
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 09 September 2022
Sec. Perinatal Psychiatry
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.986796
 Sabrina Julien-Sweerts1*
Sabrina Julien-Sweerts1* Sandie Rousselin2Florence Raffeneau2Charlotte Xavier-David2Violette Changeur2
Sandie Rousselin2Florence Raffeneau2Charlotte Xavier-David2Violette Changeur2 Gisèle Apter3
Gisèle Apter3 Lucia Romo4,5
Lucia Romo4,5 Ludovic Gicquel2
Ludovic Gicquel2Objective: The objective was to screen for maternal postnatal depression (MPD) by administering the Edinburgh Postnatal Depression Scale (EPDS) during the first “peak” of incidence of MPD (i. e., between the 6th and the 10th week of the infant's life) and to therefore explore the relationship between mothers' EPDS scores and early clinical signs in the infant. We wanted to evaluate the relevance of a diagnostic tool that combines the EPDS with questions focused on clinical signs displayed by the infant.
Participants: Seven hundred and sixty seven mothers aged 18–46 (M = 30.5, SD = 4.9) participated in the study, representing 49.2% of all women who delivered in the study area during the research inclusion period. Main outcome measures: Sociodemographic data were collected. MPD was measured by EPDS (score ≥ 12). The presence of clinical signs in the infant was investigated by closed (i.e., yes or no) questions inquiring into whether the infant has or has had difficulty sleeping, feeding difficulties, crying difficult to calm, or other difficulties.
Results: The prevalence of MPD in our sample was 22.16%. The relationships between MPD and early clinical signs present in the infant, i.e., sleep difficulties, feeding problems, crying difficult to calm (p < 0.001), and other problems (p = 0.004), were very significant, as confirmed by a chi-square test of independence. In particular, sleep difficulties (OR = 2.05, CI 1.41–2.99) and feeding difficulties (OR = 1.59, CI 1.10–2.30) seemed to predict MPD.
Conclusions: Early clinical signs in the infant can alert the medical team to potential psychological suffering on the part of the mother, at which time the EPDS can be proposed. The use of this method has the potential to improve screening for, and therefore early management of, MPD.
The postpartum period is particularly vulnerable to decompensation and even the outbreak of psychiatric pathologies, including depression (1). Perinatal depression is defined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) as an episode of major depressive disorder (MDD) with peripartum onset, i.e., symptom onset during pregnancy or in the 4 weeks following delivery (2).
The prevalence of maternal perinatal depression (MPD) is currently considered to be 10–20% (3, 4). A recent systematic review and meta-regression suggested that the overall pooled prevalence of perinatal depression is 11.9% (95% confidence interval [CI], 11.4%−12.5%) (5). In France, it is between 5 and 20%, depending on the diagnostic criteria and measurement tools used (6).
Both biological factors (e.g., sex hormones, stress hormones, thyroid hormones) and psychosocial factors contribute to the development of postpartum depression (7). Lower socio-economic status, lower educational level, younger age, not being married, lack of support and empathy from partner, lack of social support, perceived stress, prior history of depression, current depressive symptoms, and a history of sexual or physical violence are frequently identified as potential risk factors for perinatal depression (8–11). The biopsychosocial model of MPD, as supported by several meta-analyses, attempts to comprehensively understand the risk factors for the onset of depressive symptoms as well as the protective factors associated with this disorder, with the aim of improving prevention and treatment (12–14).
In fact, MPD has major consequences for public health. In France, a recent national survey showed that suicide has become the second leading cause of postpartum maternal mortality (accounting for 13.4% of maternal deaths), behind cardiovascular diseases (13.7% of maternal deaths) (15). Untreated MPD seems to have negative consequences for both infants and mothers. A recent systematic review highlighted the adverse effects of MPD on mothers (physical health, psychological health, worse quality of life, difficulties in social relationships, and risky behaviors such as substance abuse), on mother-child interactions (attachment difficulties, insecure attachments), and on infants (anthropometry; physical health; sleep; and motor, cognitive, language, emotional, social, and behavioral development) (16). Early functional signs such as diarrhea (17, 18), constipation, colic (19), gastroesophageal reflux (20), night-time awakening, and other infant sleep troubles (21, 22) seem to be more frequent in infants with a mother suffering from MPD. Difficulty with breastfeeding has also been connected to postnatal depression (23). In general, maternal depression has been associated with excessive crying and feeding and sleeping problems in infants (24).
However, screening and diagnosis present massive difficulties. As many as half of the mothers suffering from maternal postnatal depression would not be spotted by their close circle (her family, friends, doctors) (25). In light of the potential consequences, early screening for the risk of postnatal depression seems essential.
The Edinburgh Postnatal Depression Scale (EPDS) is one of the most widely used screening instruments for assessing symptoms of maternal postnatal depression (26, 27). The main objective of the present study was to assess the prevalence of MPD in a French area of practice by administering the EPDS during the first “peak” of MPD incidence (i.e., between the 6th and the 10th week of the infant's life) and to concomitantly screen for early clinical signs in the infant. The objective was to explore the relationship between mothers' sociodemographic characteristics and EPDS scores and any early clinical signs present in the infant, for the purpose of evaluating a potential screening tool for use in the general population that would combine the EPDS with questions focused on functional signs in the infant. In other words, could early clinical signs in the infant signal possible psychological suffering on the part of the mother—and therefore offer an avenue for improving the detection of MPD and beginning treatment as early as possible?
Women who delivered between 18 December 18 2017 and 30 April 30 2018 and who visited the Vienne PMI (a free public health service offering consultations for children from 0 to 6 years old) were contacted to participate in the study. The inclusion criteria were: mothers having given birth, having an infant aged between 6 and 10 weeks, living in Vienne (a department in eastern France), having internet access, and having given informed consent for the study. We chose “having an infant aged between 6 and 10 weeks” as a criterion because many researchers consider the DSM-5's definition of “postpartum period” (i.e., 4 weeks) to be too short, given what is already well-established in professional practice and in scientific research on the subject (4). The best estimates of the point prevalence of major and minor disorders are in the first three months postpartum. Regarding major depression alone, there are three seemingly “peak” periods of incidence: during the second trimester of pregnancy, 2 months postpartum, and 6 months postpartum (28). The first peak of MPD incidence would therefore be between the 6th and the 10th week of the infant's life (29). The exclusion criterion was low French language or literacy skills, and the outcome of the study was infant death.
Sociodemographic data were collected. MPD was measured by the French version of the EPDS, a validated 10-item self-report questionnaire that can be completed in just a few minutes (30, 31). The EPDS can detects depression in mothers from the 4th week postpartum (31) by assessing emotional experiences over the past 7 days (26). Mothers respond on a Likert scale between 0 (“not at all”) and 3 (“yes, most of the time” or “quite a lot”). The French version has good psychometric properties, and item comprehension is excellent and unequivocal (30).
The best cutoff value for the EPDS to screen for depression, according to both the DSM-5 and the International Classification of Diseases, Tenth Revision (ICD-10), would be 11 or higher (32), as this value maximizes the combined sensitivity and specificity (81 and 88%, respectively) (27). In the French study, a cutoff score of 11.5 for screening for major depressive disorder provided optimum results, with 80% sensitivity and specificity (30). For the present study, the EPDS cutoff value was 12.
Finally, the presence of early clinical signs in the infant was investigated via the use of closed (i.e., yes or no) questions, that asked whether the infant has or has had difficulty sleeping, feeding difficulties, crying difficult to calm, or other difficulties identified by the mother. Mothers were also able to add a comment to express themselves freely on points not addressed or to clarify a response.
The statistical analyses were carried out using Jamovi, version 1.0.8.0. The present study first examined postpartum depression based on the EPDS score, a quantitative variable. The Pearson correlation test was used to study the relationship between this variable and age (a quantitative variable). The study then focused on EPDS score as a qualitative variable (negative if EPDS <12 and positive if ≥ 12, our threshold score for postpartum depression). The relationship between the EPDS qualitative variable and other qualitative variables (e.g., parity, marital status, occupational status, presence of early functional signs in the infant) was studied using the chi-square test of independence. Finally, a multivariate analysis of the qualitative variable EPDS was carried out.
Nearly half (49.2%) of all women who delivered in the study area during the research period participated in the study, representing a total of 767 mothers aged between 18 and 46 (M = 30.5, SD = 4.9), 40.38% of whom were primiparous. In terms of their relationship status, 3.65% were single, 33.12% were in partnered relationships, 2.35% were in partnered relationships living separately, and 60.89% were married couples. Concerning their professional activities, 6.13% had resumed their activity at the time of the survey, 77.44% were on maternity leave, 2.61% were on parental leave, 0.91% were students, and 12.91% were unemployed.
The average EPDS score of our sample was 7.42, with a standard deviation of 4.98; the minimum score was 0 and the maximum was 25 (n = 767).
In the present study, 22.16% of mothers (n = 170) had EPDS scores ≥12, 77.84% (n = 597) had scores <12, 25.13% (n =193) had scores >10, and 9.5% (n=73) had scores >14.
Age and MPD status were not correlated [r (765) = −0.008, p = 0.83].
Table 1 summarizes the results between the MPD status and the other qualitative variables.
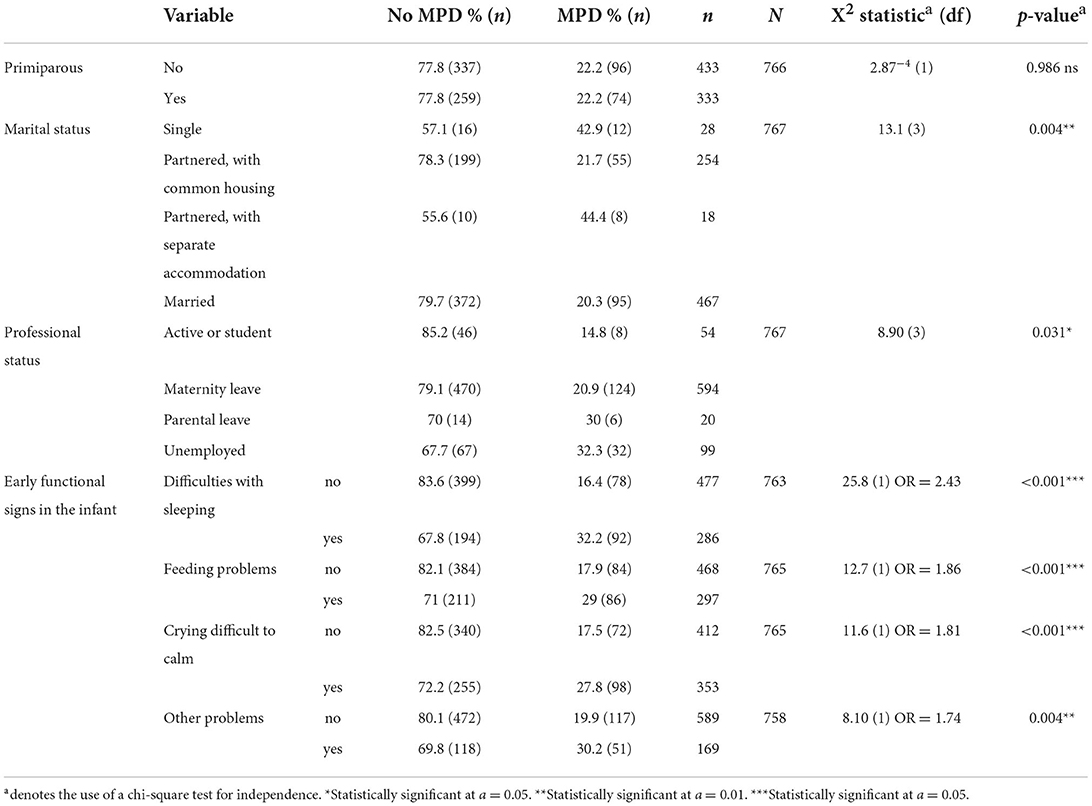
Table 1. Association between MPD status and other qualitative variables.
Figure 1 shows the distribution of EPDS scores. There was no significant relationship between MPD status and being primiparous. A chi-square test of independence was performed to examine the relationship between MPD and being primiparous. The relationship between these variables was not significant.
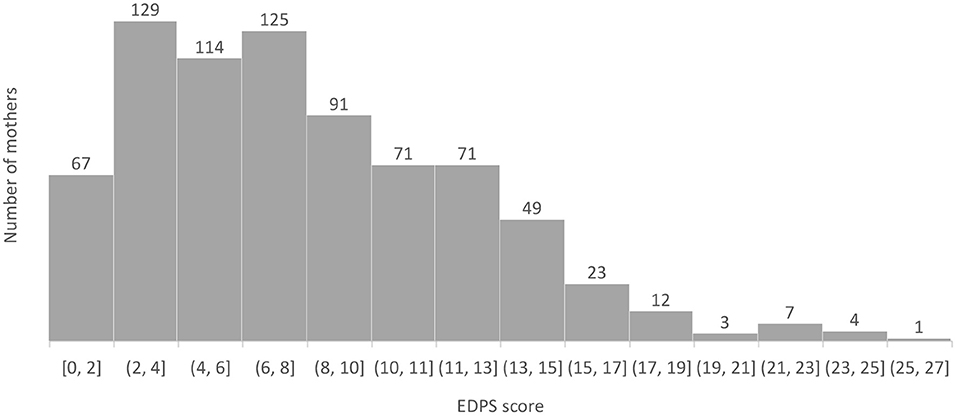
Figure 1. Distribution of EPDS scores.
We detected a significant relationship between these variables. In this study, single mothers or Mothers in couples with separate housing seemed to have an increased risk of MPD. More precisely, 42.9% of single mothers and 44.4% of single mothers of their spouse in our sample met the criteria for MPD.
The relationship between these variables was also significant (We therefore performed a binomial logistic regression to investigate further). Professional status explained only 1% of the MPD observed in the present study. However, the risk of MPD was 2.75 times greater for unemployed women than for women who were students or actively employed.
The relationship between sleep difficulties in the infant and MPD in the mother was very significant. In the present study, 54.1% of infants whose mothers suffered from MPD had sleep problems, compared to 32.7% of infants whose mothers did not suffer from MPD. The risk of having a mother with MPD was 2.43 times greater for an infant suffering from sleep difficulties than for an infant with no sleep difficulties (OR [odds ratio] = 2.43).
The relationship between feeding problems in the infant and MPD in the mother was also significant. In the present study, 50.6% of infants whose mothers suffered from MPD had feeding problems, compared to 35.5% of infants whose mothers did not suffer from MPD (OR = 1.86).
The relationship between infants experiencing crying that was difficult to calm and mothers experiencing MPD was significant (OR = 1.81).
The relationship between infants experiencing other types of distress and mothers experiencing MPD was significant (OR = 1.74).
In the binomial logistic regression, we combined the presence of early functional signs in the infant (i.e., sleep or feeding difficulties, crying difficult to calm) with mothers' marital and professional statuses. This model explained only 6.67% of the observed variance in MPD (pseudo R2 = 0.067). Mothers' marital status, especially the status of single vs. married (OR = 2.43), along with the presence of sleep difficulties (OR = 2.05) or feeding difficulties (OR = 1.59) in the infant, seemed to be the best predictors of MPD. Table 2 summarizes the results of the logistic regression.
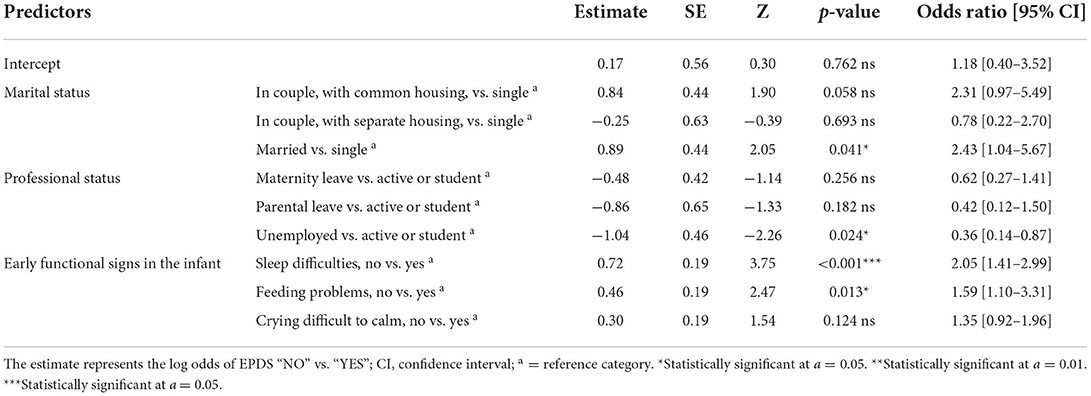
Table 2. Predictors of MPD.
The prevalence of MPD in our sample, 22.16%, is consistent with the literature, although rather high. However, with an EPDS cutoff value of 12, it is unlikely that we have overestimated the prevalence. Indeed, according to a recent review, the mean EPDS cutoff score used in the literature is 11.5 (range 10 to 14), while the most frequently used score is 104. Concerns about overestimation could arise from the fact that the EPDS, the tool most often used in studies, also captures adjustment disorder, a stress-related, time-limited, and non-psychotic disturbance that features anxiety, depressed mood, and a feeling of inability to cope and plan ahead. Adjustment disorder is seen as an understandable but maladaptive response to a stressful event, in this context the birth of an infant, that resolves spontaneously when the stressor is removed or a new level of adaptation is reached (33). In all cases, the mother suffers from a mental disorder and her infant feels it. Yet, the mother's mental health during pregnancy and the first year postpartum is very important for the cognitive, social, and emotional development of her child (34). It should be noted that the data were collected before the COVID-19 pandemic. It is very likely that the prevalence is even higher today because the pandemic has had a significant impact on the mental health of mothers (35).
In our study, and in accordance with the literature, being a single mother or being part of a couple that does not share accommodation was positively associated with the risk of MPD. This variable can even be the most highly predictive of MPD, with one study finding an OR of 3.06 for the latter (36). As of 2018, 59.3% of French women were legally single, divorced, or widowed (37) yet these risk categories would concern “only” 8.4% of mothers. More recently, the COVID-19 pandemic has increased the lack of social support (via measures such as lockdowns, isolation, and social distancing) as well as the risk of depression among vulnerable populations, such as pregnant women (38). It therefore may be appropriate to provide home-based care for these single mothers.
Being unemployed appears to be associated with an increased risk of MPD (OR = 0.36), but being on maternity or parental leave does not. This suggests that is not the fact of not working that increases the risk of MPD, but rather the professional uncertainty and/or financial precarity that accompany being unemployed. Indeed, lower socioeconomic status and lack of financial support have already been identified as risk factors in several studies (8).
We also found an association between sleep or feeding difficulties in the infant and MPD in the mother. According to the literature, 15% to 35% of parents observe sleep difficulties in their child during the first 6 months of life (39). The high percentage we observed can be explained by our methodology, namely, a question linked to the subjective interpretation of the mother without defined criteria. In fact, 37.4% of mothers in our study reported that their infants had difficulty sleeping: 32.7% in the non-MPD group and 54.1% in the MPD group. Newborn babies of depressed mothers have more sleep disorders, including decreased durations of deep sleep and increased durations of disorganized sleep (40). If the sleeping difficulties experienced by infants are correlated with MPD in mothers, perhaps this sign should alert practitioners to screen for MPD in the mother. This is especially important because a baby's sleep problems disrupt the parents' sleep, which can lead to parental fatigue, reduced ability to care for the baby effectively, and symptoms of postpartum depression (41). Taking care of these mothers as early as possible is therefore essential for them and their baby.
In our study, feeding difficulties included colic, regurgitation, gastroesophageal reflux, difficulties in breastfeeding or bottle feeding, and difficulties with weight gain. Feeding difficulties were observed by 35.5% of mothers in the non-MPD group and 50.6% of mothers in the MPD group, and these results are concordant with the literature. Breastfeeding difficulties and concerns about infant weight gain are predictors of maternal distress (36). In addition, colic in infants is associated with a higher risk of depression in the mother, with odds ratios between 2 (95% CI 1.1–3.7) (42) and 3.7 (95% CI 1.4–10.1) (43). The presence of colic is associated with a higher depression score in mothers at 2 months, and this can extend up to 4 months later even if the colic resolves (43). The identification of feeding problems in infants should therefore alert the pediatrician to potential psychological distress in the mother, as this can allow for early management of MPD.
Our study has some limitations. The prevalence in our study is an estimation conducted at the moment of the first “peak” of MPD (between the 6th and the 10th week of the infant's life). It is also plausible that, in recruiting the most available participants for the study, we excluded women with more significant symptoms. The figure of 22.16% therefore may not reflect the complete prevalence. Moreover, our study does not provide information on the mothers' experiences with depression and/or anxiety before and during pregnancy. Another study that conducted a longitudinal investigation using structural equation modeling found that prenatal depressive symptoms were the greatest predictor of postpartum depression (44). It is therefore likely that several mothers among the 22.16% experienced depression before or during the pregnancy that continued afterwards, in line with the findings of several other studies (45, 46). This highlights the relevance of the concept of perinatal depression for the prevention and screening of this disorder. Moreover, even as the analyses carried out here allow us to talk about infants' clinical signs as potential predictors of postnatal depression, it is obvious that postnatal depression in the mother could also be considered a predictor of clinical signs found in the infant. Nevertheless, whatever the predictors used, the presence of one allows us to look for the presence of the other due to their correlation.
Routine screening is strongly encouraged by the American College of Obstetricians and Gynecologists (ACOG), the US Preventive Services Task Force, and the National Collaborating Centre for Mental Health in the UK (47). ACOG recommends early postpartum follow-up care, including screening for depression and anxiety, for all postpartum women (8). In France, a national survey on maternal mortality highlighted that maternal suicides are not only one of the two leading causes of maternal death, but also one of the most preventable (15). Experts recommend screening for psychological disorders, to identify the warning signs, to understand the indications for psychiatric hospitalization, to train and raise awareness of mental health in perinatal care, and to develop resources within the geographic territory. The use of the EPDS, a very rapid tool recommended many countries' postpartum programs in the primary health care setting, could facilitate the following of these recommendations (48). Pediatricians observing functional signs such as sleep or feeding difficulties in the infant could propose this 10-item questionnaire to the mother.
MPD is a common disorder, affecting more than one in five mothers. It requires early management to prevent negative consequences for both infants and mothers. Single women or women who live separately from their partners are at higher risk for developing MPD than mothers who are married or live under the same roof as their partners. In addition, clinical signs in the infant such as difficulties with sleeping or feeding are associated with a higher risk of depression in the mother. Their presence should alert the pediatrician to potential psychological suffering on the part of the mother. The EPDS, a 10-item rapid self-assessment scale, should then be used as a first-line tool for this screening.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Henri Laborit Hospital, 370 avenue Jacques Coeur, 86 021 POITIERS CEDEX. The patients/participants provided their written informed consent to participate in this study.
SR designed the study and wrote the protocol. SJ-S performed the main data analysis and wrote the first draft of the manuscript. FR, CX-D, VC, and LG contributed to the assessments and data collection. SJ-S, GA, LR, and LG contributed to the analysis of the results and to the writing of the manuscript. All authors contributed to this article, have approved the final manuscript, have agreed both to be personally accountable for their own contributions, and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated and resolved, and the resolution documented in the literature.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Zivoder I, Martic-Biocina S, Veronek J, Ursulin-Trstenjak N, Sajko M, Paukovic M. Mental disorders/difficulties in the postpartum period. Psychiatr Danub. (2019) 31(Suppl. 3):338–44.
2. APA AP. DSM-5 - Manuel Diagnostique et Statistique des Troubles Mentaux. 5 éd. Issy-les-Moulineaux: Elsevier Masson (2015).
3. Halbreich U, Karkun S. Cross-cultural and social diversity of prevalence of postpartum depression and depressive symptoms. J Affect Disord. (2006) 91:97–111. doi: 10.1016/j.jad.2005.12.051
4. Moraes GP de A, Lorenzo L, Pontes GAR, Montenegro MC, Cantilino A. Screening and diagnosing postpartum depression: when and how? Trends Psychiatry Psychother. (2017) 39:54–61. doi: 10.1590/2237-6089-2016-0034
5. Woody CA, Ferrari AJ, Siskind DJ, Whiteford HA, Harris MG. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J Affect Disord. (2017) 219:86–92. doi: 10.1016/j.jad.2017.05.003
6. Agbokou C, Ferreri F, Nuss P, Peretti CS. Clinique des Dépressions Maternelles Postnatales. Datatraitesps37-56087. (2011). Available online at: https://www.em-consulte.com/en/article/299633/auto#N101BC (accessed December 2, 2019).
7. Šebela A, Hanka J, Mohr P. Etiology, risk factors, and methods of postpartum depression prevention. Ceska Gynekol. (2018) 83:468–73.
8. US Preventive Services Task Force, Curry SJ, Krist AH, Owens DK, Barry MJ, Caughey AB, et al. Interventions to prevent perinatal depression: US preventive services task force recommendation statement. JAMA. (2019) 321:580–7. doi: 10.1001/jama.2019.0007
9. Howard LM, Oram S, Galley H, Trevillion K, Feder G. Domestic violence and perinatal mental disorders: a systematic review and meta-analysis. PLoS Med. (2013) 10:e1001452. doi: 10.1371/journal.pmed.1001452
10. El-Hachem C, Rohayem J, Bou Khalil R, Richa S, Kesrouani A, Gemayel R, et al. Early identification of women at risk of postpartum depression using the Edinburgh Postnatal Depression Scale (EPDS) in a sample of Lebanese women. BMC Psychiatry. (2014) 14:242. doi: 10.1186/s12888-014-0242-7
11. Sagayadevan V, Lee SP, Abdin E, Vaingankar J, Chen H, Chong SA, et al. Retrospective observation of mental disorders during postpartum period: results from the Singapore mental health study. BMC Womens Health. (2015) 15:119. doi: 10.1186/s12905-015-0279-x
12. Biaggi A, Conroy S, Pawlby S, Pariante CM. Identifying the women at risk of antenatal anxiety and depression: a systematic review. J Affect Disord. (2016) 191:62–77. doi: 10.1016/j.jad.2015.11.014
13. Milgrom J, Martin PR, Negri L. Treating Postnatal Depression: A Psychological Approach for Health Care Practitioners. John Wiley&Sons (1999). Available online at: https://www.wiley.com/en-us/Treating+Postnatal+Depression%3A+A+Psychological+Approach+for+Health+Care+Practitioners-p-9780471986454 (accessed August 5, 2022).
14. Norhayati MN, Nik Hazlina NH, Asrenee AR, Wan Emilin WMA. Magnitude and risk factors for postpartum symptoms: a literature review. J Affect Disord. (2015) 175:34–52. doi: 10.1016/j.jad.2014.12.041
15. Santé publique France. Les Morts Maternelles en France : Mieux Comprendre Pour Mieux Prévenir. 6e Rapport de l'Enquête Nationale Confidentielle sur les Morts Maternelles (ENCMM), 2013-2015. (2021). Available online at: http://www.epopé-inserm.fr/en/grandes-enquetes/enquete-nationale-confidentielle-sur-les-morts-maternelles (accessed July 5, 2022).
16. Slomian J, Honvo G, Emonts P, Reginster JY, Bruyère O. Consequences of maternal postpartum depression: a systematic review of maternal and infant outcomes. Womens Health Lond Engl. (2019) 15:1745506519844044. doi: 10.1177/1745506519844044
17. Adewuya AO, Ola BO, Aloba OO, Mapayi BM, Okeniyi JAO. Impact of postnatal depression on infants' growth in Nigeria. J Affect Disord. (2008) 108:191–3. doi: 10.1016/j.jad.2007.09.013
18. Rahman A, Bunn J, Lovel H, Creed F. Maternal depression increases infant risk of diarrhoeal illness: –a cohort study. Arch Dis Child. (2007) 92:24–8. doi: 10.1136/adc.2005.086579
19. Akman I, Kusçu K, Ozdemir N, Yurdakul Z, Solakoglu M, Orhan L, et al. Mothers' postpartum psychological adjustment and infantile colic. Arch Dis Child. (2006) 91:417–19. doi: 10.1136/adc.2005.083790
20. de Kruijff I, Choenni V, Groeneweg JT, Vlieger AM, Benninga MA, Kok R, et al. Gastrointestinal symptoms in infants of mothers with a psychiatric history and the role of depression and bonding. J Pediatr Gastroenterol Nutr. (2019) 69:662–7. doi: 10.1097/MPG.0000000000002484
21. Gress-Smith JL, Luecken LJ, Lemery-Chalfant K, Howe R. Postpartum depression prevalence and impact on infant health, weight, and sleep in low-income and ethnic minority women and infants. Matern Child Health J. (2012) 16:887–93. doi: 10.1007/s10995-011-0812-y
22. Pinheiro KAT, Pinheiro RT, da Silva RA, Coelho FM, Quevedo Lde Á, Godoy RV, et al. Chronicity and severity of maternal postpartum depression and infant sleep disorders: a population-based cohort study in southern Brazil. Infant Behav Dev. (2011) 34:371–3. doi: 10.1016/j.infbeh.2010.12.006
23. Brown A, Rance J, Bennett P. Understanding the relationship between breastfeeding and postnatal depression: the role of pain and physical difficulties. J Adv Nurs. (2016) 72:273–82. doi: 10.1111/jan.12832
24. Petzoldt J, Wittchen HU, Einsle F, Martini J. Maternal anxiety versus depressive disorders: specific relations to infants' crying, feeding and sleeping problems. Child Care Health Dev. (2016) 42:231–45. doi: 10.1111/cch.12292
25. Godfroid IO. [DSM IV criteria for post-partum depression: debatable?]. L'Encephale. (1997) 23:224.
26. Shrestha SD, Pradhan R, Tran TD, Gualano RC, Fisher JRW. Reliability and validity of the Edinburgh Postnatal Depression Scale (EPDS) for detecting perinatal common mental disorders (PCMDs) among women in low-and lower-middle-income countries: a systematic review. BMC Pregn Child. (2016) 16:72. doi: 10.1186/s12884-016-0859-2
27. Levis B, Negeri Z, Sun Y, Benedetti A, Thombs BD, DEPRESsion Screening Data (DEPRESSD) EPDS Group. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: systematic review and meta-analysis of individual participant data. BMJ. (2020) 371:m4022. doi: 10.1136/bmj.m4022
28. Gaynes BN, Gavin N, Meltzer-Brody S, Lohr K. Prevalence Incidence of Perinatal Depression. Agency for Healthcare Research Quality (US) (2005). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK37751/ (accessed May 30, 2022).
29. Missonnier S, Blazy M, Boige N, Presme N, Tagawa O, Jaillardon C. Manuel de Psychologie Clinique de La Périnatalité. Paris: Elsevier Masson (2012).
30. Adouard F, Glangeaud-Freudenthal NMC, Golse B. Validation of the Edinburgh postnatal depression scale (EPDS) in a sample of women with high-risk pregnancies in France. Arch Womens Ment Health. (2005) 8:89–95. doi: 10.1007/s00737-005-0077-9
31. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry J Ment Sci. (1987) 150:782–6. doi: 10.1192/bjp.150.6.782
32. Smith-Nielsen J, Matthey S, Lange T, Væver MS. Validation of the Edinburgh postnatal depression scale against both DSM-5 and ICD-10 diagnostic criteria for depression. BMC Psychiatry. (2018) 18:393. doi: 10.1186/s12888-018-1965-7
33. O'Keeffe N, Ranjith G. Depression, demoralisation or adjustment disorder? Understanding emotional distress in the severely medically ill. Clin Med. (2007) 7:478–81. doi: 10.7861/clinmedicine.7-5-478
34. Goodman JH. Perinatal depression and infant mental health. Arch Psychiatr Nurs. (2019) 33:217–24. doi: 10.1016/j.apnu.2019.01.010
35. Kotlar B, Gerson E, Petrillo S, Langer A, Tiemeier H. The impact of the COVID-19 pandemic on maternal and perinatal health: a scoping review. Reprod Health. (2021) 18:10. doi: 10.1186/s12978-021-01070-6
36. Staehelin K, Kurth E, Schindler C, Schmid M, Zemp Stutz E. Predictors of early postpartum mental distress in mothers with midwifery home care: results from a nested case-control study. Swiss Med Wkly. (2013) 143:w13862. doi: 10.4414/smw.2013.13862
37. INSEE. État Matrimonial Légal des Personnes Selon le Sexe. (2019). Available online at: https://www.insee.fr/fr/statistiques/2381496#tableau-Tableau2 (accessed March 7, 2020).
38. Saccone G, Florio A, Aiello F, Venturella R, De Angelis MC, Locci M, et al. Psychological impact of coronavirus disease 2019 in pregnant women. Am J Obstet Gynecol. (2020) 223:293–5. doi: 10.1016/j.ajog.2020.05.003
39. Cook F, Bayer J, Le HN, Mensah F, Cann W, Hiscock H. Baby Business: a randomised controlled trial of a universal parenting program that aims to prevent early infant sleep and cry problems and associated parental depression. BMC Pediatr. (2012) 12:13. doi: 10.1186/1471-2431-12-13
40. Field T, Diego M, Hernandez-Reif M, Figueiredo B, Schanberg S, Kuhn C. Sleep disturbances in depressed pregnant women and their newborns. Infant Behav Dev. (2007) 30:127–3. doi: 10.1016/j.infbeh.2006.08.002
41. Bayer JK, Hiscock H, Hampton A, Wake M. Sleep problems in young infants and maternal mental and physical health. J Paediatr Child Health. (2007) 43:66–73. doi: 10.1111/j.1440-1754.2007.01005.x
42. Radesky JS, Zuckerman B, Silverstein M, Rivara FP, Barr M, Taylor JA, et al. Inconsolable infant crying and maternal postpartum depressive symptoms. Pediatrics. (2013) 131:e1857–64. doi: 10.1542/peds.2012-3316
43. Vik T, Grote V, Escribano J, Socha J, Verduci E, Fritsch M, et al. Infantile colic, prolonged crying and maternal postnatal depression. Acta Paediatr. (2009) 98:1344–8. doi: 10.1111/j.1651-2227.2009.01317.x
44. Gerardin P. Spécificité et enjeux de la dépression de la grossesse. Principaux résultats d'une recherche longitudinale sur les dépressions du péripartum, du troisieme trimestre de grossesse au 12e mois de l'enfant. Neuropsychiatr Enfance Adolesc. (2012) 60:138–46. doi: 10.1016/j.neurenf.2011.10.006
45. O'Hara MW. La dépression du post-partum: les études de l'Iowa. Devenir. (2001) 13:7–20. doi: 10.3917/dev.013.0007
46. English S, Steele A, Williams A, Blacklay J, Sorinola O, Wernisch L, et al. Modelling of psychosocial and lifestyle predictors of peripartum depressive symptoms associated with distinct risk trajectories: a prospective cohort study. Sci Rep. (2018) 8:12799. doi: 10.1038/s41598-018-30874-z
47. Martínez-Borba V, Suso-Ribera C, Osma J, Andreu-Pejó L. Predicting postpartum depressive symptoms from pregnancy biopsychosocial factors: a longitudinal investigation using structural equation modeling. Int J Environ Res Public Health. (2020) 17:8445. doi: 10.3390/ijerph17228445
Keywords: screening, maternal postnatal depression, psychopathology, early clinical signs, management
Citation: Julien-Sweerts S, Rousselin S, Raffeneau F, Xavier-David C, Changeur V, Apter G, Romo L and Gicquel L (2022) Toward early screening for early management of postnatal depression? Relationships between clinical signs present in the infant and underlying maternal postnatal depression. Front. Psychiatry 13:986796. doi: 10.3389/fpsyt.2022.986796
Received: 05 July 2022; Accepted: 18 August 2022;
Published: 09 September 2022.
Edited by:
Çiçek Hocaoğlu, Recep Tayyip Erdoğan University, TurkeyReviewed by:
Nicole Rascle, Université de Bordeaux, FranceCopyright © 2022 Julien-Sweerts, Rousselin, Raffeneau, Xavier-David, Changeur, Apter, Romo and Gicquel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sabrina Julien-Sweerts, c2FicmluYWp1bGllbnN3ZWVydHNAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.