
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry , 05 September 2023
Sec. Mood Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1207653
 Pratap Chokka1*
Pratap Chokka1* Ash Bender2
Ash Bender2 Stefan Brennan3
Stefan Brennan3 Ghalib Ahmed4
Ghalib Ahmed4 Marc Corbière5
Marc Corbière5 David J. A. Dozois6Jeff Habert7
David J. A. Dozois6Jeff Habert7 John Harrison8
John Harrison8 Martin A. Katzman9
Martin A. Katzman9 Roger S. McIntyre10Yang S. Liu11
Roger S. McIntyre10Yang S. Liu11 Karen Nieuwenhuijsen12
Karen Nieuwenhuijsen12 Carolyn S. Dewa13
Carolyn S. Dewa13Major depressive disorder (MDD) and other mental health issues pose a substantial burden on the workforce. Approximately half a million Canadians will not be at work in any week because of a mental health disorder, and more than twice that number will work at a reduced level of productivity (presenteeism). Although it is important to determine whether work plays a role in a mental health condition, at initial presentation, patients should be diagnosed and treated per appropriate clinical guidelines. However, it is also important for patient care to determine the various causes or triggers including work-related factors. Clearly identifying the stressors associated with the mental health disorder can help clinicians to assess functional limitations, develop an appropriate care plan, and interact more effectively with worker’s compensation and disability programs, as well as employers. There is currently no widely accepted tool to definitively identify MDD as work-related, but the presence of certain patient and work characteristics may help. This paper seeks to review the evidence specific to depression in the workplace, and provide practical tips to help clinicians to identify and treat work-related MDD, as well as navigate disability issues.
Although the deleterious impact of major depressive disorder (MDD) on the workforce has been described over the past 15 years, there continues to be a critically high burden in terms of prevalence, lost work days, reduced productivity at work, higher unemployment risks, higher healthcare costs, and poorer quality of life (1–8). For example, studies have found that a 1% increase in unemployment is associated with a 1% increase in the suicide rate (9, 10). Thus, these data continue to support the need for action. The COVID-19 global pandemic, which affected both employment and mental health, further highlighted their interconnectedness (10–13). A systematic review including 18 studies found that, although there were conflicting findings, the majority of studies reported an increasing trend of suicidal attempts during compared to before the COVID-19 pandemic (14).
The aim of this report is to provide practical guidance to clinicians to assist them in assessing and treating work-related depression. The term “work-related” encompasses patients in whom work-related stressors have contributed to the development of their disorder, those who have developed their disorder subsequent to a physical or psychological work-related injury, and those who suffer an exacerbation of a pre-existing condition as a result of work-related stressors. Our target audience is clinicians, particularly primary care physicians in Canada, who are often the first line providers of treatment for MDD and for mitigating its impact on patients, their families, and their workplaces (15). There is a critical need for practical strategies to help clinicians efficiently and effectively provide the best possible care for their patients, as well as to help them to navigate the complex world of disability assessments, employee-employer relations, Workers’ Compensation Boards, and other reimbursement/insurance regulations. In addition, the information presented here may be of interest to employers.
Work-related MDD is increasingly requiring clinicians to serve as an intermediary between patients, employers, insurance providers and worker compensation systems. This has contributed to an urgent need for clinician-oriented guidance and education that will support accurate assessment and diagnosis of work-related MDD, and provide return to work principles, proper documentation procedures, effective workplace accommodations, and evidence-based treatments to specifically improve productivity.
Guidelines such as the national standards from the Mental Health Commission of Canada (MHCC) (16), and those from the World Health Organization (WHO) (17), are available to assist employers in creating and sustaining psychologically healthy work environments to prevent mental health issues in the workplace. However, there is little guidance to assist clinicians in assessing and treating work-related MDD. Canadian healthcare providers (HCPs) often lack specific training to assess for potential functional impairment due to mental health issues in a work context (18). In addition, the frustration that clinicians experience when treating workers struggling with a disability, and interacting with insurance providers and employers, can erode the therapeutic relationship and inhibit timely assessment and treatment (19).
For Canadians with major depressive disorder (MDD), the prevalence of unemployment and disability has been reported to be as high as 30% (2, 20), and in 2016 mental health claims represented 70% of the total cost of all disability claims (2). In addition, the rate of presenteeism was about 60% among those with MDD and/or an anxiety disorder (21). The annual estimated costs attributable to absenteeism and presenteeism associated with MDD in Canada were $2.5 billion and $6.8 billion, respectively (22).
Whereas MDD and other mental disorders can lead to temporary or permanent loss of employment, unemployment can lead to further deterioration in mental health and reduced chances of gaining employment (23, 24). Long term work absence and disability are associated with a range of poor health outcomes including increased mortality rates (25, 26), especially from cardiovascular disease and suicide (9, 10, 25, 26), increased rates of pain, obesity, chronic illnesses, disability, and healthcare utilization and cost, and decreased quality of life have also been reported (25–27).
Recently, the COVID-19 global pandemic has had a substantial effect on both employment and mental health (10–12, 28). The associated increases in the incidence of psychosocial problems, unemployment and financial uncertainty substantially increased the risk of suicide (9, 10, 28). Therefore, addressing work-related mental health and preventing suicide is becoming a public and employer health priority.
A World Health Organization (WHO) study found that every dollar spent on treatment for depression and anxiety can result in as much as US$4.00 in better health and improved economic productivity (29). Better treatment could lead to faster recovery, which globally, could translate to an extra 43 million years of healthy life over 15 years (29). The Conference Board of Canada estimated that improving MDD treatment for employed Canadians would add approximately $32.3 billion to Canada’s economy (21).
Strategies in the workplace to improve psychological health and safety can have positive benefits for employers in areas such as risk mitigation, business outcomes or profitability, recruitment and retention, and organizational excellence and sustainability (16). Organizations with a proactive approach to maintaining their employees’ psychological wellbeing can benefit from reductions in absenteeism and presenteeism, as well as lower rates of turnover, disability, injury, conflict, grievance, and poor morale (16, 30). In a survey of 784 Canadians with a mental disorder, 83% required some form of workplace accommodation, yet only 30% had received it (31). This is unfortunate since it has been demonstrated that workplace accommodation can significantly reduce the risk of a persistent mental disorder (32). Improved productivity resulting from the appropriate accommodation and effective management of mental health issues can provide substantial cost-savings for employers (33).
Although general awareness of mental disorders has improved, stigma remains a barrier to disclosing illness and obtaining care. A 2014 survey found that one-third of workers would not tell their employer if they had a mental health problem (34). One of their major concerns was fear of career damage, such as lost opportunities for promotion. In one survey, 26% of patients with MDD reported experiencing workplace discrimination, more than 50% expected to face discrimination, and 73% concealed their mental diagnosis (35). Similarly, a survey of the general public found that many do not regard depression as a valid reason for sickness absence (36). Stigma may also play a part in the workplace response to mental health injuries. When an employee suffers a physical work-related injury, they are usually given immediate treatment to manage their condition, but an immediate response to work-related mental health injuries can be impeded by the stigma around disclosing work-related mental health issues. Unfortunately, many work sites do not have a policy for safe disclosure (34).
The goal of this paper is to assist Canadian HCPs in the assessment and management of work-related depression. The guidance, developed by a committee of the Workplace Mental Health Network (WHMN), a non-profit organization focusing on the assessment and management of mental health disorders for clinicians, considered current evidence and the context of clinical challenges. Although this document focuses on a Canadian perspective, the general principles discussed have global implications and utility. This document is not a systematic review or a clinical guideline due to the paucity of evidence-based research in the literature to support some of the recommendations. However, the committee sought to provide guidance for clinicians, bridging gaps in the literature that lack strong evidence and addressing a real clinical problem, by using expert consensus.
Committee members were invited to participate in this process based on their area of interest, and their clinical and research expertise. Committee members were responsible for overseeing the development of the guidance and were assigned to review and provide critical feedback on each of the main topics based on their clinical expertise and research in mood disorders and occupational mental health. The topic assignments were as follows: introduction and summary sections (PC), guidance development and consensus methods (CD, PC, KN), assessment and diagnosis of work-related depression (AB, JH, GH, SB), pharmacotherapy (MK, RM, SB, JH, PC), psychotherapy (JH, MC, DD), and patient communication and advocacy (CD, AB, PC). In addition, each member of the committee reviewed the entire manuscript and provided feedback. Due to the impact of the COVID-19 pandemic, this guidance was developed through an iterative process involving videoconferencing, telephone, and email communication.
The committee initially reviewed and discussed the document, “Clinical guidelines for the diagnosis and management of work-related mental health conditions in general practice” developed in Australia, and published in 2019 (37). The quality of its guideline development methods was evaluated by two reviewers (CS, KN) using the AGREE II rating system (38). The Guideline Technical Report and the Administrative Report provided useful background information to support the quality of the guidelines (39, 40). The guideline development methods were rated according to the 23 AGREE II items and six dimensions. Each of the two reviewers independently scored each item (on a scale of 1 for the lowest quality to 7 for the highest quality), and disagreements were discussed until consensus on item scores was reached. Each dimension was then scored. The maximum dimension quality score was 100%, which indicated the percentage of items within the dimension that was rated at the highest level (score = 7). The AGREE II scores for six dimensions were (1): scope and purpose (100%) (2), stakeholder involvement (94%) (3), rigor of development (76%) (4), clarity of presentation (94%) (5), applicability (75%), and (6) editorial independence (100%). Of the six dimensions, the “rigor of development” dimension had one of the lowest scores. This was in large part related to little information about the point estimates and uncertainty of the estimates of the research upon which the recommendations were based and the mechanism to be used for updating the guidelines with new and emerging literature. This, however, did not have a meaningful impact on this committee’s work.
The Australian guidelines systematically reviewed the evidence published prior to mid-2017 and explicitly described the link between the recommendations and the supporting evidence. Although the guidelines reviewed most aspects of workplace depression treatments, it was mostly restricted to multi-pronged interventions focusing on specific workplace outcomes and did not thoroughly capture psychotherapy and pharmacotherapy interventions (37, 41). To address this gap, we conducted detailed literature searches for psychotherapy and pharmacotherapy interventions in work-related depression. The search terms included various versions of work or workplace, psychotherapy, and pharmacotherapy (including specific agents), with a supplemental search focusing on cognition and functioning (see Supplementary material S1). In addition, evidence was also identified and evaluated through the experts on the committee, and hand-searching the bibliographies of identified references.
In summary, the recommendations in this paper were based on the Australian guidelines and the author’s updated supplemental and targeted literature search to February 2023 using PubMed1 and expert consensus. Additionally, the recommendations incorporate real-world perspectives of Canadian and international clinicians with expertise in psychiatry, psychology, occupational medicine, family medicine, and public and occupational health. Patient cases that illustrate clinical situations encountered by HCPs when patients present with symptoms suggestive of a work-related mental health disorder are included in Supplementary material S2. A summary of clinical tips for assessing and managing workplace-related MDD is shown in Supplementary material S3.
The diagnosis of a mental disorder should be based on a thorough clinical assessment, using The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria (42). Additionally, validated tools and scoring systems can be very helpful in screening, diagnosing, and assessing the severity of depressive symptoms. Primary care physicians are very accurate in ruling out mental disorders, but less so in identifying the presence of disorders (43, 44).
The Australian guidelines completed a GRADE review of the evidence for tools to diagnose and assess the severity of workers presenting with mental health symptoms (37, 39). They assessed 46 distinct tools including both patient- and clinician-completed questionnaires. Based on evidence from studies conducted in a work context, the Australian guideline recommended the Patient Health Questionnaire-9 (PHQ-9) for depression, and the Depression Anxiety Stress Scale (DASS) for anxiety disorders (37). However, based on the evidence and recommendations of other guidelines, they also recommended the Generalized Anxiety Disorder 7-item (GAD-7) for anxiety disorders (37). These tools are short and patient-completed. It is important to remember that while tools can improve accuracy, the diagnosis should always be confirmed with a comprehensive clinical assessment.
The differential diagnosis of MDD within the context of work should also consider other mental health disorders such as, but not limited to bipolar disorder, attention-deficit/hyperactivity disorder (ADHD), substance use disorders, and adjustment disorder as defined in the DSM-5 (42). Medical conditions, and in the case of work-related symptoms, the role of stress and burnout should also be considered. Useful screening tools to identify comorbid conditions associated with work-related MDD include the Mood Disorder Questionnaire (MDQ) for bipolar spectrum disorders (45), the ADHD Self-Report Scale (ASRS) (46), and Alcohol Use Disorders Identification Test (AUDIT) (47). Recently, validated, digital and machine-learning-based screening instruments such as EarlyDetect, promise some modern approaches in screening for MDD and other comorbid disorders such as ADHD and bipolar disorder (48–50). However, more research and clinical experience are required before such programs can replace traditional screening instruments.
In addition to symptom assessment in workplace MDD, it is important to evaluate how symptoms cause clinically relevant distress and impairment in social, occupational, or other areas of functioning. Assessing cognitive impairment is essential since it is significantly associated with social, occupational, and global functioning (51–53). Perceived cognitive function has been shown to have a greater impact on workplace dysfunction than the severity of depression among working adults with MDD (54, 55).
Abnormalities in executive function, working memory, attention, and psychomotor processing speed, have been shown to impact work performance in patients with MDD (54, 56, 57). In addition, improvements in cognitive symptoms are highly significantly correlated with improvements in workplace productivity (58).
Given the importance of cognitive impairment on functioning at work, home, and school, tools to assess cognition should be a part of the assessment of patients with work-related mental disorders. Examples of some of the validated tools for the assessment of cognitive functioning are shown in Table 1 (59–64). One caution when using these tools is the need for suitable norms, i.e., considering age, education, sex, and occupation.
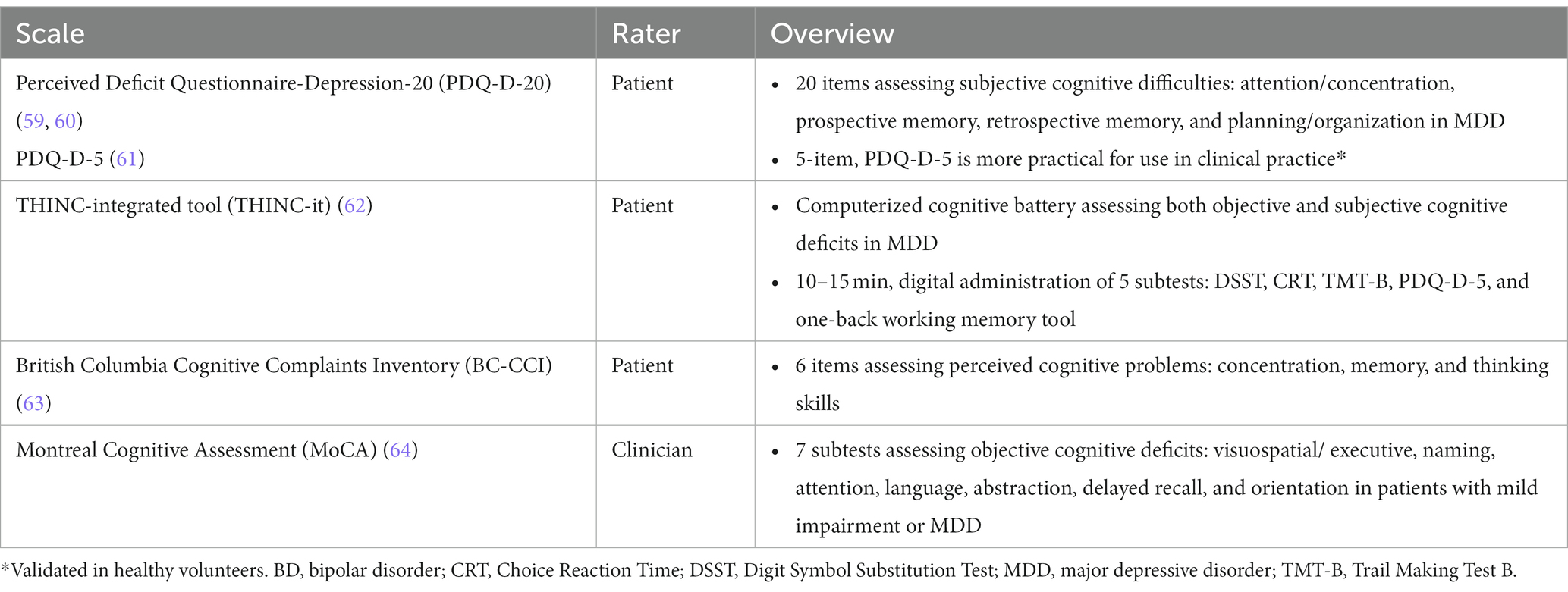
Table 1. Examples of tools to assist clinicians in assessing cognition.
It is important to differentiate between subjective (e.g., as measured by the PDQ-D) and objective cognitive deficits [e.g., as measured by Digit Symbol Substitution Test (DSST)] (61, 65–67). Subjective cognition has been related to depression severity, whereas age has been found to be a greater predictor of objective cognitive ability (66, 67). Self-perceived cognitive function can be affected by emotional state and the severity of depressive symptoms to a greater extent than objective cognitive measures. In addition, subjectively-rated cognitive symptoms have been shown to be a stronger predictor of functional impairment, than have objectively-measured cognitive impairments (68). However, in one study of patients with MDD, 48% had subjective, and 64% had objective cognitive impairment (65). Overall, 80% of patients with MDD met the criteria for one or the other, but only 31% met the criteria for both. Therefore, it is important to measure both to get an accurate measure of cognitive functioning. The THINC-it tool combines objective and subjective cognitive testing (62).
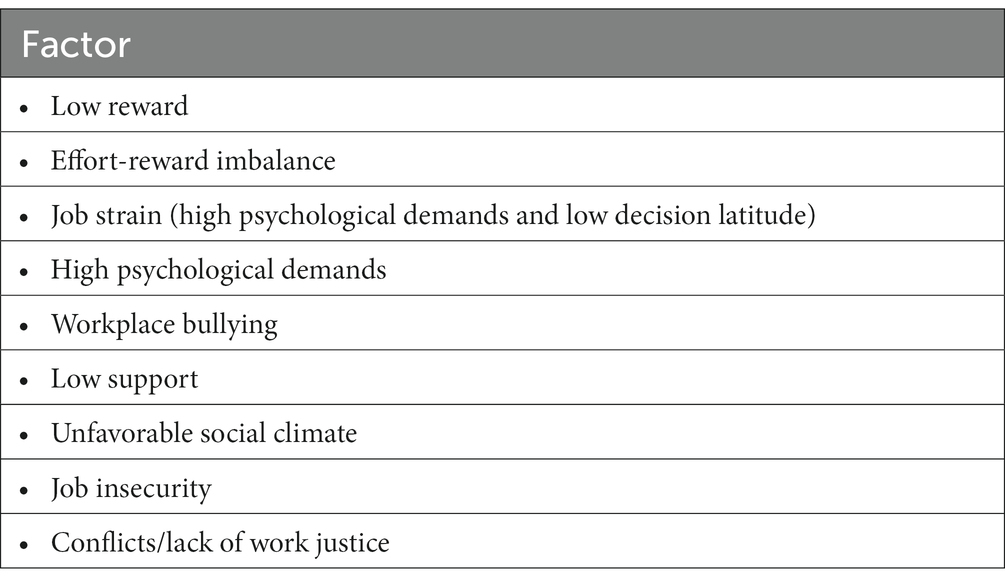
It is important for clinicians to assess work and patient factors that may contribute to workplace mental health disorders, specifically MDD. For example, in a 2013 survey of work-related mental disorders, 31–33% of claims were due to work pressure, and 18–27% to harassment or bullying at work (69). Work pressures were related to work deadlines, interpersonal conflicts with employers or colleagues, disciplinary actions, performance reviews, and promotion disappointments (69). Meta-analyzes of prospective and case–control studies have identified several workplace factors associated with depressive symptoms and absenteeism (Table 2) (70, 71).
In addition to workplace factors, certain patient characteristics may also indicate a higher likelihood of a work-related mental disorder, particularly among those who have experienced a physical or psychological work-related injury (37). These may include specific depressive symptoms of insomnia, low mood, anhedonia, and suicidal thoughts; chronic physical health problems; poor social and personal support system; history of past or current depression, anxiety, substance use, or other mental disorder. Thus, the relationship of a mental diagnosis to work should be based on the clinical assessment and assessment of the factors described in Table 2, and the timing of pressures, events, or changes in the workplace relative to symptom onset (16, 37, 70, 71).
Although screening tools to determine that a mental disorder is related to workplace factors are absent, tools to assess functioning and work impairment can be very useful in clinical assessment. Examples of some of the tools that have been validated for the assessment of functioning are shown in Table 3 (72–78). In addition, the Occupational Depression Inventory (ODI), a validated 10-item instrument, has shown utility to quantify the severity of work-attributed depressive symptoms (77, 78).
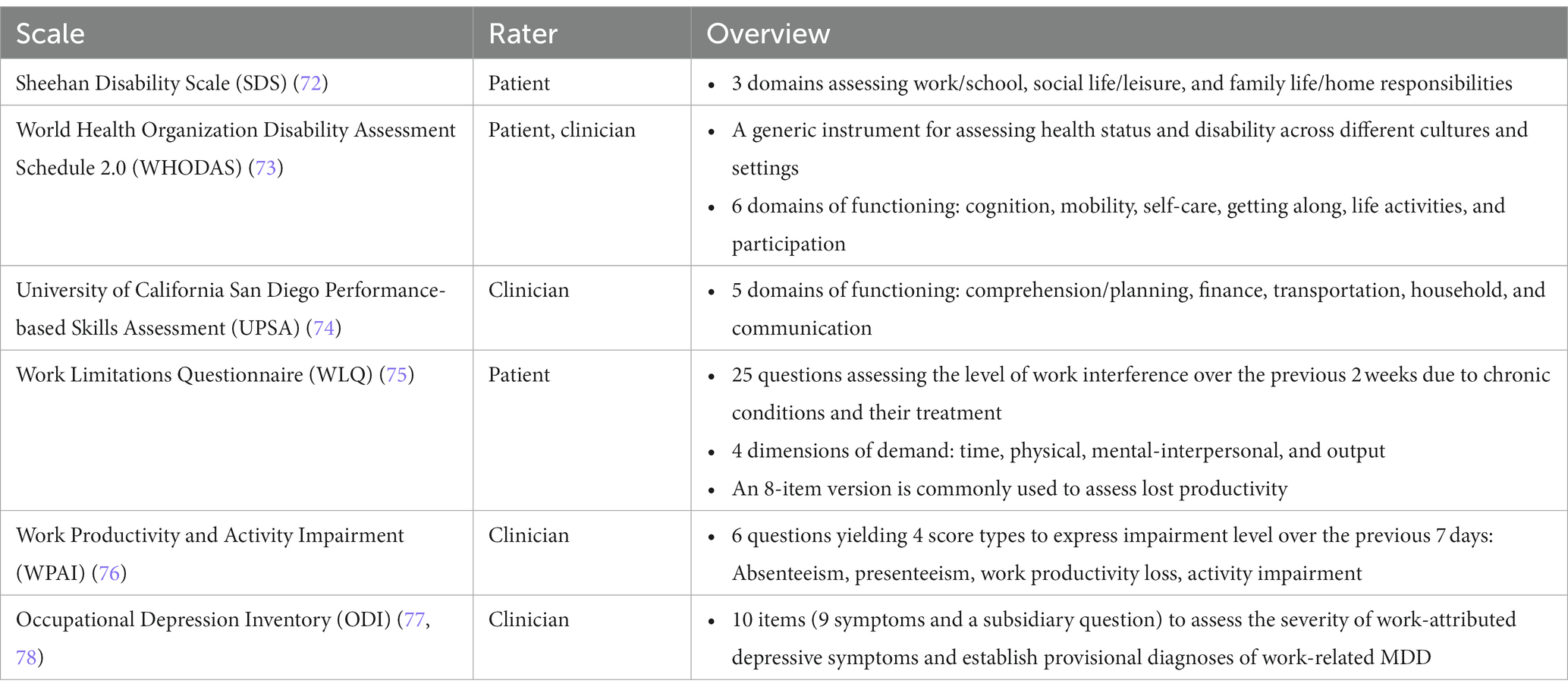
Table 3. Examples of tools to assist clinicians in assessing functioning or work productivity.
Burnout is defined in the International Classification of Diseases 11th Revision (ICD-11) as a syndrome resulting from chronic workplace stress, and it is specific to the occupational context (79). The three dimensions of burnout are exhaustion, mental distancing from one’s job, and reduced professional efficacy (79). There are no DSM-5 diagnostic criteria for burnout (42). Burnout resembles depression, and although some evidence suggests it is a distinct condition (80), this remains controversial (81). A systematic review examining the relationships between burnout and depression or anxiety concluded that the conditions were associated but did not conclusively overlap; burnout appeared to be a different construct (80). However, person-centered longitudinal analysis of symptom clusters found burnout and depression both develop in tandem at similar levels, suggesting conceptual similarity in the work context (82). A meta-analysis of 14 studies suggests the core symptoms of burnout, exhaustion, largely overlap with depression, compared to the putative dimension of detachment and efficacy (83). Both burnout and MDD have each been shown to predict suicide risk; however, burnout was not consistently associated with other suicide risk factors when MDD was present (84). In addition, people who suffer from burnout may present with many symptoms that look like those seen in patients with MDD (Table 4) (79, 80, 85).
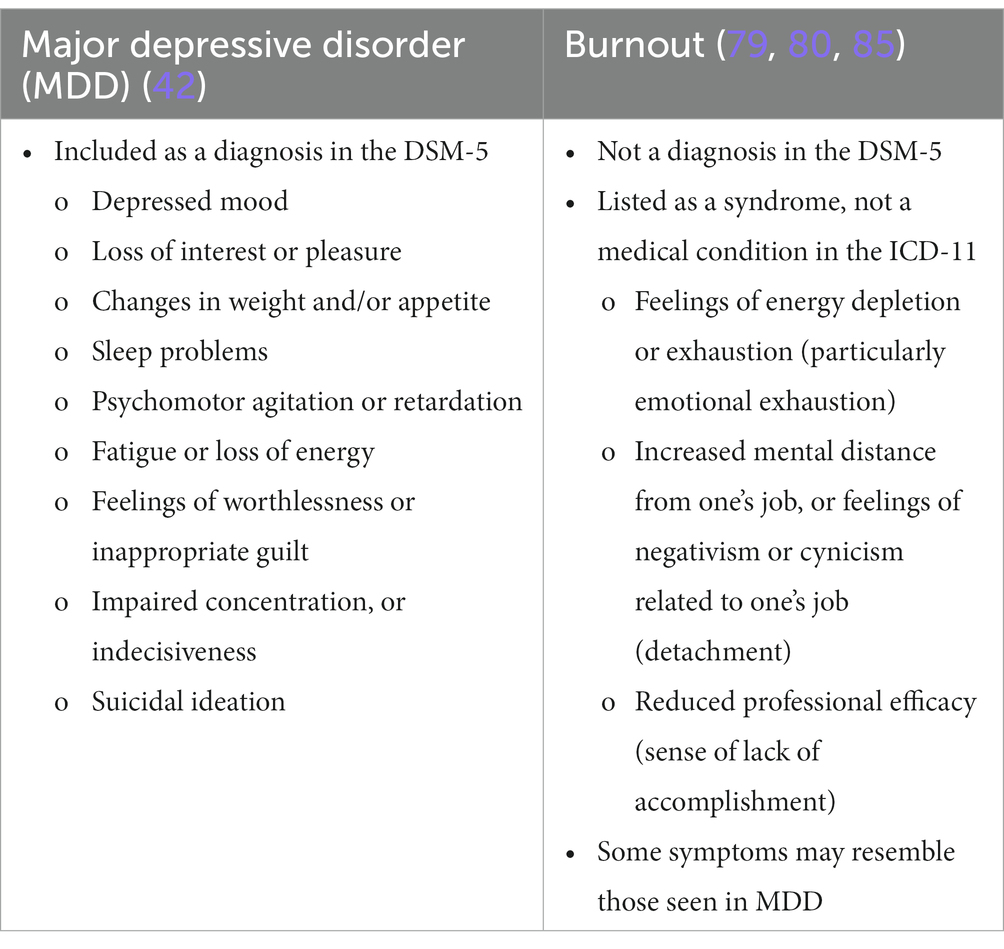
Table 4. Comparing burn-out and major depressive disorder (MDD).
Burnout is commonly assessed using the Maslach Burnout Inventory (MBI) (86, 87). However, because the symptoms included in burnout scales are very similar to some but not all of the symptoms that characterize depression, it is important to determine if patients presenting with burnout have MDD according to the DSM-5 criteria (88).
There are key differences between presentations of malingering, somatoform, and factitious disorder (Table 5) (42, 89, 90). It is important to be aware of and identify individuals who may have alternative gain and do not want to return to work, and to consider these other presentations in the differential diagnosis.
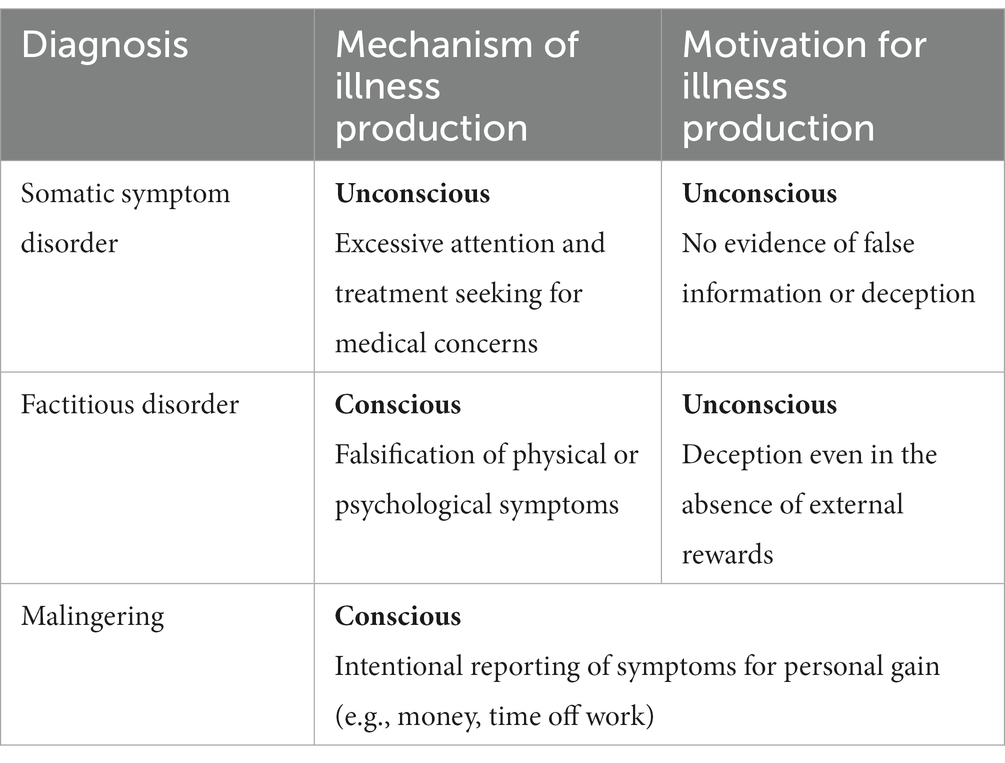
Table 5. Differences between somatoform disorder, factitious disorder, and malingering (42, 89, 90).
Malingering is not a medical diagnosis, and it can be difficult to identify with certainty. It is generally defined as fabricating or exaggerating symptoms (mental or physical) for secondary gains, such as financial compensation, obtaining drugs, avoiding obligations or discipline at school or work, or getting attention (91). Certain factors can increase the suspicion of malingering such as presentation in a medico-legal context, a discrepancy between self-reported stress or disability and medical findings, poor cooperation during an assessment, poor compliance or poor response to prescribed treatments, an unexpected escalation of symptoms, vagueness around prior management strategies, use of multiple different healthcare providers, and a history of antisocial behavior (90, 92). Studies have shown that patients who are malingering report more symptoms than those with confirmed MDD (89, 93). They may endorse suggested symptoms indiscriminately, including those that are atypical or rare, believing this will be more convincing of severe illness (93). Conversely, genuine patients report only the symptoms that they are really experiencing.
It is very challenging to identify malingering in the absence of a patient’s confession or contradictory objective information. The reliability of patient self-reports should be well documented in the patient’s records, and requests be made for an independent medical opinion to clarify the presence of genuine illness and impairment. Malingering might be suspected after conducting a thorough medical history, identifying inconsistency in symptom presentation, and observed mental status, and perhaps employing diagnostic tools such as the Minnesota Multiphasic Personality Inventory (MMPI-3) or the Personality Assessment Inventory (PAI) (94, 95). In the absence of proof of a conscious motivation for obvious personal gain, factitious disorder or somatic symptom disorder should also be considered after a thorough evaluation (Table 5) (42, 89, 90).
Comorbid medical conditions and other mental disorders confer more disability, require more complex treatment approaches, and are associated with longer time to recovery, and a lower likelihood of achieving functional recovery. As a result, comorbid conditions can lead to greater work disability and more absenteeism than MDD alone (20, 96). Depression and anxiety are frequently comorbid, with around 50% of patients with MDD also suffering an anxiety disorder in their lifetime (97, 98). Comorbid anxiety has been associated with increased rates of suicide, poorer response to treatment, increased severity, increased risk of chronicity and recurrence, and differences in neurobiology compared to depression alone (99, 100). Substance use disorders are also common comorbidities in patients with MDD (101). Patients with depressive symptoms should be routinely assessed for anxiety, substance use, and suicide risk. Useful tools were mentioned previously.
An estimated 2.2 million Canadian adults have both physical and mental comorbidity [Canadian Community Health Survey (CCHS), 2014] (102). The presence of a comorbid mental condition in patients with chronic medical conditions were associated with lower health-related quality of life (HRQoL), increased annual healthcare costs, and an increased risk of suicidal ideation (27, 102). Common comorbid conditions included hypertension, cancer, post-stroke, arthritis, cataracts, chronic obstructive pulmonary disease, diabetes, epilepsy, heart disease, pain, migraine, and thyroid disease (27, 103). In patients with cognitive impairments, which are associated with mental health disorders, the diagnosis of early-onset Alzheimer’s disease may also be considered. Comorbid medical conditions may be particularly important to consider when patients experience a mental disorder after suffering a work-related injury (37). Patients with acute or chronic medical conditions who have high rates of absenteeism or presenteeism, or those who fail to return to work after a physical or psychological injury, should be evaluated for a mood disorder. A Canadian study found higher odds of functional limitations in patients with comorbid mental and physical health disorders, highlighting the importance of treating both mental and physical health to improve functioning and prevent future decline (104).
Factors to be considered when conveying a diagnosis of work-related MDD to the patient include information on the diagnosis, the importance of therapeutic alliance, and educational information to address patient concerns, such as stigma/discrimination, loss of employment, isolation, and financial insecurity (37). In helping patients return to work, multiple factors should be considered including weighing various clinical factors, the nature of the work-related stress, the severity of disability and limitations, the motivation of the worker to continue working and the availability of support systems, integrated services, and coordinated treatment plans.
The Australian guidelines reviewed evidence from seven cross-sectional or cohort studies that assessed patient characteristics and work-related factors that are associated with longer-term inability to work (37). These characteristics shown in Table 6 can help a clinician determine when a person with a mental disorder has the capacity to return to work. Similarly, a prospective observational study of patients on sick leave being treated for mental disorders found that several work characteristics influenced return to work. These included control over decision making, support from colleagues, respect and recognition, and job promotion opportunities (105). Additionally, the person’s self-assessed present and future ability to work and symptom burden also predicted return to work.
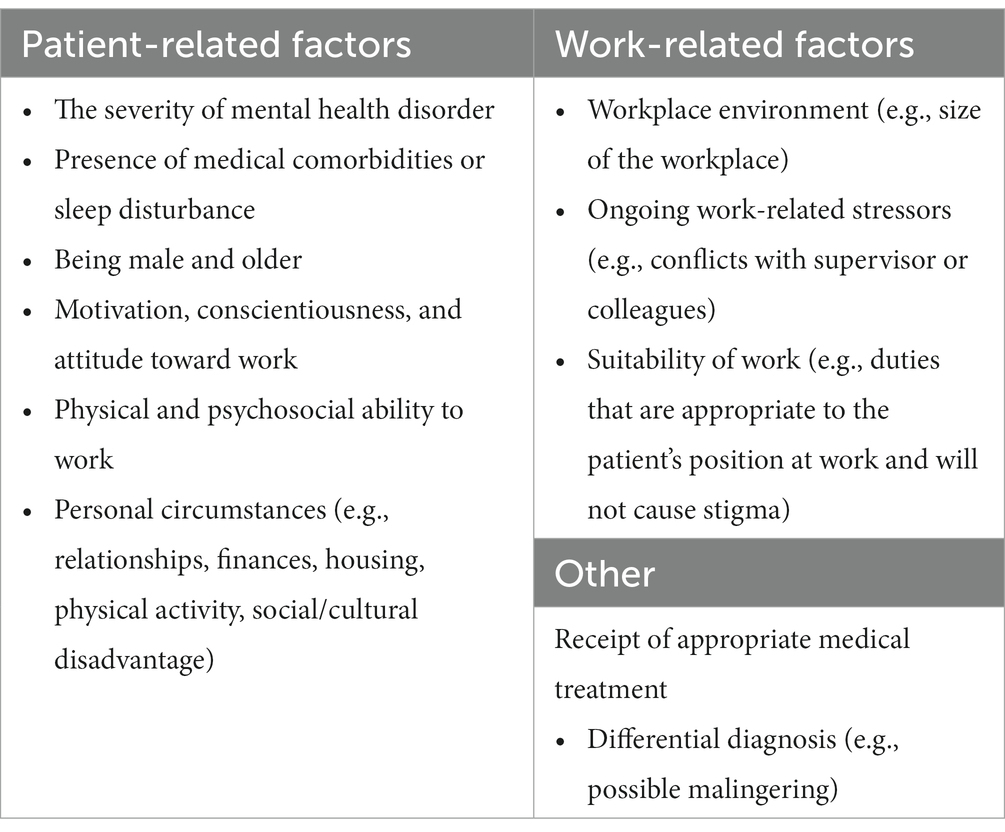
Table 6. Factors to consider when evaluating a patient’s capacity to work (37).
From a psychiatric perspective, impairment and disability are substantially different. An individual with a psychiatric impairment does not necessarily have a related work disability. The clinical assessment of work functioning in individuals with mental health conditions is complex and assessment practices are highly variable. The occupational medicine concepts–impairment, capacity, limitations, restrictions, disability, accommodation, and worklessness–can help clinicians organize their approach to the evaluation of the patient’s functional capacity, sick-leave/disability or return to work status (106). Furthermore, understanding and assessing these concepts are critical to evaluating fitness to work, completing insurance forms, and tracking functional outcomes.
Impairment is what is considered “wrong” with the body’s or, in these cases, the mind’s functioning and is formally defined as “A significant deviation, loss, or loss of use of any body structure or body function in an individual with a health condition, disorder, or disease” (107). Impairment with regard to a psychiatric diagnosis is usually related to the severity of the symptoms, and the degree of functional impairments in various domains such as work, family and social life, and cognition (See Tables 1, 3).
Capacity in the context of workplace evaluation usually refers to the employee’s current ability or strengths to do their required work. In terms of physical aspects, it includes attributes such as strength, flexibility, and aerobic endurance. In mental health disorders, it includes evaluating mood, anxiety, emotional stability, and cognitive functions such as attention, concentration, and memory among others. Capacity can vary depending on the nature of job demands and context. An important aspect of capacity assessment is understanding job description, expectations, and role of the employee, which is often provided by the employer (see Section 6).
Functional limitations include the things an individual reasonably cannot do, despite a good effort, as a result of a medical or psychiatric condition. A physical example would be an inability to lift heavy items, due to a fracture or sprain. From a psychological perspective, it may be useful to assess limitations associated with MDD within cognitive, emotional, social, and physical domains (Table 7) (108). Examples of cognitive limitations include problems with memory, concentration, multitasking, completing assignments, meeting deadlines, prioritizing tasks, and reading social cues. Emotionally, patients with MDD often have poor motivation, a low tolerance for stress, social interaction, and getting along with customers or fellow employees. Physically, individuals often have slow response times, trouble sustaining energy and maintaining the stamina to work productively. Clinicians should be mindful of the potential side effects of medications causing workplace limitations due to headaches, gastrointestinal upset, sedation, fatigue, and tremors. It should be emphasized that patients may experience impairment but not have a functional limitation in work role.
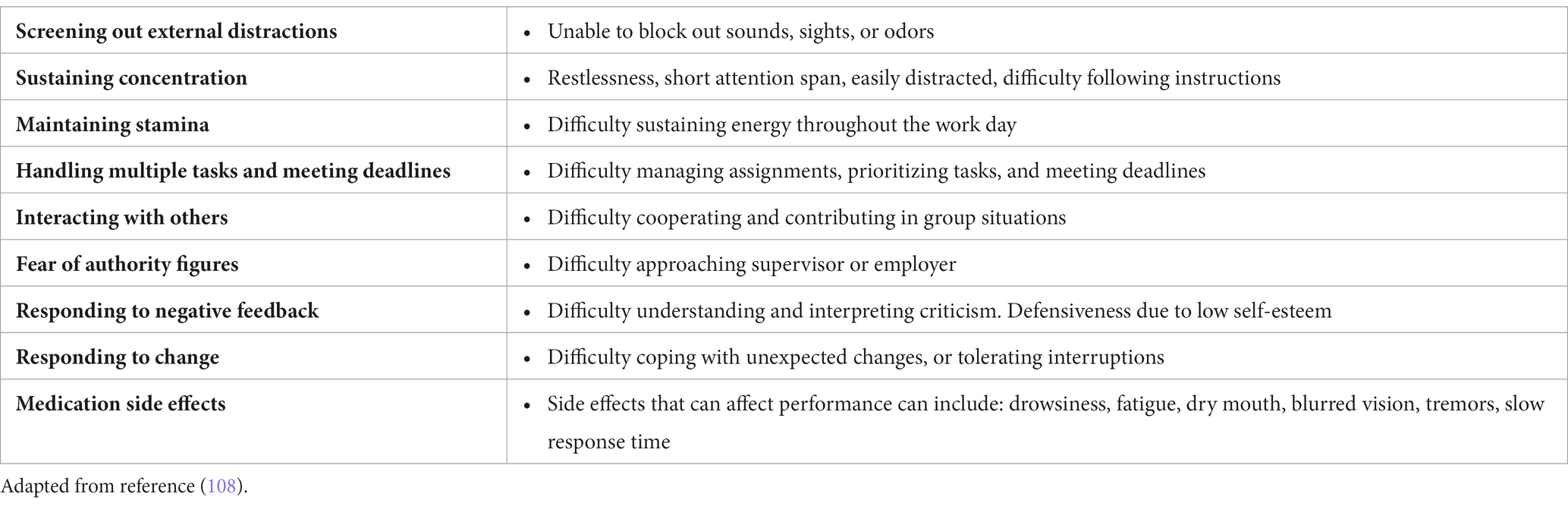
Table 7. Examples of functional limitations related to mental health disorders.
After a thorough medical evaluation, restrictions are activities that clinicians advise against performing as it may cause harm or worsen symptoms. A well-known physical example is the restriction on driving following a diagnosis of epilepsy due to the unpredictable risk of seizure and the danger involved. A psychiatric restriction may apply to someone like a law enforcement officer at risk for suicide who should be temporarily restricted from firearm access. Other examples of restrictions include operating machinery or working in a safety-sensitive position. Temporary restrictions can also apply to potential medication side effects such as sedation, cognitive impairment, and gastrointestinal upset. Restrictions and limitations can be temporary or permanent (Table 7) (108).
Disability can be thought of as an inability to fulfill a role, such as a job, due to an impairment and is formally defined as “Activity limitations and/or participation restrictions in an individual with a health condition, disorder, or disease” (107). A work-related psychiatric disability would be an inability to participate fully in a job role due to the effects of symptoms of the disease on the job demands and subsequent limitations with or without restrictions.
An accommodation is an adjustment to the job or work environment that makes it possible for an individual with restrictions or limitations to return to work earlier and safely and re-enable them to perform most of their job duties. For example, an accommodation for an individual with insomnia could be a later start to the workday for a defined period of time or upon reassessment of the response to treatment (see Section 5).
More than just losing gainful employment, worklessness speaks about the impact of a loss of meaningful roles in life, such as a worker, student, volunteer, or a parent. The term was introduced in the 2006 British report “Is Work Good for Your Health and Well-Being?” (26). As described above, there is evidence that unemployment is generally harmful to health (25, 26). Avoiding the potential health consequences of worklessness is the foundation of ethical return-to-work/stay-at-work assessments in that it is usually healthier to be at work, in a safe and timely manner.
The phrase “fitness for duty” is often used in the context of jobs that include a safety-sensitive component, such as police, fire, or railway workers. Safety-sensitivity could include a danger to self, coworkers, the general public, or the environment. When making disability assessments the clinician should be aware that public safety may trump the individual’s right to work (see Section 6) (109).
The assessment of fitness to remain at work or to consider time off can be challenging. As a clinician, it is important to understand the relationship between mental health symptoms, disorders, and impairments that interfere with carrying out work duties. Primarily, impairments (a deviation or loss of functioning due to a disorder) may or may not lead to a limitation or restriction. It is essential to determine a relationship between how a specific symptom interferes with performance of a specific job requirement. Most existing mental health screening tools, neuropsychological tests, and the mental status examination help in screening for mental health disorders but have limited value in determining performance of work demands or the entire work role. Furthermore, disentangling daily life stressors and work factors can make the fitness assessment challenging.
A fitness assessment should include collateral information about the work environment, reported work stress, conflicts, negative evaluations, and details of the type of work. Functioning assessment will involve an integrative approach using self-report, collateral information from employer and disability professionals, as well as functional and cognitive screening tools such as the SDS, WHO-DAS, or PDQ-5 (see Tables 1, 3). Urine drug screening may be helpful for those with concurrent substance use issues or relapses due to medication non-adherence.
Finally, a formal assessment of barriers to return to work should be identified. Some of the barriers to return to work include the severity of disease, motivation to return to work, work stress, and barriers to mental health services such as recognizing the need for treatment, attitudes associated with stigma, treatment, and a desire to handle the disease independently, and structural issues around finances and access to services.
Numerous studies, systematic reviews, and meta-analyzes have shown that antidepressants are more efficacious than placebo in adults with MDD (110, 111). Current Canadian guidelines from CANMAT recommend most second-generation antidepressants for the first-line treatment of patients with moderate or severe MDD (Tables 8, 9) (112). Nonpharmacological treatments are preferred for patients with mild MDD.
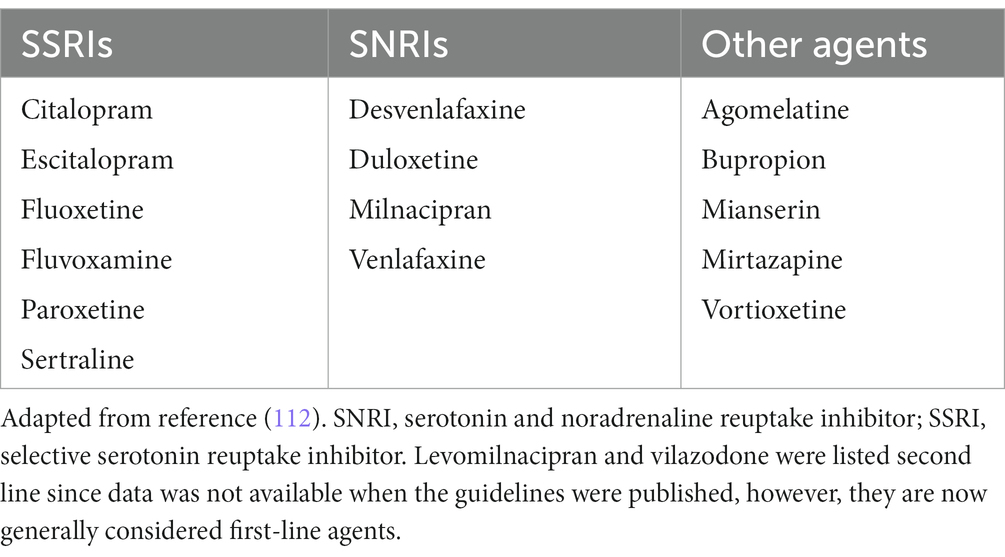
Table 8. 2016 CANMAT guideline recommended first-line antidepressant treatments for MDD in the general population.
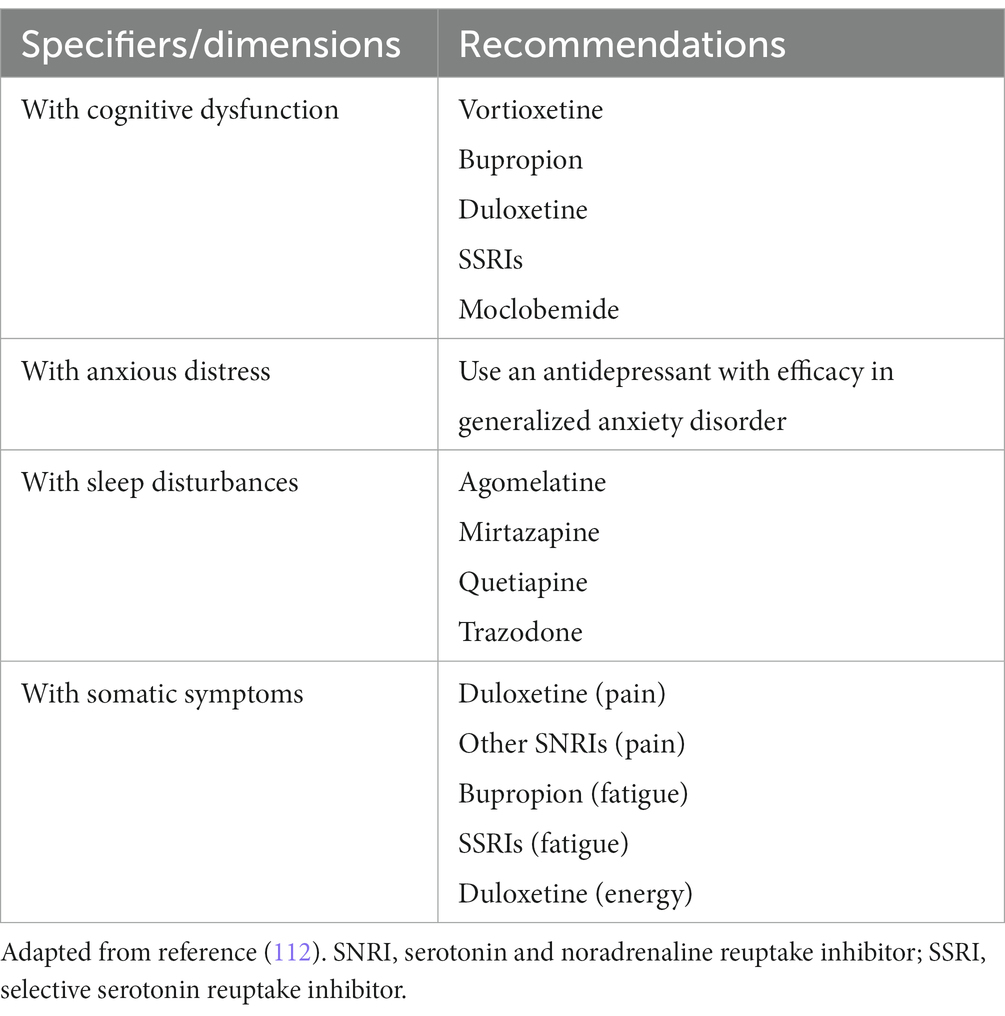
Table 9. 2016 CANMAT guideline recommended antidepressant treatments according to specifiers or dimensions of MDD (112).
An important caveat is that existing guidelines and recommendations for pharmacological and nonpharmacological approaches include data drawn from clinical trials, which generally do not include comorbid populations and, therefore, differ substantially from the patients seen in real-world clinical practice.
When evaluating therapies for work-related MDD, it is important to assess antidepressants beyond their effect on depressive symptoms and to consider other outcomes such as cognition and reward processing, work function, sick leave, and return to work.
As discussed in Section 3, impairments in cognition play a major role in workplace dysfunction. Cognitive impairment has been associated with decrements in social, occupational, and global functioning, and has been shown to have a greater impact on workplace dysfunction than the severity of depressive symptoms (51–55, 57).
A meta-analysis of 9 placebo-controlled RCTs, which included mainly vortioxetine, duloxetine, and SSRIs, found that antidepressants had a positive effect on psychomotor speed and delayed recall (113). Canadian guidelines include suggestions for specific pharmacological treatments based on clinical specifiers and dimensions of MDD (112). For patients with cognitive dysfunction preferred pharmacotherapies include: vortioxetine (level 1), bupropion, duloxetine, or an SSRI (level 2), or moclobemide (level 3) (112). Nonetheless, the issue of generalizability of the clinical trial data to work-related MDD is lacking.
As described in Section 3, measurement tools to assess functioning can be very useful during clinical assessment. One of the most commonly used measures of work-related functional outcomes is the Sheehan Disability Scale (SDS), and in particular the SDS-work item (i.e., the symptoms have disrupted your work/school work; rated on a scale of 0–10) (72). One limitation of the SDS is that it captures role functioning at work rather than work functioning. Although other tools such as Work Limitations Questionnaire (WLQ) (75) and Work Productivity and Activity Impairment (WPAI) (76) capture work functioning, they are not routinely used by most clinicians as they were developed for group-level usage.
Antidepressant treatment trials with work-related outcomes were identified from systematic reviews (114–117), updated with Medline searches as of February 2023. A total of 27 RCTs were identified that provided subjective measures of work-related disability and/or productivity (mainly SDS-work measures). Functional outcomes are generally secondary endpoints in RCTs and often the data are not included in the primary study publication. For this review, studies were included if they were randomized, double-blind, placebo- or active comparator-controlled study design, included a work functioning outcome measured at baseline and endpoint, and the data were available in the primary publication or one of the systematic reviews. The results of 22 studies comparing an antidepressant to placebo (118–139), and 5 studies comparing 2 different antidepressants (140–144) are shown in Supplementary material S4. Most selective serotonin reuptake inhibitors (SSRI), serotonin and noradrenaline reuptake inhibitors (SNRI), noradrenaline and dopamine reuptake inhibitors (NDRI), and multi-modal antidepressants showed positive benefits on measures of work impairment; however, results of individual studies were highly variable. This may be due in part to the fact that work outcomes were secondary endpoints, and studies may not have been powered to adequately assess these outcomes.
In summary, the body of evidence suggests that antidepressants from different classes are associated with secondary improvements in work functioning, but there is little evidence to suggest a specific medication is preferable for patients with work-related MDD.
A systematic review of interventions to improve return to work in patients with MDD identified 6 studies assessing the effects of antidepressants on the duration of sickness absence (Table 10) (41, 145–150). The results of 3 studies comparing SSRI to SNRI were inconsistent (41, 145–147), with 2 studies showing no differences between agents (145, 146), and one showing a greater benefit with the SSRI, escitalopram compared to the SNRI, duloxetine (147). Another study also showed a benefit with escitalopram compared to another SSRI, citalopram (148). No differences were found between a SSRI and a TCA in reducing sickness absence or work functioning as measured by the Social Adjustment Scale (SAS) work composite (149). Compared to placebo, one study found no benefit of a TCA or a MAO on sickness absence, but a significant positive effect on the work (150).
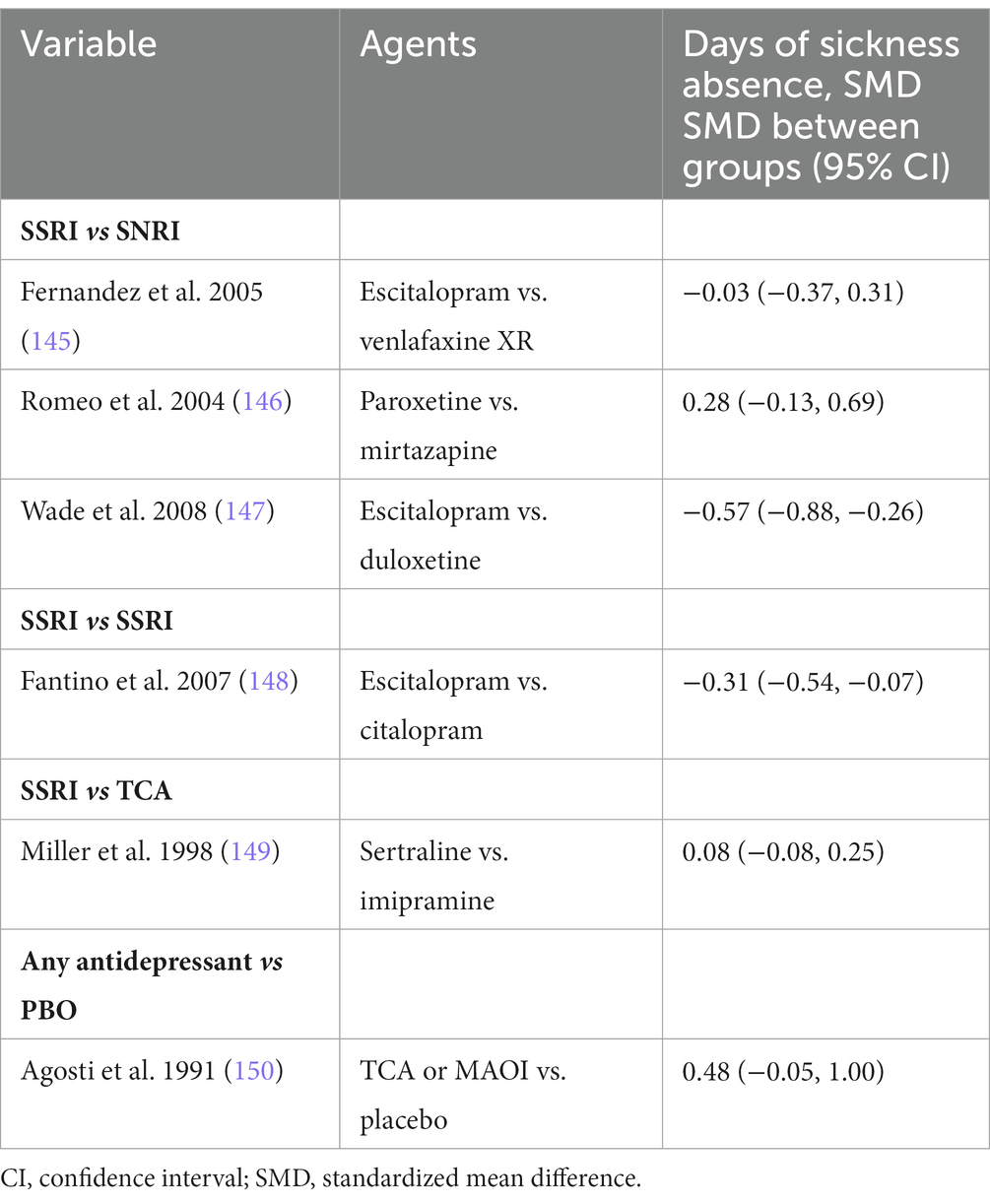
Table 10. Randomized controlled trials measuring the effects of antidepressants on sick leave (41).
Two other studies looked at the number of underproductive or lost days per week as measured by the SDS subscores (118, 143). One study found decreases with both vortioxetine (from 5.3 to 2.7 days) and venlafaxine XR (from 5.2 to 3.0 days) at week 8, but between-group statistics were not reported (143). In another study, reductions were significantly greater with agomelatine compared to placebo (number of lost work days −1.13 days, and number of underproductive days −2.03) (118). In summary, antidepressants seem to reduce sick leave and earlier return to work, but no differences were identified between classes.
The benefits of antidepressant treatment on work functioning, including absenteeism and presenteeism, have also been demonstrated in observational studies conducted in real-world settings.
The Prospective Epidemiological Research on Functioning Outcomes Related to Major depressive disorder (PERFORM) study was a large 2-year European observational study (151). Initiation (79% of patients) or switch of antidepressant monotherapy (21%) (per routine clinical practice) was associated with improvements in both depressive symptoms (e.g., PDQ-5, PHQ-9 scores) and functional impairment (e.g., SDS total score, WPAI absenteeism and presenteeism scores) (151).
The Assessment in Work productivity and the Relationship with Cognitive symptoms (AtWoRC) study was a real-world open-label study in Canadian working adults with MDD. The study showed significant improvements in cognitive function and workplace productivity with vortioxetine at both week 12 (58), and 1 year (68). WPAI presenteeism was more strongly correlated with other measures of workplace productivity (i.e., SDS work/school and the overall WLQ productivity loss score) than WPAI absenteeism (152). Results of a pharmacoeconomic analysis showed that these improvements were associated with a savings of $4,550/per patient/per week (2017 CAN$) over the 1-year study (33). In the Real-Life Effectiveness of Vortioxetine in Depression (RELIEVE) study, vortioxetine significantly improved all work productivity measures (sick leave, absenteeism, and presenteeism) compared to baseline at week 24 (153).
Recently there has been interest in the use of esketamine and ketamine, with CANMAT recommending ketamine as a third-line choice for patients with treatment resistant depression (154). In terms of effects on functioning, a meta-analysis of randomized and observation studies found mixed results were reported with respect to effects on general functioning (155). Data from the Canadian Rapid Treatment Center of Excellence on the use of ketamine in 171 patients with treatment resistant depression in community practice found a significant reduction in workplace disability, and symptoms of presenteeism and absenteeism (156).
In the general population, RCTs, systematic reviews, and meta-analyzes, have shown that psychotherapies, particularly CBT, are effective for the treatment of MDD compared to placebo (157–161).
Canadian guidelines from CANMAT recommend CBT, interpersonal therapy (IPT), and behavioral activation (BA) for the first-line treatment of acute MDD (Table 11) (162). Combination therapy with antidepressants is preferred as this has generally been shown to be more effective than either treatment alone, particularly for patients with moderate to severe depression (25, 26, 160, 161).
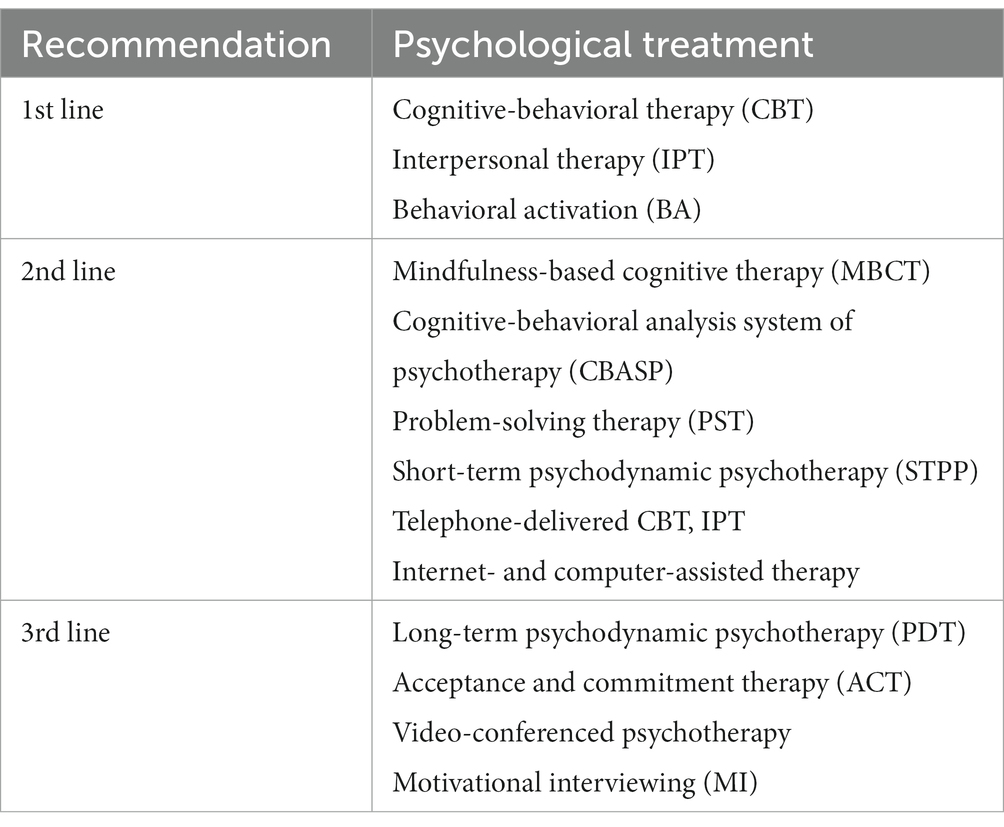
Table 11. Psychological therapies for acute treatment of MDD (162).
A meta-analysis of RCTs found that both psychotherapy and pharmacotherapy had significant beneficial effects on functioning (SDS or SAS) and quality of life (Q-LES-Q or SF-36) in patients with depression (163). The combination was more effective than either treatment alone.
In a meta-analysis of 28 studies of the effectiveness of workplace-delivered digital mHealth interventions (e.g., CBT, mindfulness/meditation, stress management) there was a small, but significant effect on engagement and productivity, but effects on absenteeism and presentism were not significant (164). In a pragmatic trial, a digital mindfulness app showed similar benefits; however, drop-out rates were very high with only 15% of participants completing all 5 assessments over 8 weeks (165). An analysis of studies over time found no evidence of an increase in efficacy of these interventions over the past decade, despite a tripling of the number of studies and the advances in technology (166). Of note, most of these studies were on unselected employees, and only a minority were on individuals with mental health conditions or high stress levels (164–166).
A pilot study showed a significant improvement in work productivity associated with a brief group CBT intervention that was tailored to work-related issues (167).
In terms of specific work-related outcomes, a systematic review and meta-analysis found 16 RCTs that assessed the efficacy of psychotherapies for return to work in patients on sickness absence due to mental disorders (depression, stress disorders, and mixed diagnoses) (168) Among patients with mental disorders, the psychological interventions were significantly more effective in reducing sickness absence overall, and compared to treatment as usual (effect sizes = 0.13) (Table 12). There were no significant differences between different psychological treatments (0.21) or psychological vs. non-psychological treatments (0.37). In addition, studies that included an intervention that targeted work-related processes (9 of 30 trials) were more effective than those that did not (Table 13) (168). In these studies, the types of return to work interventions varied substantially, and the key mechanisms to target in work-focused interventions remain unclear.
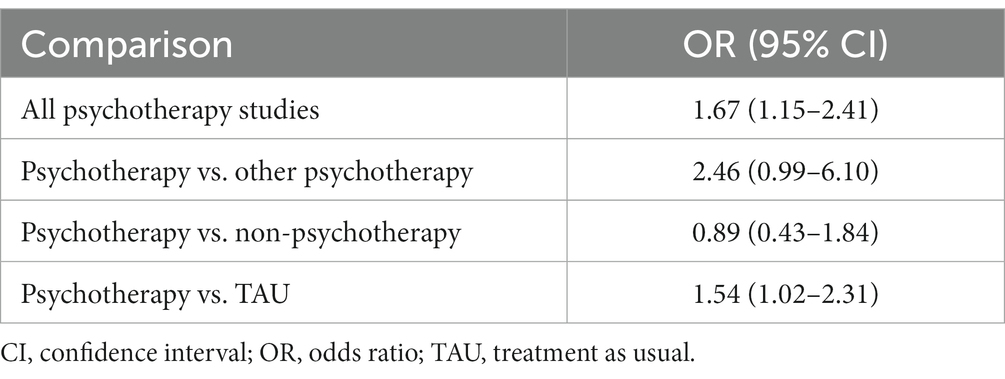
Table 12. Effect sizes (odds ratios) for proportions of patients with mental disorders with partial or full return to work (168).
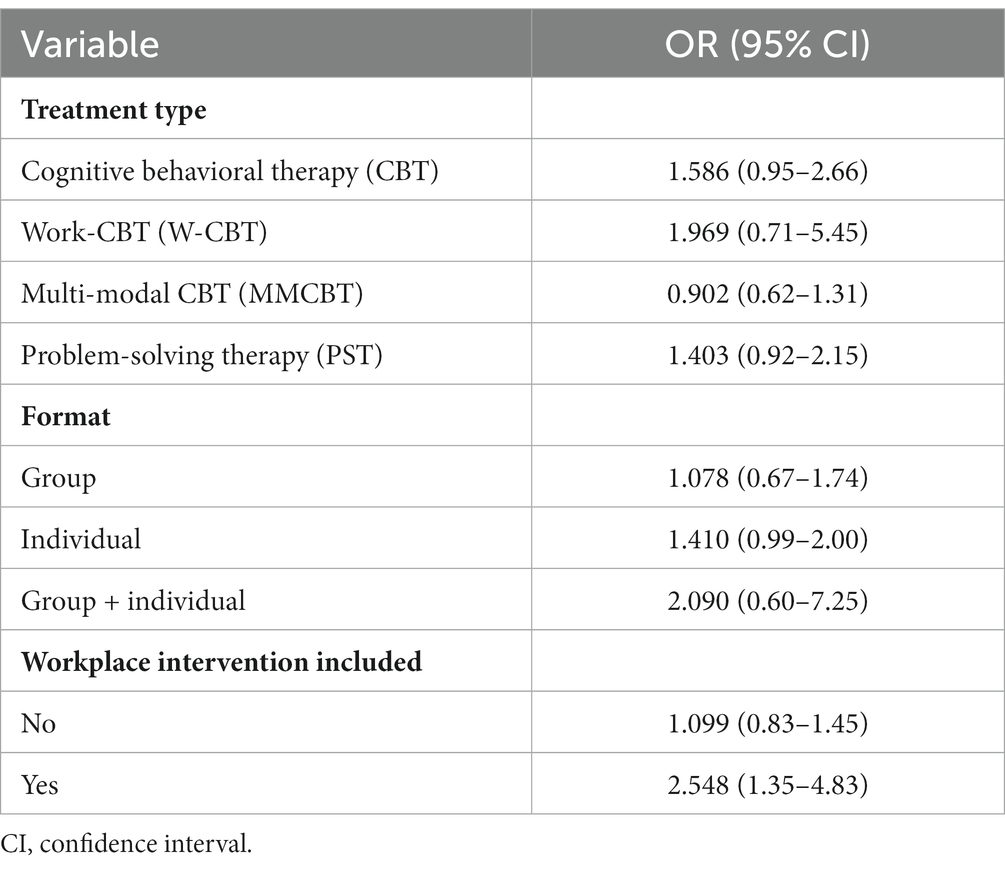
Table 13. Effect sizes (odds ratios) for proportions of patients with mental disorders with partial or full return to work according to the type of psychotherapy (168)
Similarly, a meta-analysis of 45 RCTs, found small but significant reductions in sick leave and symptoms with psychological treatments in patients with common mental disorders (e.g., diagnosis or symptoms of depression, anxiety, stress or insomnia) (169). There were no significant differences between CBT, collaborative care, work-focused interventions, or problem-solving therapy. An analysis that included 21 RCTs found that web-based psychological interventions delivered in the workplace had significant effects on both psychological well-being and work effectiveness compared with control groups (170). In this meta-analysis, no significant differences were found between CBT versus other psychological therapies, and offering guidance versus self-guidance for the work effectiveness outcome. In another meta-analysis of 6 studies internet-delivered CBT was not associated with a reduction in sickness absence compared to control groups (171).
Clinicians managing patients with work-related depression have multiple roles including patient care, as well as integrating with the workplace (e.g., human resources) and insurance provider (Figure 1) (37). Factors in the work environment that impact return to work were discussed in Section 2 (16, 37, 105). Although physicians may not be able to directly impact factors at work, they should be aware of the challenges their patients might be facing, and any workplace programs that are available to their patients. The need for sick leave, workplace accommodations, or referral to other specialties (e.g., occupational medicine specialist, occupational therapy, psychology, physiotherapy, or patient advocacy groups), may be mediated in part by the resources currently available at the patient’s workplace. As a part of integrative treatment strategies, the sections below will address the role of the clinician with the patient (employee), workplace (employer), and insurance provider.
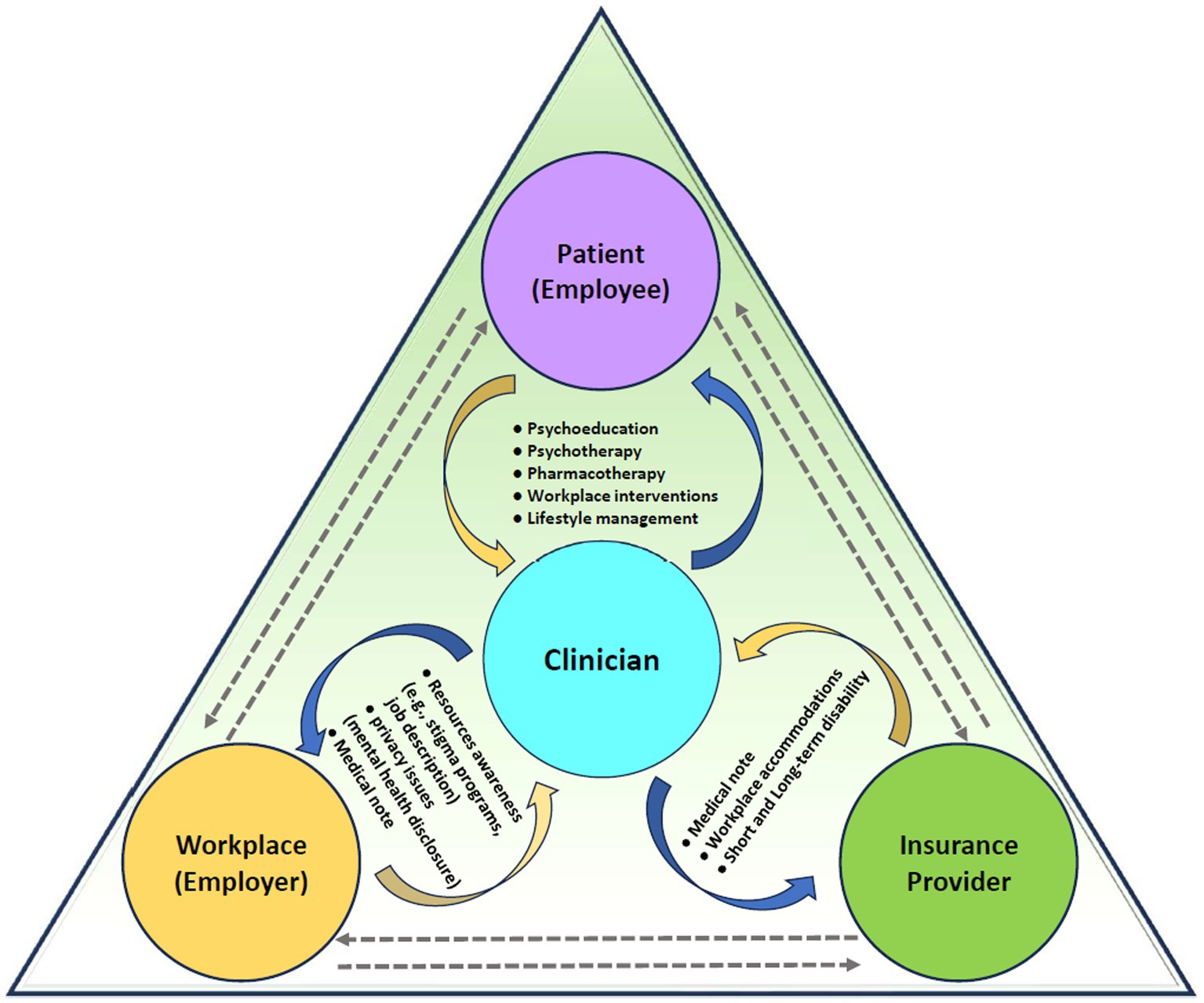
Figure 1. Elements of integrated care for patients with work-related mental health disorders.
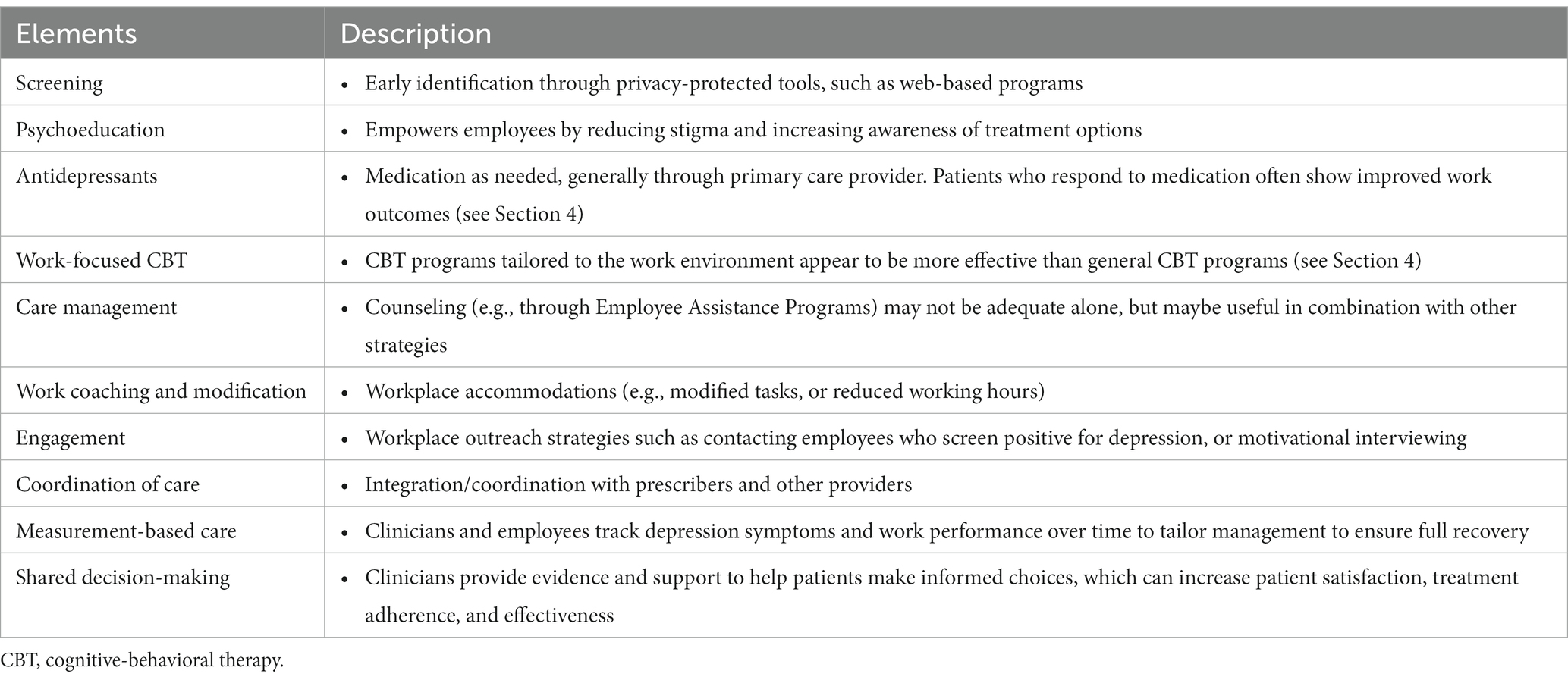
For patients with work-related mental disorders, effective interventions include psychoeducation, pharmacotherapy, and psychotherapy (see Section 4), and work-focused interventions (e.g., addressing interpersonal conflicts, providing work accommodations) (Table 14) (16, 172). A systematic review including 36 studies found that multi-domain interventions that included at least 2 of 3 domains (e.g., healthcare provision, service coordination, and work accommodation) significantly reduced duration away from work and had a positive impact on cost outcomes among patients with mental disorders (173). For example, the addition of psychological treatment, such as online CBT, to usual care reduced sick leave by 15 days (41). Other interventions, such as improving or streamlining the organization of care, adding a structured telephone outreach and care management program to pharmacotherapy, or adding specific providers for depression care, also helped to reduce sickness absence days (41).
Clinicians alone cannot affect all the dimensions needed to ensure a patient’s functional recovery and return to fully productive work. In addition to clinical care, clinicians must be aware of possible workplace interventions as this has been shown to improve outcomes in work-related depression. A meta-analysis of nine studies in patients with MDD found that a combination of a work-focused intervention and a clinical intervention reduced sickness absences by 25 days within the first year of follow-up, in addition to reducing depressive symptoms (41). Work-focused interventions assisted employees in getting changes in work tasks or working hours, supported a gradual return to work, or helped workers adjust to work situations (41).
In addition to pharmacotherapy, psychotherapy and workplace interventions, lifestyle management approaches such as exercise should be strongly considered to manage workplace depression. While many studies have assessed the use of exercise-based interventions for mental disorders, specific evidence supporting the use of such modalities for improving work-related outcomes is scarce. A Cochrane systematic review of interventions to improve return to work in patients with MDD included two randomized controlled trials (41, 174, 175). For the outcome of reducing sickness absence, supervised strength exercise was more effective than relaxation, whereas aerobic exercise was not more effective than relaxation or stretching. Two additional randomized trials were found (176, 177). In a 12-week trial among 946 patients with depression, physical exercise was as effective as usual care by a physician in improving self-rated work capacity (176). Another study found that while both treatments lowered the rates of long-term sick leave over time, physical exercise was significantly superior to treatment as usual at 3 months, but not at 1 year (177).
In treating work-related depression clinicians are encouraged to engage with the workplace to enhance treatment outcomes. Unfortunately, multidisciplinary collaboration for the management of patients with work-related mental disorders may be under-used in clinical practice (178). In one survey, 40% of primary care physicians had never had contact with an occupational health physician, and 49% had not had contact with psychotherapists (179).
Clinicians should liaise with workplace coordinators (with the permission of the patient). Some companies (especially larger organizations) have dedicated personnel to manage disability claims and coordinate care, whereas others may offer these services through their insurance companies. A scoping review found that the lack of coordination between stakeholders involved in the process creates confusion around returning to work for patients with a mental disorder. A coordinator can help involve all relevant stakeholders (178). The coordinator should be knowledgeable about rehabilitation and mental health services, organizational procedures and management values, and the needs of workers and the organizations (178). Liaising with these coordinators (with permission of the patient) can help ensure access to comprehensive treatment including medication and psychotherapy, facilitate communication with patients on sick leave, monitor progress, and develop a plan for returning to work. These coordinators have the added benefit of helping to ensure that patients do not feel cut-off and isolated, especially if they have limited social support.
Coordination of care between the various stakeholders is vital to promote successful return to work. With the patient’s consent, clinicians are obliged to communicate with other care providers, the patient’s employer, or other individuals or entities involved to facilitate the return to work process and prevent the fragmentation of care. Often, it may be helpful to have the patient participate in these conversations. An additional benefit of constructive communication between the clinician and a patient’s employer is the identification of workplace factors, both medical and non-medical, hindering worker recovery. Such a collaborative approach provides a greater opportunity to address potential barriers (37).
Achieving successful return to work has some essential ingredients, regardless of the health condition. Physicians are just part of the recipe. The Institute for Work and Health has developed a booklet called “Seven principles for successful return to work”2 which can help clinicians understand the process (180).
Even when a patient provides consent for a clinician to communicate with third-parties, an employer is not entitled to know the specifics of a worker’s mental health diagnosis. However, an employer may request that a clinician confirm that the employee’s condition limits or restricts them from performing the essential duties of their role. If they are unable to work in any capacity, then medical documentation would need to meet thresholds for “disability” as defined by an insurance provider.
When discussing a work-related mental disorder with a patient’s employer or providing information to other relevant third parties such as a private insurer, it is the clinician’s responsibility to ensure that the focus is on the workplace and the employee’s needs and functional capacities as they relate to the work role. Clinicians may find it helpful to obtain a detailed job description, or checklist describing the duties and expectations of the job. The Canadian Medical Association has published a policy statement outlining the role of clinicians in the completion of third-party forms (Table 15) (181).
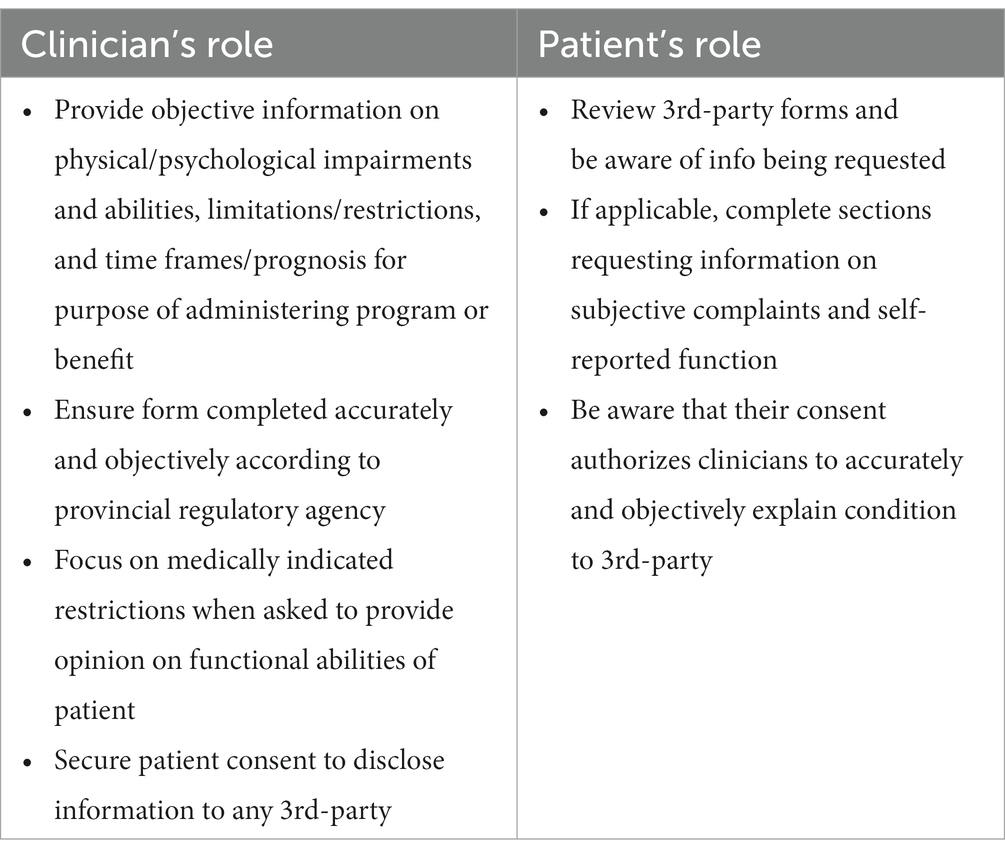
Table 15. Summary of Canadian Medical Association policy statement on third-party forms (181).
The individual worker must decide whether, and to what extent, to discuss their mental disorder with their supervisor or other relevant individuals at the workplace. There are situations where such a discussion would be beneficial or even necessary to provide the required accommodation and support. The worker should be encouraged to engage their supervisor as support, as this will facilitate an understanding of changes in work behavior, and a discussion of the eventual resumption of usual productivity levels. It also should be noted that there are instances in which workers may decline to disclose their disability to their employer and continue to be productive at work. The decision to discuss their mental disorder with a supervisor should be made while considering the type of job and culture of the workplace.
Although workers are legally entitled to accommodation, a knowledge and skills gap may exist among employers regarding their awareness of the legal expectations, and effective approaches regarding how to discuss and provide needed accommodations for a worker. Similarly, workers also may not know how to articulate the difficulties they are experiencing with their job assignments, or not know how to communicate their needs. Patients should be reminded that it is their responsibility to inform their employer about specific needs as they arise and be prepared to provide supporting medical documentation if requested.
In the 4-part series, Healthy Brains at Work, conducted by the Conference Board of Canada, 93% of employers surveyed had supportive policies and practices in place to provide the flexibility needed for workers to remain on the job while receiving treatment or recovering (182).
The decision of whether to inform co-workers about a mental health issue remains entirely with the patient. There is a greater potential for a more supportive working environment (105, 183, 184). Supervisor and colleague support have been identified as important factors in predicting return to work among patients with mental disorders (105, 183, 184).
Factors that might influence a worker’s decision to disclose their mental health disorder include: receiving advice from a trusted person (e.g., a physician, a colleague, or a personal contact), managerial changes (e.g., new policy, the manager begins talking about mental health issues, or the manager is replaced), and experiences of colleagues (seeing others have positive response among others at work) (185, 186).
Clinicians must be aware of the type and quality of rehabilitation services as an important factor in promoting return to work (37). A study of two vocational approaches found that the most important factors predicting return to work were: feelings of hope and self-esteem/efficacy among patients, positive attitudes and behaviors among professionals (e.g., genuine interest, engagement, and support), and integration of both health and vocational services in return to work programs (187). Meta-analyzes and RCTs show that interventions by occupational health services (generally problem-solving treatment or CBT) can reduce the number of sick days compared to usual care among patients with work-related mental disorders (187). However, these interventions did not consistently improve symptoms of mental disorders, underscoring the need to simultaneously target both return to work and improvement of symptoms with an integrated approach.
As discussed in Section 1, stigma regarding mental health disorders continues to exist in the workplace. In this case, there are a number of things to consider in the disclosure decision (1): who to disclose to (2), timing (3), message content, and (4) communication style (188). In workplaces in which stigma exists, patients may have concerns around perceived or actual negative effects on career opportunities, or non-supportive environments (185, 186). As a clinician, be prepared to challenge and help the patient to work through possible distortions associated with mental health disorders such as feelings of persecution, personalization, and “catastrophizing.” Ultimately, self-stigmatization may be a greater barrier to accessing the needed support to achieve a successful return to work. However, after these discussions, clinicians should be accepting of the patient’s perceptions of their individual workplace and support their decision.
Clinicians should also be aware of the potential impact of stigma in the workplace on patient recovery from a work-related mental disorder, particularly MDD. Stigmatizing attitudes in employers, refusal to implement accommodations, as well as pressure toward productivity and performance, have been documented as negatively influencing the return to work of employees with depression (189, 190).
A systematic review of 16 studies found that anti-stigma interventions at the workplace can improve employee knowledge and supportive behaviors toward people with mental disorders (191). Workplace awareness and stigma reduction programs have also been shown to encourage employees to seek treatment for mental health disorders (192).
In Canada, educational workplace initiatives such as The Working Mind program developed by the Mental Health Commission of Canada are effective in reducing stigma and increasing resilience and coping abilities, across a variety of settings (193), and benefits were maintained at a 3-month follow-up (194). These workplace programs include strategies to reduce stigma, improve awareness of the symptoms of mental disorders, promote coping skills, and provide information about workplace policies and practices to help employees who experience problems (193).
As a part of the management of work-related depression clinicians must collaborate with the insurance provider with regular and updated information. The amount of required documentation of the patient’s disease progress, limitations, restrictions, prognosis, and time to return to work can be overwhelming and frustrating to clinicians as they navigate through the disability process. However, knowledge on the medical note, assessing short and long-term disability, and workplace accommodations can help alleviate the clinician’s burden.
In completing the medical note (sick note), clinicians should be aware that the Canadian Medical Association (CMA) policy position is that sick notes are an unnecessary burden for clinicians and that employers should be restricted from requiring an employee to provide a sick note for short leaves of absence due to personal illness, injury, or medical emergency (195). However, whether employers can require clinicians’ confirmation of the employee’s inability to go to work varies widely. Some provinces have legislation pending addressing the issue of sick notes and some individual employers have introduced policies abandoning sick notes for short-term absences. Reporting to the Workers’ Compensation Boards in Canada may be necessary.
As described in section 1, sustained unemployment has many negative consequences. For individuals in jobs with a safety-sensitive component (e.g., emergency services, heavy equipment operators, pilots, transportation workers), return to work assessments are more comprehensive and focused on limiting risk. As a guiding principle in fitness for duty assessments, public safety may trump the individual’s right to work. The policy of the CMA states: “The treating physician must be aware of the risks to the patient, his or her coworkers or the public that could arise from the patient’s condition or drug therapy. If the patient’s medical condition and the nature of the work performed are likely to endanger the safety of others significantly, the physician must put the public interest before that of the patient/employee” (109).
In order to return to safety-sensitive work after a period of illness the worker must demonstrate normal or adequate capacity to reliably perform and respond to safety-sensitive demands. For example, as described in the Canadian railway medical guides (196), “The individual’s bipolar I disorder has been in remission for a continuous period of 1 year during which the individual has been maintained on a stable dose of medication.” In essence, there must be no imminent risk of relapse of the mental health disorder.
Finally, if a medical code is requested, provide ICD-11 or DMS-5 codes, rather than non-descript terms such as “mental health” or “stress.” Consider the sick note as a medical intervention with associated clinical benefits and risks.
Clinician should facilitate setting up work accommodations to help address functional limitations in patients with mental disorders, and improve their ability to successfully complete work-related tasks (Table 16) (30). Occupational health and human resources are the first points of contact when making accommodation requests and submitting relevant medical forms. They can ensure that any restrictions and limitations are communicated to the manager, without conveying diagnosis or other sensitive medical information, so that appropriate accommodation can be implemented and monitored. Using booklets such as “Supporting Employee Success”3 can be helpful in understanding the process (180).

Table 16. Types of workplace accommodations to address functional limitations in patients with mental disorders (30).
A systematic review of 15 studies found that work accommodations reduced limitations in the work place, improved length of job tenure, and reduced the severity of some mental disorders (30). Work accommodations have been shown to increase job tenure by between 7 to 24 months compared to individuals receiving no accommodations (197, 198). A study of 715 Canadian employees with a current mental disorder found that receiving needed work accommodations was associated with a 25% lower risk of having a mood/anxiety disorder during the 1-year follow-up (32). Programs such as job coaching are associated with minimal costs for both start-up and maintenance, and employee assistance programs have minimal direct and indirect costs (30, 199).
Failing to disclose a workplace-related mental disorder can limit access to accommodations (30, 198, 200). It is important to educate patients on the importance and benefits of workplace accommodations, and patients may need to talk to their employer about specific accommodations that could be helpful (Table 16).
Assessing accommodations is a collaborative effort between the clinician, patient, and workplace. Clinicians should obtain consent from the patient prior to communicating with other stakeholders to better understand job description and role, to help determine possible accommodations such as reduced work hours or workload, re-evaluate job responsibilities, or a possible transfer to a new role. Accommodation can be temporary or permanent in nature and should be re-evaluated periodically to monitor and evaluate treatment effects on patient outcomes.
Furthermore, the Work Accommodation and Natural Support Scale (WANSS) has been developed and validated for people with mental illness returning to work (200). Two versions are available for implementing accommodations in the workplace, which consider the needs for employees and the feasibility for managers/supervisors (201–203). The tools described in Table 3 can also be useful to monitor the effects of MDD on functioning and work productivity, and may be helpful when assessing the need for workplace accommodations.
If a patient is unable to return to work after the sick leave, the clinician must assess if the patient can return to work with or without accommodation or be eligible for disability. Short-term disability refers to a limited period of time that qualifies a person for benefits. Depending on the insurance provider the disability benefits and their definition of short-term may vary. In Canada, most short-term disability benefits are between 3 and 6 months before transitioning into long-term disability.
Charts to track recovery can also be very helpful, such as those in the booklet “Supporting Employee Success,” or those published in the “Global Business and Economic Roundtable on Mental Health”4 (1). These charts can help clinicians track the patient’s symptoms and functioning, and their ability to perform job duties, and can be useful when completing insurance forms. It should be noted that a decrease in symptoms may not necessarily be accompanied by an increase in work functioning.
Clinicians should be aware of a number of patient, treatment, and workplace factors that may adversely affect the management of work-related MDD (Table 17) (37). These data were identified in a systematic review of studies assessing factors that predict return to work in patients with mental disorders conducted for the Australian guidelines (37). The review identified primarily observational, cohort studies, but included over 300,000 patients, and the findings were very consistent. Patient-related factors include high stress levels unrelated to work, poor treatment adherence, and poor attitudes toward returning to work (Table 17) (37). Poor health prior to sick leave, duration and severity of the mental disorder, physical injury, and poor health behaviors (e.g., smoking, substance use, over or under weight) should also be considered in patients having trouble returning to work. Finally, factors in the work environment such as harassment, stress, and poor communication play a role (see Section 3) (16, 37, 70, 71, 105). Furthermore, there are gaps in evidence such as the relative lack of data on marginalized groups and low-wage workers, which will impact recovery and return to work.
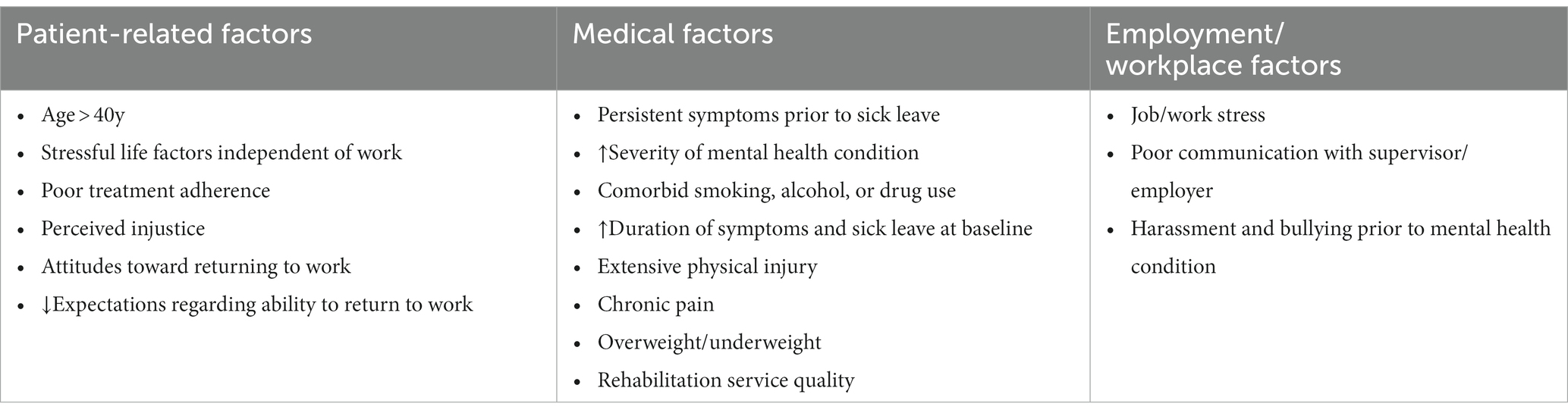
Table 17. Factors that might impair the management of workplace-related MDD (37).
In other systematic reviews, the most important predictive factors for sickness absence among workers with a mental disorder were previous mental disorders, greater symptom severity, previous absenteeism, comorbidity, high job demands, low job control, high job strain, female gender, lower educational level, smoking, and low perceived general health (204, 205). Factors predicting return to work included perceived supervisor- and colleague-support, work accommodations, positive attitudes, self-efficacy, young age, and higher education levels (184, 205, 206). In addition, delay in initiation of antidepressant therapy after diagnosis of MDD has been associated with longer duration of sick leave, including a 6-fold higher risk of having more than 30 sick days (207).
In addition, clinicians should be aware that low social support is an independent predictor of poorer mental health and lower work ability compared to high social support (51–53). In addition, supervisor, colleague, and non-work-related social support have an impact on workplace bullying, mental distress, and sickness absence (183). Physicians should recognize the importance of identifying people who have limited access to social support and refer them to advocacy or other groups.
Canadian employers have a legal obligation to maintain a physically and psychologically healthy and safe work environment (208). Although some patients may be aware of their rights, it is useful for clinicians to remind patients that employers cannot discriminate based on the presence of any illness, including addictions, and that there is a legal right to accommodation in Canada (16, 208, 209). In fact, the Canadian Labor Code states that “no employer shall dismiss, suspend, lay off, demote or discipline an employee because of absence from work due to work-related illness or injury” (209). While Canadian labor law is clear regarding a worker’s right to appropriate accommodation, it is not incumbent upon the employer to solicit information from the employee as to their specific needs (See Section 4 for a discussion of workplace accommodations).
Employers have a duty to inquire when they are concerned about health-related impairment. They should recommend the worker seek help but ultimately the onus is on the worker to do so. In some cases, workers may need legal assistance to exercise their rights.
It is the responsibility of the employee to inform their employer of their need for accommodation, and to participate in finding solutions. Workers (patients) need to be flexible if their employer suggests alternative solutions that may work better for the employer while still meeting the employee’s needs. If a worker is reluctant to disclose their need for accommodations, they may need help identifying someone at work who they trust and who is in a position to give work-related advice. This work ally can help the employee in determining how much to disclose, what accommodations they can ask for, and how to ask for them. When the worker decides to disclose their need for accommodations, it is important that identifying and implementing workplace accommodations be done collaboratively between employer and employee (210), and be reviewed over time depending on changes in the course of the worker’s condition. Most accommodation is temporary but may become permanent if further improvement is not expected with the worker’s condition.
Using booklets such as “Supporting Employee Success” (see text footnote 3) can be helpful in understanding the process (180). Charts to track recovery can also be very helpful, such as those in the booklet.
Identifying relevant programs and navigating complex forms from federal or provincial government agencies can be challenging in the best of circumstances and seemingly insurmountable for patients with work-related mental disorders.
The resource lists provided in Tables 18–20 can be useful resources for clinicians to discuss with their patients. Table 18 provides resources to help patients better understand their condition and identify support services. Table 19 lists useful resources for those needing help communicating with their supervisor, the human resources department, or work colleagues about their mental health issues. Finally, useful websites for disability or benefit-related information are provided in Table 20.
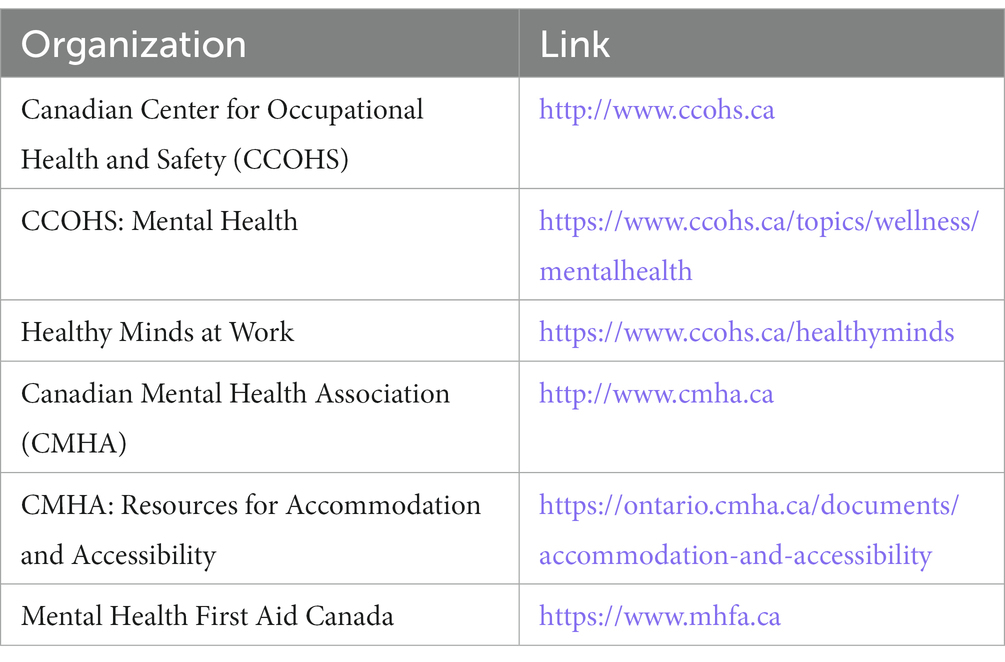
Table 18. Resources for patients on mental health disorders and social support programs.
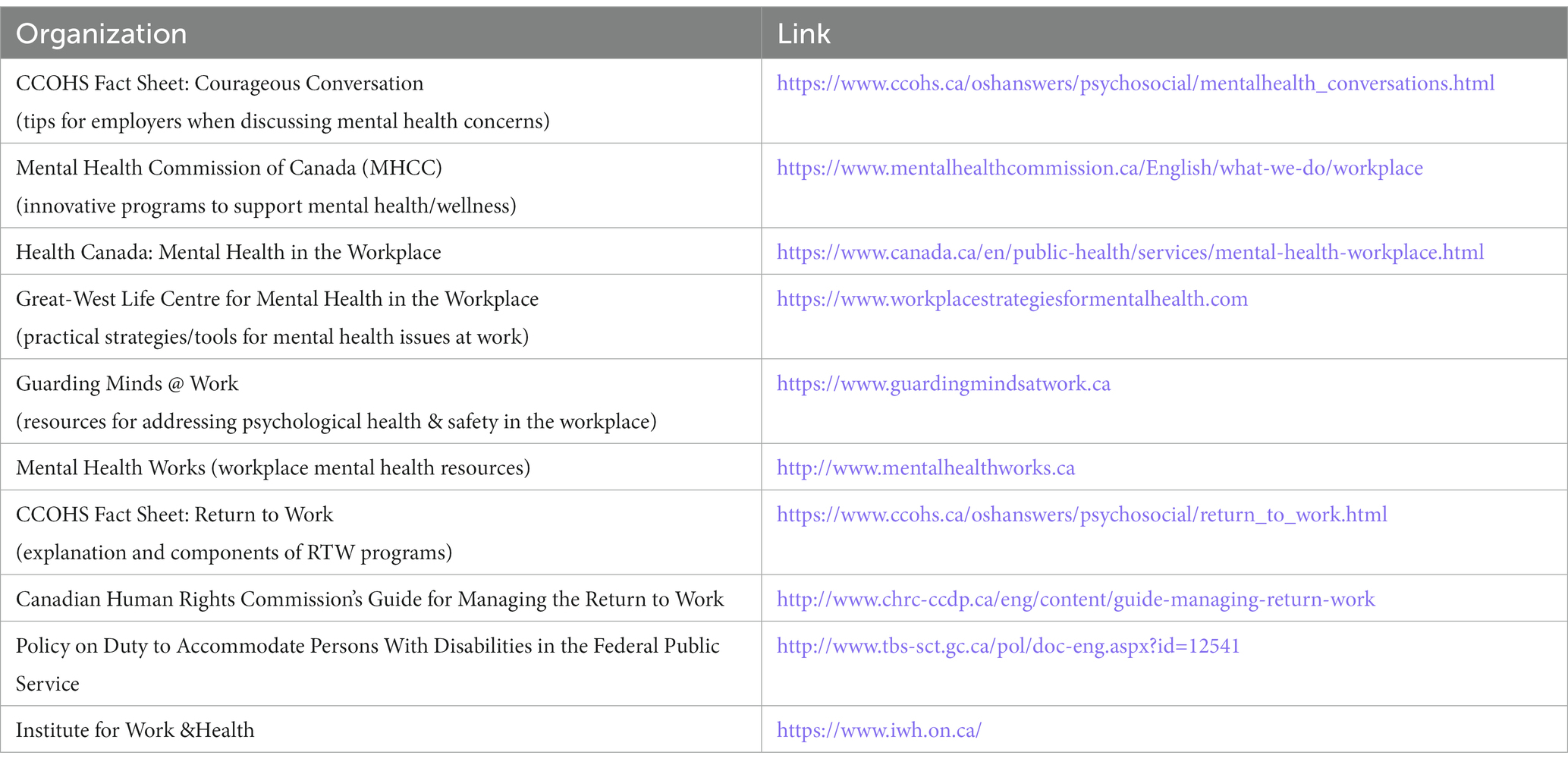
Table 19. Resources for patients on communicating with their workplace.
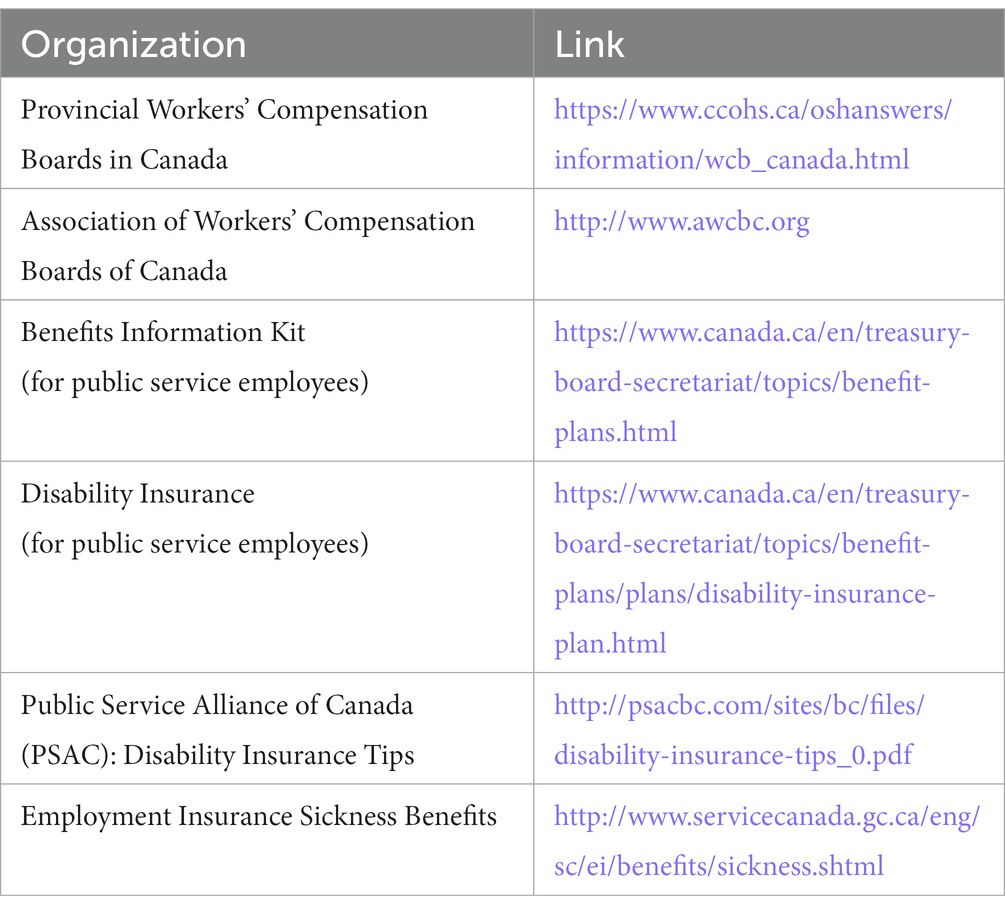
Table 20. Resources for patients on disability and benefit-related programs.
The assessment and treatment of work-related MDD is a complex process involving patients, clinicians, employers, occupational health, and disability providers. Although major strides have been achieved in this area, challenges remain due in a large part to clinician and patient mistrust of the disability process, limited knowledge awareness, poor communication, and a lack of coordinated and collaborative approaches to return to work or to improve work productivity.
From a clinician perspective, a consensus and GRADE level evidence-based standards of care for the assessment and management of work-related MDD are lacking. Future coordinated research with patients, employers, and researchers, hopefully, will provide much-needed guidance on the appropriate screening tools for the diagnosis of work-related MDD, and functioning instruments to assess more precisely abilities, limitations, and restrictions. Research that provides more clarity and precision on the timelines that are optimal to return to work, duration of the sick note, and the utility of time off work in achieving better outcomes such as functioning or return to work is lacking.
The extant literature regarding antidepressants to treat work-related MDD does not provide any clear choices for clinicians. Although challenging, future medication research around the treatment of work-related MDD must assess workplace function as a primary outcome measure and randomize workers. Research incorporating medications, specific and targeted psychotherapies, workplace interventions, and lifestyle approaches in single or multiple interventions is crucial to personalize the most effective treatment.
Finally, starting in medical school, residency and extending through the years in clinical practice, education should focus on the prevalence and impact of mental health disorders in the workplace. More specifically, this document intends to provide practical recommendations and solutions to a complex clinical problem in the absence of adequate research that is needed to provide confident recommendations. However, the committee hopes that this document is an initial step in establishing a future national standard, with GRADE-like evidence and recommendations to help clinicians manage patients who experience work-related MDD.
PC drafted the initial manuscript. All authors critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of the work ensuring integrity and accuracy.
This study received funding via arms-length grants to the Workplace Mental Health Network from Allergan Inc., Lundbeck Canada Inc., Janssen Inc., Otsuka Canada Pharmaceutical Inc. and Telus Mobility. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
The authors would like to thank the sponsors for their generous support of the development of this paper. The group would like to thank the following people for their contributions: Michael Hill [MultiDimensional Healthcare (MDH); administrative and technical support], Pauline Lavigne and Steven Portelance (unaffiliated; editorial assistance) who were supported by the Workplace Mental Health Network. They would also like to thank Chris Patterson, MD from the University of British Columbia and Integra Medical Consulting, in Vancouver, BC, Canada for their valuable contributions to the manuscript.
PC: Support for the present manuscript from Abbvie, Janssen, Lundbeck, Otsuka, Takeda, and Telus; and consulting fees and payment or honoraria from Abbvie, Elvium, Janssen, Lundbeck, Otsuka, and Takeda. AB: Consulting fees from RBC Insurance, WSIB (Ontario), and the Liquor Control Board of Ontario (LCBO); honoraria for speaking engagement from Osgoode School of Law; payment for expert testimony from the Canadian Medical Malpractice Agency; participation on a data safety monitoring board or advisory board for Lundbeck; and an unpaid leadership or fiduciary role with the Cunningham Society. SB: Consulting fees from Abbvie and Otsuka; payment for lectures or educational events from Janssen-Ortho, Lundbeck, Takeda, Otsuka, and Abbvie; travel support for meeting attendance from Otsuka; and board membership for the Saskatchewan chapter of the Canadian Psychiatric Association. GA: Consulting fees from Abbvie, Allergan, Amgen, Astellas Pharma, AstraZeneca, CCRN, CCPDHM/CHRC, Esai, Galderma, Janssen, Lundbeck, MD Briefcase, MedPlan, Novo Nordisk, Otsuka, Purdue, Takeda, The Academy, Valeant, and Novartis; payment or honoraria for speakers bureaus from Elvium, Sunovion, Esai, Janssen, Takeda, Lundbeck, Valeant, Allergan, Otsuka; and board membership (volunteer) for the Canadian ADHD Resource Alliance (CADDRA). MC: Institutional research grants from the Canadian Institutes of Health Research (CIHR), Social Sciences and Humanities Research Council of Canada (SSHRC), Fonds de recherche du Québec (FRQSC), and funding of a research chair position at the Institut Universitaire en Santé Mentale de Montréal (IUSMM); payment or honoraria from IGF Québec, Les Affaires, Canadian Pension and Benefits Institute (CPBI-ICRA), Swiss Society of Social Psychiatry, University of Montréal, Colloque Insertion Vaud 2022, and AMPQ. DD: Grants or contracts from SSHRC; book royalties from Guilford Press, American Psychological Association, Elsevier, and Pearson; consulting fees from Otsuka; payment or honoraria for presentation from McGill University; board membership for Mental Health Research Canada and the International Association of Applied Psychology; editorial board membership for Clinical Psychology: Science and Practice, Canadian Psychology, Cognitive Therapy and Research, and Canadian Journal of Behavioral Science. JeH: Consulting fees from Otsuka, HLS, Amgen, Pfizer, Eisai, Eli-Lilly, Janssen, Lundbeck, Novo-Nordisk, Valeo, Abbvie, Elvium, and Bausch; and payment or honoraria for speakers bureaus from Pfizer, Amgen, Abbvie, GSK, Bayer, Boehringer, Eli-Lilly, Purdue, Bausch, Allergan, AstraZeneca, Novartis, Lundbeck, Novo-Nordisk, Janssen, Eisai, HLS, Otsuka, Sunovion, MDBriefcase, Liv, MedPlan, Master Clinician Alliance, Academy, Bridge, PeerVoice, Seacourses, Thrombosis Canada, Meducom, Antibody, CHRC, CTC, STA, CCRN, CPD Network, Telus Health, EOCI, AgenceUnik, and Pri-Med. JoH: Employment with Metis Cognition Ltd. Royalties or licenses from Metis Cognition Ltd. for BASIC; consulting fees (paid to Metis Cognition Ltd) from Actinogen, Alzecure, ADvantage, AstraZeneca, Athira Therapeutics, Axoltis, Axon Neuroscience, Bial Biotech, Biogen Idec, Boehringer Ingelheim, Brands2Life, Cerecin, Cognition Therapeutics, Compass Pathways, Corlieve, Curasen, EcoR1, Eisai, EIP Pharma, Eli Lilly, EQT Life, Games for Health EU, Heptares, Ki-Elements, Lundbeck, Lysosome Therapeutics, MyCognition, Neurotrack, NHS, Novartis, Novo Nordisk, Nutricia, Recognify, Remynd, Roche, Rodin Therapeutics, Signant Health, Syndesi Therapeutics, Takeda, Vivoryon Therapeutics, Winterlight Labs, Stoke Therapeutics, Alto Pharma; payment or honoraria (paid to Metis Cognition Ltd) for presentations from Roche; travel support for meeting attendance (paid to Metis Cognition Ltd) from Roche and Biogen; patent for MyCognition; participation on a data safety monitoring board or advisory board for Esai; and stock or stock options from Neurotrack. MK: Grants or contracts from Abbvie, AstraZeneca, Biotics, Canopy, Eisai, Janssen, Lundbeck, Otsuka, Shire, Takeda, and Biohaven; consulting fees from Janssen, Eli Lily, Novartis, Merck, Otsuka, Pfizer, Purdue, Sante Cannabis, Sunovion, Takeda, and Tilray; payment or honoraria from Abbvie, Biron, Alefia Cannabis, Allergan, Bausch Health, Canopy, Eisai, Elvium, Empower Cannabis, Lundbeck; participation on a data safety monitoring board or advisory board for Abbvie, Lundbeck, Biron, Elsai, and Ironshore; board membership for ASPARD; and receipt of equipment, materials, drugs, medical writing, gifts, or other services from Biron. RM: Grants from CIHR/GACD/National Natural Science Foundation of China (NSFC) and the Milken Institute; consulting fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, Abbvie, and Atai Life Sciences; and is CEO of Braxia Scientific Corp. YL: Institutional grant support from MITACS and Chokka Center for Integrative Health. KN: Institutional grants from the Dutch Social Security Agency, Netherlands Organization for Health Research and Development, and the Dutch Ministry of Education. CD: Consulting fees from Modern Health. Funding Statement: This study received funding via arms-length grants to the Workplace Mental Health Network from Allergan Inc., Lundbeck Canada Inc., Janssen Inc., Otsuka Canada Pharmaceutical Inc. and Telus Mobility. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1207653/full#supplementary-material
1. ^www.pubmed.ncbi.nlm.nih.gov
3. ^Available on The Institute for Work and Health website https://aced.iwh.on.ca/
4. ^Available at http://www.mentalhealthroundtable.ca
1. Wilkerson, B. Global business and economic roundtable on addiction and mental health. An agenda for progress global business and economic roundtable on mental health. 2006 business and economic plan for mental health and productivity. (2006). Available at: http://www.mentalhealthroundtable.ca/20060328/2006BusinessPlan.pdf (Accessed April 1, 2021).
2. Mental Health Commission of Canada. Issue brief: Workplace mental health. (2016). Available at: https://www.mentalhealthcommission.ca/sites/default/files/2017-01/Issue_Brief_workplace_mental_health_eng.pdf (Accessed Apr 3, 2020).
3. Mental Health Commission of Canada. Making the case for investing in mental health in Canada. (2013). Available at: https://www.mentalhealthcommission.ca/sites/default/files/2016-06/Investing_in_Mental_Health_FINAL_Version_ENG.pdf (Accessed May 14, 2020).
4. Mental Health Commission of Canada. Strengthening the case for investing in Canada’s mental health system: Economic considerations. (2017). Available at: https://www.mentalhealthcommission.ca/sites/default/files/2017-03/case_for_investment_eng.pdf (Accessed May 14, 2020).
5. Lundberg, J, Cars, T, Loov, SA, Soderling, J, Sundstrom, J, Tiihonen, J, et al. Association of treatment-resistant depression with patient outcomes and health care resource utilization in a population-wide study. JAMA Psychiat. (2023) 80:167–75. doi: 10.1001/jamapsychiatry.2022.3860
6. Lundberg, J, Cars, T, Loov, SA, Soderling, J, Tiihonen, J, Leval, A, et al. Clinical and societal burden of incident major depressive disorder: a population-wide cohort study in Stockholm. Acta Psychiatr Scand. (2022) 146:51–63. doi: 10.1111/acps.13414
7. Jain, S, Gupta, S, Li, VW, Suthoff, E, and Arnaud, A. Humanistic and economic burden associated with depression in the United States: a cross-sectional survey analysis. BMC Psychiatry. (2022) 22:542. doi: 10.1186/s12888-022-04165-x
8. Rojanasarot, S, Bhattacharyya, SK, and Edwards, N. Productivity loss and productivity loss costs to United States employers due to priority conditions: a systematic review. J Med Econ. (2023) 26:262–70. doi: 10.1080/13696998.2023.2172282
9. McIntyre, RS, and Lee, Y. Preventing suicide in the context of the COVID-19 pandemic. World Psychiatry. (2020) 19:250–1. doi: 10.1002/wps.20767
10. McIntyre, RS, and Lee, Y. Projected increases in suicide in Canada as a consequence of COVID-19. Psychiatry Res. (2020) 290:113104. doi: 10.1016/j.psychres.2020.113104
11. Czeisler, ME, Lane, RI, Petrosky, E, Wiley, JF, Christensen, A, Njai, R, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:1049–57. doi: 10.15585/mmwr.mm6932a1
12. Ettman, CK, Abdalla, SM, Cohen, GH, Sampson, L, Vivier, PM, and Galea, S. Prevalence of depression symptoms in us adults before and during the COVID-19 pandemic. JAMA Netw Open. (2020) 3:e2019686. doi: 10.1001/jamanetworkopen.2020.19686
13. Dozois, D, Mental Health Research Canada. Anxiety and depression in Canada during the COVID-19 pandemic: a national survey. Can Psychol. (2021) 62:136–42. doi: 10.1037/cap0000251
14. Pathirathna, ML, Nandasena, H, Atapattu, A, and Weerasekara, I. Impact of the COVID-19 pandemic on suicidal attempts and death rates: a systematic review. BMC Psychiatry. (2022) 22:506. doi: 10.1186/s12888-022-04158-w
15. College of Family Physicians of Canada. A new vision for Canada: Family Practice—the Patient’s Medical Home 2019. (2019). https://patientsmedicalhome.ca/vision/ (Accessed February 17, 2022).
16. National Standard of Canada. CAN/CSA-Z1003-13/BNQ 9700–803/2013-Psychological health and safety in the workplace: Prevention, promotion, and guidance to staged implementation. (2013). Available at: https://www.csagroup.org/article/cancsa-z1003-13-bnq-9700-803-2013-r2018/ (Accessed Apr 3, 2020).
17. World Health Organization. Guidelines on mental health at work. (2022). Available at: https://www.who.int/publications/i/item/9789240053052 (Accessed March 30, 2023).
18. Bender, A. Restoring function in MDD: balancing efficacy and tolerability to optimally manage major depressive disorder. Can J Diagnosis. (2011) 28:13–21.
19. Bender, A. Psychiatric disability requires careful clinical management. Can Psychiatry Aujourdhui. (2008) 4:9.
20. Rizvi, SJ, Cyriac, A, Grima, E, Tan, M, Lin, P, Gallaugher, LA, et al. Depression and employment status in primary and tertiary care settings. Can J Psychiatr. (2015) 60:14–22. doi: 10.1177/070674371506000105
21. Sutherland, G, and Stonebridge, C. Healthy brains at work: Estimating the impact of workplace mental health benefits and programs. The Conference Board of Canada: Ottawa, ON (2016).
22. Evans-Lacko, S, and Knapp, M. Global patterns of workplace productivity for people with depression: absenteeism and presenteeism costs across eight diverse countries. Soc Psychiatry Psychiatr Epidemiol. (2016) 51:1525–37. doi: 10.1007/s00127-016-1278-4
23. Hong, JP, Lee, CH, Lee, YH, Escorpizo, R, Chiang, YC, and Liou, TH. Functional status and return to work in people with major depression: a 3-year national follow-up study. Soc Psychiatry Psychiatr Epidemiol. (2022) 57:1179–88. doi: 10.1007/s00127-022-02240-y
24. Pedersen, J, Framke, E, Thorsen, SV, Sorensen, K, Andersen, MF, Rugulies, R, et al. The linkage of depressive and anxiety disorders with the expected labor market affiliation (ELMA): a longitudinal multi-state study of Danish employees. Int Arch Occup Environ Health. (2023) 96:93–104. doi: 10.1007/s00420-022-01906-z
25. Australasian Faculty of Occupational and Environmental Medicine. Australasian consensus statement on the health benefits of work. (2015). Available at: https://www.racp.edu.au/docs/default-source/advocacy-library/realising-the-health-benefits-of-work.pdf (Accessed April 14, 2020).
26. Waddell, G, and Burton, A. Is work, good for your health and wellbeing? (2006). Available at: https://cardinal-management.co.uk/wp-content/uploads/2016/04/Burton-Waddell-is-work-good-for-you.pdf (Accessed June 12, 2020).
27. Armbrecht, E, Shah, A, Schepman, P, Shah, R, Pappadopulos, E, Chambers, R, et al. Economic and humanistic burden associated with noncommunicable diseases among adults with depression and anxiety in the United States. J Med Econ. (2020) 23:1032–42. doi: 10.1080/13696998.2020.1776297
28. Banerjee, D, Kosagisharaf, JR, and Sathyanarayana Rao, TS. ‘The dual pandemic’ of suicide and COVID-19: a biopsychosocial narrative of risks and prevention. Psychiatry Res. (2021) 295:113577. doi: 10.1016/j.psychres.2020.113577
29. Chisholm, D, Sweeny, K, Sheehan, P, Rasmussen, B, Smit, F, Cuijpers, P, et al. Scaling-up treatment of depression and anxiety: a global return on investment analysis. Lancet Psychiatry. (2016) 3:415–24. doi: 10.1016/S2215-0366(16)30024-4
30. Zafar, N, Rotenberg, M, and Rudnick, A. A systematic review of work accommodations for people with mental disorders. Work. (2019) 64:461–75. doi: 10.3233/WOR-193008
31. Wang, J, Patten, S, Currie, S, Sareen, J, and Schmitz, N. Perceived needs for and use of workplace accommodations by individuals with a depressive and/or anxiety disorder. J Occup Environ Med. (2011) 53:1268–72. doi: 10.1097/JOM.0b013e31822cfd82
32. Bolo, C, Sareen, J, Patten, S, Schmitz, N, Currie, S, and Wang, J. Receiving workplace mental health accommodations and the outcome of mental disorders in employees with a depressive and/or anxiety disorder. J Occup Environ Med. (2013) 55:1293–9. doi: 10.1097/JOM.0b013e31829fd065
33. Lachaine, J, Beauchemin, C, Bibeau, J, Patenaude, J, Chokka, P, Proulx, J, et al. Canadian economic impact of improved workplace productivity in patients with major depressive disorder treated with vortioxetine. CNS Spectr. (2019) 25:372–9. doi: 10.1017/S1092852919000853
34. Dewa, CS. Worker attitudes towards mental health problems and disclosure. Int J Occup Environ Med. (2014) 5:175–86.
35. Yoshimura, Y, Bakolis, I, and Henderson, C. Psychiatric diagnosis and other predictors of experienced and anticipated workplace discrimination and concealment of mental illness among mental health service users in England. Soc Psychiatry Psychiatr Epidemiol. (2018) 53:1099–109. doi: 10.1007/s00127-018-1561-7
36. Bertilsson, M, Love, J, Martinsson, J, Wangnerud, L, and Hensing, G. Association of stigmatizing attitudes with people’s opinion of depression as a valid reason for sickness absence: a Swedish vignette study. Work. (2022) 73:495–504. doi: 10.3233/WOR-205181
37. Mazza, D, Brijnath, B, and Chakraborty, S, The Guideline Development Group. Clinical guideline for the diagnosis and management of work-related mental health conditions in general practice. Melbourne, Australia: Monash University (2019).
38. Consortium ANS. Appraisal of guidelines for Research & Evaluation II (AGREE II) instrument. (2017). Available at: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf (Accessed December 1, 2022).
39. Mazza, D, Brijnath, B, Chakraborty, S, Rasekaba, TR, and Clements, JC, The Guideline Development Group. Technical report for the clinical practice guideline for the diagnosis and management of work-related mental health conditions in general practice. Melbourne, Australia: Monash University (2019).
40. Mazza, D, Brijnath, B, and Chakraborty, S, The Guideline Development Group. Administrative report for clinical guideline for the diagnosis and management of work-related mental health conditions in general practice. Melbourne, Australia: Monash University (2019).
41. Nieuwenhuijsen, K, Verbeek, JH, Neumeyer-Gromen, A, Verhoeven, AC, Bultmann, U, and Faber, B. Interventions to improve return to work in depressed people. Cochrane Database Syst Rev. (2020) 10:CD006237. doi: 10.1002/14651858.CD006237.pub4
42. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5). Washington, DC: American Psychiatric Association (2013).
43. Olariu, E, Forero, CG, Castro-Rodriguez, JI, Rodrigo-Calvo, MT, Alvarez, P, Martin-Lopez, LM, et al. Detection of anxiety disorders in primary care: a meta-analysis of assisted and unassisted diagnoses. Depress Anxiety. (2015) 32:471–84. doi: 10.1002/da.22360
44. Mitchell, AJ, Vaze, A, and Rao, S. Clinical diagnosis of depression in primary care: a meta-analysis. Lancet. (2009) 374:609–19. doi: 10.1016/S0140-6736(09)60879-5
45. Hirschfeld, RM, Williams, JB, Spitzer, RL, Calabrese, JR, Flynn, L, Keck, PE, et al. Development and validation of a screening instrument for bipolar spectrum disorder: the mood disorder questionnaire. Am J Psychiatry. (2000) 157:1873–5. doi: 10.1176/appi.ajp.157.11.1873
46. Kessler, RC, Adler, L, Ames, M, Demler, O, Faraone, S, Hiripi, E, et al. The World Health Organization adult ADHD self-report scale (ASRS): a short screening scale for use in the general population. Psychol Med. (2005) 35:245–56. doi: 10.1017/s0033291704002892
47. Babor, T, Higgins-Biddle, J, Saunders, J, and Monteiro, M. The alcohol use disorders identification test: guidelines for use in primary care. Geneva: World Health Organization (2001).
48. Liu, Y, Hankey, J, Cao, B, and Chokka, P. Screening for major depressive disorder in a tertiary mental health Centre using EarlyDetect: a machine learning-based pilot study. J Affect Dis Rep. (2021) 3:100062. doi: 10.1016/j.jadr.2020.100062
49. Liu, YS, Chokka, S, Cao, B, and Chokka, PR. Screening for bipolar disorder in a tertiary mental health Centre using EarlyDetect: a machine learning-based pilot study. J Affect Dis Rep. (2021) 6:100215. doi: 10.1016/j.jadr.2021.100215
50. Liu, YS, Cao, B, and Chokka, PR. Screening for aulthood ADHD and comorbidities in a tertiary mental health center using earlydetect: a machine learning-based pilot study. J Atten Disord. (2023) 27:324–31. doi: 10.1177/10870547221136228
51. Cambridge, OR, Knight, MJ, Mills, N, and Baune, BT. The clinical relationship between cognitive impairment and psychosocial functioning in major depressive disorder: a systematic review. Psychiatry Res. (2018) 269:157–71. doi: 10.1016/j.psychres.2018.08.033
52. Haro, JM, Hammer-Helmich, L, Saragoussi, D, Ettrup, A, and Larsen, KG. Patient-reported depression severity and cognitive symptoms as determinants of functioning in patients with major depressive disorder: a secondary analysis of the 2-year prospective PERFORM study. Neuropsychiatr Dis Treat. (2019) 15:2313–23. doi: 10.2147/NDT.S206825
53. Cha, DS, Carmona, NE, Subramaniapillai, M, Mansur, RB, Lee, Y, Hon Lee, J, et al. Cognitive impairment as measured by the THINC-integrated tool (THINC-it): association with psychosocial function in major depressive disorder. J Affect Disord. (2017) 222:14–20. doi: 10.1016/j.jad.2017.06.036
54. Woo, YS, Rosenblat, JD, Kakar, R, Bahk, WM, and McIntyre, RS. Cognitive deficits as a mediator of poor occupational function in remitted major depressive disorder patients. Clin Psychopharmacol Neurosci. (2016) 14:1–16. doi: 10.9758/cpn.2016.14.1.1
55. McIntyre, RS, Soczynska, JZ, Woldeyohannes, HO, Alsuwaidan, MT, Cha, DS, Carvalho, AF, et al. The impact of cognitive impairment on perceived workforce performance: results from the international mood disorders collaborative project. Compr Psychiatry. (2015) 56:279–82. doi: 10.1016/j.comppsych.2014.08.051
56. McIntyre, RS, Cha, DS, Soczynska, JK, Woldeyohannes, HO, Gallaugher, LA, Kudlow, P, et al. Cognitive deficits and functional outcomes in major depressive disorder: determinants, substrates, and treatment interventions. Depress Anxiety. (2013) 30:515–27. doi: 10.1002/da.22063
57. Watanabe, K, Marumoto, T, Ge, H, Moriguchi, Y, Fujikawa, K, and Fernandez, JL. Association between baseline cognitive symptoms and the subsequent presenteeism and global function in patients with major depressive disorder. J Psychiatr Res. (2022) 154:324–31. doi: 10.1016/j.jpsychires.2022.07.036
58. Chokka, P, Bougie, J, Rampakakis, E, and Proulx, J. Assessment in work productivity and the relationship with cognitive symptoms (AtWoRC): primary analysis from a Canadian open-label study of vortioxetine in patients with major depressive disorder (MDD). CNS Spectr. (2019) 24:338–47. doi: 10.1017/S1092852918000913
59. Lam, RW, Lamy, FX, Danchenko, N, Yarlas, A, White, MK, Rive, B, et al. Psychometric validation of the perceived deficits questionnaire-depression (PDQ-D) instrument in US and UK respondents with major depressive disorder. Neuropsychiatr Dis Treat. (2018) 14:2861–77. doi: 10.2147/NDT.S175188
60. Sullivan, J, Edgley, K, and Dehoux, E. A survey of multiple sclerosis. Part 1. Perceived cognitive problems and compensatory strategy use. Can J Rehabil. (1990) 4:99–105.
61. Harrison, JE, Barry, H, Baune, BT, Best, MW, Bowie, CR, Cha, DS, et al. Stability, reliability, and validity of the THINC-it screening tool for cognitive impairment in depression: a psychometric exploration in healthy volunteers. Int J Methods Psychiatr Res. (2018) 27:e1736. doi: 10.1002/mpr.1736
62. McIntyre, RS, Best, MW, Bowie, CR, Carmona, NE, Cha, DS, Lee, Y, et al. The THINC-integrated tool (THINC-it) screening assessment for cognitive dysfunction: validation in patients with major depressive disorder. J Clin Psychiatry. (2017) 78:873–81. doi: 10.4088/JCP.16m11329
63. Iverson, GL, and Lam, RW. Rapid screening for perceived cognitive impairment in major depressive disorder. Ann Clin Psychiatry. (2013) 25:135–40.
64. Srisurapanont, M, Eurviriyanukul, K, Suttajit, S, and Varnado, P. Internal consistency and concurrent validity of the Montreal cognitive assessment in individuals with major depressive disorder. Psychiatry Res. (2017) 253:333–7. doi: 10.1016/j.psychres.2017.04.014
65. Fava, M, Mahableshwarkar, AR, Jacobson, W, Zhong, W, Keefe, RS, Olsen, CK, et al. What is the overlap between subjective and objective cognitive impairments in MDD? Ann Clin Psychiatry. (2018) 30:176–84.
66. Srisurapanont, M, Suttajit, S, Eurviriyanukul, K, and Varnado, P. Discrepancy between objective and subjective cognition in adults with major depressive disorder. Sci Rep. (2017) 7:3901. doi: 10.1038/s41598-017-04353-w
67. Zlatar, ZZ, Muniz, M, Galasko, D, and Salmon, DP. Subjective cognitive decline correlates with depression symptoms and not with concurrent objective cognition in a clinic-based sample of older adults. J Gerontol B Psychol Sci Soc Sci. (2018) 73:1198–202. doi: 10.1093/geronb/gbw207
68. Chokka, P, Bougie, J, Proulx, J, Tvistholm, AH, and Ettrup, A. Long-term functioning outcomes are predicted by cognitive symptoms in working patients with major depressive disorder treated with vortioxetine: results from the AtWoRC study. CNS Spectr. (2019) 24:616–27. doi: 10.1017/S1092852919000786
69. Safe Work Australia. Work-related mental health disorders profile. (2015). Available at: https://www.safeworkaustralia.gov.au/system/files/documents/1702/work-related-mental-disorders-profile.pdf (Accessed Apr 2, 2020).
70. Theorell, T, Hammarstrom, A, Aronsson, G, Traskman Bendz, L, Grape, T, Hogstedt, C, et al. A systematic review including meta-analysis of work environment and depressive symptoms. BMC Public Health. (2015) 15:738. doi: 10.1186/s12889-015-1954-4
71. Duchaine, CS, Aube, K, Gilbert-Ouimet, M, Vezina, M, Ndjaboue, R, Massamba, V, et al. Psychosocial stressors at work and the risk of sickness absence due to a diagnosed mental disorder: a systematic review and meta-analysis. JAMA Psychiat. (2020) 77:842–51. doi: 10.1001/jamapsychiatry.2020.0322
72. Sheehan, DV, Harnett-Sheehan, K, and Raj, BA. The measurement of disability. Int Clin Psychopharmacol. (1996) 11:89–95. doi: 10.1097/00004850-199606003-00015
73. World Health Organization. WHO Disability Assessment Schedule 2.0 (WHODAS 2.0). (2018). Available at: https://www.who.int/classifications/icf/more_whodas/en/ (Accessed Apr 28, 2020).
74. Christensen, MC, Sluth, LB, and McIntyre, RS. Validation of the University of California san Diego Performance-based skills assessment (UPSA) in major depressive disorder: replication and extension of initial findings. J Affect Disord. (2019) 245:508–16. doi: 10.1016/j.jad.2018.11.034
75. Lerner, D, Amick, BC 3rd, Rogers, WH, Malspeis, S, Bungay, K, and Cynn, D. The work limitations questionnaire. Med Care. (2001) 39:72–85. doi: 10.1097/00005650-200101000-00009
76. Reilly, MC, Zbrozek, AS, and Dukes, EM. The validity and reproducibility of a work productivity and activity impairment instrument. PharmacoEconomics. (1993) 4:353–65. doi: 10.2165/00019053-199304050-00006
77. Bianchi, R, and Schonfeld, IS. The occupational depression inventory: a new tool for clinicians and epidemiologists. J Psychosom Res. (2020) 138:110249. doi: 10.1016/j.jpsychores.2020.110249
78. Bianchi, R, Verkuilen, J, Sowden, JF, and Schonfeld, IS. Towards a new approach to job-related distress: a three-sample study of the occupational depression inventory. Stress Health. (2023) 39:137–53. doi: 10.1002/smi.3177
79. World Health Organization. International Classification of Diseases 11th Revision (ICD-11). (2020). Available at: https://icd.who.int/en (Accessed April 7, 2021).
80. Koutsimani, P, Montgomery, A, and Georganta, K. The relationship between burnout, depression, and anxiety: a systematic review and meta-analysis. Front Psychol (2019), 10:284. doi: 10.3389/fpsyg.2019.00284 30918490
81. Durand-Moreau, QV. Is burn-out finally a disease or not? Occup Environ Med. (2019) 76:938. doi: 10.1136/oemed-2019-106094
82. Ahola, K, Hakanen, J, Perhoniemi, R, and Mutanen, P. Relationship between burnout and depressive symptoms: a study using the person-centred approach. Burn Res. (2014) 1:29–37. doi: 10.1016/j.burn.2014.03.003
83. Bianchi, R, Verkuilen, J, Schonfeld, IS, Hakanen, JJ, Jansson-Fröjmark, M, Manzano-García, G, et al. Is burnout a depressive condition? A 14-sample meta-analytic and bifactor analytic study. Clin Psycholog Sci. (2021) 9:579–97. doi: 10.1177/2167702620979597
84. Zisook, S, Doran, N, Mortali, M, Hoffman, L, Downs, N, Davidson, J, et al. Relationship between burnout and major depressive disorder in health professionals: a HEAR report. J Affect Disord. (2022) 312:259–67. doi: 10.1016/j.jad.2022.06.047
85. Maslach, C, and Leiter, MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry. (2016) 15:103–11. doi: 10.1002/wps.20311
86. Maslach, C, and Jackson, S. The measurement of experienced burnout. J Occupat Behav. (1981) 2:99–113.
87. Maslach, C, Jackson, S, and Leiter, M. The Maslach burnout inventory-test manual. 3rd ed. Palo Alto, CA: Consulting Psychologists Press (1996).
88. Schonfeld, IS, and Bianchi, R. From burnout to occupational depression: recent developments in research on job-related distress and occupational health. Front Public Health. (2021) 9:796401. doi: 10.3389/fpubh.2021.796401
89. Monaro, M, Toncini, A, Ferracuti, S, Tessari, G, Vaccaro, MG, De Fazio, P, et al. The detection of malingering: a new tool to identify made-up depression. Front Psych. (2018) 9:249. doi: 10.3389/fpsyt.2018.00249
90. Heer, JS, and Purcell, T. Factitious disorders and malingering In: RM Walls, RS Hockberger, M Gausche-Hill, TB Erickson, and SR Wilcox, editors. Rosen’s emergency medicine. 7th ed. Philadelphia, PA: Mosby Elsevier (2010). 1458–62.
91. Bass, C, and Wade, DT. Malingering and factitious disorder. Pract Neurol. (2019) 19:96–105. doi: 10.1136/practneurol-2018-001950
92. Bass, C, and Halligan, P. Factitious disorders and malingering: challenges for clinical assessment and management. Lancet. (2014) 383:1422–32. doi: 10.1016/S0140-6736(13)62186-8
94. Cassano, A, and Grattagliano, I. Lying in the medicolegal field: malingering and psychodiagnostic assessment. Clin Ter. (2019) 170:e134–41. doi: 10.7417/CT.2019.2123
95. Tylicki, JL, Gervais, RO, and Ben-Porath, YS. Examination of the MMPI-3 over-reporting scales in a forensic disability sample. Clin Neuropsychol. (2022) 36:1878–901. doi: 10.1080/13854046.2020.1856414
96. Hendriks, SM, Spijker, J, Licht, CM, Hardeveld, F, de Graaf, R, Batelaan, NM, et al. Long-term work disability and absenteeism in anxiety and depressive disorders. J Affect Disord. (2015) 178:121–30. doi: 10.1016/j.jad.2015.03.004
97. Fava, M, Rush, AJ, Alpert, JE, Balasubramani, GK, Wisniewski, SR, Carmin, CN, et al. Difference in treatment outcome in outpatients with anxious versus nonanxious depression: a STAR*D report. Am J Psychiatry. (2008) 165:342–51. doi: 10.1176/appi.ajp.2007.06111868
98. Zhou, Y, Cao, Z, Yang, M, Xi, X, Guo, Y, Fang, M, et al. Comorbid generalized anxiety disorder and its association with quality of life in patients with major depressive disorder. Sci Rep. (2017) 7:40511. doi: 10.1038/srep40511
99. Seo, HJ, Jung, YE, Kim, TS, Kim, JB, Lee, MS, Kim, JM, et al. Distinctive clinical characteristics and suicidal tendencies of patients with anxious depression. J Nerv Ment Dis. (2011) 199:42–8. doi: 10.1097/NMD.0b013e3182043b60
100. Gaspersz, R, Nawijn, L, Lamers, F, and Penninx, B. Patients with anxious depression: overview of prevalence, pathophysiology and impact on course and treatment outcome. Curr Opin Psychiatry. (2018) 31:17–25. doi: 10.1097/YCO.0000000000000376
102. Dai, H, Mei, Z, An, A, and Wu, J. Epidemiology of physical and mental comorbidity in Canada and implications for health-related quality of life, suicidal ideation, and healthcare utilization: a nationwide cross-sectional study. J Affect Disord. (2020) 263:209–15. doi: 10.1016/j.jad.2019.11.146
103. Patten, SB, Williams, JVA, Lavorato, DH, Wang, JL, Jette, N, Sajobi, TT, et al. Patterns of association of chronic medical conditions and major depression. Epidemiol Psychiatr Sci. (2018) 27:42–50. doi: 10.1017/S204579601600072X
104. Fisher, K, Griffith, LE, Gruneir, A, Kanters, D, Markle-Reid, M, and Ploeg, J. Functional limitations in people with multimorbidity and the association with mental health conditions: baseline data from the Canadian longitudinal Study on aging (CLSA). PLoS One. (2021) 16:e0255907. doi: 10.1371/journal.pone.0255907
105. Lau, B, Shiryaeva, O, Ruud, T, and Victor, M. What are they returning to? Psychosocial work environment as a predictor of returning to work among employees in treatment for common mental disorders: a prospective observational pre-post study. PLoS One. (2019) 14:e0215354. doi: 10.1371/journal.pone.0215354
106. World Health Organization. International classification of functioning, disability and health. (2001). Available at: https://www.who.int/classifications/international-classification-of-functioning-disability-and-health (Accessed April 11, 2022).
107. Rondinelli, RD, Genovese, E, and Brigham, CR. Guides to the evaluation of permanent impairment. Chicago, Illinois: American Medical Association (2008).
108. University of Washington. What are some of the functional limitations related to mental illness? (2021). Available at: https://www.washington.edu/doit/what-are-some-functional-limitations-related-mental-illness (Accessed April 11, 2022).
109. Canadian Medical Association. The treating physicians’ role in helping patients return to work after an illness or injury. (2013). Available at: https://policybase.cma.ca/documents/policypdf/PD13-05.pdf (Accessed March 7, 2021).
110. Hieronymus, F, Emilsson, JF, Nilsson, S, and Eriksson, E. Consistent superiority of selective serotonin reuptake inhibitors over placebo in reducing depressed mood in patients with major depression. Mol Psychiatry. (2016) 21:523–30. doi: 10.1038/mp.2015.53
111. Cipriani, A, Furukawa, TA, Salanti, G, Chaimani, A, Atkinson, LZ, Ogawa, Y, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. (2018) 391:1357–66. doi: 10.1016/S0140-6736(17)32802-7
112. Kennedy, SH, Lam, RW, McIntyre, RS, Tourjman, SV, Bhat, V, Blier, P, et al. Canadian network for mood and anxiety treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 3. Pharmacol Treatment Can J Psychiatry. (2016) 61:540–60. doi: 10.1177/0706743716659417
113. Rosenblat, JD, Kakar, R, and McIntyre, RS. The cognitive effects of antidepressants in major depressive disorder: a systematic review and meta-analysis of randomized clinical trials. Int J Neuropsychopharmacol. (2015) 19:19. doi: 10.1093/ijnp/pyv082
114. Lee, Y, Rosenblat, JD, Lee, J, Carmona, NE, Subramaniapillai, M, Shekotikhina, M, et al. Efficacy of antidepressants on measures of workplace functioning in major depressive disorder: a systematic review. J Affect Disord. (2018) 227:406–15. doi: 10.1016/j.jad.2017.11.003
115. Evans, VC, Alamian, G, McLeod, J, Woo, C, Yatham, LN, and Lam, RW. The effects of newer antidepressants on occupational impairment in major depressive disorder: a systematic review and meta-analysis of randomized controlled trials. CNS Drugs. (2016) 30:405–17. doi: 10.1007/s40263-016-0334-7
116. Sheehan, DV, Nakagome, K, Asami, Y, Pappadopulos, EA, and Boucher, M. Restoring function in major depressive disorder: a systematic review. J Affect Disord. (2017) 215:299–313. doi: 10.1016/j.jad.2017.02.029
117. Cao, B, Xu, L, Chen, Y, Wang, D, Lee, Y, Rosenblat, JD, et al. Comparative efficacy of pharmacological treatments on measures of self-rated functional outcomes using the Sheehan disability scale in patients with major depressive disorder: a systematic review and network meta-analysis. CNS Spectr. (2021) 2021:1–9. doi: 10.1017/S1092852921000171
118. Kennedy, SH, Avedisova, A, Belaidi, C, Picarel-Blanchot, F, and de Bodinat, C. Sustained efficacy of agomelatine 10 mg, 25 mg, and 25-50 mg on depressive symptoms and functional outcomes in patients with major depressive disorder. A placebo-controlled study over 6 months. Eur Neuropsychopharmacol. (2016) 26:378–89. doi: 10.1016/j.euroneuro.2015.09.006
119. Nierenberg, AA, Greist, JH, Mallinckrodt, CH, Prakash, A, Sambunaris, A, Tollefson, GD, et al. Duloxetine versus escitalopram and placebo in the treatment of patients with major depressive disorder: onset of antidepressant action, a non-inferiority study. Curr Med Res Opin. (2007) 23:401–16. doi: 10.1185/030079906X167453
120. Hewett, K, Chrzanowski, W, Schmitz, M, Savela, A, Milanova, V, Gee, M, et al. Eight-week, placebo-controlled, double-blind comparison of the antidepressant efficacy and tolerability of bupropion XR and venlafaxine XR. J Psychopharmacol. (2009) 23:531–8. doi: 10.1177/0269881108089602
121. Asnis, GM, Bose, A, Gommoll, CP, Chen, C, and Greenberg, WM. Efficacy and safety of levomilnacipran sustained release 40 mg, 80 mg, or 120 mg in major depressive disorder: a phase 3, randomized, double-blind, placebo-controlled study. J Clin Psychiatry. (2013) 74:242–8. doi: 10.4088/JCP.12m08197
122. Hewett, K, Gee, MD, Krishen, A, Wunderlich, HP, Le Clus, A, Evoniuk, G, et al. Double-blind, placebo-controlled comparison of the antidepressant efficacy and tolerability of bupropion XR and venlafaxine XR. J Psychopharmacol. (2010) 24:1209–16. doi: 10.1177/0269881109106953
123. Bakish, D, Bose, A, Gommoll, C, Chen, C, Nunez, R, Greenberg, WM, et al. Levomilnacipran ER 40 mg and 80 mg in patients with major depressive disorder: a phase III, randomized, double-blind, fixed-dose, placebo-controlled study. J Psychiatry Neurosci. (2014) 39:40–9. doi: 10.1503/jpn.130040
124. Montgomery, SA, Mansuy, L, Ruth, A, Bose, A, Li, H, and Li, D. Efficacy and safety of levomilnacipran sustained release in moderate to severe major depressive disorder: a randomized, double-blind, placebo-controlled, proof-of-concept study. J Clin Psychiatry. (2013) 74:363–9. doi: 10.4088/JCP.12m08141
125. Boyer, P, Montgomery, S, Lepola, U, Germain, JM, Brisard, C, Ganguly, R, et al. Efficacy, safety, and tolerability of fixed-dose desvenlafaxine 50 and 100 mg/day for major depressive disorder in a placebo-controlled trial. Int Clin Psychopharmacol. (2008) 23:243–53. doi: 10.1097/YIC.0b013e32830cebed
126. Sambunaris, A, Bose, A, Gommoll, CP, Chen, C, Greenberg, WM, and Sheehan, DV. A phase III, double-blind, placebo-controlled, flexible-dose study of levomilnacipran extended-release in patients with major depressive disorder. J Clin Psychopharmacol. (2014) 34:47–56. doi: 10.1097/JCP.0000000000000060
127. Dunlop, BW, Reddy, S, Yang, L, Lubaczewski, S, Focht, K, and Guico-Pabia, CJ. Symptomatic and functional improvement in employed depressed patients: a double-blind clinical trial of desvenlafaxine versus placebo. J Clin Psychopharmacol. (2011) 31:569–76. doi: 10.1097/JCP.0b013e31822c0a68
128. Liebowitz, MR, Manley, AL, Padmanabhan, SK, Ganguly, R, Tummala, R, and Tourian, KA. Efficacy, safety, and tolerability of desvenlafaxine 50 mg/day and 100 mg/day in outpatients with major depressive disorder. Curr Med Res Opin. (2008) 24:1877–90. doi: 10.1185/03007990802161923
129. Detke, MJ, Wiltse, CG, Mallinckrodt, CH, McNamara, RK, Demitrack, MA, and Bitter, I. Duloxetine in the acute and long-term treatment of major depressive disorder: a placebo- and paroxetine-controlled trial. Eur Neuropsychopharmacol. (2004) 14:457–70. doi: 10.1016/j.euroneuro.2004.01.002
130. Iwata, N, Tourian, KA, Hwang, E, Mele, L, and Vialet, C. Efficacy and safety of desvenlafaxine 25 and 50 mg/day in a randomized, placebo-controlled study of depressed outpatients. J Psychiatr Pract. (2013) 19:5–14. doi: 10.1097/01.pra.0000426323.59698.64
131. Perahia, DG, Wang, F, Mallinckrodt, CH, Walker, DJ, and Detke, MJ. Duloxetine in the treatment of major depressive disorder: a placebo- and paroxetine-controlled trial. Eur Psychiatry. (2006) 21:367–78. doi: 10.1016/j.eurpsy.2006.03.004
132. Liebowitz, MR, Tourian, KA, Hwang, E, Mele, L, and Study, I. A double-blind, randomized, placebo-controlled study assessing the efficacy and tolerability of desvenlafaxine 10 and 50 mg/day in adult outpatients with major depressive disorder. BMC Psychiatry. (2013) 13:94. doi: 10.1186/1471-244X-13-94
133. Boyer, P, Vialet, C, Hwang, E, and Tourian, KA. Efficacy of desvenlafaxine 50 mg/d versus placebo in the long-term treatment of major depressive disorder: a randomized, double-blind trial. Prim Care Companion CNS Disord. (2015) 17:1711. doi: 10.4088/PCC.14m01711
134. Boulenger, JP, Loft, H, and Olsen, CK. Efficacy and safety of vortioxetine (Lu AA21004), 15 and 20 mg/day: a randomized, double-blind, placebo-controlled, duloxetine-referenced study in the acute treatment of adult patients with major depressive disorder. Int Clin Psychopharmacol. (2014) 29:138–49. doi: 10.1097/YIC.0000000000000018
135. Mahableshwarkar, AR, Zajecka, J, Jacobson, W, Chen, Y, and Keefe, RS. A randomized, placebo-controlled, active-reference, double-blind, flexible-dose study of the efficacy of vortioxetine on cognitive function in major depressive disorder. Neuropsychopharmacology. (2015) 40:2025–37. doi: 10.1038/npp.2015.52
136. Gaynor, PJ, Gopal, M, Zheng, W, Martinez, JM, Robinson, MJ, Hann, D, et al. Duloxetine versus placebo in the treatment of major depressive disorder and associated painful physical symptoms: a replication study. Curr Med Res Opin. (2011) 27:1859–67. doi: 10.1185/03007995.2011.609540
137. Mahableshwarkar, AR, Jacobsen, PL, Serenko, M, Chen, Y, and Trivedi, MH. A randomized, double-blind, placebo-controlled study of the efficacy and safety of 2 doses of vortioxetine in adults with major depressive disorder. J Clin Psychiatry. (2015) 76:583–91. doi: 10.4088/JCP.14m09337
138. Gaynor, PJ, Gopal, M, Zheng, W, Martinez, JM, Robinson, MJ, and Marangell, LB. A randomized placebo-controlled trial of duloxetine in patients with major depressive disorder and associated painful physical symptoms. Curr Med Res Opin. (2011) 27:1849–58. doi: 10.1185/03007995.2011.609539
139. Oakes, TM, Myers, AL, Marangell, LB, Ahl, J, Prakash, A, Thase, ME, et al. Assessment of depressive symptoms and functional outcomes in patients with major depressive disorder treated with duloxetine versus placebo: primary outcomes from two trials conducted under the same protocol. Hum Psychopharmacol. (2012) 27:47–56. doi: 10.1002/hup.1262
140. Montgomery, SA, Nielsen, RZ, Poulsen, LH, and Haggstrom, L. A randomised, double-blind study in adults with major depressive disorder with an inadequate response to a single course of selective serotonin reuptake inhibitor or serotonin-noradrenaline reuptake inhibitor treatment switched to vortioxetine or agomelatine. Hum Psychopharmacol. (2014) 29:470–82. doi: 10.1002/hup.2424
141. Boyer, P, Danion, JM, Bisserbe, JC, Hotton, JM, and Troy, S. Clinical and economic comparison of sertraline and fluoxetine in the treatment of depression. A 6-month double-blind study in a primary-care setting in France. PharmacoEconomics. (1998) 13:157–69. doi: 10.2165/00019053-199813010-00015
142. Soczynska, JK, Ravindran, LN, Styra, R, McIntyre, RS, Cyriac, A, Manierka, MS, et al. The effect of bupropion XL and escitalopram on memory and functional outcomes in adults with major depressive disorder: results from a randomized controlled trial. Psychiatry Res. (2014) 220:245–50. doi: 10.1016/j.psychres.2014.06.053
143. Wang, G, Gislum, M, Filippov, G, and Montgomery, S. Comparison of vortioxetine versus venlafaxine XR in adults in Asia with major depressive disorder: a randomized, double-blind study. Curr Med Res Opin. (2015) 31:785–94. doi: 10.1185/03007995.2015.1014028
144. Wade, A, Gembert, K, and Florea, I. A comparative study of the efficacy of acute and continuation treatment with escitalopram versus duloxetine in patients with major depressive disorder. Curr Med Res Opin. (2007) 23:1605–14. doi: 10.1185/030079907x210732
145. Fernandez, JL, Montgomery, S, and Francois, C. Evaluation of the cost effectiveness of escitalopram versus venlafaxine XR in major depressive disorder. PharmacoEconomics. (2005) 23:155–67. doi: 10.2165/00019053-200523020-00007
146. Romeo, R, Patel, A, Knapp, M, and Thomas, C. The cost-effectiveness of mirtazapine versus paroxetine in treating people with depression in primary care. Int Clin Psychopharmacol. (2004) 19:125–34. doi: 10.1097/00004850-200405000-00002
147. Wade, AG, Fernandez, JL, Francois, C, Hansen, K, Danchenko, N, and Despiegel, N. Escitalopram and duloxetine in major depressive disorder: a pharmacoeconomic comparison using UK cost data. PharmacoEconomics. (2008) 26:969–81. doi: 10.2165/00019053-200826110-00008
148. Fantino, B, Moore, N, Verdoux, H, and Auray, JP. Cost-effectiveness of escitalopram vs. citalopram in major depressive disorder. Int Clin Psychopharmacol. (2007) 22:107–15. doi: 10.1097/YIC.0b013e3280128d16
149. Miller, IW, Keitner, GI, Schatzberg, AF, Klein, DN, Thase, ME, Rush, AJ, et al. The treatment of chronic depression, part 3: psychosocial functioning before and after treatment with sertraline or imipramine. J Clin Psychiatry. (1998) 59:608–19. doi: 10.4088/jcp.v59n1108
150. Agosti, V, Stewart, JW, and Quitkin, FM. Life satisfaction and psychosocial functioning in chronic depression: effect of acute treatment with antidepressants. J Affect Disord. (1991) 23:35–41. doi: 10.1016/0165-0327(91)90033-o
151. Hammer-Helmich, L, Haro, JM, Jonsson, B, Tanguy Melac, A, Di Nicola, S, Chollet, J, et al. Functional impairment in patients with major depressive disorder: the 2-year PERFORM study. Neuropsychiatr Dis Treat. (2018) 14:239–49. doi: 10.2147/NDT.S146098
152. Chokka, P, Tvistholm, AH, Bougie, J, Clerzius, G, and Ettrup, A. Improvements in workplace productivity in working patients with major depressive disorder: results from the AtWoRC atudy. J Occup Environ Med. (2020) 62:e94–e101. doi: 10.1097/JOM.0000000000001805
153. Mattingly, G, Brunner, E, Chrones, L, Lawrence, DF, Simonsen, K, and Ren, H. Effectiveness of vortioxetine for major depressive disorder in real-world clinical practice: US cohort results from the global RELIEVE study. Front Psych. (2022) 13:977560. doi: 10.3389/fpsyt.2022.977560
154. Swainson, J, McGirr, A, Blier, P, Brietzke, E, Richard-Devantoy, S, Ravindran, N, et al. The Canadian network for mood and anxiety treatments (CANMAT) task force recommendations for the use of racemic ketamine in adults with major depressive disorder. Can J Psychiatr. (2021) 66:113–25. doi: 10.1177/0706743720970860
155. Ng, J, Rosenblat, JD, Lui, LMW, Teopiz, KM, Lee, Y, Lipsitz, O, et al. Efficacy of ketamine and esketamine on functional outcomes in treatment-resistant depression: a systematic review. J Affect Disord. (2021) 293:285–94. doi: 10.1016/j.jad.2021.06.032
156. Rodrigues, NB, McIntyre, RS, Lipsitz, O, Lee, Y, Subramaniapillai, M, Kratiuk, K, et al. The effect of repeated doses of intravenous ketamine on measures of workplace attendance and productivity in adults with major depressive and bipolar disorder: results from the Canadian rapid treatment Center of Excellence. Psychiatry Res. (2021) 300:113860. doi: 10.1016/j.psychres.2021.113860
157. Linde, K, Rucker, G, Sigterman, K, Jamil, S, Meissner, K, Schneider, A, et al. Comparative effectiveness of psychological treatments for depressive disorders in primary care: network meta-analysis. BMC Fam Pract. (2015) 16:103. doi: 10.1186/s12875-015-0314-x
158. Tolin, DF. Is cognitive-behavioral therapy more effective than other therapies? A meta-analytic review. Clin Psychol Rev. (2010) 30:710–20. doi: 10.1016/j.cpr.2010.05.003
159. Cuijpers, P, Cristea, IA, Karyotaki, E, Reijnders, M, and Huibers, MJ. How effective are cognitive behavior therapies for major depression and anxiety disorders? A meta-analytic update of the evidence. World Psychiatry. (2016) 15:245–58. doi: 10.1002/wps.20346
160. Cuijpers, P, Berking, M, Andersson, G, Quigley, L, Kleiboer, A, and Dobson, KS. A meta-analysis of cognitive-behavioural therapy for adult depression, alone and in comparison with other treatments. Can J Psychiatr. (2013) 58:376–85. doi: 10.1177/070674371305800702
161. Cuijpers, P, Miguel, C, Harrer, M, Plessen, CY, Ciharova, M, Ebert, D, et al. Cognitive behavior therapy vs. control conditions, other psychotherapies, pharmacotherapies and combined treatment for depression: a comprehensive meta-analysis including 409 trials with 52,702 patients. World Psychiatry. (2023) 22:105–15. doi: 10.1002/wps.21069
162. Parikh, SV, Quilty, LC, Ravitz, P, Rosenbluth, M, Pavlova, B, Grigoriadis, S, et al. Canadian network for mood and anxiety treatments (CANMAT) 2016 clinical guidelines for the Management of Adults with major depressive disorder: section 2. Psychol Treatment Can J Psychiatry. (2016) 61:524–39. doi: 10.1177/0706743716659418
163. Kamenov, K, Twomey, C, Cabello, M, Prina, AM, and Ayuso-Mateos, JL. The efficacy of psychotherapy, pharmacotherapy and their combination on functioning and quality of life in depression: a meta-analysis. Psychol Med. (2017) 47:414–25. doi: 10.1017/S0033291716002774
164. Stratton, E, Jones, N, Peters, SE, Torous, J, and Glozier, N. Digital mHealth interventions for employees: systematic review and meta-analysis of their effects on workplace outcomes. J Occup Environ Med. (2021) 63:e512–25. doi: 10.1097/JOM.0000000000002267
165. Huberty, JL, Espel-Huynh, HM, Neher, TL, and Puzia, ME. Testing the pragmatic effectiveness of a consumer-based mindfulness mobile app in the workplace: randomized controlled trial. JMIR Mhealth Uhealth. (2022) 10:e38903. doi: 10.2196/38903
166. Stratton, E, Lampit, A, Choi, I, Malmberg Gavelin, H, Aji, M, Taylor, J, et al. Trends in effectiveness of organizational eHealth interventions in addressing employee mental health: systematic review and meta-analysis. J Med Internet Res. (2022) 24:e37776. doi: 10.2196/37776
167. Corbière, M, Lachance, JP, Jean-Baptiste, F, Hache-Labelle, C, Riopel, G, and Lecomte, T. Healthy minds: group cognitive-behavioral intervention for sustainable return to work after a sick leave due to depression. J Occup Rehabil. (2022) 32:505–14. doi: 10.1007/s10926-021-09991-6
168. Finnes, A, Enebrink, P, Ghaderi, A, Dahl, J, Nager, A, and Ost, LG. Psychological treatments for return to work in individuals on sickness absence due to common mental disorders or musculoskeletal disorders: a systematic review and meta-analysis of randomized-controlled trials. Int Arch Occup Environ Health. (2019) 92:273–93. doi: 10.1007/s00420-018-1380-x
169. Salomonsson, S, Hedman-Lagerlof, E, and Ost, LG. Sickness absence: a systematic review and meta-analysis of psychological treatments for individuals on sick leave due to common mental disorders. Psychol Med. (2018) 48:1954–65. doi: 10.1017/S0033291718000065
170. Carolan, S, Harris, PR, and Cavanagh, K. Improving employee well-being and effectiveness: systematic review and meta-analysis of web-based psychological interventions delivered in the workplace. J Med Internet Res. (2017) 19:e271. doi: 10.2196/jmir.7583
171. Udd-Granat, L, Lahti, J, Donnelly, M, Treanor, C, Pirkola, SP, Lallukka, T, et al. Internet-delivered cognitive behavioral therapy (iCBT) for common mental disorders and subsequent sickness absence: a systematic review and meta-analysis. Scand J Public Health. (2023) 51:137–47. doi: 10.1177/14034948221075016
172. Bond, G, Lemer, D, Drake, R, Reidy, C, and Choi, J. Work-focused interventions for depression: Final report. (2019). Available at: https://aspe.hhs.gov/basic-report/work-focused-interventions-depression-final-report.
173. Cullen, KL, Irvin, E, Collie, A, Clay, F, Gensby, U, Jennings, PA, et al. Effectiveness of workplace interventions in return-to-work for musculoskeletal, pain-related and mental health conditions: An update of the evidence and messages for practitioners. J Occup Rehabil. (2018) 28:1–15. doi: 10.1007/s10926-016-9690-x
174. Krogh, J, Saltin, B, Gluud, C, and Nordentoft, M. The DEMO trial: a randomized, parallel-group, observer-blinded clinical trial of strength versus aerobic versus relaxation training for patients with mild to moderate depression. J Clin Psychiatry. (2009) 70:790–800. doi: 10.4088/jcp.08m04241
175. Krogh, J, Videbech, P, Thomsen, C, Gluud, C, and Nordentoft, M. DEMO-II trial. Aerobic exercise versus stretching exercise in patients with major depression–a randomised clinical trial. PLoS One. (2012) 7:e48316. doi: 10.1371/journal.pone.0048316
176. Hallgren, M, Kraepelien, M, Öjehagen, A, Lindefors, N, Zeebari, Z, Kaldo, V, et al. Physical exercise and internet-based cognitive-behavioural therapy in the treatment of depression: randomised controlled trial. Br J Psychiatry. (2015) 207:227–34. doi: 10.1192/bjp.bp.114.160101
177. Kaldo, V, Lundin, A, Hallgren, M, Kraepelien, M, Strid, C, Ekblom, Ö, et al. Effects of internet-based cognitive behavioural therapy and physical exercise on sick leave and employment in primary care patients with depression: two subgroup analyses. Occup Environ Med. (2018) 75:52–8. doi: 10.1136/oemed-2017-104326
178. Corbière, M, Mazaniello-Chezol, M, Bastien, MF, Wathieu, E, Bouchard, R, Panaccio, A, et al. Stakeholders’ role and actions in the return-to-work process of workers on sick-leave due to common mental disorders: a scoping review. J Occup Rehabil. (2020) 30:381–419. doi: 10.1007/s10926-019-09861-2
179. Rothermund, E, Michaelis, M, Jarczok, MN, Balint, EM, Lange, R, Zipfel, S, et al. Prevention of common mental disorders in employees. Perspectives on collaboration from three health care professions. Int J Environ Res Public Health. (2018):15. doi: 10.3390/ijerph15020278
180. ACED. Accommodating and communicating about episodic disabilities (ACED) project. Supporting employee success. (2019). Available at: https://aced.iwh.on.ca/tools/partner-tools/supporting-employee-success (Accessed March 8, 2021).
181. Canadian Medical Association. CMA Policy: Third-party forms. (2017). Available at: https://policybase.cma.ca/documents/Policypdf/PD17-02.pdf (Accessed July 31, 2020).
182. Chénier, L, and Boyer, C. Healthy brains at work: Employer-sponsored mental health benefits and programs. (2016). Available at: https://www.conferenceboard.ca/e-library/abstract.aspx?did=7707 (Accessed April 10, 2020).
183. Nielsen, MB, Christensen, JO, Finne, LB, and Knardahl, S. Workplace bullying, mental distress, and sickness absence: the protective role of social support. Int Arch Occup Environ Health. (2020) 93:43–53. doi: 10.1007/s00420-019-01463-y
184. Etuknwa, A, Daniels, K, and Eib, C. Sustainable return to work: a systematic review focusing on personal and social factors. J Occup Rehabil. (2019) 29:679–700. doi: 10.1007/s10926-019-09832-7
185. Dewa, CS, Weeghel, JV, Joosen, MC, and Brouwers, EP. What could influence workers’ decisions to disclose a mental illness at work? Int J Occup Environ Med. (2020) 11:119–27. doi: 10.34172/ijoem.2020.1870
186. Toth, KE, Yvon, F, Villotti, P, Lecomte, T, Lachance, JP, Kirsh, B, et al. Disclosure dilemmas: how people with a mental health condition perceive and manage disclosure at work. Disabil Rehabil. (2022) 44:7791–801. doi: 10.1080/09638288.2021.1998667
187. Porter, S, Lexen, A, Johanson, S, and Bejerholm, U. Critical factors for the return-to-work process among people with affective disorders: voices from two vocational approaches. Work. (2018) 60:221–34. doi: 10.3233/WOR-182737
188. Brouwers, EPM, Joosen, MCW, van Zelst, C, and Van Weeghel, J. To disclose or not to disclose: a multi-stakeholder focus group study on mental health issues in the work environment. J Occup Rehabil. (2020) 30:84–92. doi: 10.1007/s10926-019-09848-z
189. Corbière, M, Bergeron, G, Negrini, A, Coutu, M-F, Samson, E, Sauve, G, et al. Employee perceptions about factors influencing their return to work after a sick-leave due to depression. J Rehabil. (2018) 84:3–13.
190. Yvon, F, and Corbière, M. Implicit and explicit attitudes of employers toward hiring people who have experienced depression. J Occup Rehabil. (2021) 31:903–15. doi: 10.1007/s10926-021-09977-4
191. Hanisch, SE, Twomey, CD, Szeto, AC, Birner, UW, Nowak, D, and Sabariego, C. The effectiveness of interventions targeting the stigma of mental illness at the workplace: a systematic review. BMC Psychiatry. (2016) 16:1. doi: 10.1186/s12888-015-0706-4
192. Doty, B, Grzenda, A, Hwang, S, Godar, S, Gruttadaro, D, Hauge, KA, et al. An ecological study of a universal employee depression awareness and stigma reduction intervention: “right direction”. Front Psych. (2021) 12:581876. doi: 10.3389/fpsyt.2021.581876
193. Dobson, KS, Szeto, A, and Knaak, S. The working mind: a meta-analysis of a workplace mental health and stigma reduction program. Can J Psychiatr. (2019) 64:39S–47S. doi: 10.1177/0706743719842559
194. Dobson, KS, Markova, V, Wen, A, and Smith, LM. Effects of the anti-stigma workplace intervention “working mind” in a Canadian health-care setting: a cluster-randomized trial of immediate versus delayed implementation. Can J Psychiatr. (2021) 66:495–502. doi: 10.1177/0706743720961738
195. Canadian Medical Association. CMA Submission: Maintaining Ontario’s leadership on prohibiting the use of sick notes for short medical leaves. Submission to the Standing Committee on Finance and Economic Affairs. (2018). Available at: https://policybase.cma.ca/documents/Briefpdf/BR2019-03.pdf (Accessed July 31, 2020).
196. Railway Association of Canada. Canadian railway medical rules handbook. (2020). Available at: https://www.railcan.ca/wp-content/uploads/2020/01/Canadian-Railway-Medical-Rules-Handbook-FINAL-February-2020-03-13.pdf (Accessed July 31, 2020).
197. Chow, CM, Cichocki, B, and Croft, B. The impact of job accommodations on employment outcomes among individuals with psychiatric disabilities. Psychiatr Serv. (2014) 65:1126–32. doi: 10.1176/appi.ps.201300267
198. Fabian, ES, Waterworth, A, and Ripke, B. Reasonable accommodations for workers with serious mental illness: type, frequency, and associated outcomes. Psychosocial Rehab J. (1993) 17:163.
199. MacDonald-Wilson, KL, Rogers, ES, Massaro, JM, Lyass, A, and Crean, T. An investigation of reasonable workplace accommodations for people with psychiatric disabilities: quantitative findings from a multi-site study. Community Ment Health J. (2002) 38:35–50. doi: 10.1023/a:1013955830779
200. Corbière, M, Villotti, P, Lecomte, T, Bond, GR, Lesage, A, and Goldner, EM. Work accommodations and natural supports for maintaining employment. Psychiatr Rehabil J. (2014) 37:90–8. doi: 10.1037/prj0000033
201. Villotti, P, Corbière, M, Fossey, E, Fraccaroli, F, Lecomte, T, and Harvey, C. Work accommodations and natural supports for employees with severe mental illness in social businesses: An international comparison. Comm Mental Health J. (2017) 53:864–70. doi: 10.1007/s10597-016-0068-5
202. Corbière, M, Villotti, P, Dewa, CS, Sultan-Taïeb, H, Fraccaroli, F, Zaniboni, S, et al. Work accommodations in Canadian social firms: supervisors’ and workers’ perspectives. Can J Comm Mental Health. (2019) 37:37–56. doi: 10.7870/cjcmh-2018-026
203. Negrini, A, Corbière, M, Lecomte, T, Coutu, MF, Nieuwenhuijsen, K, St-Arnaud, L, et al. How can supervisors contribute to the return to work of employees who have experienced depression? J Occup Rehabil. (2018) 28:279–88. doi: 10.1007/s10926-017-9715-0
204. De Vries, H, Fishta, A, Weikert, B, Rodriguez Sanchez, A, and Wegewitz, U. Determinants of sickness absence and return to work among employees with common mental disorders: a scoping review. J Occup Rehabil. (2018) 28:393–417. doi: 10.1007/s10926-017-9730-1
205. Villotti, P, Gragnano, A, Lariviere, C, Negrini, A, Dionne, CE, and Corbière, M. Tools appraisal of organizational factors associated with return-to-work in workers on sick leave due to musculoskeletal and common mental disorders: a systematic search and review. J Occup Rehabil. (2021) 31:7–25. doi: 10.1007/s10926-020-09902-1
206. Gragnano, A, Villotti, P, Lariviere, C, Negrini, A, and Corbière, M. A systematic search and review of questionnaires measuring individual psychosocial factors predicting return to work after musculoskeletal and common mental disorders. J Occup Rehabil. (2021) 31:491–511. doi: 10.1007/s10926-020-09935-6
207. Roca, M, Bonelli, A, Cattaneo, A, Comandini, A, Di Dato, G, Heiman, F, et al. Factors associated with sick leave duration in patients suffering from major depressive disorder initiating antidepressant treatment: a real-world evidence study in Germany and Spain. Int J Psychiatry Clin Pract. (2022) 2022:1–10. doi: 10.1080/13651501.2022.2092515
208. Government of Canada/Gouvernement du Canada. Canada Occupational Health and Safety Regulations (SOR/86–304). (2020). Available at: https://laws.justice.gc.ca/eng/regulations/sor-86-304/index.html (Accessed July 31, 2020).
209. Government of Canada/Gouvernement du Canada. Canada Labour Code (R.S.C., 1985, c. L-2). (2020). Available at: https://laws-lois.justice.gc.ca/eng/acts/L-2/ (Accessed July 31, 2020).
210. Government of Canada/Government du Canada. The Fundamentals–Duty to Accommodate: Roles and Responsibilities. (2011). Available at: https://www.canada.ca/en/government/publicservice/wellness-inclusion-diversity-public-service/health-wellness-public-servants/disability-management/fundamentals-duty-accommodate-roles-responsibilities.html (Accessed July 31, 2020).
Keywords: mental health, major depressive disorder, occupational health, absenteeism, presenteeism, disability, return to work, workplace
Citation: Chokka P, Bender A, Brennan S, Ahmed G, Corbière M, Dozois DJA, Habert J, Harrison J, Katzman MA, McIntyre RS, Liu YS, Nieuwenhuijsen K and Dewa CS (2023) Practical pathway for the management of depression in the workplace: a Canadian perspective. Front. Psychiatry. 14:1207653. doi: 10.3389/fpsyt.2023.1207653
Edited by:
Hikaru Hori, Fukuoka University, JapanReviewed by:
Debra Lerner, Tufts Medical Center, United StatesCopyright © 2023 Chokka, Bender, Brennan, Ahmed, Corbière, Dozois, Habert, Harrison, Katzman, McIntyre, Liu, Nieuwenhuijsen and Dewa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pratap Chokka, cHJhdGFwY2hva2thQGNob2trYWNlbnRlci5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.