 Yihan Zhang
Yihan Zhang Geng Li
Geng Li Chengzhen Liu1
Chengzhen Liu1 Zifu Shi
Zifu Shi- 1School of Educational Science, Hunan Normal University, Changsha, China
- 2College of Physical Education, Hunan Normal University, Changsha, China
Purpose: Depression disorder is the most commonly diagnosed type of mental illness among youths. Although a plethora of evidence suggests a positive relationship between exercise and lower levels of depression in youths, the findings regarding the variation in magnitude of this relationship are inconclusive with respect to the preventive and therapeutic effects of different types of exercise. This network meta-analysis aimed to determine the best type of exercise for the treatment and prevention of depression in youths.
Methods: A comprehensive search of databases, including PubMed, EMBASE, The Cochrane Library, Web of Science, PsychINFO, ProQuest, Wanfang, and CNKI, was conducted to identify relevant research on exercise interventions for depression in youth populations. The risk of bias in the included studies was evaluated using Cochrane Review Manager 5.4 according to the Cochrane Handbook 5.1.0 Methodological Quality Evaluation Criteria. The network meta-analysis was performed using STATA 15.1 to calculate the standardized mean difference (SMD) of all concerned outcomes. The node-splitting method was used to test the local inconsistency of the network meta-analysis. Funnel plots were used to evaluate the potential impact of bias in this study.
Result: Utilizing data extracted from 58 studies (10 countries, 4,887 participants), we found that for depressed youths, exercise is significantly better than usual care in reducing anxiety (SMD = −0.98, 95% CI [-1.50, −0.45]). For non-depressed youths, exercise is significantly better than usual care in reducing anxiety (SMD = −0.47, 95% CI [ −0.66, −0.29]). In the treatment of depression, resistance exercise (SMD = −1.30, 95% CI [ −1.96, −0.64]), aerobic exercise (SMD = −0.83, 95% CI [-1.10 −0.72]), mixed exercise (SMD = −0.67, 95% CI [−0.99, −0.35]), and mind-body exercise (SMD = −0.61, 95% CI [−0.84, −0.38]) all showed significant efficacy over usual care. For the prevention of depression, resistance exercise (SMD = −1.18, 95% CI [-1.65, −0.71]), aerobic exercise (SMD = −0.72, 95% CI [−0.98, −0.47]), mind-body exercise (SMD = −0.59, 95% CI [-0.93, −0.26]), and mixed exercise (SMD = −1.06, 95% CI [−1.37 to −0.75]) were all significantly effective compared to usual care. According to the test of the surface under the cumulative ranking score (SUCRA), the ranking of exercises for the treatment of depression in depressed youths is as follows: resistance exercise (94.9%) > aerobic exercise (75.1%) > mixed exercise (43.8%) > mind-body exercise (36.2%) > usual care (0%). For the prevention of depression in non-depressed youths, resistance exercise (90.3%) > mixed exercise (81.6%) > aerobic exercise (45.5%) > mind-body exercise (32.6%) > usual care (0%). Resistance exercise thus had the best comprehensive effect on both the treatment and prevention of depression in youths (clusterank value = 1914.04). Subgroup analyses show that a frequency of 3–4 times per week, a duration of 30–60 min, and a length of more than 6 weeks were found to be the most effective interventions for depression (P > 0.001).
Conclusion: This study provides compelling evidence that exercise is a viable intervention for improving depression and anxiety in young individuals. In addition, the study emphasizes the importance of selecting the appropriate type of exercise to optimize treatment and prevention. Specifically, the results suggest that resistance exercise, performed 3–4 times per week, with sessions lasting 30–60 min and a length of more than 6 weeks, yields optimal results for the treatment and prevention of depression in young individuals. These findings have significant implications for clinical practice, particularly given the challenges associated with implementing effective interventions and the economic burden of treating and preventing depression in young people. However, it is worth noting that additional head-to-head studies are necessary to confirm these findings and strengthen the evidence base. Nevertheless, this study provides valuable insights into the role of exercise as a potential treatment and preventative measure for depression in young people.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=374154, identifier: 374154.
1. Introduction
Depression is a mood disorder characterized by persistent feelings of sadness, loss of interest in activities, and other symptoms that impair daily functioning (1). It has become a significant public health issue for today's youth (2, 3). During the period of transition from adolescence to adulthood, which typically ranges from 15 to 24 years of age (4), individuals are psychologically underdeveloped and have an increased risk for depression (5, 6). The deleterious effects of depression can extend to a youth's social relationships (7) and academic performance (8) and can even lead to suicidal ideation (9). In most countries, clinical interventions for depression primarily involve psychotherapy and medication (10). However, despite the adequate implementation of such treatments, a significant portion of patients do not experience sufficient symptom relief, with 50% experiencing at least one new depressive episode after 6–12 months of treatment (11). Although psychotherapy can be effective, it can also be expensive and stigmatizing (12). In addition, despite their potential benefits, there is substantial evidence to suggest that antidepressant medications can have adverse effects including an increased risk of suicidal behavior (13) and a high rate of discontinuation among patients, with 20 to 59% discontinuing their medication within 3 weeks (14, 15). Therefore, it is crucial to implement cost-effective and robust interventions to establish recovery and prevent relapse of depression in youths.
In recent years, there has been growing interest in the use of physical exercise as a treatment for depression or as an adjunct to traditional therapies (16). In this context, “physical exercise” refers to planned, structured, repetitive, and purposeful physical activities aimed at improving or maintaining one or more of the components of physical fitness (17). Research to date has suggested that exercise has promising antidepressant effects as it increases the production of monoamines such as dopamine and serotonin, which are crucial for the treatment of depression (18–20). Exercise-induced changes in neuroplasticity and brain-derived neurotrophic factor (BDNF) may also contribute to its antidepressant effects (21). A growing body of cross-sectional studies has shown that inadequate physical activity is a significant risk factor for depression (22). For these reasons, numerous randomized controlled trials (RCTs) have been conducted and found to show that structured exercise programs can effectively alleviate depression (23, 24). For example, an 8-week aerobic exercise intervention improved depression in depressed patients by improving their cognitive control function and rumination patterns (25). Similarly, a 20-week RCT found that depression was significantly reduced by resistance training, and the effect persisted for 26 months after the end of the intervention (26). Mind-body exercise has also been found to be effective in reducing depression, anger, and fatigue (27). Moreover, mixed exercise interventions have been found to improve cardiorespiratory fitness and significantly improve depression and anxiety (28). Furthermore, systematic reviews and meta-analyses have reported moderate-to-large antidepressant effects of exercise interventions in different age groups, including children (29), adolescents (30), young adults 13), and older adults (31). Although exercise is now known to be generally beneficial for depression, different types of exercise elicit different physical mechanisms (32). It is hypothesized, therefore, that different types of exercise may have varying degrees of effectiveness in treating depression. While numerous meta-analyses have assessed the efficacy of exercise interventions, uncertainty remains over the relative efficacy of different exercise types in treating depression.
If the development of depression is uncontrolled during youth, it often becomes chronic in adulthood (33). Therefore, the early effective prevention of depression in youths is crucially important. Moreover, physical exercise has a protective effect against the development of depression (34). This is because, first, exercise may cause changes in the levels of various neurotransmitters in the brain, such as serotonin, dopamine, and norepinephrine. These neurotransmitters play important roles in regulating mood and alterations in their levels can affect the development of depression. Second, exercise can also trigger the release of endorphins, which are natural opioids produced by the body that can reduce pain and promote feelings of wellbeing and euphoria; they also play a role in preventing depression. Third, engaging in exercise can provide opportunities for social interaction and support, which can also have a positive impact on mental health and the prevention of depression. Overall, these mechanisms highlight the importance of exercise for improving the physiological and psychological factors associated with depression and suggest that exercise has both direct and indirect effects in preventing depression. While Rebars' meta-meta-analyses further support the preventive efficacy of exercise, uncertainty remains over the relative preventive efficacy of different exercise types in depression.
Anxiety is an excessive concern, unease, and fear about specific things or situations (1); it is frequently co-morbid with depression (35). Feelings of anxiety can interfere with an individual's ability to carry out daily activities and can lead to a reduced quality of life (36). In fact, anxiety and depression share many symptoms and thus can be difficult to differentiate (35). Prior studies have demonstrated that the co-occurrence of anxiety and depression is associated with a higher risk of developing more severe symptoms (37), increased rates of disability, and reduced response to treatment (38). However, several studies have demonstrated that exercise has favorable effects on anxiety (39). Individuals experiencing anxiety often report bodily tension and discomfort (36). Exercise has been shown to dissipate excess energy, alleviate muscular tension (40), and enhance metabolic processes (41), leading to a reduction in anxiety (42). While meta-analyses have found that exercise is effective in improving anxiety (39), uncertainty remains about whether exercise has different effects on anxiety in depressed vs. non-depressed youths. Therefore, it is necessary to examine the effect of exercise intervention on improving anxiety in depressed vs. non-depressed youths to scrutinize the mechanism by which exercise affects depression.
Meta-analyses have limitations when comparing multiple interventions as pooling individual trial effects may prevent such comparisons (43). However, network meta-analysis (NMA) is a commonly employed methodology to integrate evidence across multiple studies with varying interventions. By circumventing the assumption of homogeneity in treatments (44), network meta-analysis mitigates potential biases stemming from small study effects and accounts for the inherent variations in the control group. Furthermore, network meta-analysis can comprehensively rank the effectiveness of interventions on two outcomes simultaneously, which renders it a more suitable option in the current research context for evaluating the comparative efficacy of diverse types of exercise (45–47). Miller et al. (43) network meta-analysis has provided compelling evidence for the effectiveness of different exercise interventions in ameliorating depression in older adults. However, an exploration of the comparative effectiveness of different types of exercise and the comprehensive rankings of those types of exercise for the treatment and prevention of depression in youths have not yet been undertaken.
Given that this is the case, this study seeks to answer four specific research questions: (i) which type of exercise provides the best therapeutic effect for depression in youths? (ii) Which type of exercise provides the best preventive effect for depression in youths? (iii) Does exercise have a positive impact on anxiety levels in both depressed and non-depressed youths? Additionally, the study aims to investigate (iv) whether certain types of exercise can be combined for maximum therapeutic and preventive effects for depression in youths. Answering these questions could contribute to the development of more effective exercise interventions for depression and anxiety in youths.
2. Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was used to report this systematic review and network meta-analysis (48). This review was registered in the PROSPERO international prospective register of systematic reviews (CRD42022374154).
2.1. Search strategy
The authors GL and CL performed a systematic search using a search strategy based on the Cochrane Handbook of Systematic Reviews (49) and the PICOS principle.
Participants: youths aged 15–24 years.
Interventions: aerobic exercise, resistance exercise, mind-body exercise, and mixed exercise.
Comparisons: usual care including daily care, waitlist control conditions, placebo, or other social activities.
Outcomes: depression and anxiety in depressed or non-depressed youths were measured by structured clinical interviews using established diagnostic criteria and validated using above-threshold depressive symptoms screening measures. Scales for measuring depression included the Beck Depression Inventory (BDI), the Patient Health Questionnaire (PHQ-9), the Center for Epidemiologic Studies Depression Scale (CES-D), and the Hamilton Rating Scale for Depression (HAM-D). Scales for measuring anxiety included the Hamilton Anxiety Rating Scale (HAM-A), the Beck Anxiety Inventory (BAI), and the Zung Self-Rating Anxiety Scale (SAS). More information about the established diagnostic criteria and scales used in the included studies can be found in the Supplementary material.
Study: randomized controlled trials (RCTs).
The search databases included PubMed, EMBASE, The Cochrane Library, Web of Science, PsychINFO, ProQuest, Wanfang, and CNKI. The corresponding search strategies were tailored to the characteristics of each database. In order to guarantee the comprehensiveness and precision of our network meta-analysis, we did not restrict searches by year of publication or language and implemented a meticulous data acquisition methodology. Specifically, the reference lists for each coded full-text article were examined to identify additional eligible studies. We endeavored to establish communication with the corresponding authors of studies that satisfied the predetermined eligibility standards but lacked essential data in an effort to procure the requisite information. All studies included in the analysis were collected and coded in November 2022. During the search process, the lists of articles were revised and finalized based on the discussion and evaluation. The detailed search strategy, the definitions of variables, and the assumptions and simplifications used in this study are provided in the Supplementary material.
2.2. Exclusion criteria
This study excluded: (1) non-randomized controlled trials, case reports, physician experiences, book reports, and literature reviews; (2) animal studies; (3) purely descriptive studies; (4) repeated data studies; (5) studies with an unclear diagnosis of depression or other co-morbidities; (6) studies with unclear results, incomplete data, or unsuccessful contact with full-text authors; (7) studies with unclear definitions of the types of exercise included; (8) exercise combined with drug interventions.
2.3. Study selection
NoteExpress literature management software was utilized to efficiently handle the downloaded literature data by detecting duplicate titles and merging the outcomes of literature searches from the various databases. This helped to create an information database and facilitated a full-text download of the studies. Subsequently, in line with the inclusion and exclusion criteria, two researchers independently evaluated the titles and abstracts of the studies. Following this initial assessment, the researchers read the complete texts to determine whether to exclude them. Relevant information was extracted from any studies meeting the inclusion criteria. Lastly, the two researchers cross-checked their screening outcomes. Any differences found were discussed to arrive at a resolution, or a third researcher was consulted to resolve the disagreement.
2.4. Data extraction
To assess the effectiveness of exercise interventions in improving depression, we initially categorized the included studies into depressed and non-depressed groups using screening measures of the structured clinical interviews, established diagnostic criteria, and validated above-threshold depressive symptoms. For example, a score on the Beck Depression Inventory-II (BDI-II) >13 was depressed groups, while a score on the Self-rated Depression Scale (SDS) >50 was depressed groups. Subsequently, by comparing changes in depression scores between the exercise intervention group and the control group that did not receive any exercise intervention, we could determine whether the exercise intervention had a positive impact on alleviating depression.
The study extracted the following information from the literature: (1) essential details regarding the included studies such as the first author, journal, year of publication, and study title; (2) information concerning the experimental and control groups featured in each study, including the number of experimental and control groups, participants' ages, and outcome measures; (3) information about the study design and quality assessment of the included studies; (4) data on the outcomes measured; (5) information on the interventions used in the experimental group, including the type of exercise, duration, frequency, and length of the intervention.
2.5. Risk of bias in individual studies
The assessment of bias was conducted using Cochrane Review Manager 5.4 in accordance with the Methodological Quality Evaluation Criteria outlined in the Cochrane Handbook 5.1.0. The studies included in the analysis were evaluated on six metrics, including the random assignment method, allocation concealment, blinding, completeness of the outcome data, selective reporting of study results, and other sources of bias. The authenticity of the study outcome report and any other potential sources of bias were also evaluated. Each metric was categorized as having a high, low, or uncertain risk of bias. The risk of bias was evaluated qualitatively based on the descriptions provided in the included studies.
2.6. Statistical analysis
The present study utilized the “network” package in Stata 15.1 software to perform a network meta-analysis based on the frequency framework. This method efficiently handled data from multi-arm trials, enabling comprehensive comparisons across multiple interventions while maintaining statistical power and precision of the estimates (44). Given that the outcome indicators were continuous variables measured on different scales, the effect size indicators used were the standardized mean difference (SMD) and the 95% confidence interval (CI). To ensure the appropriateness of the statistical model, we assessed model fit and heterogeneity using the Q test and I2 in the forest plot, with statistical significance set at p < 0.05. The appropriate variance structure was determined from I2, with the fixed-effects model applied when I2 was < 50% and the random-effects model applied when I2 was ≥50% (50). Inconsistency in closed loops of network plots was investigated using the node-splitting method, with a loop inconsistency factor (IF) lower than or close to zero taken to indicate good agreement between direct and indirect evidence (51).
Intervention rankings were determined by comparing the surface under the cumulative ranking score (SUCRA), with a higher SUCRA value taken to indicate a higher probability of ranking (52). A two-dimensional cluster ranking plot was constructed based on the SUCRA values of different exercise types used for the treatment and prevention of depression to determine the best suitable choice for youths. Subgroup analysis and meta-regression analysis were used to explore the underlying moderators. A funnel plot was used to determine whether there was a small sample effect between the studies. Sensitivity analysis was performed to explore sources of heterogeneity, such as removing studies with a high risk of bias or evaluating the impact of different statistical models on the results (50). Overall, exploring the geometry of the treatment network and potential biases by the above methods helped to ensure the validity and reliability of the network meta-analysis results.
3. Results
3.1. Literature selection
The initial search of the literature yielded 25,804 references, of which 368 were from PubMed, 2,466 were from EMBASE, 9,013 were from The Cochrane Library, 731 were from Web of Science, 513 were from PsychINFO, 1,076 were from CNKI, 10,265 were from ProQuest, 1,372 were from Wanfang, and 43 were from citation searches. This selection was independently screened and re-screened by two researchers according to the inclusion and exclusion criteria. Ultimately, 58 articles were obtained (Figure 1).
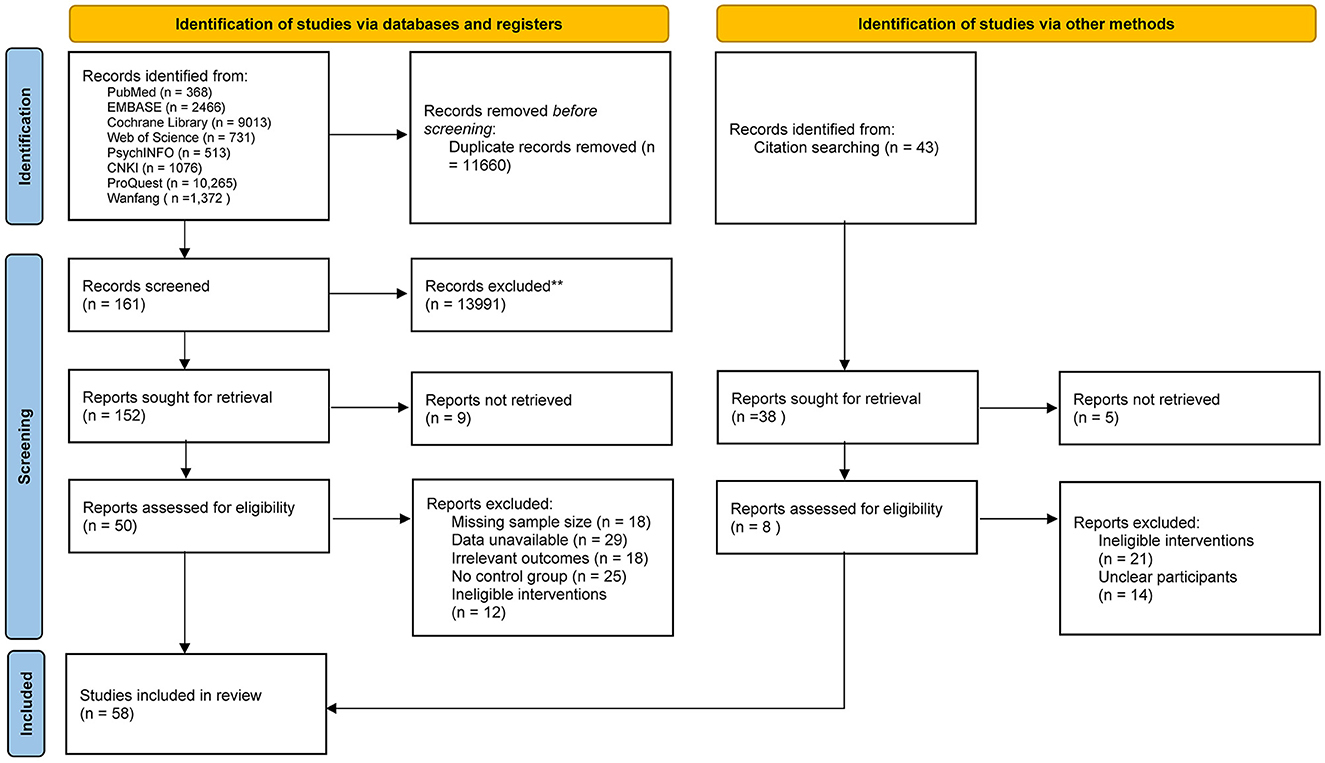
Figure 1. PRISMA flow diagram.
3.2. Characteristics of the included studies
The above-described 58 academic papers consisted of studies involving 4,887 participants from 10 distinct countries. The average age of the participants ranged from 15 to 22 years old, and they were randomly assigned to either an experimental or control group. The studies investigated the effects of four exercise interventions including aerobic, resistance, mind-body, and mixed exercises on depression and anxiety scores among depressed and non-depressed youths. More detailed information about the studies can be found in Table 1.
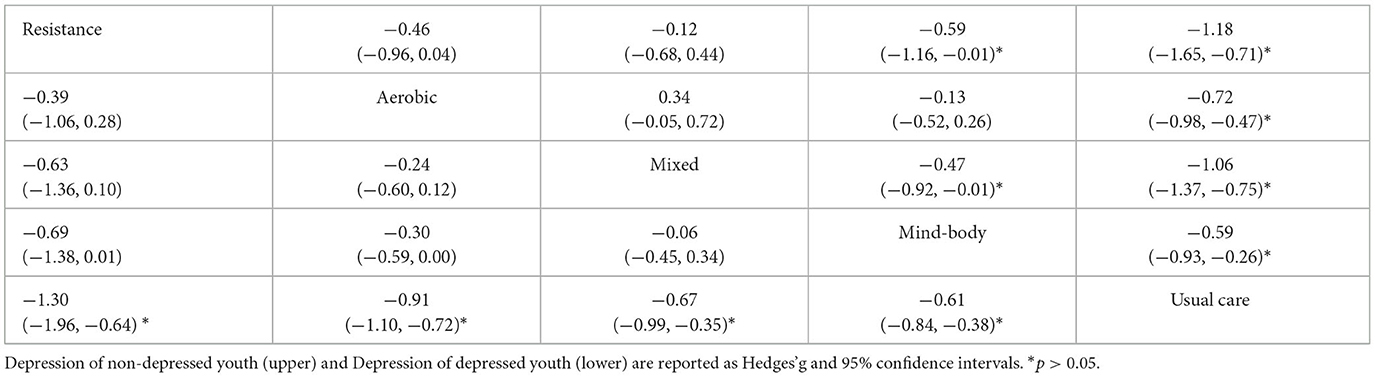
Table 1. League table for head-to-head comparisons.
3.3. Results of risk of bias assessment
Of the 58 included studies (see Figure 2), 32 studies had a low risk of bias for random sequence generation and the remaining 26 studies did not describe the allocation method in detail. Twelve studies indicated concealment of allocation. Most studies did not adopt a double-blind experimental protocol because the characteristics of the exercise intervention made it difficult to use blinding of the participants and main subjects (53). There was a low risk of bias for incomplete outcomes in 36 of the 58 studies, and detailed information on the risk of bias for the included studies is available in the Supplemental material.
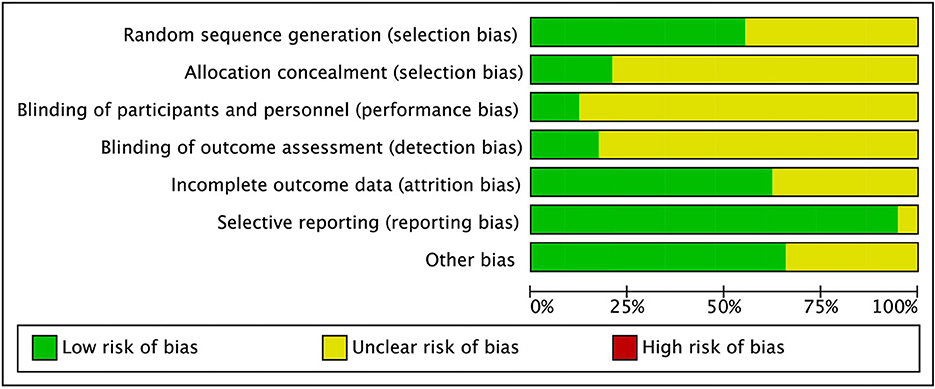
Figure 2. Risk of bias graph.
3.4. Anxiety
Due to the limited availability of studies including anxiety indicators in both depressed and non-depressed youths, only a meta-analysis was performed (see Supplemental material).
3.4.1. Anxiety in depressed youths
Three studies with a total of 316 participants, 165 in the experimental group and 151 in the control group, were included in this part of the study. The meta-analysis results showed relatively large heterogeneity with I2 = 64.8, indicating the need for a randomized model. The combined-effects result was SMD = −0.98, 95% CI [−1.50, −0.45], indicating that exercise had a significant effect on reducing anxiety in depressed youths compared to usual care.
3.4.2. Anxiety in non-depressed youths
Eleven studies with 1,352 participants, 720 in the experimental group and 632 in the control group, were included in this part of the study. The meta-analysis revealed a relatively large heterogeneity with I2 = 53.1, indicating the need for a randomized model. The combined-effects result was SMD = −0.47, 95% CI [−0.66, −0.29], indicating that exercise had a significant effect on reducing anxiety in non-depressed youths compared to usual care.
3.5. Depression
All network meta-analyses in this study share the principles of coherence, transferability, and consistency. Figure 3 presents the studies included in this study. Specifically, the size of the nodes reflects the number of participants for that type of intervention, and the thickness of the lines linking interventions reflects the number of studies that compare those interventions. Table 1 shows the head-to-head comparisons between different types of exercise and usual care. Figure 4 shows the rankings of interventions according to their likelihood of being the best choice for non-depressed or depressed youths. Figure 5 illustrates the combined benefits of different interventions in terms of their therapeutic and preventive effects.
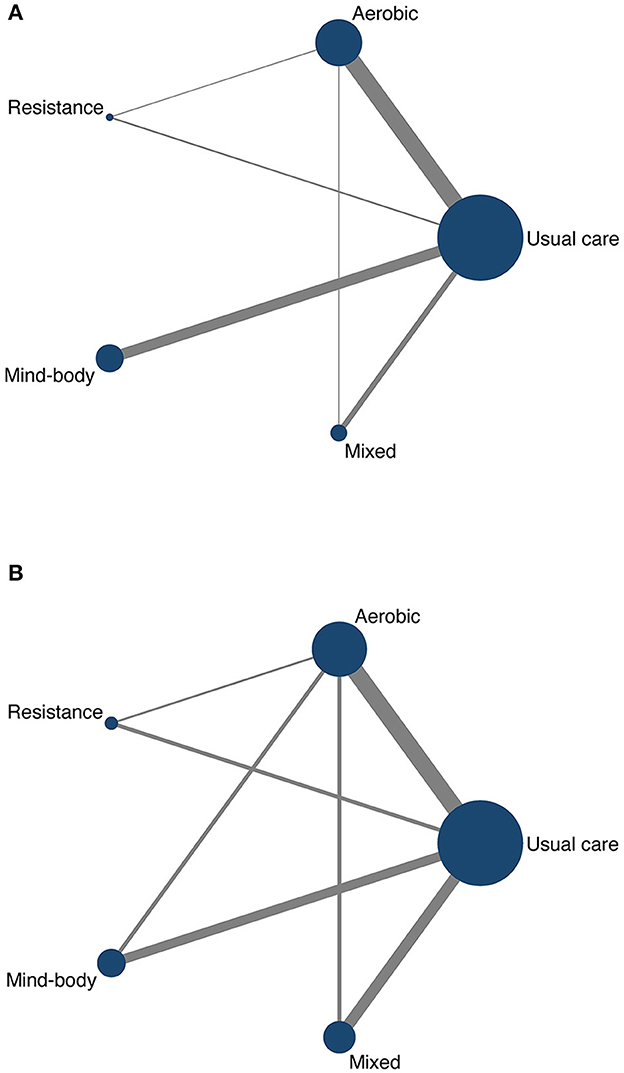
Figure 3. Network plot of depressed youths (A) and non-depressed youths (B).
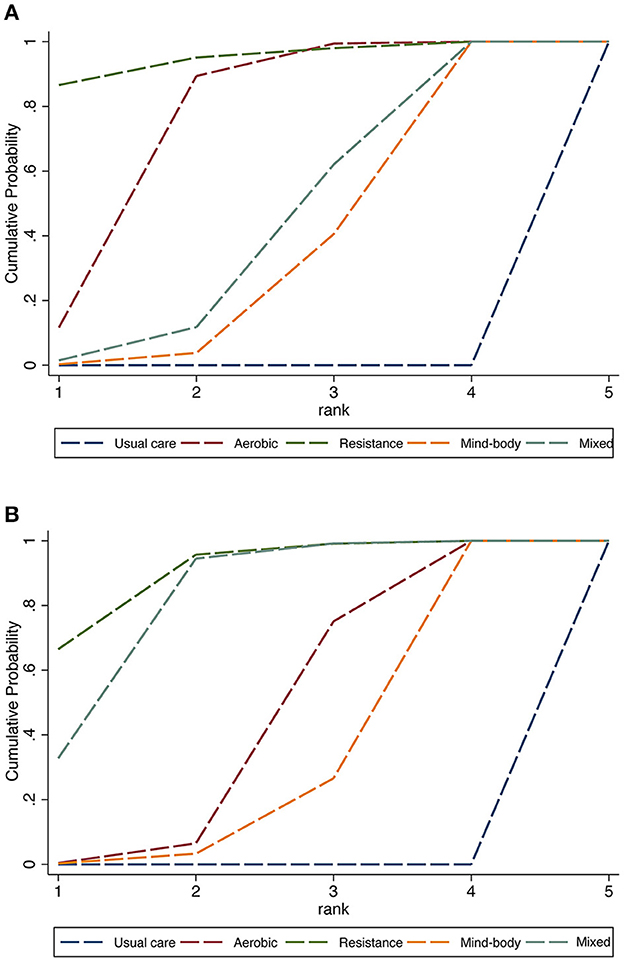
Figure 4. Rank probability of interventions in depressed youths (A) and non-depressed youths (B).
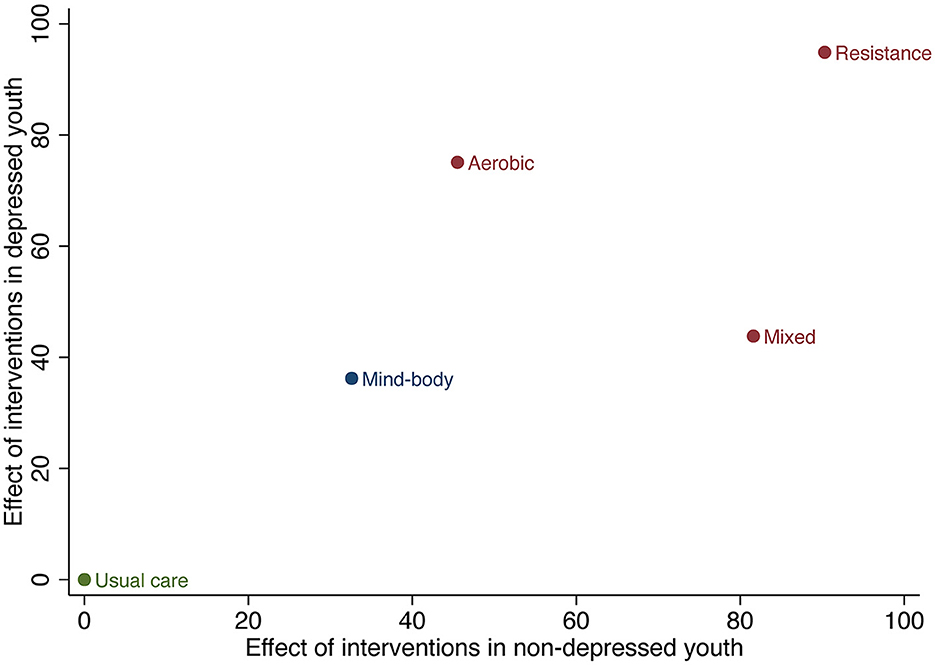
Figure 5. Two-dimensional cluster ranking plot of interventions in depressed youths and non-depressed youths.
3.5.1. Depression in depressive youths
Forty-one studies, covering 2668 participants and four types of exercise contributed to the NMA used to assess depression in depressed youths. The network relationship was centered on usual care and formed three closed loops (see Figure 3A). We performed local inconsistency tests on the closed loops using the node-splitting method; all passed the test, and thus further network meta-analysis was performed. The analysis showed IF values in the range of 0.02 to 0.33, indicating no significant inconsistency in the closed loops.
The head-to-head comparisons are shown in Table 1, where different interventions are compared individually with usual care. However, resistance exercise (SMD = −1.30, 95% CI [−1.96, −0.64]), aerobic exercise (SMD = −0.83, 95% CI [−1.10, −0.72]), mixed exercise (SMD = −0.67, 95% CI [−0.99, −0.35]), and mind-body exercise (SMD = −0.61, 95% CI [−0.84, −0.38]) were all significantly effective in decreasing depression when compared to the usual care received by the control group. Finally, the area under the SUCRA was used to rank the four exercise intervention types and usual care. As can be seen in Figure 4A, the results show that resistance exercise (94.9%) > aerobic exercise (75.1%) > mixed exercise (43.8%) > mind-body exercise (36.2%) > usual care (0%).
3.5.2. Depression in non-depressed youths
Seventeen studies, covering 2219 participants and four types of exercise contributed to the NMA assessing the depression level in non-depressed youths. The network relationship was centered on usual care and formed four closed loops, as shown in Figure 3B. We performed the local inconsistency test on the closed loops using the node-splitting method; all passed the test, and thus further network meta-analysis was performed. The results of the analysis showed that the lower limit of 95% CI for all closed loops was zero, indicating that there was no significant inconsistency between the closed loops.
The head-to-head comparisons can be seen in Table 2, where different interventions are individually compared with usual care. Overall, resistance exercise (SMD = −1.18, 95% CI [−1.65, −0.71]), aerobic exercise (SMD = −0.72, 95% CI [-0.98, −0.47]), mixed exercise (SMD = −1.06, 95% CI [-1.37, −0.75]), and mind-body exercise (SMD = −0.59, 95% CI [-0.93, −0.26]) were all significantly effective in decreasing depression when compared to the usual care received by the control group. Finally, SUCRA was used to rank the four types of exercise intervention and usual care. As can be seen in Figure 4B, resistance exercise (90.3%) > mixed exercise (81.6%) > aerobic exercise (45.5%) > mind-body exercise (32.6%) > usual care (0%).
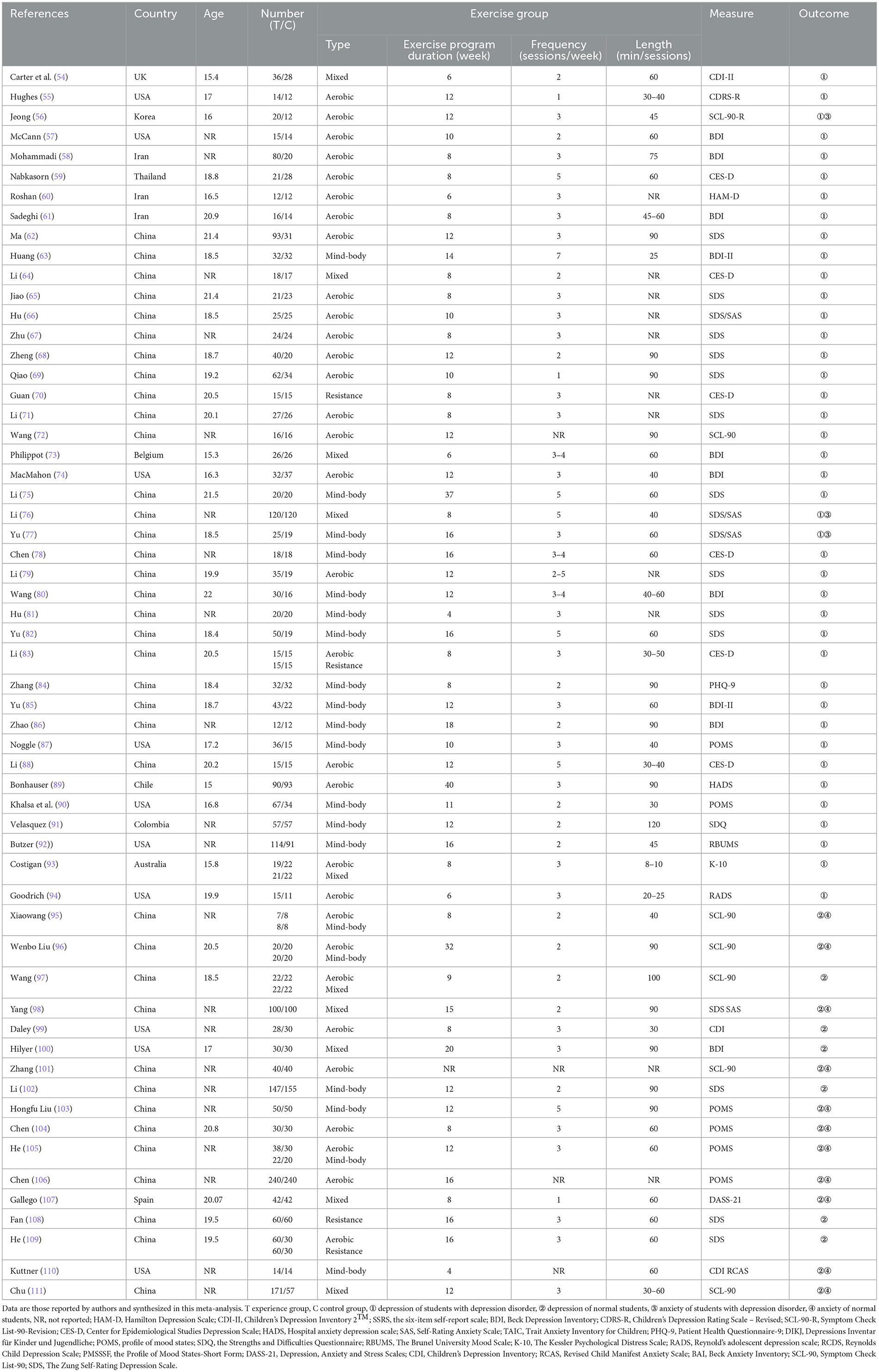
Table 2. Characteristics of included studies.
3.5.3. The combined effect of treatment and prevention for depression
The two-dimensional cluster ranking plot in Figure 5 illustrates the overall therapeutic and preventive effects of various interventions on depression in youths. Based on these results, resistance exercise appears to be the most suitable type of exercise for depression in youths, surpassing other exercise types and usual care in terms of both its therapeutic and preventive effects (cluster ranking value: 1914.04).
3.6. Moderators of effectiveness: meta-regression and subgroup analysis
Meta-regression (Table 3) showed that there was no statistically significant association between the study characteristics (year, age, country, number of participants, and measurement tools) and intervention effectiveness for depression (p > 0.05). Table 4 provides the results of the subgroup analyses. However, the frequency, duration, and length of the interventions were found to be influential features (p > 001).
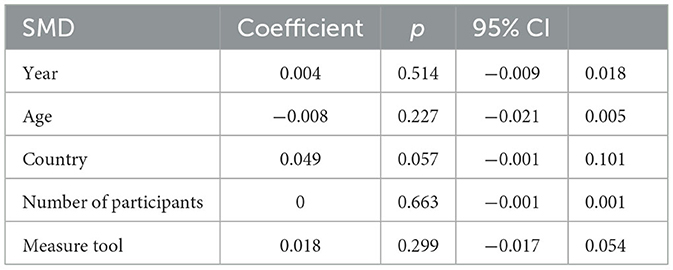
Table 3. Random–effects meta regression of SMD according to publication year, age, country, number of participants and measure tool.
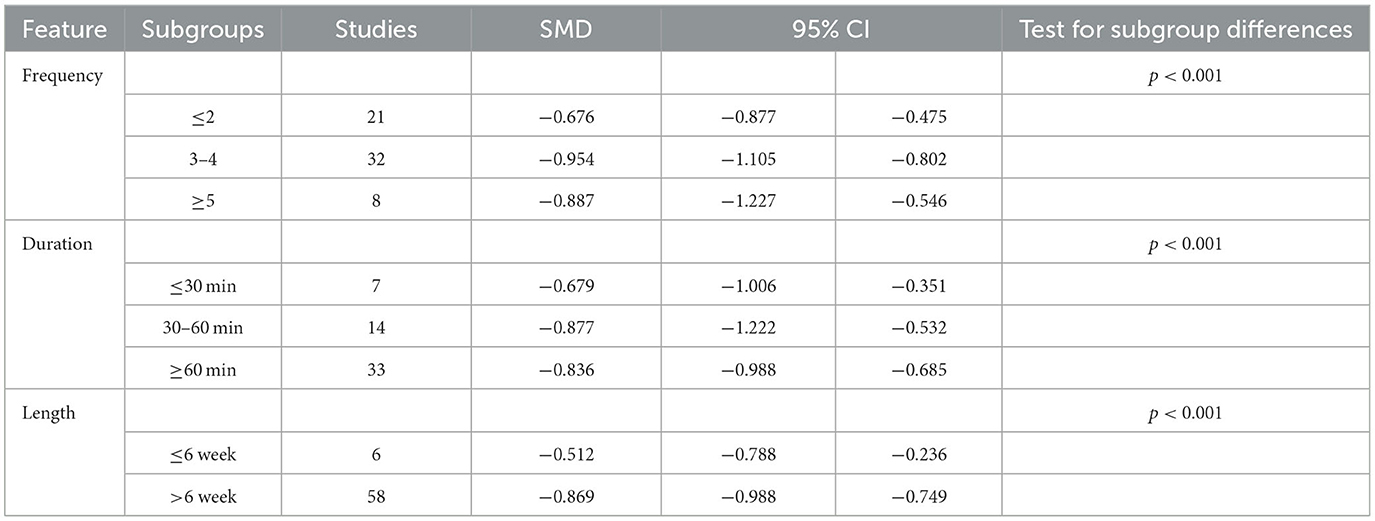
Table 4. Subgroup analysis of SMD according to frequency, session duration and program duration.
3.7. Publication bias
We conducted publication bias tests for each indicator used to assess the validity of our study's findings. Figure 6 shows that the studies were symmetrically dispersed and evenly distributed on both sides of the midline although several studies fell outside the funnel. The latter fact indicates some impact on the outcomes of the corresponding indicators and suggests the possibility of a publication bias or a small sample effect. Therefore, we conducted a screen-by-exclusion sensitivity analysis and discovered that all the data remained unaltered, suggesting some degree of stability for the study's findings.
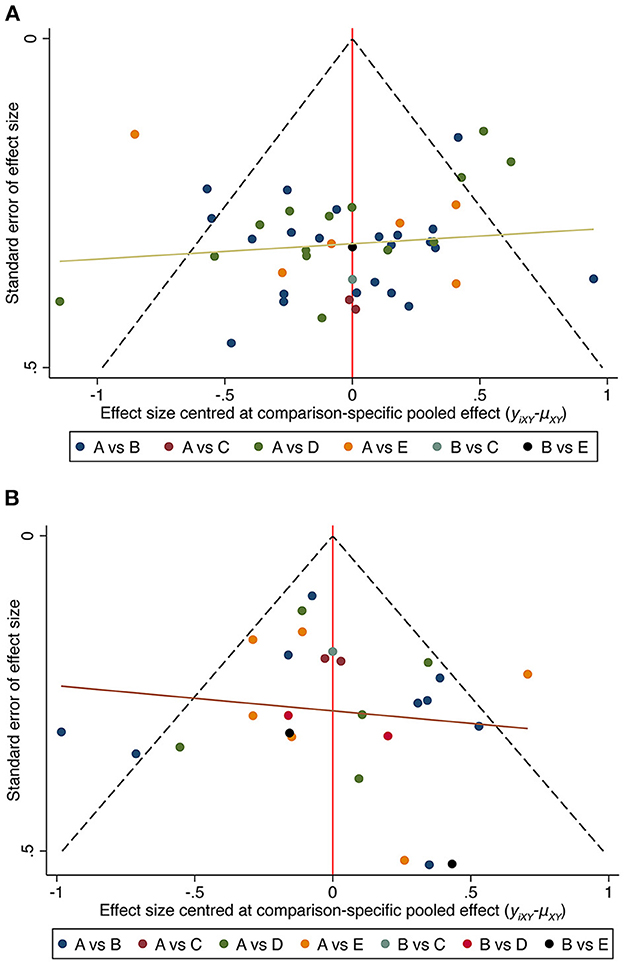
Figure 6. Funnel plots of interventions in depressed youths (A) and non-depressed youths (B). A, Usual care; B, Aerobic exercise; C, Resistance exercise; D, Mind-body exercise; E, Mixed exercise.
4. Discussion
The current study employed both meta-analysis and network meta-analysis to investigate the preventive and therapeutic effects of various types of exercise on depression and anxiety in youths. Exercise interventions were found to be significantly superior to usual care in both depressed and non-depressed youths. Further analysis of the combined therapeutic and preventive effects of different types of exercise for depression in youths revealed that resistance exercise is the most advantageous of the various exercise types. This study also found that interventions of 3–4 times per week, with a duration of 30–60 min, and a program length of more than 6 weeks were the most effective for depression interventions in youths.
The first result indicates a significant improvement in anxiety among both non-depressed and depressed youths through exercise intervention, compared to usual care. This is consistent with previous meta-analyses that have evaluated the impact of exercise interventions on anxiety across all age groups, which reported that exercise interventions can be equally as effective as medication interventions (112). Exercise appears to have neurobiological effects on several neural mechanisms that are related to anxiety (113, 114). In particular, mildly psychologically stressful stimuli may result in an attenuated glucocorticoid response, which may manifest as anxious behavior in novel situations. Exercise interventions may mitigate anxiety by influencing the hypothalamic-pituitary-adrenal axis and reducing the glucocorticoid response to stressful stimuli (112, 113). However, it is important to acknowledge that the effects of exercise can differ based on developmental stages related to age. Childhood and adulthood are marked by significant biological, psychological, and psychosocial transformations, as described by Carter et al. (115). Our study addresses the lack of focus on youth populations in prior research and provides evidence supporting the positive impact of exercise on anxiety reduction in youths.
The second finding of our study reveals that a range of exercise types when compared to usual care have significant therapeutic and preventive effects on depression in youths. This suggests that all types of exercise are effective measures for treating and preventing depression, and the findings may be generalizable to both depressed youths and non-depressed youths. Our results are consistent with those of other meta-analyses that investigated the therapeutic effects of exercise on depressed youths (115–117). The positive impact of exercise on depression can be explained through a single theory that appears to be limited in its scope, given the complex interactions involved between psychological and neurophysiological mechanisms (118). Low self-esteem is a predictor of depression in youths (119), and an increase in physical activity is associated with an increase in self-esteem (120, 121). Regular exercise may enhance an individual's self-esteem and alleviate depression by evoking positive feedback from others (20). Furthermore, abnormal oxidative stress is one of the primary causes of depression (122), and exercise can effectively improve oxidative stress (123). Our study not only addresses the lack of research focusing on non-depressed youth populations, but it also employs an innovative use of network meta-analysis to further investigate the effects of different exercise types in treating and preventing depression.
The third result is that resistance exercise is the most effective type of exercise intervention for the comprehensive treatment and prevention of depression in youths. This differs from the results reported by Miller et al. (43), who used the same network meta-analysis method but with older adults as a research object to determine the most effective intervention among different exercise types. The difference in our findings may be due to the physical condition of older adults, who prefer mind-body exercises with low intensity to improve depression (124, 125). The effects of resistance exercise on depression are unlikely to be due to a single, simple process given the complexity of both resistance exercises and mental health (29, 126). A range of biological, psychological, and social factors are plausible reasons for the benefits of exercise in alleviating depression. One possible biological explanation is that resistance exercise, being high-frequency and short-duration, triggers an increase in serum BDNF, promoting central neurotransmitter release and thereby effectively improving depression (127). Furthermore, resistance exercise exerts an anti-inflammatory effect by down-regulating pro-inflammatory markers such as TNF-α and IL-1β mRNA, which have been implicated in depression (128). By contrast, one likely psychological explanation is self-efficacy, a central concept in Bandura et al. (129) social cognitive theory, as successful experiences can increase an individual's self-efficacy and thereby decrease the likelihood of depression and anxiety (119). Specifically, strength is a very significant indicator because increasing strength resulting from resistance exercise is clearly perceptible, whereas improvements in speed and endurance may be less noticeable (130). Consistent with this, prior studies have found that increasing strength is positively related to self-efficacy (131) and inversely related to depression (132). Therefore, resistance exercise can improve inhibition deficits and insufficient pleasure by producing more psychologically positive feedback and counteracting negative emotions (133–135). This study bridges a research gap involving youth populations and includes depressed and non-depressed youths to consider the therapeutic and preventive effects of different types of exercise, supporting the use of resistance exercise as the optimal type of exercise intervention in both depressed and non-depressed youths.
The fourth result shows that the frequency, duration, and length of the interventions are the moderators of their effectiveness. First, we found that interventions carried out 3–4 times per week were more effective in improving depression in youths when compared to interventions conducted <2 times per week or more than 5 times per week. This finding agrees with those of Giles et al. (136), who used the exercise intervention to investigate the improvement of major depressive disorder in youths. Regular exercise can provide a sense of routine and structure, and these may be particularly beneficial for individuals with depression, who may struggle with feelings of disorganization or lack of purpose (137). However, too much exercise may lead to physical and mental health problems such as overuse injuries, burnout, and increased stress (138). Second, exercise interventions of 30–60 min duration were associated with greater improvements in depression than shorter sessions. This finding is consistent with previous meta-analyses that have evaluated the impact of exercise interventions in people without clinical depression across all age groups (139). One possible reason for this is that longer exercise sessions may lead to a greater increase in body temperature, which can stimulate the production of hormones and neurotransmitters involved in mood regulation (140). However, research also suggests that the number of endorphins released during exercise is proportional to the duration of the exercise (141). Thus, shorter exercise duration in a session, such as <30 min, may not provide enough stimulus to trigger a significant release of endorphins, and this could limit the mood-enhancing effects of exercise (142). Meanwhile, longer exercise durations, such as more than 1 h, may be more difficult to maintain over time due to scheduling conflicts, time constraints, or other factors, and this can lead to a decrease in compliance (143). Third, interventions that were longer in terms of the overall length of the exercise program were found to be more effective in decreasing depression than those that were shorter in length. Studies have shown that regular exercise can lead to physiological adaptations that improve cardiovascular health, increase the release of endorphins, and reduce stress levels (144). However, these adaptations may take some time to occur. Meanwhile, exercise programs that involve group or supervised sessions may provide opportunities for social support, which has been shown to be a protective factor for mental health (145). Longer exercise programs may provide more opportunities for individuals to develop supportive relationships with other participants or with exercise professionals (146), and this could, in turn, contribute to greater improvements in depression. This study bridges a gap in the lack of research focusing on youth populations and depression to consider the specific exercise setting during the intervention.
Overall, resistance exercise interventions with a frequency of 3–4 times per week, session duration of 30–60 min, and more than 6 weeks in length were associated with the greatest improvements in depression. This suggests that exercise interventions with these specific characteristics may be more effective in reducing depression than interventions with different exercise types, frequencies, session durations, or program lengths. This highlights the importance of carefully considering the design and implementation of exercise interventions for individuals with depression and suggests that interventions with these specific characteristics may be a promising avenue for future research and clinical practice.
4.1. Practical implications
This study has significant practical implications for schools regarding the development of physical education curricula for youths that would promote the prevention and treatment of depression. It is well-established that patients with mild to moderate depression often refuse treatment due to the associated stigma and high costs and side effects of medication, which may exacerbate their depression and increase the likelihood of recurrence and suicidal behavior (147). The results of this study rank different types of exercise in terms of their efficacy for the treatment and prevention of depression, offering valuable guidance for school psychological counselors and administrators. As youths spend a significant portion of their social lives in school, the school environment presents a unique opportunity for effective intervention in stress and anger management. Moreover, schools possess the necessary infrastructure for implementing both prevention and treatment programs. Therefore, the inclusion of resistance exercises in daily physical education curricula may not only prevent depression in youths but also circumvent the associated stigma of treatment for depressed youths. Such an approach promises greater compliance and improved treatment outcomes.
4.2. Limitations and future directions
We recognize that this study has several limitations. (1) We only combined all relevant studies and explored the differences of effects in the treatment or prevention of depression between different exercise types by a network meta-analysis. Future studies should further explore the mechanisms of their effects. (2) There was a lack of investigation of youths' adherence to different types of exercise interventions. Future research should assess adherence to different exercise interventions in order to determine the optimal exercise type under the consideration of a combined effect. (3) The majority of studies included in this analysis were of low quality, relying on self-reported outcomes measured through scales, and only a few provided clear details on blinded outcome assessment and allocation concealment. This is in line with previous meta-analyses conducted by Wang et al. (124), McDermott et al. (148), and Larun et al. (149). Despite the efforts made in this study to enhance the robustness of the results by including more eligible studies, there is still a need for more studies in the field that adhere to the highest methodological standards and use clinical diagnosis. (4) The clinical presentation of somatic disturbances, characterized by decreased cognitive function, diminished interest, and impaired motor activity, is commonly observed in patients with moderate to severe depression (150). Consequently, individuals with depression have significant differences in their physical motor capabilities compared to those without (151). Specifically, depressed youths exhibit a heightened susceptibility to fatigue during physical activity (152), and a negative correlation exists between youths' motor proficiency and physical fitness and their depression severity (153). Therefore, there is an urgent need for comprehensive investigations and personalized interventions to facilitate exercise participation among depressed youths. (5) Some of the studies included in our analysis did not report key data or used different outcome measures, limiting our ability to perform a more comprehensive meta-analysis. Therefore, we must emphasize the importance of standardized reporting in future studies to facilitate more comprehensive meta-analyses. Standardization of outcome measures and data reporting will increase the quality and comparability of research findings, ultimately leading to more robust and generalizable conclusions. (6) While this study focused on the immediate effects of exercise interventions, it is possible that the benefits may diminish over time without continued support or reinforcement. Future studies could examine the impact of follow-up interventions or ongoing support on long-term effectiveness. Additionally, exploring any factors that may influence adherence to follow-up interventions could also be valuable for optimizing sustainability. Despite these limitations, this study is the first to explore the treatment and prevention effects of different types of exercise for depression in youths.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
ZS and YiZ conceived the study design, collected, analyzed the data, and drafted the manuscript. GL and CL participated in the study design, collected, and analyzed data. YuZ and JG assisted in revising the manuscript, reviewed the first, and final versions of the manuscript. All authors contributed to this article and agreed to the submitted version of the manuscript.
Funding
This work was supported by the Ministry of Education Research Project of the Department of Higher Education (No. 202102389009), Scientific Research Fund of Hunan Provincial Education Department (No. 21A0061), and Hunan Province College Students Research Learning and Innovative Experiment Project (S202210542164).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1199510/full#supplementary-material
References
1. APA. Diagnostic and Statistical Manual of Mental Disorders: DSM-5™. New York, NY: American Psychiatric Publishing, Inc (2013).
2. Potrebny T, Wiium N, Lundegård MMI. Temporal trends in adolescents' self-reported psychosomatic health complaints from 1980-2016: a systematic review and meta-analysis. PLoS ONE. (2017) 12:e0188374. doi: 10.1371/journal.pone.0188374
3. Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. (2012) 380:2163–96. doi: 10.1016/S0140-6736(12)61729-2
4. Lamb MR, Fayorsey R, Nuwagaba-Biribonwoha H, Viola V, Mutabazi V, Alwar T, et al. High attrition before and after ART initiation among youth (15–24 years of age) enrolled in HIV care. AIDS. (2014) 28:559. doi: 10.1097/QAD.0000000000000054
5. Kaufman J, Martin A, King RA, Charney D. Are child-, adolescent-, and adult-onset depression one and the same disorder? Biol psychiatry. (2001) 49: 980. doi: 10.1016/S0006-3223(01)01127-1
6. Pine DS, Cohen P, Gurley D, Brook J, Ma Y. The risk for early-adulthood anxiety and depressive disorders in adolescents with anxiety and depressive disorders. Arch Gen Psychiatry. (1998) 55:56–64. doi: 10.1001/archpsyc.55.1.56
7. Guberman C, Manassis K. Symptomatology and family functioning in children and adolescents with comorbid anxiety and depression. J Can Acad Child Adolescent Psychiatry. (2011) 20:186.
8. Lundy SM, Silva GE, Kaemingk KL, Goodwin JL, Quan SF. Cognitive functioning and academic performance in elementary school children with anxious/depressed and withdrawn symptoms. Open Pediatr Med J. (2010) 4:1. doi: 10.2174/1874309901004010001
9. World Health Organization. The World health Report: 2001 Mental Health: New Understanding, New Hope. Geneva: World Health Organization. (2001).
10. Bailey AP, Hetrick SE, Rosenbaum S, Purcell R, Parker AG. Treating depression with physical activity in adolescents and young adults: a systematic review and meta-analysis of randomised controlled trials. Psychol Med. (2018) 48:1068–83. doi: 10.1017/S0033291717002653
11. Bahr R. Aktivitetshåndboken. Fysisk Aktivitet i Forebygging og behandling: Helsedirektoratet (2009).
12. Helsedirektoratet. Nasjonale Retningslinjer for Diagnostisering og Behandling av Voksne Med Depresjon i Primær- Og Spesialisthelsetjenesten. (2009), 15–1561.
13. Cipriani A, Zhou X, Del Giovane C, Hetrick SE, Qin B, Whittington C, et al. Comparative efficacy and tolerability of antidepressants for major depressive disorder in children and adolescents: a network meta-analysis. Lancet. (2016) 388:881–90. doi: 10.1016/S0140-6736(16)30385-3
14. Lawlor DA, Hopker SW. The effectiveness of exercise as an intervention in the management of depression: systematic review and meta-regression analysis of randomised controlled trials. BMJ. (2001) 322:763. doi: 10.1136/bmj.322.7289.763
15. Thomson J, Rankin H, Ashcroft GW, Yates CM, McQueen JK, Cummings SW, et al. The treatment of depression in general practice: a comparison of L-tryptophan, amitriptyline, and a combination of L-tryptophan and amitriptyline with placebo. Psychol Med. (1982) 12:741–51. doi: 10.1017/S0033291700049047
16. Wunram HL, Hamacher S, Hellmich M, Volk M, Jänicke F, Reinhard F, et al. Whole body vibration added to treatment as usual is effective in adolescents with depression: a partly randomized, three-armed clinical trial in inpatients. Eur Child Adolescent Psychiatry. (2018) 27:645–62. doi: 10.1007/s00787-017-1071-2
17. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. (1985) 100:126–31.
18. Kvam S, Kleppe CL, Nordhus IH, Hovland A. Exercise as a treatment for depression: A meta-analysis. J Affect Disord. (2016) 202:67–86. doi: 10.1016/j.jad.2016.03.063
19. Greenwood BN, Fleshner M. Exercise, learned helplessness, and the stress-resistant brain. Neuromol Med. (2008) 10:81–98.
20. Dishman RK, Hales DP, Pfeiffer KA, Felton GA, Saunders R, Ward DS, et al. Physical self-concept and self-esteem mediate cross-sectional relations of physical activity and sport participation with depression symptoms among adolescent girls. Health Psychol. (2006) 25:396–407. doi: 10.1037/0278-6133.25.3.396
21. Russo-Neustadt AA, Beard RC, Huang YM, Cotman CW. Physical activity and antidepressant treatment potentiate the expression of specific brain-derived neurotrophic factor transcripts in the rat hippocampus. Neuroscience. (2000) 101:305–12. doi: 10.1016/s0306-4522(00)00349-3
22. Stubbs B, Koyanagi A, Schuch FB, Firth J, Rosenbaum S, Veronese N, et al. Physical activity and depression: a large cross-sectional, population-based study across 36 low-and middle-income countries. Acta Psychiatr Scand. (2016) 134:546–56. doi: 10.1111/acps.12654
23. Bruin D, van der Zwan EIJE, Bögels SM. A RCT comparing daily mindfulness meditations, biofeedback exercises, and daily physical exercise on attention control, executive functioning, mindful awareness, self-compassion, and worrying in stressed young adults. Mindfulness. (2016) 7:1182–92. doi: 10.1007/s12671-016-0561-5
24. Doose M, Ziegenbein M, Hoos O, Reim D, Stengert W, Hoffer N, et al. Self-selected intensity exercise in the treatment of major depression: a pragmatic RCT. Int J Psychiatry Clin Pract. (2015) 19:266–75. doi: 10.3109/13651501.2015.1082599
25. Olson RL, Brush CJ, Ehmann PJ, Alderman BL. A randomized trial of aerobic exercise on cognitive control in major depression. Clin Neurophysiol. (2017) 128:903–13. doi: 10.1016/j.clinph.2017.01.023
26. Singh NA, Clements KM, Singh MAF. The efficacy of exercise as a long-term antidepressant in elderly subjects: a randomized, controlled trial. The J Gerontol Biol Sci Med Sci. (2001) 56:M497–504. doi: 10.1093/gerona/56.8.M497
27. Felver JC, Butzer B, Olson KJ, Smith IM, Khalsa SBS. Yoga in public school improves adolescent mood and affect. Contemp School Psychol. (2015) 19:184–92. doi: 10.1007/s40688-014-0031-9
28. Wu MH, Lee CP, Hsu SC, Chang CM, Chen CY. Effectiveness of high-intensity interval training on the mental and physical health of people with chronic schizophrenia. Neuropsychiatr Dis Treatment. (2015) 27:1255–1263. doi: 10.2147/NDT.S81482
29. Axelsdottir B, Biedilæ S, Sagatun Å, Nordheim LV, Larun L. Exercise for depression in children and adolescents–a systematic review and meta-analysis. Child Adolesc Ment Health. (2021) 26:347–56. doi: 10.1111/camh.12438
30. Oberste M, Medele M, Javelle F, Lioba Wunram H, Walter D, Bloch W, et al. Physical activity for the treatment of adolescent depression: a systematic review and meta-analysis. Front Physiol. (2020) 11:185. doi: 10.3389/fphys.2020.00185
31. Bridle C, Spanjers K, Patel S, Atherton NM, Lamb SE. Effect of exercise on depression severity in older people: systematic review and meta-analysis of randomised controlled trials. Br J Psychiatry. (2012) 201:180–5. doi: 10.1192/bjp.bp.111.095174
32. McGee SL, Hargreaves M. Exercise adaptations: molecular mechanisms and potential targets for therapeutic benefit. Nature Rev Endocrinol. (2020) 16:495–505. doi: 10.1038/s41574-020-0377-1
33. Clayborne ZM, Varin M, Colman I. Systematic review and meta-analysis: adolescent depression and long-term psychosocial outcomes. J Am Acad Child Adolesc Psychiatry. (2019) 58:72–9. doi: 10.1016/j.jaac.2018.07.896
34. Martinsen EW. Physical activity in the prevention and treatment of anxiety and depression. Nord J Psychiatry. (2008) 62:25–9. doi: 10.1080/08039480802315640
35. Schoevers RA, Deeg DJ, van Tilburg W, Beekman AT. Depression and generalized anxiety disorder: co-occurrence and longitudinal patterns in elderly patients. Am J Geriatr Psychiatry. (2005) 13:31–9. doi: 10.1097/00019442-200501000-00006
36. Nechita D, Nechita F, Motorga R. A review of the influence the anxiety exerts on human life. Rom J Morphol Embryol. (2018) 59:1045–51.
37. Hirschfeld RM. The comorbidity of major depression and anxiety disorders: recognition and management in primary care. Prim Care Companion J Clin Psychiatry. (2001) 3:244. doi: 10.4088/PCC.v03n0609
39. McDowell CP, Dishman RK, Gordon BR, Herring MP. Physical activity and anxiety: a systematic review and meta-analysis of prospective cohort studies. Am J Prev Med. (2019) 57:545–56. doi: 10.1016/j.amepre.2019.05.012
40. Rosales LM, Schneditz D, Chmielnicki H, Shaw K, Levin NW. Exercise and extracorporeal blood cooling during hemodialysis. ASAIO J. (1998) 44:M574–8. doi: 10.1097/00002480-199809000-00053
41. Hargreaves M, Spriet LL. Skeletal muscle energy metabolism during exercise. Nature Metabolism. (2020) 2:817–28. doi: 10.1038/s42255-020-0251-4
42. Stonerock GL, Hoffman BM, Smith PJ, Blumenthal JA. Exercise as treatment for anxiety: systematic review and analysis. Ann Behav Med. (2015) 49:542–56. doi: 10.1007/s12160-014-9685-9
43. Miller KJ, Goncalves-Bradley DC, Areerob P, Hennessy D, Mesagno C, Grace F, et al. Comparative effectiveness of three exercise types to treat clinical depression in older adults: a systematic review and network meta-analysis of randomised controlled trials. Ageing Res Rev. (2020) 58:100999. doi: 10.1016/j.arr.2019.100999
44. Zhang T, Song Y. Application of Stata software network group command in reticulated Meta-analysis. Chin J Evid Based Med. (2015) 11:1352–6.
46. Salanti G, Higgins JP, Ades AE, Ioannidis JP. Evaluation of networks of randomized trials. Stat Methods Med Res. (2008) 17:279–301. doi: 10.1177/0962280207080643
47. Caldwell DM, Ades AE, Higgins JPT. Simultaneous comparison of multiple treatments: combining direct and indirect evidence. BMJ. (2005) 331:897–900. doi: 10.1136/bmj.331.7521.897
48. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:1–11. doi: 10.1186/s13643-021-01626-4
49. Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions. London: John Wiley and Sons. (2019).
50. Ma J, Liu Y, Zhong LP. Application and comparison of the Jadad Scale and the cochrane risk of bias assessment tool in the quality assessment of randomized controlled trials. Chin J Oral Maxillof Surg. (2012) 10:417.
51. Chao Z, Jinzhu Y, Feng S, Qing L, Yi G, Xiantao Z. Identification and treatment methods for consistency of reticulated Meta-analysis. Chinese J Evid Based Med. (2014) 7:884–8.
52. Salanti G, Ades AE, Ioannidis JP. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J Clin Epidemiol. (2011) 64:163–71. doi: 10.1016/j.jclinepi.2010.03.016
53. Chen J, Han B, Wu C. On the superiority of a combination of aerobic and resistance exercise for fibromyalgia syndrome: A network meta-analysis. Front Psychol. (2022) 13:949256–949256. doi: 10.3389/fpsyg.2022.949256
54. Carter T, Guo B, Turner D, Morres I, Khalil E, Brighton E, et al. Preferred intensity exercise for adolescents receiving treatment for depression: a pragmatic randomised controlled trial. BMC Psychiatry. (2015) 15:1–12. doi: 10.1186/s12888-015-0638-z
55. Hughes CW, Barnes S, Barnes C, Defina LF, Nakonezny P, Emslie GJ. Depressed Adolescents Treated with Exercise (DATE): A pilot randomized controlled trial to test feasibility and establish preliminary effect sizes. Ment Health Phys Act. (2013) 6:10.1016/j.mhpa.2013.06.006. doi: 10.1016/j.mhpa.2013.06.006
56. Jeong YJ, Hong SC, Lee MS, Park MC, Kim YK, Suh CM. Dance movement therapy improves emotional responses and modulates neurohormones in adolescents with mild depression. Int J Neurosci. (2005) 115:1711–20. doi: 10.1080/00207450590958574
57. McCann IL, Holmes DS. Influence of aerobic exercise on depression. J Pers Soc Psychol. (1984) 46:1142–7. doi: 10.1037//0022-3514.46.5.1142
58. Mohammadi M. A study and comparison of the effect of team sports (soccer and volleyball) and individual sports (table tennis and badminton) on depression among high school students. Aust J Basic Appl Sci. (2011) 5:1005–11.
59. Nabkasorn C, Miyai N, Sootmongkol A, Junprasert S, Yamamoto H, Arita M, et al. Effects of physical exercise on depression, neuroendocrine stress hormones and physiological fitness in adolescent females with depressive symptoms. Eur J Public Health. (2006) 16:179–84. doi: 10.1093/eurpub/cki159
60. Dabidy Roshan V, Pourasghar M, Mohammadian Z. The efficacy of intermittent walking in water on the rate of MHPG sulfate and the severity of depression. Iran J Psychiatry Behav Sci. (2011) 5:26–31.
61. Sadeghi K, Ahmadi SM, Ahmadi SM, Rezaei M, Miri J, Abdi A, et al. A comparative study of the efficacy of cognitive group therapy and aerobic exercise in the treatment of depression among the students. Glob J Health Sci. (2016) 8:54171. doi: 10.5539/gjhs.v8n10p1
62. Ma M. Evaluation of the intervention effect of different exercise programs on Zhuang depressed and anxious college students. China School Health. (2017) 38:112–4.
63. Huang B. The effect of simplified twenty-four styles of Taijiquan on depression levels of female college students. Beijing Sports University, Beijing, China. (2008).
64. Li N. Experiment on depression and physical exercise intervention among college students. J. Sport. (2001) 4:32-6. doi: 10.16237/j.cnki.cn44-1404/g8.2001.04.011
65. Jiao H. Effects of aerobic exercise intervention on depression in teacher education college students. Chin J Health Psychol. (2010) 18:939–41. doi: 10.13342/j.cnki.cjhp.2010.08.035
66. Hu D, Liu J. A study on the effects of physical exercise on depression and anxiety states of college students. J Shandong Educ Coll. (2011) 26:36–8.
67. Zhu L, Yu S. Experimental study on the effect of middle and long-distance running on depressive symptoms in college students. J Huangshan Coll. (2011) 13:79–82.
68. Zheng Q. An Experimental Study on the Effect of Badminton on Depression in Female College Students. Capital Institute of Physical Education (2015).
69. Qiao Z. Research on the Effect of Aerobics on Depression Among Female College Students. Inner Mongolia Normal University (2010).
70. Guan S, Li Q, Zhang S. The effect of strength training on depression and monoamine levels in depressed female college students. J Wuhan Instit Phys Educ. (2018) 10:7—4. doi: 10.15930/j.cnki.wtxb
71. Li H. An experimental study of aerobics exercise to alleviate depression in female college students. J Taiyuan City Vocat Technol Coll. (2012) 9:107–9. doi: 10.16227/j.cnki.tycs.2012.09.097
72. Wang Y, Liu X. A study on the psychological intervention of depression among female college students based on basketball. J Weinan Norm Coll Comprehen Edn. (2012) 2:96–9.
73. Philippot A, Dubois V, Lambrechts K, Grogna D, Robert A, Jonckheer U, et al. Impact of physical exercise on depression and anxiety in adolescent inpatients: A randomized controlled trial. J Affect Disord. (2022) 301:145–53. doi: 10.1016/j.jad.2022.01.011
74. MacMahon JR, Gross RT. Physical and psychological effects of aerobic exercise in delinquent adolescent males. Am J Dis Child. (1988) 142:1361–6. doi: 10.1001/archpedi.1988.02150120115053
75. Li C, Tan Z, Liu S. An experimental study on the treatment of depression in college students with Badaanjin exercise. Sports Sci Res. (2014) 18:72–5.
76. Li Y. A study on physical exercise to alleviate anxiety and depression among secondary school students in disaster areas. J Guizhou Norm Univ. (2011) 27:41–3.
77. Yu L, Yi G, Xia J. Effects of Traditional Sports and Exercise Prescription on Mood and Sleep Quality of Female College Students With Mild Depression. Sichuan Sports Science (2021).
78. Chen J, Li Y, Wu Y. Effects of tai chi Exercise on Depressive Mood and Serum Inflammatory Factors in Female College Students. Chinese School Health (2019).
79. Li H. An experimental study on the effect of aerobics exercise on alleviating depressive tendencies of female college students. J Tianjin Sports Institut. (2008) 5:450–2.
80. Wang D, Qin Q. Fitness Qigong. Evaluation of the effect of Five Animal Play on the intervention of mild depression in college students. Contemp Sports Technol. (2015) 23:29–30.
81. Hu J. An experimental study of taijiquan combined with mind-tuning operation to intervene depression in college students. Sports. (2017) 24:1–1.
82. Yu L, Xia J. The Effect of Traditional Sports and Wellness Exercise Prescription on Depression Among College Students. Sports Science and Technology (2020).
83. Li Q, Guan S, Yin L. A study on the effect of physical exercise on depressive state and monoamine transmitters in depressed female college students. Chin J Mod Med. (2014) 8:86–90.
84. Zhang J, Qin S, Zhou Y, Meng L, Su H, Zhao S. A randomized controlled trial of mindfulness-based Tai Chi Chuan for subthreshold depression adolescents. Neuropsychiatr Dis Treat. (2018) 14:2313–21. doi: 10.2147/NDT.S173255
85. Yu L, Xia J, Yi G, Chen J, Zhao, K. (2022). The effects of cheerleading integration inside and outside the classroom on depression and body self-esteem of depressed female college students. Psychol Month. (2022) 17:5–7+67. doi: 10.19738/j.cnki.psy
86. Zhao S, Liu Y, Yang S, Zhang L. A study on the improvement of depression in college students after 18 weeks of physical activity in and out of class. Youth Sports. (2019) 11:42–3.
87. Noggle JJ, Steiner NJ, Minami T, Khalsa SB. Benefits of yoga for psychosocial well-being in a US high school curriculum: a preliminary randomized controlled trial. J Dev Behav Pediatr. (2012) 33:193–201. doi: 10.1097/DBP.0b013e31824afdc4
88. Li Q, Guan S, Zhang S. Effects of aerobic exercise on depressive state and monoamine transmitters in depressed female college students. J Xi'an Sports Coll. (2009) 01:121–124+128.
89. Bonhauser M, Fernandez G, Püschel K, Yañez F, Montero J, Thompson B, et al. Improving physical fitness and emotional well-being in adolescents of low socioeconomic status in Chile: results of a school-based controlled trial. Health Promot Int. (2005) 20:113–22. doi: 10.1093/heapro/dah603
90. Khalsa SBS, Hickey-Schultz L, Cohen D, Steiner N, Cope S. Evaluation of the mental health benefits of yoga in a secondary school: A preliminary randomized controlled trial. J Behav Health Serv Res. (2012) 39:80–90. doi: 10.1007/s11414-011-9249-8
91. Velásquez AM, López MA, Quiñonez N, Paba DP. Yoga for the prevention of depression, anxiety, and aggression and the promotion of socio-emotional competencies in school-aged children. Educ Res Evaluat. (2015) 2:407–21.
92. Butzer B, LoRusso A, Shin SH, Khalsa SB. Evaluation of yoga for preventing adolescent substance use risk factors in a middle school setting: A preliminary group-randomized controlled trial. J Youth Adolesc. (2017) 46:603–32. doi: 10.1007/s10964-016-0513-3
93. Costigan SA, Eather N, Plotnikoff RC, Hillman CH, Lubans DR. High-intensity interval training for cognitive and mental health in adolescents. Med Sci Sports Exerc. (2016) 48:1985–93. doi: 10.1249/MSS.0000000000000993
94. Goodrich FG. The Effects of Aerobic Fitness Training on Hostility and Depression in a College Population. Hofstra University (1984).
95. Xiaowang Y, Xixiang Y, Guochang Y, Daming Q. Experimental intervention of basketball and aerobics on college students' mental health. J Beijing Sports Univ. (2007) 3:338–339+347. doi: 10.19582/j.cnki.11-3785/g8.2007.03.018
96. Wenbo L. Research on the impact of ball sports intervention on college students' mental health. J Beijing Sport Univ. (2008) 7:951–3. doi: 10.19582/j.cnki.11-3785/g8.2008.07.029
97. Wang J. A study on the efficacy of collective rivalry sports on depression among college students in medical schools. Med Soc. (2008) 8:58–60.
98. Yang D. The effect of physical exercise on the anxiety and depression of college students. New West. (2010) 5:240+230.
99. Daley AJ, Copeland RJ, Wright NP, Roalfe A, Wales JK. Exercise therapy as a treatment for psychopathologic conditions in obese and morbidly obese adolescents: a randomized, controlled trial. Pediatrics. (2006) 118:2126–34. doi: 10.1542/peds.2006–1285
100. Hilyer JC, Wilson DG, Dillon C, Caro L, Jenkins C, Spencer WA, et al. Physical fitness training and counseling as treatment for youthful offenders. J Counsel Psychol. (1982) 29:292–303.
101. Zhang W. Research on exercise prescription teaching and physical and mental health of college students. Sports Sci Technol. (2011) 32:63–5.
102. Li W. A pilot study on the effect of fitness aerobics on college students' depression. J Wuxi Vocat Tech Coll. (2015) 2:93–6.
103. Hongfu L. The effect of fitness qigong-Baduanjin on the state of mind of college students in medical schools. Med Soc. (2007) 11:60–2.
104. Chen T. The effect of aerobic exercise on female college students' body self-esteem and state of mind. J Guangzhou Instit Phys Educ. (2007) 5:73–75+79.
105. He L. An experimental study on the effects of physical activity on college students' moods and emotions. J Beijing Sports Univ. (2007) 4:481–482+488. doi: 10.19582/j.cnki.11-3785/g8
106. Chen C. An experimental study on the effect of basketball on the mental health of general male college students. J Guangzhou Instit Phys Educ. (2009) 29:80–2. doi: 10.13830/j.cnki.cn44-1129/g8.2009.06.020
107. Gallego J, Aguilar-Parra JM, Cangas AJ, Langer ÁI, Mañas I. Effect of a mindfulness program on stress, anxiety and depression in university students. Span J Psychol. (2015) 17:E109. doi: 10.1017/sjp.2014.102
108. Fan Y. The effect of strength exercise on depression level of college students. Shandong Sports Sci Technol. (2003) 1:47–8. doi: 10.14105/j.cnki.1009-9840.2003.01.019
109. He Y, Ji L. The effect of different types of physical exercise on depression level of college students and its psychological mediating variable (Body-esteem). Sports Sci. (2004) 5:32–35+52. doi: 10.16469/j.css.2004.05.011
110. Kuttner L, Chambers CT, Hardial J, Israel DM, Jacobson K, Evans K. A randomized trial of yoga for adolescents with irritable bowel syndrome. Pain Res Manag. (2006) 11:217–23. doi: 10.1155/2006/731628
111. Chu KF, Wei CL. A study on the correlation between physical exercise on improving anxiety and depression among college students. Fujian Sports Sci Technol. (2004) 6:57–9.
112. Wegner M, Helmich I, Machado S, Nardi E, Arias-Carrion AO, Budde H. Effects of exercise on anxiety and depression disorders: review of meta-analyses and neurobiological mechanisms. CNS Neurol Disorders Drug Targets. (2014) 13:1002–1014. doi: 10.2174/1871527313666140612102841
113. Duman CH, Schlesinger L, Russell DS, Duman RS. Voluntary exercise produces antidepressant and anxiolytic behavioral effects in mice. Brain Res. (2008) 1199:148–58. doi: 10.1016/j.brainres.2007.12.047
114. Fuss J, Ben Abdallah NMB, Vogt MA, Touma C, Pacifici PG, Palme R, et al. Voluntary exercise induces anxiety-like behavior in adult C57BL/6J mice correlating with hippocampal neurogenesis. Hippocampus. (2010) 20:364–76. doi: 10.1002/hipo.20634
115. Carter T, Morres ID, Meade O, Callaghan P. The effect of exercise on depressive symptoms in adolescents: a systematic review and meta-analysis. J Am Acad Child Adolesc Psychiatry. (2016) 55:580–90. doi: 10.1016/j.jaac.2016.04.016
116. Radovic S, Gordon MS, Melvin GA. Should we recommend exercise to adolescents with depressive symptoms? A meta-analysis. J Paediatr Child Health. (2017) 53:214–20. doi: 10.1111/jpc.13426
117. Brown HE, Pearson N, Braithwaite RE, Brown WJ, Biddle SJ. Physical activity interventions and depression in children and adolescents. Sports Med. (2013) 43:195–206. doi: 10.1007/s40279-012-0015-8
118. Ströhle A. Physical activity, exercise, depression and anxiety disorders. J Neural Transm. (2009) 116:777–84. doi: 10.1007/s00702-008-0092-x
119. Martin B, Peck B, Terry D. Young Children's Experiences with Yoga after School. J Occupational Ther Schools Early Interv. (2022) 2:1–18. doi: 10.1080/19411243.2022.2037490
120. Ekeland E, Heian F, Hagen K, Coren E. Can exercise improve self-esteem in children and young people? A systematic review of randomised controlled trials. Br J Sports Med. (2005) 39:792–8. doi: 10.1136/bjsm.2004.017707
121. Spence SH, Sheffield JK, Donovan CL. Long-term outcome of a school-based, universal approach to prevention of depression in adolescents. J Consult Clin Psychol. (2005) 73:160–7. doi: 10.1037/0022-006X.73.1.160
122. Michel TM, Pülschen D, Thome J. The role of oxidative stress in depressive disorders. Curr Pharm Des. (2012) 18:5890–9. doi: 10.2174/138161212803523554
123. Yen CJ, Hung CH, Tsai WM, Cheng HC, Yang HL, Lu YJ, et al. Effect of exercise training on exercise tolerance and level of oxidative stress for head and neck cancer patients following chemotherapy. Front Oncol. (2020) 10:1536. doi: 10.3389/fonc.2020.01536
124. Wang SK, Wang SQ, Wang YJ, Xu ZH. Research progress on the effect of exercise on depression and its neurobiological mechanism. Chinese Family Medicine. (2022) 27:3443–51.
125. Vankova H, Holmerova I, Machacova K, Volicer L, Veleta P, Celko AM, et al. The effect of dance on depressive symptoms in nursing home residents. J Am Med Dir Assoc. (2014) 15:582–7. doi: 10.1016/j.jamda.2014.04.013
126. Faulkner G. Promoting physical activity for mental health: A complex intervention? Mental Health Phys Activity. (2009) 2:1–3. doi: 10.1016/j.mhpa.2009.04.001
127. Perraton LG, Kumar S, Machotka Z. Exercise parameters in the treatment of clinical depression: a systematic review of randomized controlled trials. J Eval Clin Pract. (2010) 16:597–604. doi: 10.1111/j.1365-2753.2009.01188.x
128. Liu Y, Chu JMT, Yan T, Zhang Y, Chen Y, Chang RCC, et al. Short-term resistance exercise inhibits neuroinflammation and attenuates neuropathological changes in 3xTg Alzheimer's disease mice. J Neuroinflammation. (2020) 17:1–16. doi: 10.1186/s12974-019-1653-7
129. Bandura A, Freeman WH, Lightsey R. Self-Efficacy: The Exercise of Control. Berlin: Springer (1999).
130. Marsh HW, Redmayne RS. A multidimensional physical self-concept and its relations to multiple components of physical fitness. J Sport Exercise Psychology. (1994) 16:43–55. doi: 10.1123/jsep.16.1.43
131. Yang C. The relationship between physical exercise and self-efficacy among college students: the mediating role of endurance quality. J Nanjing Sports College. (2013) 27:72–7.
132. Aidar FJ, Carneiro AL, Patrocínio Oliveira CE, Garrido ND, Raineh I, Vilaça JM, Gama de Matos D. Effects of resistance training on the physical condition of people with multiple sclerosis. J Sports Med Phys Fitness. (2017) 58:1127–1134. doi: 10.23736/S0022-4707.17.07621-6
133. Tucker LA, Mortell R. Comparison of the effects of walking and weight training programs on body image in middle-aged women: an experimental study. Am J Health Promot. (1993) 8:34–42. doi: 10.4278/0890-1171-8.1.34
134. Tsukamoto H, Suga T, Takenaka S, Takeuchi T, Tanaka D, Hamaoka T, et al. An acute bout of localized resistance exercise can rapidly improve inhibitory control. PLoS ONE. (2017) 12:e0184075. doi: 10.1371/journal.pone.0184075
135. Brush CJ, Olson RL, Ehmann PJ, Osovsky S, Alderman BL. Dose–response and time course effects of acute resistance exercise on executive function. J Sport Exercise Psychol. (2016) 38:396–408. doi: 10.1123/jsep.2016-0027
136. Giles A, Nasstasia Y, BakerAL, Kelly BJ, Dascombe BJ, Halpin SA, et al. Exercise as treatment for youth with major depression: the healthy body healthy mind feasibility study. J Psychiatric Prac. (2020) 26:444–60. doi: 10.1097/PRA.0000000000000516
137. Cooney GM, Dwan K, Greig CA, Lawlor DA, Rimer J, Waugh FR, et al. Exercise for depression. Cochrane Datab Syst Rev. (2013) 2013:CD004366. doi: 10.1002/14651858.CD004366.pub6
138. Peluso MAM, Andrade LHSG. Physical activity and mental health: the association between exercise and mood. Clinics. (2005) 60:61–70. doi: 10.1590/S1807-59322005000100012
139. Bellón J, Conejo-Cerón S, Sánchez-Calderón A, Rodríguez-Martín B, Bellón D, Rodríguez-Sánchez E, et al. Effectiveness of exercise-based interventions in reducing depressive symptoms in people without clinical depression: systematic review and meta-analysis of randomised controlled trials. Br J Psychiatry. (2021) 219:578–87. doi: 10.1192/bjp.2021.5
140. Périard JD, Eijsvogels TM, Daanen HA. Exercise under heat stress: thermoregulation, hydration, performance implications, and mitigation strategies. Physiol Rev. (2021) 17:2020. doi: 10.1152/physrev.00038.2020
141. Harber VJ, Sutton JR. Endorphins and exercise. Sports Medicine. (1984) 1:154–71. doi: 10.2165/00007256-198401020-00004
142. Craft LL, Landers DM. The effect of exercise on clinical depression and depression resulting from mental illness: a meta-analysis. J Sport Exer Psychol. (1998) 20:339–57. doi: 10.1123/jsep.20.4.339
143. Lee HH, Emerson JA, Williams DM. The exercise–affect–adherence pathway: an evolutionary perspective. Front Psychol. (2016) 7:1285. doi: 10.3389/fpsyg.2016.01285
144. Woods JA, Hutchinson NT, Powers SK, Roberts WO, Gomez-Cabrera MC, Radak Z, et al. The COVID-19 pandemic and physical activity. Sports Med Health Science. (2020) 2:55–64. doi: 10.1016/j.smhs.2020.05.006
145. Resnick B, Orwig D, Magaziner J, Wynne C. The effect of social support on exercise behavior in older adults. Clin Nurs Res. (2002) 11:52–70. doi: 10.1177/105477380201100105
147. Chen FX, Zhao ZS, Qin HQ. Factors associated with outpatient depression affecting adherence. J Clin Psycho Disorders. (2004) 4:300–2.
148. McDermott B, Baigent M, Chanen A, Fraser L, Graetz B, Hayman N, et al. Clinical Practice Guidelines: Depression in Adolescents and Young Adults. Melbourne: Beyondblue: The National Depression Initiative (2010).
149. Larun L, Nordheim LV, Ekeland E, Hagen KB, Heian F. Exercise for preventing and treating anxiety and depression in children and young people. Cochrane Datab Syst Rev. (2009) 3:19.
150. Penninx BW, Milaneschi Y, Lamers F, Vogelzangs N. Understanding the somatic consequences of depression: biological mechanisms and the role of depression symptom profile. BMC Med. (2013) 11:1–14. doi: 10.1186/1741-7015-11-129
151. Burton C, McKinstry B, Szentagotai Tătar A, Serrano-Blanco A, Pagliari C, Wolters M, et al. Activity monitoring in patients with depression: a systematic review. J Affect Disord. (2013) 145:21–8. doi: 10.1016/j.jad.2012.07.001
152. Shim EJ, Noh HL, Yoon J, Mun HS, Hahm BJ. A longitudinal analysis of the relationships among daytime dysfunction, fatigue, and depression in college students. J Ame College Health. (2019) 67:51–8. doi: 10.1080/07448481.2018.1462819
Keywords: depression, anxiety, exercise, youth, treatment, prevention
Citation: Zhang Y, Li G, Liu C, Guan J, Zhang Y and Shi Z (2023) Comparing the efficacy of different types of exercise for the treatment and prevention of depression in youths: a systematic review and network meta-analysis. Front. Psychiatry 14:1199510. doi: 10.3389/fpsyt.2023.1199510
Received: 03 April 2023; Accepted: 03 May 2023;
Published: 02 June 2023.
Edited by:
Shengyan Sun, Huzhou University, ChinaCopyright © 2023 Zhang, Li, Liu, Guan, Zhang and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zifu Shi, U2hpemZAaHVubnUuZWR1LmNu