
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 03 January 2024
Sec. Psychological Therapy and Psychosomatics
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1214266
This article is part of the Research Topic The Role of Emotion Regulation on the Developmental Course of Eating Disorders, Obesity and Food Addiction View all 9 articles
 Geovanny Genaro Reivan Ortiz1*
Geovanny Genaro Reivan Ortiz1* Ximena Campoverde2
Ximena Campoverde2 Juan Vinañzaca1
Juan Vinañzaca1 Johanna Estrada1
Johanna Estrada1 Rafael Yanza2
Rafael Yanza2 Roser Granero3
Roser Granero3Background: Food addiction (FA) is a construct that has gained interest in recent years, but its relevance in the Ecuadorian population has not yet been explored. The aims of this study were to explore the differences in the psychological profile (including FA) between university students from Ecuador and to identify the underlying structure of the relationships of the FA severity level through a mediational model.
Methods: The sample consisted of 972 university students, women and men (mean age: 20.1 years old, SD = 2.6), recruited from four Ecuadorian regions. The assessment tools included a unidimensional scale of FA, eating-related measures, emotion regulation state, impulsivity, and psychopathology state. Path analysis modeled the direct and indirect effects explaining the FA severity level.
Results: The results indicated that higher psychopathological levels were associated with FA. Similarly, no differences in FA were observed between the Ecuadorian regions. The path analysis suggested that older age, female sex, and higher difficulties in emotional regulation, impulsivity, negative mood, and anxiety trigger disordered eating; subsequently, more impaired eating behavior impacted the FA level.
Conclusion: FA is a complex clinical entity that includes multiple components related to eating disorders (EDs) and other mental health problems. The results of this study provide empirical knowledge for designing evidence-based prevention and treatment strategies.
Obesity has become a priority condition in the world due to its high prevalence and various chronic diseases associated with it (1, 2). Additionally, obesity is associated with a poorer quality of life and leads to high public health costs (3).
In Ecuador, 6 out of 10 people have presented problems of overweight (BMI > 25) and obesity (BMI > 30), being more prevalent during adolescence and early adulthood. Women (65.5%) have the highest frequency than men (34.5%). Despite the country's security measures, the number of people with overweight/obesity is increasing (4). This topic shows the need to go even deeper into the study of the various factors that may be involved in its development in order to improve prevention and treatment programs.
As indicated, studies show that obesity is a problem in the adult population, especially women, with increasing frequency in older age groups (5). Similarly, empirical evidence mentions that this higher trend in women than in men is positively correlated with age, and there may be a greater vulnerability to suffering from disordered eating behaviors (6–9).
Food addiction (FA) has become a widely recognized issue as one of the key players that can explain the processes or behaviors that contribute to the development and maintenance of obesity and eating disorders (EDs) (10–15). Recently, high levels of FA have been found to be the most important psychological factor in unsuccessful weight loss (16). Despite its importance, FA is poorly studied in the Ecuadorian population.
FA is defined as hedonic eating behavior involving the consumption of highly palatable foods (i.e., foods high in salt, fat, and sugar) in quantities beyond homeostatic energy requirements (17). The FA model has been proposed considering the similarities between the processes found in substance abuse disorders (18) and the consumption of certain foods that have been described as potentially addictive, such as sweet, salty, fatty, and processed foods (17, 19, 20). Similar to the mechanism described in addictive behaviors, FA is associated with the compulsive search for and consumption of these foods despite their negative consequences, the presence of tolerance, withdrawal, and activation in the same brain areas. The effects involve activity in the nucleus accumbens, including activation of the brain's dopamine and opioid signaling system (21).
Several variables have been closely linked to FA, emerging as risk patterns. A risk pattern refers to any identifiable trait or situation in an individual or group that is known to increase the likelihood of experiencing, developing, or being particularly vulnerable to a specific pathology or disease; for example, impulsivity (22–26), denoted as a personality trait characterized by fast, unexpected and excessive reactions. Studies indicate that impulsivity increases the risk of FA (27, 28).
Moreover, studies indicate that FA presents significantly higher scores when associated with anxiety (29–33). For some people, compulsive eating is a way of coping with anxiety (30, 34). Similarly, a large body of literature indicates that anxiety and other variables and affective dysregulation (35–41) have a mediating effect on many mental disorders, such as EDs.
Another indirect and etiopathogenic factor of FA is emotional dysregulation, which refers to the difficulty in the way people experience and express their emotions (42). Precisely, high rates of emotional dysregulation have been found in FA (18, 43, 44). Although the precise role of this construct needs to be further explored, FA behaviors could also be used to cope with negative affects, such as fear, sadness, anger, disgust, and guilt (45–47).
To summarize, higher levels of the aforementioned variables may be associated with addiction to food and, hence, with elevated eating psychopathology, greater preponderance of pathognomonic features associated with EDs, and higher BMI (48, 49).
As previously stated, FA has been minimally researched in Ecuador, although research on the effects of hypercaloric diets has gained interest in Latin America (50, 51). It has been found that, in the young population, it is highly influenced by the eating context and FA (49, 52, 53). However, there are no studies that examine the prevalence of FA among Ecuadorian young adults, as well as studies that explore the influence of various factors and interactions on its development.
Despite the efforts of health organizations imposed by the government in the incorporation of preventive strategies for obesity, the high rates and comorbidities associated with it (high blood pressure, high cholesterol, type 2 diabetes, coronary diseases, attacks or stroke, gallbladder diseases, etc.), mortality rates continue to rise in the Ecuadorian population. This behavior constitutes an alarm signal for the region.
This reality is not unfamiliar to the university sector. Research reveals that Ecuadorian students are overweight and obese, sedentary for extended periods, engage in limited physical activity, consume alcohol, get inadequate sleep, lack discipline in their eating habits, and consume ultra-processed foods that are low in nutritional value but high in salt, saturated fats, sugar, and even exhibit FA tendencies. This situation is the impetus for our research, which seeks to ascertain the prevalence of FA in young Ecuadorian adults and explore the various contributing factors and their interplay in its onset.
Therefore, this study proposed two objectives: to assess the psychological characteristics associated with the different results of the AF screening (whether absent, probable, or present) and to formulate a predictive model that can measure the severity of FA in the Ecuadorian population.
We propose that the screening for addiction to present food will have a worse psychological profile in Ecuadorians. Finally, despite the fact that the literature indicates an association between the etiological factors in isolation, the total composition of these has not been investigated through an integrated model; for this, we propose the hypotheses according to structural models proposed according to the study of Munguía et al. (54) and Wolz et al. (55), in this way, we organize the routes, of their risk patterns: elevated levels of FA are associated with increased: impulsivity, anxiety, and difficulties in emotional regulating; older age is linked to increased impulsivity and emotional imbalance; and the female sex is often associated with more challenges in eating behaviors.
The sample was selected using a non-probabilistic convenience design. Based on the researchers' access to potential participants, 2,654 students from mid-level undergraduate programs, such as Business Administration, Accounting, Psychology, Nursing, and Medicine, were invited. These students were from various departments and extensions of the Catholic University throughout Ecuador. The constituted cities, whose participants are native, were made up of the following regions: Galapagos (Isabela Island), Coast (Machala, Pasaje, and Guayaquil), Mountain (Quito and Cuenca), and East (Macas, Sucua, Limón Indaza, and Gualaquiza). Participants ranged in age from 17 to 29 and belonged to the middle socioeconomic class. Only those who agreed to participate underwent evaluation. The ultimate sample included 972 participants, comprising 688 women and 284 men, representing all four regions of Ecuador: Galapagos, Coast, Mountain, and East. Detailed breakdowns are provided in Table 1. The participants were recruited as volunteers, and all of them signed the informed consent. Participants under 18 years of age who participated in the study also presented informed consent signed by their parents. No compensation was awarded for participating in the study. Assessed by a questionnaire adapted from the DSM-5 Structured Clinical Interview for Eating Disorders (SCID-5), no participant reported having had an eating disorder (ED) in their lifetime. Participants were not evaluated for any other medical or psychiatric problem.
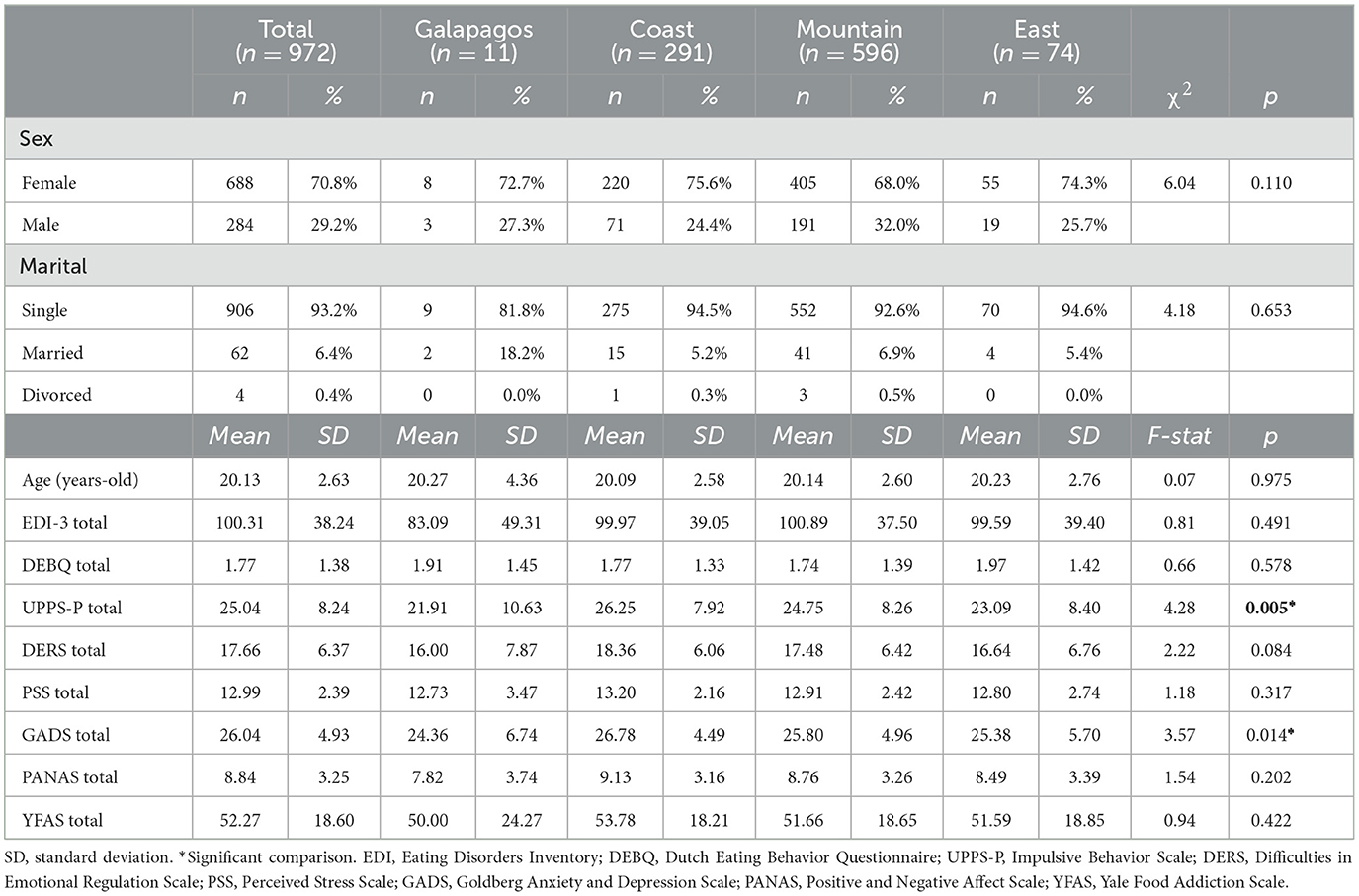
Table 1. Descriptive for the variables of the study.
In addition to a targeted sociodemographic questionnaire capturing key variables like sex, marital status, and age, other instruments were also employed. A detailed description of all study measures can be found in Table 1, while the correlation matrix for these variables is presented in Table 2.
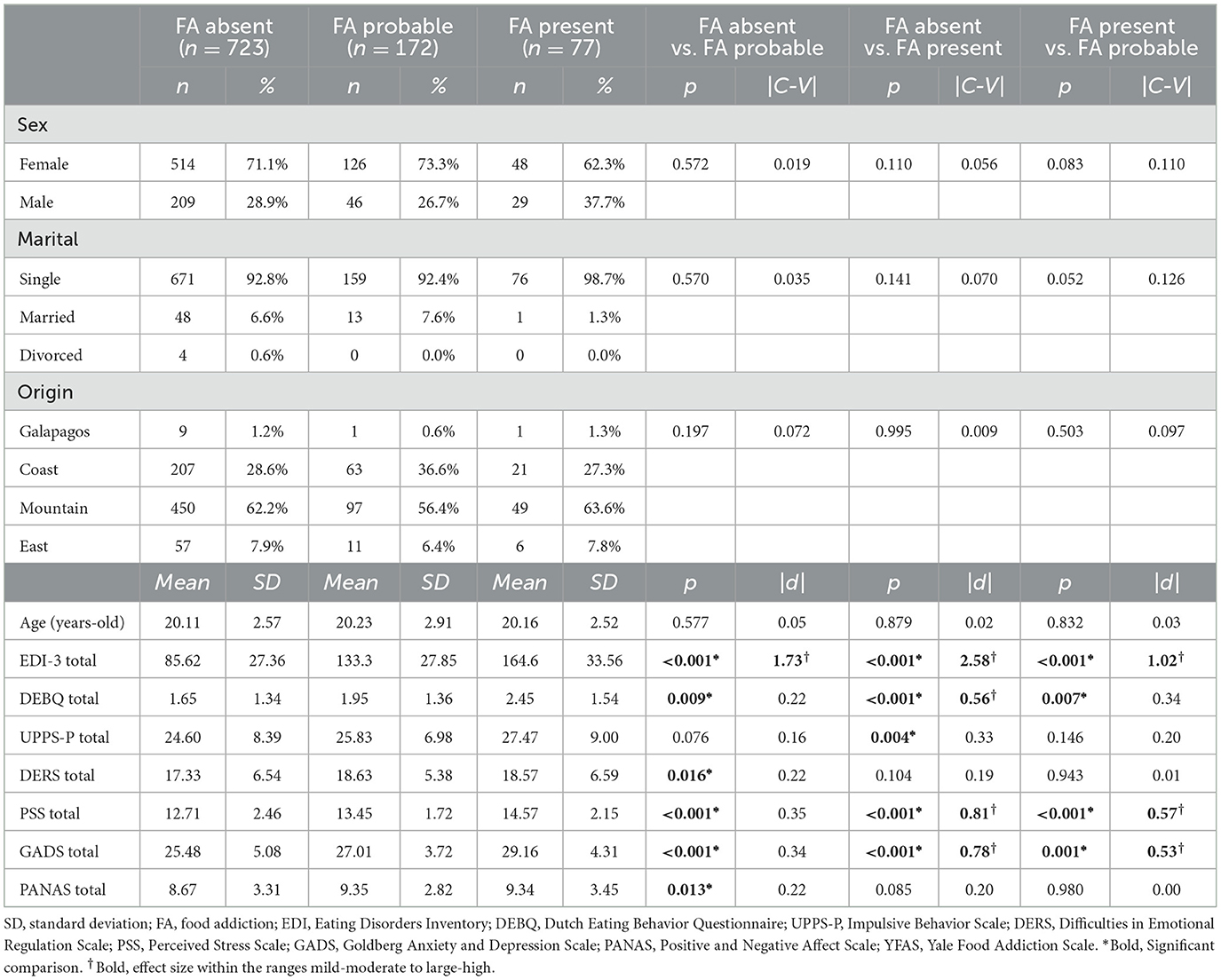
Table 2. Comparison between the FA screening groups.
Yale Food Addiction Scale 2.0 YFAS 2.0 (56) is a 35-item self-report questionnaire to measure addictive eating behaviors during the previous 12 months. The original instrument (YFAS) was based on the substance dependence criteria of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) (57) and was adapted to the context of food consumption. The YFAS 2.0 is based on the DSM-5 (58) and assesses 11 symptoms. The score produces two measures: (a) a continuous symptom count score that reflects the number of diagnostic criteria met (ranging from 0 to 11) and (b) an FA threshold based on the number of symptoms (at least 2) and self-reported clinically significant impairment or distress. This final measure allows for binary classification of FA (present vs. absent). In addition, according to the revised taxonomy of the DSM-5 (58), it is possible to establish cut-off points for severity: mild (2–3 symptoms), moderate (4–5 symptoms), and severe (6–11 symptoms). The FA risk groups were calculated according to a previous study (54) as follows: absent FA, those who do not have any diagnostic criteria in the YFAS 2.0; probable FA, those who meet one diagnostic criterion and those who have two or more criteria but do not present clinical deterioration; and present FA, those who have two diagnostic criteria and also present clinical deterioration. Thus, the probable group of FA will correspond to the clinical concept of high or subthreshold risk, that is, patients who do not strictly meet the diagnostic criteria of taxonomy but who present symptoms. Subthreshold psychiatric symptoms do not meet the full criteria for a particular disorder in a reference diagnostic taxonomy (such as Axis I disorders within the DSM) but do present with significant clinical deterioration. In some cases, subthreshold symptoms are more common than their respective Axis I disorders, and empirical research has suggested that these groups are associated with greater disability and many other negative consequences (59). In the present study, the validation of the scale in Spanish was used (60). The internal consistency of the YFAS 2.0 in our sample was α = 0.85.
Characteristics of eating disorders. Eating Disorders Inventory (EDI-3) (61). The EDI-3 is a standardized measure that is easy to apply and correct, offering objective scores and profiles that are highly useful for people with characteristics or suspected diagnoses of ED. of eating behavior. It is composed of 91 items, organized into 12 main scales: 3 scales specific to EDs and 9 general psychological scales that are highly relevant to, but not specific to, ED. It also provides six indices: one specific to eating disorders (ED risk) and five integrative psychological construct indices (inefficacy, interpersonal problems, affective problems, excess control, and general psychological maladjustment). Compared to previous versions, it incorporates three validity scales that allow professionals to detect inconsistent or strange response patterns: inconsistency, infrequency, and negative impression. The total sum of the instrument measures the characteristics of the present ED. The multiple validations reflect alphas and omegas ≥0.75 for the total scale (62–64). In the present study, the instrument reported an alpha of 0.79 using the Spanish version (65).
Disordered eating behavior. Dutch Eating Behavior Questionnaire [DEBQ; (66)]. The English version of the DEBQ (67). The Dutch Eating Behavior Questionnaire (DEBQ) is a 33-item self-report questionnaire developed by Van Strien et al. (66) to assess three distinct eating behaviors in adults: (1) emotional eating, (2) external eating, and (3) restricted eating. Items on the DEBQ are scored from 1 (never) to 5 (very often), with higher scores indicating greater approval of the disordered eating behavior. The psychometric properties of the DEBQ are solid and show good internal consistency in non-clinical samples for the entire scale, ranging from 0.92 to 0.94 Cronbach's alpha coefficient. In the present study, an alpha of 0.89 was obtained by applying the Spanish version of the scale (68).
Impulsivity. The UPPS-P Impulsive Behavior Scale (69) is a 59-item scale designed to assess impulsivity, determined in five subscales: lack of deliberation, lack of perseverance, negative urgency, positive urgency, and sensation seeking. The items are evaluated from 1 (totally agree) to 4 (totally disagree). Internal consistency reliability estimates indicate that the overall scale and the subscales have an internal consistency >0.80. In the current sample, the internal consistency coefficient indicated an alpha of 0.83, respectively applied to the Spanish version (70).
Negative affect. The short version in Spanish of the PANAS is a self-applied instrument consisting of two sections of 20 items each, 10 of which measure positive affects and 10 negative affects. The first section evaluates the presence of affects “in recent weeks” (affect as a state), and the second section evaluates them “generally” (affect as a trait). The items are made up of words that describe different emotions and feelings and are answered by indicating a number in a range from 1 to 5, where 1 means “very little or not at all” and 5 “extremely.” The subscales of the instrument indicate good reliability, ranging from 0.75 to 0.92 for positive affect and 0.78 to 0.93 for negative affect. In the present study, an alpha of 0.78 was obtained for the negative affect and 0.80 for the positive affect, applying the Ecuadorian version (71).
Stress. Perceived Stress Scale [EEP; (72)]. Scale made up of 10 items that measure perceived stress—the extent to which everyday life situations are perceived as stressful. The scale includes a series of direct inquiries that explore the level of stress experienced. The paragraphs are easy to understand. The scale provides five response options: “never,” “almost never,” “occasionally,” “many times,” and “always,” which are classified from zero to four. However, items 4, 5, 7, and 8 are scored in reverse or inverted form. The EEP-4 is limited to items 2, 4, 5, and 10. The higher the score, the greater the perceived stress.
Anxiety. Goldberg Anxiety and Depression Scale [GADS; (73)]. This instrument is made up of two subscales of nine binary items (yes/no) each. The first anxiety subscale (questions 1–9) and the second subscale for depression (questions 10–18). Higher point values indicate greater anxiety and greater depression. The original scale and adapted versions indicate good internal consistency, ranging from 0.70 to 0.92 for both subscales. The present study sample presented Cronbach's alpha of 0.80 for the anxiety scale and 0.79 for the depression subscale, using the Ecuadorian version (74).
Difficulties in emotion regulation: Difficulties in Emotional Regulation Scale (DERS) (42) is a 36-item scale used to assess emotional dysregulation. The DERS consists of the following six subscales: non-acceptance of emotional responses, difficulties engaging in goal-directed behaviors when experiencing strong emotions, difficulties controlling impulses, lack of emotional awareness, limited access to emotion-regulation strategies, and lack of emotional clarity. Participants are asked to respond to each item using a five-point Likert scale ranging from 1 (almost never) to 5 (almost always). Higher scores indicate greater problems with emotion regulation. The general scale and subscales present good reliability, with alphas and omegas ranging from 0.71 to 0.86, respectively. The DERS scale has its Ecuadorian validation (75), and the total reliability of the DERS in our sample was 0.81, respectively.
Permission for researchers to access classrooms was granted by the Rectorate and the Teaching Department of the Catholic University of Cuenca. Researchers visited each classroom across the offered courses, introduced the study, and extended an invitation to students to participate. The study's objectives, its voluntary nature, and the data collection schedule during school hours were communicated. Only students who agreed and provided signed informed consent were evaluated on the predetermined date. During the evaluation, questionnaires were completed individually in a group setting, overseen by a seasoned psychologist. The instruments were not arranged in any specific order. To maintain privacy, participants were spaced sufficiently apart to prevent potential influence from peers' responses. Each session took about an hour. This psychologist received guidance from Spanish psychometrician colleagues. In line with the Declaration of Helsinki, the study received approval from the local Ethics Committee of the Catholic University of Cuenca under the code UCACUE-UASB-P-CEISH-2022-096 in Ecuador. All participants were required to sign informed consent.
Statistical analysis was carried out with Stata17 for Windows. Chi-square tests (χ2) assessed the relationship between the categorical variables of the study (expected frequencies higher than 5 were achieved, guaranteeing the conditions for conducting the tests). The comparison between quantitative variables between the groups was done with a one-way ANOVA (which also met the assumptions of high sample sizes and common variance). It was tested that these methods fulfilled the statistical analysis assumptions in this study. The effect size for these procedures was performed with Cramer's-V coefficient for the contingency tables analyzed with χ2-tests and Cohen (76) d coefficient for the pairwise comparisons in the ANOVA.
Pearson's correlation (R) explored the relationship between the quantitative variables of the study. Due to the strong association between this model and the sample size (low-correlation values tend to achieve significant results in large samples, while high-correlation values tend to achieve non-significant results in small samples), relevant correlations were considered for |R| coefficients within the mild–moderate to large–high ranges (the cut-offs are 0.24 and 0.37, respectively) (77).
Path analysis assessed the direct and indirect links between the FA severity and the other variables of the study. In this study, this mode was implemented through the structural equation model (SEM), using the maximum-likelihood estimation (MLE) procedure, which is the most commonly used method for estimation and testing in SEMs (78). The rationale for the path diagram (i.e., the model specification) was based on the theoretical background provided by the cumulated empirical evidence (as summarized in the Introduction section), with the restrictions of the available measurement tools/data, adequate fitting and guaranteeing the clinical significance of whole model (78). All the parameters in the SEM were free estimates, and with the aim of obtaining a more parsimonious model and increasing statistical power, parameters with no significant tests were deleted, and the model was re-specified and re-adjusted (79). A goodness-of-fit was valued with the usual indexes (80): χ2-test, root mean squared error of approximation (RMSEA), comparative fit index (CFI), the Tucker–Lewis index (TLI), and the standardized root-mean-square residual (SRMR). Adequate fitting was considered for non-significant results in the χ2 test (p > 0.05), RMSEA <0.09, CFI > 0.90, TLI > 0.90, and SRMR <0.10. The global predictive capacity for the model was measured with the coefficient of determination (CD).
Most participants in the study were women (n = 688, 70.8%) and single (n = 906, 93.2%). Mean age was 20.13 years old (SD=2.63). Table 1 displays the descriptive of the variables analyzed in the study and the comparison of the groups defined for the geographic origin. Significant differences were only observed in impulsivity and the GADS total score, with the coast group recording the highest mean values and the Galapagos group the lowest.
Table 2 shows the comparison of the participants with absent, probable, and present screening scores in the YFAS 2.0. A greater proportion contributed to the female sex, presenting high values in AF absent (71.1%), AF probable (73.3%), and AF present (62.3%) than the male sex. No differences between the groups were found for the sociodemographic features (sex, marital status, origin, and age). However, differences were obtained for the variables related to the clinical state (Figure 1). As a whole, the FA absent group was characterized by the best functional profile, with the lowest scores in the ED symptom problems (EDI-3 and DEBQ), impulsivity levels (UPPS-P), difficulties in emotion regulation (DERS), stress perceived level, anxiety (GADS), and negative emotion (PANAS). The worst functional clinical profile was related to the FA present group.
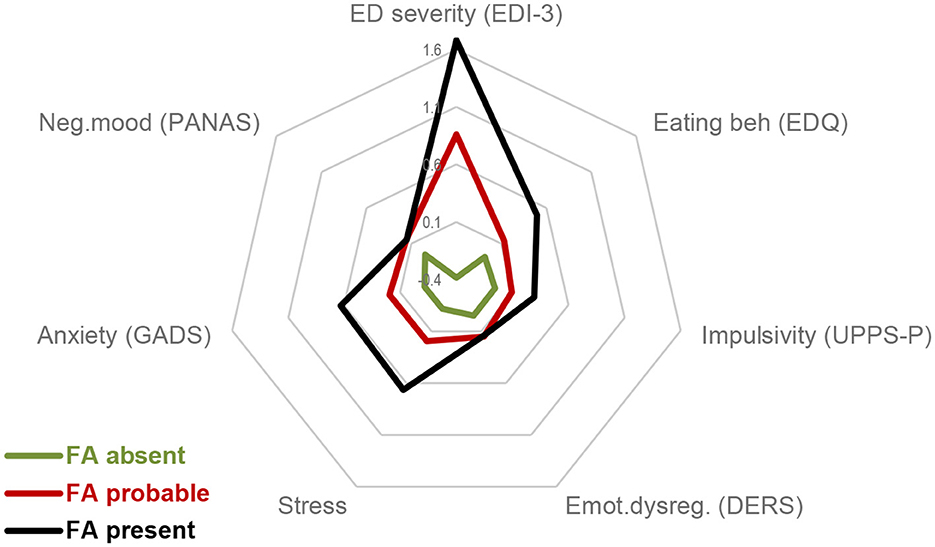
Figure 1. Radar chart. FA, food addiction. Standardized z-mean scores are plotted.
Figure 2 shows the path diagram with the standardized coefficients obtained in the SEM (Supplementary Table S1, displays the complete results, including tests for direct, indirect, and total effects). Only significant parameters were retained in the final model to allow easier interpretation. Adequate goodness-of-fit was achieved as follows: χ2 = 16.47 (p = 0.792), RMSEA = 0.001 [95% confidence interval (CI): 0.000–0.018], CFI = 0.999, TLI = 0.998, SRMR = 0.018. The global predictive capacity was CD = 0.35 (35%). No significant difference was obtained in the chi-square tests (χ2 = 14.96, p = 0.528) comparing this final model vs. the initial model that included all the direct and direct effects [χ2 = 1.55 (p = 0.959), RMSEA = 0.001, CFI = 0.999, TLI = 0.999, SRMR = 0.003, CD = 0.45].
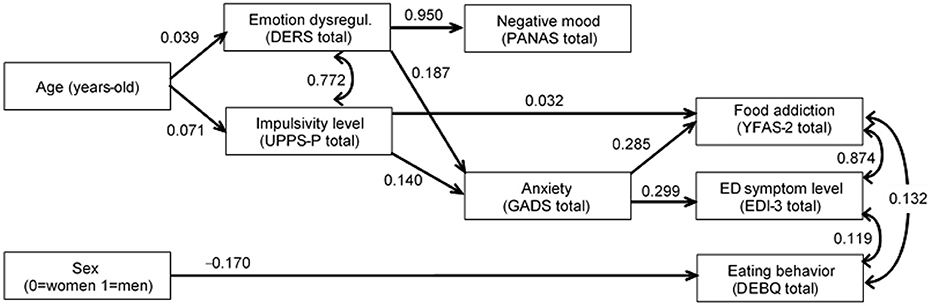
Figure 2. Path diagram: standardized coefficients. Only significant parameters retained in the final model. Fit statistics: χ2 = 16.47 (p = 0.792), RMSEA = 0.001 (95% CI: 0.000 to 0.018), CFI = 0.999, TLI = 0 0.998, SRMR = 0.018.
The likelihood of higher FA levels was directly related to higher impulsivity and anxiety levels. Anxiety was also identified as a mediational link in the following two paths: (a) higher impulsivity levels contributed to a higher anxiety state and, therefore, to a more severe FA profile, and (b) higher difficulties in the emotion regulation impacted the anxiety state, and once more to a higher FA level.
Three other pathways were observed: (a) older age contributed to higher levels of impulsivity and emotion dysregulation, (b) female sex was related to more difficulties in eating behaviors, and (c) the higher the impairment in emotion regulation, the worse the negative mood state.
Finally, positive correlations were found between emotional dysregulation with impulsivity levels, FA with and ED symptoms and ED behaviors, and ED symptoms with and ED behaviors.
Research on FA has seen a surge in recent years, but its exploration within the Ecuadorian population remains limited. This study proposed two objectives: to assess the psychological characteristics associated with the different results of the AF screening (whether absent, probable, or present) and to formulate a predictive model that can measure the severity of FA in the Ecuadorian population.
The results of the first objective indicated that a worse psychological profile is associated with a present FA. This result is consistent with previous studies that indicate the dysfunction of the psychological areas is predominant when an eating disorder such as FA occurs (81–84). The second objective led to the formulation of a refined predictive model for the intensity of FA in the Ecuadorian populace. The findings align with existing research. Our analysis corroborates these outcomes, highlighting that FA has a positive correlation with impulsivity and anxiety. This suggests a parallel between FA and substance use disorders. Precisely, as indicated, FA and drug use disorders share analogous etiological variables such as impulsivity (85) and anxiety (30, 86). This result demonstrates that high drive levels are related to higher values in FA (87). Studies presented in this line strengthen our analysis since FA has been related to worse executive functioning and impulse control in university students, which may be a factor that contributes to a worse quality of life in this population (88–90). One aspect of impulse control that has been found to be particularly relevant to FA and eating behaviors is the tendency to have difficulty with impulse control during negative mood states (91), which was not accounted for in this study. Therefore, future research in this direction could deepen our comprehension of FA. For their part, diet and anxiety can become a recurring adverse pattern with FA (33, 92). The temptation and guilt that comes from snacking on a favorite food can lead to anxiety. While cross-sectional studies suggest an empirical connection between anxiety and FA, the direct and indirect (mediating) direction of our study's connection strengthens those results (31, 32). Studies in this line report that FA has been associated with typical anxiety and addiction phenomena such as restlessness, intense excitement, extreme insecurity, brain reward dysfunction, worry, risky consumption, impaired control, and relapse (92, 93), which would be important to address in future lines of research. Given that the literature shows that women are more prone than men to present anxiety and addiction to food and that the connection between anxiety and ED could be moderated by gender (31), Our study corroborates these findings, showing a direct influence of sex on disordered eating behavior.
In contrast, this study tested the hypotheses about the mediating role of anxiety between the indirect influence of impulsivity and emotional dysregulation on FA. Our results confirm the mediating role of anxiety in increasing ED symptoms (94), indicating that people are more likely to act impulsively when they are anxious with the certainty of increasing the probability of triggering an FA. In other words, anxiety potentiates the indirect effect of impulsivity on FA, generating a greater consumption of food. Similarly, our results confirm the role played by emotional dysregulation in EDs. Precisely, our analyses are consistent with recent studies (36, 40, 95), indicating that emotional dysregulation is significantly associated with overeating (96–98). Thus, a greater consumption of food downregulates emotional intensity, demonstrating the indirect role of emotional dysregulation on FA and symptoms associated with EDs. Moreover, dysregulation of emotions has been postulated and empirically supported as a primary transdiagnostic phenomenon across the spectrum of EDs (18, 44, 99). Finally, emotional dysregulation explains significantly more the variation in binge eating by sex, food restriction, weight assessment, and body shape (98, 100, 101). While these criteria were not explored in this study, we suggest that incorporating them in future research would enrich the analysis of the associations between emotional dysregulation and problematic eating.
Another hypothesis that was validated is the link between age, impulsivity, and emotional dysregulation. This result strengthens studies that report the role of impulsivity and emotional dysregulation during adolescence and early adulthood, precisely where there is a higher incidence of suffering from an eating disorder (22, 102–104). Furthermore, it is known that impulsivity plays an important role in addictions. Although there is situational, useful, and adaptive impulsivity, our study reflected on impulsivity as a trait frequently related to behaviors that are harmful to the individual such as inappropriate eating acts. Similar to impulsivity, several studies (105–107) corroborate our results, indicating that emotional dysregulation manages to be representative in age adolescents and young adults, essentially in the university context.
Although we did not make the direct relational hypothesis of emotion regulation and FA in our study, difficulties with emotion regulation have been shown to increase the risk of psychopathology (108–111). A review of longitudinal studies on university students investigated the relationship between emotional regulation and various EDs (112). The results suggest that dysregulation of emotions is an important factor in university students at risk of FA. Similarly, previous studies have indicated that difficulties in regulating emotions positively predicted high scores on the YFAS (22, 113) and that this strength of association is similar in patients with ED and healthy controls (43, 114). Hence, we believe these data align with the analyses presented, suggesting that behaviors associated with FA serve as a means to regulate maladaptive emotions.
According to the contrasted hypothesis on the relationship of the female sex with disordered eating behaviors, several studies ratify these results (115–117). The evidence presented to date indicates that the female sex has been very strongly associated with the presence of EDs (118). Our analysis strengthens the classic studies where the predisposition of the female sex is mentioned in the prevalence of ED, denoting it to be a predisposing factor for FA. Furthermore, we believe that this result is overshadowed by “standard factors” that are also present in EDs that were not included in this study, such as familial and socioeconomic factors (119–121).
Finally, the hypothesis on the relationship between impaired emotional regulation and negative mood was contrasted. The literature has identified both negative affect and the dysregulation of emotions as central elements of various forms of psychopathology, such as EDs (45, 47, 122, 123). Our results support these investigations and strengthen the conceptualization of emotional dysregulation as a different construct related to, but not reducible to, negative affect. Therefore, these data suggest that negative affect may be as or more strongly related to some forms of psychopathology as is the case with dysregulation of emotions in an integrated model of FA.
Based on our findings, our model demonstrates satisfactory goodness-of-fit metrics, mirroring the model introduced by Munguía et al. (54) for FA, whose direct predictors were made up of disordered eating behavior, difficulties in emotional regulation, and impulsivity and whose indirect predictors were made up of age and the characteristics of EDs. Our study diverges by successfully incorporating negative affect, anxiety, and sex, thereby enriching the comprehension of FA within the Ecuadorian context. Similarly, our findings bolster the model presented by Wolz et al. (55), which integrates impulsivity, emotional regulation difficulties, and ED traits, resulting in a tailored SEM predictive model for FA. Other models have either examined FA independently or in tandem, weaving in predictors like impulsivity and emotional regulation (43) or age and sex (124), obtaining similarly adjusted results in the proposed models. Complementing this, a study that incorporated psychological and sociocultural variables (125) consistently indicated that the dysfunctional psychological profile emerges as a significant predictor of FA, a notion we have elaborated on extensively in our research.
As highlighted earlier, this marks the inaugural study in the Ecuadorian population aiming to integrate clinical variables linked to FA. Yet, it is essential to interpret these findings in light of certain limitations. Initially, the sample size was not evenly distributed across the regions examined, given that data collection occurred in its natural setting.
In addition, our study could be assessed as underpowered due to the use of path analysis. However, it must be considered that sample size requirements for SEMs rely on outdated rules of thumb and that current studies using Monte Carlo procedures that have explored requirements for some common types of models (including variation by the number of factors, the number of indicators, the strength of the indicator loadings and the regressive paths, and the amount of missing data per indicator), have evidenced that the statistical power, the bias in the parameter estimates, and the overall solution propriety, can be adequately achieved with sample sizes into a large range (from 30 to 460) (126, 127).
Moreover, the sample predominantly consisted of university students, potentially affecting the broader applicability of the findings. In a similar vein, the research focused solely on a specific age bracket, constraining the extrapolation of results to diverse age groups. Future research should thus encompass a broader spectrum of participants, spanning various age categories and additional variables to the model in question. Finally, the evaluation scales used lacked proper validation for the Ecuadorian demographic.
We deduce that elevated psychopathological levels correlate with food addiction. Additionally, there is no discernible difference in the risk of FA across Ecuadorian regions. In conclusion, our analysis indicates that older age, being female, and exhibiting heightened levels of emotional dysregulation, impulsivity, negative affect, and anxiety can precipitate EDs and, as a result, FA in the Ecuadorian population.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Ethics Committee of the Catholic University of Cuenca with the code UCACUE-UASB-P-CEISH-2022-096 - in Ecuador. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
GR did the original writing and drafting. RG developed the methodology, data analysis, and results. XC, JV, JE, and RY recruited and processed the data. All authors contributed to the conceptualization, supervision, writing, revision, and approval of the final version of the manuscript.
RG was supported by the Catalan Institution for Research and Advanced Studies (ICREA-2021 Academia Program).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1214266/full#supplementary-material
1. Jiang X, Xu J, Zhen S, Zhu Y. Obesity is associated with postoperative outcomes in patients undergoing cardiac surgery: a cohort study. BMC Anesthesiol. (2023) 23:1–7. doi: 10.1186/s12871-022-01966-1
2. Kearns K, Dee A, Fitzgerald AP, Doherty E, Perry IJ. Chronic disease burden associated with overweight and obesity in Ireland: the effects of a small BMI reduction at population level. BMC Public Health. (2014) 14:1–10. doi: 10.1186/1471-2458-14-143
3. Williams EP, Mesidor M, Winters K, Dubbert PM, Wyatt SB. Overweight and obesity: prevalence, consequences, and causes of a growing public health problem. Curr Obes Rep. (2015) 4:363–70. doi: 10.1007/s13679-015-0169-4
4. Weigel MM, Armijos RX. Food insecurity is associated with self-reported oral health in school-age Ecuadorian children and is mediated by dietary and non-dietary factors. Public Health Nutr. (2023) 26:23–32. doi: 10.1017/S1368980022002166
5. Frasca D, Blomberg BB, Paganelli R. Aging, obesity, and inflammatory age-related diseases. Front Immunol. (2017) 8:1745. doi: 10.3389/fimmu.2017.01745
6. Bjorklund J, Wiberg-Itzel E, Wallstrom T. Is there an increased risk of cesarean section in obese women after induction of labor? A retrospective cohort study. PLoS ONE. (2022) 17:e0263685. doi: 10.1371/journal.pone.0263685
7. Duclos M, Pereira PM, Barat P, Gatta B, Roger P. Increased cortisol bioavailability, abdominal obesity, and the metabolic syndrome in obese women. Obes Res. (2005) 13:1157–66. doi: 10.1038/oby.2005.137
8. Martorell R, Kettel Khan L, Hughes ML, Grummer-Strawn LM. Obesity in women from developing countries. Eur J Clin Nutr. (2000) 54:247–52. doi: 10.1038/sj.ejcn.1600931
9. Nederkoorn C, Smulders FT, Havermans RC, Roefs A, Jansen A. Impulsivity in obese women. Appetite. (2006) 47:253–6. doi: 10.1016/j.appet.2006.05.008
10. Ferrario CR. Food addiction and obesity. Neuropsychopharmacology. (2017) 42:361. doi: 10.1038/npp.2016.221
11. Finlayson G. Food addiction and obesity: unnecessary medicalization of hedonic overeating. Nat Rev Endocrinol. (2017) 13:493–8. doi: 10.1038/nrendo.2017.61
12. Lee NM, Lucke J, Hall WD, Meurk C, Boyle FM, Carter A, et al. Public views on food addiction and obesity: implications for policy and treatment. PLoS ONE. (2013) 8:e74836. doi: 10.1371/journal.pone.0074836
13. Meule A, Heckel D, Jurowich CF, Vögele C, Kübler A. Correlates of food addiction in obese individuals seeking bariatric surgery. Clin Obes. (2014) 4:228–36. doi: 10.1111/cob.12065
14. Saraswat AA, Longyear LG, Kawa AB, Ferrario CR. Cocaine-induced plasticity, motivation, and cue responsivity do not differ in obesity-prone vs obesity-resistant rats; implications for food addiction. Psychopharmacology. (2023) 240:853–70. doi: 10.1007/s00213-023-06327-5
15. Schulte EM, Tuttle HM, Gearhardt AN. Belief in food addiction and obesity-related policy support. PLoS ONE. (2016) 11:e0147557. doi: 10.1371/journal.pone.0147557
16. Cattaneo C, Mambrini SP, Gilardini L, Scacchi M, Castelnuovo G, Pagliarini E, et al. The phenomenon of abnormal eating and taste perception: What's the link in subjects with obesity and eating disorders?. Food Quality Pref. (2023) 104:104744. doi: 10.1016/j.foodqual.2022.104744
17. Cummings JR, Schiestl ET, Tomiyama AJ, Mamtora T, Gearhardt AN. Highly processed food intake and immediate and future emotions in everyday life. Appetite. (2022) 169:105868. doi: 10.1016/j.appet.2021.105868
18. Hardy R, Fani N, Jovanovic T, Michopoulos V. Food addiction and substance addiction in women: common clinical characteristics. Appetite. (2018) 120:367–73. doi: 10.1016/j.appet.2017.09.026
19. Gordon EL, Ariel-Donges AH, Bauman V, Merlo LJ. What is the evidence for “food addiction?” A systematic review. Nutrients. (2018) 10:477. doi: 10.3390/nu10040477
20. Westwater ML, Fletcher PC, Ziauddeen H. Sugar addiction: the state of the science. Eur J Nutr. (2016) 55:55–69. doi: 10.1007/s00394-016-1229-6
21. Rossi AA, Mannarini S, Castelnuovo G, Pietrabissa G. Disordered eating behaviors related to food addiction/eating addiction in inpatients with obesity and the general population: the italian version of the addiction-like eating behaviors scale (AEBS-IT). Nutrients. (2023) 15:104. doi: 10.3390/nu15010104
22. El Archi S, Barrault S, Garcia M, Branger S, Maugé D, Ballon N, et al. Adult ADHD diagnosis, symptoms of impulsivity, and emotional dysregulation in a clinical sample of outpatients consulting for a behavioral addiction. J Attent Disorders. (2023) 12:10870547231161336. doi: 10.1177/10870547231161336
23. Loxton NJ. The role of reward sensitivity and impulsivity in overeating and food addiction. Curr Addict Rep. (2018) 5:212–22. doi: 10.1007/s40429-018-0206-y
24. Maxwell AL, Gardiner E, Loxton NJ. Investigating the relationship between reward sensitivity, impulsivity, and food addiction: a systematic review. Eur Eating Disorders Rev. (2020) 28:368–84. doi: 10.1002/erv.2732
25. Raymond KL, Lovell GP. Food addiction symptomology, impulsivity, mood, and body mass index in people with type two diabetes. Appetite. (2015) 95:383–9. doi: 10.1016/j.appet.2015.07.030
26. Velázquez-Sánchez C, Ferragud A, Moore CF, Everitt BJ, Sabino V, Cottone P, et al. High trait impulsivity predicts food addiction-like behavior in the rat. Neuropsychopharmacology. (2014) 39:2463–72. doi: 10.1038/npp.2014.98
27. Kandeger A, Selvi Y, Tanyer DK. The effects of individual circadian rhythm differences on insomnia, impulsivity, and food addiction. Eating Weight Disorders Stu Anorexia Bulimia Obesity. (2019) 24:47–55. doi: 10.1007/s40519-018-0518-x
28. Murphy CM, Stojek MK, MacKillop J. Interrelationships among impulsive personality traits, food addiction, and body mass index. Appetite. (2014) 73:45–50. doi: 10.1016/j.appet.2013.10.008
29. da Silva Júnior AE, Praxedes DRS, Monteiro MBL, de Lima Macena M, Bueno NB. Prevalence of food addiction determined by the Yale food addiction scale in Latin America: a systematic review with meta-analysis. Int J Eating Disord. (2022) 7:23909. doi: 10.1002/eat.23909
30. Goldway N, Eldar E, Shoval G, Hartley CA. Computational mechanisms of addiction and anxiety: a developmental perspective. Biol Psychiatry. (2023) 93:739–50. doi: 10.1016/j.biopsych.2023.02.004
31. Hussenoeder FS, Pabst A, Conrad I, Löbner M, Engel C, Zeynalova S, et al. Anxiety and food addiction in men and women: results from the longitudinal LIFE-adult-study. Front Psychiatry. (2022) 13. doi: 10.3389/fpsyt.2022.914358
32. Nolan LJ, Jenkins SM. Food addiction is associated with irrational beliefs via trait anxiety and emotional eating. Nutrients. (2019) 11:1711. doi: 10.3390/nu11081711
33. Romero-Blanco C, Hernández-Martínez A, Parra-Fernández ML, Onieva-Zafra MD, Prado-Laguna MDC, Rodríguez-Almagro J, et al. Food addiction and lifestyle habits among university students. Nutrients. (2021) 13:1352. doi: 10.3390/nu13041352
34. Sinha R, Gu P, Hart R, Guarnaccia JB. Food craving, cortisol and ghrelin responses in modeling highly palatable snack intake in the laboratory. Physiol Behav. (2019) 208:112563. doi: 10.1016/j.physbeh.2019.112563
35. Benzerouk F, Djerada Z, Bertin E, Barrière S, Gierski F, Kaladjian A, et al. Contributions of emotional overload, emotion dysregulation, and impulsivity to eating patterns in obese patients with binge eating disorder and seeking bariatric surgery. Nutrients. (2020) 12:3099. doi: 10.3390/nu12103099
36. Fiore F, Ruggiero GM, Sassaroli S. Emotional dysregulation and anxiety control in the psychopathological mechanism underlying drive for thinness. Front Psychiatry. (2014) 5:43. doi: 10.3389/fpsyt.2014.00043
37. Jen A, Saunders EF, Ornstein RM, Kamali M, McInnis MG. Impulsivity, anxiety, and alcohol misuse in bipolar disorder comorbid with eating disorders. Int J Bipolar Disorders. (2013) 1:1–9. doi: 10.1186/2194-7511-1-13
38. Sevincer GM, Ince E, Taymur I, Konuk N. Night eating syndrome frequency in university students: Association with impulsivity, depression, and anxiety. Bullet Clin Psychopharmacol. (2016) 26:238–47. doi: 10.5455/bcp.20160322093750
39. Spence S, Courbasson C. The role of emotional dysregulation in concurrent eating disorders and substance use disorders. Eat Behav. (2012) 13:382–5. doi: 10.1016/j.eatbeh.2012.05.006
40. Van Elburg A, Danner UN, Sternheim LC, Lammers M, Elzakkers I. Mental capacity, decision-making and emotion dysregulation in severe enduring anorexia nervosa. Front Psychiatry. (2021) 12:545317. doi: 10.3389/fpsyt.2021.545317
41. Waxman SE. A systematic review of impulsivity in eating disorders. European Eating Disorders Rev Prof J Eating Disorders Assoc. (2009) 17:408–25. doi: 10.1002/erv.952
42. Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difculties in emotion regulation scale. J Psychopathol Behav Assess. (2004) 26:41–54. doi: 10.1023/B:JOBA.0000007455.08539.94
43. Pivarunas B, Conner BT. Impulsivity and emotion dysregulation as predictors of food addiction. Eat Behav. (2015) 19:9–14. doi: 10.1016/j.eatbeh.2015.06.007
44. Vasiliu O. Current status of evidence for a new diagnosis: food addiction-A literature review. Front Psychiatry. (2022) 12:2545. doi: 10.3389/fpsyt.2021.824936
45. Bradley B, DeFife JA, Guarnaccia C, Phifer J, Fani N, Ressler KJ, et al. Emotion dysregulation and negative affect: association with psychiatric symptoms. J Clin Psychiatry. (2011) 72:6427. doi: 10.4088/JCP.10m06409blu
46. Donahue JJ, Goranson AC, McClure KS, Van Male LM. Emotion dysregulation, negative affect, and aggression: a moderated, multiple mediator analysis. Pers Individ Dif. (2014) 70:23–8. doi: 10.1016/j.paid.2014.06.009
47. Veilleux JC, Skinner KD, Reese ED, Shaver JA. Negative affect intensity influences drinking to cope through facets of emotion dysregulation. Pers Individ Dif. (2014) 59:96–101. doi: 10.1016/j.paid.2013.11.012
48. von Ranson KM, Klump KL, Iacono WG, McGue M. The Minnesota eating behavior survey: a brief measure of disordered eating attitudes and behaviors. Eat Behav. (2005) 6:373–92. doi: 10.1016/j.eatbeh.2004.12.002
49. Yu Z, Tan M. Disordered eating behaviors and food addiction among nutrition major college students. Nutrients. (2016) 8:673. doi: 10.3390/nu8110673
50. Figueroa C, Echeverría G, Villarreal G, Martínez X, Ferreccio C, Rigotti A, et al. Introducing plant-based mediterranean diet as a lifestyle medicine approach in latin america: opportunities within the chilean context. Front Nutr. (2021) 8:680452. doi: 10.3389/fnut.2021.680452
51. Ortega-García JA, Tellerías L, Ferrís-Tortajada J, Boldo E, Campillo-López F, van den Hazel P, et al. Threats, challenges and opportunities for paediatric environmental health in Europe, Latin America and the Caribbean. Anales Pediatría. (2019) 90:124–e1. doi: 10.1016/j.anpede.2018.11.008
52. Chen IH, Huang PC, Lin YC, Gan WY, Fan CW, Yang WC, et al. The Yale Food Addiction Scale 2, 0. and the modified yale food addiction scale 20 in Taiwan: factor structure and concurrent validity. Front Psychiatry. (2022) 13. doi: 10.3389/fpsyt.2022.1014447
53. Escrivá-Martínez T, Galiana L, Rodríguez-Arias M, Baños RM. The binge eating scale: Structural equation competitive models, invariance measurement between sexes, and relationships with food addiction, impulsivity, binge drinking, and body mass index. Front Psychol. (2019) 10:530. doi: 10.3389/fpsyg.2019.00530
54. Munguía L, Jiménez-Murcia S, Valenciano-Mendoza E, Granero R, Gaspar-Pérez A, Guzmán-Saldaña RM, et al. Risk patterns in food addiction: a Mexican population approach. Eating Weight Dis Stu Anorexia Bulimia Obesity. (2022) 27:1077–87. doi: 10.1007/s40519-021-01240-2
55. Wolz I, Agüera Z, Granero R, Jiménez-Murcia S, Gratz KL, Menchón JM, et al. Emotion regulation in disordered eating: psychometric properties of the difculties in emotion regulation scale among spanish adults and its interrelations with personality and clinical severity. Front Psychol. (2015) 6:907. doi: 10.3389/fpsyg.2015.00907
56. Gearhardt AN, Corbin WR, Brownell KD. Development of the yale food addiction scale version 2.0. Psychol Addict Behav. (2016) 30:113. doi: 10.1037/adb0000136
57. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th Edn. Washington, DC: American Psychiatric Association (2010).
58. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th Edn. Washington, DC: American Psychiatric Association (2013).
59. Rai D, Skapinakis P, Wiles N, Lewis G, Araya R. Common mental disorders, subthreshold symptoms and disability: longitudinal study. Br J Psychiatry. (2010) 197:411–2. doi: 10.1192/bjp.bp.110.079244
60. Granero R, Jiménez-Murcia S, Gearhardt AN, Agüera Z, Aymamí N, Gómez-Peña M, et al. Validation of the Spanish version of the yale food addiction scale 2.0 (YFAS 2.0) and clinical correlates in a sample of eating disorder, gambling disorder, and healthy control participants. Front Psychiatr. (2018) 9:208. doi: 10.3389/fpsyt.2018.00321
61. Garner DM. (2004). Eating Disorder Inventory- 3 Professional Manual: Psychological Assessment Resources. (2004).
62. Lizana-Calderón P, Cruzat-Mandich C, Díaz-Castrillón F, Alvarado JM, Compte EJ. Psychometric properties of the eating disorder inventory-3 (EDI-3) in chilean youth. Front Psychol. (2022) 13:806563. doi: 10.3389/fpsyg.2022.806563
63. Clausen L, Rosenvinge JH, Friborg O, Rokkedal K. Validating the eating disorder inventory-3 (EDI-3):a comparison between 561 female eating disorders patients and 878 females from the general population. J Psychopathol Behav Assessment. (2011) 33:101–10. doi: 10.1007/s10862-010-9207-4
64. Nyman-Carlsson E, Engström I, Norring C, Nevonen L. Eating disorder inventory-3, validation in Swedish patients with eating disorders, psychiatric outpatients and a normal control sample. Nordic J Psychiatry. (2015) 69:142–51. doi: 10.3109/08039488.2014.949305
65. Lehmann V, Ouwens MA, Braeken J, Danner UN, van Elburg AA, Bekker MH, et al. Psychometric properties of the Dutch version of the eating disorder inventory−3. Sage Open. (2013) 3:2158244013508415. doi: 10.1177/2158244013508415
66. Van Strien T, Frijters JE, Van Staveren WA, Defares PB, Deurenberg P. The predictive validity of the Dutch restrained eating scale. International Journal of Eating Disorders. (1986) 5:747–55. doi: 10.1002/1098-108X(198605)5:4<747::AID-EAT2260050413>3.0.CO;2-6
67. van Strien T, Frijter JE, Bergers G, Defares PB. Dutch eating behaviour questionnaire. Int J Eating Disord. (2002). doi: 10.1037/t04413-000
68. Cebolla A, Barrada JR, Van Strien T, Oliver E, Baños R. Validation of the Dutch eating behavior questionnaire (DEBQ) in a sample of Spanish women. Appetite. (2014) 73:58–64. doi: 10.1016/j.appet.2013.10.014
69. Lynam DR, Caspi A, Moffitt TE, Loeber R, Stouthamer-Loeber M. Longitudinal evidence that psychopathy scores in early adolescence predict adult psychopathy. J Abnorm Psychol. (2007) 116:155–65. doi: 10.1037/0021-843X.116.1.155
70. Cándido A, Orduña E, Perales JC, Verdejo-García A, Billieux J. Validation of a short Spanish version of the UPPS-P impulsive behaviour scale. Trastor Adict. (2012) 14:73–8. doi: 10.1016/S1575-0973(12)70048-X
71. Sanmartin R, Vicent M, Gonzálvez C, Inglés CJ, Reinoso-Pacheco R, García-Fernández JM, et al. Factorial invariance, latent mean differences of the Panas and affective profiles and its relation to social anxiety in Ecuadorian sample. Sustainability. (2020) 12:976. doi: 10.3390/su12072976
72. Trujillo HM, Gonzalez-Cabrera JM. Psychometric properties of the Spanish version of the perceived stress scale (PSS). Psicol Conductual. (2007) 15:457.
73. Goldberg D, Bridges K, Duncan-Jones P, Grayson D. Detecting anxiety and depression in general medical settings. Brit Med J. (1988) 297:897–9. doi: 10.1136/bmj.297.6653.897
74. Reivan-Ortiz G, Pineda-Garcia G, León Parias BD. Psychometric properties of the goldberg anxiety and depression scale (GADS) in Ecuadorian population. Int J Psychol Res. (2019) 12:41–8. doi: 10.21500/20112084.3745
75. Reivan-Ortiz GG, Ortiz Rodas PE, Reivan Ortiz PN. A brief version of the difficulties in emotion regulation scale (DERS): validity evidence in Ecuadorian population. Int J Psychol Res. (2020) 13:14–24. doi: 10.21500/20112084.4325
76. Cohen S. Contrasting the hassles scale and the perceived stress scale: Who's really measuring appraised stress? Am Psychol. (1986) 41:716–8. doi: 10.1037/0003-066X.41.6.716
77. Taylor R. Interpretation of the correlation coefficient: a basic review. J Diag Med Sonography. (1990) 6:35–9. doi: 10.1177/875647939000600106
78. Kline RB. Principles and Practice of Structural Equation Modeling, 2nd Edn. New York, NY: The Guilford Press (2005).
79. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. (1990) 107:238–46. doi: 10.1037/0033-2909.107.2.238
80. Barrett P. Structural equation modelling: adjudging model fit. Pers Individ Dif. (2007) 42:815–24. doi: 10.1016/j.paid.2006.09.018
81. Brown RM, James MH. Binge eating, overeating and food addiction: approaches for examining food overconsumption in laboratory rodents. Prog Neuro-Psychopharmacol Biol Psychiatry. (2023) 12:110717. doi: 10.1016/j.pnpbp.2023.110717
82. Burnatowska E, Wikarek A, Oboza P, Ogarek N, Glinianowicz M, Kocelak P, et al. Emotional eating and binge eating disorders and night eating syndrome in polycystic ovary syndrome—a vicious circle of disease: a systematic review. Nutrients. (2023) 15:295. doi: 10.3390/nu15020295
83. Gearhardt AN, Boswell RG, White MA. The association of “food addiction” with disordered eating and body mass index. Eat Behav. (2014) 15:427–33. doi: 10.1016/j.eatbeh.2014.05.001
84. Godoy-Izquierdo D, Ramírez MJ, Díaz I, Lopez-Mora C. A systematic review on exercise addiction and the disordered eating-eating disorders continuum in the competitive sport context. Int J Ment Health Addict. (2023) 21:529–61. doi: 10.1007/s11469-021-00610-2
85. Pape M, Herpertz S, Schroeder S, Seiferth C, Färber T, Wolstein J, et al. Food addiction and its relationship to weight-and addiction-related psychological parameters in individuals with overweight and obesity. Front Psychol. (2021) 12:736454. doi: 10.3389/fpsyg.2021.736454
86. Li R, Kajanoja J, Tuulari JJ, Karlsson L, Karlsson H, Karukivi M, et al. Relationships between alexithymia and food addiction: the finnish version of yale food addiction scale and preliminary test of its psychometric properties. Front Psychol. (2023) 14:1067872. doi: 10.3389/fpsyg.2023.1067872
87. Fletcher PC, Kenny PJ. Food addiction: a valid concept? Neuropsychopharmacology. (2018) 43:2506–13. doi: 10.1038/s41386-018-0203-9
88. Minhas M, Murphy CM, Balodis IM, Samokhvalov AV, MacKillop J. Food addiction in a large community sample of Canadian adults: prevalence and relationship with obesity, body composition, quality of life and impulsivity. Addiction. (2021) 116:2870–9. doi: 10.1111/add.15446
89. Rose MH, Nadler EP, Mackey ER. Impulse control in negative mood states, emotional eating, and food addiction are associated with lower quality of life in adolescents with severe obesity. J Pediatr Psychol. (2018) 43:443–51. doi: 10.1093/jpepsy/jsx127
90. Vira NH, Oyarce K, Vega MV, Goldfield GS, Guzmán-Gutiérrez E, Obregón AM, et al. No association of the dopamine D2 receptor genetic bilocus score (rs1800497/rs1799732) on food addiction and food reinforcement in Chilean adults. Front Behav Neurosci. (2023) 17: 1067384. doi: 10.3389/fnbeh.2023.1067384
91. Ramírez-Vizcaya S, Froese T. The enactive approach to habits: New concepts for the cognitive science of bad habits and addiction. Front. Psychol. (2019) 10:301. doi: 10.3389/fpsyg.2019.00301
92. Wiss D, Brewerton T. Separating the signal from the noise: how psychiatric diagnoses can help discern food addiction from dietary restraint. Nutrients. (2020) 12:2937. doi: 10.3390/nu12102937
93. Lindgren E, Gray K, Miller G, Tyler R, Wiers CE, Volkow ND, et al. Food addiction: a common neurobiological mechanism with drug abuse. Front Biosci Landmark. (2018) 23:811–36. doi: 10.2741/4618
94. Melchior C, Desprez C, Riachi G, Leroi AM, Déchelotte P, Achamrah N, et al. Anxiety and depression profile is associated with eating disorders in patients with irritable bowel syndrome. Front Psychiatry. (2020) 10:928. doi: 10.3389/fpsyt.2019.00928
95. Gander M, Sevecke K, Buchheim A. Eating disorders in adolescence: attachment issues from a developmental perspective. Front Psychol. (2015) 6:1136. doi: 10.3389/fpsyg.2015.01136
96. Casagrande M, Boncompagni I, Forte G, Guarino A, Favieri F. Emotion and overeating behavior: effects of alexithymia and emotional regulation on overweight and obesity. Eating Weight Disorders Stu Anorexia Bulimia Obesity. (2020) 25:1333–45. doi: 10.1007/s40519-019-00767-9
97. Favieri F, Marini A, Casagrande M. Emotional regulation and overeating behaviors in children and adolescents: a systematic review. Behav Sci. (2021) 11:11. doi: 10.3390/bs11010011
98. Racine SE, Horvath SA. Emotion dysregulation across the spectrum of pathological eating: comparisons among women with binge eating, overeating, and loss of control eating. Eat Disord. (2018) 26:13–25. doi: 10.1080/10640266.2018.1418381
99. Gearhardt AN, White MA, Masheb RM, Morgan PT, Crosby RD, Grilo CM, et al. An examination of the food addiction construct in obese patients with binge eating disorder. Int J Eating Disorders. (2012) 45:657–63. doi: 10.1002/eat.20957
100. Bray B, Sadowski A, Bray C, Bradley R, Zwickey H. Clinical aspects of binge eating disorder: a cross-sectional mixed-methods study of binge eating disorder experts' perspectives. Front Psychiatry. (2023) 13:3044. doi: 10.3389/fpsyt.2022.1087165
101. Rozakou-Soumalia N, Dârvariu S, Sjögren JM. Dialectical behaviour therapy improves emotion dysregulation mainly in binge eating disorder and bulimia nervosa: a systematic review and meta-analysis. J Pers Med. (2021) 11:931. doi: 10.3390/jpm11090931
102. Massa L, Abelli M, Forfori F, Paolo D, Benvenuti L, Palagini A, et al. Binge eating disorder, impulsivity and bipolar spectrum features in a sample of obese candidates for bariatric surgery. Riv Psichiatria. (2023) 58:76–83. doi: 10.1708/4022.39977
103. Del Bianco C, Ulivi M, Liguori C, Pisani A, Mercuri NB, Placidi F, et al. Alexithymia, impulsiveness, emotion, and eating dyscontrol: similarities and differences between narcolepsy type 1 and type 2. Sleep Biol Rhythms. (2023) 21:39–50. doi: 10.1007/s41105-022-00414-4
104. Lozano-Madrid M, Clark Bryan D, Granero R, Sánchez I, Riesco N, Mallorquí-Bagué N, et al. Impulsivity, emotional dysregulation and executive function deficits could be associated with alcohol and drug abuse in eating disorders. J Clin Med. (2020) 9:1936. doi: 10.3390/jcm9061936
105. Bekker MH, Van De Meerendonk C, Mollerus J. Effects of negative mood induction and impulsivity on self-perceived emotional eating. Int J Eating Disorders. (2004) 36:461–9. doi: 10.1002/eat.20041
106. Lundahl A, Wahlstrom LC, Christ CC, Stoltenberg SF. Gender differences in the relationship between impulsivity and disordered eating behaviors and attitudes. Eat Behav. (2015) 18:120–4. doi: 10.1016/j.eatbeh.2015.05.004
107. Van Swearingen KM, Noel NE. Impulsivity traits associated with disordered eating and binge drinking among female college students. J Am College Health. (2022) 21:1–6. doi: 10.1080/07448481.2022.2047696
108. Cristofanelli S, Baccini G, Centonze E, Colombesi A, Cariello M, Ferro L, et al. Can dissociation mediate the relationship between emotional dysregulation and intelligence? An empirical study involving adolescents with and without complex trauma histories. Int J Environ Res Public Health. (2023) 20:1729. doi: 10.3390/ijerph20031729
109. Horvath SA, Kolp HM, Andersen CV, Johnson EE, Racine SE, Borsari B, et al. Emotion dysregulation moderates the relationship between alcohol use and eating pathology among heavy-drinking college men. J Clin Psychol. (2021) 77:1763–75. doi: 10.1002/jclp.23157
110. Hughes AE, Crowell SE, Uyeji L, Coan JA. A developmental neuroscience of borderline pathology: Emotion dysregulation and social baseline theory. J Abnorm Child Psychol. (2012) 40:21–33. doi: 10.1007/s10802-011-9555-x
111. Pollock NC, McCabe GA, Southard AC, Zeigler-Hill V. Pathological personality traits and emotion regulation difficulties. Pers Individ Dif. (2016) 95:168–77. doi: 10.1016/j.paid.2016.02.049
112. Mallorquí-Bagué N, Vintró-Alcaraz C, Sánchez I, Riesco N, Agüera Z, Granero R, et al. Emotion regulation as a transdiagnostic feature among eating disorders: Cross-sectional and longitudinal approach. European Eating Disorders Rev. (2018) 26:53–61. doi: 10.1002/erv.2570
113. Gonçalves S, Moreira CS, Machado BC, Bastos B, Vieira AI. Psychometric properties and convergent and divergent validity of the portuguese yale food addiction scale 2, 0. (P-YFAS 2.0). Eating Weight Disorders Stu Anorexia Bulimia Obesity. (2021) 18:1–11. doi: 10.21203/rs.3.rs-432446/v1
114. Oliveira J, Colombarolli MS, Cordas TA. Prevalence and correlates of food addiction: systematic review of studies with the YFAS 2.0. Obesity Res Clin Prac. (2021) 15:191–204. doi: 10.1016/j.orcp.2021.03.014
115. Matthews-Ewald MR, Zullig KJ, Ward RM. Sexual orientation and disordered eating behaviors among self-identified male and female college students. Eat Behav. (2014) 15:441–4. doi: 10.1016/j.eatbeh.2014.05.002
116. Nagata JM, Garber AK, Tabler JL, Murray SB, Bibbins-Domingo K. Prevalence and correlates of disordered eating behaviors among young adults with overweight or obesity. J Gen Intern Med. (2018) 33:1337–43. doi: 10.1007/s11606-018-4465-z
117. Parker LL, Harriger JA. Eating disorders and disordered eating behaviors in the LGBT population: a review of the literature. J Eating Disorders. (2020) 8:1–20. doi: 10.1186/s40337-020-00327-y
118. Cao Z, Cini E, Pellegrini D, Fragkos KC. The association between sexual orientation and eating disorders-related eating behaviours in adolescents: a systematic review and meta-analysis. Eur Eating Disorders Rev. (2023) 31:46–64. doi: 10.1002/erv.2952
119. Burnette CB, Luzier JL, Weisenmuller CM, Boutté RL. A systematic review of sociodemographic reporting and representation in eating disorder psychotherapy treatment trials in the United States. Int J Eating Disorders. (2022) 55:423–54. doi: 10.1002/eat.23699
120. Gadalla TM. Eating disorders and associated psychiatric comorbidity in elderly Canadian women. Archives Women's Mental Health. (2008) 11:357–62. doi: 10.1007/s00737-008-0031-8
121. Romano KA, Lipson SK, Beccia AL, Quatromoni PA, Gordon AR, Murgueitio J, et al. Changes in the prevalence and sociodemographic correlates of eating disorder symptoms from 2013 to 2020 among a large national sample of US young adults: a repeated cross-sectional study. Int J Eating Disorders. (2022) 55:776–89. doi: 10.1002/eat.23709
122. Hofmann SG, Sawyer AT, Fang A, Asnaani A. Emotion dysregulation model of mood and anxiety disorders. Dep Anxiety. (2012) 29:409–16. doi: 10.1002/da.21888
123. Smith AL, Cross D, Winkler J, Jovanovic T, Bradley B. Emotional dysregulation and negative affect mediate the relationship between maternal history of child maltreatment and maternal child abuse potential. J Fam Violence. (2014) 29:483–94. doi: 10.1007/s10896-014-9606-5
124. Tatsi E, Kamal A, Turvill A, Regina H. Emotion dysregulation and loneliness as predictors of food addiction. J Health Soc Sci. (2019) 4:43–58. doi: 10.19204/2019/mtnd5
125. Farah MF, Shahzad MF. Fast-food addiction and anti-consumption behaviour: the moderating role of consumer social responsibility. Int J Consumer Stud. (2020) 44:379–92. doi: 10.1111/ijcs.12574
126. von Oertzen T. Power equivalence in structural equation modelling. Br J Math Stat Psychol. (2010) 62:257–72. doi: 10.1348/000711009X441021
Keywords: food addiction, eating disorder, path analysis, emotion regulation, Ecuadorians
Citation: Reivan Ortiz GG, Campoverde X, Vinañzaca J, Estrada J, Yanza R and Granero R (2024) Factors increasing the risk for food addiction in Ecuadorian students. Front. Psychiatry 14:1214266. doi: 10.3389/fpsyt.2023.1214266
Received: 29 April 2023; Accepted: 06 November 2023;
Published: 03 January 2024.
Edited by:
Domenico De Berardis, ASL 4, ItalyReviewed by:
Daniel Stein, Edmond and Lily Safra Children's Hospital, IsraelCopyright © 2024 Reivan Ortiz, Campoverde, Vinañzaca, Estrada, Yanza and Granero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Geovanny Genaro Reivan Ortiz, Z3JlaXZhbm9AdWNhY3VlLmVkdS5lYw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.