
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 06 September 2023
Sec. Public Mental Health
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1201193
This article is part of the Research Topic Psychometrics in Psychiatry 2022: Mood Disorders View all 8 articles
 Ali Mehrabi1
Ali Mehrabi1 Azam Naghavi2Mohammad Ershad Afsharzada2Sören Friedrich3Thomas Forkmann4
Azam Naghavi2Mohammad Ershad Afsharzada2Sören Friedrich3Thomas Forkmann4 Heide Glaesmer5
Heide Glaesmer5 Tobias Teismann3*
Tobias Teismann3*Objective: Suicide ideation and suicide attempts are prevalent in Farsi speaking populations. The present study aimed at validating the Farsi version of the Suicide Ideation and Behavior Scale (SIBS).
Methods: Reliability and validity of the Farsi version of the SIBS were established in a highly burdened Afghan student sample (N = 279). Internal consistency, convergent and discriminant validity were investigated, and confirmatory factor analysis was conducted.
Results: The Farsi version of the SIBS was shown to have a unidimensional structure with excellent internal consistency, as well as good convergent and divergent validity.
Discussion: The results suggest that the SIBS is a brief, reliable, and valid measure of current suicidal ideation and behavior that can be used in Farsi speaking populations.
Suicide ideation and suicidal behavior is prevalent in Iran (1, 2) and Afghanistan (3, 4). Furthermore, suicide ideation and suicide attempts are frequent in migrant populations from the respective countries (5). Suicide ideation and suicide attempts are among the strongest risk factors for suicide (6), and they are deeply distressing (7). Accordingly, it is important to have validated instruments for assessing suicide ideation and suicidal behavior for both research and clinical practice. In clinical practice, the use of questionnaires is justified in particular by the fact that affected persons regularly find it easier to disclose suicidal ideation in a questionnaire than in a personal conversation (8).
At this time, there are two validated questionnaire to assess suicidal ideation and behavior available in Farsi: the Suicidal Behavior Questionnaire-Revised [SBQ-R; (9)] and the Depressive Symptom Inventory–Suicidality Subscale [F-DSI-SS; (10)]. The SBQ-R has originally been developed by Osman et al. (11) and comprises four items that capture different facets of suicide ideation and behavior (lifetime suicidal thoughts, plans, and attempts; suicidal thoughts during the past 12 months; expression of suicidal intentions; likelihood of future suicidal acts). The Farsi version of the SBQ-R showed good internal consistency (α = 0.82) in an Iranian undergraduate sample and was shown to be positively correlated with single item assessments of suicide acceptability and lifetime suicide ideation [rs > 0.30; (9)]. However, the SBQ-R has been criticized for using an inconsistent item response format and mixing of different time perspectives (prospective, retrospective) within the four items (12). Furthermore, the SBQ-R does not assess current suicide ideation. The DSI-SS has originally been developed by Joiner et al. (13) and assesses with four items the frequency and intensity of suicidal ideation within the past 2 weeks. The Farsi version of the DSI-SS showed good internal consistency (α = 0.89) in an Iranian college student sample and was shown to be positively correlated with a measure of suicide-specific rumination (10). However, the DSI-SS does not capture suicidal intentions or attempts.
On this background, a frequently used German questionnaire, the Suicide Ideation and Behavior Scale [SIBS; (14), German name: Skala Suizidales Erleben und Verhalten, SSEV], was developed and translated into Farsi. The SIBS comprises nine items to measure the frequency and intensity of passive and active suicidal thoughts, suicidal intentions, suicidal impulses, suicidal plans and suicide attempts within the last 4 weeks. Lifetime suicide attempts are assessed with two additional items. Teismann et al. (14) created the SIBS based on existing guidelines for the exploration of suicide ideation and behavior (15) and under acknowledgement of current classification systems and definitions of suicidal ideation and behavior (16). The scale has a unidimensional structure and showed good internal consistency (α = 0.92) in German non-clinical and clinical adult samples. Furthermore, the scale has been shown to significantly correlate with depression, hopelessness, perceived burdensomeness as well as positive mental health. Scores in the SIBS did not differ between men and women; yet, clinical samples displayed higher scores than non-clinical samples (14). In a recent adaptation of the scale for children and adolescents (aged > 11 years), the unidimensional structure of the scale was replicated in a sample of adolescent German outpatients (17). The SIBS for Kids has a good internal consistency (α = 0.89) and shows significant correlations with symptom burden, perceived burdensomeness and thwarted belongingness; girls displayed higher scores than boys.
Taken together, it seems as if the SIBS is a reliable and valid assessment tool for suicide ideation and behavior. To enable cross-cultural research as well as clinical work in refugee populations the scale has recently been translated into various languages (Albanian, Arabic, English, French, Kurmanji, Russian, Spanish, Sorani, Tigrinya, Turkish, Ukrainian; all versions available on www.q-cultural.de). Psychometric evaluation studies on the different language versions of the SIBS are pending. On this background, the current study aimed to examine the factor structure, psychometric properties and construct validity of the Farsi version of the SIBS within an Afghan student sample. Afghan students have been shown to suffer from high levels of posttraumatic stress, depression and suicidality (3) making it a very relevant population to focus on. Furthermore, Shoib et al. (18) recently called for the adaptation of validated assessment tools for the Afghan population in order to improve psychosocial and medical care in the country.
In light of the aforementioned studies (14, 17), we expected to replicate the unidimensional structure of the SIBS in this Farsi speaking sample. Furthermore, significant positive correlations were expected between SIBS scores and depression, PTSD and suicide ideation/behavior scores; whereas a significant negative correlation was expected between positive mental health and the SIBS score. Finally, we did not expected to find gender differences in SIBS scores [cf. (3, 14)]. The present validation study was implemented as part of a larger study on psychological well-being of Afghan students (19).
The sample consisted of 279 university students (61.6% women; age: 18–21 years: 43%; 22–24: 36.6%; 25–27: 6.5%; 28–30: 14%) affiliated with Herat University, Eshragh University, Jami University and Ghaleb University in Afghanistan. Participants were recruited via personal invitations or invitations forwarded via social media between July and November 2022. The study invitation indicated that the survey would address suicidal ideation as well as traumatic experiences. The participation was voluntary and participants received no compensation for taking part in the study. The Ethics Committee of the Faculty of Psychology, Ruhr-Universität Bochum approved the implementation of the present study (790/2022). All participants were properly instructed and provided their informed consent to participate online.
Suicide Ideation and Behavior Scale [SIBS; (14)]: The SIBS comprises six items assessing (passive/active) suicide ideation, suicidal intent, suicidal impulses and suicide planning within the last 4 weeks. Items are rated on a 6-point Likert-type scale (0 = never, 5 = many times a day). Three further items assess the occurrence of a suicide attempt within the last 4 weeks as well as occurrence/frequency of lifetime suicide attempts. The questionnaire was translated to Farsi using the back translation method (20): The English version of the SIBS was translated by a researcher from Iran, than it was reviewed by two researchers from an Afghan background. Afterwards it was back-translated to English by a different Farsi speaking researcher, who was unfamiliar with the original SIBS items. The original items and instructions of the SIBS and the back-translated items and instructions were than independently compared by two clinical researchers from Germany. There were no substantial discrepancies regarding all SIBS items. Furthermore, there were no specific issues that arised during the translation process, as such there were no words or expressions that were difficult to translate from English to Farsi [cf. (9, 10)].
Suicide Behaviors Questionnaire-Revised [SBQ-R; (11); Farsi version: (9)]: The SBQ-R comprises four items assessing different facets of suicidal ideation and behavior (lifetime suicide ideation, suicide plans, suicide attempts, 12-month suicide ideation, suicidal communication, and one’s estimation of how likely a future suicide attempt might be). Each item utilizes a different Likert scale with a sum score of 18 points indicating the highest severity of suicidal risk. Internal consistency was good (α = 0.79) in the current sample. At the time the present study was conducted, the SBQ-R was the only validated suicide questionnaire available in Farsi and was therefore chosen to establish convergent validity.
PTSD Checklist [PCL-5; (21); Farsi version: (22)]: The PCL-5 assesses symptoms of PTSD (e.g., intrusion, avoidance, cognitive and mood alteration, arousal) with 20 items (e.g., “In the past month, how much have you been bothered by: Having strong negative feelings such as fear, horror, anger, guilt, or shame?”) that are rated on a 5-point Likert-type scale (0 = not at all, 4 = extremely). The higher the sum score, the higher the symptoms of PTSD. Internal consistency was α = 0.91 in the current sample.
Patient Health Questionnaire [PHQ-9; (23); Farsi version: (24)]: The Patient Health Questionnaire (PHQ-9) assesses symptoms of depression (e.g., lack of interest, feeling down, poor appetite) with nine items (e.g., “Over the last 2 weeks, how often have you been bothered by any of the following problems: Little interest or pleasure in doing things?”) that are rated on a 4-point Likert-type scale (0 = not at all, 3 = nearly every day). Internal consistency was α = 0.88 in the current sample.
Positive Mental Health Scale [PMH-Scale; (25); Farsi version: (26)]: The PMH-Scale assesses subjective and psychological aspects of well-being across nine items (e.g., “I manage well to fulfill my needs”; “I feel that I am actually well equipped to deal with life and its difficulties”) that are rated on a 4-point Likert-scale (0 = do not agree, 3 = agree). Higher scores indicate higher levels of PMH. Internal consistency was α = 0.85 in the current sample.
IBM SPSS Statistics Version 27 (27) and R (version 4.1.3, Package:lavaan) were used for statistical analysis. Participants who scored higher than 0 in the SIBS were classified as suffering from suicidal ideation [cf. (28)]. Participants who affirmed the SIBS item on lifetime suicide attempts (item 8) were classified as lifetime suicide attempters. Distribution of the data was verified using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Subsequently, the means, standard deviations as well as skewness and kurtosis of all items, as well as their influence on the internal consistency of the scale were analyzed. In order to check the fit of the one-factorial model determined by Teismann et al. (14), a confirmatory factor analysis (CFA) based on items 1 to 6 was carried out. Due to the ordinal scale level of the SIBS, the Robust Weighted Least Square Estimator (WLSM) was used. The following fit indices were used to assess the model fit: Fit Index χ2 according to Satorra-Bentler-correction (29), the Root Mean-Square Error of Approximation (RMSEA) with 90% confidence interval (90% CI), the Comparative-Fit-Index (CFI), the Tucker-Lewis Index (TLI) and the standardized Root Mean Square Residual (SRMR). The cut-off values were interpreted according to the guidelines of Hu and Bentler (30): RMSEA values of <0.05 indicate a good model fit, values between <0.08 and >0.05 indicate an adequate model fit (31). Values of >0.90 for the CFI and the TLI and for the SMRM values of <0.09 indicate good model fit (30). Next, to investigate the validity of the SIBS, its associations with positive mental health, as well as with depressive symptoms, PTSD and suicide ideation/behavior were assessed by the calculation of zero-order bivariate correlation analyses. Group differences in SIBS scores between participants with or without lifetime suicide attempts were tested using a t-test. Gender differences regarding suicidal ideation and lifetime suicide attempts were tested using a t-test and a Chi-Square Test.
Mean scores and standard deviations of all questionnaires are displayed in Table 1. In total 44.4% of the participants reported suicidal ideation within the past 4 weeks (SIBS > 0). Thirty-six participants (12.9%) reported a lifetime suicide attempt.
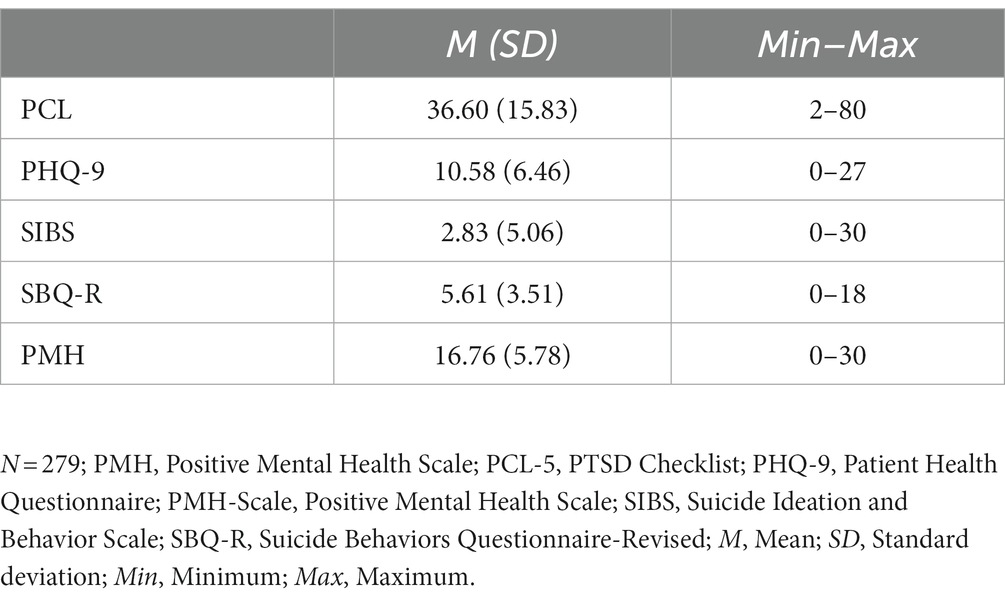
Table 1. Descriptive statistics of the investigated variables (N = 279).
The results of the Kolmogorov–Smirnov as well as the Shapiro–Wilk-test showed that the participants answers were not normally distributed (p < 0.001). These results were confirmed by the item analysis (see Table 2). Selectivity is good for all items (>0.3).
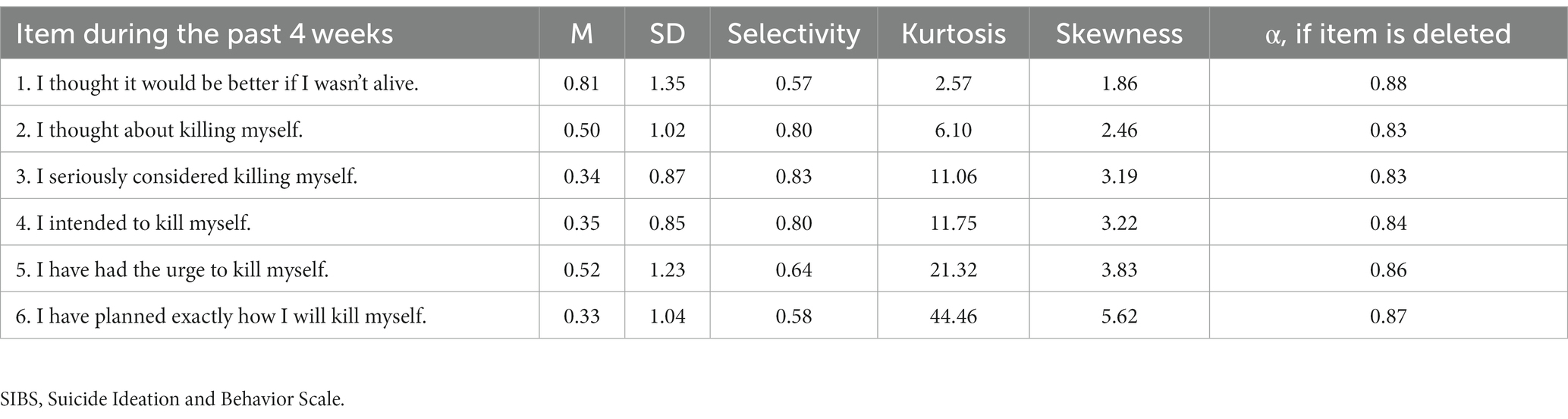
Table 2. Results of the item analysis of the SIBS (N = 279).
The one factorial model determined from the exploratory factor analysis (EFA) and subsequent principal component analysis (PCA) by Teismann et al. (14) was tested using confirmatory factor analysis (CFA). The results of the confirmatory factor analysis indicate a good global model fit: Satorra-Bentler corrected χ2 = 19.481 (df = 8, p = 0.012), CFI = 0.989, TLI = 0.980, RMSEA = 0.072 (90%-CI = 0.031–0.113) and SRMR = 0.025. Local fit was good as well, as all factor loadings were >0.60 (see Table 3).
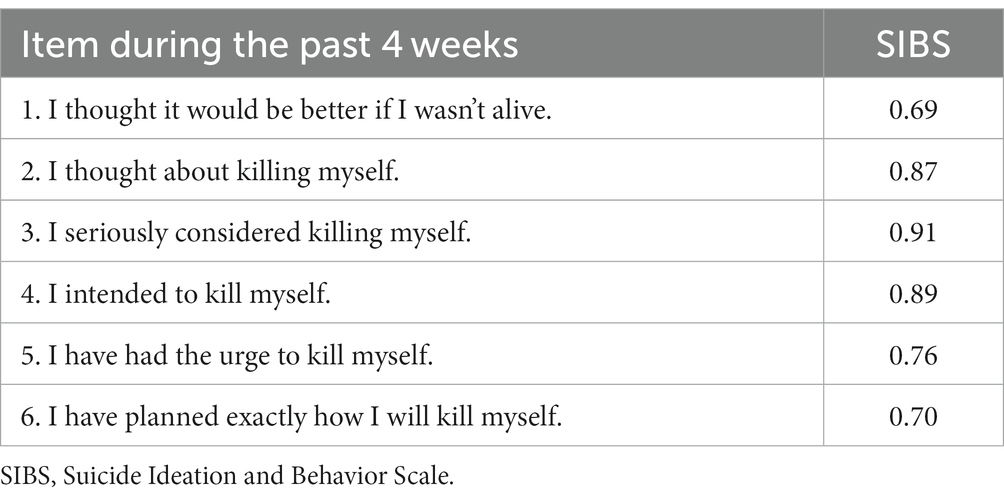
Table 3. Factor loadings of the SIBS items (N = 279).
Internal consistency was assessed using Cronbach’s α. In the current study, it was α = 0.875.
The SIBS was positively correlated with depression (r = 0.404, p 0.000), posttraumatic stress disorder symptoms (r = 0.390, p 0.000) and suicide ideation/behavior as assessed with the SBQ-R (r = 0.654, p 0.000). The SIBS was negatively correlated with positive mental health (r = −0.430, p 0.000). Men and women did neither differ in suicide ideation, t(277) = −0.397, p = 0.692, nor in lifetime suicide attempts, χ2 = 0.44, df = 1, p = 0.51. Participants with lifetime suicide attempts (n = 36) suffered from higher levels of concurrent suicidal ideation as measured by the SIBS (M = 10.583, SD = 7.911) than participants without lifetime suicide attempts (n = 243; M = 1.687, SD = 3.191), t(277) = −12.152, p 0.000.
In the present study, the reliability and construct validity as well as the postulated factor structure of the Farsi version of the Suicide Ideation and Behavior Scale (SIBS) were investigated. In line with the original version of the SIBS (14) and the version for children and adolescents (17), the Farsi version of the SIBS had a unidimensional factor structure and an excellent internal consistency. Construct validity of the SIBS was supported by expected associations between the SIBS and depressive symptoms, posttraumatic stress symptoms, suicide ideation/behavior as assessed with the SBQ-R and positive mental health. SIBS suicide ideation scores (items 1 to 6) differentiated between participants with vs. without lifetime suicide attempts. In line with previous investigations (3, 14), men and women did not differ in suicide ideation scores in the current study. Taken together, findings indicate that the Farsi version of the SIBS is a reliable and valid instrument. The SIBS also meets the following evaluation criteria—established by Batterham et al. (32)—for assessing suicidal ideation and suicidal behavior: (1) It explicitly captures suicidal ideation and suicidal behavior, (2) it is brief and easy to complete, (3) it collects quantitative data, and 4. it is available free of charge.1
However, it should be highlighted that the SIBS only assesses current suicidal ideation and behavior; with the exception of lifetime suicide attempts. Other instruments must therefore be used if information on suicidal ideation over different time periods has to be assessed. The SIBS and SBQ-R complement each other rather well in this regard and may be used in conjunction. It should also be noted that the SIBS—just as any other assessment instrument—can help to make an assessment of the severity and nature of suicide ideation and behavior; it cannot be used to predict suicidal behavior and/or suicide death or to be seen as a marker of immediate suicide risk (33, 34). In general questionnaires should only ever be used as a supplement to a more detailed conversation about suicidal ideation and behavior.
Several limitations have to be considered when interpreting the current results. First, since 100% of the sample were Afghan students, it is unclear how the findings would generalize to a more diverse Farsi speaking population and to clinical populations. Yet, with regard to suicide ideation/behavior, student populations are a group of special concern (35). Moreover, the proportion of those who affirmed suicidal ideation and suicide attempts in the present study was as large as otherwise found in clinical samples (36). It is possible that a differentiation between clinical and non-clinical samples in highly stressed societies—with low access to mental health facilities—such as Afghanistan is therefore less meaningful. Sadly, it must be emphasized that due to the fact that the Taliban banned female students from universities in December 2022 (37), a study of Afghan female students will hardly be possible in future studies. Second, the cross-sectional design of the current study precludes analyses of test–retest reliability over short periods of time. Longitudinal studies on this issue are warranted. Third, the current study utilized only self-report measures. This method has certain advantages, for example, the measures are economical and easy to administer. However, self-report measures may fail to capture suicide ideation/behavior, depressive symptoms, or post-traumatic symptoms in their full complexity. Fourth, to keep the assessment as confidential as possible [cf. (38)], only gender and age group were assessed to characterize the sample. Therefore, it is not possible to give more details on the sample composition. Finally, the questionnaire can only be used by Farsi (Persian) speakers in Iran and Afghanistan (or Persian speaking minorities in Tajikistan or Uzbekistan). The scale has not been validated for use with Afghans who speak Dari or regional dialects.
Despite these limitations, the current results suggest that the Farsi version of the SIBS is a brief, reliable, and valid measure of concurrent suicidal ideation and behavior that can be used to complement mental health assessments in research and practice. With regard to the use of the questionnaire, it should finally be emphasized that questionnaires cannot be used meaningfully for the prediction of suicidal behavior (33), that answering questions about suicidality does not instill or intensify suicidality in respondents (39), but that nevertheless—in the context of studies on suicide or suicide-associated constructs—participants must always be provided with emergency contact information (40). The latter represents a real challenge in countries such as Afghanistan, where help for mental health problems is in general only inadequately available (41).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Ethics Committee of the Faculty of Psychology, Ruhr-Universität Bochum, Germany. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
AM, AN, MA, SF, TF, HG, and TT contributed to the conception and design of the study as well as the interpretation of the data. MA conducted the acquisition of data. TF, SF, HG, and TT conducted the data analysis. AM, AN, and TT drafted a first version of the article and finalized the revised version. All authors contributed to the article and approved the submitted version.
The authors acknowledge support by the Open Access Publication Funds of the Ruhr-Universität Bochum.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hassanian-Moghaddam, H, and Zamani, N. Suicide in Iran: the facts and the Figures from Nationwide reports. Iran J Psychiatry. (2017) 12:73–7.
2. Mohammadi, MR, Ghanizadeh, A, Rahgozart, M, Noorbala, AA, Malekafzali, H, Davidian, H, et al. Suicidal attempt and psychiatric disorders in Iran. Suicide Life Threat Behav. (2005) 35:309–16. doi: 10.1521/suli.2005.35.3.309
3. Naghavi, A, Afsharzada, MS, Brailovskaia, J, and Teismann, T. Mental health and suicidality in Afghan students after the Taliban takeover in 2021. J Affect Disord. (2022) 307:178–83. doi: 10.1016/j.jad.2022.04.001
4. Sabawoon, A, Keyes, KM, Karam, E, and Kovess-Masfety, V. Associations between traumatic event experiences, psychiatric disorders, and suicidal behavior in the general population of Afghanistan: findings from Afghan National Mental Health Survey. Inj Epidemiol. (2022) 9:31. doi: 10.1186/s40621-022-00403-8
5. Haase, E, Schönfelder, A, Nesterko, Y, and Glaesmer, H. Prevalence of suicidal ideation and suicide attempts among refugees: a meta-analysis. BMC Public Health. (2022) 22:635. doi: 10.1186/s12889-022-13029-8
6. Franklin, JC, Ribeiro, JD, Fox, KR, Bentley, KH, Kleiman, EM, Huang, X, et al. Risk factors for suicidal thoughts and behaviors. Psychol Bull. (2017) 143:187–232. doi: 10.1037/bul0000084
7. Jobes, DA, and Joiner, TE. Reflections on suicidal ideation. Crisis. (2019) 40:227–30. doi: 10.1027/0227-5910/a000615
8. Vannoy, SD, and Robins, LS. Suicide-related discussions with depressed primary care patients in the USA. BMJ. (2011) 1:e000198. doi: 10.1136/bmjopen-2011-000198
9. Amini-Tehrani, M, Nasiri, M, Jalali, T, Sadeghi, R, and Zamania, H. Validation and psychometric properties of suicide Behaviors questionnaire-revised (SBQ-R) in Iran. Asian J Psychiatr. (2020) 47:101856. doi: 10.1016/j.ajp.2019.101856
10. Sahlan, RN, Grunewald, W, and Smith, AR. Validations of the Farsi versions of the depressive symptom inventory suicidality subscale (F-DSI-SS) and suicide rumination scale (F-SRS) among Iranian college students. Suicide Life Threat Behav. (2023) 53:16–28. doi: 10.1111/sltb.12917
11. Osman, A, Bagge, CL, Gutierrez, PM, Konick, LC, Kopper, BA, and Barrios, FX. The suicidal Behaviors questionnaire-revised (SBQ-R). Assessment. (2001) 8:443–54. doi: 10.1177/107319110100800409
12. Forkmann, T, Teismann, T, and Glaesmer, H. Diagnostik von Suizidalität. Göttingen: Hogrefe (2017).
13. Joiner, TE, Pfaff, JJ, and Acres, JG. A brief screening tool for suicidal symptoms in adolescents and young adults in general health settings: reliability and validity data from the Australian national general practice youth suicide prevention project. Behav Res Ther. (2002) 40:471–81. doi: 10.1016/S0005-7967(01)00017-1
14. Teismann, T, Forkmann, T, Glaesmer, H, Juckel, G, and Cwik, JC. Skala Suizidales Erleben und Verhalten (SSEV): Faktorstruktur und psychometrische Eigenschaften. Diagnostica. (2021) 67:115–25. doi: 10.1026/0012-1924/a000269
15. Chu, C, Klein, KM, Buchman-Schmitt, JM, Hom, MA, Hagan, CR, and Joiner, TE. Routinized assessment of suicide risk in clinical practice: an empirically informed update. J Clin Psychol. (2015) 71:1186–200. doi: 10.1002/jclp.22210
16. Posner, K, Brodsky, B, Yershova, K, Buchanan, J, and Mann, J. The classification of suicidal behavior In: M Nock, editor. The Oxford handbook of suicide and self-injury. Oxford: Oxford University Press (2014). 7–22.
17. Friedrich, S, Schneider, S, Forkmann, T, Glaesmer, H, and Teismann, T. Validierung der Skala Suizidales Erleben und Verhalten (SSEV-KJ) für den Einsatz bei Kindern und Jugendlichen Z. Kindheit Entwick (2023) (In press).
18. Shoib, S, Saeed, F, Dazhamyar, AR, Armiyau, AY, Badawy, MM, Shah, J, et al. Women in Afghanistan: a call for action. Lancet Psychiatry. (2022) 9:342–3. doi: 10.1016/S2215-0366(22)00039-6
19. Mehrabi, A, Naghavi, A, Afsharzada, ME, Afsharzada, MS, Brailovskaia, J, and Teismann, T. Trust in higher guidance and suicidality in Afghan students under the Taliban regime. Int J Clin Health Psychol. (2023) 23:100398. doi: 10.1016/j.ijchp.2023.100398
20. Wild, D, Grove, A, Martin, M, Eremenco, S, McElroy, S, Verjee-Lorenz, A, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. (2015) 8:94–104. doi: 10.1111/j.1524-4733.2005.04054.x
21. Blevins, CA, Weathers, FW, Davis, MT, Witte, TK, and Domino, JL. The posttraumatic stress disorder checklist for DSM-5 (PCL-5): development and initial psychometric evaluation. J Trauma Stress. (2015) 28:489–98. doi: 10.1002/jts.22059
22. Sadeghi, M, Taghva, A, Goudarzi, N, and Rah Nejat, A. Validity and reliability of Persian version of post-traumatic stress disorder scale in war veterans. Iran J War Pub Health. (2016) 8:243–9.
23. Kroenke, K, Spitzer, RL, and Williams, JB. The PHQ-9. Validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
24. Ardestani, MS, Ashtiani, RD, Rezaei, Z, Vasegh, S, and Gudarzi, SS. Validation of Persian version of PHQ-9 for diagnosis of major depressive episode in psychiatric wards in Iran. J Appl Behav Sci. (2019) 5:1–8. doi: 10.22037/ijabs.v5i2.21094
25. Lukat, J, Margraf, J, Lutz, R, van der Veld, WM, and Becker, ES. Psychometric properties of the positive mental health scale (PMH-scale). BMC Psychol. (2016) 4:8. doi: 10.1186/s40359-016-0111-x
26. Naghavi, A, Teismann, T, Asgari, Z, Eizadifard, R, and Brailovskaia, J. Validation of the Persian version of the positive mental health scale. BMC Psychiatry. (2021) 21:472. doi: 10.1186/s12888-021-03487-6
27. IBM Corporation. IBM SPSS statistics for windows, version 27.0. Armonk, NY: IBM Corporation (2020).
28. Liu, RT, Bettis, AH, and Burke, TA. Characterizing the phenomenology of passive suicidal ideation: a systematic review and meta-analysis of its prevalence, psychiatric comorbidity, correlates, and comparisons with active suicidal ideation. Psychol Med. (2020) 50:367–83. doi: 10.1017/S003329171900391X
29. Satorra, A, and Bentler, PM. A scaled difference chi-square test statistic for moment structure analysis. Psychometrika. (2001) 66:507–14. doi: 10.1007/BF02296192
30. Hu, L, and Bentler, PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. (1999) 6:1–55. doi: 10.1080/10705519909540118
31. MacCallum, RC, Widaman, KF, Zhang, S, and Hong, S. Sample size in factor analysis. Psychol Methods. (1999) 4:84–99. doi: 10.1037/1082-989X.4.1.84
32. Batterham, P, Ftanou, M, Pirkis, J, Brewer, J, Mackinnon, A, Beautrais, A, et al. A systematic review and evaluation of measures for suicidal ideation and behaviors in population-based research. Psychol Assess. (2015) 27:501–12. doi: 10.1037/pas0000053
34. Carter, G, Milner, A, McGill, K, Pirkis, J, Kapur, N, and Spittal, MJ. Predicting suicidal behaviours using clinical instruments: systematic review and meta-analysis of positive predictive values for risk scales. Br J Psychiatry. (2017) 210:387–95. doi: 10.1192/bjp.bp.116.182717
35. Mortier, P, Auerbach, RP, Alonso, J, Axinn, WG, Cuijpers, P, Ebert, DD, et al. Suicidal thoughts and behaviors among college students and same-aged peers: results from the world health organization world mental. L health surveys. Soc Psychiatry Psychiatr Epidemiol. (2018) 53:279–88. doi: 10.1007/s00127-018-1481-6
36. Bernal, M, Haro, JM, Bernert, S, Brugha, T, de Graaf, R, Bruffaerts, R, et al. Risk factors for suicidality in Europe: results from the ESEMED study. J Affect Disord. (2007) 101:27–34. doi: 10.1016/j.jad.2006.09.018
37. Neyazi, A, Padhi, B, and Sah, R, members of the Global Centre for Public Health Collaborators. Girls’ education and the future of healthcare in Afghanistan. BMJ. (2023) 380:561. doi: 10.1136/bmj.p561
38. Deming, CA, Harris, JA, Castro-Ramirez, F, Glenn, JJ, Cha, CB, Millner, AJ, et al. Inconsistencies in self-reports of suicidal ideation and attempts across assessment methods. Psychol Assess. (2021) 33:218–29. doi: 10.1037/pas0000976
39. DeCou, CR, and Schumann, ME. On the iatrogenic risk of assessing suicidality: a meta-analysis. Suicide Life Threat Behav. (2018) 48:531–43. doi: 10.1111/sltb.12368
40. Nock, MK, Kleiman, EM, Abraham, M, Bentley, KH, Brent, DA, Buonopane, RJ, et al. Consensus statement on ethical & safety practices for conducting digital monitoring studies with people at risk of suicide and related behaviors. Psychiat Res Clin Prac. (2021) 3:57–66. doi: 10.1176/appi.prcp.20200029
Keywords: suicide ideation, suicide attempts, assessment, Afghanistan, validation study
Citation: Mehrabi A, Naghavi A, Afsharzada ME, Friedrich S, Forkmann T, Glaesmer H and Teismann T (2023) Validation of the Farsi version of the Suicide Ideation and Behavior Scale. Front. Psychiatry. 14:1201193. doi: 10.3389/fpsyt.2023.1201193
Edited by:
Daniel Stjepanović, The University of Queensland, AustraliaReviewed by:
Sharon Abramowitz, Georgetown University, United StatesCopyright © 2023 Mehrabi, Naghavi, Afsharzada, Friedrich, Forkmann, Glaesmer and Teismann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tobias Teismann, dG9iaWFzLnRlaXNtYW5uQHJ1Yi5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.