 Huiling Liu1
Huiling Liu1 Meijin Ouyang
Meijin Ouyang- 1Department of Gynecology, Shunde Hospital, Southern Medical University (The First People’s Hospital of Shunde), Foshan, China
- 2Nursing Department, Shunde Hospital, Southern Medical University (The First People’s Hospital of Shunde), Foshan, China
- 3Department of Clinical Psychology, Shunde Hospital, Southern Medical University (The First People’s Hospital of Shunde), Foshan, China
Aim: This study aimed to investigate the effects of intensive psychological intervention care on adverse emotions and post-traumatic stress disorder (PTSD) symptoms in female teenage patients after induced abortion.
Methods: This prospective cohort study included 100 teenage female patients seeking induced abortion who were randomly divided into two groups: the intervention group (n = 50) and the control group (n = 50). The intervention group received intensive psychological intervention care, while the control group received standard routine nursing. The scores of the PTSD checklist for DSM-5 (PCL-5), self-rating depression (SDS), and self-rating anxiety scale (SAS) were compared between the two groups at 1 month and 3 months after the operation.
Results: The intervention group had lower risk of developing PTSD (24% vs. 44%), depression (10% vs. 32%), and anxiety (0% vs. 12%) symptoms at 1 month after the surgery. However, there were no significant differences observed between the two groups at 3 months after the surgery. Furthermore, the intervention group had significantly lower scores in PCL-5 (27.4 ± 5.4 vs. 31.8 ± 5.7; 20.5 ± 7.1 vs. 25.0 ± 7.5; p < 0.05), SDS (31.8 ± 5.4 vs. 37.8 ± 6.6; 26.8 ± 5.0 vs. 31.4 ± 7.2; p < 0.05), and SAS (32.7 ± 5.0 vs. 39.8 ± 6.9; 25.0 ± 2.7 vs. 27.5 ± 2.8; p < 0.05) at 1 month and 3 months after induced abortion.
Conclusion: These findings suggest that intensive psychological intervention care can reduce the incidence and severity of depression, anxiety, and PTSD symptoms in teenage patients who undergo induced abortion.
Clinical trial registration: https://www.chictr.org.cn/showproj.html?proj=185200, identifier ChiCTR2300067531.
Introduction
Globally, the high rates of induced abortion among young women are a significant public health concern (1). In the United States, nearly 1 million women seek induced abortion each year, with 37% of them being under the age of 25 in 2018 (2). Similarly, in China, 47.5% of women seeking induced abortion were under the age of 25 (3, 4). A study conducted in Singapore revealed that 9.1% of women seeking induced abortion were under the age of 20 (5). Compared to women over the age of 20, younger women are more likely to undergo abortion due to limited knowledge about reproduction and contraception, as well as lack of access to post-abortion care services. Induced abortion during adolescence increases the risk of adverse pregnancy outcomes in later pregnancies, such as anemia, stillbirth, premature delivery, and low birth weight infants (6). The experience of induced abortion can have long-term physical and psychosocial impacts on women, particularly for those aged 15–18, who may struggle to fully cope with the clinical and social consequences (7).
Psychological sequelae resulting from induced abortion have long been a topic of concern among researchers (8). Posttraumatic stress disorder (PTSD) or posttraumatic stress symptoms (PTSS) are highly prevalent in the general female population due to genetic susceptibility, personality factors, and ongoing mental stress (9). A cross-sectional study conducted in Sweden revealed that that the lifetime prevalence rate of PTSD in women who underwent induced abortion was 7%, with a point prevalence rate of 4%. Additionally, the prevalence rate of PTSS during the abortion procedure was found to be 23% (10). Another Swedish multi-centre cohort study discovered that the lifetime prevalence of PTSD in women who had undergone induced abortion was 7.2% at baseline, 2.9% at 3 months, and 2.3% at 6 months. It is worth noting that among females aged 15 to 19, 42.1% (24/57) experienced PTSD or PTSS during post-abortion observation, compared to 28.8% (197/684) in women over 20 years of age (11). Furthermore, a large epidemiological study demonstrated that women with PTSD had an increased risk of ectopic pregnancy, spontaneous abortion, premature delivery, and fetal overgrowth (12). Effective management of PTSD can be achieved through psychological and pharmacological interventions (13, 14). To reduce or prevent the occurrence of PTSD, it is important to provide psychological intervention to adolescent patients who have undergone induced abortion.
Multiple studies have shown that anxiety and depression are risk factors for PTSD (15). Additionally, there is evidence suggesting that anxiety and depression often coexist with PTSD in the majority of cases (16). It is clear that depression and anxiety have negative effects on women after abortion, both at an individual and social level. A longitudinal single-arm cohort study found that there is no significant difference in the incidence of depression and PTSD between postpartum and induced abortion patients. At 3 months after delivery/abortion, 6.3 and 11.1% of pregnant women experienced mild and severe depression, respectively (17). In a study comparing the mental health of women who had undergone induced abortion with who had not, it was found that the former group experienced worse outcomes in terms of anxiety, self-esteem, life satisfaction, and emotions (18).
Previous research has primarily concentrated on the occurrence and risk factors of teenage mental health issues following induced abortion, with limited exploration on prevention or treatment. Teenagers who experience post-traumatic stress disorder (PTSD) after induced abortion exhibit distinct pathophysiological characteristics compared to adults, highlighting the need for enhanced psychological interventions.
Methods
This prospective cohort study enrolled 100 female teenage patients who underwent induced abortion and were admitted to Shunde Hospital of Southern Medical University from June 2021 to September 2021. The patients were randomly divided into two groups: the control group (n = 50) and the intervention group (n = 50). Ethics approval (20201216) was obtained from the ethics committee of Shunde Hospital, Southern Medical University (The First People’s Hospital of Shunde). Written informed consent was obtained from all patients.
The study consort diagram is shown in Figure 1.
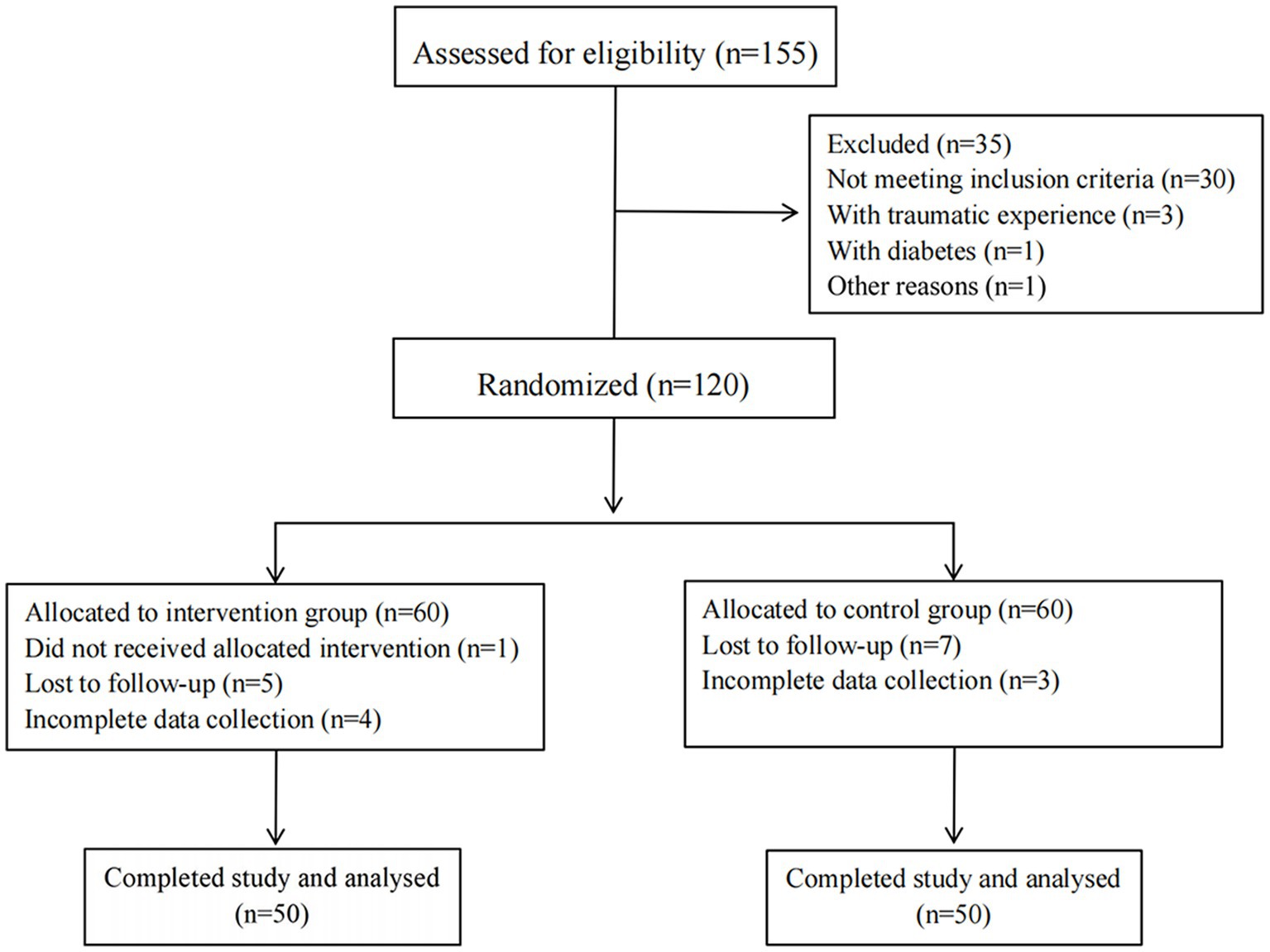
Figure 1. A CONSORT flow diagram outlining the study protocol.
Inclusion/exclusion criteria
Inclusion criteria
The study included pregnant teenagers aged 14–19 years old who came to the hospital seeking abortion and had a gestational age within 12 weeks.
Exclusion criteria
(1) Severe underlying diseases such as diabetes, hypertension, and cancers; (2) mental health problems; (3) traumatic experiences in the past year (physical or sexual abuse, natural disasters, accidents, etc.); and (4) inability to complete the follow-up.
Interventions
The control group patients received routine nursing care, which included medical services for complications of abortion, post-abortion family planning services (PAFPS), counseling services, community services, and comprehensive reproductive health services.
Intervention group patients received intensive psychological intervention care through phone interviews. This included one-on-one stress support treatment, which was conducted four times (once a week, starting from the first week after the abortion). The treatment incorporated various cognitive behavioral therapies such as emotional expression, normalization, psychological education, and cognitive re-evaluation. Each session lasted approximately 30 min and was conducted by the same trained nurse. Throughout the treatment, patients in the intervention group were encouraged to utilize relaxation and recovery techniques, such as relaxation music and meditation exercises.
Measurement
Psychological conditions were assessed using the PTSD Checklist for DSM-5 (PCL-5), the self-rating anxiety scale (SAS), and the self-rating depression scale (SDS) at 1 month and 3 months after the induced abortion.
For PCL-5, individuals assess the severity of 20 symptoms on a five-point scale (0 = none at all, 4 = very serious), and a reasonable cut score is 33. Symptom severity of PTSD was generally higher with a higher score (19).
The Self-rating Depression Scale (SDS) is composed of 20 items and has a cutoff value of 53 points. If the SDS score is ≤52, there are no signs of depression. A score of 53–62 indicates mild depression, 63–72 indicates moderate depression, and ≥73 indicates severe depression (20).
The SAS score is calculated based on the scores of 20 items, with each item scored between 0 and 4 points. The SAS scores are cut off at 50 points, and a higher SAS score indicating greater risk of anxiety (21, 22).
Statistical analysis
Based on previous interviews, the estimated PTSD prevalence of teenage patients seeking an induced abortion was 50%. To ensure statistical accuracy, bilateral α was set at 0.05 and power was set at 80%. Additionally, a loss of follow-up and rejection rate of 10–20% was taken into consideration. Therefore, a total of 50 participants are required for each group in the trial.
The data analysis and processing were performed using SPSS 21.0 software. For continuous variables that followed a normal distribution, mean and standard deviation (SD) were calculated, and an independent t-test was conducted. For categorical variables and continuous variables that did not follow a normal distribution, the Mann–Whitney U test or chi-square test was employed. A value of p of 0.05 was considered statistically significant.
Results
Demographic information of the participants
Intervention and control groups consisted of individuals aged between 15–20 years old. There were no significant differences in age, gestational weeks, education, and family structure between the two groups, as shown in Table 1.

Table 1. Sociodemographic characteristics of 100 teenage female with induced abortion.
Comparison of PCL-5 scores and prevalence of PTSD symptoms among two groups of teenage patients with induced abortion
The overall prevalence of PTSD symptoms among all teenage females 1 month and 3 months after induced abortion was 34% (34/100) and 19% (19/100) respectively. The intervention group had significantly fewer cases with PTSD symptoms compared to the control group (24% vs. 44%, p = 0.035), and lower PCL-5 scores at 1 month after the operation (27.4 ± 5.4 vs. 31.8 ± 5.7, p < 0.001). There were no statistically significant differences in the incidence of PTSD symptoms between the two groups at 3 months after the operation, although the intervention group had a lower incidence of PTSD symptoms (14% vs. 24%, p = 0.203). However, the intervention group had lower PCL-5 scores 3 months after the operation (20.5 ± 7.1 vs. 25.0 ± 7.5, p = 0.003) (Table 2).
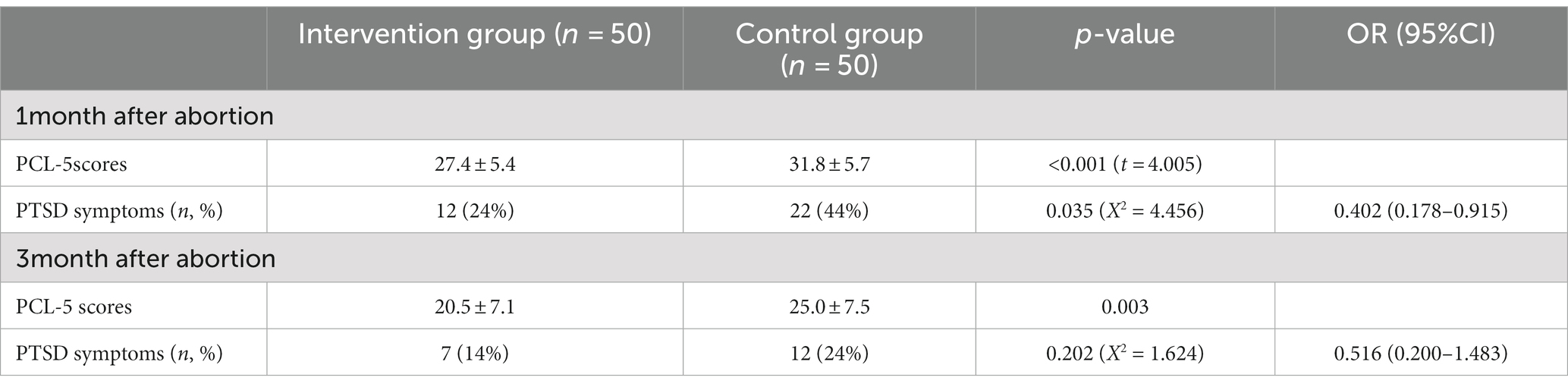
Table 2. Comparison of PCL-5 scores and prevalence of PTSD symptoms among two groups of teenage patients with induced abortion.
Comparison of SDS scores and prevalence of depression symptoms among two groups of teenage patients with induced abortion
The overall prevalence of depression symptoms was found to be 21% (21/100) at 1 month and 8% (8/100) at 3 months after the procedure. The intervention group exhibited a significantly lower prevalence of depression symptoms at 1 month after induced abortion (5% vs. 16%, p < 0.001); but no significant differences were observed at 3 months after the procedure (4% vs. 12%, p = 0.269). Furthermore, the intervention group showed significantly lower SDS scores compared to the control group at both 1 month and 3 months after induced abortion (31.8 ± 5.4 vs. 37.8 ± 6.6, 26.8 ± 5.0 vs. 31.4 ± 7.2, p < 0.05, respectively) (Table 3).
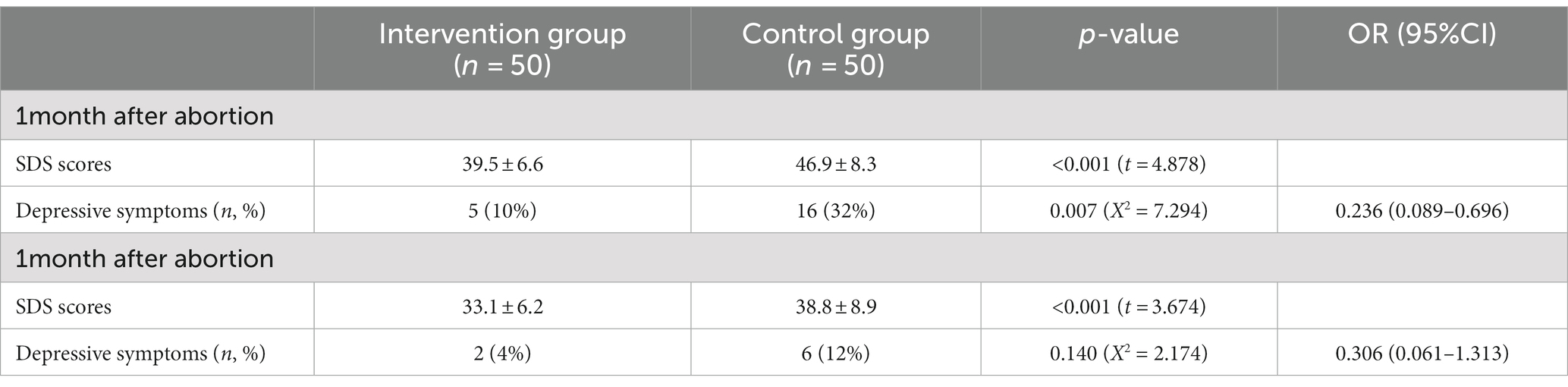
Table 3. Comparison of SDS scores and prevalence of depression symptoms among two groups of teenage patients with induced abortion.
Comparison of SAS scores and prevalence of anxiety symptoms among two groups of teenage patients with induced abortion
It was found that the anxiety characteristics in teenagers with induced abortion were not significant, with an overall anxiety prevalence rate of 6% (6/100) at 1 month and 0% (0/100) at 3 months. When comparing the incidence of anxiety between the two groups, no significant difference was observed at 1 month and 3 months after induced abortion (0% vs. 6%, p = 0.027; 0% vs. 0%, NS). However, the intervention group displayed lower SAS scores than the control group at 1 month and 3 months after abortion (32.7 ± 5.0 vs. 39.8 ± 6.9, 25.0 ± 2.7 vs. 27.5 ± 2.8, p < 0.05, respectively) (Table 4).
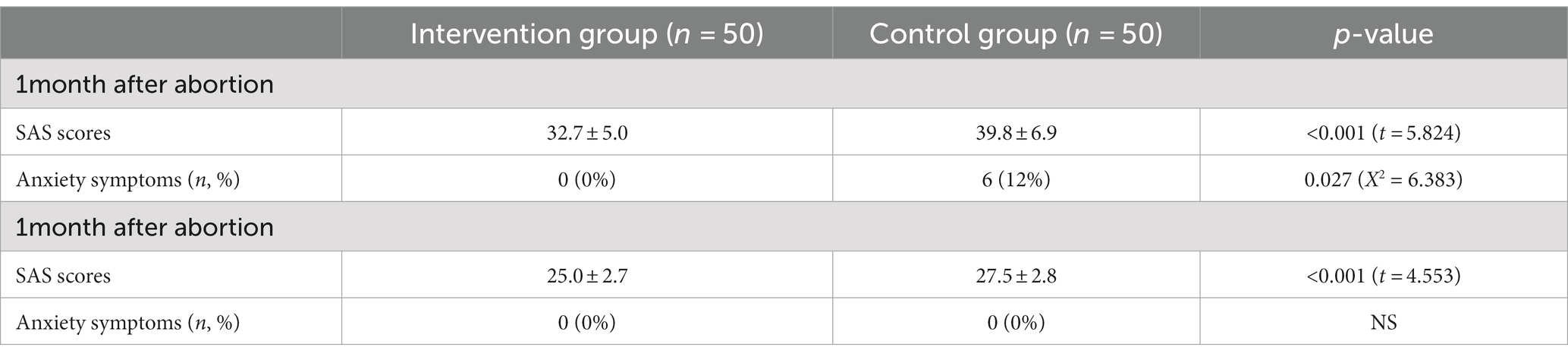
Table 4. Comparison of SAS scores and prevalence of anxiety symptoms among two groups of teenage patients with induced abortion.
Discussion
Patients who undergo abortions may experience emotional distress, although research indicates that the abortion procedure itself typically does not lead to mental health issues. However, factors such as personal susceptibility and societal prejudice can contribute to negative emotions among these individuals. Consequently, many patients may experience intense negative emotions following an abortion, thereby increasing the likelihood of developing mental illness. Offering psychological guidance to patients can help alleviate their psychological burden and eliminate negative emotions. The aim of this study was to investigate the impact of intensive post-abortion care (PAC) psychological nursing on adverse emotions and post-traumatic stress disorder in female adolescent patients who have undergone induced abortion.
The incidence of PTSD following induced abortion varies significantly across different studies. A study conducted by the University of California found that 40% of women who had undergone an abortion experienced one or more symptoms of PTSD, with 16% meeting the diagnostic, criteria for PTSD (23). Another prospective study revealed that 32.5% of women exhibited symptoms of PTSD within 7 days after having an induced abortion (24). Furthermore, research on the lifetime prevalence of PTSD among different age groups indicated that the highest rates of PTSD were observed in women aged 15–24 years (25). Additionally, the risk of PTSD in adolescents who had undergone induced abortion were approximately five times more likely to develop PTSD compared to those who had not. Our study found that the overall incidence of PTSD among adolescent women was 34% at 1 month and 19% at 3 months after abortion. Several factors may contribute to the disparities in PTSD incidence between China and Western countries, including cultural variations in attitudes towards induced abortion and mental health, differences in access to mental health services, and variations in socioeconomic conditions. Age, gender, educational level, and family structure have all been identified as risk factors for the development of PTSD. Our cohort exhibited several characteristics that may explain the high incidence of PTSD. It is reported that the risk of PTSS and PTSD decreased over time among teenage women who had undergone induced abortion, which was also supported by our study. Specifically, in our study, we observed that the incidence of PTSD and the severity of symptoms at 3 months were significantly lower compared to those at 1 month. It is worth noting that appropriate psychological intervention has proven to be an effective measure in reducing or even preventing the occurrence of PTSD. Furthermore, our study revealed that the incidence of PTSD and the PCL-5 score in the intervention group, both at 1 month and 3 months after induced abortion, were significantly lower than those in the control group. Collectively, these studies highlight the effectiveness and necessity of psychological interventions for women who have undergone induced abortion, as they can help mitigate the occurrence of postoperative PTSD.
Anxiety and depression are both risk factors for PTSD. In turn, individuals with PTSD often experience co-morbid symptoms of depression and anxiety (26). Among women with PTSD, a high percentage had symptoms of anxiety (90%) and depression (76%). The incidence of depression and anxiety among teenage women who underwent induced abortion in our cohort was lower than in previous studies, with rates of 1 and 8% at 1 month, respectively. However, women with PTSD/PTSS often felt that post-abortion care was inadequate. Therefore, additional support is necessary, and simple efforts such as providing adequate pain relief, support, and privacy during this period may improve their outcomes (27). Our study demonstrated that intensive psychological intervention significantly improved the psychological well-being of post-abortion adolescent women. The intervention group exhibited lower levels of depression and anxiety symptoms at 1 month and 3 months after abortion compared to the control group, and the incidence of depression at 1 month after abortion was also lower in the intervention group. Furthermore, patients in the intervention group experienced fewer negative emotions and were able to maintain a positive attitude during the recovery period.
This study has certain limitations that should be considered. Firstly, we did not assess the baseline levels of PTSD, depression, and anxiety in the two groups of patients. However, randomization helps to guarantee that the two groups are similar in terms of characteristics such as age, gender, and incidence of PTSD, depression, and anxiety. Additionally, this study did not evaluate the likelihood of women developing lifelong PTSD, depression, and anxiety without a clinical diagnosis. Lastly, the specific source of trauma experienced by females in this study could not be determined.
In summary, intensive psychological intervention care has been shown to reduce the incidence and severity of depression, anxiety, and PTSD in teenage adolescent patients who have undergone induced abortion. The implementation of these interventions can lead to significant health benefits for teenage patients, making them highly valuable for widespread clinical application.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the ethics committee of Shunde Hospital, Southern Medical University (The First People’s Hospital of Shunde). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
MO designed the manuscript and enhanced the figures and language. HL, FW, GL, and SM conducted the clinical trial. HL prepared the figure and drafted this manuscript and edited and revised manuscript. All authors contributed to the article and approved the submitted version.
Funding
The present study was funded by the Foshan Science and Technology Bureau (2020001005577).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Upadhyay, UD, Raymond, EG, Koenig, LR, Coplon, L, Gold, M, Kaneshiro, B, et al. Outcomes and safety of history-based screening for medication abortion: a retrospective multicenter cohort study. JAMA Intern Med. (2022) 182:482–91. doi: 10.1001/jamainternmed.2022.0217
2. Kortsmit, K, Jatlaoui, TC, Mandel, MG, Reeves, JA, Oduyebo, T, Petersen, E, et al. Abortion surveillance – United States, 2018. MMWR Surveill Summ. (2020) 69:1–29. doi: 10.15585/mmwr.ss6907a1
3. Luo, H, Wu, S, Wang, K, Xu, J, Tang, L, Temmerman, M, et al. Repeat induced abortion in 30 Chinese provinces: a cross-sectional study. Int J Gynaecol Obstet. (2021) 154:532–9. doi: 10.1002/ijgo.13620
4. Wang, Z, Lou, C, Jin, L, Miao, M, Tu, X, Liang, H, et al. Attitudes and practices related to intrauterine devices for nulliparous women among Chinese health care providers. Reprod Health. (2019) 16:10. doi: 10.1186/s12978-019-0678-9
5. Lim, L, Wong, H, Yong, E, and Singh, K. Profiles of women presenting for abortions in Singapore: focus on teenage abortions and late abortions. Eur J Obstet Gynecol Reprod Biol. (2012) 160:219–22. doi: 10.1016/j.ejogrb.2011.11.017
6. Phupong, V, and Suebnukarn, K. Obstetric outcomes in nulliparous young adolescents. Southeast Asian J Trop Med Public Health. (2007) 38:141–5.
7. Banerjee, B, Pandey, G, Dutt, D, Sengupta, B, Mondal, M, and Deb, S. Teenage pregnancy: a socially inflicted health hazard. Indian J Community Med. (2009) 34:227–31. doi: 10.4103/0970-0218.55289
8. Frans, O, Rimmo, PA, Aberg, L, and Fredrikson, M. Trauma exposure and post-traumatic stress disorder in the general population. Acta Psychiatr Scand. (2005) 111:291–07. doi: 10.1111/j.1600-0447.2004.00463.x
9. Steinberg, JR, and Russo, NF. Abortion and anxiety: what’s the relationship? Soc Sci Med. (2008) 67:238–52. doi: 10.1016/j.socscimed.2008.03.033
10. Wallin Lundell, I, Sundström Poromaa, I, Frans, O, Helström, L, Högberg, U, Moby, L, et al. The prevalence of posttraumatic stress among women requesting induced abortion. Eur J Contracept Reprod Health Care. (2013) 18:480–8. doi: 10.3109/13625187.2013.828030
11. Wallin Lundell, I, Georgsson Öhman, S, Frans, O, Helström, L, Högberg, U, Nyberg, S, et al. Posttraumatic stress among women after induced abortion: a Swedish multi-centre cohort study. BMC Womens Health. (2013) 13:52. doi: 10.1186/1472-6874-13-52
12. Seng, JS, Oakley, DJ, Sampselle, CM, Killion, C, Graham-Bermann, S, and Liberzon, I. Posttraumatic stress disorder and pregnancy complications. Obstet Gynecol. (2001) 97:17–22. doi: 10.1097/00006250-200101000-00004
13. Jiang, C, Li, Z, Du, C, Zhang, X, Chen, Z, Luo, G, et al. Supportive psychological therapy can effectively treat post-stroke post-traumatic stress disorder at the early stage. Front Neurosci. (2022) 16:1007571. doi: 10.3389/fnins.2022.1007571
14. Roberts, NP, Kitchiner, NJ, Kenardy, J, Robertson, L, Lewis, C, and Bisson, JI. Multiple session early psychological interventions for the prevention of post-traumatic stress disorder. Cochrane Database Syst Rev. (2019) 8:D6869. doi: 10.1002/14651858.CD006869.pub3
15. Christiansen, DM, and Elklit, A. Risk factors predict post-traumatic stress disorder differently in men and women. Ann General Psychiatry. (2008) 7:24. doi: 10.1186/1744-859X-7-24
16. The Cochrane CollaborationUllman, AJ, Aitken, LM, Rattray, J, Kenardy, J, le Brocque, R, et al. Diaries for recovery from critical illness. Cochrane Database Syst Rev. (2014) 2014:D10468. doi: 10.1002/14651858.CD010468
17. Wang, Y, Chen, L, Wu, T, Shi, H, Li, Q, Jiang, H, et al. Impact of Covid-19 in pregnancy on mother’s psychological status and infant’s neurobehavioral development: a longitudinal cohort study in China. BMC Med. (2020) 18:347. doi: 10.1186/s12916-020-01825-1
18. Jerman, J, Frohwirth, L, Kavanaugh, ML, and Blades, N. Barriers to abortion care and their consequences for patients traveling for services: qualitative findings from two states. Perspect Sex Reprod Health. (2017) 49:95–102. doi: 10.1363/psrh.12024
19. Bovin, MJ, Marx, BP, Weathers, FW, Gallagher, MW, Rodriguez, P, Schnurr, PP, et al. Psychometric properties of the PTSD checklist for diagnostic and statistical manual of mental disorders-fifth edition (PCL-5) in veterans. Psychol Assess. (2016) 28:1379–91. doi: 10.1037/pas0000254
20. Sakamoto, S, Kijima, N, Tomoda, A, and Kambara, M. Factor structures of the Zung self-rating depression scale (SDS) for undergraduates. J Clin Psychol. (1998) 54:477–87. doi: 10.1002/(SICI)1097-4679(199806)54:4<477::AID-JCLP9>3.0.CO;2-K
21. Zung, WW. A rating instrument for anxiety disorders. Psychosomatics. (1971) 12:371–9. doi: 10.1016/S0033-3182(71)71479-0
22. Gao, RC, Wu, L, Shi, PL, Sang, N, Hao, M, and Wu, GC. The impact of distress disclosure and anxiety on the association between social support and quality of life among Chinese women with systemic lupus erythematosus. Front Psych. (2022) 13:893235. doi: 10.3389/fpsyt.2022.893235
23. Biggs, MA, Rowland, B, Mcculloch, CE, and Foster, DG. Does abortion increase women’s risk for post-traumatic stress? Findings from a prospective longitudinal cohort study. BMJ Open. (2016) 6:e9698. doi: 10.1136/bmjopen-2015-009698
24. Vukelic, J, Kapamadzija, A, and Kondic, B. Investigation of risk factors for acute stress reaction following induced abortion. Med Pregl. (2010) 63:399–403. doi: 10.2298/MPNS1006399V
25. Kessler, RC, Sonnega, A, Bromet, E, Hughes, M, and Nelson, CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry. (1995) 52:1048–60. doi: 10.1001/archpsyc.1995.03950240066012
26. Asadzadeh, L, Jafari, E, Kharaghani, R, and Taremian, F. Effectiveness of midwife-led brief counseling intervention on post-traumatic stress disorder, depression, and anxiety symptoms of women experiencing a traumatic childbirth: a randomized controlled trial. BMC Pregnancy Childbirth. (2020) 20:142. doi: 10.1186/s12884-020-2826-1
Keywords: intensive psychological intervention care, induced abortion, adolescent, PTSD, anxiety, depression
Citation: Liu H, Wu F, Liao G, Mai S and Ouyang M (2023) Impact of the intensive psychological intervention care on post-traumatic stress disorder and negative emotions of teenage female patients seeking an induced abortion. Front. Psychiatry. 14:1033320. doi: 10.3389/fpsyt.2023.1033320
Edited by:
Anne-Laure Sutter-Dallay, Centre Hospitalier Charles Perrens, FranceReviewed by:
Xiaolei Xue, Xinjiang Medical University, ChinaValentina Lucia La Rosa, University of Catania, Italy
Hui Li, Taixing People’s Hospital, China
Elena Commodari, University of Catania, Italy
Copyright © 2023 Liu, Wu, Liao, Mai and Ouyang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Meijin Ouyang, NDkxMjQyNDYxQHFxLmNvbQ==