 Che Jiang
Che Jiang Wei Chen
Wei Chen Ling Tao3
Ling Tao3 Zijuan Qi
Zijuan Qi Xifu Zheng
Xifu Zheng
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Psychiatry , 15 February 2023
Sec. Anxiety and Stress Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1090290
This article is part of the Research Topic Women in Psychiatry 2022: Anxiety and Stress Disorders View all 3 articles
Introduction: Hospital is a stressful place of employment, and a high proportion of healthcare workers, especially the ICU (Intensive Care Unit) nurses were found to be at risk of PTSD. Previous studies showed that taxing working memory through visuospatial tasks during the reconsolidation process of aversive memories can reduce the number of intrusions afterwards. However, the finds could not be replicated by some researches, indicating there may be some boundary conditions that are subtle and complex.
Methods: We performed a randomized controlled trial (ChiCTR2200055921; URL: www.chictr.org.cn). In our study, a series of ICU nurses or probationers who performed a cardiopulmonary resuscitation (CPR) were enrolled and instructed to play a visuospatial music tapping game (“Ceaseless Music Note”, CMN; Beijing Muyuan Technology Co., Ltd., Beijing, China) at the fourth day after CPR. The numbers of intrusions each day were recorded from the first to the seventh days (24 h×6 day), and the vividness and emotionality of CPR memories were rated at the 4th and 7th days. These parameters were compared between different groups (game with background sound; game with sound off; sound only; none).
Results: The game-matching background music can have an add-on effect for single tapping game with no sound in reducing the emotionality of previous aversive memories.
Discussion: We proposed that flow experience (the subjective experience of effortless attention, reduced self-awareness, and enjoyment, and may be induced by optimal skill-demands compatibility in challenging tasks) as a key boundary condition for successful reconsolidation intervention.
Clinical trial registration: www.chictr.org.cn, identifier: ChiCTR2200055921.
Exposure therapy represents a major cognitive behavioral treatment for anxiety disorders like posttraumatic stress disorder (PTSD) (1, 2). Through repeated exposing of individuals to the feared objects or situations in a safe environment, the fear is to be reduced. Yet, despite its efficacy, exposure therapy has some shortcomings including high drop-out rate [estimated to be 36% among individuals with PTSD (3)] and relapse rate [the estimated return of fear ranges from 19% to 62% (4)], and it is not always effective (5, 6). Specifically, the cause of high relapse rate is considered owing to the mechanism underlying the exposure therapy, which relies on the competition between the memory of the past distressing experience and the newly-formed memory of safety. Accordingly, efforts have been made to directly change the original distressful memory to reduce the possibility of relapse. Over the past two decades, abundant studies have demonstrated that under certain retrieval conditions, even long-established and consolidated memories can be induced to a transient labile state, during which they are susceptible to interference before being reconsolidated (7–9). Thus, the process of reconsolidation intervention comprised two dissociable stages: a prior stage of retrieval to induce destabilization of the targeted memory and a following stage of restabilization in an updated form (10). Behavioral therapies and pharmacological agents are two ways of interference in the second stage.
Behavioral ways include exposure therapy (11, 12) and taxing working memory through visuospatial tasks [e.g., concealed complex pattern tapping (13), eye movement desensitization and reprocessing, and the computer game Tetris (14)]. It is important to note that these behavioral procedures targeted different aspects of the memory. In the Tetris game, different shaped blocks fall from the top to the bottom of the screen one at a time, and players gain scores by using arrow keys to rotate and move each block when it is falling to form a full horizontal line. All full lines of blocks are removed. The speed of block falling increases gradually, and the game ends when the blocks are stacked to the top of the screen. Playing the Tetris game was recently found to be a simple and easily-accessible procedure that can effectively reduce the number of intrusive memories, which is the “core clinical feature” [a term forwarded by Kupfer and Regier (15)] of PTSD and acute stress disorder (16), of both experimental traumas (17–19) and real-world traumas (20–22). The theoretical basis for the effectiveness of visuospatial tasks is that most intrusive memories are visual imageries (23, 24), thus can be selectively disrupted by taxing working memory via competition for limited cognitive resources (25–27) when that memory is labile. However, this theory was challenged by some researches with negative results (28, 29), and also the effects of Tetris game play could not be replicated by some researchers (30, 31). These results indicate that there may be some boundary conditions that are subtle and complex. One of the proposed factors that may be critical for the psychobiological impact of gameplay is “flow experience” (29), which refers to the subjective experience of effortless attention, reduced self-awareness, and enjoyment, and may be induced by optimal skill-demands compatibility in challenging tasks (32).
In the studies of auditory intrusions, results showed that taxing working memory during memory recall would result in decreases in vividness and emotionality, and this effect may be modality matching (33, 34) as well as cross modal (i.e., a mismatch between visual modality of the intervention and the auditory modality of the recalled memory) (35–37). Thus, one would presume that adding auditory intervention may increase the interventional effect of visuospatial tasks.
Hospital is a stressful place of employment, and a high proportion of healthcare workers were found to be at risk for PTSD (38). Specifically, the ICU nurses are frequently exposed to work-related stresses, such as end-of-life issues, performing cardiopulmonary resuscitation (CPR), postmortem care, and prolonging life by artificial support to critically ill patients (39). They are predisposed to develop work-related psychological disorders including PTSD, the prevalence of which is approaching 25% (39, 40). These findings underlined the importance of developing preventive therapies and treatment of PTSD for ICU nurses. This will not only improve their mental health, but also improve their job satisfaction, and reduce the growing exodus of nursing from their profession (40). It is estimated that between 40 and 84% of all CPR attempts in ICU result in immediate or imminent death of the patient within 24 h (41–45). During CPR, the physical signs and sounds (e.g., color changes, gasping, emesis, and indignities suffered by patients) are perceived as stressful by nurses (46). Unsuccessful CPR represents one of the major traumatic events for ICU nurses, and may eventually lead to PTSD (39, 47, 48).
In the present study, we conducted a randomized controlled trial with a series of ICU nurses or probationers who performed a CPR in <12 h. We tested the hypothesis that: (a) a new visuospatial music tapping game (“Ceaseless Music Note”, CMN; Beijing Muyuan Technology Co., Ltd., Beijing, China) applied at 3 days after CPR can reduce the number of intrusive memories, as well as the vividness and emotionality of CPR recalls; (b) background music can have an add-on effect in this reconsolidation intervention, especially for auditory intrusions, either by exerting additional cognitive taxing on players or by the state of flow experience.
This was an exploratory open-label randomized controlled trial (ChiCTR2200055921). The investigation was carried out in accordance with the latest version of the Declaration of Helsinki, and was approved by The Ethics Committee of General Hospital of Southern Theatre Command. This study's design and hypotheses were preregistered; see [www.chictr.org.cn]. The data was shared on the website www.medresman.org.cn. The flow diagram was shown in Figure 1.
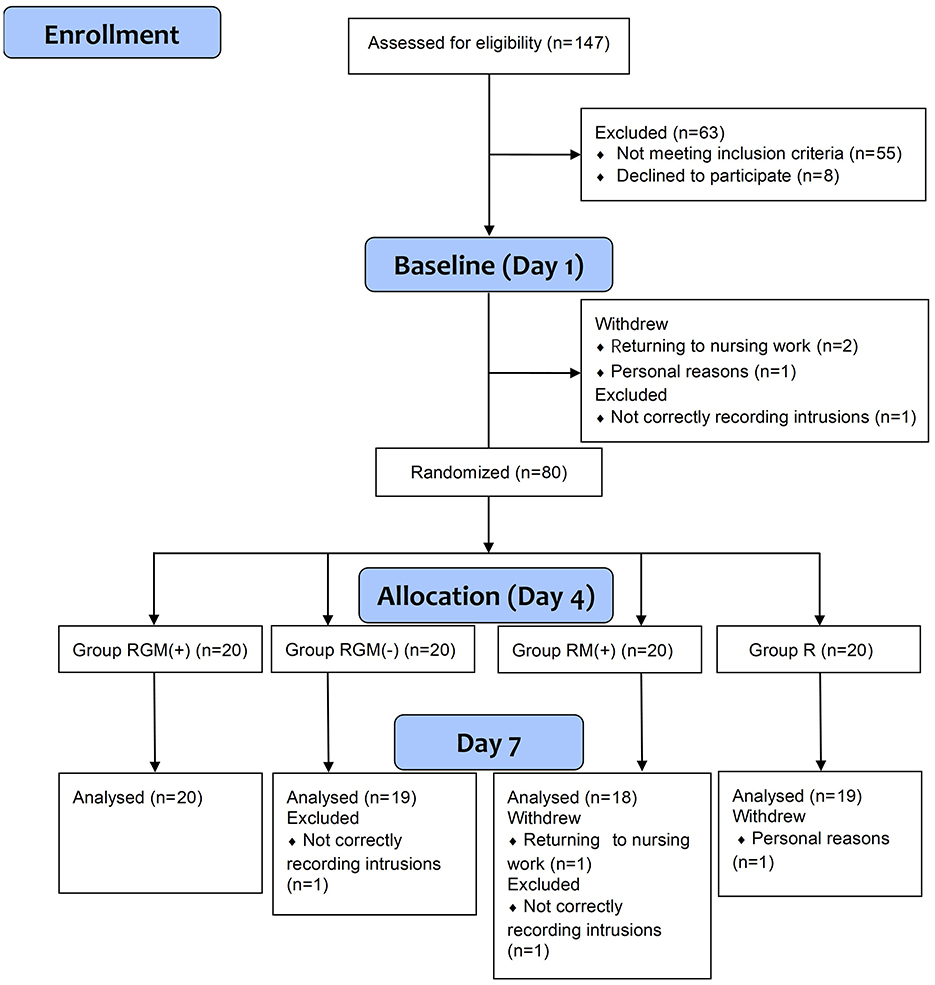
Figure 1. Flow diagram of this study.
Female nurses or probationers who had participated a CPR during the previous 12 h in the General Hospital of Southern Theatre Command were screened. Inclusion criteria were as follows: nurses participating CPRs in our hospital within 12 h; after CPR, they can change from clinical nursing work to clerical work for the next 6 days; female sex; aged between 18 and 40 years; no acute serious illness; mother tongue is Chinese; signed written informed consent. Exclusion criteria were as follows: frequent CMN players; have experienced other CPRs in the past 1 month; participate in CPR twice or more during the trial period; failure to sleep on time due to CPR; history of mental illness; alcohol or drug abuse; have experienced severe traumatic events recently; hearing impairment. Participants who did not complete the whole process of this trial were further excluded. Potential participants were identified by a staff of our research team. Eligibility was assessed by face-to-face interview. All participants were asked to keep to a regular daily schedule during the trial period.
Sample size was calculated based on results of previous studies (49). We set α = 0.05, β = 0.1, Ψ = 2.17, = 10, = 8, = 5, = 5, S1 = 6, S2 = 5, S3 = 5, S4 = 4. By referring to the sample size estimation table, we got a total sample size of n=80 for four parallel groups.
Eighty female nurses were randomized. One participant withdrew from the trial due to accidental reasons that they had to return to nursing work. One participant withdrew from the trial for personal reasons. Two participant was excluded for not correctly recording intrusions. Thus, a total of 76 participants were included for the final analysis.
The participants were randomly assigned in a 1:1:1:1 ratio to four groups by random number table: reminder plus playing CMN with background music [group RGM (+)], reminder plus playing CMN with background music off [group RGM (-)], reminder plus only background music [group RM (+)], and only reminder (group R).
Age, the second edition of Beck Depression Inventory (BDI-II) (50), State-Trait Anxiety Inventory (STAI-T) (51), and negative emotion caused by CPR were recorded.
The Chinese version of BDI-II was used to measure depressive symptoms. It contains 21 items with each item evaluated ranging from 0 to 3. Higher total scores indicate higher severity of depression. Total scores of ≤ 10 indicate no depressive symptoms. The BDI-II has high internal consistency in clinical outpatients (α = 0.92) and student samples (α = 0.93) (50).
The Chinese version of the trait subscale of STAI (STAI-T) was used to evaluate trait anxiety. It consists of 20 items, and each item is rated from 1 (not at all) to 4 (extremely). Higher scores indicate higher severity of trait anxiety.
Also, participants rated their mood responses after CPR: “to what extent do you feel sad/fearful/shocked about the event?” from 0 (not at all) to 10 (extremely).
Intrusive memory was defined as the spontaneous appearance of the CPR scene (not memories that are deliberately recalled), and the content must be image-based (visually) or sound-based (auditory; replay of the scene, including both verbal and nonverbal sound). The diary was divided into three sections (morning, afternoon and evening). Participants were required to mark in the corresponding sections when intrusive memory occurs, and record the content and categories overleaf. The diary was checked to be up-to-date at a fixed time every day. On day 4 and day 7, participants rated their compliance to diaries of the past 72 h (0–10 points: 0 points means completely inaccurate, and 10 points means very accurate).
For the memory reminder cue, all participants were asked to think back to the CPR and briefly tell the researcher the worst moments that came to mind (≈1 min).
Vividness and emotionality of the recalled event were rated respectively on visual analog scales (VASs) from 0 (not at all vivid/unpleasant) to 100 (very vivid/unpleasant). Vividness is defined as “memories that are very clear and detailed”, and emotionality is defined as “memories that give you an unpleasant feeling when you recall them”.
“Ceaseless Music Note (CMN)” (Beijing Muyuan Technology Co., Ltd., Beijing, China) is a visual spatial tapping game played on smartphone app. In the game, when music/songs are being played, there are boxes fall with a stable speed from the top of the screen to the bottom of the screen in four routes and players need to tap on one of the four keys at the bottom of the route when boxes pass the key. The boxes pass the key in a pace conformed to the music, and the more exact the players press the key, the higher they score in the game. The boxes may be blue (needs single press) or green with a trajectory (needs press and horizontal slip to nearby keys). Most of the music in the game are popular songs. The game can also be played with sound off when participants only press the falling boxes without listening. All participants wore headphones whether the sound was on or not. Participants in the music only group simply chose and listened to the listed music in the game but were not allowed to see or tap on the screen.
Concentration (How well did you concentrate on the game/music?), enjoyment (How much did you enjoy the game/music?), difficulty (How difficult was the game for you?), and addiction (How much do you want to continue the game/music you just played/listened?) were rated on separate scales from 0 (not at all) to 10 (extremely).
The Intrusion subscale of IES-R (52) was applied on Day 7 to assess participants' distress related to the experimental trauma during the past 6 days. The 22-item scale is comprised of 3 subscales representative of the major symptom clusters of posttraumatic stress: intrusion (8 items), avoidance (8 items), and hyperarousal (6 items). Each item is rated from 0 (not at all) to 4 (extremely).
On day 7, participants were asked to rate how much they believed playing the game/listening to the music 3 days after CPR would increase or decrease the intrusive visual or auditory memories from −10 (extremely decrease), 0 (no impact) to 10 (extremely increase).
Day 1: (Figure 2) Participants were recruited according to inclusion and exclusion criteria, and signed informed consents. Baseline characteristics were recorded: age, BDI-II, STAI-T. Participants rated their mood responses after CPR. Then, participants practiced playing CMN game for 3 min with matching music. They were instructed to note down intrusive memories in the next 72 h.
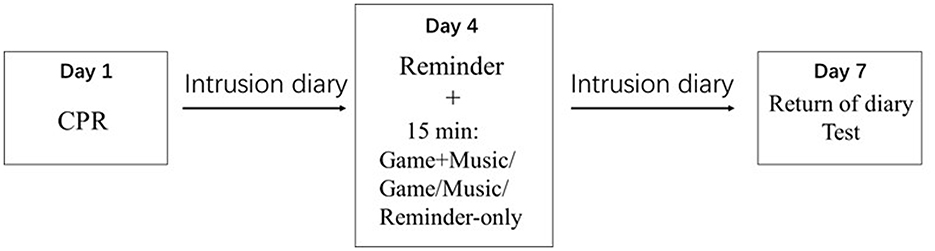
Figure 2. General study design.
Day 4: Participants returned to the laboratory, handed in their diaries, and rated their compliance to diaries. Participants were then randomly allocated in a 1:1:1:1 ratio to four parallel treatment conditions [RGM (+), RGM (-), RM (+), and R)]. For the memory reminder cue, all participants were asked to think back to the CPR and briefly told the researcher the worst moment that came to mind (<1 min). Then participants rated the vividness and emotionality of the recalled event respectively. After 5 min' break, the intervention began: participants in the RGM (+) group started game with music; those in the RGM (-) group started game without music; those in the RM (+) group listened to music, but were not allowed to play the tapping game; those in the R group sat quietly for 15 min. Each piece of music (or single game without music) lasted for ~1.5 min. Participants were given several seconds of interval to choose their preferred music to play, and for ~15 min in total. We chose the duration of 15 min because it's an average interventional duration for Tetris game, and many studies have demonstrated its efficacy. Additionally, the CMN game used in our study seemed to be more attracting than Tetris (images more colorful and with pleasant music), so we did not increase the playing time. The difficulty levels were set as “simple” (5 pieces) and “difficult” (4 pieces) and “master” (1 piece). This difficulty ensured that the majority of the boxes could be pressed by the participants but with some difficulty, so that the participants could keep concentrated and feel enjoyable. Participants were encouraged to reach scores as high as they can. After the game/music, participants needed to rate the levels of concentration, enjoyment, difficulty, and addiction. Participants were instructed to note down intrusive memories in the next 72 h.
Day 7: Participants returned to the laboratory, handed in their diaries, and rated their compliance to diaries. They again thought back to the CPR and told it to the researcher, and then rated the vividness and emotionality. Participants were also asked to complete the IES-R scales for the impact of CPR in the past week, and to rate the demand ratings. Finally, all participants were thanked and reimbursed for taking part.
Baseline variables (age, BDI-II, STAI-T, sad/fearful/shocked level), diary compliance, game scores, pre-intervention vividness/emotionality of CPR memories, the mean number of pre-intervention intrusions (days 1 to 3), concentration/difficulty/enjoyment/addiction level, demand ratings, IES-R were analyzed using Kruskal-Wallis tests or Mann-Whitney U tests.
Quade test (non-parametric ANCOVA) was used to test between-group comparisons in the mean number of intrusions post-intervention (days 4 to 6) and in the post-intervention vividness/emotionality, followed by planned comparisons (Games-Howell corrected) (49).
Day-to-day differences in the number of intrusions from day 3 to 4 were analyzed using a two-way mixed ANOVA with time as within-subjects factor and group as between-subjects factor.
Statistical analysis was performed by Statistical Package for the Social Sciences (version 19.0 for Windows; SPSS, Chicago, IL, USA). Two-tailed tests were used and a P < 0.05 was considered significant.
Baseline characteristics, diary accuracy, demand ratings, and game score/difficulty of the 76 participants were listed in Table 1. No significant difference of these variables was found among different groups.
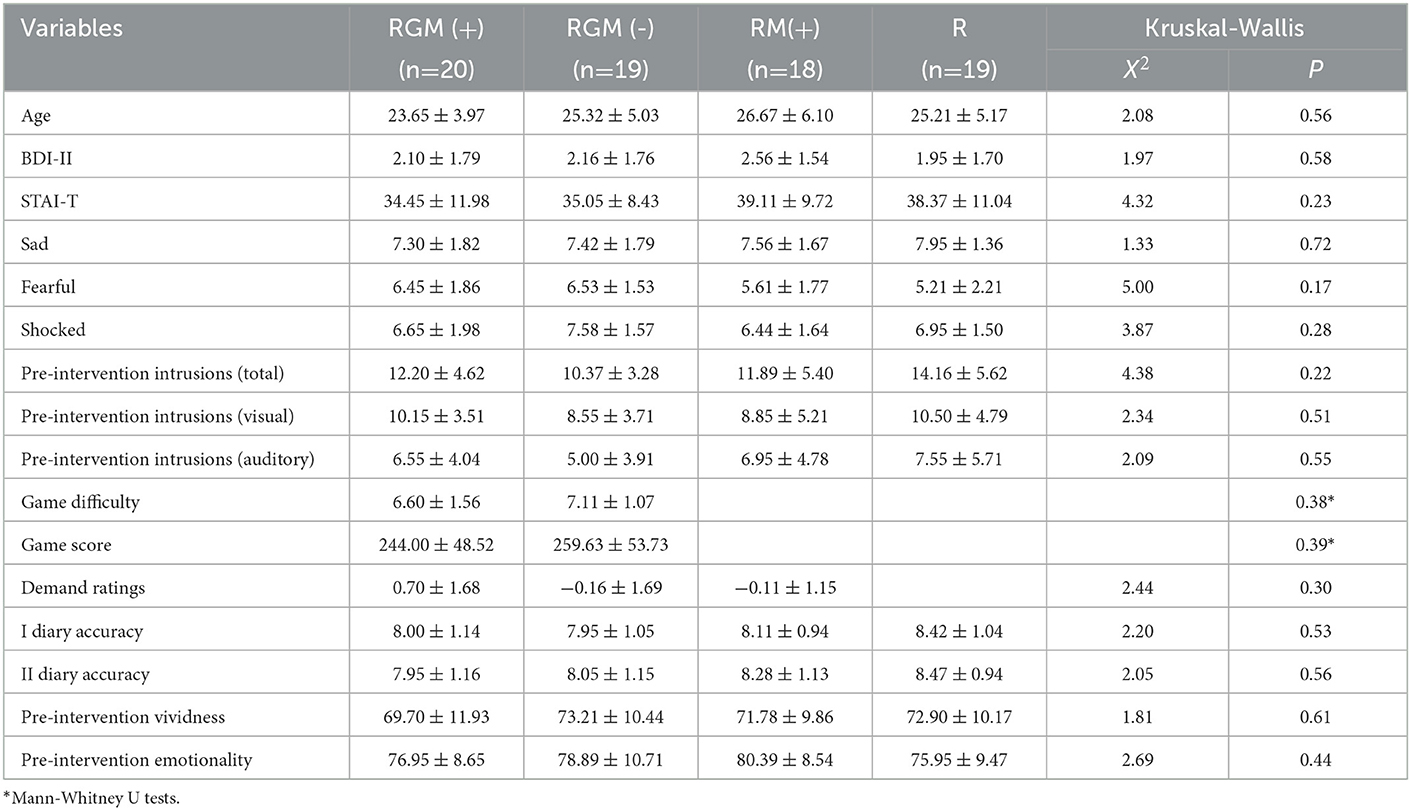
Table 1. Baseline characteristics (variables were presented as mean ± SD).
The mean number of intrusions on each day were shown in Figure 3. The Quade test and one-way ANOVA test of unstandardized residuals of a regression analysis (number of intrusions before intervention on number of intrusions after intervention) showed no significant effect of intervention type on numbers of total intrusions or visual or auditory intrusions (MRGM(+) = −4.60 ± 5.32, MRGM(−) = −3.32 ± 4.58, MRM(+) = −4.56 ± 4.79, MR = −7.26 ± 6.05, F3,72 = 0.35, P = 0.79, η2 = 0.014 for total intrusions; F3,72 = 0.63, P = 0.60, η2 = 0.026 for visual intrusions; F3,72 = 0.82, P = 0.49, η2 = 0.033 for auditory intrusions).
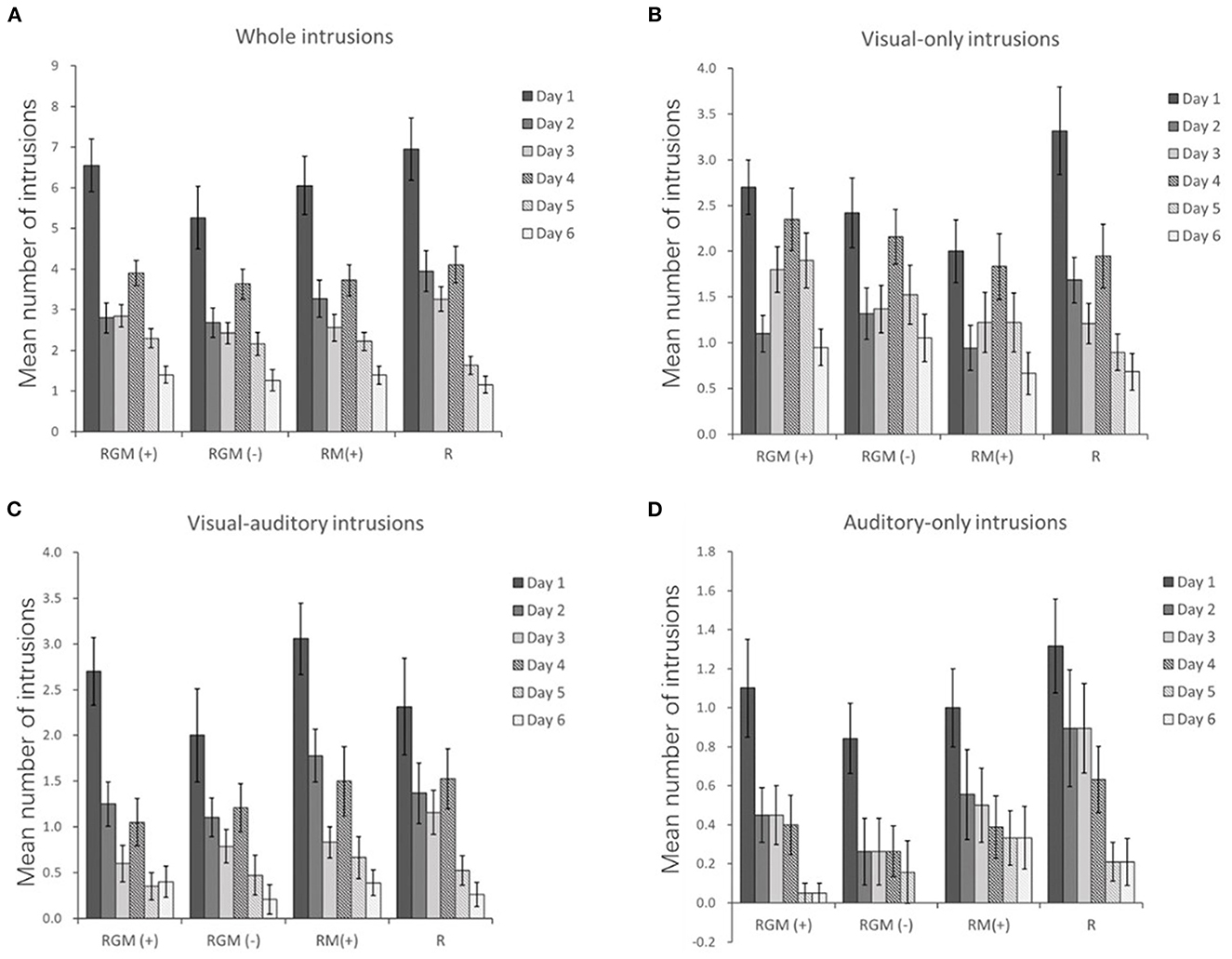
Figure 3. Trajectory of mean number of whole (A), visual-only (B), visual-auditory (C), and auditory-only (D) intrusions. Error bars depict SEMs.
To analyze the number of intrusions from day 3 to day 4 between groups, a two-way mixed ANOVA revealed a significant main effect of time (F1,43.23=19.77; P<0.001; η2 = 0.12), but no significant main effect of group (F3,3.20 = 1.46; P = 0.23; η2 = 0.03) or a time×group interaction (F3,0.26 = 0.12; P = 0.95; η2 = 0.002).
The Quade test and one-way ANOVA test of unstandardized residuals of a regression analysis (vividness before intervention on vividness after intervention) showed no significant effect of intervention type on the degree of vividness (MRGM(+) = −6.45 ± 7.72, MRGM(−) = −5.00 ± 8.78, MRM(+) = −3.06 ± 7.56, MR = −7.84 ± 6.85; F3,72 = 1.97, P = 0.13, η2 = 0.076; Figure 4A).
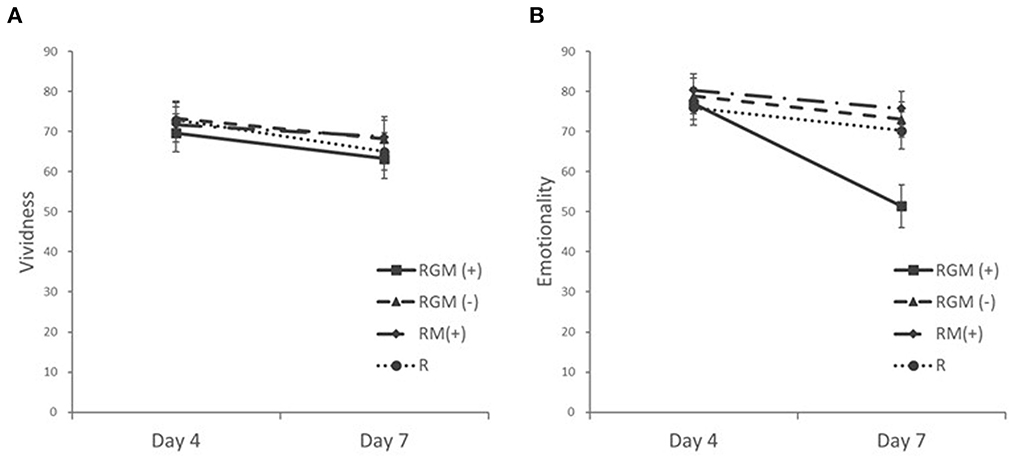
Figure 4. Mean vividness (A) and emotionality (B) ratings at pre-intervention (Day 4) and post-intervention (Day 7). Error bars depict SEMs.
The Quade test and one-way ANOVA test of unstandardized residuals of a regression analysis (emotionality before intervention on emotionality after intervention) showed a significant effect of intervention type (MRGM(+) = −25.55 ± 13.59, MRGM(−) = −5.84 ± 7.78, MRM(+) = −4.56 ± 8.70, MR = −5.63 ± 7.33; F3,72 = 17.76, P<0.001, η2 = 0.425; Figure 4B). Planned comparisons (Games-Howell) between all groups showed that the RGM (+) group had a significantly larger decrease in emotionality after intervention compared to the RGM (-) group (Mean differenceResiduals = −26.47, SE = 4.73, P<0.001), the RM (+) group (Mean differenceResiduals = −29.63, SE = 5.08, P<0.001) and the R group (Mean differenceResiduals = −25.32, SE = 4.93, P < 0.001).
No significant difference of IES-R intrusions subscale scores was found between the four groups (MRGM(+) = 9.65 ± 4.63, MRGM(−) = 8.79 ± 4.86, MRM(+) = 7.89 ± 3.20, MR = 9.11 ± 5.11; X2 = 1.03, P = 0.79).
Kruskal-Wallis tests showed significant difference of concentration (X2 = 10.58, P = 0.01), enjoyment (X2 = 29.15, P < 0.001), and addiction (X2 = 22.95, P < 0.001) ratings among the three groups. Mann-Whitney U tests further showed significant difference of enjoyment (MRGM(+) = 8.45 ± 1.24, MRGM(−) = 5.42 ± 1.35, P<0.001) and addiction (MRGM(+) = 7.15 ± 1.80, MRGM(−) = 3.47 ± 1.98, P<0.001) ratings between RGM(+) group and RGM(-) group, and significant difference of concentration (MRGM(+) = 8.40 ± 1.20, MRM(+) = 7.00 ± 1.25, P = 0.002), enjoyment (MRM(+) = 7.06 ± 1.09, P = 0.001), and addiction (MRM(+) = 5.39 ± 1.64, P = 0.004) between RGM(+) group and RM(+) group. Mann-Whitney U tests also showed significant difference of concentration (MRGM(−) = 7.84 ± 1.14, P = 0.049), enjoyment (MRGM(−) = 5.42 ± 1.35, P = 0.001), and addiction (MRGM(−) = 3.47 ± 1.98, P = 0.006) between RGM (-) group and RM (+) group.
Previous studies rarely measured the vividness/emotionality ratings and intrusive memories at the same time (19, 28), and visuospatial game play was generally with sound-off (53). As far as we know, the present study was the first to show that the game-matching background music can have an add-on effect for single tapping game with no sound in reducing the emotionality of previous aversive memories. However, we did not find a positive effect in reducing the number of intrusions or the vividness of aversive memories by playing the visuospatial music tapping game CMN applied at 3 days after CPR.
Implementing dual tasks can reduce the vividness and emotionality of aversive memories, such as eye movement desensitization and reprocessing (EMDR) therapy (54–56), drawing complex figures (57), and mental arithmetic (27). The underlying mechanism is assumed to be the working memory (WM) theory. According to this theory, the aversive memory can be affected upon recalling when one is doing another task, which taxes one's limited working memory capacity (58). Playing Tetris game has also been suggested to involve both storage and processing resources within visuospatial WM (14), and there were also studies showing that playing Tetris could reduce the vividness and emotionality of aversive memories (59) or cravings (60).
Music therapy has been suggested as a viable and effective treatment for improving PTSD symptoms (61), and it was effective in reducing the physiological signs of agitation and anxiety (62–69). It was suggested that music can help individuals improve their ability to both express and regulate emotions (70), and help evoke vivid autobiographical memories (71). In the military population, active music making such as drumming was considered most beneficial (70). Although the music therapy lacks a standard protocol, there were studies indicating a general rule to consider is preferred music lasting 20–30 uninterrupted minutes, at least twice daily, in a comfortable position and environment (72, 73). When the music is simple, familiar to the patient, and contains 60–80 beats per minute, it is most effective (62).
In our study, we did not use dual tasks paradigm but intervened after a short retrieval of aversive memories. The game scores were not significantly different between group RGM (+) and group RGM (-), which suggests that the background music exerted no additional cognitive taxing on players. Thus, it is unlikely that the effect of RGM (+) group in reducing emotionality attributed to the working memory taxed by background music. The background music did not seem to meet the standard of music therapy, since it is relatively fragmented (about 10 pieces), short (totaling 15 min) and applied only once. In our study, no effect in reducing emotionality was found for background music only [group RM (+)] or game play only [group RGM (-)]. So, it is also unlikely that the effect of gameplay plus background music in the group RGM (+) is due to the simple summation effect of two methods. As expected, the RGM (+) group had the highest ratings in concentration, enjoyment and addiction among the groups. These accorded with the feature of the so-called flow experience (74), which seemed to be the underlying mechanism for the add-on effect of background music. Our results showed a reduction of emotionality but not vividness in the group RGM (+), which is different from methods such as EMDR which can lower both emotionality and vividness. We assumed two possibilities for this discrepant effect of the gameplay plus background music. One is due to the different mechanism of reconsolidation and dual tasks, and the other is that the emotional aspect of aversive memories is easier to be influenced than declarative aspect (75).
As for visuospatial games, although it has been repeatedly reported that playing Tetris game can reduce the number of intrusions in experimental conditions (19, 31, 49, 53, 76, 77), real-world traumas (20, 21, 75, 78), and PTSD patients (22), and in either the consolidation (1920, 31, 73) or the reconsolidation time window (22, 49, 53, 77), there were some studies finding null results with Tetris game (30) or visuospatial tasks either quite similar to (28) or different from (28, 29) Tetris. One of the important reasons they attributed to for the null results was the possibility of less interesting and attention-grabbing of games, which is the basis of flow state.
Previous studies mostly assessed only visual intrusions or only auditory intrusions, and the intervention was also visually or auditorily focused. In our study, we assessed both visual and auditory intrusions. In the hospital settings, nurses experienced CPR have both visual and auditory intrusive memories, and some of those were combined. However, we did not find a positive effect of reducing the number of intrusive memories in any modality by CMN game. It is interesting to reveal the relationship between emotionality and intrusion number. The two were expected to be positively correlated. One explanation for our contradictory results is that the number of intrusions decreased rapidly in all groups, and the ceiling effect prevents us from finding a positive results. The second explanation is that the emotionality may be more susceptible than intrusions by the intervention of playing visuospatial games. As listed above that some previous studies also showed negative results for reducing intrusions, on the contrary, studies showing negative results for reducing emotionality are rare. In the study by Holmes et al. (19), results showed that playing Tetris game did not reduce emotionality immediately after intervention compared with no tasks. Similarly, in another study by Asselbergs et al. (28), results also revealed no significant difference between playing visuospatial games and no tasks at 7 days post-intervention. In both studies, the scholars used trauma film as an experimental analog, and the mood ameliorated rapidly in all groups. So, there may be a ceiling effect: in the former study, Tetris-playing group did show better (although insignificant) mood condition after intervention than no-task group in two separate experiments (mood assessment in experiment 1: 42.3 vs. 58.1% of full scores; experiment 2: 37.8 vs. 47.6% of full scores); in the latter study, dual tasks groups (playing game whilst recalling aversive film memory) also showed better (although insignificant) emotionality scores than no task control group in two separate experiments.
It has been reported that careers can be facilitated by improving resistance to chronic stress (79). In the clinical settings, anxiety is common among both patients (80, 81) and doctors (82), and relaxing music is beneficial to surgery (82) and cardiovascular disease (81). ICU nurses are frequently exposed to traumatic events while providing care to vulnerable patient populations. Playing visuospatial game CMN may be a simple and accessible way to ameliorate the distress emotions. It may be helpful for improving nursing career satisfaction and reducing turnover rate. Furthermore, wider applications of this self-help therapy can be expected for individuals exposed other traumatic events, especially those causing massive casualties (e.g., natural disasters and wars), when psychologists are lacking.
Since our results indicate flow experience as a key boundary condition for successful intervention, future study may focus on whether the effect is game modality-specific or any kind of game can have this effect as long as the player is immersed in the playing. Additionally, it is also interesting to investigate whether playing Tetris can reduce the number of intrusive memories for these populations.
First, since reconsolidation intervention may have different effects on female and male participants (83), we only recruited female participants, which constitute the majority of nurse population. Thus, the effect of playing CMN games can not necessarily be translated to males; second, considering that this video game may not attract elder players, and elder nurses may have different mental status compared to younger ones (e.g., due to different work experience and endocrine changes), the participants in our study were relatively young, all under the age of 41. So, whether this intervention method is suitable for elder players and has similar effects needs further study. Third, since flow experience could not be evaluated by objective methods, and it's only a potential explanation of the results. We cannot rule out the possibility that other mechanisms underlie the effect. These problems are to be solved in the future.
As far as we know, the present study was the first to show that the game-matching background music can have an add-on effect for single tapping game with no sound in reducing the emotionality of previous aversive memories. We proposed that flow experience as a key boundary condition for successful reconsolidation intervention. With the advent of virtual reality (VR) technique featuring immersive experience, the combination of VR with behavioral therapies has broad prospects in the realm of psychology and deserves extensive study.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by the Ethics Committee of General Hospital of Southern Theatre Command. The patients/participants provided their written informed consent to participate in this study.
XZ, ZQ, and CJ designed the research. CJ and WC analyzed the data and wrote the manuscript. JW, KC, and YZ collected the data. LT draw the figures and critically reviewed the manuscript. XZ approved the final manuscript. All authors contributed to the article.
This work was supported by the National Natural Science Foundation of China (Grant numbers: 32200899 and 31970996) and the Science and Technology Planning Project of Guangzhou (Grant number: 202102021268).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. McHugh RK, Smits JA, Otto MW. Empirically supported treatments for panic disorder. Psychiatric Clinics North Am. (2009) 32:593–610. doi: 10.1016/j.psc.2009.05.005
2. Hofmann SG, Smits JA. Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J Clin Psychiatry. (2008) 69:621–32. doi: 10.4088/jcp.v69n0415
3. Imel ZE, Laska K, Jakupcak M, Simpson TL. Meta-analysis of dropout in treatments for posttraumatic stress disorder. J Consult Clin Psychol. (2013) 81:394–404. doi: 10.1037/a0031474
4. Craske MG, Mystkowski JL. Exposure therapy and extinction: clinical studies. In:MG Craske, D Hermans, D Vansteenwegen, , editors. Fear and Learning: From Basic Processes to Clinical Implications. Washington, DC: Am Psychiatr Assoc. (2006) p. 217–33. doi: 10.1037/11474-011
5. Bystritsky A. Treatment-resistant anxiety disorders. Mol Psychiatry. (2006) 11:805–14. doi: 10.1038/sj.mp.4001852
6. Schottenbauer MA, Glass CR, Arnkoff DB, Tendick V, Gray SH. Nonresponse dropout rates in outcome studies on PTSD: review and methodological considerations. Psychiatry. (2008) 71:134–68. doi: 10.1521/psyc.2008.71.2.134
7. Graff J, Joseph NF, Horn ME, Samiei A, Meng J, Seo J, et al. Epigenetic priming of memory updating during reconsolidation to attenuate remote fear memories. Cell. (2014) 156:261–76. doi: 10.1016/j.cell.2013.12.020
8. Robinson MJ, Franklin KB. Reconsolidation of a morphine place preference: impact of the strength and age of memory on disruption by propranolol and midazolam. Behav Brain Res. (2010) 213:201–7. doi: 10.1016/j.bbr.2010.04.056
9. Suzuki A, Josselyn SA, Frankland PW, Masushige S, Silva AJ Kida S. Memory reconsolidation and extinction have distinct temporal and biochemical signatures. J Neurosci. (2004) 24:4787–95. doi: 10.1523/JNEUROSCI.5491-03.2004
10. Lee JL. Reconsolidation: maintaining memory relevance. Trends Neurosci. (2009) 32:413–20. doi: 10.1016/j.tins.2009.05.002
11. Maples-Keller JL, Price M, Jovanovic T, Norrholm SD, Odenat L, Post L, et al. Targeting memory reconsolidation to prevent the return of fear in patients with fear of flying. Depress Anxiety. (2017) 34:610–20. doi: 10.1002/da.22626
12. Telch MJ, York J, Lancaster CL, Monfils MH. Use of a brief fear memory reactivation procedure for enhancing exposure therapy. Clin Psychol Sci. (2017) 5:367–78. doi: 10.1177/2167702617690151
13. Holmes EA, Brewin CR, Hennessy RG. Trauma films, information processing, and intrusive memory development. J Exp Psychol. (2004) 133:3–22. doi: 10.1037/0096-3445.133.1.3
14. Lau-Zhu A, Holmes EA, Butterfield S, Holmes J. Selective association between Tetris game play and visuospatial working memory: a preliminary investigation. Appl Cogn Psychol. (2017) 31:438–45. doi: 10.1002/acp.3339
15. Kupfer DJ, Regier DA. Neuroscience, clinical evidence, and the future of psychiatric classification in DSM-5. Am J Psychiatry. (2011) 168:672−4. doi: 10.1176/appi.ajp.2011.11020219
16. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Arlington: American Psychiatric Publishing. (2013). doi: 10.1176/appi.books.9780890425596
17. James EL, Lau-Zhu A, Clark IA, Visser RM, Hagenaars MA, Holmes EA. The trauma film paradigm as an experimental psychopathology model of psychological trauma: Intrusive memories and beyond. Clin Psychol Rev. (2016) 47:106–42. doi: 10.1016/j.cpr.2016.04.010
18. Holmes EA, James EL, Coode-Bate T, Deeprose C. Can playing the computer game “Tetris” reduce the build-up of flashbacks for trauma? A proposal from cognitive science. PLoS ONE. (2009) 4:e4153. doi: 10.1371/journal.pone.0004153
19. Holmes EA, James EL, Kilford EJ, Deeprose C. Key steps in developing a cognitive vaccine against traumatic flashbacks: visuospatial tetris vs. verbal Pub Quiz. PLoS ONE. (2010) 5:e13706. doi: 10.1371/journal.pone.0013706
20. Iyadurai L, Blackwell SE, Meiser-Stedman R, Watson PC, Bonsall MB, Geddes JR, et al. Preventing intrusive memories after trauma via a brief intervention involving Tetris computer game play in the emergency department: a proof-of-concept randomized controlled trial. Mol Psychiatry. (2018) 23:674–82. doi: 10.1038/mp.2017.23
21. Horsch A, Vial Y, Favrod C, Harari MM, Blackwell SE, Watson P, et al. Reducing intrusive traumatic memories after emergency caesarean section: a proof-of-principle randomized controlled study. Behav Res Ther. (2017) 94:36–47. doi: 10.1016/j.brat.2017.03.018
22. Kessler H, Holmes EA, Blackwell SE, Schmidt AC, Schweer JM, Bücker A, et al. Reducing intrusive memories of trauma using a visuospatial interference intervention with inpatients with posttraumatic stress disorder (PTSD). J Consult Clin Psychol. (2018) 86:1076–90. doi: 10.1037/ccp0000340
23. Ehlers A, Hackmann A, Michael T. Intrusive re-experiencing in post-traumatic stress disorder: phenomenology, theory, and therapy. Memory. (2004) 12:403–15. doi: 10.1080/09658210444000025
24. Speckens AE, Ehlers A, Hackmann A, Ruths FA, Clark DM. Intrusive memories and rumination in patients with posttraumatic stress disorder: a phenomenological comparison. Memory. (2007) 15:249–57. doi: 10.1080/09658210701256449
25. Baddeley AD, Andrade J. Working memory and the vividness of imagery. J Exp Psychol. (2000) 129:126–45. doi: 10.1037/0096-3445.129.1.126
26. Kavanagh DJ, Freese S, Andrade J, May J. Effects of visuospatial tasks on desensitization to emotive memories. Br J Clin Psychol. (2001) 40:267–80. doi: 10.1348/014466501163689
27. Engelhard IM, van den Hout MA, Smeets MAM. Taxing working memory reduces vividness and emotional intensity of images about the Queen's Day tragedy. J Behav Ther Exp Psychiatry. (2011) 42:32–7. doi: 10.1016/j.jbtep.2010.09.004
28. Asselbergs J, Sijbrandij M, Hoogendoorn E, Cuijpers P, Olie L, Oved K, et al. Development and testing of traumagameplay: an iterative experimental approach using the trauma film paradigm. Eur J Psychotraumatol. (2018) 9:1424447. doi: 10.1080/20008198.2018.1424447
29. Meyer T, Brewin CR, King JA, Nijmeijer D, Woud ML, Becker ES. Arresting visuospatial stimulation is insufficient to disrupt analogue traumatic intrusions. PLoS ONE. (2020) 15:e0228416. doi: 10.1371/journal.pone.0228416
30. Brennen T, Blix I, Nissen A, Holmes EA, Skumlien M, Solberg Ø. Investigating the frequency of intrusive memories after 24 h using a visuospatial interference intervention: a follow-up and extension. Eur J Psychotraumatol. (2021) 12:1953788. doi: 10.1080/20008198.2021.1953788
31. Brühl A, Heinrichs N, Bernstein EE, McNally RJ. Preventive efforts in the aftermath of analogue trauma: the effects of Tetris and exercise on intrusive images. J Behav Ther Exp Psychiatry. (2019) 64:31–5. doi: 10.1016/j.jbtep.2019.01.004
32. Harmat L, de Manzano Ö, Theorell T, Högman L, Fischer H, Ullén F. Physiological correlates of the flow experience during computer game playing. Int J Psychophysiol. (2015) 97:1–7. doi: 10.1016/j.ijpsycho.2015.05.001
33. Kemps E, Tiggemann M. Reducing the vividness and emotional impact of distressing autobiographical memories: the importance of modality-specific interference. Memory. (2007) 15:412–22. doi: 10.1080/09658210701262017
34. Matthijssen SJMA, van Schie K, van den Hout MA. The Effect of modality specific interference on working memory in recalling aversive auditory and visual memories. Cogn Emot. (2019) 33:1169–80. doi: 10.1080/02699931.2018.1547271
35. Kristjánsdóttir K, Lee CW. A comparison of visual versus auditory concurrent tasks on reducing the distress and vividness of aversive autobiographical memories. J EMDR Pract Res. (2011) 5:34–41. doi: 10.1891/1933-3196.5.2.34
36. Matthijssen SJMA, Verhoeven LCM, van den Hout MA, Heitland I. Auditory visual memories in PTSD patients targeted with eye movements and counting: the effect of modality specific loading of working memory. Front Psychol. (2017) 8:1–7. doi: 10.3389/fpsyg.2017.01937
37. Matthijssen SJMA, Heitland I, Verhoeven LCM, van den Hout MA. Reducing the emotionality of auditory hallucination memories in patients suffering from auditory hallucinations. Front Psychiatry. (2019) 10:637. doi: 10.3389/fpsyt.2019.00637
38. Luftman K, Aydelotte J, Rix K, Ali S, Houck K, Coopwood TB, et al. PTSD in those who care for the injured. Injury. (2017) 48:293–6. doi: 10.1016/j.injury.2016.11.001
39. Mealer ML, Shelton A, Berg B, Rothbaum B, Moss M. Increased prevalence of post-traumatic stress disorder symptoms in critical care nurses. Am J Respir Crit Care Med. (2007) 175:693–7. doi: 10.1164/rccm.200606-735OC
40. Mealer ML, Burnham EL, Goode CJ, Rothbaum B, Moss M. The prevalence and impact of post traumatic stress disorder and burnout syndrome in nurses. Depress Anxiety. (2009) 26:1118–26. doi: 10.1002/da.20631
41. Chang S, Huang C, Shih C, Lee C, Chang W, Chen Y, et al. Who survives cardiac arrest in the intensive care units? J Crit Care. (2009) 24:408–14. doi: 10.1016/j.jcrc.2008.10.006
42. Enohumah KO, Moerer O, Kirmse C, Bahr J, Neumann P, Quintel M. Outcome of cardiopulmonary resuscitation in intensive care units in a university hospital. Resuscitation. (2006) 71:161–70. doi: 10.1016/j.resuscitation.2006.03.013
43. Hinderer KA. Reactions to patient death: the lived experience of critical care nurses. Dimens Crit Care Nurs. (2012) 31:252–9. doi: 10.1097/DCC.0b013e318256e0f1
44. Gershengorn HB, Li G, Kramer A, Wunsch H. Survival and functional outcomes after cardiopulmonary resuscitation in the intensive care unit. J Crit Care. (2012) 27:421.e9–e17. doi: 10.1016/j.jcrc.2011.11.001
45. Pembeci K, Yildirim A, Turan E, Buget M, Camci E, Senturk M, et al. Assessment of the success of cardiopulmonary resuscitation attempts performed in a Turkish university hospital. Resuscitation. (2006) 68:221–9. doi: 10.1016/j.resuscitation.2005.07.003
46. Issak C, Paterson B. Critical care nurses' lived experience of unsuccessful resuscitation. West J Nurs Res. (1996) 18:688–702. doi: 10.1177/019394599601800606
47. McMeekin DE, Hickman RL Jr, Douglas SL, Kelley CG. Stress Coping of critical care nurses after unsuccessful cardiopulmonary resuscitation. Am J Crit Care. (2017) 26:128–35. doi: 10.4037/ajcc2017916
48. Kolehmainen C, Stahr A, Kaatz A, Brennan M, Vogelman B, Cook J, et al. Post-Code PTSD symptoms in internal medicine residents who participate in cardiopulmonary resuscitation events: a mixed methods study. J Grad Med Educ. (2015) 7:475–9. doi: 10.4300/JGME-D-14-00424.1
49. Kessler H, Schmidt A, James EL, Blackwell SE, von Rauchhaupt M, Harren K, et al. Visuospatial computer game play after memory reminder delivered three days after a traumatic film reduces the number of intrusive memories of the experimental trauma. J Behav Ther Exp Psychiatry. (2020) 67:101454. doi: 10.1016/j.jbtep.2019.01.006
50. Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corp (1996).
51. Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. Manual for State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press (1983).
52. Weiss DS, Marmer CR. The impact of event scale-revised. In:Wilson JP, Keane TM, , editors. Assessing Psychological Trauma and PTSD: A Handbook for Practitioners. New York, NY: Guilford Press (1997). p. 399–411.
53. James EL, Bonsall MB, Hoppitt L, Tunbridge EM, Geddes JR, Milton AL, et al. Computer game play reduces intrusive memories of experimental trauma via reconsolidation-update mechanisms. Psychol Sci. (2015) 26:1201–15. doi: 10.1177/0956797615583071
54. Matthijssen SJMA, Brouwers T, van Roozendaal C, Vuister T, de Jongh A. The effect of EMDR vs. EMDR 2.0 on emotionality and vividness of aversive memories in a non-clinical sample. Eur J Psychotraumatol. (2021) 12:1956793. doi: 10.1080/20008198.2021.1956793
55. Van Veen SC, Engelhard IM, van den Hout MA. The effects of eye movements on emotional memories: using an objective measure of cognitive load. Eur J Psychotraumatol. (2016) 7:30122. doi: 10.3402/ejpt.v7.30122
56. Leer A, Engelhard IM, van den Hout MA. How eye movements in EMDR work: changes in memory vividness and emotionality. J Behav Ther Exp Psychiatry. (2014) 45:396–401. doi: 10.1016/j.jbtep.2014.04.004
57. Gunter RW, Bodner GE. How eye movements affect unpleasant memories: support for a working-memory account. Behav Res Ther. (2008) 46:913–31. doi: 10.1016/j.brat.2008.04.006
58. Van den Hout MA, Engelhard IM. How does EMDR work? J Exp Psychopathol. (2012) 3:724–38. doi: 10.5127/jep.028212
59. Engelhard IM, van Uijen SL, van den Hout MA. The impact of taxing working memory on negative and positive memories. Eur J Psychotraumatol. (2010) 1. doi: 10.3402/ejpt.v1i0.5623
60. Skorka-Brown J, Andrade J, May J. Playing 'Tetris' reduces the strength, frequency and vividness of naturally occurring cravings. Appetite. (2014) 76:161–5. doi: 10.1016/j.appet.2014.01.073
61. Wellman R, Pinkerton J. The development of a music therapy protocol: a music 4 life case report of a veteran with PTSD. Music Med. (2015) 7:24. doi: 10.47513/mmd.v7i3.408
62. Chlan LL, Weinert CR, Heiderscheit A, Tracy MF, Skaar DJ, Guttormson JL, et al. Effects of patient-directed music intervention on anxiety and sedative exposure in critically ill patients receiving mechanical ventilatory support: a randomized clinical trial. JAMA. (2013) 309:2335–44. doi: 10.1001/jama.2013.5670
63. Korhan EA, Khorshid L, Uyar M. The effect of music therapy on physiological signs of anxiety in patients receiving mechanical ventilatory support. J Clin Nurs. (2011) 20:1026–34. doi: 10.1111/j.1365-2702.2010.03434.x
64. Han L, Li JP, Sit JW, Chung L, Jiao ZY, Ma WG. Effects of music intervention on physiological stress response and anxiety level of mechanically ventilated patients in China: a randomised controlled trial. J Clin Nurs. (2010) 19:978–87. doi: 10.1111/j.1365-2702.2009.02845.x
65. Hunter BC, Oliva R, Sahler OJ, Gaisser D, Salipante DM, Arezina CH. Music therapy as an adjunctive treatment in the management of stress for patients being weaned from mechanical ventilation. J Music Ther. (2010) 47:198–219. doi: 10.1093/jmt/47.3.198
66. Aghaie B, Rejeh N, Heravi-Karimooi M, Ebadi A, Moradian ST, Vaismoradi M, et al. Effect of nature-based sound therapy on agitation and anxiety in coronary artery bypass graft patients during the weaning of mechanical ventilation: a randomised clinical trial. Int J Nurs Stud. (2014) 51:526–38. doi: 10.1016/j.ijnurstu.2013.08.003
67. Saadatmand V, Rejeh N, Heravi-Karimooi M, Tadrisi SD, Zayeri F, Vaismoradi M, et al. Effect of nature-based sounds' intervention on agitation, anxiety, and stress in patients under mechanical ventilator support: a randomised controlled trial. Int J Nurs Stud. (2013) 50:895–904. doi: 10.1016/j.ijnurstu.2012.11.018
68. DeLoach D. Procedural-support music therapy in the healthcare setting: a cost-effectiveness analysis. J Pediatr Nurs. (2005) 20:276–84. doi: 10.1016/j.pedn.2005.02.016
69. Susino M, Schubert E. Musical emotions in the absence of music: a cross-cultural investigation of emotion communication in music by extra-musical cues. PLoS ONE. (2020) 15:e0241196. doi: 10.1371/journal.pone.0241196
70. Gooding LF, Langston DG. Music therapy with military populations: a scoping review. J Music Ther. (2019) 56:315–47. doi: 10.1093/jmt/thz010
71. Belfi AM, Karlan B, Tranel D. Music evokes vivid autobiographical memories. Memory. (2015) 24:979–89. doi: 10.1080/09658211.2015.1061012
72. Chlan L, Halm MA. Does music ease pain and anxiety in the critically ill? Am J Crit Care. (2013) 22:528–32. doi: 10.4037/ajcc2013998
73. Tracy MF, Chlan L. Nonpharmacological interventions to manage common symptoms in patients receiving mechanical ventilation. Crit Care Nurse. (2011) 31:19–28. doi: 10.4037/ccn2011653
74. Csikszentmihalyi M, Nakamura J. Effortless attention in everyday life: A systematic phenomenology. In:Bruya B, , editors. Effortless Attention: A New Perspective in the Cognitive Science of Attention and Action. Massachusetts: The MIT Press. (2010) p. 179–190. doi: 10.7551/mitpress/9780262013840.003.0009
75. Kanstrup M, Singh L, Göransson KE, Widoff J, Taylor RS, Gamble B, et al. Reducing intrusive memories after trauma via a brief cognitive task intervention in the hospital emergency department: an exploratory pilot randomised controlled trial. Transl Psychiatry. (2021) 11:30. doi: 10.1038/s41398-020-01124-6
76. Lau-Zhu A, Henson RN, Holmes EA. Intrusive memories and voluntary memory of a trauma film: differential effects of a cognitive interference task after encoding. J Exp Psychol Gen. (2019) 148:2154–80. doi: 10.1037/xge0000598
77. Hagenaars MA, Holmes EA, Klaassen F, Elzinga Tetris B. Word games lead to fewer intrusive memories when applied several days after analogue trauma. Eur J Psychotraumatol. (2017) 8:1386959. doi: 10.1080/20008198.2017.1386959
78. Kanstrup M, Kontio E, Geranmayeh A, Olofsdotter Lauri K, Moulds ML, Holmes EA. A single case series using visuospatial task interference to reduce the number of visual intrusive memories of trauma with refugees. Clin Psychol Psychother. (2021) 28:109–23. doi: 10.1002/cpp.2489
79. Sallen J, Hemming K, Richartz A. Facilitating dual careers by improving resistance to chronic stress: Effects of an intervention programme for elite student athletes. Eur J Sport Sci. (2018) 18:112–22. doi: 10.1080/17461391.2017.1407363
80. Aust H, Eberhart L, Sturm T, Schuster M, Nestoriuc Y, Brehm F, et al. A cross-sectional study on preoperative anxiety in adults. J Psychosom Res. (2018) 111:133–9. doi: 10.1016/j.jpsychores.2018.05.012
81. Montinari MR, Giardina S, Minelli P, Minelli S. History of music therapy and its contemporary applications in cardiovascular diseases. South Med J. (2018) 111:98–102. doi: 10.14423/SMJ.0000000000000765
82. Alam M, Roongpisuthipong W, Kim NA, Goyal A, Swary JH, Brindise RT, et al. Utility of recorded guided imagery and relaxing music in reducing patient pain and anxiety, surgeon anxiety. during cutaneous surgical procedures: A single-blinded randomized controlled trial. J Am Acad Dermatol. (2016) 75:585–9. doi: 10.1016/j.jaad.2016.02.1143
Keywords: cardiopulmonary resuscitation, intrusive memories, visuospatial game, reconsolidation intervention, flow experience
Citation: Jiang C, Chen W, Tao L, Wang J, Cheng K, Zhang Y, Qi Z and Zheng X (2023) Game-matching background music has an add-on effect for reducing emotionality of traumatic memories during reconsolidation intervention. Front. Psychiatry 14:1090290. doi: 10.3389/fpsyt.2023.1090290
Received: 05 November 2022; Accepted: 30 January 2023;
Published: 15 February 2023.
Edited by:
Laura Fusar-Poli, University of Catania, ItalyReviewed by:
Vsevolod Konstantinov, Penza State University, RussiaCopyright © 2023 Jiang, Chen, Tao, Wang, Cheng, Zhang, Qi and Zheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xifu Zheng,  emhlbmd4aWZ1QG0uc2NudS5lZHUuY24=; Zijuan Qi, cXpqdWFuMTAyNkAxNjMuY29t
emhlbmd4aWZ1QG0uc2NudS5lZHUuY24=; Zijuan Qi, cXpqdWFuMTAyNkAxNjMuY29t
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.