 Kewei Zheng
Kewei Zheng Huimin Xu1†
Huimin Xu1† Ping Sun
Ping Sun- 1School of Humanities and Social Sciences, Binzhou Medical University, Yantai, China
- 2Qingdao Mental Health Center, Qingdao, China
Background: Interpersonal Psychotherapy-Adolescent Skills Training (IPT-AST) is a standardized depression prevention program for adolescents conducted in campus settings. The purpose of this review is to examine the randomized controlled trials of IPT-AST for the prevention of adolescent depression in the past 20 years.
Methods: A systematic search of relevant electronic databases (PubMed, WOS, Embase, PsycINFO, the Cochrane Library, CNKI and WANFANG DATA) and study reference lists was conducted. Any study investigating the effectiveness of IPT-AST in 12- to 20-year-olds with depressive symptoms was eligible. Synthesis was via narrative summary and meta-analysis.
Results: A total of 6 studies met the inclusion criteria. Meta-analysis results showed a remarkable improvement in patients’ depressive symptoms after IPT-AST intervention (WMD = −5.05, 95% CI = −8.11 to −1.98, p < 0.05, I2 = 77%). Six month follow-up data showed that the intervention outcomes of IPT-AST remained significant (WMD = −3.09, 95% CI: −5.23 to −0.94, p < 0.05, I2 = 57%).
Conclusion: This meta-analysis showed that IPT-AST was effective in adolescents with depressive symptoms at post-prevention and at 6-month follow-up. However, these conclusions are cautious, as they are based on a small number of studies and the presence of author duplication. Future studies should use multi-center, large-sample randomized controlled trials to evaluate the efficacy of IPT-AST for preventing depression in adolescents.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42023393047.
1. Introduction
Adolescent depression is a very common mental illness that can seriously damage the physical and mental health of adolescents (1). Epidemiological surveys show that the prevalence of depression in adolescents ranges from 0.4 to 8.3%, and the prevalence of depressive symptoms ranges from 22 to 60% (2, 3). The ages of 12 to 17 are the high-risk period for adolescent depression (4). A research from Lancet also indicates that approximately one in every five adolescents experiences a depressive episode before the end of puberty (5). Although medication and psychological therapy are commonly used to treat depression and they have been proven to be effective treatments for depression (6–11), evidence suggests that these treatment methods have been found to work for only about 50–60% (12). Therefore, it is necessary to reduce the incidence of depression in adolescents and to prevent it.
The Institute of Medicine (IOM) defines prevention as preventive interventions taken when symptoms have not yet met diagnostic criteria but are present (13). A randomized controlled trial in 2021 showed that timely prevention was effective in reducing depressive symptoms in adolescents (14). Currently, prevention like psychotherapy and psychoeducation are widely employed (13). There is evidence that psychotherapy can effectively prevent depression by alleviating depressive symptoms (15). For adolescents, many studies have shown that poor interpersonal relationships are one of the significant factors contributing to the development of depression in adolescents (16–18). Several studies support the idea that improving relationships may be an important breakthrough in alleviating depressive symptoms and preventing depression (19–21). Interpersonal Psychotherapy - Adolescents (IPT-A) is precisely an interpersonal relationship-based prevention and treatment approach for adolescent depression (22, 23) and focuses on four interpersonal concerns (interpersonal conflicts, role transitions, grieving reactions, and lack of interpersonal relationships) in order to reduce depressive symptoms and enhance interpersonal abilities (24). A meta-analysis showed that IPT-A has a positive effect on alleviating depressive symptoms and preventing depression in adolescents (25). However, traditional psychotherapy such as IPT-A often requires a professional environment, which makes it difficult for some adolescents to obtain timely and effective interventions due to reasons such as distance, cost, or stigma (26).
Interpersonal Psychotherapy-Adolescent Skills Training (IPT-AST) is a school-based preventative approach to manage depression in adolescents (27). It is based on IPT-A and emphasizes that schools are an ideal environment for teaching social skills to adolescents and preventing depression (28). It advocates for improving adolescents’ understanding of depressive symptoms and interpersonal relationship problems through group therapy and psychological education (27). IPT-AST not only overcomes the limitations of traditional psychotherapy locations, but also group therapy delivered in school helps alleviate the adverse effects of cost and shame on adolescents (28). A meta-analysis showed that implementing depression prevention programs in school environments helps adolescents alleviate depressive symptoms and achieve prevention goals (29). In order to test the effectiveness of IPT-AST in preventing depression, Annette (30) implemented it on campus in 14 adolescents aged between 14 and 18 years, who had depressive symptoms but did not meet the diagnostic criteria yet, and the results showed that IPT-AST could effectively prevent depression in adolescents, reduce depressive symptoms and obtain more social support from friends. Therefore, implementing IPT-AST in school for adolescents who have just developed depressive symptoms seems to be an effective measure for preventing depression.
Although IPT-AST has been shown to be effective, the duration of its effect is unclear. Researchers have formed two different views based on multiple studies. Some studies suggest that the prevention effect can last for only 6 months. For example, a randomized controlled trial showed a significant preventive effect of IPT-AST, but its effect did not continue beyond 6 months (31). However, other studies have shown that the preventive effect of IPT-AST can last for 6 months or even longer. Young compared the prevention effects of IPT-AST and School Counseling. The results showed that compared with School Counseling, IPT-AST significantly alleviated the depressive symptoms of adolescents, and the effects lasted for 6 months or longer (32). Currently, there is no systematic review of the duration of prevention effect of IPT-AST. This meta-analysis will comprehensively examine the preventive and follow-up effects of IPT-AST on adolescent depression by including as many randomized controlled trials as possible.
2. Methods
2.1. Protocol and registration
The primary design of present review was registered on PROSPERO (CRD42023393047), and was conformed to the Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) guidelines regarding evidence selection, quality assessment, evidence synthesis, and research reporting [Hutton et al. (33)].
2.2. Search strategy
We use keywords searching in multiple electronic database from January 1,2000 to October 30,2022. The keywords we used for searching include Interpersonal Psychotherapy-Adolescent Skills Training or IPT-AST; and Depression or Depressive symptoms; and Adolescen* or Teen* or Youth* or Young people and we also screened reference lists for additional articles. The databases include PsycINFO; Web of Science; EMBASE; Pubmed; the Cochrane Library; CNKI and WANFANG DATA.
2.3. Inclusion criteria
Studies that met the following criteria were included in the selection:
(1) Participants were adolescents (age from 12 to 20 years old),
(2) Depressive symptoms (scoring above cut-off on a standardized depression rating scale according to the original authors’ definition but does not meet diagnosis of depression),
(3) IPT-AST or minor modifications of IPT-AST,
(4) Compared to any control conditions,
(5) Randomized controlled trials (RCTs),
(6) When data were duplicated in different studies, newly published and data-complete studies were selected.
2.4. Outcomes
Because the IPT-AST is a group depression prevention program conducted on campus, we chose the Center for Epidemiologic Studies-Depression Scale (CES-D), a widely used self-report depression measure with strong psychometric properties with adolescents, to evaluate depression symptoms (34). In the included studies, the main indicator of efficacy was the difference in scores on the standardized scale after prevention and at follow-up.
2.5. Study selection
The search results are extracted and stored in the data management software. Two reviewers (KWZ and HMX) independently reviewed the identified studies and derived data from the enrolled studies. If there is disagreement, it is resolved through discussion and, if necessary, a third author is consulted to reach a final decision.
2.6. Data extraction
The outcomes of interest for this review were depression from validated scales. Two reviewers (KWZ and HMX) independently extracted the data. Relevant data for each measure was entered into Stata 14.0. We examined baseline and post-prevention scores between groups to assess the effectiveness of depression and follow-up effects. If sufficient data were not available in the article, the authors were consulted and additional information requested.
2.7. Assessment of study quality
Two reviewers (KWZ and HMX) independently evaluated the risk of bias in the enrolled studies using the Cochrane Collaboration’s Risk of Bias tool (33). The following criteria were assessed: sequence generation, allocation concealment, blinding of participants and care providers, blinding of outcome assessors, incomplete outcome data, selective outcome reporting and other sources of bias. Each criterion was evaluated as either “high,” “unclear” or “low” risk of bias according to the Cochrane Handbook (35).
2.8. Data items
The following study data were drawn: study characteristics (author, year, study type, follow-up); population characteristics (sample size, age, gender); experimental conditions (prevention group, control group); and outcomes (mean and standard error of scale scores at baseline, post-prevention, and follow-up).
2.9. Statistical analysis
The extracted data was stored in Stata 14.0. Checked for publication bias by Egger’s test. The Q test and I2 statistic were used to examine the heterogeneity, with Q > 0.05 and I2 ≤ 50% indicating low heterogeneity. Sensitivity analyses were performed by removing each eligible study to see whether the significance and the pooled effect size would be affected.
3. Results
3.1. Selection and inclusion of studies
After searching, a total of 119 studies were retrieved; after removing duplicates, 46 studies remained. Two reviewers (KWZ and HMX) performed the initial screening of titles and abstracts, and 31 were excluded, leaving 15 for full-text screening. Finally, 6 studies were included (Figure 1). 757 participants in total for all trials, with participants aged 11 to 18 years and predominantly female, including 366 in the experimental group and 391 in the control group.
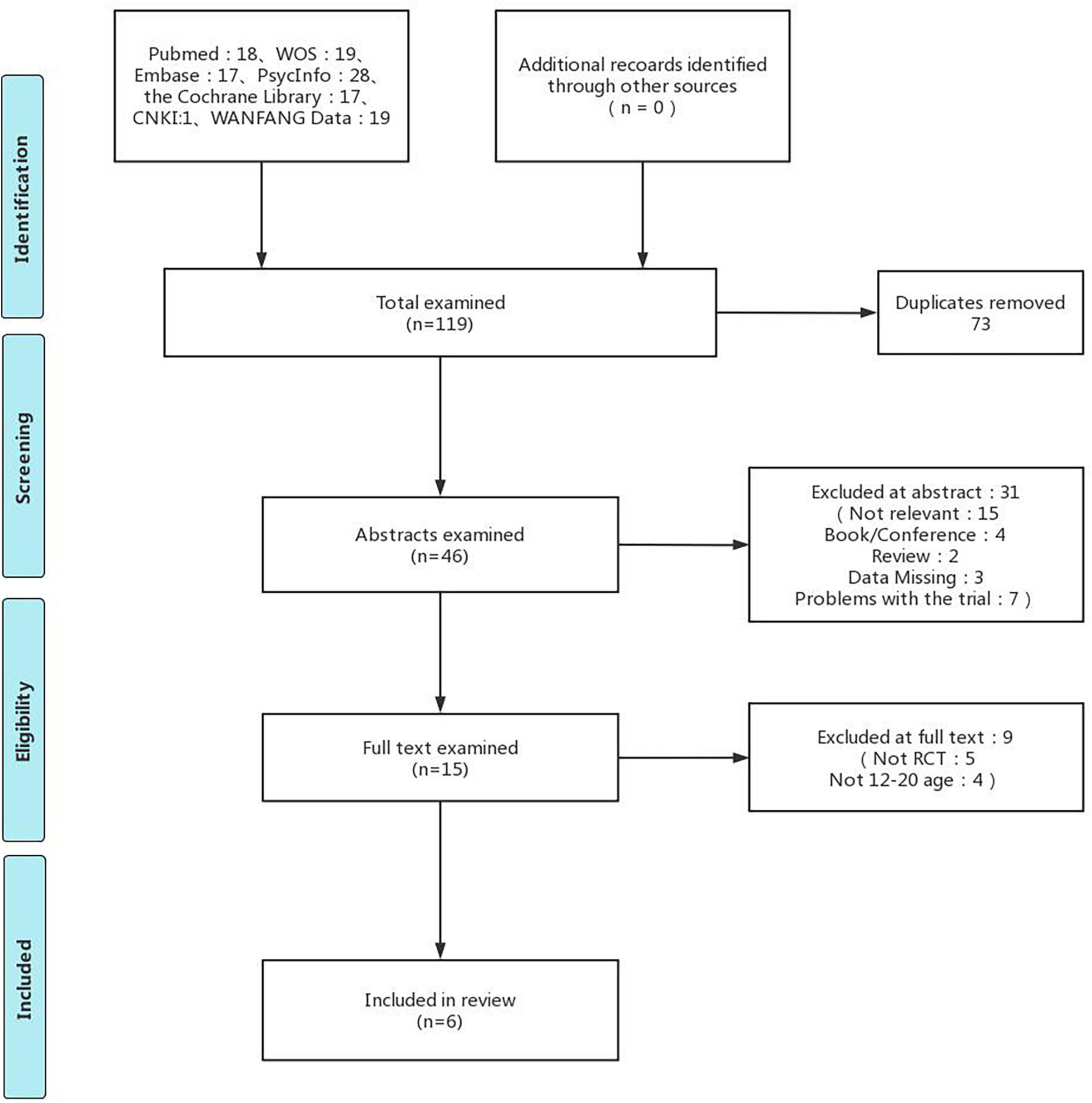
Figure 1. Flow diagram for evidence source search. Adapted with permission from (47), licensed under CC BY-NC 2.0.
3.2. Study characteristics
Among the six enrolled studies (28, 31, 36–39), the age range of the participants was 11–16 years with a mean age of 13.77 years (see Table 1). All studies were conducted in schools, with the experimental group using IPT-AST, five studies (28, 36–39) using school counseling or group counseling on campus as a control group, and one study (31) had a control group without any prevention approach. The studies all used the CES-D to measure participants’ depressive symptoms at baseline, post-prevention, and follow-up. For follow-up, all studies collected data from participants at 6 months of follow-up, and 2 studies (36, 39) collected results at 12 months and beyond.
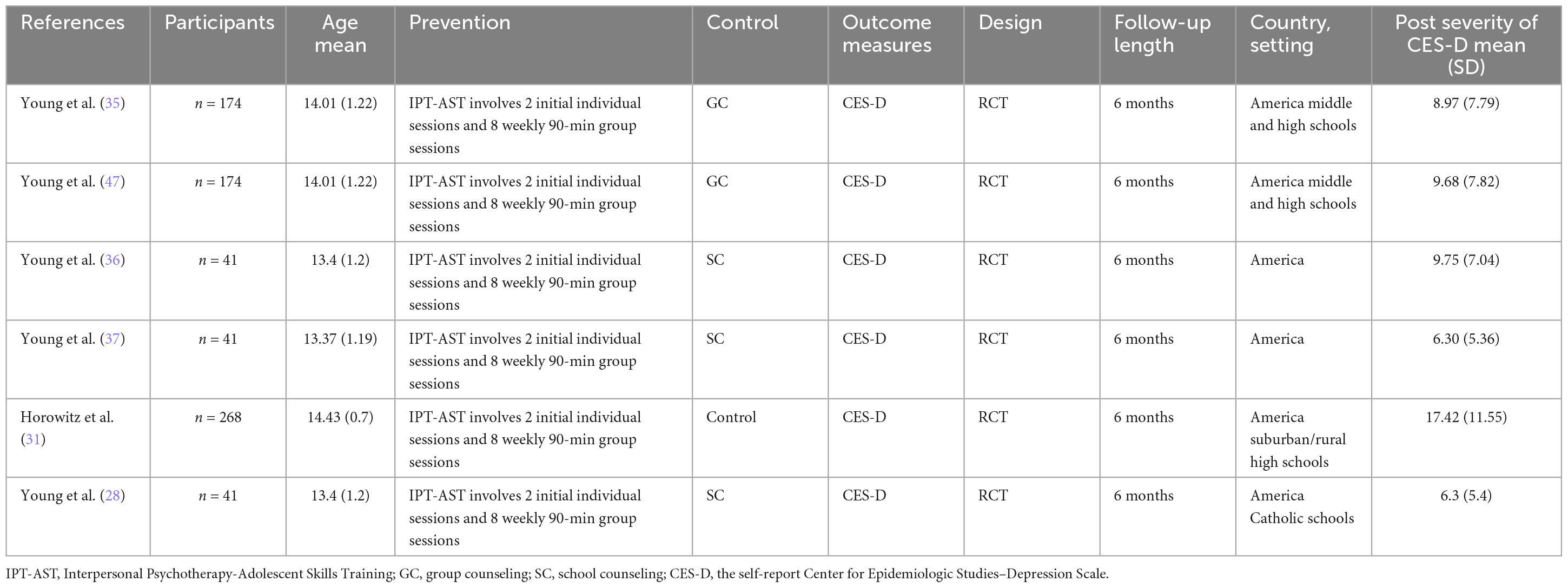
Table 1. Summary description of studies reviewed.
3.3. Risk of bias
The quality of included studies was assessed using the Cochrane Risk of Bias tool (40), and their results are presented (Figure 2). Five studies (28, 31, 36, 37, 39) used a random number table method for random grouping, and one study (38) did not describe the method of random assignment. Six researches explained allocation concealment, and subjects and researchers were unable to predict the outcome of allocation. Five studies (28, 36–39) did not describe in detail the method of blinding of investigators and subjects, and there may be bias. Six studies described methods for blinding study outcome evaluators. Of the follow-up results, five studies (28, 36–39) reported on the presence of missed visits/withdrawals and the reasons for missed visits/withdrawals.
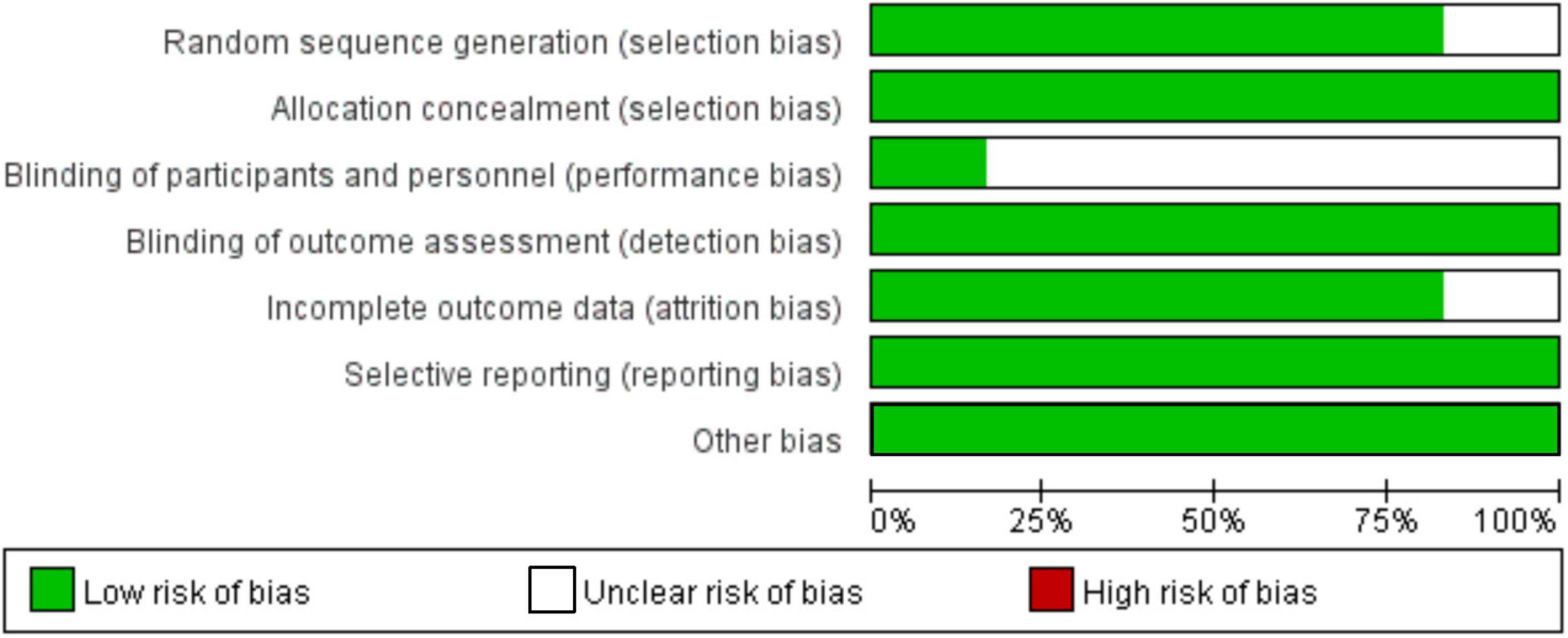
Figure 2. Risk-of-bias chart for studies included in the quantitative analysis.
3.4. Prevention effect of IPT-AST on adolescents with depression
3.4.1. Depression (post-prevention)
For changes in depressive symptoms after the prevention, the results of all six studies were pooled for meta-analysis. The results showed significant improvement in depressive symptoms after the IPT-AST prevention (WMD = −5.05, 95% CI = −8.11 to −1.98, p < 0.05). See forest plot in Figure 3.
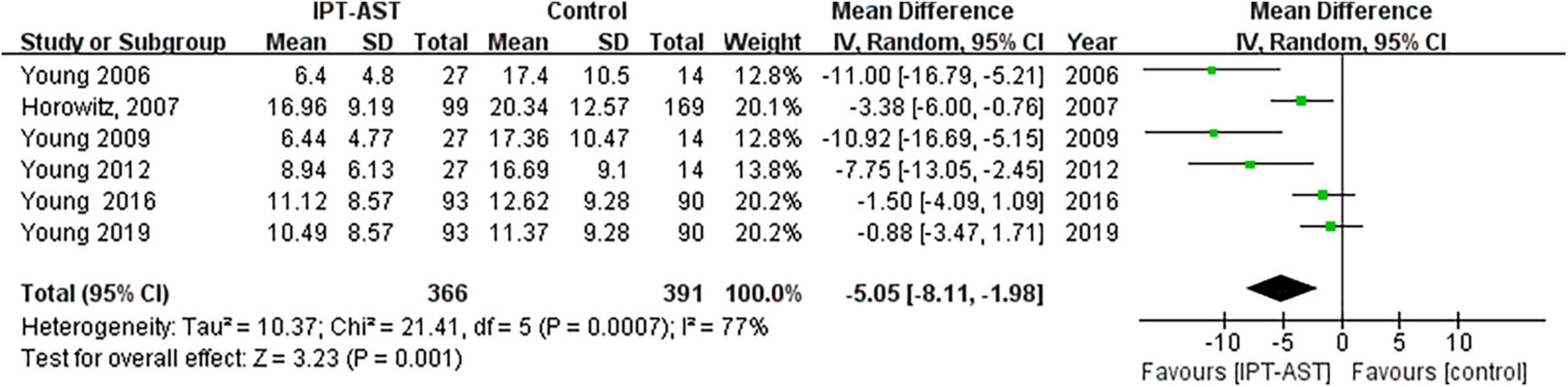
Figure 3. Forest plot showing the outcome of depressive symptoms after prevention.
The results of the meta-analysis of the six trials had a high heterogeneity (I2 = 77%), which may be due, among other things, to the small number of included literature.
3.4.2. Depression (follow-up)
Six trials (n = 729) reported depression at 6-month follow-up; however, 18 individuals were lost to follow-up from prevention. The results showed a significant follow-up effect of IPT-AST for depressive symptoms (WMD = −3.09, 95% CI: −5.23 to −0.94; p < 0.05) and low heterogeneity between studies (I2 = 57%). See forest plot in Figure 4.
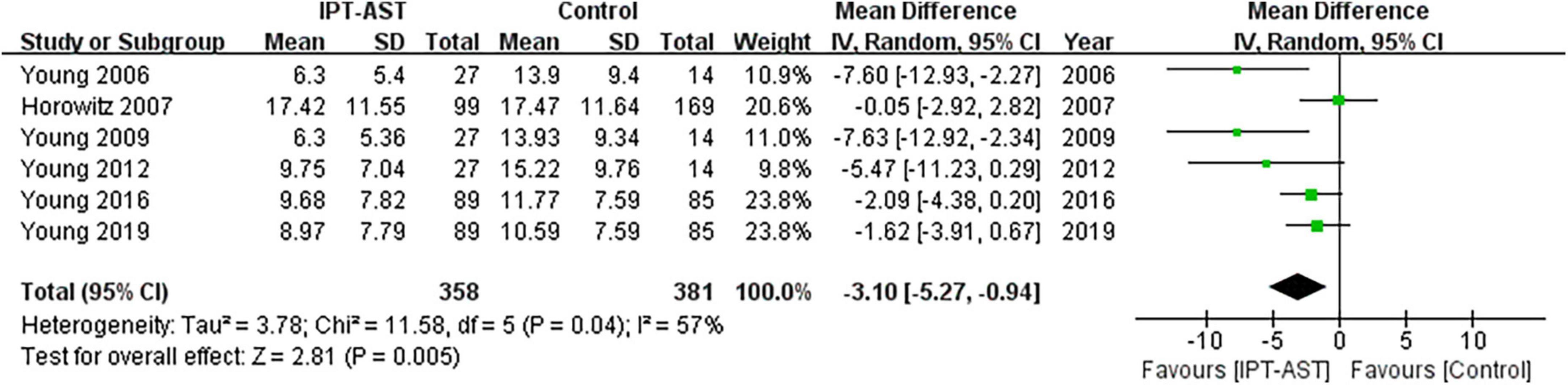
Figure 4. Forest plot showing the outcome of depressive symptoms at follow-up.
4. Discussion
This is the first meta-analysis evaluating the preventive and follow-up effects of IPT-AST on adolescent depression. By summarizing six studies, we found that IPT-AST as a preventative approach was effective in adolescents with depressive symptoms at post-prevention and at a 6-month follow-up. IPT-AST delivered in school overcomes the limitations of traditional treatment settings making it more accessible and promoted (27, 28). Adolescents are more familiar with and accepting of the school environment, so the prevention is easier to carry out there than in hospitals, treatment rooms, and other settings. In addition, IPT-AST focuses on interpersonal relationships which may be a key reason for its effectiveness in preventing depression in adolescents (5). IPT-AST encourages adolescents to practice social skills on campus, which allows them to cope with the interpersonal problems in daily life and maintain the preventive effects. These findings will provide school mental health educators and psychotherapists with new ideas for preventing depression in adolescents.
However, there are several limitations to this study which require caution in interpreting the results. Firstly, IPT-AST was exclusively evaluated in a limited number of schools within the United States; therefore, it is necessary to verify its efficacy in managing adolescent depression symptoms across diverse settings (beyond merely school-based environments) and cultural contexts in future research. Second, five of the six studies included in the meta-analysis belonged to the same research team, but these studies were not conducted at the same time and did not use the same participants and its data; therefore, these studies can be considered as different studies included in the meta-analysis. It is possible that the fact that IPT-AST is in an emerging phase has led to this situation, but this situation may also potentially limit the generalizability of our study findings. Therefore, it should be further explored in future studies. Third, the included studies did not examine the factors (age, country, ethnicity, etc.) that may influence the effectiveness of IPT-AST prevention, so these factors could be further explored in future studies.
Undoubtedly, the current research has systematically evaluated the preventive and follow-up effects of Interpersonal Psychotherapy-Adolescent Skills Training (IPT-AST), and has affirmed its effectiveness within a certain scope. With the outbreak of COVID-19, the concern for physical health has reached a new level along with the concern for mental health. Mental health concerns and research on adolescent populations have increased subsequently (41). One study (42) compared the psychological changes of adolescents before and after the epidemic and noticed that negative emotions among adolescents had significantly increased after the outbreak of the epidemic. Recent studies have also found that the incidence of depression among adolescents has increased during the spread of COVID-19 (43, 44). Therefore, it is crucial to timely prevent adolescent depression and reduce its incidence during this period. IPT-AST can meet this social demand, because it is a group-based depression prevention approach in a campus setting that greatly overcomes the limitations of traditional treatments and increases the efficiency and prevalence of depression prevention (13, 27, 45, 46).
5. Conclusion
This meta-analysis showed that IPT-AST was effective in adolescents with depressive symptoms at post-prevention and at 6-month follow-up. However, these conclusions are cautious, as they are based on a small number of studies and the presence of author duplication. Future studies should use multi-center, large-sample randomized controlled trials to evaluate the efficacy of IPT-AST for preventing depression in adolescents.
Data availability statement
The original contributions presented in this study are included in this article/supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
KZ and HX conceived the study design, searched and screened the article titles and abstracts, confirmed the data and statistical analyses, and responsible for the supervision and quality control. CQ, XS, PS, and NX drafted and supplemented the study methods. PS and NX revised their English and provided the assistance with data analysis. All authors provided the information on the direction of the study and the content of the manuscript and approved the final version of the manuscript.
Funding
This study was supported by the Medical and Health Science and Technology Development Plan of Shandong Province (grant number: 202203090255).
Acknowledgments
We sincerely appreciate thank the reviewers for their comments.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Thapar A, Eyre O, Patel V, Brent D. Depression in young people. Lancet. (2022) 400:617–31. doi: 10.1016/S0140-6736(22)01012-1
3. Egger HL, Angold A. Common emotional and behavioral disorders in preschool children: presentation, nosology, and epidemiology. Child Psychol Psychiatry. (2006) 47:313–17.
4. Herrman H, Patel V, Kieling C, Berk M, Buchweitz C, Cuijpers P, et al. Time for united action on depression: a Lancet-World Psychiatric Association Commission. Lancet. (2022) 399:957–1022. doi: 10.1016/S0140-6736(21)02141-3
5. Thapar A, Collishaw S, Pine DS, Thapar AK. Depression in adolescence. Lancet. (2012) 379:1056–67. doi: 10.1016/S0140-6736(11)60871-4
6. Grossberg A, Rice T. Depression and suicidal behavior in adolescents. Med Clin North Am. (2023) 107:169–82. doi: 10.1016/j.mcna.2022.04.005
7. Méndez J, Sánchez-Hernández Ó, Garber J, Espada JP, Orgilés M. Psychological treatments for depression in adolescents: more than three decades later. Int J Environ Res Public Health. (2021) 18:4600. doi: 10.3390/ijerph18094600
8. World Health Organization. Depression fact sheet. (2020). Available online at: https://www.who.int/news-room/fact-sheets/detail/depression (accessed March 03, 2020).
9. Cipriani A, Zhou X, Del Giovane C, Hetrick SE, Qin B, Whittington C, et al. Comparative efficacy and tolerability of antidepressants for major depressive disorder in children and adolescents: a network meta-analysis. Lancet. (2016) 388:881–90. doi: 10.1016/S0140-6736(16)30385-3
10. Chengke H, Lingli Z, Zengshou W. Research advances in the pharmacological treatment of depression in children and adolescents. Chin J Hosp Pharm. (2009) 1:63–5.
11. Murrin LC, Sanders JD, Bylund DB. Comparison of the maturation of the adrenergic and serotonergic neurotransmitter systems in the brain: implications for differential drug effects on juveniles and adults. Biochem Pharmacol. (2007) 73:1225–36. doi: 10.1016/j.bcp.2007.01.028
12. Treatment for Adolescents With Depression Study Team. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression. JAMA. (2004) 292:807–20.
13. Gladstone TR, Beardslee WR. The prevention of depression in children and adolescents: a review. Can J Psychiatry. (2009) 54:212–21. doi: 10.1177/070674370905400402
14. de Jonge-Heesen KWJ, Rasing SPA, Vermulst AA, Scholte RHJ, van Ettekoven KM, Engels RCME, et al. Secondary outcomes of implemented depression prevention in adolescents: a randomized controlled trial. Front Psychiatry. (2021) 12:643632. doi: 10.3389/fpsyt.2021.643632
15. Wiggins A, Coghill D. Can depression be prevented in children and adolescents? J Paediatr Child Health. (2018) 54:1386–8. doi: 10.1111/jpc.14267
16. Luo XM, Zheng RM, Jin X, Dai X. Global and Chinese perspectives on adolescent health and development. China J Sch Health. (2019) 40:1126–30.
17. Kemp E, Van Zalk MHW. Parent-child relationships and adolescent depression: A systematic review. Dev Rev. (2019) 51:143–67.
18. Feng X, Hu X, Cai T, Liu Q, Sun J. The association between parent-child relationship and depression among Chinese adolescents: The role of coping style. J Affect Disord. (2019) 245:1070–7.
19. Ranney ML, Patena JV, Nugent N, Spirito A, Boyer EW. Social support and depressive symptoms in high-risk adolescents. J Pediatr Health Care. (2017) 31:638–45.
20. Zequinão MA, Laureano PH, Spessato B. Social connectedness, emotional competence and depressive symptoms in adolescent students. Rev Bras Enferm. (2018) 71(Suppl. 1):542–8.
21. Nakamura BJ, Perry C, Morris SB, Okamura KH, Benuto LT, LaFromboise TD. The role of family-level factors in depression among Native Hawaiian youth. J Youth Adolesc. (2019) 48:126–38.
22. Stice E, Shaw H, Bohon C, Marti CN, Rohde P. A meta-analytic review of depression prevention programs for children and adolescents: factors that predict magnitude of intervention effects. J Consult Clin Psychol. (2009) 77:486–503. doi: 10.1037/a0015168
23. Hetrick SE, Cox GR, Merry SN. Where to go from here? An exploratory meta-analysis of the most promising approaches to depression prevention programs for children and adolescents. Int J Environ Res Public Health. (2015) 12:4758–95. doi: 10.3390/ijerph120504758
24. Moreau D, Mufson L, Weissman MM, Klerman GL. Interpersonal psychotherapy for adolescent depression: description of modification and preliminary application. J Am Acad Child Adolesc Psychiatry. (1991) 30:642–51. doi: 10.1097/00004583-199107000-00018
25. Li J, Liang JH, Li JY, Qian S, Jia RX, Wang YQ, et al. Optimal approaches for preventing depressive symptoms in children and adolescents based on the psychosocial interventions: A Bayesian Network Meta-Analysis. J Affect Disord. (2021) 280(Pt A):364–72. doi: 10.1016/j.jad.2020.11.023
26. Cui J, Shu Y, Zhou C. Research progress on the preventive effect of interpersonal psychotherapy adolescent skills training on adolescent depression. Neural Injury Funct Reconstr. (2021) 16:274–6. doi: 10.16780/j.cnki.sjssgncj.20200937
27. Kodish T, Weiss B, Duong J, Rodriguez A, Anderson G, Nguyen H, et al. Interpersonal psychotherapy-adolescent skills training with youth from Asian American and immigrant families: cultural considerations and intervention process. Cogn Behav Pract. (2021) 28:147–66. doi: 10.1016/j.cbpra.2020.05.009
28. Young JF, Mufson L, Davies M. Efficacy of interpersonal psychotherapy-adolescent skills training: an indicated preventive intervention for depression. J Child Psychol Psychiatry All Discip. (2006) 47:1254–62. doi: 10.1111/j.1469-7610.2006.01667.x
29. Werner-Seidler A, Spanos S, Calear AL, Perry Y, Torok M, O’Dea B, et al. School-based depression and anxiety prevention programs: an updated systematic review and meta-analysis. Clin Psychol Rev. (2021) 89:102079. doi: 10.1016/j.cpr.2021.102079
30. La Greca AM, Ehrenreich-May J, Mufson L, Chan S. Preventing adolescent social anxiety and depression and reducing peer victimization: intervention development and open trial. Child Youth Care Forum. (2016) 45:905–26. doi: 10.1007/s10566-016-9363-0
31. Horowitz JL, Garber J, Ciesla JA, Young JF, Mufson L. Prevention of depressive symptoms in adolescents: a randomized trial of cognitive-behavioral and interpersonal prevention programs. J Consult Clin Psychol. (2007) 75:693–706. doi: 10.1037/0022-006X.75.5.693
32. Young JF, Mufson L, Gallop R. Preventing depression: a randomized trial of interpersonal psychotherapy-adolescent skills training. Depress Anxiety. (2010) 27:426–33. doi: 10.1002/da.20664
33. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. (2015) 162:777–84.
34. Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol Meas. (1977) 1:385–401. doi: 10.1177/014662167700100306
35. Schunemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou PP, et al. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JPT, Deeks JJ editors. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. London: Cochrane (2011).
36. Young JF, Jones JD, Sbrilli MD, Benas JS, Spiro CN, Haimm CA, et al. Long-term effects from a school-based trial comparing interpersonal psychotherapy-adolescent skills training to group counseling. J Clin Child Adolesc Psychol. (2019) 48(sup1):S362–70. doi: 10.1080/15374416.2018.1479965
37. Young JF, Benas JS, Schueler CM, Gallop R, Gillham JE, Mufson L. A randomized depression prevention trial comparing interpersonal psychotherapy–adolescent skills training to group counseling in schools. Prev Sci. (2016) 17:314–24. doi: 10.1007/s11121-015-0620-5
38. Young JF, Makover HB, Cohen JR, Mufson L, Gallop RJ, Benas JS. Interpersonal psychotherapy-adolescent skills training: anxiety outcomes and impact of comorbidity. J Clin Child Adolesc Psychol. (2012) 41:640–53. doi: 10.1080/15374416.2012.704843
39. Young JF, Gallop R, Mufson L. Mother-child conflict and its moderating effects on depression outcomes in a preventive intervention for adolescent depression. J Clin Child Adolesc Psychol. (2009) 38:696–704. doi: 10.1080/15374410903103577
40. Higgins JP, Altman DG, Sterne JA. Assessing risk of bias in included studies. In: Higgins JPT, Green S editors. Cochrane Handbook for Systematic Reviews of Interventions: Version 5.1. London: Cochrane (2011).
41. Gabriel IWM, Lima DGS, Pires JP, Vieira NB, Brasil AAGM, Pereira YTG, et al. Impacts of COVID-19 on children and adolescents: A systematic review analyzing its psychiatric effects. World J Psychiatry. (2022) 12:1313–22. doi: 10.5498/wjp.v12.i11.1313
42. Molnar DS, Thai S, Blackburn M, Zinga D, Flett GL, Hewitt PL. Dynamic changes in perfectionism dimensions and psychological distress among adolescents assessed before and during the COVID-19 pandemic. Child Dev. (2022) 94:254–71. doi: 10.1111/cdev.13855
43. Petruzzelli MG, Furente F, Colacicco G, Annecchini F, Margari A, Gabellone A, et al. Implication of COVID-19 pandemic on adolescent mental health: an analysis of the psychiatric counseling from the emergency room of an Italian University hospital in the years 2019-2021. J Clin Med. (2022) 11:6177. doi: 10.3390/jcm11206177
44. Mercader Rubio I, Sánchez-López P, Ángel NG, Ruiz NFO. Psychological consequences of fear of COVID-19: symptom analysis of triggered anxiety and depression disorders in adolescents and young adults. Int J Environ Res Public Health (2022) 19:14171. doi: 10.3390/ijerph192114171
45. Sbrilli MD, Jones JD, Kanine RM, Gallop R, Young JF. The depression prevention initiative: trauma as a moderator of prevention outcomes. J Emot Behav Disord. (2022) 30:247–59. doi: 10.1177/1063426620945665
46. Filia K, Eastwood O, Herniman S, Badcock P. Facilitating improvements in young people’s social relationships to prevent or treat depression: a review of empirically supported interventions. Transl Psychiatry. (2021) 11:1–10. doi: 10.1038/s41398-021-01406-7
Keywords: Interpersonal Psychotherapy-Adolescent Skills Training, depression, adolescents, systematic review, meta-analysis
Citation: Zheng K, Xu H, Qu C, Sun X, Xu N and Sun P (2023) The effectiveness of Interpersonal Psychotherapy-Adolescent Skills Training for adolescents with depression: a systematic review and meta-analysis. Front. Psychiatry 14:1147864. doi: 10.3389/fpsyt.2023.1147864
Received: 19 January 2023; Accepted: 17 July 2023;
Published: 31 July 2023.
Edited by:
Iman Permana, Muhammadiyah University of Yogyakarta, IndonesiaReviewed by:
Rolf Holmqvist, Linköping University, SwedenPaul Badcock, The University of Melbourne, Australia
Copyright © 2023 Zheng, Xu, Qu, Sun, Xu and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Na Xu, TWVuZ2ZlaTk5XzBAMTYzLmNvbQ==; Ping Sun, cWRzdW5waW5nOTlAc2luYS5jb20=
†These authors have contributed equally to this work