 Assia Boudjerida
Assia Boudjerida Jean-Marc Guilé
Jean-Marc Guilé Jean-Jacques Breton
Jean-Jacques Breton Xavier Benarous
Xavier Benarous David Cohen
David Cohen Réal Labelle
Réal Labelle- 1Department of Psychology and Centre for Research and Intervention on Suicide, Ethical Issues and End-of-Life Practices, Université du Québec à Montréal, Montréal, QC, Canada
- 2Department Head, Child and Adolescent Psychiatry, EPSM Somme and CHU Amiens, Picardie Jules Verne University, Amiens, France
- 3Department of Psychiatry, Rivière-des-Prairies Mental Health Hospital, Université de Montréal, Montréal, QC, Canada
- 4Department of Child and Adolescent Psychopathology CHU Amiens-Picardie, Amiens, France
- 5Department Head, Child and Adolescent Psychiatry, Public Assistance-Hospitals of Paris, APHP, Pitié-Salpêtrière Hospital Group and National Center for Scientific Research-Joint Research Unit, Institute for Intelligent and Robotic Systems Sorbonne Université, Paris, France
Objective: The aim of this study was to explore consensus among clinicians and researchers on how to assess and treat Disruptive Mood Dysregulation Disorder (DMDD).
Methods: The Delphi method was used to organize data collected from an initial sample of 23 child psychiatrists and psychologists. Three rounds of closed/open questions were needed to achieve the objective.
Results: Fifteen experts in the field completed the whole study. Finally, 122 proposals were validated and 5 were rejected. Globally, consensus was more easily reached on items regarding assessment than on those regarding treatment. Specifically, experts agreed that intensity, frequency, and impact of DMDD symptoms needed to be measured across settings, including with parents, siblings, peers, and teachers. While a low level of consensus emerged regarding optimal pharmacological treatment, the use of psychoeducation, behavior-focused therapies (e.g., dialectical behavior therapy, chain analysis, exposure, relaxation), and systemic approaches (parent management training, family therapy, parent–child interaction therapy) met with a high degree of consensus.
Conclusion: This study presents recommendations that reached a certain degree of consensus among researchers and clinicians regarding the assessment and treatment of youths with DMDD. These findings may be useful to clinicians working with this population and to researchers since they also highlight non-consensual areas that need to be further investigated.
Introduction
Disruptive Mood Dysregulation Disorder (DMDD) was coined as a separate diagnostic entity in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). The disorder’s main criterion is persistently irritable mood punctuated by recurrent, intense temper outbursts and the diagnosis should be made for the first time between ages 6 and 18 years (see Table 1 for a summary of the DSM-5 criteria). The disorder’s prevalence in the general population has been estimated at 2.5% (1–4). This diagnosis came into being in the wake of the controversy concerning the surge in pediatric bipolar disorder (PBD) diagnoses in the United States.
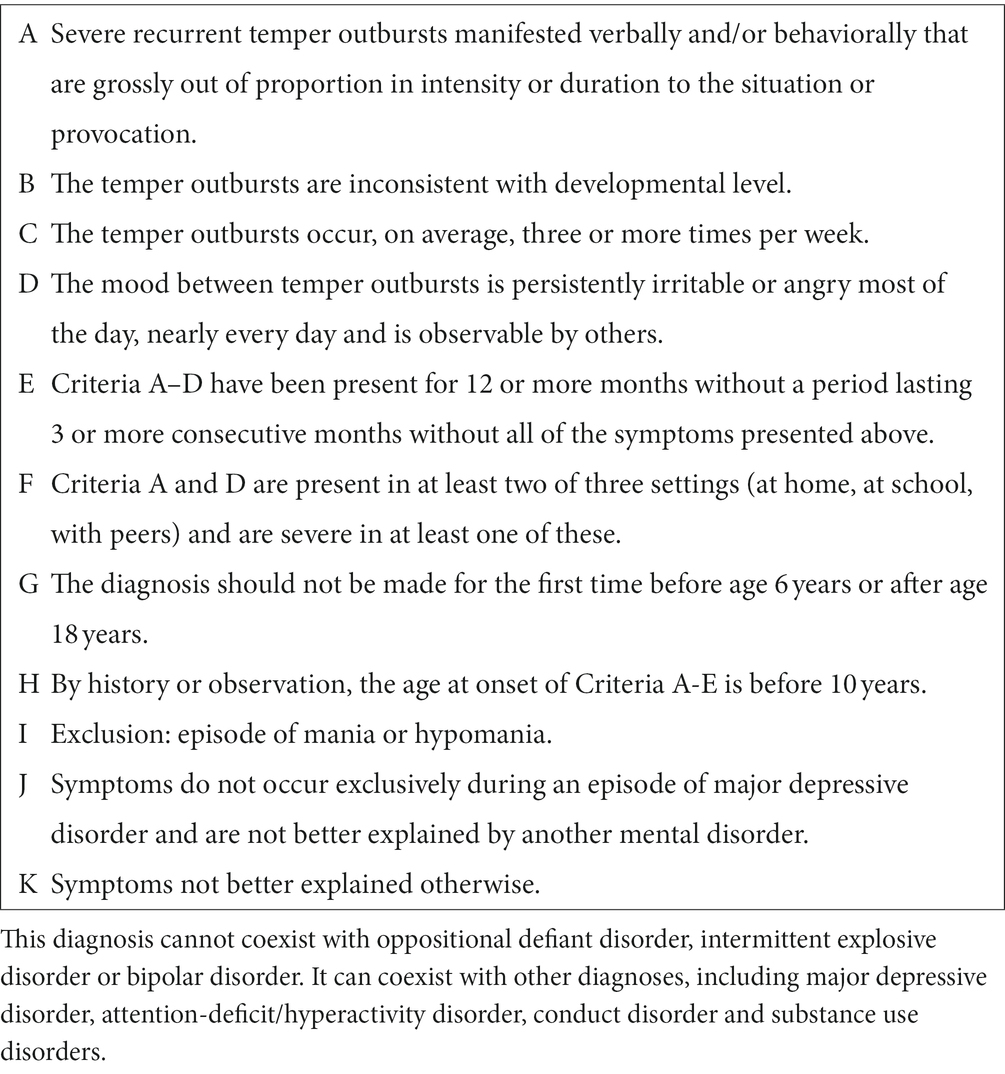
Table 1. Diagnostic criteria for DMDD.
PBD was first proposed in 1995 by researchers who were keen to identify this disorder early and who postulated that mania might occur in early childhood but differently from adulthood. The research hypothesis presented two phenotypes: multiple mood episodes per day (5) or chronic irritability generally without elevated mood (6). Whereupon, according to Moreno et al. (7), the number of medical visits associated with bipolar disorder diagnoses in children had increased fortyfold from 1994 to 2003. Some authors indicate that “the increase in rates of bipolar disorder in children has been controversial and it remains unclear whether this trend represented an increase in recognition, an increase in incidence, or a broadening of the application of the diagnostic criteria” (8). Yet, the PBD diagnostic increase remains mostly confined to the United States (9). Some explanations can be given. First, it seems that in the United States, diagnoses of more serious conditions allow for greater reimbursement and access to resources than less serious ones (9). Therefore, if in doubt, it seems more useful to diagnose a PBD than an oppositional defiant disorder (ODD) for example. Second, the PBD increase could also reflect the problem of reification. It’s a cognitive bias which consists in considering an abstract idea as a concrete entity. Some researchers evoke that the model of the DSM developed to foster interrater reliability facilitates reification, which leads to a false sense of validity (10).
Nevertheless, in 2003, Leibenluft and colleagues at the National Institute of Mental Health (NIMH) proposed a series of studies to document the links between chronic irritability and bipolar disorder (11). Research on this controversy was largely motivated by its treatment implications (12). These researchers, named the syndrome “Severe Mood Dysregulation” (SMD) to identify children with chronic irritability associated with temper outbursts and non-episodic symptoms. In a systematic review, this team concluded that chronic irritability in childhood was not a symptom associated with bipolar disorder but rather unipolar disorder (13). Which should lead to a considerable paradigm shift for treatments. Thus the DSM-5 Task Force (1) deemed the NIMH studies to be sufficiently conclusive to include SMD as a new diagnostic entity among mood disorder under a new name: Disruptive Mood Dysregulation Disorder (14). DMDD was placed in the depressive disorders section based on a series of arguments that underscored its continuity with depression in adulthood in terms of family history, neurocognitive disturbances, genetic factors and, particularly, on outcome studies (13, 15).
However, DMDD’s validity as an independent diagnostic entity has been questioned for different reasons. First, the extrapolation of data on SMD to DMDD is not necessarily obvious. A study showed that only 58% of young people with SMD also met the criteria for DMDD, and only 47% of those with DMDD met the criteria for SMD (4). Second, a study on DSM-5 field trials indicated that DMDD has low level of evidence on the temporal stability of symptoms and the reliability of diagnostic criteria (16). Third, the very high level of comorbidity of DMDD with other psychiatric disorders (varies between 60 and 95% according to certain studies) (17) is an important limit to the validity of the diagnosis. In fact, the main criteria of DMDD (outbursts and irritability) are also found in other disorders (ODD, attention-deficit/hyperactivity disorder, anxiety, depression) which complicates things. Hence, some authors suggest that “This lack of phenomenological distinction means that the diagnosis has failed to achieve its primary goal, namely, to inform treatment” (18). In fact, alternatively to DMDD’s diagnosis, in ICD-11, chronic irritability accompanied by outbursts, is more of a specifier in ODD (19). Additionally, outbursts are core symptoms in intermittent explosive disorder (IED) in both DSM-5 and ICD-11. Thus, several experts in the field of irritability indicate that “The lack of a standard definition or diagnostic home has relegated outbursts to nosological orphanhood” (20). It is therefore a fairly recent and still evolving field of study.
Even so, in clinical practice, youths who fit the DMDD profile have recurrent temper outbursts that have a real impact on the quality of their family and peer relationships, and on their academic performance (1). They often present comorbidities, particularly neurodevelopmental disabilities (e.g., Attention deficit with or without hyperactivity-ADHD) (21, 22). Children with DMDD experience a higher level of social problems and are more often suspended from school than other students are (3). Moreover, compared with youths with other psychopathologies, they are more likely to report impairment in activities of daily life and more suicidal ideation and behaviors (2). Finally, youths with DMDD make greater use of health services (23). The addition of this diagnosis to the DSM-5 (1) and the knowledge about the individual and collective burden associated with this disorder have led us to explore how clinicians and researchers perceive, assess and treat these youths. Ten years after the publication of the latest DSM, there is still no consensus in this regard (24).
As controversies remain on the diagnostic and therapeutic approaches that should be prioritized in the care of DMDD patients, the current study focusses on expert’ opinions. Our goal was to combine the experiences of these professionals to offer consensual recommendations on DMDD.
Materials and methods
The Delphi method
The Delphi method serves to collect the opinions of experts on a specific subject. It has been used to build a consensus among experts on numerous clinical protocols and has proved effective in the field of mental health (25). The idea is to query a group of experts by way of self-administered questionnaires, in an iterative and interactive manner, without any direct communication between them (26–28). Moreover, it is a simple, cost-effective, flexible method that eliminates geographical boundaries, enables knowledge sharing, and allows freedom of expression through the use of anonymity (29). Under the classic version of the method, experts are queried four times (30), first through open-ended questions on a given issue and then through closed-ended questions (31). However, to minimize time burden and participant attrition, many authors have proposed cutting the rounds of questioning to two or three (32–34). For the purposes of our study, we opted for three rounds.
The scientific literature does not propose any guidelines regarding the number of participants that should be involved (25). This depends on several factors, including the characteristics of the subject under investigation and the number of experts potentially available (35). Many exponents of the Delphi method, including Parenté and Anderson-Parenté (36) and Linstone and Turoff (27), have deemed a minimum of 10 participants to be enough when the sample is a rather homogenous group of experts. Other authors have suggested involving from 8 to 12 participants for a panel of specialized experts (37, 38). In our study, all of the participants recruited were either psychiatrists or psychologists and experts in the field. They constituted a fairly uniform group.
Definition of consensus
To date, there are no clear guidelines regarding the definition of consensus (35). Some researchers have deemed a consensus reached with 51% of respondents in agreement whereas others have placed the bar at 70% or 80% (39). According to Sumsion (40) and McKenna, Hasson (41), for example, 70% of respondents in agreement would constitute a sufficiently strong consensus. The literature recommends, also, using a Likert scale and measures of central tendency, such as the median, to give participants feedback, regardless of how consensus is defined (42–44). These elements were taken into consideration in conducting our study.
Procedure
First, few months before beginning the study, a pilot run was carried out to test the use of the online platform and fine-tuning the wording of questions in English and French as previously recommended (35, 39, 45). For the first round, in order to reproduce the concept of brainstorming, as recommended in the Delphi Method (46), four open-ended questions were formulated as follows: (i) Name at least three key elements that you consider essential for an effective assessment of DMDD; (ii) Name at least three key elements of pharmacological intervention for DMDD; (iii) Name at least three key elements of psychosocial intervention for DMDD; (iv) Name at least three main targets of intervention for DMDD. A dozen student-researchers completed the first two rounds of the survey and evaluated the questionnaires in terms of design and clarity. Minor changes were made to the questionnaires thanks to this feedback. For example, comment boxes were added at various points to catch participants’ reactions and opinions. According to Tremblay-Boudreault and Dionne (47), such adaptations tends to enhance the overall level of experts’ participation.
Next, three-round survey was carried out online from July 2021 to May 2022. In the first round, participants received a questionnaire with three parts: (i) consent form; (ii) list of sociodemographic information; and (iii) four open-ended questions on assessment and intervention practices. Thus, the experts could identify what, in their opinion, were the key elements in the assessment and treatment of DMDD. In the second round, participants received a list of items proposing different practices based on the responses collected in the first round. They were asked to rate how much they agreed with these proposals. Items where a consensus (in agreement or disagreement) existed were then either retained or rejected. In the third round, participants were asked to re-assess how much they agreed with items on which there was no consensus after being informed of where the group stood (median) on these following the second round.
Participants
Participants had to meet three criteria: (i) to be a psychiatrist or psychologist; (ii) to have had an article published in a scientific journal about DMDD or to self-identify as treating youths with main symptoms of DMDD (criterion A, C, and D; see Table 1 for a summary of the criteria); and (iii) to be fluent in English or French. Potential participants were identified through existing publications on the subject of DMDD and snowball sampling. In other words, participants selected on the basis of publications were asked to recommend colleagues who also worked with this client group (48). In the end, 103 experts were solicited by email.
Ethical considerations
In the first round of the study, prior to any question, participants had to confirm having read the consent form, indicate that they met the inclusion criteria, and declare no conflict of interest. In this regard, each expert was informed in writing that he could not receive a benefit (financial, moral or professional) from a third party (pharmaceutical company or health company) in the choice of the selected proposals. In fact, the only contribution, but still valuable, was to advance knowledge. Then, participants could choose whether to be named and thanked in articles derived from the study. This was meant as a token of appreciation for their time spent on the project. The experts were free to withdraw from the study at any time without justification. The project was approved by the Human Research Ethics Board of Université du Québec à Montréal, in Canada (Approval no. 4953).
Descriptive statistics
The questionnaires were hosted on LimeSurvey, a free and open source online statistical survey web app, and statistical analyses were performed using Microsoft Excel. The open-ended responses in the first round were subjected to conventional content analysis (49, 50). Accordingly, they were parsed and grouped under themes that emerged during data analysis. An independent researcher with no connection to this study repeated the data analysis process for the purpose of assessing inter-judge agreement (51). This allowed us to create the short proposals that were rated in the second round. Participants had to indicate how much they agreed with each item on a five-point Likert scale, though they could abstain from responding if they wanted. Statistical analyses in the second round consisted in assessing level of agreement among participants. For the purposes of our study, items were retained by consensus when at least 70% of the participants responded agree or strongly agree (41). Items were rejected by consensus when at least 70% of the participants responded disagree or strongly disagree. Otherwise, items were considered equivocal and were re-assessed in the third round. Items could be considered equivocal also if the group median fell close to the neutral position on the Likert scale. Figure 1 illustrates the criteria used to determine consensus. These analyses were repeated after the third round.
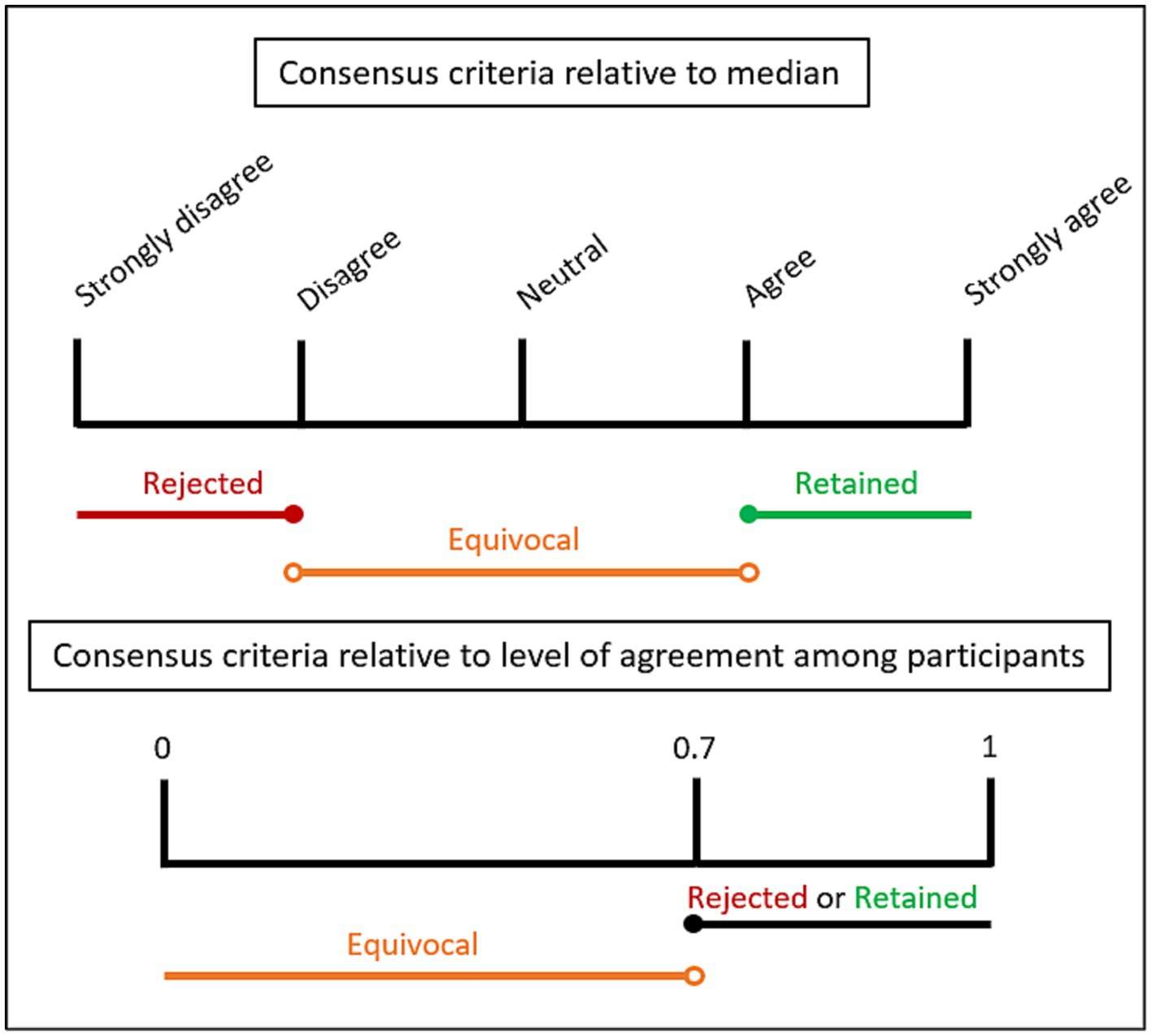
Figure 1. Consensus level criteria.
Results
1st round
Of the 103 experts contacted, 23 completed the first round of the study and, of these, 43% were women. The majority of the respondents were psychiatrists (70%) and the rest were fully qualified psychologists. Furthermore, 70% of the experts were both researchers and clinicians, 17% did research only, and 13% were clinical practitioners only. Moreover, 87% worked in the public sector, part of which have a dual private-public practice. Regarding years of practice, 13% of respondents reported less than 5 years, 43% reported 5–14 years, 22% reported 15–24 years, and 22% reported 25 years or more. Finally, participants came from eight different countries: United States (n = 8), Canada (n = 4), France (n = 4), Australia (n = 2), Turkey (n = 2), Switzerland (n = 1), Ireland (n = 1), and Brazil (n = 1). Figure 2 is a flowchart showing participant retention and number of proposals retained after each round. The responses provided by the experts allowed us to formulate 160 proposals regarding DMDD. Of these, 40 related to assessment, 112 to treatment (26 to intervention targets, 40 to psychosocial interventions, and 46 to pharmacological interventions), and 8 to general comments.
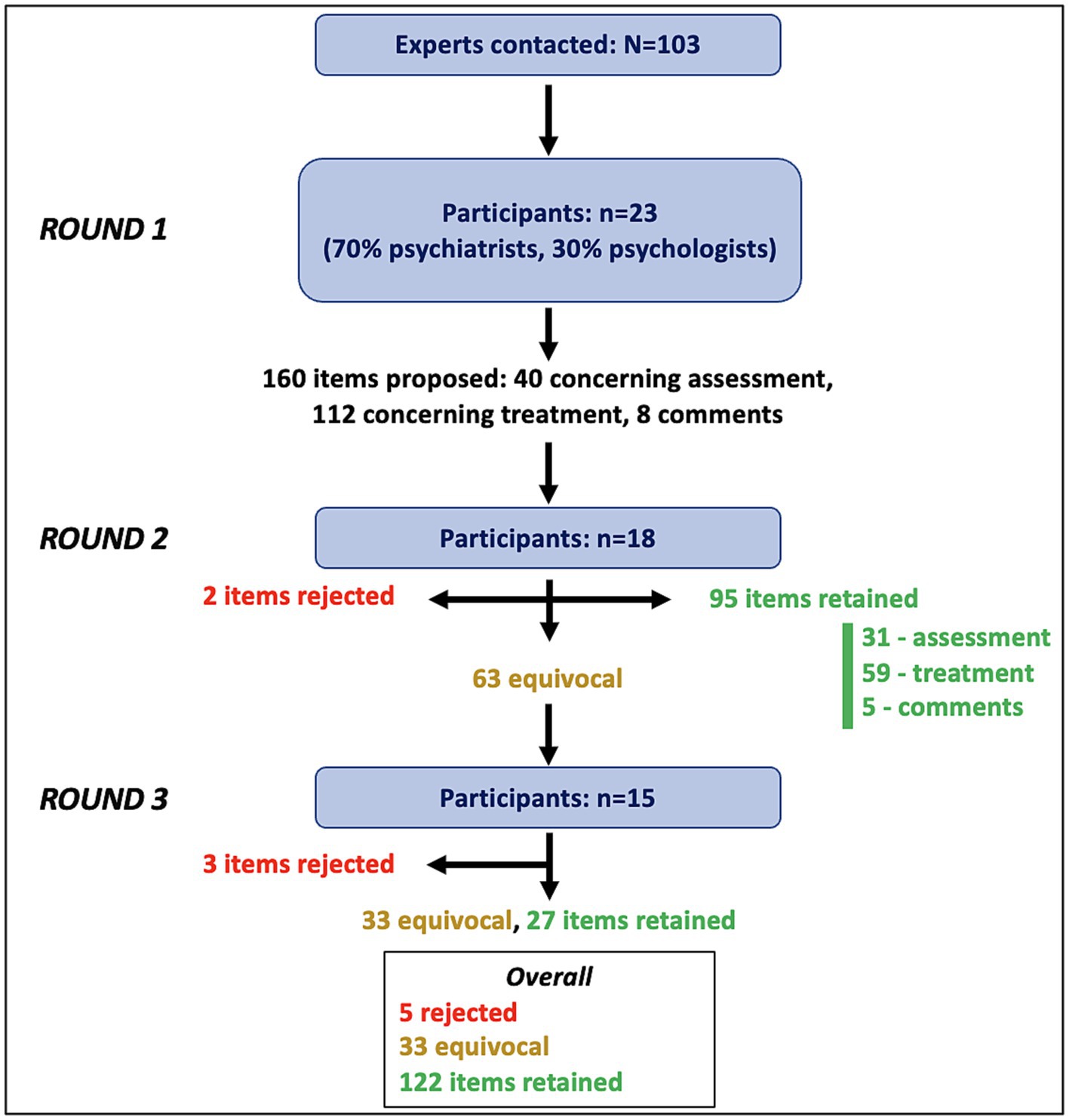
Figure 2. Flowchart illustrating three rounds of survey.
2nd round
Eighteen of the 23 experts completed the second round, for a retention rate of 78%. Of these, 39% were women, 61% were psychiatrists, 72% of the experts were both researchers and clinicians, 22% did research only, and 6% were clinical practitioners only and 89% worked in the public sector. Regarding years of practice, 11% of respondents reported less than 5 years, 50% reported 5–14 years, 17% reported 15–24 years, and 22% reported 25 years or more. Finally, there are still participants from the 8 countries named above. Of 160 proposals submitted, 95 were retained and 2 were rejected by consensus. The other 63 items were considered equivocal and were submitted again in the third round. More specifically, the vast majority of the assessment items were retained (31/40). Where treatment was concerned, aside from the item regarding sensorimotor integration, the proposals regarding intervention targets were all retained (25/26). As for psychosocial interventions, responses were rather mixed: half of the items were retained and the other half were equivocal (20/40). Regarding pharmacological interventions, almost no item was retained other than general concepts (14/46). In this section, two items were rejected outright: use of oxcarbazepine and use of lithium. Finally, a few comments were retained following this round (5/8).
3rd and final round
Fifteen experts completed the final round of the study, which results in a retention rate of 83% relative to the second round and of 65% relative to the first. Of these, 40% were women, 60% were psychiatrists, 80% of the experts were both researchers and clinicians, 20% did research only, none were clinical practitioners only, and 87% worked in the public sector. Regarding years of practice, 7% of respondents reported less than 5 years, 53% reported 5–14 years, 13% reported 15–24 years, and 27% reported 25 years or more. At this point, there were no more experts from Brazil, so the participants came from seven different countries: United States (n = 5), Canada (n = 2), France (n = 3), Australia (n = 1), Turkey (n = 2), Switzerland (n = 1), and Ireland (n = 1). Of the 63 items proposed again in this round, 27 were retained by consensus, 33 remained equivocal, and 3 were rejected by consensus.
After the third round (Figure 2), of the 40 assessment proposals, 36 were retained. Moreover, as in the second round, of the 26 DMDD intervention targets, all were retained except for the one regarding sensorimotor integration. Of the 40 psychosocial intervention items, 32 were retained and the rest remained equivocal. Of the 46 pharmacological intervention proposals, 22 were retained and 5 were rejected. Finally, 7 of 8 comments were validated by consensus.
In sum, consensus was more easily achieved on items concerning assessment than on those concerning treatment. Specifically, the experts approved the idea that the intensity, frequency and consequences of DMDD had to be measured across different contexts (e.g., with parents, siblings, peers, teachers). The pharmacological proposals were the most controversial whereas the items regarding psychoeducation and behavioral interventions were more consensual (e.g., dialectical behavior therapy, relaxation), as were those regarding family approaches (parent management training, family therapy, therapy focused on parent–child interaction). The 122 proposals retained and the 5 rejected by the group of experts are given in Table 2, along with their respective degree of agreement. The comments, made in the free text boxes, retained by the participants are presented in Table 3 and the equivocal proposals are detailed in Table 4.

Table 2. Level of agreement on retained and rejected initial proposals.
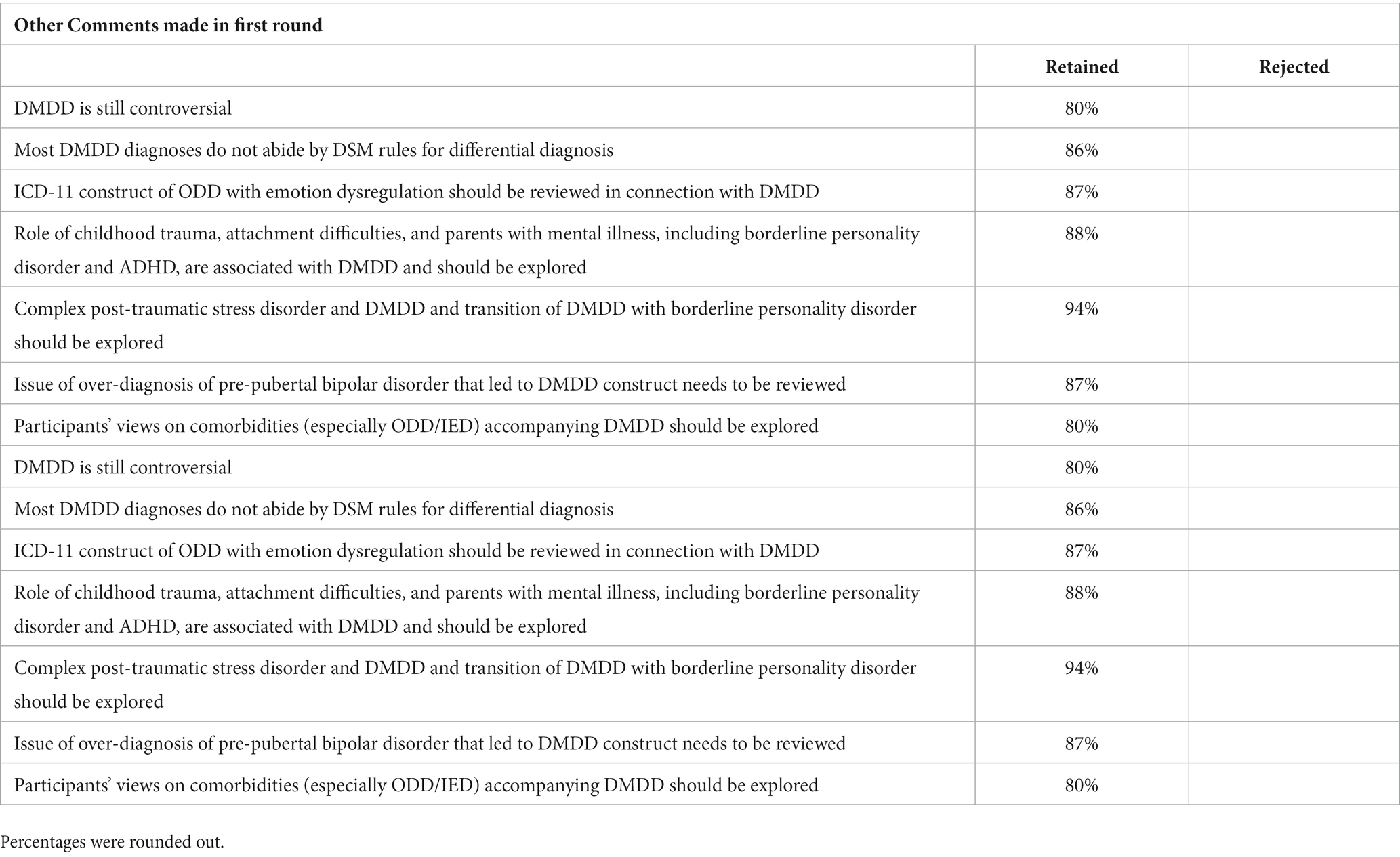
Table 3. Other comments made in first round.
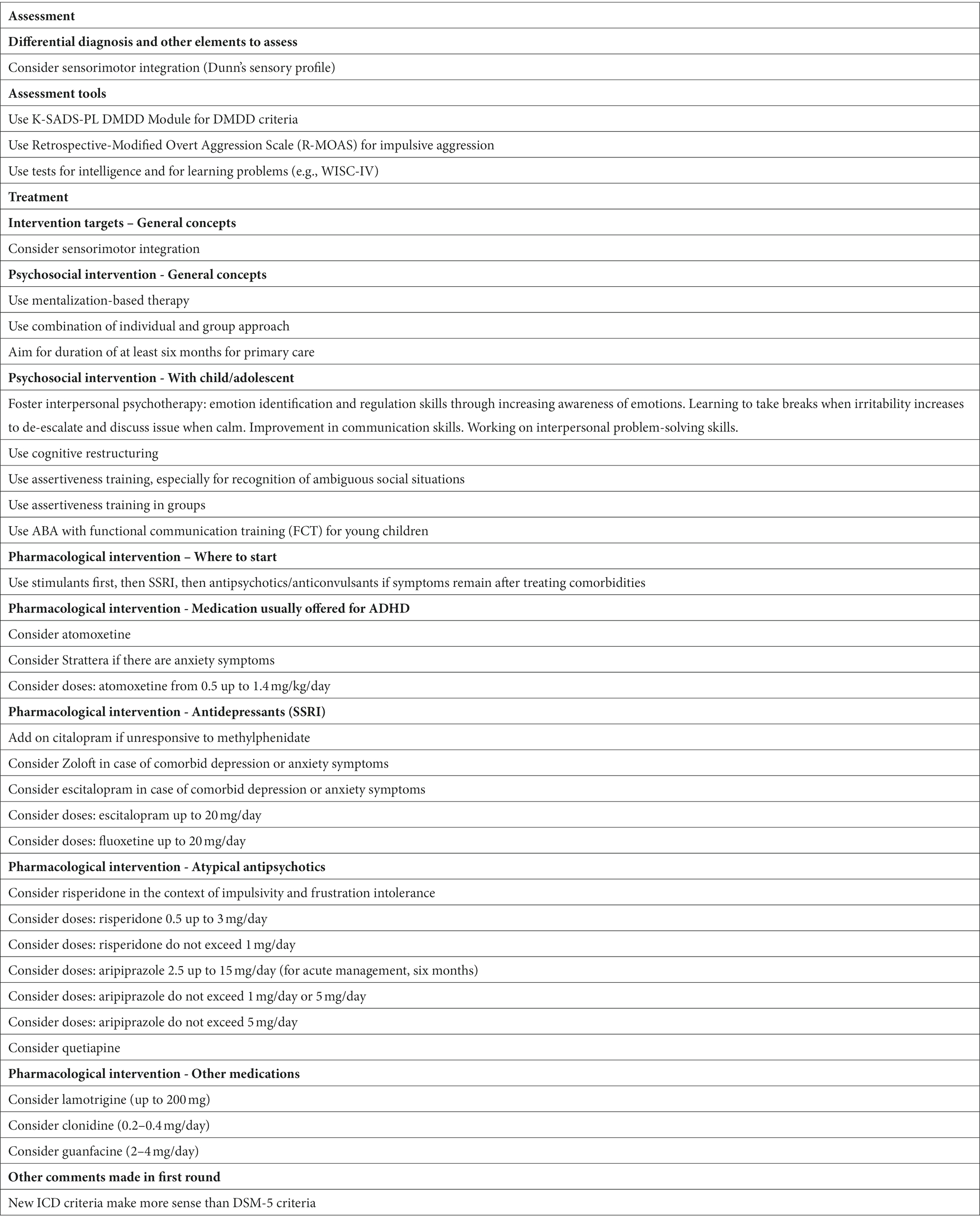
Table 4. List of equivocal proposals and other comments made in first round.
Discussion
This study presents recommendations that reached some degree of consensus among researchers and clinicians regarding the assessment and treatment of youths with DMDD. The expertise of psychiatrists and psychologists shed light on issues regarding DMDD that remain unanswered in the literature. Moreover, the equivocal proposals that emerged from our study, as well as the numerous comments formulated by the participants, are grey areas to be explored in future research (Table 4). Those findings could help improve how these youths are identified and managed.
This study is not without limitations. Above all, our group of participants was rather small and was not representative of all the mental health experts of the world. It would have been interesting to have a larger sample and to be able to examine the international differences, especially considering that the DSM-5 and the ICD offer a different understanding of symptoms. Moreover, clinicians self-identified as treating patients with core DMDD symptoms. Hence, they may vary in the amount of actual hands-on clinical experience with DMDD youth. Also, while the participation rate was adequate from one round to the next, it was difficult to recruit experts initially. Aside from the usual inherent challenges and obstacles, some professionals refused to participate on account of the debate surrounding DMDD’s validity as an independent diagnostic entity.1 Yet, it would have been extremely enlightening to gather their views, as this would certainly have nuanced certain positions. Seeing the debate still surrounding DMDD’s validity, it would benefit the scientific community to investigate this issue further.
Also, it is necessary to underscore that use of the Delphi method may result in issues being oversimplified or lacking nuance (47), as mentioned earlier. To address this issue, we added comment boxes in every section of the questionnaires. However, this generated little data, particularly in the section on pharmacological interventions. In hindsight, we might have done better to use clinical vignettes instead. Moreover, providing participants with the median score in the third round, as recommended in the Delphi Method (35), may have biased responses. Finally, as stated by Tremblay-Boudreault and Dionne (47), it is important to bear in mind that reaching a consensus does not mean that an issue has been settled once and for all. Still, the Delphi method did allow us to structure the discussion and define the remaining areas of debate (39, 52). Clearly, further research will be required to refine the results of this study. For example, future studies could examine treatment efficacy in DMDD for both psychological and pharmacological interventions.
In addition, we must keep in mind that the study was carried out over 2021 and 2022. It is possible that, in this context, major studies in the field have been published since and influence the general understanding of DMDD without this study taking account of this. Finally, the fact that this study was conducted entirely online could have hampered participation (53). Some experts might never have read our invitation to participate in the study if emails ended up among their junk mail.
Contributing to the assessment of DMDD, Mürner-Lavanchy, Kaess (54) recently published a systematic review of the psychometric instruments used. While no instrument serves as a gold standard, these authors reported several that seem useful, including the Kiddie Schedule for Affective Disorders and Schizophrenia Present and Lifetime Version, the Preschool Age Psychiatric Assessment, and the Child and Adolescent Psychiatric Assessment. However, these instruments did not meet with a consensus among our study participants, who indicated, though, that it was preferable to use clinical interviews and different validated measures.
The experts also emphasized the elements to assess, such as intensity, frequency and impact of DMDD symptoms in various contexts and relationships (e.g., parents, siblings, peers and teachers). Accordingly, it seemed appropriate to work in collaboration with the youth, the parents, and the school community. Also, participants suggest that clinicians should have access to observational reports or even to directly observe these youths in their usual environment during home-visits. Epidemiologic studies (2, 3) and clinical studies (22, 55) have found learning difficulties frequently co-occur with DMDD. Indeed, youths with severe and persistent irritability present a high rate of academic failure and learning difficulties, which justifies focusing on how they function at school (21).
Moreover, various components to be assessed regarding temper outbursts and mood (e.g., aggression, impulsivity, frustration intolerance, emotional instability). Ideally, temper outbursts should be described using a systematic approach (measuring at least the frequency, intensity, duration, triggers, environmental context, and settings). Mood, for its, part, should be observed longitudinally. In this regard, participants proposed using the Affective Reactivity Index, which has been applied in research and clinical practice to measure irritability (56). Furthermore, the families of youths who have temper outbursts tend to make accommodations to prevent these. It is important to explore caregivers’ coping strategies to DMDD symptoms, also influenced by their own emotional regulation abilities, in the course of assessment. Moreover, according to the participants, family antecedents, chronological history of mood symptoms, general functioning, and risk and protective factors, also, should be considered. To collect all of this information, it is essential for clinicians to involve in the assessment process different people who play a significant role in the life of these youths (57).
Obviously, in the course of assessment, youths should be screened more broadly for different physical and mental problems, particularly those mentioned among the DMDD exclusion criteria, namely, oppositional defiant disorder, intermittent explosive disorder, and bipolar disorder (1). According to our participants, potential contributing factors to emotion dysregulation should also be explored, including maltreatment (58), family problems (4), substance use (59), and recent negative life events (e.g., school bullying, change in custody) (60). Where differential diagnosis and comorbidities are concerned, various elements need to be taken into account: depression symptoms, suicidal behavior, sleep difficulties, anxiety symptoms, attention deficit disorder with or without hyperactivity symptoms, and comorbidity with other neurodevelopmental disorders (including specific learning disabilities). Moreover, because the idea of assessing sleep and language problems was proposed by participants in the final round of the survey, it could not be put to the rest of the group. However, it is evident that sleep difficulties (61) and language impairments (62) can have an impact on emotion regulation and the development of psychopathologies.
The section on assessment tools was the only one where no consensus was reached. Some respondents expressed a preference for clinical interviews over questionnaires. Others specified that questionnaires should be used only once potential comorbidities have been identified. In this regard, some tools, such as the Children’s Depression Rating Scale for depression symptoms (63), the Conners for ADHD symptoms (64), and the Child Behavior Checklist for emotional and behavioral problems (65) could be useful but not necessarily essential to assessing DMDD. Finally, one participant pointed out in the last round the possibility of using a questionnaire published very recently concerning DMDD specifically, namely, the Disruptive Mood Dysregulation Disorder Questionnaire (66). That said, the lack of consensus regarding evaluation tools is not a surprising finding. This issue was raised, among others, by Carlson in 1998 regarding PBD (67). She criticized the use of symptom checklists in the form of structured clinical interviews because they relied on a descriptive psychiatric paradigm that neglected contextual and developmental factors (67). According to her, a structured clinical interview could not replace longitudinal assessment with multiple informants. More recently, Galanter (68) issued the same criticisms, specifying that structured interviews “are only as good as the experience, intellect and empathic capacity of the interviewers, all of which is complicated by the perspective the interviewer has on the boundaries of bipolar disorder” (69). These critiques though related to PBD remain relevant in relation to DMDD.
Furthermore, participants proposed a four-step process for performing child psychiatric assessments: (1) interview with parents and child together; (2) meeting with parents only, preferably conducted by a different professional; (3) individual examination of child; and (4) meeting with parents and child, along with all professionals involved, to sum up the situation. This way of proceeding should be adapted to each healthcare environment.
Regarding DMDD therapy, all of the intervention targets proposed in the first round were retained, except for sensorimotor integration. The targets are presented in Table 2 by category (general concepts, emotion regulation, and interpersonal relationships). The only comment made by participants concerned the attention that should be paid to targets more specific to comorbidities. For example, if a child has comorbid DMDD and a language impairment, it is important to identify therapeutic possibilities specific to this issue.
Several experts nuanced the role of psychosocial intervention and suggested that it should apply on the results of a full-blown assessment, including developmental stage, family situation and comorbidities. Later, in comments made in the last round, several respondents expressed concerns in this regard. In the first round, some experts proposed targeted intervention techniques (e.g., chain analysis), while others recommended more comprehensive therapy programs (e.g., dialectical behavior therapy). This imbalance seemed to have bothered some participants, which might have biased part of the results. However, overall, psychoeducation, behavior-focused therapy (e.g., dialectical behavioral therapy, chain analysis, exposition, relaxation) and systemic therapy (parent management training, family therapy, parent–child interaction therapy) met consensus. Also, all proposals regarding intervention targeting parents and the family were validated by the second tour. These results echo the psychosocial interventions published in the field: interpersonal psychotherapy (70, 71), dialectical behavior therapy (72), cognitive behavioral therapy (73, 74), parent management training (74), anger management program (75), and Triple P – Positive Parenting Program (76). However, these intervention programs have their pros and cons. For example, they are more or less structured, they are more or less available in the community. Instead of adopting comprehensive intervention programs, our experts seemed to prefer using different intervention strategies depending on their patients’ needs (20), which resonates with recent proposals like those of Evans, to opt for a modular approach to treat severe irritability (77).
Other elements appeared useful to DMDD psychosocial intervention: learning emotion regulation and anger management techniques, developing coping skills. Close partnership with the school community was largely endorsed in view of generalizing learned emotional skills during therapy in children’ routine behaviors. Furthermore, our experts mentioned that the additional support of a social worker often proved useful.
One participant put forth some new ideas in the first round. He underscored the importance of establishing above all a bond of trust with the family (78). Then, he suggested addressing how to manage destructive and self-destructive behaviors with the youth in question and their family. This expert recommended using behavioral and family approaches before proposing more structured individual therapy to patients. He stressed the importance of not undertaking a structured or cognitive treatment too soon, seeing how patients were not ready emotionally to engage in the required learning (79). Also, cognitive restructuring was considered equivocal by the study participants, in addition to the duration and the format (individual/group) of intervention that should be preferred. We might imagine that these elements vary considerably across practice settings (e.g., outpatient vs. inpatient).
Regarding proposals related to pharmacological interventions, results must be interpreted with caution as this was the section with the largest number of equivocal and rejected items. First and foremost, it should be noted that only the participants who were psychiatrist were able to contribute to this part of the study. Then, the respondents themselves mentioned consensually that there was insufficient scientific evidence in this field at present to reach any decisions. They also noted that it was hard to choose the best treatment option with regard to the brevity of the assumption and the lack of context (e.g., clinical vignettes). Despite this, the experts agree on certain general guidelines. For example, it is preferable to turn to a child and adolescent psychiatrist, and if a possible a professional well-trained in pediatric mood disorders. Also, comorbidity and symptom targets can be used to guide treatment choice. Comorbidities should be treated first. For example, in the presence of comorbid ADHD, stimulants should be optimized. If DMDD is still present thereafter, other drugs may be considered as add-on. Here are the pharmacological proposals published to date regarding DMDD: stimulants (80–84), atypical antipsychotics (85, 86), mood stabilizers (84, 87), selective serotonin reuptake inhibitors (88), and atomoxetine, a selective noradrenaline reuptake inhibitor (89).
Certain drugs, such as atypical antipsychotics, mood stabilizer and anticonvulsant medications, sometimes combined (90), have been and are prescribed by proponents of PBD to reduce perceived “childhood mania” (91–94). However, since DMDD has been associated with depression, rather than bipolar disorder (13), participants appear to favor the use of SSRIs over antipsychotic. Indeed, SSRIs are a second line therapy to psychosocial interventions and medication for insomnia in youth suffering from depression, with informed consent provision about potential activation syndromes and hostility or suicidality adverse events (95). This line of reasoning follows logic and seems especially advantageous when we take into account the harmful side effects of antipsychotics on developing bodies (96, 97). Yet, the results of Findling’s study (98) are as interesting as they are worrying. The authors state that “Diagnosis of DMDD has had rapid uptake in clinical practice but is associated with increased antipsychotic and polypharmacy prescriptions and higher rates of comorbidity and inpatient hospitalization in youth with a DMDD diagnosis compared with a PBD diagnosis.” The issue of pharmacological interventions for DMDD, particularly in the context of high comorbidity, really needs to be further studied. Moreover, these results seem to indicate that even though the participants in this study emphasize the use of psychosocial treatments, currently it does not seem to be the norm in mental health practice.
Other comments
All but one of the comments made in the first round, in the free text boxes, were validated by the participants. For example, they agreed that DMDD remained controversial and that most DMDD diagnoses did not abide by the DSM-5 rules for differential diagnosis (1). Our experts also made four proposals for future research on the subject: (i) the ICD-11 construct of ODD with emotion dysregulation should be reviewed in connection with DMDD (99, 100); (ii) childhood trauma, attachment difficulties, and parents with mental illness, including borderline personality disorder and ADHD, are associated with DMDD and their role should be explored (55, 101); (iii) complex post-traumatic stress disorder and DMDD, as well as the transition of DMDD with borderline personality disorder, should be explored (102); and (iv) the issue of the over-diagnosis of pre-pubertal bipolar disorder that led to the creation of the DMDD construct should also be reviewed in future (8, 98).
In addition, some participants had hoped that DMDD comorbidities, particularly ODD and IED, would be addressed more directly in this study. A few comments to this effect were collected in the last round. Some experts pointed out that the symptoms of these orders overlapped considerably. Other participants were critical of the fact that ODD was considered first and foremost a behavior disorder that did not sufficiently take account of mood symptoms or context. According to some participants, IED seemed extremely rare in the pediatric population. Finally, a few experts found that the differential diagnosis rules for DMDD were absurd and should be reviewed (e.g., cannot coexist with ODD, symptoms do not occur exclusively during an episode of major depressive disorder but DMDD can coexist with major depressive disorder). Future research and an APA DSM Task Force could certainly contribute to demystify these issues.
Conclusion
In sum, the participants in our study seemed to indicate that a multidisciplinary team and an integrative approach, including family-focused interventions, should be favored to treat youths with DMDD. As much as possible, families should be offered support and professionals should work in close collaboration with the schools in communities. In this study, various psychosocial proposals are retained. A modular approach, as proposed by Evans, could be an interesting way to tackle treatment (77). The research in the field of psychosocial treatments is generally encouraging (24). Nevertheless, future studies remain necessary in this area. Furthermore, medication is, at times, a necessary option, mostly when comorbidities such as ADHD occur. However, to this date, there has been insufficient research to allow clear recommendations for DMDD in this regard. Indeed, comorbidities can widely influence DMDD treatment plans (psychosocial and pharmacological). Overall, a comprehensive clinical assessment was endorsed as the cornerstone of the therapeutic approach for youths with DMDD. We hope that this study will aid the scientific community to (i) get a better understanding of youths with DMDD symptoms, (ii) provide relevant information to clinicians, and (iii) raise new research questions and projects.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Human Research Ethics Board of Université du Québec à Montréal, in Canada (Approval no. 4953). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual (s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
AB wrote the first draft of the manuscript as part of her thesis. RL reviewed all versions of the manuscript in preparation for the final draft of the article. AB and RL were the capacity of her thesis research supervisor, had full access to all the study data and ensured its integrity and the accuracy of data analysis. J-MG, J-JB, XB, and DC contributed to the interpretation of the results and to drafting the manuscript. All authors contributed to revising the manuscript and read and approved the submitted version.
Acknowledgments
The following psychiatrists and psychologists who participated in this study consented to be named in the acknowledgments: Mary A. Fristad, Gonca Ozyurt, Joel Stoddard, Pablo Vidal-Ribas, Evren Tufan, Bojan Mirkovic, Ankit Parmar, Tiago N. Munhoz, Gary Byrne, Johanne Renaud, Leslie A. Hulvershorn, Ines Mürner-Lavanchy, Hélène Lahaye, Melissa Mulraney, Rachel H.B. Mitchell, and Soumya Basu. We thank them dearly for their time and effort. The study would not have been possible without their contribution.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^For example, after sending a reminder about the possibility of participating in the first round, a potential participant wrote this: “I feel guilty every time I get your invitation and do not respond. It is not that I do not have time. It is that I’m not sure that I believe that DMDD is a real entity. We are struggling with how to deal with children who have problems with irritability and emotional outbursts. DMDD is neither a reliable diagnosis or an especially valid one. For that reason, I think it is premature to talk about diagnosing and treating it.”
References
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders DSM-5. 5th ed. Arlington: American Psychiatric Publishing (2013).
2. Althoff, RR, Crehan, ET, He, J-P, Burstein, M, Hudziak, JJ, and Merikangas, KR. Disruptive mood dysregulation disorder at ages 13–18: results from the National Comorbidity Survey—Adolescent Supplement. J Child Adolesc Psychopharmacol. (2016) 26:107–13. doi: 10.1089/cap.2015.0038
3. Copeland, WE, Angold, A, Costello, EJ, and Egger, H. Prevalence, comorbidity, and correlates of DSM-5 proposed disruptive mood dysregulation disorder. Am J Psychiatr. (2013) 170:173–9. doi: 10.1176/appi.ajp.2012.12010132
4. Dougherty, LR, Smith, VC, Bufferd, SJ, Carlson, GA, Stringaris, A, Leibenluft, E, et al. DSM-5 disruptive mood dysregulation disorder: correlates and predictors in young children. Psychol Med. (2014) 44:2339–50. doi: 10.1017/S0033291713003115
5. Geller, B, Sun, K, Zimerman, B, Luby, J, Frazier, J, and Williams, M. Complex and rapid-cycling in bipolar children and adolescents: a preliminary study. J Affect Disord. (1995) 34:259–68. doi: 10.1016/0165-0327(95)00023-G
6. Wozniak, J, Biederman, J, Kiely, K, Ablon, JS, Faraone, SV, Mundy, E, et al. Mania-like symptoms suggestive of childhood-onset bipolar disorder in clinically referred children. J Am Acad Child Adolesc Psychiatry. (1995) 34:867–76. doi: 10.1097/00004583-199507000-00010
7. Moreno, C, Laje, G, Blanco, C, Jiang, H, Schmidt, AB, and Olfson, M. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Arch Gen Psychiatry. (2007) 64:1032–9. doi: 10.1001/archpsyc.64.9.1032
8. Le, J, Feygin, Y, Creel, L, Lohr, WD, Jones, VF, Williams, PG, et al. Trends in diagnosis of bipolar and disruptive mood dysregulation disorders in children and youth. J Affect Disord. (2020) 264:242–8. doi: 10.1016/j.jad.2019.12.018
9. Parry, PI, Allison, S, and Bastiampillai, T. Reification of the paediatric bipolar hypothesis in the USA. Lancet Psychiatry. (2015) 2:14–6. doi: 10.1016/S2215-0366(14)00075-3
10. Hyman, SE. The diagnosis of mental disorders: the problem of reification. Annu Rev Clin Psychol. (2010) 6:155–79. doi: 10.1146/annurev.clinpsy.3.022806.091532
11. Leibenluft, E, Charney, DS, Towbin, KE, Bhangoo, RK, and Pine, DS. Defining clinical phenotypes of juvenile mania. Am J Psychiatr. (2003) 160:430–7. doi: 10.1176/appi.ajp.160.3.430
12. Leibenluft, E. Chronic irritability in children is not pediatric bipolar disorder: implications for treatment. Bipolar Disord. (2019) 22:195–6. doi: 10.1111/bdi.12881
13. Leibenluft, E. Severe mood dysregulation, irritability, and the diagnostic boundaries of bipolar disorder in youths. Am J Psychiatr. (2011) 168:129–42. doi: 10.1176/appi.ajp.2010.10050766
14. Masi, L, Guilé, J-M, and Mille, C. Dysrégulation émotionnelle et comportementale sévère chez l’enfant: évolution nosologique et affiliation aux pathologies de l’humeur. Neuropsychiatr Enfance Adolesc. (2014) 62:65–71. doi: 10.1016/j.neurenf.2014.01.013
15. Mikita, N, and Stringaris, A. Mood dysregulation. Eur Child Adolesc Psychiatry. (2013) 22:11–6. doi: 10.1007/s00787-012-0355-9
16. Regier, DA, Narrow, WE, Clarke, DE, Kraemer, HC, Kuramoto, SJ, Kuhl, EA, et al. DSM-5 field trials in the United States and Canada, part II: test-retest reliability of selected categorical diagnoses. Am J Psychiatr. (2013) 170:59–70. doi: 10.1176/appi.ajp.2012.12070999
17. Vidal-Ribas, P, Brotman, MA, Valdivieso, I, Leibenluft, E, and Stringaris, A. The status of irritability in psychiatry: a conceptual and quantitative review. J Am Acad Child Adolesc Psychiatry. (2016) 55:556–70. doi: 10.1016/j.jaac.2016.04.014
18. Malhi, GS, and Bell, E. Fake views: DMDD, indeed! Austral New Zealand Journal of Psychiatry. (2019) 53:706–10. doi: 10.1177/0004867419863162
19. World Health Organization. International classification of diseases for mortality and morbidity statistics (11th revision). (2020). Available: http://www.who.int/classifications/icd/en/ (Accessed February 2020).
20. Carlson, GA, Singh, MK, Amaya-Jackson, L, Benton, TD, Althoff, RR, Bellonci, C, et al. Narrative review: impairing emotional outbursts: what they are and what we should do about them. J Am Acad Child Adolesc Psychiatry. (2023) 62:135–50. doi: 10.1016/j.jaac.2022.03.014
21. Benarous, X, Iancu, C, Guilé, J-M, Consoli, A, and Cohen, D. Missing the forest for the trees? A high rate of motor and language impairments in disruptive mood dysregulation disorder in a chart review of inpatient adolescents. Eur Child Adolesc Psychiatry. (2021) 30:1579–90. doi: 10.1007/s00787-020-01636-y
22. Carlson, GA, Potegal, M, Margulies, D, Gutkovich, Z, and Basile, J. Rages—what are they and who has them? J Child Adolesc Psychopharmacol. (2009) 19:281–8. doi: 10.1089/cap.2008.0108
23. Rao, U. DSM-5: disruptive mood dysregulation disorder. Asian J Psychiatr. (2014) 11:119–23. doi: 10.1016/j.ajp.2014.03.002
24. Hendrickson, B, Girma, M, and Miller, L. Review of the clinical approach to the treatment of disruptive mood dysregulation disorder. Int Rev Psychiatry. (2019) 32:202–11. doi: 10.1080/09540261.2019.1688260
25. Jorm, AF. Using the Delphi expert consensus method in mental health research. Austral New Zealand J Psychiatry. (2015) 49:887–97. doi: 10.1177/0004867415600891
26. Dalkey, N, and Helmer, O. Delphi technique: characteristics and sequence model to the use of experts. Manag Sci. (1963) 9:458–67. doi: 10.1287/mnsc.9.3.458
28. Lynn, MR, Layman, EL, and Englebardt, SP. Nursing administration research priorities: a national Delphi study. JONA. (1998) 28:7–11. doi: 10.1097/00005110-199805000-00002
29. Avella, JR. Delphi panels: research design, procedures, advantages, and challenges. Int J Dr Stud. (2016) 11:305–21. doi: 10.28945/3561
30. Young, WH, and Hogben, D. An experimental study of the Delphi technique. Educ Res Perspect. (1978) 5:57–62.
31. Gibson, JM. Using the Delphi technique to identify the content and context of nurses' continuing professional development needs. J Clin Nurs. (1998) 7:451–9. doi: 10.1046/j.1365-2702.1998.00175.x
32. Procter, S, and Hunt, M. Using the Delphi survey technique to develop a professional definition of nursing for analysing nursing workload. J Adv Nurs. (1994) 19:1003–14. doi: 10.1111/j.1365-2648.1994.tb01180.x
33. Green, B, Jones, M, Hughes, D, and Williams, A. Applying the Delphi technique in a study of GPs’ information requirements. Health Soc Care Community. (1999) 7:198–205. doi: 10.1046/j.1365-2524.1999.00176.x
34. Beech, B. Studying the future: a Delphi survey of how multi-disciplinary clinical staff view the likely development of two community mental health centres over the course of the next two years. J Adv Nurs. (1997) 25:331–8. doi: 10.1046/j.1365-2648.1997.1997025331.x
35. Keeney, S, McKenna, H, and Hasson, F. The Delphi technique in nursing and health research. Chichester: John Wiley & Sons (2011).
36. Parenté, FJ, and Anderson-Parenté, JK. Delphi inquiry systems. In: Wright, G, and Ayton, P (Editords), Judgmental Forecasting. United Kingdom, Chichester: John Wiley (1987):129–56.
37. Cavalli-Sforza, V, and Ortolano, L. Delphi forecasts of land use: transportation interactions. J Transp Eng. (1984) 110:324–39. doi: 10.1061/(ASCE)0733-947X(1984)110:3(324)
38. Novakowski, N, and Wellar, B. Using the Delphi technique in normative planning research: methodological design considerations. Environ Plan A. (2008) 40:1485–500. doi: 10.1068/a39267
39. Hasson, F, Keeney, S, and McKenna, H. Research guidelines for the Delphi survey technique. J Adv Nurs. (2000) 32:1008–15. doi: 10.1046/j.1365-2648.2000.t01-1-01567.x
40. Sumsion, T. The Delphi technique: an adaptive research tool. Br J Occup Ther. (1998) 61:153–6. doi: 10.1177/030802269806100403
41. McKenna, H, Hasson, F, and Smith, M. A Delphi survey of midwives and midwifery students to identify non-midwifery duties. Midwifery. (2002) 18:314–22. doi: 10.1054/midw.2002.0327
42. Hill, KQ, and Fowles, J. The methodological worth of the Delphi forecasting technique. Technol Forecast Soc Chang. (1975) 7:179–92. doi: 10.1016/0040-1625(75)90057-8
43. Eckman, C. Development of an instrument to evaluate intercollegiate athletic coaches: a modified Delphi study [dissertation]. West Virginia University, Morgantown (1983).
44. Jacobs, JM. Essential assessment criteria for physical education teacher education programs: a Delphi study [dissertation]. West Virginia University, Morgantown (1996).
45. Powell, C. The Delphi technique: myths and realities. J Adv Nurs. (2003) 41:376–82. doi: 10.1046/j.1365-2648.2003.02537.x
46. Murry, JWJr, and Hammons, JO. Delphi: a versatile methodology for conducting qualitative research. Rev High Educ. (1995) 18:423–36. doi: 10.1353/rhe.1995.0008
47. Tremblay-Boudreault, V, and Dionne, C. L’approche Delphi: application dans la conception d’un outil clinique en réadaptation au travail en santé mentale. Méthodes qualitatives, quantitatives et mixtes. Montréal: Presses de l’Université du Québec (2020).
48. Steurer, J. The Delphi method: an efficient procedure to generate knowledge. Skelet Radiol. (2011) 40:959–61. doi: 10.1007/s00256-011-1145-z
50. Hsieh, H-F, and Shannon, SE. Three approaches to qualitative content analysis. Qual Health Res. (2005) 15:1277–88. doi: 10.1177/1049732305276687
51. Mayring, P. Qualitative content analysis: theoretical foundation, basic procedures and software solution. Austria: Klagenfurt Press. (2014).
52. Jones, J, and Hunter, D. Consensus methods for medical and health services research. BMJ. Br Med J. (1995) 311:376–80. doi: 10.1136/bmj.311.7001.376
53. Cole, ZD, Donohoe, HM, and Stellefson, ML. Internet-based Delphi research: case based discussion. Environ Manag. (2013) 51:511–23. doi: 10.1007/s00267-012-0005-5
54. Mürner-Lavanchy, I, Kaess, M, and Koenig, J. Diagnostic instruments for the assessment of disruptive mood dysregulation disorder: a systematic review of the literature. Eur Child Adolesc Psychiatry. (2023) 32:17–39. doi: 10.1007/s00787-021-01840-4
55. Benarous, X, Renaud, J, Breton, JJ, Cohen, D, Labelle, R, and Guilé, J-M. Are youths with disruptive mood dysregulation disorder different from youths with major depressive disorder or persistent depressive disorder? J Affect Disord. (2020) 265:207–15. doi: 10.1016/j.jad.2020.01.020
56. Stringaris, A, Goodman, R, Ferdinando, S, Razdan, V, Muhrer, E, Leibenluft, E, et al. The affective reactivity index: a concise irritability scale for clinical and research settings. J Child Psychol Psychiatry. (2012) 53:1109–17. doi: 10.1111/j.1469-7610.2012.02561.x
57. De Los, RA, Augenstein, TM, Wang, M, Thomas, SA, Drabick, DA, Burgers, DE, et al. The validity of the multi-informant approach to assessing child and adolescent mental health. Psychol Bull. (2015) 141:858–900. doi: 10.1037/a0038498
58. Dvir, Y, Ford, JD, Hill, M, and Frazier, JA. Childhood maltreatment, emotional dysregulation, and psychiatric comorbidities. Harv Rev Psychiatry. (2014) 22:149–61. doi: 10.1097/HRP.0000000000000014
59. Mikolajczak, M, and Desseilles, M. Traité de régulation des émotions. Bruxelles: De Boeck Supérieur (2012).
60. McLaughlin, KA, and Hatzenbuehler, ML. Mechanisms linking stressful life events and mental health problems in a prospective, community-based sample of adolescents. J Adolesc Health. (2009) 44:153–60. doi: 10.1016/j.jadohealth.2008.06.019
61. Gregory, AM, and Sadeh, A. Sleep, emotional and behavioral difficulties in children and adolescents. Sleep Med Rev. (2012) 16:129–36. doi: 10.1016/j.smrv.2011.03.007
62. Yew, S, and O'Kearney, R. Early language impairments and developmental pathways of emotional problems across childhood. Int J Lang Commun Disord. (2015) 50:358–73. doi: 10.1111/1460-6984.12142
63. Poznanski, EO, Cook, SC, and Carroll, BJ. A depression rating scale for children. Pediatrics. (1979) 64:442–50. doi: 10.1542/peds.64.4.442
65. Achenbach, TM, and Rescorla, LA. Manual for the ASEBA School-age Forms & Profiles. Burlington (US): University of Vermont (2001).
66. Boudjerida, A, Labelle, R, Bergeron, L, Berthiaume, C, Guilé, J-M, and Breton, J-J. Development and initial validation of the disruptive mood dysregulation disorder questionnaire among adolescents from clinic settings. Front Psychiatr. (2022) 13:7991. doi: 10.3389/fpsyt.2022.617991
67. Carlson, GA. Mania and ADHD: comorbidity or confusion. J Affect Disord. (1998) 51:177–87. doi: 10.1016/S0165-0327(98)00179-7
68. Galanter, CA, Hundt, SR, Goyal, P, Le, J, and Fisher, PW. Variability among research diagnostic interview instruments in the application of DSM-IV-TR criteria for pediatric bipolar disorder. J Am Acad Child Adolesc Psychiatry. (2012) 51:605–21. doi: 10.1016/j.jaac.2012.03.010
69. Parry, P. 'Paediatric bipolar Disorder': why did it occur, the iatrogenic consequences, and the implications for medical ethics and psychiatric nosology. Flinders University, Australia: College of Medicine and Public Health (2021).
70. Miller, L, Hlastala, SA, Mufson, L, Leibenluft, E, and Riddle, M. Interpersonal psychotherapy for adolescents with mood and behavior dysregulation: evidence-based case study. Evidence-Based Practice Child Adolescent Mental Health. (2016) 1:159–75. doi: 10.1080/23794925.2016.1247679
71. Miller, L, Hlastala, SA, Mufson, L, Leibenluft, E, Yenokyan, G, and Riddle, M. Interpersonal psychotherapy for mood and behavior dysregulation: pilot randomized trial. Depress Anxiety. (2018) 35:574–82. doi: 10.1002/da.22761
72. Perepletchikova, F, Nathanson, D, Axelrod, SR, Merrill, C, Walker, A, Grossman, M, et al. Randomized clinical trial of dialectical behavior therapy for preadolescent children with disruptive mood dysregulation disorder: feasibility and outcomes. J Am Acad Child Adolesc Psychiatry. (2017) 56:832–40. doi: 10.1016/j.jaac.2017.07.789
73. Kircanski, K, Clayton, ME, Leibenluft, E, and Brotman, MA. Psychosocial treatment of irritability in youth. Current Treatment Options in Psychiatry. (2018) 5:129–40. doi: 10.1007/s40501-018-0141-5
74. Waxmonsky, JG, Waschbusch, DA, Belin, P, Li, T, Babocsai, L, Humphery, H, et al. A randomized clinical trial of an integrative group therapy for children with severe mood dysregulation. J Am Acad Child Adolesc Psychiatry. (2016) 55:196–207. doi: 10.1016/j.jaac.2015.12.011
75. Dixit, A, Mahour, P, and Agarwal, V. Cognitive Behavioural therapy for disruptive mood dysregulation disorder. Indian Journal of Mental Health. (2020) 7:158. doi: 10.30877/IJMH.7.2.2020.158-162
76. Byrne, G, and Connon, G. The use of standard parenting management training in addressing disruptive mood dysregulation disorder: a pilot study. J Contemp Psychother. (2021) 51:259–63. doi: 10.1007/s10879-021-09489-5
77. Evans, SC, Wei, MA, Harmon, SL, and Weisz, JR. Modular psychotherapy outcomes for youth with different latent profiles of irritability and emotion dysregulation. Front Psych. (2021) 12:618455. doi: 10.3389/fpsyt.2021.618455
78. Valot, L, and Lalau, J-D. L’alliance thérapeutique. Médecine des Maladies Métaboliques. (2020) 14:761–7. doi: 10.1016/j.mmm.2020.09.005
79. Vera, L. Les thérapies comportementales et cognitives chez l’enfant et l’adolescent: modèles théoriques. Paris: Elsevier Masson (2014).
80. Waxmonsky, J, Pelham, WE, Gnagy, E, Cummings, MR, O’Connor, B, Majumdar, A, et al. The efficacy and tolerability of methylphenidate and behavior modification in children with attention-deficit/hyperactivity disorder and severe mood dysregulation. J Child Adolesc Psychopharmacol. (2008) 18:573–88. doi: 10.1089/cap.2008.065
81. Winters, DE, Fukui, S, Leibenluft, E, and Hulvershorn, LA. Improvements in irritability with open-label methylphenidate treatment in youth with comorbid attention deficit/hyperactivity disorder and disruptive mood dysregulation disorder. J Child Adolesc Psychopharmacol. (2018) 28:298–305. doi: 10.1089/cap.2017.0124
82. Baweja, R, Belin, PJ, Humphrey, HH, Babocsai, L, Pariseau, ME, Waschbusch, DA, et al. The effectiveness and tolerability of central nervous system stimulants in school-age children with attention-deficit/hyperactivity disorder and disruptive mood dysregulation disorder across home and school. J Child Adolesc Psychopharmacol. (2016) 26:154–63. doi: 10.1089/cap.2015.0053
83. de la Cruz, LF, Simonoff, E, McGough, JJ, Halperin, JM, Arnold, LE, and Stringaris, A. Treatment of children with attention-deficit/hyperactivity disorder (ADHD) and irritability: results from the multimodal treatment study of children with ADHD (MTA). J Am Acad Child Adolesc Psychiatry. (2015) 54:62–70.e3. doi: 10.1016/j.jaac.2014.10.006
84. Blader, JC, Pliszka, SR, Jensen, PS, Schooler, NR, and Kafantaris, V. Stimulant-responsive and stimulant-refractory aggressive behavior among children with ADHD. Pediatrics. (2010) 126:e796–806. doi: 10.1542/peds.2010-0086
85. Krieger, FV, Pheula, GF, Coelho, R, Zeni, T, Tramontina, S, Zeni, CP, et al. An open-label trial of risperidone in children and adolescents with severe mood dysregulation. J Child Adolesc Psychopharmacol. (2011) 21:237–43. doi: 10.1089/cap.2010.0123
86. Pan, P-Y, Fu, A-T, and Yeh, C-B. Aripiprazole/methylphenidate combination in children and adolescents with disruptive mood dysregulation disorder and attention-deficit/hyperactivity disorder: an open-label study. J Child Adolesc Psychopharmacol. (2018) 28:682–9. doi: 10.1089/cap.2018.0068
87. Dickstein, DP, Towbin, KE, Van Der Veen, JW, Rich, BA, Brotman, MA, Knopf, L, et al. Randomized double-blind placebo-controlled trial of lithium in youths with severe mood dysregulation. J Child Adolesc Psychopharmacol. (2009) 19:61–73. doi: 10.1089/cap.2008.044
88. Towbin, K, Vidal-Ribas, P, Brotman, MA, Pickles, A, Miller, KV, Kaiser, A, et al. A double-blind randomized placebo-controlled trial of citalopram adjunctive to stimulant medication in youth with chronic severe irritability. J Am Acad Child Adolesc Psychiatry. (2020) 59:350–61. doi: 10.1016/j.jaac.2019.05.015
89. Benarous, X, Ferrafiat, V, Zammit, J, Consoli, A, Gérardin, P, Guilé, J-M, et al. Effective use of atomoxetine to treat six inpatient youths with disruptive mood dysregulation disorder without attention deficit disorder. CNS Spectr. (2020) 25:455–7. doi: 10.1017/S1092852919001020
90. Dusetzina, SB, Weinberger, M, Gaynes, BN, Farley, JF, Sleath, B, and Hansen, RA. Prevalence of bipolar disorder diagnoses and psychotropic drug therapy among privately insured children and adolescents. Pharmacotherapy. (2012) 32:1085–94. doi: 10.1002/phar.1148
91. Delbello, MP, Schwiers, ML, Rosenberg, HL, and Strakowski, SM. A double-blind, randomized, placebo-controlled study of quetiapine as adjunctive treatment for adolescent mania. J Am Acad Child Adolesc Psychiatry. (2002) 41:1216–23. doi: 10.1097/00004583-200210000-00011
92. Findling, RL, McNamara, NK, Gracious, BL, Youngstrom, EA, Stansbrey, RJ, Reed, MD, et al. Combination lithium and divalproex sodium in pediatric bipolarity. J Am Acad Child Adolesc Psychiatry. (2003) 42:895–901. doi: 10.1097/01.CHI.0000046893.27264.53
93. Marchand, WR, Wirth, L, and Simon, C. Quetiapine adjunctive and monotherapy for pediatric bipolar disorder: a retrospective chart review. J Child Adoles Psychopharmacol. (2004) 14:405–11. doi: 10.1089/cap.2004.14.405
94. Wagner, KD, Weller, EB, Carlson, GA, Sachs, G, Biederman, J, Frazier, JA, et al. An open-label trial of divalproex in children and adolescents with bipolar disorder. J Am Acad Child Adolesc Psychiatry. (2002) 41:1224–30. doi: 10.1097/00004583-200210000-00012
95. Hetrick, SE, McKenzie, JE, Bailey, AP, Sharma, V, Moller, CI, Badcock, PB, et al. New generation antidepressants for depression in children and adolescents: a network meta-analysis. Cochrane Database Syst Rev. (2021) 2021:CD013674. doi: 10.1002/14651858.CD013674.pub2
96. Ray, WA, Stein, CM, Murray, KT, Fuchs, DC, Patrick, SW, Daugherty, J, et al. Association of antipsychotic treatment with risk of unexpected death among children and youths. JAMA Psychiatry. (2019) 76:162–71. doi: 10.1001/jamapsychiatry.2018.3421
97. Libowitz, MR, and Nurmi, EL. The burden of antipsychotic-induced weight gain and metabolic syndrome in children. Front Psych. (2021) 12:623681. doi: 10.3389/fpsyt.2021.623681
98. Findling, RL, Zhou, X, George, P, and Chappell, PB. Diagnostic trends and prescription patterns in disruptive mood dysregulation disorder and bipolar disorder. J Am Acad Child Adolesc Psychiatry. (2022) 61:434–45. doi: 10.1016/j.jaac.2021.05.016
99. Runions, K, Stewart, R, Moore, J, Martinez Ladino, Y, Rao, P, and Zepf, F. Disruptive mood dysregulation disorder in ICD-11: a new disorder or ODD with a specifier for chronic irritability? Eur Child Adolesc Psychiatry. (2016) 25:331–2. doi: 10.1007/s00787-015-0789-y
100. Evans, SC, Burke, JD, Roberts, MC, Fite, PJ, Lochman, JE, Francisco, R, et al. Irritability in child and adolescent psychopathology: an integrative review for ICD-11. Clin Psychol Rev. (2017) 53:29–45. doi: 10.1016/j.cpr.2017.01.004
101. Uran, P, and Kılıç, BG. Family functioning, comorbidities, and behavioral profiles of children with ADHD and disruptive mood dysregulation disorder. J Atten Disord. (2020) 24:1285–94. doi: 10.1177/1087054715588949
Keywords: disruptive mood dysregulation disorder, Delphi study, experts consensus, mental health, quality of care
Citation: Boudjerida A, Guilé J-M, Breton J-J, Benarous X, Cohen D and Labelle R (2024) A Delphi consensus among experts on assessment and treatment of disruptive mood dysregulation disorder. Front. Psychiatry. 14:1166228. doi: 10.3389/fpsyt.2023.1166228
Edited by:
Glen Spielmans, Metropolitan State University, United StatesReviewed by:
Bertrand Olliac, University of Limoges, FrancePeter Parry, The University of Queensland, Australia
Copyright © 2024 Boudjerida, Guilé, Breton, Benarous, Cohen and Labelle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Réal Labelle, bGFiZWxsZS5yZWFsQHVxYW0uY2E=