
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 17 April 2023
Sec. Mood Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1151397
 Ulises Ríos1,2,3*
Ulises Ríos1,2,3* Javier Morán2,3,4Jimena Hermosilla1,5René González6Paulina Muñoz7
Javier Morán2,3,4Jimena Hermosilla1,5René González6Paulina Muñoz7 Marcelo Arancibia2,8
Marcelo Arancibia2,8 Luisa Herrera9
Luisa Herrera9 Juan Pablo Jiménez3,10
Juan Pablo Jiménez3,10 Pablo R. Moya6,11
Pablo R. Moya6,11Background: Most studies on cognitive impairment in bipolar disorder have neglected the role of early stress, despite the high frequency of childhood maltreatment in this clinical group. The aim of this study was to establish a connection between a history of emotional, physical, and sexual abuse in childhood and social cognition (SC) in patients with bipolar disorder type I (BD-I) in euthymia, and to test a possible moderating effect of the single nucleotide polymorphism rs53576 in the oxytocin receptor gene (OXTR).
Methods: One hundred and one participants were included in this study. History of child abuse was evaluated using the Childhood Trauma Questionnaire-Short Form. Cognitive functioning was appraised using The Awareness of Social Inference Test (social cognition). The interaction effect between the independent variables OXTR rs53576 (AA/AG and GG) and the absence or presence of any one type of child maltreatment or a combination of types was analyzed using a generalized linear model regression.
Results: BD-I patients who had been victims of physical and emotional abuse in childhood and were carriers of the GG genotype at OXTR rs53576 displayed greater SC alterations, specifically in emotion recognition.
Discussion: This gene–environment interaction finding suggests a differential susceptibility model of a genetic variants that can be plausibly associated with SC functioning and might help to identify at-risk clinical subgroups within a diagnostic category. Future research aimed at testing the interlevel impact of early stress constitutes an ethical-clinical duty given the high rates of childhood maltreatment reported in BD-I patients.
Bipolar disorder (BD) has been linked to social cognition (SC) impairment, even during periods of euthymia (1, 2). Important heterogeneity exists, however, with measurable SC deficits being present in about one third of BD patients (3). Although most studies indicate that SC impairments do not predict functional outcomes beyond neurocognitive deficits in people with BD (4), there is also evidence suggesting that impairments in specific SC domains could be associated with psychosocial functioning in at least a subgroup of patients (5). Despite the vast literature on cognition impairments in BD, few authors have analyzed the impact of early stress (6). The lack of attention on this aspect may be relevant, given the importance of early stress on later neural development and cognitive functioning (7) as well as the substantial data demonstrating the high frequency of child abuse in BD patients (8, 9).
The few studies that have taken into account a history of childhood maltreatment in BD patients have reported significant differences in both SC and neurocognitive tests (10, 11). Greater cognitive deficits in BD patients with a history of childhood trauma may have a plausible biological basis (12).
The oxytocin system regulates several processes involved in SC functioning (13), both in the cognitive route of SC—i.e., theory of mind (14) and emotion recognition (15, 16)- and in the affective route of SC—i.e., empathy (17). Some of these studies have examined genetic variations of the single nucleotide polymorphism rs53576 (G/A), located in the third intron of the oxytocin receptor gene (OXTR), which has been linked to social behavioral phenotypes in humans (18).
There is a lack of work evaluating the hypothesis relating oxytocin to mood disorders in BD (19). Increased serum oxytocin levels in BD patients have been found in both symptomatic periods and euthymia (20). Given high phenotypic variability in BD, others have measured intermediate functioning dimensions, such as SC (21).
OXTR variants have been associated with outcomes at various levels, including schizophrenia (22), suicidal behavior (23) and depressive symptomatology (24). Meyer-Lindenberg et al. (25) evaluated associations of OXTR variants with intermediate phenotypes as a strategy to identify groups of patients with a common neurobiological substrate to target with more specific interventions. Studies that have taken this approach have reported an association between OXTR variants and SC functioning (26, 27).
Studies focused on intermediate phenotypes may be strengthened by designs that analyze gene–environment interactions. Most studies on OXTR variants have shown that the G allele of rs53576 is associated with protective social traits, such as prosocial behavior (28) and greater empathic ability (17). However, authors who have evaluated its interaction with a background of early trauma have reported a pattern of greater vulnerability for this allelic variant. Studies on the interaction between OXTR, history of child abuse and emotional regulation in adult life have shown that carriers of the rs53576 GG genotype display less emotional regulation if they had been victims of early trauma (29, 30). This pattern of differential vulnerability of the OXTR rs53576 G allele has also been observed in functional imaging studies, which report strong gray matter reduction in the bilateral ventral striatum, along with increased amygdala responsiveness to emotional facial expressions (31). Malhi et al. (32) found that AA homozygotes OXTR rs53576 carriers exposed to emotional trauma exhibited smaller left hippocampal volumes. Ebbert et al. (33) support the notion of being A carrier as a vulnerability factor. They reported, in a large cross-sectional study (n = 614), that the effect of emotional child abuse on family relationships during the adulthood was moderated by OXTR rs53576, observing that carriers of A allele had less supportive family relationships. However, not all studies support the relationship between child abuse, OXTR rs53576 and depressive symptoms (34). Nevertheless, the available evidence on BD patients is extremely scarce.
Gene–environment interaction studies in patients with BD generally focus on neurocognitive measures and have involved other gene variants, such as BDNF val66met (35, 36). To the best of our knowledge, this is the first study to test a OXTR-SC gene–environment interaction in patients with BD. Considering the possible differential effects on brain development linked to subtypes of child abuse (37) and the evidence that certain subtypes of child abuse result in SC alterations (11, 38), we evaluated the association between a history of childhood abuse and SC functioning in patients with BD type I (BD-I) in euthymia, and the potential moderating effect of OXTR rs53576. We hypothesize that carriers of the G allelic variant will display a differential sensitivity pattern dependent on the subtype of child abuse.
One hundred and one euthymic BD outpatients were recruited from the Mood Disorders Unit of Hospital Psiquiátrico del Salvador (Valparaíso, Chile) and the Outpatient Psychiatry Unit of Hospital Dr. Gustavo Fricke (Viña del Mar, Chile). Inclusion criteria were as follows: (a) BD-I DSM-IV-TR diagnosis, (b) age 18–65 years, (c) fulfilling euthymia criteria for at least 3 months, defined as a score of ≤6 on the Young Mania Rating Scale (YMRS) (39) and of ≤8 on the Hamilton Depression Rating Scale (HDRS) (40) and (d) the capacity to provide written informed consent. We excluded patients who were active drug users and who had received electroconvulsive therapy over the previous 3 months.
The subjects’ history of child abuse was evaluated using the Spanish language version of the Childhood Trauma Questionnaire-Short Form (CTQ-SF) (41, 42). Briefly, this self-report instrument comprises 28 items that refer to five subtypes of child abuse: sexual abuse (SA), emotional abuse (EA), physical abuse (PA), physical neglect, and emotional neglect. For ethical-clinical reasons, the self-report instrument was completed by each patient in a clinical setting, confidentially and in the presence of their treating physician. We only considered the abuse scales, as recommended by Aas et al. (36).
Cognitive functioning was evaluated with social and non-social cognition tests. For the former dimension, we used the Spanish language version of The Awareness of Social Inference Test (TASIT) (43), specifically the emotion evaluation task. This test evaluates the ability to recognize emotions by showing 20 micro-videos in which actors simulate situations that represent the basic emotions of fear, disgust, surprise, sadness, and anger. Neurocognitive aspects were evaluated with the Addenbrooke’s Cognitive Examination-Revised (ACE-R), Chilean version (44).
This study was approved by the research ethics committee of the Valparaíso-San Antonio Health Service, Chile. All patients were informed about the study and gave their signed consent.
After the interview, blood samples (6 ml) were taken from the patients and placed in EDTA-coated tubes. The DNA extraction was performed using the NucleoSpin Blood kit (Macherey-Nagel, Germany) following manufacturer’s protocol. The allelic OXTR rs53576 variants were genotyped using a TaqMan® probe (SNP ID C___3290335_20, Applied Biosystems, USA) in a AriaMX thermocycler (Agilent, USA) following the manufacturer’s protocol. Hardy–Weinberg equilibrium was tested by comparing the observed and expected genotypes using χ2.
Using generalized linear model regression, we evaluated the interaction effect between the independent variables OXTR rs53576, coded as AA/AG (0) and GG (1), and the absence (0) or presence (1) of any one type of child abuse or a combination of types. We used cut-off scores for “moderate” to “extreme” levels in the CTQ for SA (higher than 7 points), PA (higher than 9 points), and EA (higher than 12 points). The dependent variable was the total score on the TASIT.
First, we sought to identify if the presence of any subtype of abuse had an interaction effect with OXTR on SC. Second, to evaluate whether specific differences associated with each subtype of abuse, we repeated the analysis to evaluate the interaction between OXTR and the CTQ-SF subscales. In addition, as a way of assessing the presence of combinations of abuse subtypes, we generated three new variables: PA + SA; PA + EA; SA + EA. Lastly, we conducted a factorial ANOVA, for which we generated an ordinal variable based on abuse subtypes and combinations found to have interaction effects in the previous step.
Participants were 45.5 years old on average (13.9 SD); 65.7% of them were women. 64% of the patients reported being victims of at least one type of abuse as a child. The frequencies per subtype of abuse were 42% for SA, 30% for PA and 23% for EA (Table 1). Regarding abuse combinations, 10% of the patients were victims of three subtypes of abuse and 17% of at least two subtypes. Our analysis by sex showed that 71% of the women and 51% of the men had suffered at least one type of abuse as children (p < 0.02).
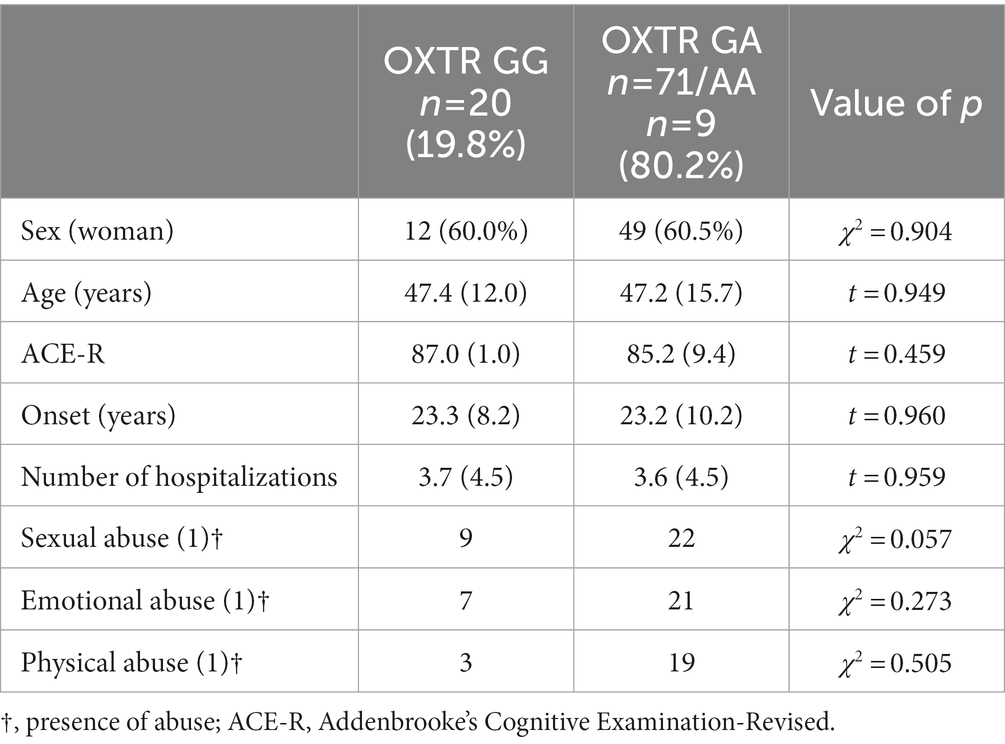
Table 1. Demographic and clinical characteristics of study sample.
We genotyped the rs53576 single nucleotide polymorphism located in OXTR. This variant was not in Hardy–Weinberg equilibrium (χ2 = 19.8, value of p = 0.000009), which might be explained by sample selection: patients with BD-I and not the general population. This is plausible as rs53576 has been linked to several behavioral traits and may contribute to the phenotype under study. The genotype frequencies of OXTR rs53576 were 20% GG and 80% GA + AA; we did not find differences by sex or age. There were no differences in the age of BD onset or number of hospitalizations.
Presence of abuse, determined by subscales of the CTQ-SF that surpass the score for moderate abuse, was not associated either as a simple effect (β = −0.565; p = 0.465) and did not show interaction with OXTR allelic variants (β = 1.802; p = 2.45; Table 2).
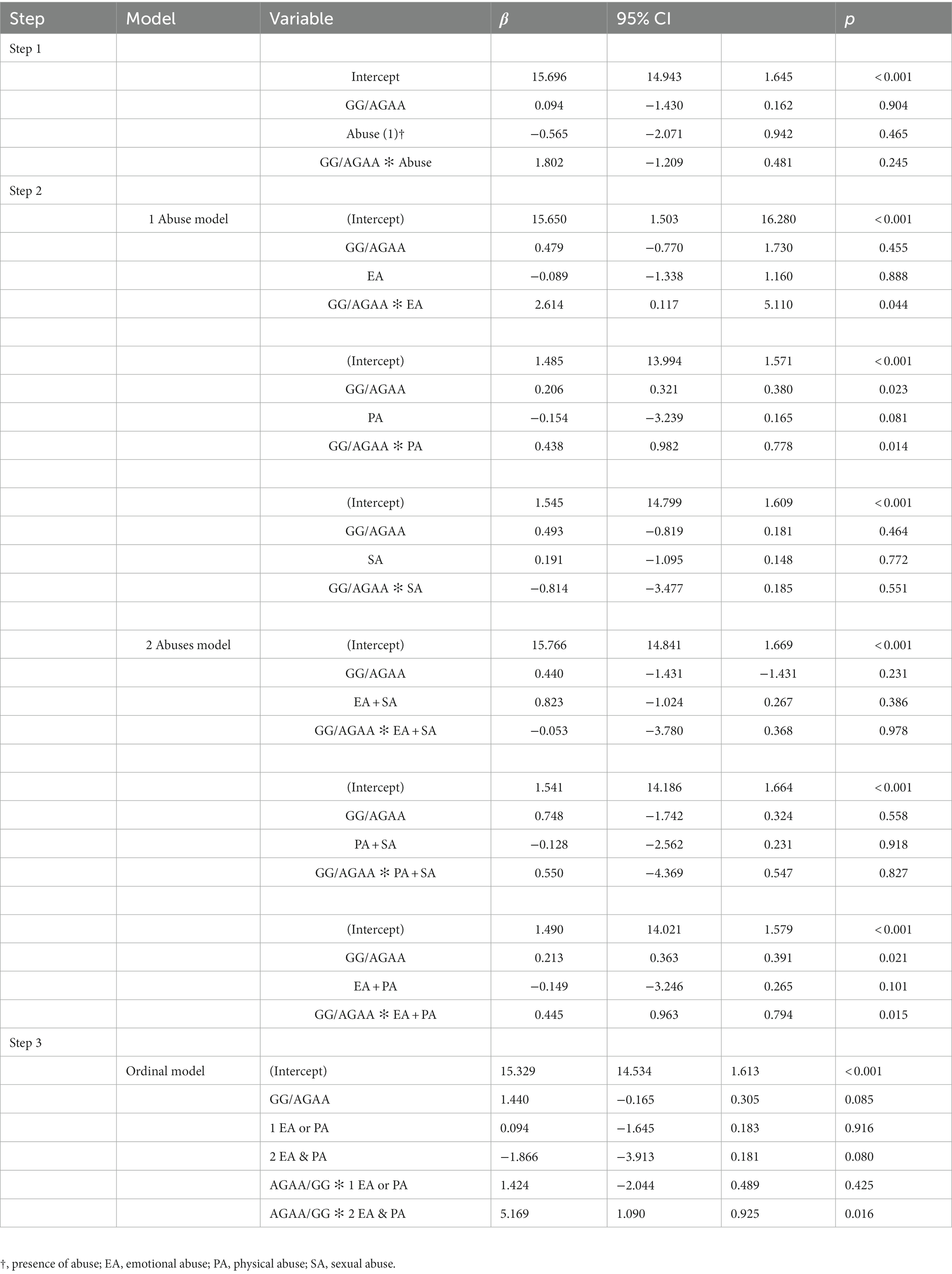
Table 2. Gene–environment interaction and SC functioning by presence of abuse.
The lacck of a simple interaction effect between the variables under study prompted the evaluation of the type of child abuse and its interaction with rs53576 genotypes. None of the subtypes of abuse displayed a simple association effect with SC. EA (β = 2.614; p = 0.044) and PA (β = 0.438; p = 0.014) displayed an interaction effect with the genetic variable. When evaluating whether the sum of two types of abuse interacted with OXTR, only PA + EA displayed an association with SC (β = 0.445; p = 0.015).
An ordinal variable was generated: we coded EA and PA as “1 abuse type” and EA + PA as “2 abuse types.” Although the presence of 1 abuse type is not associated with differences between the different rs53576 genotypes (β = 1.424; p = 4.25), the presence of 2 abuse types demonstrated altered emotion recognition scores in BD-I patients who carry the GG genotype (β = 5.169; p = 0.016; Figure 1).
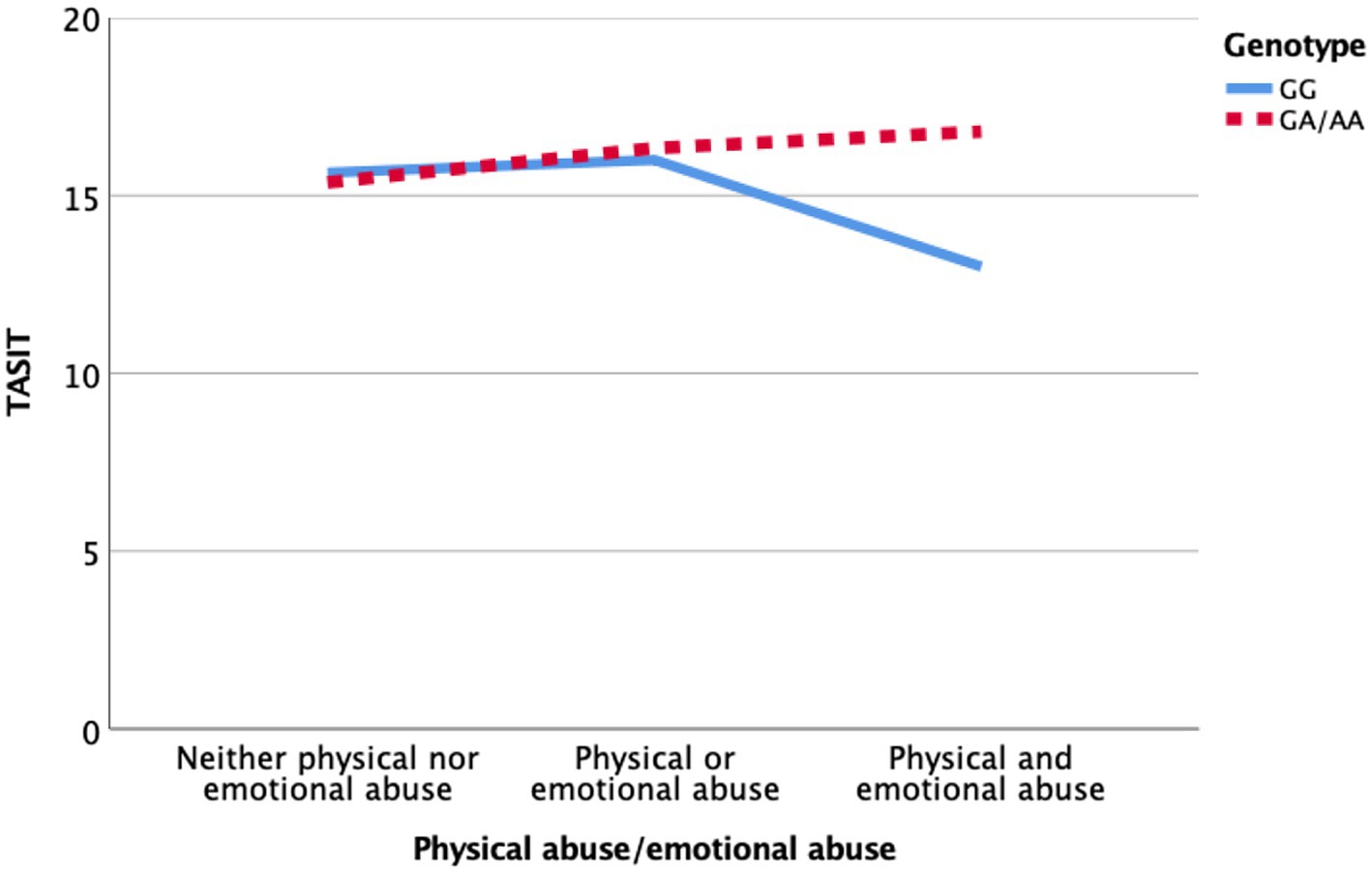
Figure 1. Impact of the interaction between OXTR rs53576 (GG vs. GA/AA), physical abuse, and emotional abuse on performance on an emotion recognition test (TASIT).
Our study revealed that euthymic patients with BD-I that were victims of both PA and EA as children and that were carriers of the OXTR rs53576 GG genotype displayed greater SC alterations, especially in an emotion recognition test.
In our sample, the frequencies of different types of abuse were remarkably high: 42% for SA, 30% for PA and 23% for EA. These frequencies are similar to those found by Vitriol et al. (45) in a prevalence study with a Chilean sample of patients with depressive disorder (n = 440). They found that 82% had experienced at least one traumatic childhood event, i.e., 49% domestic violence and 40% sexual abuse. In a systematic review by Maniglio et al. (46) including 3,407 BD patients (from 20 studies), a prevalence of 24% was found for SA. The authors state that this rate might be underestimated, since many studies restricted their definitions to the most severe forms of SA. In addition, the findings suggest that BD patients exhibited higher rates of SA in comparison to healthy individuals. Post et al. (47) showed an incidence of 50% of child abuse in BD patients (22% of SA in the entire sample; up to 36% in the US).
Our findings support the hypotheses of previous studies (29, 30) suggesting that the OXTR rs53576 GG genotype constitutes a differential susceptibility genotype (48) when dealing with early stress conditions. The gene–environment interaction model has been confirmed in studies focused on outcomes belonging to various levels including increased depressive symptomatology (49), alterations in emotional regulation tests (29, 30), and morpho-functional modifications in the limbic system (31).
The present study adds evidence for gene–environment interaction, focusing on an intermediate phenotype such as SC functioning, and thus providing data that may improve our comprehension of previous hypotheses centered on more complex variables. In other words, alterations in emotional recognition tasks may well be related to greater demands on emotional regulation processes and their morpho-functional correlates in the limbic system. Such a clinical context may also shed light on why depressive symptomatology indexes are greater in carriers of the OXTR rs53576 GG genotype who have been affected by child abuse.
Our findings also highlight differences on the role of the child abuse subtypes. Most studies have employed general measures of child abuse, neglecting the more specific characteristics of the traumatic experience and its possible differential effects on the brain (37). Our results revealed an interaction only in the presence of PA and EA, with no interaction with SA, despite the evidence indicating its undeniable impact on the life cycle of BD patients (46). These results are consistent with previous studies that have reported an association between the PA and EA subtypes and SC performance, specifically in emotional recognition tests (11, 38). In light of these results, the hypothesis that SA experiences have a course in a person’s development that differs from that of other types of abuse (50) should be taken into account in future research. Nevertheless, due to limitations such as our relatively small sample size and methodological aspects of the genotype grouping (GG vs. GA + AA), these hypotheses should be weighed with caution. Similarly, interpretation of the results should be cautious given the limited information on the more specific characteristics of each person’s traumatic experience during childhood. As suggested in studies on the effect of early interventions (51), this variable may attenuate or revert the long-term impact on brain function. Similarly, future research should consider the age at which the abuse occurred, as there is evidence of differential vulnerability in specific brain regions depending on the period of neural development period in which the stressor occurs (52).
The relevance of generating evidence, specifically in relation to BD, lies in the fact that cognitive alterations in this group have led to the design of therapeutic interventions and preventive strategies (53) that have overlooked the role of early stress. Most recommended therapeutic interventions are based on the assumption that this diagnostic category carries an inherent cognitive deficit, presuming that neuroprogression occurs as a consequence of the allostatic load of the disease (54). This perspective might reflect a possible biomedical bias, which has omitted the analysis of early psychosocial variables in studies of cognitive dysfunction in BD.
Among the limitations of our study, the assessment of traumatic episodes such as child abuse could be limited by characteristics of the instrument used that do not allow a sufficiently precise and deep characterization among the subtypes of maltreatment. In addition, TASIT was the only measure of SC and ACE-R might be a limited test when examining neurocognitive functioning in BD patients. On the other hand, a larger sample size might have allowed a more adequate analysis of the association between other dimensions of SC and OXTR variants.
Our findings highlight the need to rethink the design of new therapeutic approaches from a preventive perspective, with strategies aimed at reducing the incidence of child abuse in populations known to be at higher risk (8, 9) as well as through interventions aimed at fostering specific emotional regulation and mentalization skills (55) from a relational perspective. Conducting research aimed at testing interventions that reduce the inter-level impact of early stress (56) represents an ethical-clinical imperative in light of the high rates of child abuse in patients with BD.
This study has pioneered the exploration of SC in patients with BD-I using a gene–environment interaction model. Our aim was to provide data about SC deficits employing a hypothesis that presumes that adverse relational events in early life have an impact and interact with genetic variants of a plausibly related polymorphism such as OXTR rs53576. The description of a differential susceptibility genotype associated with the functioning of intermediate phenotypes may contribute to the identification of at-risk clinical subgroups within a diagnostic category with well-established intra-group heterogeneity such as BD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comite etico cientifico del Servicio de Salud Valparaiso San Antonio Chile. The patients/participants provided their written informed consent to participate in this study.
UR designed the study and managed the literature searches. JH and PM were in charge of administering the questionnaires. PRM and RG were in charge of genetics analysis. JM was in charge of the statistical analysis. All authors contributed to the article and approved the submitted version.
The study receive funding from ANID - Millennium Science Initiative Program/Millennium Institute for Research on Depression and Personality-MIDAP ICS13_005.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Samamé, C. Social cognition throughout the three phases of bipolar disorder: a state-of-the-art overview. Psychiatry Res. (2013) 210:1275–86. doi: 10.1016/j.psychres.2013.08.012
2. Ríos, U, Arancibia, M, Jiménez, JP, and Bermpohl, F. The forgotten affective route of social cognition in patients with bipolar disorders. J Exp Psychopathol. (2022) 13:204380872211354. doi: 10.1177/20438087221135422
3. Varo, C, Solé, B, Jiménez, E, Bonnín, CM, Torrent, C, Valls, E, et al. Identifying social cognition subgroups in euthymic patients with bipolar disorder: a cluster analytical approach. Psychol Med. (2022) 52:159–68. doi: 10.1017/S0033291720001865
4. Martino, D, Samamé, C, and Strejilevich, SA. Social cognition in schizophrenia and bipolar disorder: just quantitative differences? Schizophr Res. (2017) 183:164–5. doi: 10.1016/j.schres.2016.11.023
5. van Rheenen, T, and Rossell, SL. Phenomenological predictors of psychosocial function in bipolar disorder: is there evidence that social cognitive and emotion regulation abnormalities contribute? Aust N Z J Psychiatry. (2014) 48:26–35. doi: 10.1177/0004867413508452
6. Aas, M, Henry, C, Andreassen, O, Bellivier, F, Melle, I, and Etain, B. The role of childhood trauma in bipolar disorders. Int J Bipolar Disord. (2016) 4:1–10. doi: 10.1186/s40345-015-0042-0
7. Pechtel, P, and Pizzagalli, D. Effects of early life stress on cognitive and affective function: an integrated review of human literature. Psychopharmacologia (Berlin). (2011) 214:55–70. doi: 10.1007/s00213-010-2009-2
8. Agnew-Blais, J, and Danese, A. Childhood maltreatment and unfavourable clinical outcomes in bipolar disorder: a systematic review and meta-analysis. Lancet Psychiatry. (2016) 3:342–9. doi: 10.1016/S2215-0366(15)00544-1
9. Ríos, U, Moya, PR, Urrejola, Ó, Hermosilla, J, Gonzalez, R, Munõz, P, et al. History of child abuse among patients with bipolar disorders. Rev Med Chil. (2020) 148:204–10. doi: 10.4067/s0034-98872020000200204
10. Jiménez, E, Solé, B, Arias, B, Mitjans, M, Varo, C, Reinares, M, et al. Impact of childhood trauma on cognitive profile in bipolar disorder. Bipolar Disord. (2017) 19:363–74. doi: 10.1111/bdi.12514
11. Russo, M, Mahon, K, Shanahan, M, Solon, C, Ramjas, E, Turpin, J, et al. The association between childhood trauma and facial emotion recognition in adults with bipolar disorder. Psychiatry Res. (2015) 229:771–6. doi: 10.1016/j.psychres.2015.08.004
12. Danese, A, and Baldwin, JR. Hidden wounds? Inflammatory links between childhood trauma and psychopathology. Annu Rev Psychol. (2017) 68:517–44. doi: 10.1146/annurev-psych-010416-044208
13. Meyer-Lindenberg, A, Domes, G, Kirsch, P, and Heinrichs, M. Oxytocin and vasopressin in the human brain: social neuropeptides for translational medicine. Nat Rev Neurosci. (2011) 12:524–38. doi: 10.1038/nrn3044
14. Schneider-Hassloff, H, Straube, B, Jansen, A, Nuscheler, B, Wemken, G, Witt, S, et al. Oxytocin receptor polymorphism and childhood social experiences shape adult personality, brain structure and neural correlates of mentalizing. Neuroimage Rep. (2016) 134:671–84. doi: 10.1016/j.neuroimage.2016.04.009
15. Shahrestani, S, Kemp, A, and Guastella, A. The impact of a single administration of intranasal oxytocin on the recognition of basic emotions in humans: a meta-analysis. Neuropsychopharmacology. (2013) 38:1929–36. doi: 10.1038/npp.2013.86
16. Schulze, L, Lischke, A, Greif, J, Herpertz, S, Heinrichs, M, and Domes, G. Oxytocin increases recognition of masked emotional faces. Psychoneuroendocrinology. (2011) 36:1378–82. doi: 10.1016/j.psyneuen.2011.03.011
17. Gong, P, Fan, H, Liu, J, Yang, X, Zhang, K, and Zhou, X. Revisiting the impact of OXTR rs53576 on empathy: a population-based study and a meta-analysis. Psychoneuroendocrinology. (2017) 80:131–6. doi: 10.1016/j.psyneuen.2017.03.005
18. Ebstein, R, Knafo, A, Mankuta, D, Chew, S, and Lai, P. The contributions of oxytocin and vasopressin pathway genes to human behavior. Horm Behav. (2012) 61:359–79. doi: 10.1016/j.yhbeh.2011.12.014
19. Cochran, D, Fallon, D, Hill, M, and Frazier, J. The role of oxytocin in psychiatric disorders: a review of biological and therapeutic research findings. Harv Rev Psychiatry. (2013) 21:219–47. doi: 10.1097/HRP.0b013e3182a75b7d
20. Turan, T, Uysal, C, Asdemir, A, and Kılıç, E. May oxytocin be a trait marker for bipolar disorder? Psychoneuroendocrinology. (2013) 38:2890–6. doi: 10.1016/j.psyneuen.2013.07.017
21. Tas, C, Brown, E, Onur, E, Aydemir, O, and Brune, M. The associations between endogenous oxytocin levels and emotion recognition in bipolar disorder. Klin Psikofarmakol Bülteni. (2016) 25:19–26. doi: 10.5455/bcp.20140514043545
22. Montag, C, Brockmann, E, Bayerl, M, Rujescu, D, Müller, D, and Gallinat, J. Oxytocin and oxytocin receptor gene polymorphisms and risk for schizophrenia: a case-control study. World J Biol Psychiatry: Off J World Federation Soc Biol Psychiatry. (2013) 14:500–8. doi: 10.3109/15622975.2012.677547
23. Parris, M, Grunebaum, M, Galfalvy, H, Andronikashvili, A, Burke, A, Yin, H, et al. Attempted suicide and oxytocin-related gene polymorphisms. J Affect Disord. (2018) 238:62–8. doi: 10.1016/j.jad.2018.05.022
24. Thompson, S, Hammen, C, Starr, L, and Najman, J. Oxytocin receptor gene polymorphism (rs53576) moderates the intergenerational transmission of depression. Psychoneuroendocrinology. (2014) 43:11–9. doi: 10.1016/j.psyneuen.2014.01.012
25. Meyer-Lindenberg, A, and Weinberger, D. Intermediate phenotypes and genetic mechanisms of psychiatric disorders. Neuroscience. (2006) 7:818–27. doi: 10.1038/nrn1993
26. Uzefovsky, F, Shalev, I, Israel, S, Edelman, S, Raz, Y, Mankuta, D, et al. Oxytocin receptor and vasopressin receptor 1a genes are respectively associated with emotional and cognitive empathy. Horm Behav. (2015) 67:60–5. doi: 10.1016/j.yhbeh.2014.11.007
27. Davis, M, Horan, W, Nurmi, E, Rizzo, S, Li, W, Sugar, C, et al. Associations between oxytocin receptor genotypes and social cognitive performance in individuals with schizophrenia. Schizophr Res. (2014) 159:353–7. doi: 10.1016/j.schres.2014.09.006
28. Kogan, A, Saslow, L, Impett, E, Oveis, C, Keltner, D, and Rodrigues Saturn, S. Thin-slicing study of the oxytocin receptor (OXTR) gene and the evaluation and expression of the prosocial disposition. PNAS Nexus. (2011) 108:19189–92. doi: 10.1073/pnas.1112658108
29. Bradley, B, Westen, D, Mercer, K, Binder, E, Jovanovic, T, Crain, D, et al. Association between childhood maltreatment and adult emotional dysregulation in a low-income, urban, African American sample: moderation by oxytocin receptor gene. Dev Psychopathol. (2011) 23:439–52. doi: 10.1017/S0954579411000162
30. Hiraoka, D, and Nomura, M. Maternal childhood adversity, OXTR genotype and cognitive load impact on perceptual and behavioral responses to infant crying. Psychoneuroendocrinology. (2019) 104:195–202. doi: 10.1016/j.psyneuen.2019.03.005
31. Dannlowski, U, Kugel, H, Grotegerd, D, Redlich, R, Opel, N, Dohm, K, et al. Disadvantage of social sensitivity: interaction of oxytocin receptor genotype and child maltreatment on brain structure. Biol Psychiatry. (2016) 80:398–405. doi: 10.1016/j.biopsych.2015.12.010
32. Malhi, GS, Das, P, Outhred, T, Dobson-Stone, C, Bell, E, Gessler, D, et al. Interactions of OXTR rs53576 and emotional trauma on hippocampal volumes and perceived social support in adolescent girls. Psychoneuroendocrinology. (2020) 115:1–8. doi: 10.1016/j.psyneuen.2020.104635
33. Ebbert, AM, Infurna, FJ, Luthar, SS, Lemery-Chalfant, K, and Corbin, WR. Examining the link between emotional childhood abuse and social relationships in midlife: the moderating role of the oxytocin receptor gene. Child Abuse Negl. (2019) 98:1–12. doi: 10.1016/j.chiabu.2019.104151
34. Tollenaar, MS, Molendijk, ML, BWJH, P, Milaneschi, Y, and Antypa, N. The association of childhood maltreatment with depression and anxiety is not moderated by the oxytocin receptor gene. Eur Arch Psychiatry Neurol Sci. (2017) 267:517–26. doi: 10.1007/s00406-017-0784-z
35. Savitz, J, van der Merwe, L, Stein, D, Solms, M, and Ramesar, R. Genotype and childhood sexual trauma moderate neurocognitive performance: a possible role for brain-derived neurotrophic factor and apolipoprotein E variants. Biol Psychiatry. (2007) 62:391–9. doi: 10.1016/j.biopsych.2006.10.017
36. Aas, M, Haukvik, U, Djurovic, S, Bergmann, Ø, Athanasiu, L, Tesli, M, et al. BDNF val66met modulates the association between childhood trauma, cognitive and brain abnormalities in psychoses. Prog Neuro-Psychopharmacol Biol Psychiatry. (2013) 46:181–8. doi: 10.1016/j.pnpbp.2013.07.008
37. Teicher, M, Samson, JA, Anderson, CM, and Ohashi, K. The effects of childhood maltreatment on brain structure, function and connectivity. Neuroscience. (2016) 17:652–66. doi: 10.1038/nrn.2016.111
38. Nicol, K, Pope, M, and Hall, J. Facial emotion recognition in borderline personality: an association with childhood experience. Psychiatry Res. (2014) 218:256–8. doi: 10.1016/j.psychres.2014.04.017
39. Young, R, Biggs, J, Ziegler, V, and Meyer, D. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry Suppl. (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
40. Hamilton, R. A rating scale for depression. J Neurol Neurosurg Psychiatry. (1960) 23:56–62. doi: 10.1136/jnnp.23.1.56
41. Bernstein, D, Fink, L, Handelsman, L, Foote, J, Lovejoy, M, Wenzel, K, et al. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am J Psychiatry. (1994) 151:1132–6. doi: 10.1176/ajp.151.8.1132
42. Behn, A, Vöhringer, P, Martínez, P, Domínguez, A, González, A, Carrasco, M, et al. Validation of the childhood trauma questionnaire-short form in Chile. Rev Med Chil. (2020) 148:336–43. doi: 10.4067/S0034-98872020000300336
43. McDonald, S, Flanagan, S, Rollins, J, and Kinch, J. TASIT: a new clinical tool for assessing social perception after traumatic brain injury. J Head Trauma Rehabil. (2003) 18:219–38. doi: 10.1097/00001199-200305000-00001
44. Muñoz-Neira, C, Henríquez, F, Ihnen, J, Sánchez, M, Flores, P, and Slachevsky, A. Psychometric properties and diagnostic usefulness of the Addenbrooke’s cognitive examination-revised in a Chilean elderly sample. Rev Med Chil. (2012) 140:1006–13. doi: 10.4067/S0034-98872012000800006
45. Vitriol, V, Cancino, A, Leiva-Bianchi, M, Serrano, C, Ballesteros, S, Asenjo, A, et al. Childhood trauma and psychiatric comorbidities in patients with depressive disorder in primary care in Chile. J Trauma Dissociation. (2017) 18:189–205. doi: 10.1080/15299732.2016.1212449
46. Maniglio, R. The impact of child sexual abuse on the course of bipolar disorder: a systematic review. Bipolar Disord. (2013) 15:341–58. doi: 10.1111/bdi.12050
47. Post, RM, Altshuler, L, Leverich, G, Nolen, W, Kupka, R, Grunze, H, et al. More stressors prior to and during the course of bipolar illness in patients from the United States compared with the Netherlands and Germany. Psychiatry Res. (2013) 210:880–6. doi: 10.1016/j.psychres.2013.08.007
48. Belsky, J, and Pluess, M. Beyond diathesis stress: differential susceptibility to environmental influences. Psychol Bull. (2009) 135:885–908. doi: 10.1037/a0017376
49. Mc Quaid, R, Mc Innis, O, Stead, J, Matheson, K, and Anisman, H. A paradoxical association of an oxytocin receptor gene polymorphism: early-life adversity and vulnerability to depression. Front Neurosci. (2013) 7:28. doi: 10.3389/fnins.2013.00128
50. Gibb, B, Chelminski, I, and Zimmerman, M. Childhood emotional, physical, and sexual abuse, and diagnoses of depressive and anxiety disorders in adult psychiatric outpatients. Depress Anxiety. (2007) 24:256–63. doi: 10.1002/da.20238
51. Sheridan, M, Fox, N, Zeanah, C, Mc Laughlin, K, and Nelson, C. Variation in neural development as a result of exposure to institutionalization early in childhood. PNAS Nexus. (2012) 109:12927–32. doi: 10.1073/pnas.1200041109
52. Andersen, S, Tomada, A, Vincow, E, Valente, E, Polcari, A, and Teicher, M. Preliminary evidence for sensitive periods in the effect of childhood sexual abuse on regional brain development. J Neuropsychiatr Clin Neurosci. (2008) 20:292–301. doi: 10.1176/jnp.2008.20.3.292
53. Solé, B, Jiménez, E, Torrent, C, Reinares, M, Bonnin, C, Torres, I, et al. Cognitive impairment in bipolar disorder: treatment and prevention strategies. Int J Neuropsychopharmacol. (2017) 20:670–80. doi: 10.1093/ijnp/pyx032
54. Kapczinski, N, Mwangi, B, Cassidy, R, Librenza-Garcia, D, Bermudez, M, Kauer-Sant’anna, M, et al. Neuroprogression and illness trajectories in bipolar disorder. Expert Rev Neurother. (2017) 17:277–85. doi: 10.1080/14737175.2017.1240615
55. Schwarzer, N, Nolte, T, Fonagy, P, and Gingelmaier, S. Mentalizing and emotion regulation: evidence from a nonclinical sample. IFP. (2021) 30:34–45. doi: 10.1080/0803706X.2021.1873418
Keywords: bipolar disorders, social cognition, child abuse, oxytocin receptors, environment
Citation: Ríos U, Morán J, Hermosilla J, González R, Muñoz P, Arancibia M, Herrera L, Jiménez JP and Moya PR (2023) The interaction of the oxytocin receptor gene and child abuse subtypes on social cognition in euthymic patients with bipolar disorder type I. Front. Psychiatry. 14:1151397. doi: 10.3389/fpsyt.2023.1151397
Edited by:
Hengyi Cao, Feinstein Institute for Medical Research, United StatesReviewed by:
Cecilia Samame, Catholic University of Uruguay, UruguayCopyright © 2023 Ríos, Morán, Hermosilla, González, Muñoz, Arancibia, Herrera, Jiménez and Moya. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ulises Ríos, dWxpc2VzLnJpb3NAdXYuY2w=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.