK helped to distribute the survey. DK performed data cleaning and analyses. KB, CW, and KC drafted the manuscript. KB, KC, CW, MH, NG, NK, CF, JB, and DK provided significant feedback and critically revised the manuscript. All authors contributed to the article and approved the submitted version.
KB’s effort on this publication was partially supported by the National Institute on Drug Abuse of the National Institutes of Health under K01DA049219. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors declare no other funding sources.
We are grateful to study participants who generously shared their time to complete this survey.
NG owns stock in Cybin Inc., Mind Medicine Inc., Numinus Wellness, Revive Therapeutics, Braxia Scientific, and Compass Pathways. CW owns stock in Mind Medicine Inc., Numinus Wellness, and Tryp Therapeutics. KB has received grant funding from Tryp Therapeutics for protocol development and sits on a data safety and monitoring board for an ongoing clinical trial with Vireo Health (unpaid). JB is the Founder/President of the Michigan Psychedelic Society, Co-Founder of Decriminalize Nature Michigan, Executive Director of Decriminalize Nature Ann Arbor, Psychedelic Integration and Music Therapist at Blue Sage Health Consulting.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Siegel, JS, Daily, JE, Perry, DA, and Nicol, GE. Psychedelic drug legislative reform and legalization in the US. JAMA Psychiat. (2023) 80:77–83. doi: 10.1001/jamapsychiatry.2022.4101
2. Davis, AK, Agin-Liebes, G, Espana, M, Pilecki, B, and Luoma, J. Attitudes and beliefs about the therapeutic use of psychedelic drugs among psychologists in the United States. J Psychoactive Drugs. (2021) 54:309–18. doi: 10.1080/02791072.2021.1971343
3. Barnett, BS, Beaussant, Y, Ft, K, and Doblin, R. Psychedelic knowledge and opinions in psychiatrists at two professional conferences: an exploratory survey. J Psychoactive Drugs. (2021) 54:269–77. doi: 10.1080/02791072.2021.1957183
4. Carhart-Harris, R, Giribaldi, B, Watts, R, Baker-Jones, M, Murphy-Beiner, A, Murphy, R, et al. Trial of psilocybin versus escitalopram for depression. N Engl J Med. (2021) 384:1402–11. doi: 10.1056/NEJMoa2032994
5. Goodwin, GM, Aaronson, ST, Alvarez, O, Arden, PC, Baker, A, Bennett, JC, et al. Single-dose psilocybin for a treatment-resistant episode of major depression. N Engl J Med. (2022) 387:1637–48. doi: 10.1056/NEJMoa2206443
6. Davis, AK, Barrett, FS, May, DG, Cosimano, MP, Sepeda, ND, Johnson, MW, et al. Effects of psilocybin-assisted therapy on major depressive disorder: a randomized clinical trial. JAMA Psychiat. (2021) 78:481–9. doi: 10.1001/jamapsychiatry.2020.3285
7. Griffiths, RR, Johnson, MW, Carducci, MA, Umbricht, A, Richards, WA, Richards, BD, et al. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: a randomized double-blind trial. J Psychopharmacol. (2016) 30:1181–97. doi: 10.1177/0269881116675513
8. Grob, CS, Danforth, AL, Chopra, GS, Hagerty, M, McKay, CR, Halberstadt, AL, et al. Pilot study of psilocybin treatment for anxiety in patients with advanced-stage cancer. Arch Gen Psychiatry. (2011) 68:71–8. doi: 10.1001/archgenpsychiatry.2010.116
9. Ross, S, Bossis, A, Guss, J, Agin-Liebes, G, Malone, T, Cohen, B, et al. Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: a randomized controlled trial. J Psychopharmacol. (2016) 30:1165–80. doi: 10.1177/0269881116675512
10. Johnson, MW, Garcia-Romeu, A, Cosimano, MP, and Griffiths, RR. Pilot study of the 5-HT2AR agonist psilocybin in the treatment of tobacco addiction. J Psychopharmacol. (2014) 28:983–92. doi: 10.1177/0269881114548296
11. Johnson, MW, Garcia-Romeu, A, and Griffiths, RR. Long-term follow-up of psilocybin-facilitated smoking cessation. Am J Drug Alcohol Abuse. (2017) 43:55–60. doi: 10.3109/00952990.2016.1170135
12. Bogenschutz, MP, Ross, S, Bhatt, S, Baron, T, Forcehimes, AA, Laska, E, et al. Percentage of heavy drinking days following psilocybin-assisted psychotherapy vs placebo in the treatment of adult patients with alcohol use disorder: a randomized clinical trial. JAMA. Psychiatry. (2022) 79:953. doi: 10.1001/jamapsychiatry.2022.2096
13. Mitchell, JM, Bogenschutz, M, Lilienstein, A, Harrison, C, Kleiman, S, Parker-Guilbert, K, et al. MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study. Nat Med. (2021) 27:1025–33. doi: 10.1038/s41591-021-01336-3
14. Jerome, L, Feduccia, AA, Wang, JB, Hamilton, S, Yazar-Klosinski, B, Emerson, A, et al. Long-term follow-up outcomes of MDMA-assisted psychotherapy for treatment of PTSD: a longitudinal pooled analysis of six phase 2 trials. Psychopharmacology. (2020) 237:2485–97. doi: 10.1007/s00213-020-05548-2
15. Palhano-Fontes, F, Barreto, D, Onias, H, Andrade, KC, Novaes, MM, Pessoa, JA, et al. Rapid antidepressant effects of the psychedelic ayahuasca in treatment-resistant depression: a randomized placebo-controlled trial. Psychol Med. (2019) 49:655–63. doi: 10.1017/S0033291718001356
16. Sanches, RF, de Lima, OF, Dos Santos, RG, Macedo, LR, Maia-de-Oliveira, JP, Wichert-Ana, L, et al. Antidepressant effects of a single dose of ayahuasca in patients with recurrent depression: a SPECT study. J Clin Psychopharmacol. (2016) 36:77–81. doi: 10.1097/JCP.0000000000000436
17. Marcantoni, WS, Akoumba, BS, Wassef, M, Mayrand, J, Lai, H, Richard-Devantoy, S, et al. A systematic review and meta-analysis of the efficacy of intravenous ketamine infusion for treatment resistant depression: January 2009–January 2019. J Affect Disord. (2020) 277:831–41. doi: 10.1016/j.jad.2020.09.007
18. Holze, F, Gasser, P, Müller, F, Dolder, PC, and Liechti, ME. Lysergic acid diethylamide–assisted therapy in patients with anxiety with and without a life-threatening illness: a randomized, double-blind, placebo-controlled phase II study. Biol Psychiatry. (2023) 93:215–23. doi: 10.1016/j.biopsych.2022.08.025
19. McNamee, S, Devenot, N, and Buisson, M. Studying harms is Key to improving psychedelic-assisted therapy-participants call for changes to research landscape. JAMA Psychiat. (2023) 80:411. doi: 10.1001/jamapsychiatry.2023.0099
20. MacBride, K. Psychedelic-assisted therapy is bigger than ever, but it’s at risk of being compromised by alleged abuse. Inverse; (2021), Available at: https://www.inverse.com/mind-body/grossbard-bourzat-psychedelic-assisted-therapy-abuse
21. Livne, O, Shmulewitz, D, Walsh, C, and Hasin, DS. Adolescent and adult time trends in US hallucinogen use, 2002–19: any use, and use of ecstasy. LSD PCP Addict. (2022) 117:3099–109. doi: 10.1111/add.15987
22. Glynos, NG, Fields, CW, Barron, J, Herberholz, M, Kruger, DJ, and Boehnke, KF. Naturalistic Psychedelic Use: A World Apart from Clinical Care. J Psychoactive Drugs. (2022):1–10. doi: 10.1080/02791072.2022.2108356
23. Johnson, M, Richards, W, and Griffiths, R. Human hallucinogen research: guidelines for safety. J Psychopharmacol. (2008) 22:603–20. doi: 10.1177/0269881108093587
24. McClure-Begley, TD, and Roth, BL. The promises and perils of psychedelic pharmacology for psychiatry. Nat Rev Drug Discov. (2022) 21:463–73. doi: 10.1038/s41573-022-00421-7
25. Kruger, DJ, Enghoff, O, Herberholz, M, Barron, J, and Boehnke, KF. How do I learn more about this?: utilization and trust of psychedelic information sources among people naturalistically using psychedelics. J Psychoactive Drugs. (2023) 1-9:1–9. doi: 10.1080/02791072.2023.2201263
26. Sarparast, A, Thomas, K, Malcolm, B, and Stauffer, CS. Drug-drug interactions between psychiatric medications and MDMA or psilocybin: a systematic review. Psychopharmacology. (2022) 239:1945–76. doi: 10.1007/s00213-022-06083-y
27. Malcolm, B, and Thomas, K. Serotonin toxicity of serotonergic psychedelics. Psychopharmacology. (2022) 239:1881–91. doi: 10.1007/s00213-021-05876-x
28. Dobry, Y, Rice, T, and Sher, L. Ecstasy use and serotonin syndrome: a neglected danger to adolescents and young adults prescribed selective serotonin reuptake inhibitors. Int J Adolesc Med Health. (2013) 25:193–9. doi: 10.1515/ijamh-2013-0052
29. Aday, JS, Skiles, Z, Eaton, N, Fredenburg, L, Pleet, M, Mantia, J, et al. Personal psychedelic use is common among a sample of psychedelic therapists: implications for research and practice. Psyc Med. (2023) 1:27–37. doi: 10.1089/psymed.2022.0004
30. Mocanu, V, Mackay, L, Christie, D, and Argento, E. Safety considerations in the evolving legal landscape of psychedelic-assisted psychotherapy. Subst Abuse Treat Prev Policy. (2022) 17:37. doi: 10.1186/s13011-022-00468-0
31. Pinto, RZ, Ferreira, ML, Oliveira, VC, Franco, MR, Adams, R, Maher, CG, et al. Patient-centred communication is associated with positive therapeutic alliance: a systematic review. J Physiother. (2012) 58:77–87. doi: 10.1016/S1836-9553(12)70087-5
Keywords: psychedelics, psychiatrist, antidepressants, mental health, psilocybin, primary care physician
Citation: Boehnke KF, Cox K, Weston C, Herberholz M, Glynos N, Kolbman N, Fields CW, Barron J and Kruger DJ (2023) Slouching towards engagement: interactions between people using psychedelics naturalistically and their healthcare providers. Front. Psychiatry. 14:1224551. doi: 10.3389/fpsyt.2023.1224551
Edited by:
Hannes Simon Kettner, Imperial College London, United KingdomReviewed by:
Atiqul Haq Mazumder, University of Oulu, FinlandCopyright © 2023 Boehnke, Cox, Weston, Herberholz, Glynos, Kolbman, Fields, Barron and Kruger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kevin F. Boehnke, a2JvZWhua2VAbWVkLnVtaWNoLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.