 Kevin Swierkosz-Lenart1*
Kevin Swierkosz-Lenart1* Joao Flores Alves Dos Santos2
Joao Flores Alves Dos Santos2 Julien Elowe3,4
Julien Elowe3,4 Anne-Hélène Clair5Julien F. Bally6Françoise Riquier7Jocelyne Bloch7
Anne-Hélène Clair5Julien F. Bally6Françoise Riquier7Jocelyne Bloch7 Bogdan Draganski8,9Marie-Thérèse Clerc1Beatriz Pozuelo Moyano1
Bogdan Draganski8,9Marie-Thérèse Clerc1Beatriz Pozuelo Moyano1 Armin von Gunten1
Armin von Gunten1 Luc Mallet2,10,11
Luc Mallet2,10,11- 1Department of Psychiatry, Service Universitaire de Psychiatrie de l’Age Avancé (SUPAA), Centre Hospitalier Universitaire Vaudois, Prilly, Switzerland
- 2Department of Mental Health and Psychiatry, Geneva University Hospital, Geneva, Switzerland
- 3Department of Psychiatry, Lausanne University Hospital, University of Lausanne, West Sector, Prangins, Switzerland
- 4Department of Psychiatry, Lausanne University Hospital, University of Lausanne, North Sector, Yverdon-les-Bains, Switzerland
- 5Sorbonne University, UPMC Paris 06 University, INSERM, CNRS, Institut du Cerveau et de la Moelle Épinière, Paris, France
- 6Department of Clinical Neurosciences, Service of Neurology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
- 7Department of Clinical Neuroscience, Service of Neurosurgery, Lausanne University Hospital (CHUV), University of Lausanne (UNIL), Lausanne, Switzerland
- 8Laboratory for Research in Neuroimaging (LREN), Department of Clinical Neurosciences, Centre for Research in Neurosciences, Lausanne University Hospital, University of Lausanne, Lausanne, Switzerland
- 9Department of Neurology, Max Planck Institute for Human Cognitive and Brain Sciences, Leipzig, Germany
- 10Univ Paris-Est Créteil, DMU IMPACT, Département Médical-Universitaire de Psychiatrie et d’Addictologie, Hôpitaux Universitaires Henri Mondor - Albert Chenevier, Assistance Publique-Hôpitaux de Paris, Créteil, France
- 11Sorbonne Université, Institut du Cerveau - Paris Brain Institute - ICM, Inserm, CNRS, Paris, France
Even though obsessive compulsive disorder (OCD) is one of the ten most disabling diseases according to the WHO, only 30–40% of patients suffering from OCD seek specialized treatment. The currently available psychotherapeutic and pharmacological approaches, when properly applied, prove ineffective in about 10% of cases. The use of neuromodulation techniques, especially Deep Brain Stimulation, is highly promising for these clinical pictures and knowledge in this domain is constantly evolving. The aim of this paper is to provide a summary of the current knowledge about OCD treatment, while also discussing the more recent proposals for defining resistance.
1. Introduction
According to the DSM-5, Obsessive-Compulsive Disorder (OCD) is characterized by the presence of obsessions and/or compulsions. Obsessions are recurrent and persistent thoughts, urges, or images that are experienced as intrusive and unwanted, whereas compulsions are repetitive behaviors or mental acts that an individual feels driven to perform in response to an obsession or according to rules that must be applied rigidly (1).
The WHO listed OCD within the ten medical illnesses associated with greatest worldwide disability (2), its estimated prevalence in the United States is 2.3% for lifetime OCD and 1.2% for 12 months criteria (3), while the lifetime prevalence of OCD in the general population, according to a study that considered six European countries, is estimated to be in the range of 1–2% (4). Despite the major impact of this condition on quality of life, it has been reported that only a small proportion of OCD sufferers seek psychiatric treatment, ranging from 30 to 40% (5).
Patient reluctance to consult a professional, together with the fact that OCD rarely results in situations requiring compulsory hospitalization, probably accounts for psychiatrists’ lack of opportunity to recognize and treat this condition, as found in several surveys (6, 7).
These critical issues constitute a potential risk that many patients do not access adequate treatment and will be misdiagnosed as resistant when several available treatment steps have not been offered.
The aim of this paper is to provide a summary of the current knowledge about OCD treatment, while also discussing the more recent proposals for defining resistance.
2. First-line treatment
2.1. Psychotherapy
Cognitive Behavioral Therapy (CBT) with exposure and response prevention (E/RP) is one of the first-line evidence-based treatments for OCD (8, 9). Indeed, several meta-analyses have found a significant reduction of OCD symptoms after a psychotherapy including E/RP (10–13), with 42–52% of patients achieving symptom remission (12). Moreover, CBT has been found to be more efficient than serotoninergic treatment, including Selective Serotonin Reuptake Inhibitors (SSRIs), by several studies (12, 14, 15). More recently, a review indicated a number needed to treat (NNT) of three for CBT and five for SSRIs (16), with the additional benefit of fewer side effects and relapses. However, those results should be interpreted considering potential biases, such as the exclusion from the CBT trials of patients with comorbidities or the most severe cases of OCD.
Furthermore, the limit of accessibility to CBT should be considered, SSRI remaining the most cost-effective treatments (17). Indeed, financial cost, difficulty attending sessions and fear regarding anxiety-provoking exercises are the main perceived barriers to initiate and complete CBT (18). In line with those results, a systematic meta-analysis indicated that more than 15% of eligible patients refuse CBT and about 16% dropped out, with lower dropout rates in group CBT (19), Internet based CBT (20) or other psychotherapy techniques combined with E/RP, such as acceptance and commitment therapy (ACT) could partially overcome those limits.
Nevertheless, it is suggestive of the crucial importance of psychotherapy in the treatment algorithm, especially since acceptance and commitment therapy (ACT) (21) or mindfulness (22), alone or combined with E/RP, showed promising perspectives in the treatment of OCD.
2.2. Pharmacotherapy: Serotoninergic agents
Along with CBT, SSRIs are considered a first-line treatment in OCD by the American Psychiatric Association (APA) Practice Guidelines (8). There is multiple evidence regarding the connections between serotonergic disruption and OCD: a specific genetic polymorphism for the gene encoding the serotonin transporter 5-HTT (SLC6A4) has been found in significant association with OCD patients (23, 24). An increased sensitivity of 5-HT2 receptors has also been hypothesized in OCD patients, since OCD patients show a more pronounced neuroendocrine response than healthy controls to stimulation with an agent with high affinity for 5-HT2 receptors (25). These neurophysiological findings may explain the low efficacy of antidepressants with primary norepinephrine action, such as desipramine, compared with molecules with a serotonergic action profile (26). However, there is no evidence to date of an unequivocal correlation between alterations in specific serotoninergic pathways and the clinical manifestation of symptoms. As noted in a recent comprehensive review of pharmacotherapeutic strategies, considerations of serotonergic disruption are based exclusively on empirical evidence, whereas studies on specific alterations of 5HT2A receptors have produced controversial results (27).
As such, SSRI monotherapy is suggested as an option for patients with insufficient compliance for psychotherapy. Clomipramine has been accounted for a greater efficacy in several meta-analyses (28, 29), but single trials (30, 31) comparing it head-to-head with SSRIs do not support this evidence. When SSRIs are used to treat OCD, they should be regarded as anti-obsessive agents rather than antidepressants, bearing in mind that both the dosage and the latency between the start of treatment and the response are different when compared to depression. For example, SSRI are more efficacious when used at higher doses than for depression (32, 33). Also, a meta-analysis showed that the minimum time between SSRI initiation at effective dosage and its clinical impact is 10–12 weeks (32). However, this work, which reviews seventeen randomized clinical trials, introduces an element of complexity. The first statistically significant results of symptom reduction are observed after only 2 weeks of prescribing SSRIs, and the improvement follows a logarithmic curve whereby the greatest effects of treatment are observed in the early phase. Some meta-analyses even suggest longer waiting periods, showing a progressive improvement up to 28 weeks after the initiation of SSRI therapy (34–36).
However, the framework of action of serotonergic agents remains complex and not unambiguously definable in terms of both dosage and response delay. A meta-analysis focusing on the question of correlation between dosage and clinical response, conducted on nine randomized clinical trials, concluded that there was a 7–9% higher reduction in OCD symptoms in patients in the high-dose group, although all treatment groups (low-dose, medium-dose, and high-dose) showed a greater reduction in YBOCS score than placebo group (37). Although the benefit of these higher doses has been shown, it must be born in mind that the number needed to treat (NTT) of OCD patients on monotherapy with standard-dose SSRIs is five, whereas the NTT for obtaining a response by switching to a medium or high dose ranges from 13 to 15. This testifies to the limited possibility of obtaining a response in a non-responder with dose escalation (33). A further factor to be taken into account is the fact that off-label prescriptions produce a considerable lack of access for patients to adequate dose therapy. This phenomenon prolongs the duration of untreated illness (DUI), a parameter that appears to have a significant impact in terms of outcome for patients treated with SSRIs (38).
Table 1 indicates the maximum dosage for several SSRIs used as anti-obsessive agents (26), compared to the same molecules when used as antidepressant agents.
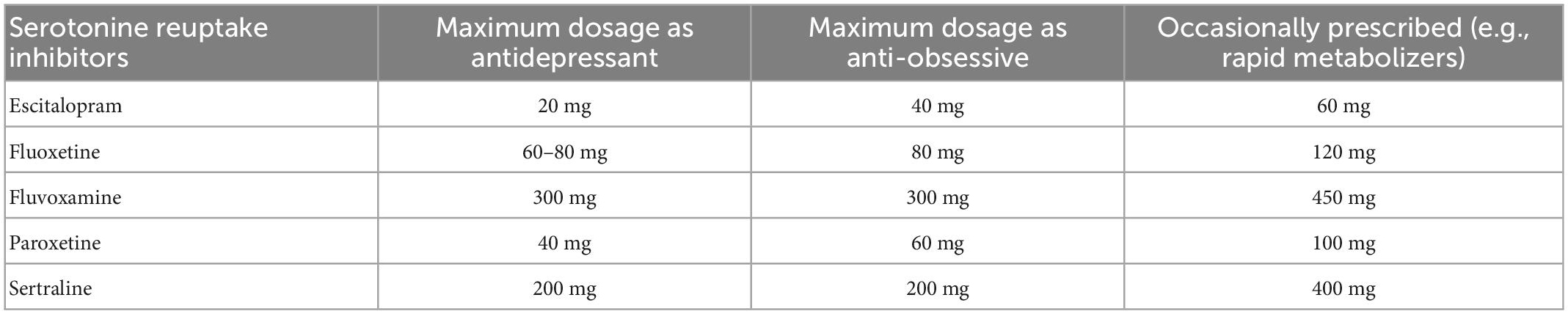
Table 1. Comparison of maximum dosage of selective serotonin re-uptake inhibitors (SSRIs) when used as antidepressants vs. anti-obsessive agents.
The use of high doses of serotonergic agents requires subsequent medical monitoring, in particular ECG monitoring (risk of QT prolongation), liver enzymes and electrolytes check at month 1, 2, 3, 6, and 12 after treatment initiation, then once a year in the absence of side effects. If necessary, drug plasma level controls and CYP450 genotyping may be useful in case of suspicion of rapid metabolizers. Particular attention must be paid when other drugs are prescribed for co-morbid conditions, to prevent serotoninergic syndrome (for instance monoamine oxidase B inhibitors).
The main psychiatric assessment tool in the follow-up of OCD therapy is the YBOCS. Data from the literature define a favorable response in terms of a reduction from the initial score of 25–35%, and there is not a generally accepted consensus in defining this threshold (39). The International Treatment Refractory OCD Consortium proposed stages for assessing the response to treatment. A reduction of 35% or greater of the YBOCS score and Clinical Global Impression (CGI) less or equal to two is considered a full response; a reduction between 25 and 35% is a partial response and a reduction inferior to 25% is a non-response (40). A retrospective study of 87 adult patients attempted to establish a correlation between the percentage reduction of YBOCS and CGI. The results show that setting a 30% or greater reduction in YBOCS has the highest efficiency of clinical predictivity, with a 91% chance of having a CGI corresponding to “improved” or “very much improved” (41).
3. Second-line treatment
Taking for granted the heterogeneity in the definition of response criteria in the literature, a recent review on pharmacotherapeutic strategies in OCD suggests that only up to 50% of patients respond to SSRIs (27). Despite research aimed at identifying the preferred molecule among SSRIs, no significant differences in terms of efficacy have been shown within this class (39, 42). Switching from one SSRI to another seems to allow an improvement of 20% in the best cases. Alternative strategies are discussed separately in the following sections.
3.1. Clomipramine
Clomipramine is a tricyclic antidepressant. Its antidepressant properties are probably due to the inhibition of neuronal re-uptake of serotonin (5-HT) and noradrenaline released into the synaptic space. Clomipramine’s pharmacological spectrum includes noradrenergic, antihistaminic and serotonergic properties. Its role in the treatment of OCD has been established since the first controlled study in 1991 (43), and its effectiveness has been confirmed several times in subsequent studies (15, 44). Despite rapidly gaining a reputation as the gold standard treatment for OCD, clomipramine showed to be non-superior to SSRIs in a recent meta-analysis including 53 articles (42). Its side-effect profile (including epilepsy, increased liver enzymes, xerostomia, increased heart rate, constipation) calls for caution when prescribing it.
Although clomipramine remains a possible second-line treatment according to the APA (8) and Canadian clinical practice guidelines (45), the most recent evidence suggests that switching from an SSRI to clomipramine is not mandatory, while preliminary data support its use as an add-on agent in cases of resistance. Further investigations in this regard remain necessary (42).
3.2. SNRIs
Venlafaxine is the most studied molecule in this class, having shown efficacy in numerous trials (45–47) at a dose of 150–375 mg/d, with a response rate of up to 60%. The interpretation of these data is limited by the heterogeneity of responder definition: 35% reduction in YBOCS (46); CGI less than or equal to two (48), CGI-I less than or equal to 2 and 25% reduction in YBOCS (48). However, the studies mentioned so far do not show a significant advantage over SSRIs. Its efficacy is probably comparable to that of clomipramine, with a side-effect profile that makes it preferable to the latter (46).
4. Add-on treatments
4.1. Antidepressant combination
Although supported by little evidence, the add-on of clomipramine in combination with SSRIs is considered by the APA Practice Guidelines (8). A 2008 trial, including 20 patients who had failed to respond to at least two trials with a SSRI and who were taking clomipramine at different doses, showed a significant response in 50% of the sample with citalopram as an add-on therapy after 1 month of treatment (49). Another work on 14 patients showed that the add-on of sertraline to clomipramine is preferable to a dose increase of clomipramine as monotherapy in case of resistance (50). A report on four cases also showed that the combination of clomipramine and fluoxetine can be effective even in cases where the individual molecules have not produced any benefit in patients (51).
4.2. Antidopaminergic agents
The role of antidopaminergic molecules in the treatment of OCD is suggested by the hypothesis of dopaminergic hyperactivation, with a disruption of the medial prefrontal cortex inhibitory circuit on the amygdala and a subsequent increased activation of anxiety (52, 53). The role of anxiety in the activation of obsessive behavior has been conceptualized from a modeling of complex tasks defined as “structured event complexes” (SECs), with respect to which the orbitofrontal cortex is implicated in reward, the anterior cingulate cortex in error detection, the basal ganglia in influencing the activation threshold of motor and behavioral programmes, while the prefrontal cortex would play the role of storing memories of these SECs. The activation of SECs could be accompanied by anxiety that is progressively alleviated by the performance of tasks, while a deficit in this process may be responsible for many OCD symptoms and have anxiety as its trigger (54). The dopamine D4 (DRD4) variable number of tandem repeats (VNTR) 7R allele polymorphism is significantly associated with OCD (55), and a worsening of obsessive symptoms has been observed in OCD patients taking dopaminergic agonist drugs (56). However, as with serotonin, the evidence is ambiguous. The link between dopaminergic dysfunction and Tourette’s syndrome, as well as for other tic disorders, is more solid, and may in part influence the conception of the pathophysiology of OCD, given the high comorbidity between these conditions.
According to the most recent trials and reviews, the most effective prescriptions are low doses of aripiprazole (1–5 mg/d) and risperidone (0.5–1 mg/d) (57–59). This evidence suggests a possible role for 5HT2A antagonism in the control of OCD symptoms. The addition of an antipsychotic to SSRIs is effective in about a third of patients, especially in the presence of tics, with a number needed to treat of about five (33, 34). A recent meta-analysis including all double-blind, randomized, placebo-controlled trials comparing augmentation of SSRIs with antipsychotics to placebo supplementation in treatment-resistant OCD revealed a clear superiority of haloperidol, aripiprazole and risperidone over placebo, while quetiapine, paliperidone and olanzapine showed no evidence of superiority. Response was defined by a reduction of at least 35% of the YBOCS score. The overall rate of attrition in the group treated with antipsychotics as add-ons ranged from 10 to 25%, attributable in part to adverse effects, the main ones reported being mouth dryness, headache, and increased appetite (36). Clozapine is not recommended, as there is sufficient evidence of its role in a possible worsening of OCD symptoms (60).
4.3. Glutamatergic agents
An increased concentration of glutamate, one of the neurotransmitters in the cortico-striato-thalamo-cortical loop, has been detected in the CSF of OCD patients (61, 62), and a specific association between OCD and polymorphisms in genes SAPAP3 and SLC1A1, which code for proteins involved in glutamatergic transmission, has been found in several studies (63–65). The clinical data reported in the following section, however, only offers evidence regarding the use of glutamatergic agents as adjunctive therapies. The etiopathogenetic role of glutamatergic disruption therefore remains to be explored, to clarify whether it is a sufficient cause or rather an added element in the determination of a polyfactorial clinical picture.
The efficacy of memantine, a NMDA receptor antagonist which regulates the effects of pathologically elevated glutamate levels, in the treatment of OCD has been studied in a randomized trial of 42 patients treated with memantine versus placebo as an add-on to fluvoxamine for 8 weeks. At the end of the study, 89% of patients on memantine met the criteria for remission, defined as YBOCS score less than or equal to 16 compared with 32% in the placebo group (66). A recent meta-analysis confirmed that patients receiving memantine were 3.61 times more likely to respond to treatment than those receiving placebo, with a response threshold set at a 35% reduction in the YBOCS score. The average reduction was of 12 points on the YBOCS compared to the scores before the add-on for the treatment group. The most common memantine-related side effects were headache, drowsiness, confusion and dizziness, usually of moderate and transient magnitude. No statistically significant differences in terms of adverse events and dropouts were reported comparing the memantine-treated group and the placebo group (67). Since a significant effect was observed in trials of memantine as add-on therapy after 12 weeks, this period is the minimum recommended for evaluating the appropriateness of this treatment strategy (68).
A recent trial compared amantadine, another glutamatergic agent, versus placebo as add-on therapy to fluvoxamine in a randomized sample of 100 patients for 12 weeks. At the end of the study, the amantadine-treated group had a significant reduction in YBOCS on the total score and on the subscale for obsessive symptoms. No significant differences were observed in the reduction of the subscale for compulsive symptoms. The two groups had no significant differences in adverse effects. The considerations made so far, in the light of this evidence, suggest a potential role for amantadine in the treatment algorithm for OCD (69).
Ketamine is a NMDA receptor antagonist as well as a non-selective agent targeting the opioid, cholinergic and monoamine systems, all of which may contribute to its efficacy in OCD (69–71). It is used in off-label clinical practice as an augmentation strategy when the better-proven approaches have failed (71–73). Most trials indicate a rapid but short-lasting effect (days to weeks), with responses varying from full remission to no benefit (74, 75).
Lamotrigine is an antiepileptic drug used in the maintenance treatment of bipolar disorder. In view of its inhibitory action on AMPA glutamatergic receptors, its possible role as an adjunctive therapy in OCD has been investigated in a few studies and case reports (75–78) all indicating that lamotrigine may be an effective and safe therapeutic option as an add-on to SSRI treatment.
Topiramate, another AMPA antagonist, showed controversial results as both improvements (79) and worsening (80) of symptoms were observed.
5. OCD resistant vs. OCD refractory
A patient meets the criteria for OCD resistant when he or she has a reduction inferior to 25% at the YBOCS despite a trial of at least 12 weeks at the highest tolerated dose of SSRIs or clomipramine, in combination with at least 30 h of CBT. Refractory OCD is defined as a non-response after 3–6 months of at least three antidepressants (including clomipramine), and at least two add-on trial with atypical antipsychotics (81). However, these operational definitions are not unequivocal in the literature, and there are those who reserve the category of refractory for those patients who show no benefit or even worsen with the proposed treatment (82). Even in cases where adequate treatment is offered to the patient, a 10% persistence of severe disability due to OCD can be observed (83). For these patients, one therapeutic option may be the addition of glutamatergic agents, according to the potential and limitations just described. As an additional criterion for the transition to interventional therapy, the use of another CBT trial with a second independent therapist is indicated as a consensual criterion. Regarding interventional psychiatry, the strongest evidence is currently available for the use of DBS, while preliminary data encourage the investigation of other alternatives.
5.1. DBS
Deep brain stimulation (DBS) is a neuromodulation technique whose application in OCD is based on a well-documented efficacy (84). A systematic review showed that, with regard to the target, there were no significant differences between the anterior limb of the internal capsule (ALIC) and the subthalamic nucleus (STN), and that up to 60% of operated patients had a reduction of at least 35% at YBOCS (85). The authors do not systematically report the inclusion criteria for all patients presented in the meta-analysis, but state that DBS is a last-line therapy. The most commonly accepted criteria for the indication of DBS in OCD patients are as follows: non-response (response being defined as at least 35% reduction in YBOCS) to two courses of SSRI treatment at the maximum dosage for at least 12 weeks; one course of clomipramine treatment at the maximum dose for at least 12 weeks; one add-on therapy with a second-generation antipsychotic for at least 8 weeks; one course of CBT, a Y-BOCS score of at least 28 points; a GAF score of less than 45 points; OCD duration of at least 5 years (79). This should be completed by the findings of a 2015 survey of 18 patients investigating the overall impact of DBS in quality of life (86). Both YBOCS responders and non-responders reported an improvement in their condition, while also reporting an improvement in their self-perception and emerging difficulties in the social sphere. These data are comparable with what has been learned about Parkinson’s patients who benefited from STN DBS (87). More recently, new targets have been proposed, such as ventral capsule/ventral striatum (VC/VS), nucleus accumbens (NAcc), anteromedial subthalamic nucleus (amSTN), or inferior thalamic peduncle (ITP) (84). The preliminary evidences of efficacy leaves open the prospect of an individual approach based on the identification of the different dimensions contributing to the heterogeneity of OCD (88). To date, the Congress of Neurological Surgeons considers the following evidence-based recommendations: the use of bilateral subthalamic nucleus DBS, combined with optimal pharmacotherapy, is recommended on a level I evidence basis. The use of bilateral nucleus accumbens or bed nucleus of stria terminalis for refractory pathology is on a type II level of evidence. These indications are the result of a systematic review conducted by the Guidelines Task Force in 2020, considering an updated literature up to 2019 (89).
Although DBS may be a viable treatment option to consider in resistant OCD, a recent Swedish survey revealed that only 29% of OCD patients are aware of its existence, that all psychotherapists surveyed estimate that their patients do not meet the criteria for an intervention, and that although psychiatrists believe 98% of the time that they have patients potentially eligible for DBS, they doubt their ability to identify them (90).
Added to this is the difficulty of insurance coverage: in the US, only 50 per cent of potential DBS recipients receive treatment, and less than 40 per cent receive coverage from their insurance company (91).
A 2022 article on the DBS access crisis identifies the lack of insurance and lack of knowledge on the part of mental health professionals as the cause of this The authors point out that this is in contrast to the mental-health parity laws enacted in 2008 (92).
A recent review, which included 40 articles and covers the last 20 years of DBS practice in OCD patients, reports the main adverse effects associated with this therapy. These can be divided into three groups: adverse effects due to surgical or hardware-related complications, stimulation-induced side effects and other types of side effects which will be listed briefly below. Electrode malpositioning or intracranial infection (which affects between 1 and 15% of Parkinson’s DBS procedures overall) are the main causes of device removal and re-implantation. Intracranial bleeding is a serious side effect that can reach rates of between 4.8 and 7.7%. Epileptic seizures, regardless of the site of stimulation, have been occasionally described in the 5 years following surgery. These have malpositioning, cranial infections, unstable somatic pathologies and abrupt changes in parameters as risk factors. The most frequent stimulation-related side effect is hypomania, although this usually resolves after adjustment of the stimulation parameters. Other adverse effects related to stimulation include weight gain, sleep disturbances, subjective memory complaints and increased anxiety. The increased risk of suicide remains controversial as this could be attributable to previous pathology or disappointment at the lack of response to the device implantation (93).
5.2. Other interventional techniques
5.2.1. rTMS
A review of 2011 (94) reports 10 studies on repetitive transcranial magnetic stimulation (rTMS) targeting dorsolateral prefrontal cortex (DLPFC), orbitofrontal cortex (OFC) and supplementary motor area (SMA), stating that it only demonstrated acute efficacy, with no significant difference with sham treatment. The most frequently reported adverse event in rTMS studies is headache, while there are anecdotal case reports on the occurrence of seizures and psychotic symptoms. In the meta-analysis under discussion, none of the side effects persisted for more than 4 weeks after the end of stimulation and no serious adverse events such as seizures and memory problems or cognitive problems occurred.
More recently, a multicenter study showed that bilateral low frequency rTMS targeting SMA significantly reduced obsessive symptoms compared to sham, with a sustained effect at 6 weeks follow-up (95). Another study showed the superiority of a 1 Hz stimulation of DLPFC over a similar 10 Hz stimulation and sham (96). Specific coils have received FDA approval for the treatment of OCD: H7 was cleared in 2018, based on evidence showing that its use in one study led to a 30% reduction in YBOCS in 38% of treated patients, compared to 11% in sham conditions (97). In 2020, the COOl D-B80 coil also received approval. According to the Clinical TMS society, the use of FDA-approved coils for OCD is recommended in case of resistance after two indicated therapies (two medications or one medication plus psychotherapy) that have been conducted for at least 8 weeks, or in case of drug intolerance after at least two trials. TMS is considered a viable alternative to relatively risky second- and third-line drug trials, such as antipsychotics, opioids, benzodiazepines and glutamatergic agents (98).
This evidence suggests that planning rTMS therapy before giving an indication for DBS is certainly desirable, considering the risks and benefits.
5.2.2. tDCS
A 2021 meta-analysis on the use of tDCS in psychiatric and neurological disorders found that a Pubmed search for the two keywords “tDCS” and “OCD” yielded a result of only eight entries. Due to the scarcity of trials, the authors exceptionally included Class IV studies in their analysis of this disorder, without excluding those involving a pediatric population (99). In this context, the authors make a recommendation of anodal pre-SMA tDCS as possibly effective in improving OCD (Level C). This is based on a class II trial (100) in which non-responders were enrolled in a subsequent open-label phase, achieving a noticeable improvement in symptom intensity despite not being able to be considered as responders. Further research is needed in this area, given these encouraging preliminary data on a technique characterized by safety and minimal invasiveness.
According to a review taking into account 567 tDCS sessions, the adverse events reported were moderate fatigue (35.3%), tingling (70.6%), slight itching at the electrode placement site (30.4%), headache (11.8%), nausea (2.9%), and insomnia (0.98%) (101). Despite its excellent safety profile, the data on the potential efficacy of tDCS in OCD do not currently justify systematically proposing this therapy in resistant or refractory cases.
6. Discussion
Less than 10% of OCD patients are currently receiving evidence-based therapy (10). The prospect of improving the offer for these patients, suffering from a highly debilitating condition lies in the adoption of common and scientifically validated practices on the one hand, and also in focusing research efforts in the directions offered by interventional psychiatry, and specifically DBS.
The scrupulous adoption of diagnostic and assessment criteria, followed by the adoption of treatment guidelines, allows reliable identification of resistant cases, which are potential beneficiaries of therapeutic approaches under research investigation. Given the impact of the disease on the patient’s quality of life, there is an increasing need to bring clinicians and researchers together to propose guidelines that integrate treatment options at the different stages of the algorithm. A graphic summary of the evidence discussed in this article is presented in Figure 1. There is a need to propose the transfer of “experimental” paradigms to the clinic, without formally demanding a high level of evidence-basis in cases of resistance, but rather focusing on sufficient data to allow clinicians to make proposals according to the clinical presentation. Clinics and research are moving together in a direction of local groups developing empirical strategies supported by a reasonable foundation. It is important for this work to continue because it is from there that solid evidence will come to produce future guidelines, capable of integrating the most recent pharmacological and technical acquisitions.
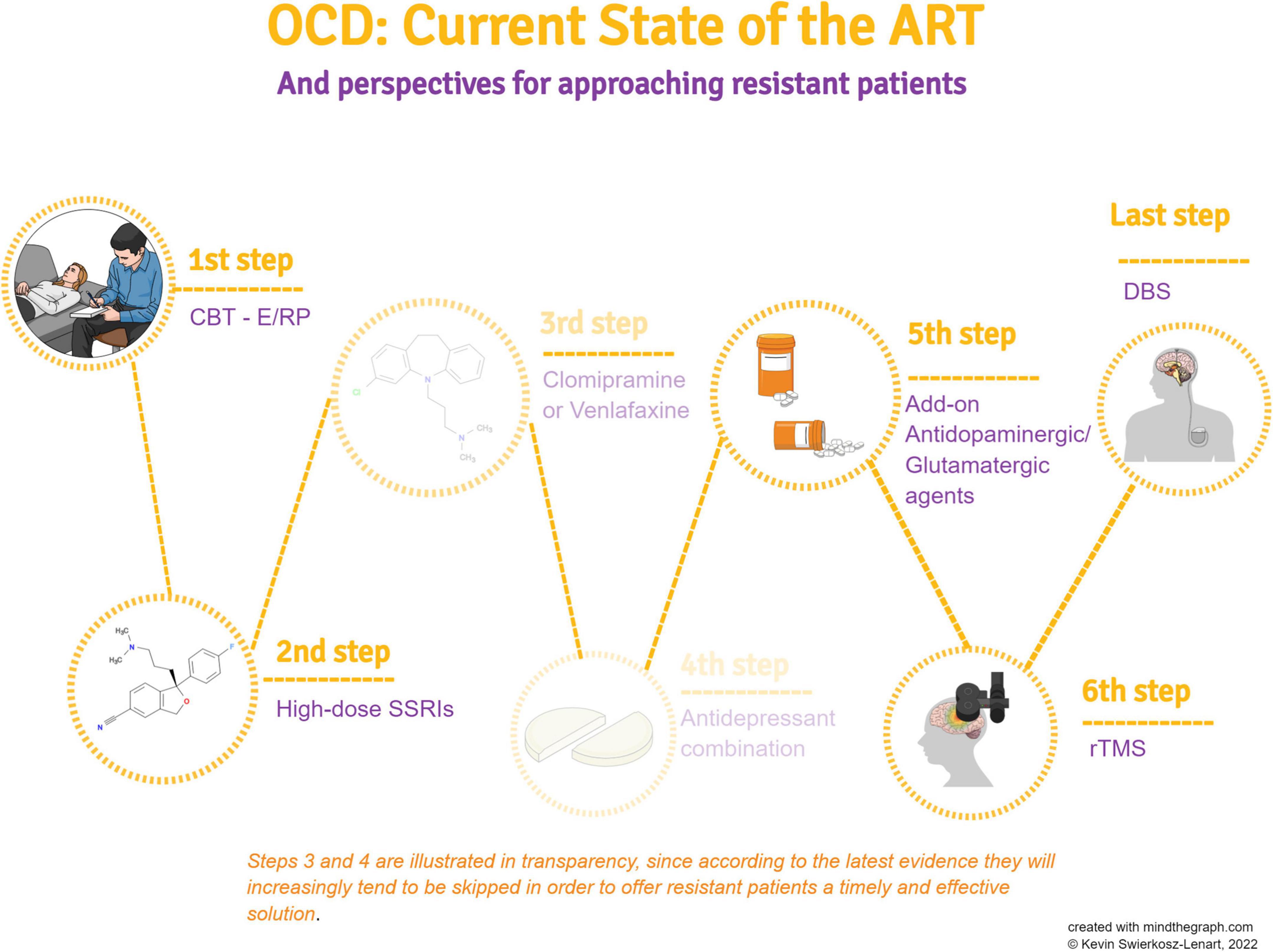
Figure 1. A schematic summary of the various treatment steps according to the best evidence in the literature.
Author contributions
JD, JE, A-HC, JB, FR, JFB, BD, M-TC, BPM, AG, and LM contributed equally, either by writing entire paragraphs in their specific field of expertise, or by providing bibliographical references, and correcting and expanding information in order to offer the reader the best state-of-the-art in the article’s field of investigation. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: American Psychiatric Association (2013).
2. Murray C, Lopez A. The global burden of diseases: a comprehensive assessment of mortality and disability from diseases, injuries and risk factors in 1990 and projected to 2020. Boston: Harvard School of Public Health (1996). 325 p.
3. Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the national comorbidity survey replication. Mol Psychiatry. (2010) 15:53–63.
4. Fullana M, Vilagut G, Rojas-Farreras S, Mataix-Cols D, de Graaf R, Demyttenaere K, et al. Obsessive-compulsive symptom dimensions in the general population: results from an epidemiological study in six European countries. J Affect Disord. (2010) 124:291–9. doi: 10.1016/j.jad.2009.11.020
5. Belloch A, Del Valle G, Morillo C, Carrió C, Cabedo E. To seek advice or not to seek advice about the problem: the help-seeking dilemma for obsessive-compulsive disorder. Soc Psychiatry Psychiatr Epidemiol. (2009) 44:257–64. doi: 10.1007/s00127-008-0423-0
6. Wahl K, Kordon A, Kuelz K, Voderholzer U, Hohagen F, Zurowski B. Obsessive-compulsive disorder (OCD) is still an unrecognised disorder: a study on the recognition of OCD in psychiatric outpatients. Eur Psychiatry. (2010) 25:374–7. doi: 10.1016/j.eurpsy.2009.12.003
7. Hantouche EG, Bouhassira M, Lancrenon S, Ravily V, Bourgeois M. Prevalence of obsessive-compulsive disorders in a large French patient population in psychiatric consultation. Encephale. (2002) 21:571–80.
8. American Psychiatric Association. Practice guideline for the treatment of patients with obsessive-compulsive disorder. Arlington, VA: American Psychiatric Association (2007).
9. Stein DJ, Costa DLC, Lochner C, Miguel EC, Reddy YCJ, Shavitt RG, et al. Obsessive-compulsive disorder. Nat Rev Dis Primers. (2019) 5:52. doi: 10.1038/s41572-019-0102-3
10. Reid J, Laws K, Drummond L, Vismara M, Grancini B, Mpavaenda D, et al. Cognitive behavioural therapy with exposure and response prevention in the treatment of obsessive-compulsive disorder: a systematic review and meta-analysis of randomised controlled trials. Compr Psychiatry. (2021) 106:152223. doi: 10.1016/j.comppsych.2021.152223
11. Olatunji B, Davis M, Powers M, Smits J. Cognitive-behavioral therapy for obsessive-compulsive disorder: a meta-analysis of treatment outcome and moderators. J Psychiatr Res. (2013) 47:33–41. doi: 10.1016/j.jpsychires.2012.08.020
12. Öst L, Havnen A, Hansen B, Kvale G. Cognitive behavioral treatments of obsessive-compulsive disorder. A systematic review and meta-analysis of studies published 1993-2014. Clin Psychol Rev. (2015) 40:156–69. doi: 10.1016/j.cpr.2015.06.003
13. Rosa-Alcázar A, Sánchez-Meca J, Gómez-Conesa A, Marín-Martínez F. Psychological treatment of obsessive-compulsive disorder: a meta-analysis. Clin Psychol Rev. (2008) 28:1310–25. doi: 10.1016/j.cpr.2008.07.001
14. Storch E, Mariaskin A, Murphy T. Psychotherapy for obsessive-compulsive disorder. Curr Psychiatry Rep. (2009) 11:296–301. doi: 10.1007/s11920-009-0043-8
15. Foa E, Liebowitz M, Kozak M, Davies S, Campeas R, Franklin M, et al. Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their combination in the treatment of obsessive-compulsive disorder. Am J Psychiatry. (2005) 162:151–61. doi: 10.1176/appi.ajp.162.1.151
17. Fineberg N, Baldwin D, Drummond L, Wyatt S, Hanson J, Gopi S, et al. Optimal treatment for obsessive compulsive disorder: a randomized controlled feasibility study of the clinical-effectiveness and cost-effectiveness of cognitive-behavioural therapy, selective serotonin reuptake inhibitors and their combination in the management of obsessive compulsive disorder. Int Clin Psychopharmacol. (2018) 33:334–48. doi: 10.1097/YIC.0000000000000237
18. Mancebo M, Eisen J, Sibrava N, Dyck I, Rasmussen S. Patient utilization of cognitive-behavioral therapy for OCD. Behav Ther. (2011) 42:399–412. doi: 10.1016/j.beth.2010.10.002
19. Leeuwerik T, Cavanagh K, Strauss C. Patient adherence to cognitive behavioural therapy for obsessive-compulsive disorder: a systematic review and meta-analysis. J Anxiety Disord. (2019) 68:102135. doi: 10.1016/j.janxdis.2019.102135
20. Andersson E, Enander J, Andrén P, Hedman E, Ljótsson B, Hursti T, et al. Internet-based cognitive behaviour therapy for obsessive-compulsive disorder: a randomized controlled trial. Psychol Med. (2012) 42:2193–203. doi: 10.1017/S0033291712000244
21. Twohig M, Abramowitz J, Smith B, Fabricant L, Jacoby R, Morrison K, et al. Adding acceptance and commitment therapy to exposure and response prevention for obsessive-compulsive disorder: a randomized controlled trial. Behav Res Ther. (2018) 108:1–9. doi: 10.1016/j.brat.2018.06.005
22. Gasnier M, Pelissolo A, Bondolfi G, Pelissolo S, Tomba M, Mallet L, et al. Les interventions basées sur la pleine conscience dans le trouble obsessionnel compulsif : mécanismes d’action et présentation d’une étude pilote [Mindfulness-based interventions in obsessive-compulsive disorder: mechanisms of action and presentation of a pilot study]. Encephale. (2017) 43:594–9. doi: 10.1016/j.encep.2016.10.004
23. Saiz P, Garcia-Portilla M, Arango C, Morales B, Bascaran M, Martinez-Barrondo S, et al. Association study between obsessive-compulsive disorder and serotonergic candidate genes. Prog Neuropsychopharmacol Biol Psychiatry. (2008) 32:765–70. doi: 10.1016/j.pnpbp.2007.12.005
24. Greenberg B, Benjamin J, Martin J, Keuler D, Huang S, Altemus M, et al. Delayed obsessive-compulsive disorder symptom exacerbation after a single dose of a serotonin antagonist in fluoxetine-treated but not untreated patients. Psychopharmacology. (1998) 140:434–44. doi: 10.1007/s002130050787
25. de Leeuw A, Westenberg H. Hypersensitivity of 5-HT2 receptors in OCD patients. An increased prolactin response after a challenge with meta-chlorophenylpiperazine and pre-treatment with ritanserin and placebo. J Psychiatr Res. (2008) 42:894–901. doi: 10.1016/j.jpsychires.2007.09.001
26. Hoehn-Saric R, Ninan P, Black D, Stahl S, Greist J, Lydiard B, et al. Multicenter double-blind comparison of sertraline and desipramine for concurrent obsessive-compulsive and major depressive disorders. Arch Gen Psychiatry. (2000) 57:76–82. doi: 10.1001/archpsyc.57.1.76
27. Pittenger C. Pharmacotherapeutic strategies and new targets in OCD. Curr Top Behav Neurosci. (2021) 49:331–84. doi: 10.1007/7854_2020_204
28. Eddy K, Dutra L, Bradley R, Westen D. A multidimensional meta-analysis of psychotherapy and pharmacotherapy for obsessive-compulsive disorder. Clin Psychol Rev. (2004) 24:1011–30. doi: 10.1016/j.cpr.2004.08.004
29. Greist J, Jefferson J, Kobak K, Katzelnick D, Serlin R. Efficacy and tolerability of serotonin transport inhibitors in obsessive-compulsive disorder. A meta-analysis. Arch Gen Psychiatry. (1995) 52:53–60. doi: 10.1001/archpsyc.1995.03950130053006
30. Mundo E, Rouillon F, Figuera M, Stigler M. Fluvoxamine in obsessive-compulsive disorder: similar efficacy but superior tolerability in comparison with clomipramine. Hum Psychopharmacol. (2001) 16:461–8. doi: 10.1002/hup.317
31. Milanfranchi A, Ravagli S, Lensi P, Marazziti D, Cassano GB. A double-blind study of fluvoxamine and clomipramine in the treatment of obsessive-compulsive disorder. Int Clin Psychopharmacol. (1997) 12:131–6. doi: 10.1097/00004850-199705000-00002
32. Issari Y, Jakubovski E, Bartley C, Pittenger C, Bloch M. Early onset of response with selective serotonin reuptake inhibitors in obsessive-compulsive disorder: a meta-analysis. J Clin Psychiatry. (2016) 77:e605–11. doi: 10.4088/JCP.14r09758
33. Pittenger C, Bloch MH. Pharmacological treatment of obsessive-compulsive disorder. Psychiatr Clin North A. (2014) 37:375–91. doi: 10.1016/j.psc.2014.05.006
34. Hirschtritt ME, Bloch MH, Mathews CA. Obsessive-compulsive disorder: advances in diagnosis and treatment. JAMA. (2017) 317:1358–67. doi: 10.1001/jama.2017.2200
35. Skapinakis P, Papatheodorou T, Mavreas V. Antipsychotic augmentation of serotonergic antidepressants in treatment-resistant obsessive-compulsive disorder: ameta-analysis of the randomized controlled trials. Eur Neuropsychopharmacol. (2007) 17:79–93.
36. Dold M, Aigner M, Lanzenberger R, Kasper S. Antipsychotic augmentation of serotonin reuptake inhibitors in treatment-resistant obsessive- compulsive disorder: an update meta-analysis of double-blind, randomized, placebo-controlled trials. Int J Neuropsychopharmacol. (2015) 18:yv047. doi: 10.1093/ijnp/pyv047
37. Bloch M, McGuire J, Landeros-Weisenberger A, Leckman J, Pittenger C. Meta-analysis of the dose-response relationship of SSRI in obsessive-compulsive disorder. Mol Psychiatry. (2010) 15:850–5. doi: 10.1038/mp.2009.50
38. Albert U, Barbaro F, Bramante S, Rosso G, De Ronchi D, Maina G. Duration of untreated illness and response to SRI treatment in obsessive-compulsive disorder. Eur Psychiatry. (2019) 58:19–26. doi: 10.1016/j.eurpsy.2019.01.017
39. Soomro G, Altman D, Rajagopal S, Oakley-Browne M. Selective serotonin re-uptake inhibitors (SSRIs) versus placebo for obsessive compulsive disorder (OCD). Cochrane Database Syst Rev. (2008) 2008:CD001765. doi: 10.1002/14651858.CD001765.pub3
40. Albert U, De Cori D, Bogetto F, Maina G. Treatment-resistant obsessive-compulsive disorder (OCD): focus on antipsychotic augmentation to SRIs. Austin J Psychiatry Behav Sci. (2014) 1:1023. doi: 10.1517/14656566.5.10.2059
41. Tolin D, Abramowitz J, Diefenbach G. Defining response in clinical trials for obsessive-compulsive disorder: a signal detection analysis of the Yale-Brown obsessive compulsive scale. J Clin Psychiatry. (2005) 66:1549–57. doi: 10.4088/jcp.v66n1209
42. Skapinakis P, Caldwell D, Hollingworth W, Bryden P, Fineberg N, Salkovskis P, et al. Pharmacological and psychotherapeutic interventions for management of obsessive-compulsive disorder in adults: a systematic review and network meta-analysis. Lancet Psychiatry. (2016) 3:730–9. doi: 10.1016/S2215-0366(16)30069-4
43. Members of The Clomipramine Collaborative Study Group. Clomipramine in the treatment of patients with obsessive-compulsive disorder. Arch Gen Psychiatry. (1991) 48:730–8. doi: 10.1001/archpsyc.1991.01810320054008
44. Fallon B, Mathew S. Biological therapies for obsessive-compulsive disorder. J Psychiatr Pract. (2000) 6:113–28. doi: 10.1097/00131746-200005000-00002
45. Katzman M, Bleau P, Blier P, Chokka P, Kjernisted K, Van Ameringen M, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders. BMC Psychiatry. (2014) 14(Suppl. 1):S1. doi: 10.1186/1471-244X-14-S1-S1
46. Albert U, Aguglia E, Maina G, Bogetto F. Venlafaxine versus clomipramine in the treatment of obsessive-compulsive disorder: a preliminary single-blind, 12-week, controlled study. J Clin Psychiatry. (2002) 63:1004–9. doi: 10.4088/jcp.v63n1108
47. Hollander E, Friedberg J, Wasserman S, Allen A, Birnbaum M, Koran L. Venlafaxine in treatment-resistant obsessive-compulsive disorder. J Clin Psychiatry. (2003) 64:546–50. doi: 10.4088/jcp.v64n0508
48. Denys D, van Megen H, van der Wee N, Westenberg H. A double-blind switch study of paroxetine and venlafaxine in obsessive-compulsive disorder. J Clin Psychiatry. (2004) 65:37–43. doi: 10.4088/jcp.v65n0106
49. Marazziti D, Golia F, Consoli G, Presta S, Pfanner C, Carlini M, et al. Effectiveness of long-term augmentation with citalopram to clomipramine in treatment-resistant OCD patients. CNS Spectr. (2008) 13:971–6. doi: 10.1017/s1092852900014024
50. Ravizza L, Barzega G, Bellino S, Bogetto F, Maina G. Therapeutic effect and safety of adjunctive risperidone in refractory obsessive-compulsive disorder (OCD). Psychopharmacol Bull. (1996) 32:677–82.
51. Browne M, Horn E, Jones T. The benefits of clomipramine-fluoxetine combination in obsessive compulsive disorder. Can J Psychiatry. (1993) 38:242–3. doi: 10.1177/070674379303800402
52. Rosenkranz J, Grace A. Cellular mechanisms of infralimbic and prelimbic prefrontal cortical inhibition and dopaminergic modulation of basolateral amygdala neurons in vivo. J Neurosci. (2002) 22:324–37. doi: 10.1523/JNEUROSCI.22-01-00324.2002
53. Denys D, Zohar J, Westenberg H. The role of dopamine in obsessive-compulsive disorder: preclinical and clinical evidence. J Clin Psychiatry. (2004) 65(Suppl. 14):11–7.
54. Huey ED, Zahn R, Krueger F, Moll J, Kapogiannis D, Wassermann E, et al. A psychological and neuroanatomical model of obsessive-compulsive disorder. J Neuropsychiatry Clin Neurosci. (2008) 20:390–408. doi: 10.1176/jnp.2008.20.4.390
55. Taj MJ, Viswanath B, Purushottam M, Kandavel T, Janardhan Reddy Y, Jain S. DRD4 gene and obsessive compulsive disorder: do symptom dimensions have specific genetic correlates? Prog Neuropsychopharmacol Biol Psychiatry. (2013) 41:18–23. doi: 10.1016/j.pnpbp.2012.10.023
56. Stein D. Obsessive-compulsive disorder. Lancet. (2002) 360:397–405. doi: 10.1016/S0140-6736(02)09620-4
57. Simpson H, Foa E, Liebowitz M, Huppert J, Cahill S, Maher M, et al. Cognitive-behavioral therapy vs risperidone for augmenting serotonin reuptake inhibitors in obsessive-compulsive disorder: a randomized clinical trial. JAMA Psychiatry. (2013) 70:1190–9. doi: 10.1001/jamapsychiatry.2013.1932
58. Veale D, Miles S, Smallcombe N, Ghezai H, Goldacre B, Hodsoll J. Atypical antipsychotic augmentation in SSRI treatment refractory obsessive-compulsive disorder: a systematic review and meta-analysis. BMC Psychiatry. (2014) 14:317. doi: 10.1186/s12888-014-0317-5
59. Albert U, Marazziti D, Di Salvo G, Solia F, Rosso G, Maina G. A systematic review of evidence-based treatment strategies for obsessive- compulsive disorder resistant to first-line pharmacotherapy. Curr Med Chem. (2018) 25:5647–61. doi: 10.2174/0929867325666171222163645
60. Grover S, Hazari N, Chakrabarti S, Avasthi A. Relationship of obsessive compulsive symptoms/disorder with clozapine: a retrospective study from a multispeciality tertiary care centre. Asian J Psychiatr. (2015) 15:56–61. doi: 10.1016/j.ajp.2015.05.002
61. Chakrabarty K, Bhattacharyya S, Christopher R, Khanna S. Glutamatergic dysfunction in OCD. Neuropsychopharmacology. (2005) 30:1735–40. doi: 10.1038/sj.npp.1300733
62. Bhattacharyya S, Khanna S, Chakrabarty K, Mahadevan A, Christopher R, Shankar S. Anti-brain autoantibodies and altered excitatory neurotransmitters in obsessive-compulsive disorder. Neuropsychopharmacology. (2009) 34:2489–96. doi: 10.1038/npp.2009.77
63. Welch J, Lu J, Rodriguiz R, Trotta N, Peca J, Ding J, et al. Cortico-striatal synaptic defects and OCD-like behaviours in Sapap3-mutant mice. Nature. (2007) 448:894–900. doi: 10.1038/nature06104
64. Samuels J, Wang Y, Riddle MA, Greenberg BD, Fyer AJ, McCracken JT, et al. Comprehensive family-based association study of the glutamate transporter gene SLC1A1 in obsessive-compulsive disorder. Am J Med Genet B Neuropsychiatr Genet. (2011) 156B:472–7. doi: 10.1002/ajmg.b.31184
65. Bozorgmehr A, Ghadirivasfi M, Shahsavand Ananloo E. Obsessive-compulsive disorder, which genes? Which functions? Which pathways? An integrated holistic view regarding OCD and its complex genetic etiology. J Neurogenet. (2017) 31:153–60. doi: 10.1080/01677063.2017.1336236
66. Ghaleiha A, Entezari N, Modabbernia A, Najand B, Askari N, Tabrizi M, et al. Memantine add-on in moderate to severe obsessive-compulsive disorder: randomized double-blind placebo-controlled study. J Psychiatr Res. (2013) 47:175–80. doi: 10.1016/j.jpsychires.2012.09.015
67. Modarresi A, Chaibakhsh S, Koulaeinejad N, Koupaei SR. A systematic review and meta-analysis: memantine augmentation in moderate to severe obsessive-compulsive disorder. Psychiatry Res. (2019) 282:112602. doi: 10.1016/j.psychres.2019.112602
68. Welter M-L, Alves Dos Santos JF, Clair A-H, Lau B, Diallo HM, Fernandez-Vidal S, et al. Deep brain stimulation of the subthalamic, accumbens, or caudate nuclei for patients with severe obsessive-compulsive disorder: a randomized crossover controlled study. Biol Psychiatry. (2020) 90:e45–7. doi: 10.1016/j.biopsych.2020.07.013
69. Naderi S, Faghih H, Aqamolaei A, Mortazavi S, Mortezaei A, Sahebolzamani E, et al. Amantadine as adjuvant therapy in the treatment of moderate to severe obsessive-compulsive disorder: a double-blind randomized trial with placebo control. Psychiatry Clin Neurosci. (2019) 73:169–74. doi: 10.1111/pcn.12803
70. Zanos P, Moaddel R, Morris P, Riggs L, Highland J, Georgiou P, et al. Ketamine and ketamine metabolite pharmacology: insights into therapeutic mechanisms. Pharmacol Rev. (2018) 70:621–60. doi: 10.1124/pr.117.015198
71. Pittenger C, Brennan B, Koran L, Mathews C, Nestadt G, Pato M, et al. Specialty knowledge and competency standards for pharmacotherapy for adult obsessive-compulsive disorder. Psychiatry Res. (2021) 300:113853. doi: 10.1016/j.psychres.2021.113853
72. Bandeira I, Lins-Silva D, Cavenaghi V, Dorea-Bandeira I, Faria-Guimarães D, Barouh J, et al. Ketamine in the treatment of obsessive-compulsive disorder: a systematic review. Harv Rev Psychiatry. (2022) 30:135–45. doi: 10.1097/HRP.0000000000000330
73. Fineberg N, Hollander E, Pallanti S, Walitza S, Grünblatt E, Dell’Osso B, et al. Clinical advances in obsessive-compulsive disorder: a position statement by the international college of obsessive-compulsive spectrum disorders. Int Clin Psychopharmacol. (2020) 35:173–93. doi: 10.1097/YIC.0000000000000314
74. Martinotti G, Chiappini S, Pettorruso M, Mosca A, Miuli A, Di Carlo F, et al. Therapeutic potentials of ketamine and esketamine in obsessive-compulsive disorder (OCD), substance use disorders (SUD) and eating disorders (ED): a review of the current literature. Brain Sci. (2021) 11:856. doi: 10.3390/brainsci11070856
75. Khalkhali M, Aram S, Zarrabi H, Kafie M, Heidarzadeh A. Lamotrigine augmentation versus placebo in serotonin reuptake inhibitors-resistant obsessive-compulsive disorder: a randomized controlled trial. Iran J Psychiatry. (2016) 11:104–14.
76. Bruno A, Mico U, Pandolfo G, Mallamace D, Abenavoli E, Di Nardo F, et al. Lamotrigine augmentation of serotonin reuptake inhibitors in treatment-resistant obsessive-compulsive disorder: a double-blind, placebo-controlled study. J Psychopharmacol. (2012) 26:1456–62.
77. Kumar T, Khanna S. Lamotrigine augmentation of serotonin re-uptake inhibitors in obsessive-compulsive disorder. Aust N Z J Psychiatry. (2000) 34:527–8. doi: 10.1080/j.1440-1614.2000.0751c.x
78. Arrojo-Romero M, Tajes Alonso M, de Leon J. Lamotrigine augmentation of serotonin reuptake inhibitors in severe and long-term treatment-resistant obsessive-compulsive disorder. Case Rep Psychiatry. (2013) 2013:612459. doi: 10.1155/2013/612459
79. Berlin H, Koran L, Jenike M, Shapira N, Chaplin W, Pallanti S, et al. Double-blind, placebo-controlled trial of topiramate augmentation in treatment-resistant obsessive-compulsive disorder. J Clin Psychiatry. (2011) 72:716–21. doi: 10.4088/JCP.09m05266gre
80. Thuile J, Even C, Guelfi J. Topiramate may induce obsessive-compulsive disorder. Psychiatry Clin Neurosci. (2006) 60:394. doi: 10.1111/j.1440-1819.2006.01520.x
81. Piccinelli M, Pini S, Bellantuono C, Wilkinson G. Effectiveness of drug treatment in OCD: a metanalytic review. B J P. (1995) 166:424–43.
82. Pallanti S, Hollander E, Bienstock C, Koran L, Leckman J, Marazziti D, et al. Treatment non-response in OCD: methodological issues and operational definitions. Int J Neuropsychopharmacol. (2002) 5:181–91. doi: 10.1017/S1461145702002900
83. Denys D. Pharmacotherapy of obsessive-compulsive disorder and obsessive-compulsive spectrum disorders. Psychiatr Clin North Am. (2006) 29:553–84. doi: 10.1016/j.psc.2006.02.013
84. Beszłej J, Wieczorek T, Kobyłko A, Piotrowski P, Siwicki D, Weiser A, et al. Deep brain stimulation: new possibilities for the treatment of mental disorders. Psychiatr Pol. (2019) 53:789–806. doi: 10.12740/PP/OnlineFirst/103090
85. Alonso P, Cuadras D, Gabriëls L, Denys D, Goodman W, Greenberg B, et al. Deep brain stimulation for obsessive-compulsive disorder: a meta-analysis of treatment outcome and predictors of response. PLoS One. (2015) 10:e0133591. doi: 10.1371/journal.pone.0133591
86. Haan S d, Rietveld E, Stokhof M, Denys D. Effects of deep brain stimulation on the lived experience of obsessive-compulsive disorder patients: in-depth interviews with 18 patients. PLoS One. (2015) 10:e0135524. doi: 10.1371/journal.pone.0135524
87. Schüpbach M, Gargiulo M, Welter ML, Mallet L, Béhar C, Houeto JL, et al. Neurosurgery in Parkinson disease: a distressed mind in a repaired body? Neurology. (2006) 66:1811–6.
88. Senova S, Clair A, Palfi S, Yelnik J, Domenech P, Mallet L. Deep brain stimulation for refractory obsessive-compulsive disorder: towards an individualized approach. Front Psychiatry. (2019) 10:905. doi: 10.3389/fpsyt.2019.00905
89. Hamani C, Pilitsis J, Rughani A, Rosenow J, Patil P, Slavin K, et al. Deep brain stimulation for obsessive-compulsive disorder. Neurosurgery. (2014) 75:327–33. doi: 10.1227/NEU.0000000000000499
90. Naesström M, Blomstedt P, Hariz M, Bodlund O. Deep brain stimulation for obsessive-compulsive disorder: knowledge and concerns among psychiatrists, psychotherapists and patients. Surg Neurol Int. (2017) 8:298. doi: 10.4103/sni.sni_19_17
91. Pinckard-Dover H, Ward H, Foote K. The decline of deep brain stimulation for obsessive-compulsive disorder following FDA humanitarian device exemption approval. Front Surg. (2021) 8:642503. doi: 10.3389/fsurg.2021.642503
92. Visser-Vandewalle V, Andrade P, Mosley P, Greenberg B, Schuurman R, McLaughlin N, et al. Deep brain stimulation for obsessive-compulsive disorder: a crisis of access. Nat Med. (2022) 28:1529–32. doi: 10.1038/s41591-022-01879-z
93. Mar-Barrutia L, Real E, Segalás C, Bertolín S, Menchón J, Alonso P. Deep brain stimulation for obsessive-compulsive disorder: a systematic review of worldwide experience after 20 years. World J Psychiatry. (2021) 11:659–80. doi: 10.5498/wjp.v11.i9.659
94. Blom R, Figee M, Vulink N, Denys D. Update on repetitive transcranial magnetic stimulation in obsessive-compulsive disorder: different targets. Curr Psychiatry Rep. (2011) 13:289–94. doi: 10.1007/s11920-011-0205-3
95. Hawken E, Dilkov D, Kaludiev E, Simek S, Zhang F, Milev R. Transcranial magnetic stimulation of the supplementary motor area in the treatment of obsessive–compulsive disorder: a multisite study. Int J Mol Sci. (2016) 17:420.
96. Elbeh K, Elserogy Y, Khalifa H, Ahmed M, Hafez M, Khedr E. Repetitive transcranial magnetic stimulation in the treatment of obsessive–compulsive disorders: double blind randomized clinical trial. Psychiatry Res. (2016) 238:264–9.
97. Carmi L, Tendler A, Bystritsky A, Hollander E, Blumberger DM, Daskalakis J, et al. Efficacy and safety of deep transcranial magnetic stimulation for obsessive compulsive disorder: a prospective multicenter randomized double-blind placebo-controlled trial. Am J Psychiatry. (2019) 176:931–8. doi: 10.1176/appi.ajp.2019.18101180
98. Clinical TMS Society. Coverage guidance for TMS for OCD. Fresno, CA: Clinical TMS Society (2021).
99. Fregni F, El-Hagrassy M, Pacheco-Barrios K, Carvalho S, Leite J, Simis M, et al. Evidence-based guidelines and secondary meta-analysis for the use of transcranial direct current stimulation in neurological and psychiatric disorders. Int J Neuropsychopharmacol. (2021) 24:256–313. doi: 10.1093/ijnp/pyaa051
100. Gowda S, Narayanaswamy J, Hazari N, Bose A, Chhabra H, Balachander S, et al. Efficacy of pre-supplementary motor area transcranial direct current stimulation for treatment resistant obsessive compulsive disorder: a randomized, double blinded, sham controlled trial. Brain Stimul. (2019) 12:922–9. doi: 10.1016/j.brs.2019.02.005
Keywords: obsessive-compulsive disorder, deep brain stimulation, neuromodulation, resistant, refractory
Citation: Swierkosz-Lenart K, Dos Santos JFA, Elowe J, Clair A-H, Bally JF, Riquier F, Bloch J, Draganski B, Clerc M-T, Pozuelo Moyano B, von Gunten A and Mallet L (2023) Therapies for obsessive-compulsive disorder: Current state of the art and perspectives for approaching treatment-resistant patients. Front. Psychiatry 14:1065812. doi: 10.3389/fpsyt.2023.1065812
Received: 10 October 2022; Accepted: 25 January 2023;
Published: 16 February 2023.
Edited by:
Stefan Borgwardt, University of Lübeck, GermanyReviewed by:
Kurt Leroy Hoffman, Autonomous University of Tlaxcala, MexicoEduardo Joaquim Lopes Alho, University of São Paulo, Brazil
Copyright © 2023 Swierkosz-Lenart, Dos Santos, Elowe, Clair, Bally, Riquier, Bloch, Draganski, Clerc, Pozuelo Moyano, von Gunten and Mallet. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kevin Swierkosz-Lenart,  a2V2aW4uc3dpZXJrb3N6LWxlbmFydEBjaHV2LmNo
a2V2aW4uc3dpZXJrb3N6LWxlbmFydEBjaHV2LmNo