
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 30 March 2023
Sec. Mood Disorders
Volume 14 - 2023 | https://doi.org/10.3389/fpsyt.2023.1077940
This article is part of the Research Topic Psychometrics in Psychiatry 2022: Mood Disorders View all 8 articles
 Natalia Karina Bartosik1
Natalia Karina Bartosik1 Rafał Frankowski1
Rafał Frankowski1 Mateusz Kobierecki1
Mateusz Kobierecki1 Kacper Deska1Aleksander Twarowski1Bartłomiej Bąk2Marcin Kosmalski2*Tadeusz Pietras2
Kacper Deska1Aleksander Twarowski1Bartłomiej Bąk2Marcin Kosmalski2*Tadeusz Pietras2Background: Compared to their peers, medical students are more exposed to stress, and many present symptoms of depression, making them a group prone to experiencing mental illnesses.
Objective: This study investigates a potential link between the occurrence of symptoms of depression and the dominating type of affective temperament in young people studying at a medical university.
Methods: One hundred thirty-four medical students were surveyed using two validated questionnaires; the Polish versions of Beck’s Depression Inventory-II (BDI-II) and the Temperament Evaluation of the Memphis, Pisa, and San Diego Autoquestionnaire (TEMPS-A).
Results: The data analysis revealed a significant link between symptoms of depression and affective temperaments, most significantly in subjects with an anxious temperament.
Conclusion: This study confirms the role of various affective temperaments as a risk factor for mood disorders, specifically depression.
Depression is a chronic (1) disorder affecting many people worldwide (2). Women are more susceptible to depression, suffering from this illness about twice as often as men (3). Age also affects the frequency of depression; the onset of the disease is most common in the second and third decades of life. This age range coincides with the studied subjects’ ages (3). In 2016 a 28% prevalence of depression in medical students was reported (4), alongside worse psychosocial well-being compared to undergraduate students in the normative sample (5). In a Mokros study assessing the prevalence of depression among medical students, 10% of participants obtained a clinically significant score of 17 or higher on the BDI (6). It is speculated that many medical students experience mental strain, which could predispose them to depression (7). Furthermore, a low number of medical students seek professional help due to the stigmatization associated with mental health disorders (8).
Early diagnosis and treatment of depression are imperative to protecting the individual’s quality of life and society’s functioning (9). The etiology of depression is multifactorial, including both environmental and genetic factors. A link has been found between the affective temperament (AT) type and the prevalence of depression (10). Affective temperaments are hypothesized to be a product of hereditary factors, hence the range of temperaments in different sexes and regions of the world (11). Interestingly, carriers of the s allele of the serotonin transporter gene score significantly higher in the TEMPS questionnaire, except in the hyperthymic temperament (12). It is widely accepted that the temperament of an individual forms in youth and remains fixed after that (13). Temperament may be a hereditary trait that makes individuals sensitized to negative stimuli throughout life (14). Research around affective temperaments presents an opportunity to screen people in risk groups for mood disorders (15); for example, certain temperament traits could indicate a predisposition or even subclinical depression (16). Potentially, temperaments may lay the foundation for affective disorders or constitute their subclinical form (17, 18). It is suggested that the habits and behaviors of an individual are the product of their temperament and environmental factors (19).
Akiskal split affective temperaments into five groups: depressive, hyperthymic, cyclothymic, irritable, and anxious. These increased the risk of affective disorders, including depression (17). On the other hand, there is speculation that a hyperthymic temperament can provide resistance to depression (20). The prognosis and course of depression could also be affected by one’s temperament (15, 21). A correlation exists between the type of temperament and the severity of one’s depressive symptoms (14). In conclusion, it is vital to investigate the relationship between the type of affective temperament and the rate of mood disorders/emotional problems in young people. Medical students are of particular interest due to their chronic stress exposure. This study aims to assess the link between affective temperaments and the prevalence of depression in a population of medical students. A study with more participants is needed before broader screening, and early intervention in depression can be introduced.
The participants recruited were students at the Medical University of Łódź, Poland. Participation in the study was voluntary; all students gave written, informed consent and did not receive compensation for their participation. The project obtained approval from the Ethics Committee at the Medical University of Łódź number RNN/260/21/KE.
Inclusion criteria were as follows: student status at the university; over 18. years of age; written and informed consent.
All participants provided primary socio-demographic data such as age, gender, year of study, and field of study. The severity of depressive symptoms was assessed using the BDI-II (22), a validated questionnaire with 21 items, each rated on a scale of 0–3 by the participant. According to a discriminant analysis concerning the Polish adaptation of Beck’s questionnaire, obtaining 0–16 points corresponds to no symptoms; 17–26 to moderate depression; 28–63 to severe depression (23); these ranges were used in the study.
The Polish version of the Temperament Scale of Memphis, Pisa, Paris, and San Diego-Autoquestionnaire (TEMPS-A) (24), translated by the Adult Psychiatry Clinic, Medical University of Poznań, was used. The translation was reviewed and accepted by Akiskal. It was used to assess affective temperaments, including depressive, cyclothymic, hyperthymic, irritable, and anxious, and contains 109 items for men and 110 for women (25).
The data were collected from December 2021 to May 2022. An anonymous questionnaire was distributed to students after class by undergraduate researchers. Volunteers were invited to complete the study. Initial questions concerned the participants’ demographic traits, such as age; gender; field of study, and year of study. Participants then completed the BDI-II (22) and TEMPS-A (26). After collecting a sufficient number of correctly filled-out questionnaires, the data were analyzed.
Scores from the BDI-II (22) and TEMPS-A (26) were used. Results were analyzed statistically using Statistica 13 software. Data was tested to assess completion of all individual statistical tests assumptions. The statistical method used was Chi-squared test to assess whether gender affects the prevalence of depression and whether medical students have a different prevalence of depression than other courses. The BDI-II score over 16 was marked as depressive symptoms and the lower score as absence of depressive symptomatology. Due to low levels of students with depressive symptomatology, Yates’s correction for continuity was used. Moreover, the two-tailed Mann–Whitney U test was also used in order to assess whether gender affects BDI-II score and whether medical students obtain a different BDI-II score than other courses. The value of p was set at <0.05. Spearman’s rank correlation test was used to identify the correlation between the levels of certain temperaments and BDI-II score. The correlation coefficient is denoted by ‘r.’
Among 136 questionnaires, two were excluded due to a lack of written consent or incomplete responses. One hundred thirty-four questionnaires were subject to statistical analysis. In the sample: 82 participants (61.2%) were medical students, 25 (18.7%) physiotherapy students, and 27 (20.1%) students of other medical sciences. More detailed information on the study group is presented in Table 1. The participants were aged between 19 and 29. The average age of the assessed students was 22.43 years (SD = 1.7). Out of 134 participants, 15 scored above 16 points on the Beck Depression Scale, indicating clinically significant symptoms of depression. Four people had major depression, which is synonymous with obtaining above 26 points on the Beck Depression Scale. The other 119 participants failed to report any symptoms of depression on the questionnaire. The study revealed the presence of a depressive temperament in 18% of students; hyperthymic in 43.3%; cyclothymic in 13.4%; irritable in 3%, and anxious in 12.6%. 9.7% of participants scored the same number of points in more than one type of affective temperament. In males, a depressive temperament was present in 13.2% of individuals; hyperthymic in 51%; cyclothymic in 11.3%; irritable in 3.8%; and anxious in 9.4%. In the female group, a depressive temperament was present in 21.0% of participants; hyperthymic in 38.3%; cyclothymic in 14.8%; irritable in 2.5%; and anxious in 14.8%. 11.3% of males and 8.6% of females had more than one affective temperament. Affective temperament and depression severity are described in Table 2. The Mann–Whitney U test revealed that gender did not significantly affect the score obtained on the BDI-II (p = 0.15). Additionally, it did not affect the prevalence of depression (p = 0.75).
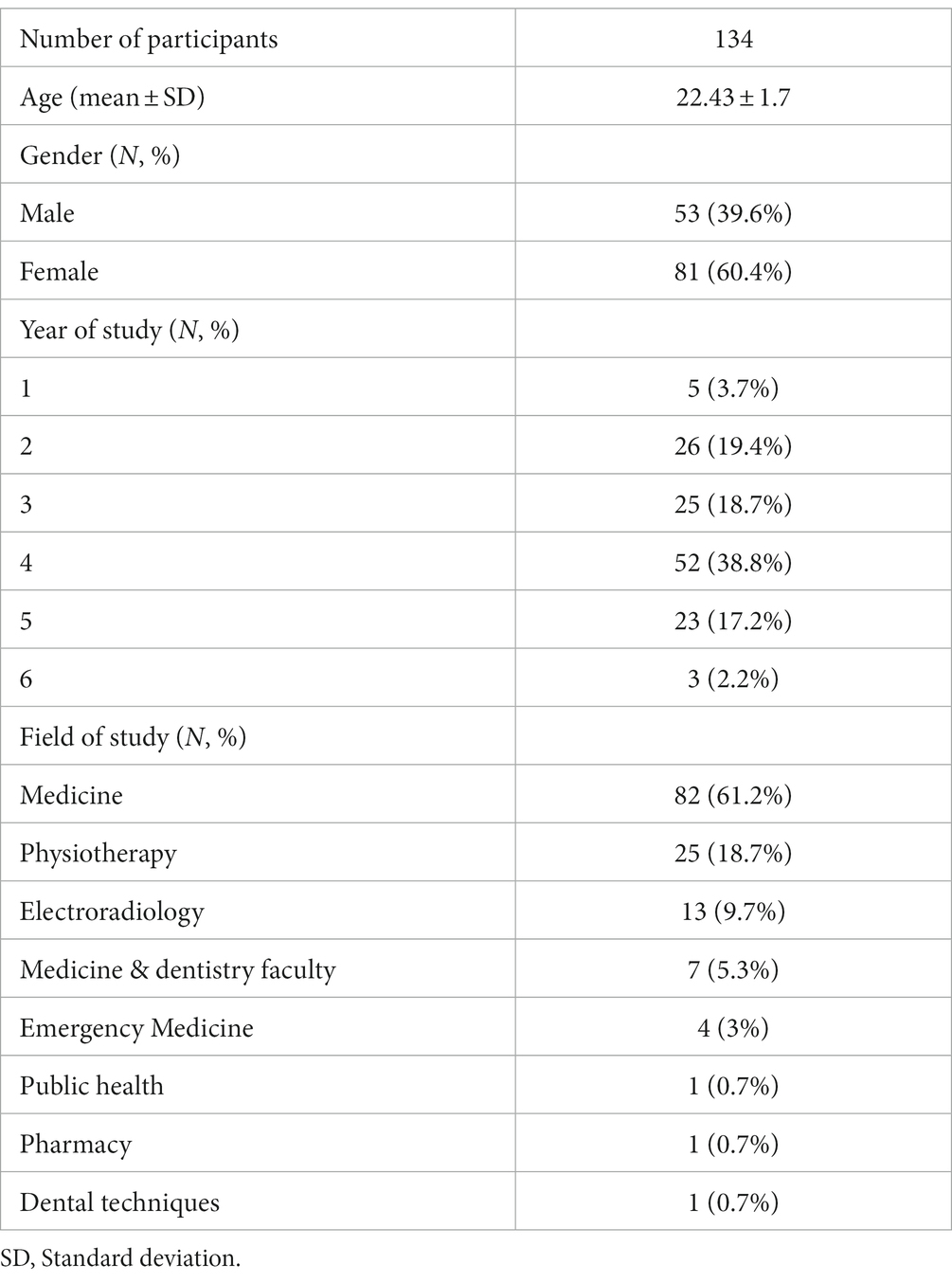
Table 1. Socio-demographic characteristics of the sample (N = 134).

Table 2. Affective temperament and depression severity.
The data showed that students from other courses scored statistically significantly higher on the BDI-II than medical students (p = 0.022). The average score obtained on the BDI-II by medical students was: 6.70, and for the other courses combined: 8.57.
The data analysis revealed a significant association between the BDI-II score (22) and particular types of affective temperament as measured by the TEMPS-A (26) within the student population of the medical university. A positive relationship between depressive symptoms with AT was revealed in a depressive temperament (r = 0.59, p < 0.001), cyclothymic temperament (r = 0.62, p < 0.001), irritable temperament (r = 0.51, p < 0.001); the most vital link was revealed with an anxious temperament (r = 0.68, p < 0.001). Depressive symptoms were weakly negatively associated with a hyperthymic temperament (r = −0.2, p = 0.02). The correlation between the levels of certain temperaments and depressive symptoms are described in Table 3.
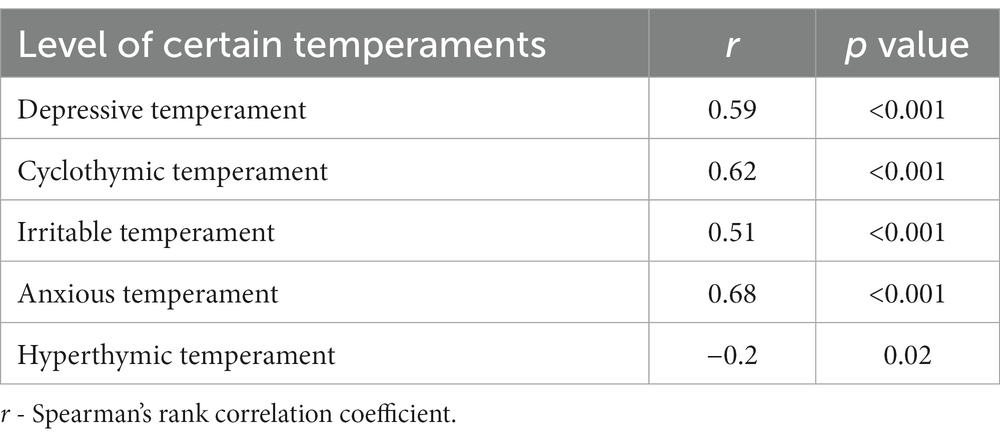
Table 3. The correlation between the levels of certain temperaments and depressive symptoms.
To the best of our knowledge, this is one of the first studies to examine the relationship between various affective temperaments and the risk of experiencing depression in a population of medical students. The study revealed a link between the BDI-II score and the type of affective temperament, with the strongest association being observed in an anxious temperament. A positive correlation between depressive symptoms and temperament type was also revealed in depressive, cyclothymic, and irritable temperaments. A weak negative correlation was observed between higher scores obtained in the BDI-II and having a hyperthymic temperament. The results obtained correspond with the Baba et al. (27) study on 314 medical students and staff from hospitals and universities, which revealed a link between depression as measured by BDI-II score and some types of affective temperaments as measured by TEMPS-A. Temperaments associated with depressive symptoms include depressive, anxious, irritable, and cyclothymic temperaments. A hyperthymic temperament hada weak negative correlation (r = −0.2) with depressive symptoms in the tested sample (27). Our result concerning the interaction between a hyperthymic temperament and the prevalence of depressive symptoms is similar to the Lazary study results (28). Based on this information, further research in this area may be worthwhile.
Medical students are admitted to university based on their personality and intellect. High entry requirements and numerous factors negatively affecting mental well-being during medical school (including high competition, very high demands, and social pressure) may negatively affect the well-being of susceptible individuals (29). Some people will develop full depression as a result of these external factors. As the research has shown - the prevalence of depression in students sometimes reaches 25.6%, a significantly higher percentage than in data from the World Health Organization (30, 31). Our results are also in line with a study conducted by Kesebir et al. (10), which revealed that people suffering from depression received higher results in TEMPS-A in terms of depressive, cyclothymic, irritable, and anxious temperaments than people who are not proven to be depressed. Moreover, the Kesebir study showed that people diagnosed with depression score lower in the TEMPS-A regarding hyperthymic temperament (10). The above data are compatible with the Shahini study, which also revealed a negative correlation between a hyperthymic temperament and depressive symptoms and a positive correlation between depression and the previously mentioned temperament types (20). According to a study conducted on subjects from the general population in Hungary, the Zung Self-Rating Depression Scale (ZSDS) score was assessed with TEMPS-A results; anxious, depressive, and cyclothymic temperaments were in substantial positive correlation with depressive scores. Restrained interaction was also observed in irritable temperaments (28).
The process of developing depressive symptoms could be inhibited by a hyperthymic temperament, acting as a safeguard against the development of many psychiatric disorders, including depression (14). A study conducted on patients with major depressive disorder (MDD) who experienced no childhood trauma and were in remission during the study revealed a strong association between psychological resilience and hyperthymic temperament (32). Interestingly, research conducted by Gonda et al. revealed that exposure to recent stress has a similar effect as individual temperaments on developing depressive symptoms (33).
In a cross-sectional study conducted on a sample of elderly, non-psychiatric patients, a hyperthymic temperament was observed more often when compared to depressive patients.
Furthermore, the most substantial connection was observed between depression and a cyclothymic temperament, and the weakest between a hyperthymic temperament and depression (34).
Our study showed that males have a hyperthymic and irritable temperament more often than females. Conversely, females score higher in cyclothymic, anxious, and depressive temperaments. Our results align with the Borkowska et al. study on 521 Polish undergraduate students, which showed a sex difference in affective temperaments measured with the TEMPS-A. A more significant proportion of males than females possess a hyperthymic temperament. On the other hand, females score higher in anxious and depressive categories. These results are in line with similar studies from other countries, e.g., Yin et al., where: in the female group, there are more individuals with depressive, anxious, and cyclothymic temperaments, and in the male group, there are more individuals with hyperthymic and irritable temperaments (11, 35).
The relatively small sample size increases the risk of selection bias and may affect the final result, therefore it may only reflect the tendencies of some medical students. Moreover, the medical students in Poland may be in a different mental state condition in comparison to students from other countries, which may not reflect the general tendency around the world. The results are also not reflective of the relationship between AT and depressive symptoms at other medical schools, as the study was only carried out at the Medical University of Łódź. The participants were students of medical sciences only, so patterns among students of other courses remain unknown. Our research was carried out from December 2021 until May 2022, which may have an impact on the results. Many mental stressors identified could have impacted the comfort and mental health of the participants at this time (7). As numerous studies have shown: the COVID-19 pandemic affects the onset of depression and anxiety in the population (30). In addition, medical students are burdened with a greater load - the stress associated with remote teaching and isolation, the prospect of working with sick patients and the fear of transmitting the virus to relatives may worsen their medical condition (31). This time also coincides with term exams and the outbreak of a war in Ukraine, a period of increased stress for students, which may impact the final results. Moreover, it is the period of the highest intensity of depressive symptoms in the course of seasonal affective disorder (36). Additionally, a significant limitation of the study was no inquiry into the current or past psychiatric treatment of the participants, which may have affected the BDI-II (22) and TEMPS-A scores (26). Additionally, the assessment of affective temperament with the TEMPS-A may have been affected by the participants’ frame of mind (37). Potentially, participants with cyclothymic or low anxious temperaments may also suffer from hypomanic or manic episodes (38). Recurrent and early onset major depressive episodes are both predictors of bipolarity (39); therefore, it is impossible to state if some participants suffer from depression or bipolar disorder. This study lacks information regarding lifetime depression or hypomania.
Our data reveal a positive correlation between every affective temperament, except hyperthermic, and the severity of depressive symptoms among students. A hyperthymic temperament may constitute protection against the onset of depressive symptoms among medical students. A study examining a larger sample size with fewer social stressors and engaging medical students also around the world is needed. Participants with prior and current psychiatric interventions should also be accounted for or excluded from future studies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The research obtained approval from the Ethics Committee of the Medical University of Lodz number RNN/260/21/KE. All students provided written informed consent to participate.
NB and RF: literature collection, literature review, and manuscript preparation. BB and KD: manuscript preparation. AT: language consultation and manuscript preparation. MK: statistical consultation and research supervision. TP: study design and research supervision. All authors contributed to the article and approved the submitted version.
This research was funded by the Medical University of Lodz, institutional grant no. 503/1-151-07/503-11-001-18.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Park, M, and Reynolds, CF. Depression among older adults with diabetes mellitus. Clin Geriatr Med. (2015) 31:117–37. doi: 10.1016/j.cger.2014.08.022
2. Kessler, RC, and Bromet, EJ. The epidemiology of depression across cultures. Annu Rev Public Health. (2013) 34:119–38. doi: 10.1146/annurev-publhealth-031912-114409
3. Malhi, GS, and Mann, JJ. Depression. Lancet. (2018) 392:2299–312. doi: 10.1016/S0140-6736(18)31948-2
4. Puthran, R, Zhang, MWB, Tam, WW, and Ho, RC. Prevalence of depression amongst medical students: a meta-analysis. Med Educ. (2016) 50:456–68. doi: 10.1111/medu.12962
5. Pacheco, JP, Giacomin, HT, Tam, WW, Ribeiro, TB, Arab, C, Bezerra, IM, et al. Mental health problems among medical students in Brazil: a systematic review and meta-analysis. Rev Bras Psiquiatr. (2017) 39:369–78. doi: 10.1590/1516-4446-2017-2223
6. Mokros, Ł, Witusik, A, Michalska, J, Łężak, W, Panek, M, Nowakowska-Domagała, K, et al. Sleep quality, chronotype, temperament and bipolar features as predictors of depressive symptoms among medical students. Chronobiol Int. (2017) 34:708–20. doi: 10.1080/07420528.2017.1316730
7. Venkatarao, E, Iqbal, S, and Gupta, S. Stress, anxiety & depression among medical undergraduate students & their socio-demographic correlates. Indian J Med Res. (2015) 141:354. doi: 10.4103/0971-5916.156571
8. Hankir, AK, Northall, A, and Zaman, R. Stigma and mental health challenges in medical students. Case Rep. (2014) 2014:bcr2014205226–6. doi: 10.1136/bcr-2014-205226
9. Toyoshima, K, Inoue, T, Masuya, J, Fujimura, Y, Higashi, S, and Kusumi, I. Affective temperaments moderate the effect of insomnia on depressive symptoms in adult community volunteers. J Affect Disord. (2021) 282:726–31. doi: 10.1016/j.jad.2020.12.138
10. Kesebir, S, Gündoğar, D, Küçüksubaşı, Y, and Tatlıdil, YE. The relation between affective temperament and resilience in depression: A controlled study. J Affect Disord. (2013) 148:352–6. doi: 10.1016/j.jad.2012.12.023
11. Borkowska, A, Rybakowski, JK, Drozdz, W, Bielinski, M, Kosmowska, M, Rajewska-Rager, A, et al. Polish validation of the TEMPS-A: the profile of affective temperaments in a college student population. J Affect Disord. (2010) 123:36–41. doi: 10.1016/j.jad.2009.09.024
12. Gonda, X, Rihmer, Z, Zsombok, T, Bagdy, G, Akiskal, KK, and Akiskal, HS. The 5HTTLPR polymorphism of the serotonin transporter gene is associated with affective temperaments as measured by TEMPS-A. J Affect Disord. (2006) 91:125–31. doi: 10.1016/j.jad.2005.12.048
13. Morvan, Y, Tibaoui, F, Bourdel, M-C, Lôo, H, Akiskal, KK, Akiskal, HS, et al. Confirmation of the factorial structure of temperamental autoquestionnaire TEMPS-A in non-clinical young adults and relation to current state of anxiety, depression and to schizotypal traits. J Affect Disord. (2011) 131:37–44. doi: 10.1016/j.jad.2011.01.008
14. Carvalho, AF, Hyphantis, TN, Taunay, TC, Macêdo, DS, Floros, GD, Ottoni, GL, et al. The relationship between affective temperaments, defensive styles and depressive symptoms in a large sample. J Affect Disord. (2013) 146:58–65. doi: 10.1016/j.jad.2012.08.038
15. Rihmer, Z, Akiskal, KK, Rihmer, A, and Akiskal, HS. Current research on affective temperaments. Curr Opin Psychiatry. (2010) 23:12–8. doi: 10.1097/YCO.0b013e32833299d4
16. Asik, M, Altinbas, K, Eroglu, M, Karaahmet, E, Erbag, G, Ertekin, H, et al. Evaluation of affective temperament and anxiety–depression levels of patients with polycystic ovary syndrome. J Affect Disord. (2015) 185:214–8. doi: 10.1016/j.jad.2015.06.043
17. Boldrini, T, Mancinelli, E, Erbuto, D, Lingiardi, V, Muzi, L, Pompili, M, et al. Affective temperaments and depressive symptoms: the mediating role of attachment. J Affect Disord. (2021) 293:476–83. doi: 10.1016/j.jad.2021.06.026
18. Janiri, D, Moccia, L, Conte, E, Palumbo, L, Chieffo, DPR, Fredda, G, et al. Emotional dysregulation, temperament and lifetime suicidal ideation among youths with mood disorders. JPM. (2021) 11:865. doi: 10.3390/jpm11090865
19. Preti, A, Vellante, M, Gabbrielli, M, Lai, V, Muratore, T, Pintus, E, et al. Confirmatory factor analysis and measurement invariance by gender, age and levels of psychological distress of the short TEMPS-A. J Affect Disord. (2013) 151:995–1002. doi: 10.1016/j.jad.2013.08.025
20. Shahini, M, Shala, M, Xhylani, P, Gashi, S, Borinca, I, and Erfurth, A. Challenging predictions between affective temperaments, depression and anxiety in a Kosovo student community sample. Int J Psychiatry Clin Pract. (2018) 22:282–8. doi: 10.1080/13651501.2018.1426771
21. Wakamatsu, M, Nakamura, M, Douchi, T, Kasugai, M, Kodama, S, Sano, A, et al. Predicting postpartum depression by evaluating temperament during pregnancy. J Affect Disord. (2021) 292:720–4. doi: 10.1016/j.jad.2021.05.106
22. Beck, AT, Steer, RA, Brown, GK, Łojek, E, and Stańczuk, J. BDI – II. Inwentarz Depresji Becka. Warszawa: Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego (2019).
24. Akiskal, HS, and Akiskal, KK. TEMPS: temperament evaluation of Memphis, Pisa, Paris and San Diego. J Affect Disord. (2005) 85:1–2. doi: 10.1016/j.jad.2004.12.003
25. Akiskal, KK, and Akiskal, HS. The theoretical underpinnings of affective temperaments: implications for evolutionary foundations of bipolar disorder and human nature. J Affect Disord. (2005) 85:231–9. doi: 10.1016/j.jad.2004.08.002
27. Baba, H, Kohno, K, Inoue, T, Nakai, Y, Toyomaki, A, Suzuki, T, et al. The effects of mental state on assessment of bipolar temperament. J Affect Disord. (2014) 161:1–3. doi: 10.1016/j.jad.2014.03.004
28. Lazary, J, Gonda, X, Benko, A, Gacser, M, and Bagdy, G. Association of depressive phenotype with affective family history is mediated by affective temperaments. Psychiatry Res. (2009) 168:145–52. doi: 10.1016/j.psychres.2008.05.002
29. Nguyen, M. Why medical school is depressing and what we should be doing about it. Aus Med Student J. (2011) 4.
30. Heitzman, J. Impact of COVID-19 pandemic on mental health. Psychiatr Pol. (2020) 54:187–98. doi: 10.12740/PP/120373
31. Debowska, A, Horeczy, B, Boduszek, D, and Dolinski, D. A repeated cross-sectional survey assessing university students’ stress, depression, anxiety, and suicidality in the early stages of the COVID-19 pandemic in Poland. Psychol Med. (2020) 2:1–4. doi: 10.1017/S003329172000392X
32. Gündoğar, D, Kesebir, S, Demirkan, AK, and Yaylacı, ET. Is the relationship between affective temperament and resilience different in depression cases with and without childhood trauma? Compr Psychiatry. (2014) 55:870–5. doi: 10.1016/j.comppsych.2014.01.016
33. Gonda, X, Eszlári, N, Sutori, S, Aspan, N, Rihmer, Z, Juhasz, G, et al. Nature and nurture: effects of affective temperaments on depressive symptoms are markedly modified by stress exposure. Front Psych. (2020) 11:599. doi: 10.3389/fpsyt.2020.00599
34. Mauer, S, de Siqueira, ASS, Borges, MK, Biella, MM, Voshaar, RCO, and Aprahamian, I. Relationship between affective temperament and major depressive disorder in older adults: A case-control study. J Affect Disord. (2020) 277:949–53. doi: 10.1016/j.jad.2020.09.038
35. Yin, L, Song, T-H, Wei, Y-Y, Zhang, L-G, Zhou, S-J, Yu, J-J, et al. Relationship between affective temperaments and suicide risk in patients with first-onset major depressive disorder. Front Psych. (2022) 13:893195. doi: 10.3389/fpsyt.2022.893195
36. Swiecicki, L, Scinska, A, Bzinkowska, D, Torbinski, J, Sienkiewicz-Jarosz, H, Samochowiec, J, et al. Intensity and pleasantness of sucrose taste in patients with winter depression. Nutr Neurosci. (2015) 18:186–91. doi: 10.1179/1476830514Y.0000000115
37. Miola, A, Baldessarini, RJ, Pinna, M, and Tondo, L. Relationships of affective temperament ratings to diagnosis and morbidity measures in major affective disorders. Eur Psychiatry. (2021) 64:e74. doi: 10.1192/j.eurpsy.2021.2252
38. Morishita, C, Kameyama, R, Toda, H, Masuya, J, Ichiki, M, Kusumi, I, et al. Utility of TEMPS-A in differentiation between major depressive disorder, bipolar I disorder, and bipolar II disorder. PLoS One. (2020) 15:e0232459. doi: 10.1371/journal.pone.0232459
Keywords: depressive symptoms, depression, affective temperament, medical university students, mood disorder
Citation: Bartosik NK, Frankowski R, Kobierecki M, Deska K, Twarowski A, Bąk B, Kosmalski M and Pietras T (2023) The association between affective temperaments and depressive symptoms in a population of medical university students, Poland. Front. Psychiatry. 14:1077940. doi: 10.3389/fpsyt.2023.1077940
Edited by:
Chien-Han Lai, National Yang-Ming University, TaiwanReviewed by:
Reiji Yoshimura, University of Occupational and Environmental Health Japan, JapanCopyright © 2023 Bartosik, Frankowski, Kobierecki, Deska, Twarowski, Bąk, Kosmalski and Pietras. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marcin Kosmalski, bWFyY2luLmtvc21hbHNraUB1bWVkLmxvZHoucGw=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.