 Anastasia Pavlidou
Anastasia Pavlidou Geoffrey Gorisse
Geoffrey Gorisse Domna Banakou
Domna Banakou Sebastian Walther
Sebastian Walther
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Psychiatry, 09 June 2023
Sec. Schizophrenia
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1191601
Introduction: Gesture performance deficits are prevalent in schizophrenia patients and are strongly associated with poor social communication skills and community functioning, affecting their overall quality of life. Currently, video-recording technology is widely used in clinical settings to assess gesture production deficits in schizophrenia patients. Nevertheless, the subjective evaluation of video-recordings can encumber task assessment. The present study will aim to use virtual reality to examine its potential use as an alternative tool to objectively measure gesture performance accuracy in schizophrenia patients and healthy controls.
Methods: Gesture performance in the virtual reality setting will be based on the well-established Test of Upper Limb Apraxia. Participants will be immersed in a virtual environment where they will experience themselves being embodied in a collocated virtual body seen from a first-person perspective. Motion trackers will be placed on participants' hands and elbows to track upper body movements in real-time, and to record gesture movement for later analysis. Participants will see a virtual agent sitting across from them, with a virtual table in between. The agent will perform various types of gestures and the participants' task will be to imitate those gestures as accurately as possible. Measurements from the tracking devices will be stored and analyzed to address gesture performance accuracy across groups.
Discussion: This study aims to provide objective measurements of gesture performance accuracy in schizophrenia patients. If successful, the results will provide new knowledge to the gesture literature and offer the potential for novel therapeutic interventions using virtual reality technologies. Such interventions can improve gesturing and thus advance social communication skills in schizophrenia patients.
Schizophrenia is a complex mental health disorder that affects ~1% of the general population. Schizophrenia is characterized by a wide range of clinical symptoms including disorganized thinking, paranoia, hallucinations, motor abnormalities, executive dysfunction, social withdrawal and affective flattening, all of which greatly disturb social communication processes leading to poor community functioning and quality of life (1–3). Successful social communication is highly dependent on one's ability to correctly perceive, interpret and execute socially relevant cues (4). In recent years, gestures serve as an important research tool in understanding social communication deficits in schizophrenia patients (5, 6).
Gestures are biological movements used alone or in combination with speech, to aid in social communication (7). Video-recordings of gesture performance in clinical settings show that schizophrenia patients and individuals at high-risk for psychosis tend to use hand gestures less frequently, or in the wrong context (8–10) and spend significantly less time fixating on the performed gestures (11). In addition, schizophrenia patients have deficits in correctly imitating meaningless and meaningful gestures following visual demonstration from an experimenter. Errors include slow movements with reduced amplitudes, extra movements, omissions, and body-part-as-object (12, 13). These errors are associated with impairments in postural knowledge, tool use, and social perception, suggesting a generalized impairment in non-verbal social communication in schizophrenia (14). Furthermore, deficits in gesture performance predict poor community functioning (15), and are strongly associated with symptom severity, motor abnormalities, and executive dysfunction, such as processing speed, attention, and working memory abilities (5, 11, 13, 14, 16–23).
Video recordings are easy to implement and have provided rich and notable insights on the mechanisms involved during gesture performance in schizophrenia (13, 14, 20, 24, 25). However, there are a few limitations to consider. In clinical settings, video-recordings can modify naturally occurring behaviors (26). In addition, when video-recordings are used to score participants' performance during a task, the data are categorical in nature and the process requires vigorous training for the scorer(s), which can be time consuming and cause inter-rater reliability issues. Further, the positioning of the camera can differ between sessions and participants' affecting viewpoint and body representations that can alter the evaluation of the task. The use of virtual reality (VR) technology can readily tackle most of these limitations (27).
In recent years, VR is increasingly used in the assessment and rehabilitation of movement execution (28). VR allows the creation of a virtual environment where users can interact with virtual characters via spoken language and hand gestures just as they would in the real world (29), supporting a highly immersive experience with increased ecological validity, reliability and reproducibility (30). Images of the virtual environment are displayed via the use of a head mounted display (HMD) where the users' head position and orientation are continuously tracked and updated as they move around (31, 32). Motion tracking devices can be used to substitute the users' body with a gender-matched virtual one seen from a first-person perspective and onto which their real movements are mapped in real-time, resulting in an illusionary ownership over the virtual body (33–35). Data from these tracking devices are multidimensional and provide an objective, reliable and unobtrusive measurement of real-time human behavior that surpasses that provided by video-recording data (36).
To our knowledge, no study to date has utilized VR to examine accuracy of hand gestures in schizophrenia patients. To this end, the aim of the present study is to apply VR technology to collect measurements of naturally occurring hand gestures during an imitation task in schizophrenia patients and compare their performance to healthy controls. Additionally, we will administer motor, socio-cognitive and community functioning assessments used in previous research from our lab to determine their relationship with hand gesture accuracy in VR. In accordance with previous studies (5, 13, 14, 20), we hypothesize that schizophrenia patients will perform the required gestures less accurately than healthy controls and that these deficits will be linked to their psychopathology, motor abnormalities, as well as compromised socio-cognitive and community functioning.
This is an exploratory cross-sectional observational study using VR technology to assess the performance accuracy of different hand gestures. An HMD will be used to immerse participants in the virtual environment. Motion trackers, attached to the hands and elbows, will provide participants with real-time upper body tracking (see section VR apparatus for more details). Data from the HMD and motion trackers will be continuously stored on a computer for analyses. We plan to recruit 60 schizophrenia patients and 60 age and gender matched controls over a 2-year period. The duration of the study is ~6 h. The assessments are separated into 2-h sessions/per day and all assessments are completed within a 72-h period.
Schizophrenia patients will be recruited from the inpatient and outpatient departments of the University hospital of Psychiatry and Psychotherapy in Bern, Switzerland. All potential schizophrenia patients will be screened using the Mini International Neuropsychiatric Interview (37) for the DSM-5 criteria. Healthy controls will be recruited through advertisement and by word-of-mouth. Inclusion criteria for all participants include: right-handedness, 18–65 years of age, no substance abuse (except nicotine), and no history of neurological disorders or any other severe mental health disorders. Additionally, for controls only, no personal, or first-degree relatives with a history of any mental health disorders.
The VR gesture task is based on the Test of Upper Limb Apraxia (TULIA), which was developed in accordance with the central domains and semantic characteristics of gesture performance (38, 39). TULIA measures accuracy of finger and hand movements in 48 items across two domains: the imitation domain (gesture performance following visual demonstration from the experimenter) and the pantomime domain (gesture performance following verbal command from the experimenter). Within these domains three different semantic categories of gestures exist: (a) meaningless (new gestures without semantic elements), (b) intransitive (highly learned communicative gestures, such as waving good-bye), and (c) transitive (tool-based gestures, such as using a toothbrush). Scores for each item are rated using a 0–5 scale. The maximum score earned in the TULIA test is 240 (120 per domain), which is indicative of superior gesture performance (38). Administration of the TULIA test requires both the participant and the experimenter to be seated across from each other with a table between them; both with their hands placed flat on the table. For the imitation domain, which is the focus of this study, participants are asked to execute the required gestures with their dominant hand only after the experimenter has demonstrated the gestures in a mirrored manner and has returned their hand to the original position (flat on the table). Participants are informed on the nature of the gestures following each block. The TULIA test is video-recorded and later quantified by an independent experimenter.
The development of the virtual environment for gesture assessment in VR was inspired from clinical applications of the TULIA task and created using the real-time 3D engine Unity 2020 LTS.1 Animations for the TULIA movements were recorded using the Glycon 3D2 motion capture software and edited with Autodesk MotionBuilder 2019.3 The virtual environment consists of an office room equipped with a table in its center (Figure 1A). Windows and a door are also present on the left and right side of the room, respectively. Across from participants, on the other side of the table, a virtual agent is seated on a chair with her hands flat on the table (Figure 1B). Outside the virtual environment, in the physical laboratory, participants are placed in a similar scenario with their hands flat on a table in front of them. Motion trackers are placed on the hands and elbows of each arm, and the HMD is adjusted for each participant (Figure 1C). The HMD provides a stereoscopic display of the virtual environment and of the autonomous agent seen from an embodied first-person perspective, while the motion trackers provide participants with virtual arms that they can control using their own movements. Participants' virtual body will be gender matched. Once immersed in the virtual environment participants will be instructed via pre-recorded verbal instructions to look around and describe what they see. In addition, they will be instructed to move their hands up and down to induce the illusion of body ownership over the virtual body, following earlier examples (33–35). After this introductory phase, participants will be trained on the task. They will be informed to closely look at the movements of the agent seated across from them performing the gestures in a mirrored manner. Their task will be to imitate those same gestures as accurately as possible using their dominant hand (right hand). To ensure that participants perform the gestures only after the agent places her hands back on the table, a red light is added as a visual cue, and participants will be informed to only perform the gestures once this light turns off. Similar to the TULIA task, participants will be informed on the nature of the gestures before each block. Each block contains 6 different gestures and will be repeated twice during the experiment. All gesture blocks (meaningless, intransitive, and transitive) will be randomized across participants. A post-experiment questionnaire will be used to record participants' subjective feeling of presence and embodiment with respect to their virtual body, as well as, other questions related to how participants evaluate the virtual female agent and their interaction, and overall experience using a −3 (“not at all”) to a 3 (“very much”) scale (Table 1). In addition, possible side effects (i.e., dizziness), as well as, personal thoughts and feelings regarding participants' exposure to VR will also be accounted for directly after the experiment and at the follow-up session, 2-weeks after exposure. The VR procedures are demonstrated in Supplementary Movie S1.

Figure 1. The virtual reality setup. (A) A third-person perspective of the virtual setup depicting the position of the participant on one side of the table and the virtual agent on the other. (B) The virtual environment as seen from the participant's first-person perspective. The participant has a view of their own hands and gender-matched body and they can see the virtual agent sitting across from them with the hands resting on the table. (C) The participant in the physical laboratory equipped with the HMD and upper body tracking devices.
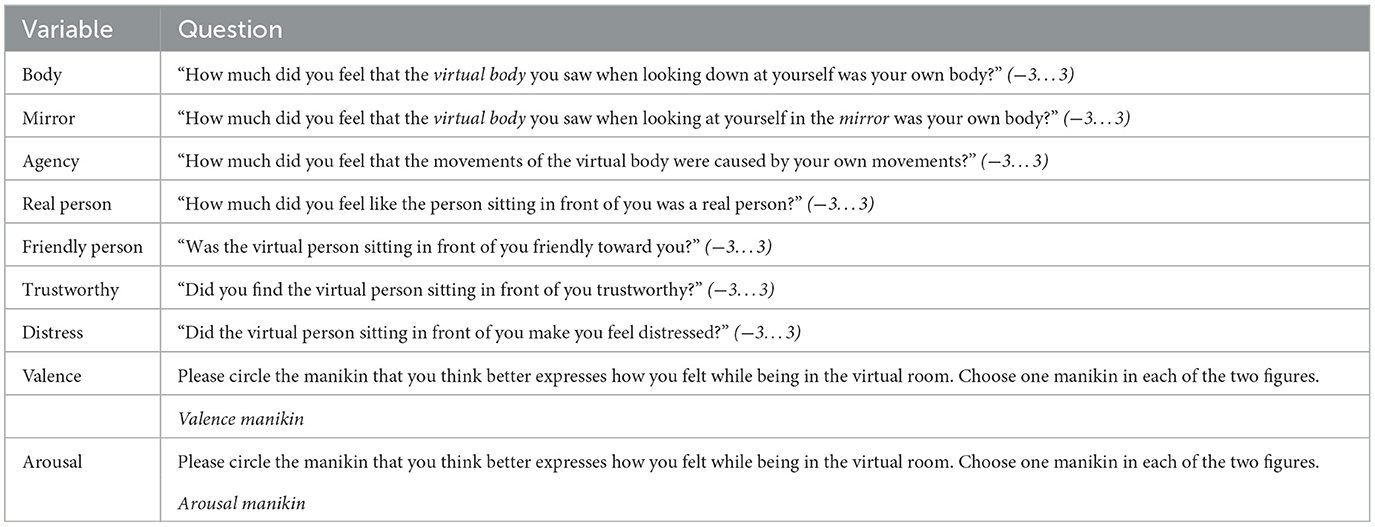
Table 1. The post-VR questionnaire.
The HTC VIVE Pro4 virtual reality headset will be used to display the virtual environment. It has a combined resolution of 2,880 × 1,600 pixels (1,440 × 1,600 pixels per eye), a refresh rate of 90 Hz, and a field of view of 110°. The motion tracking equipment which will allow participants to control their virtual body arms in real time is performed using the VIVE trackers (four in total−2 placed on the hands and 2 on the elbows as seen in Figure 1C). The application will run on a computer with a Core i9-11900H @ 3.50 processor and an Nvidia GeForce RTX 3080 graphics card.
We will include additional non-verbal communication tasks outside of VR to assess participants' ability to recognize and perceive non-verbal social cues such facial expressions, biological movements, and voice tone. Motor, cognitive and community functioning domains will be assessed using well-established standardized rating scales and symptom severity and antipsychotic medication usage in all patients will also be accounted for. All clinical, motor, socio-cognitive and community functioning assessments can be found in Table 2.
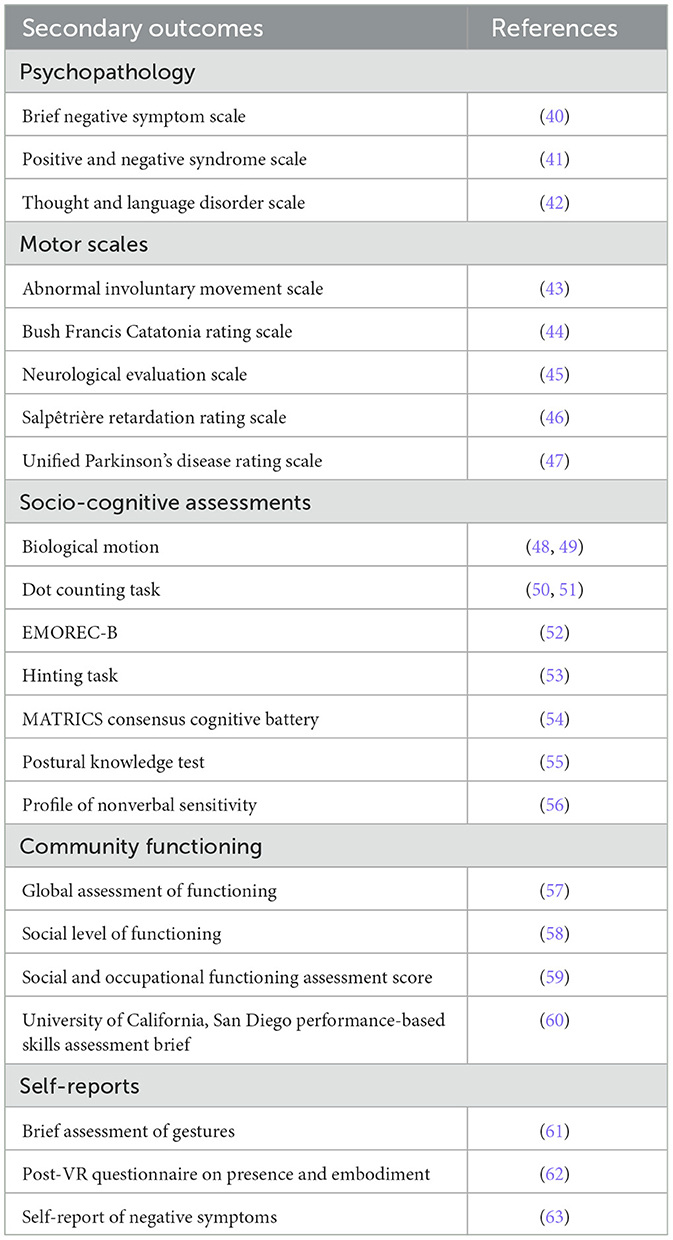
Table 2. Clinical, motor, socio-cognitive and community functioning assessments of participants.
Measurements collected from the tracking devices during gesture performance will be analyzed using linear mixed models. These will include upper body rotational data per gesture across all experimental blocks. Data are saved at a frequency of 60 Hz (16 ms). The rotational data between participants and the virtual agent performing the gestures will be compared across time based on distance metrics such as Dynamic Time Warping (DTW) that measures similarity between time series by considering the temporal relationship between rotational vectors. Group (patients and healthy controls) and gesture category (meaningless, intransitive, and transitive), as well as, their interaction will be added as fixed effects, while a single intercept parameter estimated for each participant will be added as random effects. Covariates in the model will also be considered if demographic characteristics such as age, gender or education are different between patients and controls. In addition, differences in symptom severity and motor deficits between inpatient and outpatient participants will also be considered. The Kruskal–Wallis test will be used to assess such differences. In addition, we will apply partial correlation analyses using the spearman method to examine the relationship between gesture performance accuracy in VR with symptom severity, motor, socio-cognitive and community functioning scores, while controlling for medication. This will help in determining if gesture performance accuracy using VR in patients is linked to a specific domain or is generalized across multiple domains.
Recruitment for the study begun November 1st 2022, and is expected to be completed November 2024. As of May 2023, we recruited 23 patients and 8 controls, and completed assessments for 19 patients and 7 controls.
The crucial feature of this study is the implementation of a VR setup to assess real-time movements to objectively quantify gesture performance accuracy in schizophrenia patients and healthy controls. To date, assessment of gesture performance in schizophrenia patients is mostly based on categorical data, and doesn't take into account all the attributes and features associated with gesture performance. VR captures multidimensional data that may reveal hidden insights on the mechanisms attributed to gesture deficits in schizophrenia patients. If our VR setup proves to be successful in capturing and measuring gesture deficits in schizophrenia patients this has the potential to generate new knowledge regarding non-verbal communication that can help in designing therapeutic interventions to improve treatments for schizophrenia patients (36). Such treatments are valuable as there are often substantial costs to patients, their family and friends, caregivers and to the society as a whole (64). In the following section, we briefly discuss the types of therapeutic interventions available to schizophrenia patients, and discuss future directions on how VR can support and expand their impact.
Thus far, most treatments for schizophrenia heavily relied on pharmacological interventions, with heterogeneous results (23). Recent evidence suggests that neurostimulation (65–67), cognitive remediation therapy (52, 68–70) and social skills training (70, 71) promote neuroplasticity and can alleviate non-verbal communication deficits in schizophrenia patients, such as the evaluation and interpretation of emotional expressions, eye contact and body language but none are exclusive in tackling gesture deficits. In fact, therapeutic interventions specifically targeting gesture deficits and, in particular, gesture performance deficits in schizophrenia are limited. One recent study used a specific multimodal speech-gesture training that integrates non-verbal communication, working memory abilities and natural communication (72) to improve gesture processing in schizophrenia and showed significant improvements in patients' quality of life, which was significantly correlated with changes in the neural processing of abstract speech-gesture content (73). Another study, which combines neurostimulation and social cognitive remediation therapy to examine their effectiveness in improving gesture performance in schizophrenia is currently underway (68).
While conventional therapeutic interventions are essential in recovery, they are organized in accordance to one's environment, reaching only a portion of the patients who can benefit, and are strongly dependent on the availability and expertise of therapists. The application of VR in clinical settings can provide flexible, ecologically valid, reproducible and highly-controlled environments of real-life situations offering cost-effective exposure therapy in terms of time and expenses while reaching a much larger population. This coupled with the convenience and privacy it provides, clinicians have utilized VR in pain management, cognitive and motor rehabilitation in stroke and Parkinson's patients, and therapy and training exposure for patients suffering from anxiety, depression and psychosis (74–76).
VR use in schizophrenia has been successfully applied to alleviate auditory hallucinations and paranoid ideation (77, 78) to improve interpersonal communication by having patients interact with various characters with different behaviors, and help them acquire new social and interview training skills (79, 80). Patients in such treatments have previously expressed enjoyment and increased motivation when using VR (79, 81). However, no previous studies have explored the potential of VR in movement rehabilitation in schizophrenia patients in order to improve gesture performance. Evidence from neurological patients suggests that VR as a multifaceted system promotes motor learning, a process where the acquisition of newly learned movement skills via experience and practice induces a permanent change in one's ability to execute these newly learned movements (82). If our VR setup proves effective in measuring movement discrepancies during gesture performance in schizophrenia patients, it can be applied to generate new therapeutic interventions, specifically targeting gesture deficits using motor learning, and assess potential changes over time resulting from these interventions. Moreover, VR's adaptable and diverse technological features enable its integration with existing therapies like cognitive remediation therapy and social skills training. This integration can provide more accurate and objective measurements of naturalistic behaviors arising from ongoing interactions that cannot otherwise be quantified using traditional methods. This constitutes VR the ideal candidate in providing patients with an enjoyable and add-on alternative to help in retaining and transferring motor learning in their daily life (83, 84). These newly acquired movement skills can improve how schizophrenia patients express themselves to their family, friends', doctor, or therapist, and how they handle day-to-day tasks, thus enhancing their overall social communication and functioning, whilst promoting independence.
The study does have certain limitations. First, this is a cross-sectional study measuring gesture performance accuracy in VR at a single time-point. Conducting longitudinal studies could offer a more comprehensive understanding of how gesture performance can progress over time in schizophrenia patients. Second, it is crucial to take into account the potential effects of antipsychotic medication on gesture performance. While we intend to account for antipsychotic medication use as a covariate in our analyses, it is important to acknowledge that patients might be on other types of medication that may still influence our findings. Third, although the optical body tracking was designed to avoid occlusion and reduce tracking discrepancies, tracking losses might still occur leading to potential inconsistencies in the data. Fourth, our application currently supports only gender-matched virtual bodies to substitute the participants' real body. However, in future updates, we aim to use personalized avatars that can consider ethnic characteristics as well. This enhancement could allow for accommodating potential variations in body ownership. This may be particularly important to address in patients with schizophrenia, whereas for healthy individuals it has been demonstrated that body ownership illusions can be induced over distinct virtual bodies, including different race (85–87).
The study aims to provide an objective measurement in assessing gesture performance accuracy in schizophrenia patients and healthy controls using VR. If this study proves to be successful it opens the possibility of utilizing VR paradigms to carry-out therapeutic interventions using motor learning elements to improve gesture deficits in schizophrenia patients and measure possible changes over time in response to these interventions. These types of interventions can be beneficial to other mental health disorders patients who exhibit gesture deficits such as depression (88, 89) or suffer from social cognitive deficits that interfere with non-verbal communication skills such as bipolar and autism spectrum disorders (90, 91).
The studies involving human participants were reviewed and approved by Kantonale Ethikkommision Bern (KEK 2021-02047). The patients/participants provided their written informed consent to participate in this study.
AP: conceptualization, organization, obtained ethics approval, supervision, and drafted the manuscript. GG: designed and set up the VR environment and apparatus. DB: designed and set up the VR environment and apparatus and funding. SW: funding and supervision. All authors reviewed and edited the manuscript. All authors contributed to the article and approved the submitted version.
The study was supported by intramural funding of the University of Bern. DB was funded by the Tamkeen NYU Abu Dhabi Funding Agency (#76 71220 ADHPG VP211).
We sincerely thank Ynes Bouamoud, Till Stüdeli, Hélène Chiara Cuche, and Dr. Evin Demir for their assistance in recruiting participants and acquiring data. We also thank Sofie van Känel for performing the video-recorded movements of the female agent.
SW received honoraria from Neurolite, Janssen, Mepha, Lundbeck, Sunovion and Otsuka.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1191601/full#supplementary-material
3. ^https://www.autodesk.com/products/motionbuilder
4. ^https://www.vive.com/us/product/vive-pro2-full-kit/overview/
1. Green MF, Horan WP, Lee J. Social cognition in schizophrenia. Nat Rev Neurosci. (2015) 16:620–31. doi: 10.1038/nrn4005
2. McCutcheon RA, Marques TR, Howes OD. Schizophrenia—an overview. JAMA Psychiatry. (2020) 77:201–10. doi: 10.1001/jamapsychiatry.2019.3360
3. Wible CG. Schizophrenia as a disorder of social communication. Schizophr Res Treat. (2012) 2012:920485. doi: 10.1155/2012/920485
4. Frith CD, Frith U. Social cognition in humans. Curr Biol. (2007) 17:R724–32. doi: 10.1016/j.cub.2007.05.068
5. Pavlidou A, Chapellier V, Maderthaner L, von Kanel S, Walther S. Using dynamic point light display stimuli to assess gesture deficits in schizophrenia. Schizophr Res Cogn. (2022) 28:100240. doi: 10.1016/j.scog.2022.100240
6. Walther S, Mittal VA. Why we should take a closer look at gestures. Schizophr Bull. (2016) 42:259–61. doi: 10.1093/schbul/sbv229
7. Goldin-Meadow S, Alibali MW. Gesture's role in speaking, learning, creating language. Annu Rev Psychol. (2013) 64:257–83. doi: 10.1146/annurev-psych-113011-143802
8. Lavelle M, Dimic S, Wildgrube C, McCabe R, Priebe S. Non-verbal communication in meetings of psychiatrists and patients with schizophrenia. Acta Psychiatr Scand. (2015) 131:197–205. doi: 10.1111/acps.12319
9. Lavelle M, Healey PG, McCabe R. Is nonverbal communication disrupted in interactions involving patients with schizophrenia? Schizophr Bull. (2013) 39:1150–8. doi: 10.1093/schbul/sbs091
10. Millman ZB, Goss J, Schiffman J, Mejias J, Gupta T, Mittal VA. Mismatch and lexical retrieval gestures are associated with visual information processing, verbal production, and symptomatology in youth at high risk for psychosis. Schizophr Res. (2014) 158:64–8. doi: 10.1016/j.schres.2014.06.007
11. Gupta T, Osborne KJ, Mittal VA. Abnormal gesture perception and clinical high-risk for psychosis. Schizophr Bull. (2021) 47:938–47. doi: 10.1093/schbul/sbab056
12. Walther S, Mittal VA, Stegmayer K, Bohlhalter S. Gesture deficits and apraxia in schizophrenia. Cortex. (2020) 133:65–75. doi: 10.1016/j.cortex.2020.09.017
13. Walther S, Vanbellingen T, Muri R, Strik W, Bohlhalter S. Impaired gesture performance in schizophrenia. particular vulnerability of meaningless pantomimes. Neuropsychologia. (2013) 51:2674–8. doi: 10.1016/j.neuropsychologia.2013.08.017
14. Walther S, Stegmayer K, Sulzbacher J, Vanbellingen T, Muri R, Strik W, et al. Nonverbal social communication and gesture control in schizophrenia. Schizophr Bull. (2015) 41:338–45. doi: 10.1093/schbul/sbu222
15. Walther S, Eisenhardt S, Bohlhalter S, Vanbellingen T, Muri R, Strik W, et al. Gesture performance in schizophrenia predicts functional outcome after 6 months. Schizophr Bull. (2016) 42:1326–33. doi: 10.1093/schbul/sbw124
16. Dutschke LL, Stegmayer K, Ramseyer F, Bohlhalter S, Vanbellingen T, Strik W, et al. Gesture impairments in schizophrenia are linked to increased movement and prolonged motor planning and execution. Schizophr Res. (2018) 200:42–9. doi: 10.1016/j.schres.2017.07.012
17. Matthews N, Gold BJ, Sekuler R, Park S. Gesture imitation in schizophrenia. Schizophr Bull. (2013) 39:94–101. doi: 10.1093/schbul/sbr062
18. Nagels A, Kircher T, Grosvald M, Steines M, Straube B. Evidence for gesture-speech mismatch detection impairments in schizophrenia. Psychiatry Res. (2019) 273:15–21. doi: 10.1016/j.psychres.2018.12.107
19. Park S, Matthews N, Gibson C. Imitation, simulation, and schizophrenia. Schizophr Bull. (2008) 34:698–707. doi: 10.1093/schbul/sbn048
20. Walther S, Vanbellingen T, Muri R, Strik W, Bohlhalter S. Impaired pantomime in schizophrenia: association with frontal lobe function. Cortex. (2013) 49:520–7. doi: 10.1016/j.cortex.2011.12.008
21. Chapellier V, Pavlidou A, Maderthaner L, von Kanel S, Walther S. The impact of poor nonverbal social perception on functional capacity in schizophrenia. Front Psychol. (2022) 13:804093. doi: 10.3389/fpsyg.2022.804093
22. Corcoran CM, Mittal VA, Bearden CE, Gur RE, Hitczenko K, Bilgrami Z, et al. Language as a biomarker for psychosis: a natural language processing approach. Schizophr Res. (2020) 226:158–66. doi: 10.1016/j.schres.2020.04.032
23. Wüthrich F, Pavlidou A, Stegmayer K, Eisenhardt S, Moor J, Schäppi L, et al. Nonverbal communication remains untouched: no beneficial effect of symptomatic improvement on poor gesture performance in schizophrenia. Schizophr Res. (2020) 223:258–64. doi: 10.1016/j.schres.2020.08.013
24. Straube B, Green A, Sass K, Kirner-Veselinovic A, Kircher T. Neural integration of speech and gesture in schizophrenia: evidence for differential processing of metaphoric gestures. Hum Brain Mapp. (2013) 34:1696–712. doi: 10.1002/hbm.22015
25. Choudhury M, Steines M, Nagels A, Riedl L, Kircher T, Straube B. Neural basis of speech-gesture mismatch detection in schizophrenia spectrum disorders. Schizophr Bull. (2021) 47:1761–71. doi: 10.1093/schbul/sbab059
26. Haidet KK, Tate J, Divirgilio-Thomas D, Kolanowski A, Happ MB. Methods to improve reliability of video-recorded behavioral data. Res Nurs Health. (2009) 32:465–74. doi: 10.1002/nur.20334
27. van Harten PN, Walther S, Kent JS, Sponheim SR, Mittal VA. The clinical and prognostic value of motor abnormalities in psychosis, and the importance of instrumental assessment. Neurosci Biobehav Rev. (2017) 80:476–87. doi: 10.1016/j.neubiorev.2017.06.007
28. Perez-Marcos D, Bieler-Aeschlimann M, Serino A. Virtual reality as a vehicle to empower motor-cognitive neurorehabilitation. Front Psychol. (2018) 9:2120. doi: 10.3389/fpsyg.2018.02120
29. Perez-Marcos D, Solazzi M, Steptoe W, Oyekoya O, Frisoli A, Weyrich T, et al. A fully immersive set-up for remote interaction and neurorehabilitation based on virtual body ownership. Front Neurol. (2012) 3:110. doi: 10.3389/fneur.2012.00110
30. Parsons TD, Phillips AS. Virtual reality for psychological assessment in clinical practice. Pract Innov. (2016) 1:197. doi: 10.1037/pri0000028
31. Sanchez-Vives MV, Slater M. From presence to consciousness through virtual reality. Nat Rev Neurosci. (2005) 6:332–39. doi: 10.1038/nrn1651
32. Spanlang B, Normand J-M, Borland D, Kilteni K, Giannopoulos E, Pomés A, et al. How to build an embodiment lab: achieving body representation illusions in virtual reality. Front Robot AI. (2014) 1:9. doi: 10.3389/frobt.2014.00009
33. Kilteni K, Groten R, Slater M. The sense of embodiment in virtual reality. PRESENCE Teleoperat Virtual Environ. (2012) 21:373–87. doi: 10.1162/PRES_a_00124
34. Maselli A, Slater M. The building blocks of the full body ownership illusion. Front Hum Neurosci. (2013) 7:83. doi: 10.3389/fnhum.2013.00083
35. Slater M, Spanlang B, Sanchez-Vives MV, Blanke O. First person experience of body transfer in virtual reality. PLoS ONE. (2010) 5:e10564. doi: 10.1371/journal.pone.0010564
36. Freeman D, Reeve S, Robinson A, Ehlers A, Clark D, Spanlang B, et al. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol Med. (2017) 47:2393–400. doi: 10.1017/S003329171700040X
37. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59(Suppl. 20):22–33.
38. Vanbellingen T, Kersten B, Van Hemelrijk B, Van De Winckel A, Bertschi M, Müri R, et al. Comprehensive assessment of gesture production: a new test of upper limb apraxia (TULIA). Eur J Neurol. (2010) 17:59–66. doi: 10.1111/j.1468-1331.2009.02741.x
39. Bachofner H, Scherer KA, Vanbellingen T, Bohlhalter S, Stegmayer K, Walther S. Validation of the Apraxia Screen TULIA (AST) in Schizophrenia. Neuropsychobiology. (2022) 81:311–21. doi: 10.1159/000523778
40. Kirkpatrick B, Strauss GP, Nguyen L, Fischer BA, Daniel DG, Cienfuegos A, et al. The brief negative symptom scale: psychometric properties. Schizophr Bull. (2011) 37:300–5. doi: 10.1093/schbul/sbq059
41. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
42. Kircher T, Krug A, Stratmann M, Ghazi S, Schales C, Frauenheim M, et al. A rating scale for the assessment of objective and subjective formal Thought and Language Disorder (TALD). Schizophr Res. (2014) 160:216–21. doi: 10.1016/j.schres.2014.10.024
43. Guy W. ECDEU Assessment Manual for Psychopharmacology. Rockville, MD: US Department of Health, Education, and Welfare, Public Health Service (1976). doi: 10.1037/e591322011-001
44. Bush G, Fink M, Petrides G, Dowling F, Francis A. Catatonia. I. Rating scale and standardized examination. Acta Psychiatr Scand. (1996) 93:129–36. doi: 10.1111/j.1600-0447.1996.tb09814.x
45. Buchanan RW, Heinrichs DW. The Neurological Evaluation Scale (NES): a structured instrument for the assessment of neurological signs in schizophrenia. Psychiatry Res. (1989) 27:335–50. doi: 10.1016/0165-1781(89)90148-0
46. Dantchev N, Widlocher DJ. The measurement of retardation in depression. J Clin Psychiatry. (1998) 59:19–25.
48. Pavlidou A, Schnitzler A, Lange J. Distinct spatio-temporal profiles of beta-oscillations within visual and sensorimotor areas during action recognition as revealed by ME. Cortex. (2014) 54:106–16. doi: 10.1016/j.cortex.2014.02.007
49. Pavlidou A, Schnitzler A, Lange J. Interactions between visual and motor areas during the recognition of plausible actions as revealed by magnetoencephalography. Hum Brain Mapp. (2014) 35:581–92. doi: 10.1002/hbm.22207
50. Pavlidou A, Gallagher M, Lopez C, Ferre ER. Let's share our perspectives, but only if our body postures match. Cortex. (2019) 119:575–9. doi: 10.1016/j.cortex.2019.02.019
51. Samson D, Apperly IA, Braithwaite JJ, Andrews BJ, Bodley Scott ES. Seeing it their way: evidence for rapid and involuntary computation of what other people see. J Exp Psychol Hum Percept Perform. (2010) 36:1255. doi: 10.1037/a0018729
52. Mueller DR, Schmidt SJ, Roder V. One-year randomized controlled trial and follow-up of integrated neurocognitive therapy for schizophrenia outpatients. Schizophr Bull. (2015) 41:604–16. doi: 10.1093/schbul/sbu223
53. Corcoran R, Mercer G, Frith CD. Schizophrenia, symptomatology and social inference: investigating “theory of mind” in people with schizophrenia. Schizophr Res.(1995) 17:5–13. doi: 10.1016/0920-9964(95)00024-G
54. Nuechterlein KH, Green MF, Kern RS, Baade LE, Barch DM, Cohen JD, et al. The MATRICS Consensus Cognitive Battery, part 1: test selection, reliability, and validity. Am J Psychiatry. (2008) 165:203–13. doi: 10.1176/appi.ajp.2007.07010042
55. Mozaz M, Rothi LJG, Anderson JM, Crucian GP, Heilman KM. Postural knowledge of transitive pantomimes and intransitive gestures. J Int Neuropsychol Soc. (2002) 8:958–62. doi: 10.1017/S1355617702870114
56. R. Rosenthal. Sensitivity to Nonverbal Communication: The PONS Test. Baltimore, MD: Johns Hopkins University Press (1978). doi: 10.1016/B978-0-12-761350-5.50012-4
57. Endicott J, Spitzer RL, Fleiss JL, Cohen J. The global assessment scale: a procedure for measuring overall severity of psychiatric disturbance. Arch Gen Psychiatry. (1976) 33:766–71. doi: 10.1001/archpsyc.1976.01770060086012
58. Schneider LC, Struening EL. SLOF: a behavioral rating scale for assessing the mentally ill. Soc Work Res Abstr. (1983) 19:9–21. doi: 10.1093/swra/19.3.9
59. Morosini PL, Magliano L, Brambilla LA, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social funtioning. Acta Psychiatr Scand. (2000) 101:323–9. doi: 10.1034/j.1600-0447.2000.101004323.x
60. Mausbach BT, Depp CA, Bowie CR, Harvey PD, McGrath JA, Thronquist MH, et al. Sensitivity and specificity of the UCSD Performance-based Skills Assessment (UPSA-B) for identifying functional milestones in schizophrenia. Schizophr Res. (2011) 132:165–70. doi: 10.1016/j.schres.2011.07.022
61. Nagels A, Kircher T, Steines M, Grosvald M, Straube B. A brief self-rating scale for the assessment of individual differences in gesture perception and production. Learn Individ Diff. (2015) 39:73–80. doi: 10.1016/j.lindif.2015.03.008
62. Banakou D, Slater M. Body ownership causes illusory self-attribution of speaking and influences subsequent real speaking. Proc Natl Acad Sci USA. (2014) 111:17678–83. doi: 10.1073/pnas.1414936111
63. Dollfus S, Mach C, Morello R. Self-evaluation of negative symptoms * : a novel tool to assess negative symptoms. Schizophr Bull. (2015) 42:571–8. doi: 10.1093/schbul/sbv161
64. Kotzeva A, Mittal D, Desai S, Judge D, Samanta K. Socioeconomic burden of schizophrenia: a targeted literature review of types of costs and associated drivers across 10 countries. J Med Econ. (2023) 26:70–83. doi: 10.1080/13696998.2022.2157596
65. Vanbellingen T, Pastore-Wapp M, Kubel S, Nyffeler T, Schupfer AC, Kiefer C, et al. Interhemispheric facilitation of gesturing: a combined theta burst stimulation and diffusion tensor imaging study. Brain Stimul. (2020) 13:457–63. doi: 10.1016/j.brs.2019.12.013
66. Walther S, Kunz M, Muller M, Zurcher C, Vladimirova I, Bachofner H, et al. Single session transcranial magnetic stimulation ameliorates hand gesture deficits in schizophrenia. Schizophr Bull. (2020) 46:286–93. doi: 10.1093/schbul/sbz078
67. Walther S, Alexaki D, Schoretsanitis G, Weiss F, Vladimirova I, Stegmayer K, et al. Inhibitory repetitive transcranial magnetic stimulation to treat psychomotor slowing: a transdiagnostic, mechanism-based randomized double-blind controlled trial. Schizophr Bull Open. (2020) 1:sgaa020. doi: 10.1093/schizbullopen/sgaa020
68. Chapellier V, Pavlidou A, Mueller DR, Walther S. Brain stimulation and group therapy to improve gesture and social skills in schizophrenia-the study protocol of a randomized, sham-controlled, three-arm, double-blind trial. Front Psychiatry. (2022) 13:909703. doi: 10.3389/fpsyt.2022.909703
69. Mueller DR, Roder V. Integrated psychological therapy for schizophrenia patients. Expert Rev Neurother. (2007) 7:1–3. doi: 10.1586/14737175.7.1.1
70. Morin L, Franck N. Rehabilitation interventions to promote recovery from schizophrenia: a systematic review. Front Psychiatry. (2017) 8:100. doi: 10.3389/fpsyt.2017.00100
71. Kopelowicz A, Liberman RP, Zarate R. Recent advances in social skills training for schizophrenia. Schizophr Bull. (2006) 32:S12–23. doi: 10.1093/schbul/sbl023
72. Riedl L, Nagels A, Sammer G, Straube B. A multimodal speech-gesture training intervention for patients with schizophrenia and its neural underpinnings – the study protocol of a randomized controlled pilot trial. Front Psychiatry. (2020) 11:110. doi: 10.3389/fpsyt.2020.00110
73. Riedl L, Nagels A, Sammer G, Choudhury M, Nonnenmann A, Sütterlin A, et al. Multimodal speech-gesture training in patients with schizophrenia spectrum disorder: effects on quality of life and neural processing. Schizophr Res. (2022) 246:112–25. doi: 10.1016/j.schres.2022.06.009
74. Cieślik B, Mazurek J, Rutkowski S, Kiper P, Turolla A, Szczepańska-Gieracha J. Virtual reality in psychiatric disorders: a systematic review of reviews. Complement Ther Med. (2020) 52:102480. doi: 10.1016/j.ctim.2020.102480
75. Goudman L, Jansen J, Billot M, Vets N, De Smedt A, Roulaud M, et al. Virtual reality applications in chronic pain management: systematic review and meta-analysis. JMIR Serious Games. (2022) 10:e34402. doi: 10.2196/34402
76. Tieri G, Morone G, Paolucci S, Iosa M. Virtual reality in cognitive and motor rehabilitation: facts, fiction and fallacies. Expert Rev Med Devices. (2018) 15:107–17. doi: 10.1080/17434440.2018.1425613
77. du Sert OP, Potvin S, Lipp O, Dellazizzo L, Laurelli M, Breton R, et al. Virtual reality therapy for refractory auditory verbal hallucinations in schizophrenia: a pilot clinical trial. Schizophr Res. (2018) 197:176–81. doi: 10.1016/j.schres.2018.02.031
78. Moritz S, Voigt M, Köther U, Leighton L, Kjahili B, Babur Z, et al. Can virtual reality reduce reality distortion? Impact of performance feedback on symptom change in schizophrenia patients. J Behav Ther Exp Psychiatry. (2014) 45:267–71. doi: 10.1016/j.jbtep.2013.11.005
79. Rus-Calafell M, Garety P, Sason E, Craig TJ, Valmaggia LR. Virtual reality in the assessment and treatment of psychosis: a systematic review of its utility, acceptability and effectiveness. Psychol Med. (2018) 48:362–91. doi: 10.1017/S0033291717001945
80. Valmaggia LR, Day F, Rus-Calafell M. Using virtual reality to investigate psychological processes and mechanisms associated with the onset and maintenance of psychosis: a systematic review. Soc Psychiatry Psychiatr Epidemiol. (2016) 51:921–36. doi: 10.1007/s00127-016-1245-0
81. Adery LH, Ichinose M, Torregrossa LJ, Wade J, Nichols H, Bekele E, et al. The acceptability and feasibility of a novel virtual reality based social skills training game for schizophrenia: preliminary findings. Psychiatry Res. (2018) 270:496–502. doi: 10.1016/j.psychres.2018.10.014
82. Schmidt RA, Lee TD, Winstein C, Wulf G, Zelaznik HN. Motor control and learning: a behavioral emphasis. Hum Kinet. (2018).
83. Levac DE, Sveistrup H. Motor learning and virtual reality. In:Weiss PL, Keshner EA, Levin MF, , editors. Virtual Reality for Physical and Motor Rehabilitation. New York, NY: Springer New York (2014). doi: 10.1007/978-1-4939-0968-1_3
84. Pavlidou A, Walther S. Using virtual reality as a tool in the rehabilitation of movement abnormalities in schizophrenia. Front Psychol. (2020) 11:607312. doi: 10.3389/fpsyg.2020.607312
85. Banakou D, Beacco A, Neyret S, Blasco-Oliver M, Seinfeld S, Slater M. Virtual body ownership and its consequences for implicit racial bias are dependent on social context. R Soc Open Sci. (2020) 7:201848. doi: 10.1098/rsos.201848
86. Banakou D, Hanumanthu PD, Slater M. Virtual embodiment of white people in a black virtual body leads to a sustained reduction in their implicit racial bias. Front Hum Neurosci. (2016) 10:601. doi: 10.3389/fnhum.2016.00601
87. Peck TC, Seinfeld S, Aglioti SM, Slater M. Putting yourself in the skin of a black avatar reduces implicit racial bias. Conscious Cogn. (2013) 22:779–87. doi: 10.1016/j.concog.2013.04.016
88. Pavlidou A, Viher PV, Bachofner H, Weiss F, Stegmayer K, Shankman SA, et al. Hand gesture performance is impaired in major depressive disorder: a matter of working memory performance? J Affect Disord. (2021) 292:81–8. doi: 10.1016/j.jad.2021.05.055
89. Suffel A, Nagels A, Steines M, Kircher T, Straube B. Feeling addressed! The neural processing of social communicative cues in patients with major depression. Hum Brain Mapp. (2020) 41:3541–54. doi: 10.1002/hbm.25027
90. Gillissie ES, Lui LMW, Ceban F, Miskowiak K, Gok S, Cao B, et al. Deficits of social cognition in bipolar disorder: systematic review and meta-analysis. Bipolar Disord. (2022) 24:137–48. doi: 10.1111/bdi.13163
Keywords: virtual reality, schizophrenia, gesture performance, social communication, social cognition
Citation: Pavlidou A, Gorisse G, Banakou D and Walther S (2023) Using virtual reality to assess gesture performance deficits in schizophrenia patients. Front. Psychiatry 14:1191601. doi: 10.3389/fpsyt.2023.1191601
Received: 22 March 2023; Accepted: 22 May 2023;
Published: 09 June 2023.
Edited by:
Matthew J. Smith, University of Michigan, United StatesReviewed by:
Lindsay A. Bornheimer, University of Michigan, United StatesCopyright © 2023 Pavlidou, Gorisse, Banakou and Walther. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anastasia Pavlidou, YW5hc3Rhc2lhLnBhdmxpZG91QHVwZC51bmliZS5jaA==; cGF2bGlkb3UuYW5hc3Rhc2lhQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.