 Eunhye Choi
Eunhye Choi Eun-Ha Yoon
Eun-Ha Yoon Min-Hyeon Park
Min-Hyeon Park- Department of Psychiatry, Eunpyeong St. Mary's Hospital, Catholic University of Korea, Seoul, South Korea
Mental health problems in childhood and adolescence (e. g., attention deficits, problems in emotional understanding and subclinical levels of anxiety) are reported to develop further in adulthood and/or to increase the risk of developing mental health disorders in adulthood. Although it is important to provide treatment or prevention interventions for children and adolescents in order to reduce the risk of the further development of mental health problems, the pharmacological and behavioral treatments for this age group have limitations (e.g., limited access, unsustainable treatment effects and the lack of engagement in intervention). In order to overcome the limitations of conventional treatments, the use of digital technology, especially video games for this age group, is suggested. In order to be accepted as clinical interventions, objective evidence for the therapeutic effects of digital therapeutic that used video games to treat or prevent targeted mental health problems are required. Thus, this review aims to explore whether game-based digital therapeutics (DTx) for children and adolescents showed therapeutic effects on targeted mental health problems. As game-based DTx are suggested to show sustained therapeutic effects and the transfer of cognitive functions, it also reviews the maintenance of the therapeutic effects of DTx and the extent of the transfer of cognitive functions. Game-based DTx that are developed to treat or prevent mental health problems (e.g., attention deficit, depression) in children and adolescents are found to show therapeutic effects on targeted mental health problems despite the limitations (e.g., small sample size, limited investigation of the sustainability). This review would contribute to the understanding of whether there is objective evidence of the therapeutic effects of digital therapeutics using video games that deliver treatment or prevention interventions for mental health problems in children and adolescents.
Introduction
More than 10% of children and adolescents in the world are reported to have mental health problems (1). With the improvement in diagnosis systems (2), there is an increase in the clinical diagnosis of neurodevelopmental disorders (e.g., attention deficits) in this age group compared to the past (3). An increased prevalence of affective disorders (e.g., depressive symptoms) in childhood and adolescence is also reported (3). Clinical or subclinical mental health problems (e.g., attention deficit, anxiety and depressive symptoms) in childhood and adolescence appear to be persistent into adulthood (4). About 50% of young adults show mental health disorders that are continued from their childhood psychiatric disorders (5). Moreover, children and adolescents, who report clinical or subclinical mental health conditions, are more likely to develop mental health problems later in their adulthood (6–8). As mental health problems in children and adolescents tend to be persistent and recurrent in their adulthood (9), it is important to provide effective interventions for mental health problems in this age group (10, 11).
However, a lot of children and adolescents are estimated to have difficulties receiving the interventions for their mental health problems (12) due to two barriers. One barrier is the side effects of pharmacological treatments that limit treatment options for this age group (13, 14). Pharmacological treatments that show side effects (e.g., headaches and insomnia) in some patients with attention deficits (13) are not acceptable for some children with attention deficits (15). In case of antidepressants, their safety and effectiveness in adolescents have been argued (16) despite the increased use of them in this age group (17). The other barrier is the limited access to the treatments (18). The number of adequately trained therapists or the availability of facilities is not sufficient to meet the needs for overall mental health problems (11, 19). In case of neurofeedback that aims to treat attention deficit hyperactivity disorder (ADHD), it offers visual or auditory reinforcement in order to alter activities of relevant brain regions (20, 21) that are found to show specific electroencephalography (EEG) patterns in children with ADHD (22). That is, as its treatment effects on ADHD is highly dependent on the ability of clinicians to establish links between the symptoms of a patient and his or her dysregulated EEG patterns in brain regions (20), the accessibility to the clinicians with the adequate level of trainings is required. Furthermore, the COVID-19 that results in social distancing and lockdown in some countries makes the access to face-to-face interventions even more limited (23). In order to successfully offer the interventions for mental health problems in children and adolescents by overcoming the barriers, it has become important to develop more innovative and cost-effective intervention methods for this age group (24).
Digital technology is suggested as a delivery tool for automated and self-directed interventions by improving the accessibility (25). Software-driven therapeutic interventions that aim to prevent, manage, or treat medical or chronic diseases are referred to as Digital Therapeutics (DTx) (26). Unlike wellness or other digital health products that deliver more personalized clinical care based on the understanding of health-related behaviors through digital technology (27, 28), DTx are developed to target a specific disorder or disease (29). DTx could target the conditions that are difficult to be intervened in frequently used interventions (30). As DTx are regarded as “an emerging class of medicines” (31), they also have obtained the approval of the relevant regulatory authorities (e.g., the U.S. Food and Drug Administration) (30) based on clinical evidence for the effectiveness similar to conventional medicines and medicine supplies (29). DTx that could decrease time demands of clinicians during the interventions (26) are found to be effective in the improvement of various clinical conditions (e.g., the impairment of sensorimotor functions, cognitive deficits and depression) by replacing or complementing other intervention methods (32). Among various technological platforms and systems that have been facilitated to enhance the delivery of healthcare services (26), video games (VGs) that can be helpful for mental health problems (e.g., emotion regulation, stress management, attention deficits and depression) are suggested as an attractive and immersive delivery tool for clinical interventions in children and adolescents (33, 34).
VGs, one of the most entertaining activities for children and adolescents (35), could provide them with more flexible and personalized learning environments (36) by maintaining the optimal level of challenges for players in response to their actions (37). Engagement issues and the limited consideration of individual differences in learning process are reported to limit the effective delivery of mental health interventions. For example, people with ADHD have difficulty managing their brain activities repeatedly over neurofeedback training sessions despite its effectiveness (20). The motivation level and the extent of engagement that children and adolescents show in cognitive trainings [e.g., Rational Emotive Behavior Education (REBE) interventions that focused on the cultivation of rational beliefs (11), cognitive behavioral therapy (CBT)] are also not stable during the intervention process (38, 39). That is, despite their effectiveness for anxiety symptoms (39), the way to deliver the interventions seems to be related to the decreased effectiveness (35, 40). Moreover, some children and adolescents (e.g., those with attention deficits) show difficulties learning new abilities in CBT that focuses on the shift of the anxious state trough relaxation trainings (37) and need more time to learn these skills (41). It is found to be difficult to consider the diversity of learning needs and individual differences in learning paces of children in the interventions (37).
Furthermore, the sustainability and generalization of therapeutic effects outside the intervention periods [e.g., (42)] are concerns that should be considered in order to improve the effectiveness of the interventions for mental health problems. Pharmacological and behavioral treatments show unsustainable therapeutic effects over time (43, 44). Practice activities for the generalization of skills in CBT (e.g., role-playing and homework assignments) are not effective for various reasons (e.g., limited time and subjective boredom) (37) and learned skills in traditional biofeedback interventions show limited generalization in real-world settings despite their effectiveness on the reinforcement of emotional relaxation abilities (45). However, VGs could offer opportunities for the generalized practice of learned skills by making players feel a strong sense of agency, entertainment and rewards (37). Thus, implementing VGs or gaming elements (e.g., meaningful contexts and scenarios to serve learning objectives) (41, 46) in the interventions for mental health problems of children and adolescents is suggested to have the potential to overcome the limitations of frequently used mental health interventions.
Taken together, despite the increasing needs for mental health interventions in children and adolescents, intervention options for this age group are limited and effective interventions report concerns that could influence the effectiveness during and after the interventions. The implementation of digital technology is suggested as alternative treatment or prevention interventions for mental health problems (23). Among various options of digital technology, VGs are found to be cost-effective (37) and age-appropriate (33, 34) delivery tool for children and adolescents with mental health problems. Although DTx using VGs are suggested to have the potential to treat or prevent mental health problems in children and adolescents by overcoming concerned issues of frequently used interventions, the objective evidence for the effectiveness of DTx is not sufficient (47). The safety and efficacy of DTx should be proved for the acceptance for DTx by patients and clinicians (48), and some game-based DTx do not show sustained interventions effects (32) despite the potential for the generalization of skills that are learned in interventions (37, 41). Thus, this study aims to review whether game-based DTx show therapeutic or preventive effects on targeted mental health problems in children and adolescents. It also reviews the sustainability of the therapeutic effects of game-based DTx. Moreover, the extent of transfer of cognitive functions in game-based DTx for children and adolescents is reviewed. Not only intervention outcomes (e.g., decreased risk of falls) but also cognitive functions (e.g., processing speed and selective attention) were improved in older individuals (e.g., those who aged more than 60 years) who received game-based trainings (49–52). Improved cognitive functions after the game-based training (i.e., NeuroRacer) were comparable to cognitive functions of 20-year-olds and were maintained for 6 months along with alterations in brain activation (53). The results of studies in the non-clinical population suggested that implementing VGs has the potential for neuroplasticity. However, playing VGs are found to be related to near transfer of cognitive functions [i.e., the improvement of cognitive functions (e.g., attention) that are related to characteristics of VGs] (54, 55). That is, the VG-related neuroplasticity is limited to the brain regions that are related to characteristics of VGs. As the VG-related neuroplasticity could influence the therapeutic effects of DTx, the transfer of cognitive functions in children and adolescents with subclinical or clinical levels of mental health problems after game-based DTx interventions is additionally reviewed.
Methods
Literatures search was conducted in databases (e.g., PubMed and Web of Science) and Google Scholar with search terms (e.g., “digital therapeutics”, “video game digital therapeutics”, “digital therapeutics for children and adolescents”, and “game-based digital therapeutics for children and adolescents”) without the restriction of the publication date. In the process of screening searched literatures, not only the age of children and adolescents but also the measurements for therapeutic effects of DTx were not limited. Although DTx usually get approval from the regulatory institutions (30), game-based DTx for mental health problems in children and adolescents are an emerging research field where only one game-based DTx (i.e., EndeavorRx) for this age group was identified to be FDA-approved (56). Thus, game-based DTx in this study is defined as interventions that use VGs as a delivery tool to treat or prevent targeted mental health problems in children and adolescents with or without the approval from regulatory authorities. Mental health problems in the review encompass both neurodevelopmental and affective disorders that show an increasing trend in childhood and adolescence (3). Through the process of screening the searched literatures, seven game-based DTx for this age group were identified. In order to explore all relevant literatures that examined therapeutic or preventive effects of identified DTx, the additional search of literatures was conducted by using names of DTx that were indicated in literatures (e.g., “Project:EVO” and “RAGE-Control”) as additional search terms. After the additional search, abstracts were screened to identify whether children and/or adolescents were included as participants and whether the therapeutic effects of identified DTx were examined. The inclusion criteria of the literatures in this review were (1) full-text original research articles published in English and (2) the examination of therapeutic or preventive effects of game-based DTx that aimed to target mental health problems in children and adolescents. That is, DTx that are not developed to target mental health problems in children and adolescents and that do not include gaming elements as a delivery tool were not included. Research articles that did not investigate therapeutic or preventive effects of identified DTx in children and/or adolescents were also excluded. As a result, 22 research articles that met the inclusion criteria were included in this review.
Therapeutic effects of DTx for children and adolescents
Using digital devices is suggested to have the potential for the rehabilitation of cognitive functions by enhancing the neuroplasticity (32). Based on the potential effectiveness of game-based DTx for the cognitive rehabilitation (32), there are game-based DTx that are developed for children with ADHD or autism spectrum disorder (ASD) who show impairments in attention function and inhibitory control (44, 57). Children and adolescents are reported to have not only neurodevelopmental disorders but also affective disorders (3). Some children and adolescents report difficulties regarding emotional understanding that is related to the further development of emotional disorders (11). Some of them report subclinical levels of anxiety or depression (37, 58). That is, there are also game-based DTx that aim to treat or prevent affective disorders in children and adolescents. That is, seven game-based DTx that were identified through the literature search in databases are found to target attention deficits, emotional regulation, anxiety or depressive symptoms in this age group (see Table 1). While REThink aims to offer prevention intervention by making children and adolescents learn emotion regulation skills (59), other six game-based DTx aim to offer treatment interventions for targeted mental health problems.
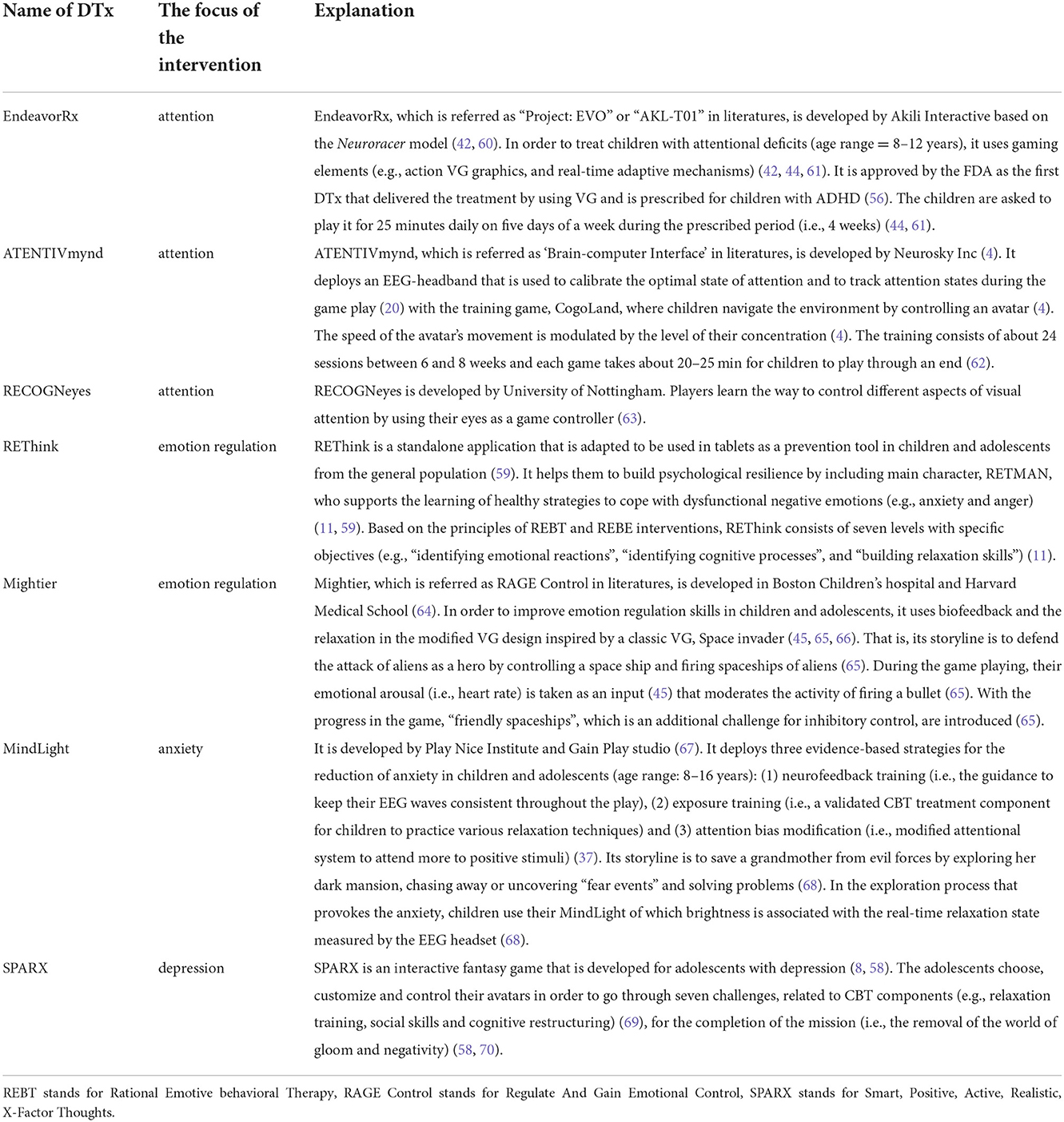
Table 1. The explanation of seven DTx for children and adolescents.
EndeavorRx
Children with ADHD showed a high level of adherence when playing EndeavorRx (42, 44, 57). EndeavorRx that was feasible in home environments and acceptable in the children (42, 57, 60) was found to significantly improve attention function in not only children with attention deficits (44, 71) but also those without the deficits (42, 60). Children, who had ASD and ADHD, also showed a trend of the improved attention function and inhibitory control (57). That is, based on parental reports, the effectiveness of EndeavorRx on decreased ADHD symptoms was found in children who had ASD and ADHD (57), children who had a recent history of pharmacological interventions for ADHD (44), and children who had ADHD without other comorbidities (71). The intervention-related improvement in attention functioning was found to be affected not by the changes in basic motoric speed but by the intervention (60, 71). Moreover, the extent of improvement in attention function through the EndeavorRx intervention was greater in children with a higher level of attention deficits (42, 60) and the improvement of attention resulted from the movement of more children, who received the intervention, into the normative ranges of attention function (44). Both one third of children who had sensory processing dysfunction (SPD) and inattentive-ADHD (60) and 44% of children who had ADHD without other comorbidities (71) did not meet the clinical threshold for inattention after the intervention. Their performance regarding attention after the intervention was comparable or even better than the baseline attention performance of typically developing children (60). Furthermore, as parental reports of reduced inattentive behaviors were associated with significantly increased middle frontal theta (MFT) activity power (60), playing EndeavorRx was related to the changes in the activations of brain regions for attention function (60, 71). Unlike the significant increases in MFT in the middle of the attention task in children with SPD and inattentive-ADHD (60), the significant increases in MFT in children who had ADHD without other comorbidities were found in the earlier and later stages of the task (71). These results suggest the therapeutic effects of EndeavorRx on attention deficits in children.
ATENTIVmynd
With a high level of compliance with ATENTIVmynd in children (4), children with ADHD showed significant decreases in inattentive symptoms after playing ATENTIVmynd (4, 72). Both parents and clinicians reported the improvement in ADHD symptoms in children through ATENTIVmynd compared to non–pharmaceutical interventions (20). Parental reports also showed the significant improvement of hyperactive-impulsive symptoms in children with the combined subtype of ADHD (4). Children with more severe attention deficits showed greater effects of ATENTIVmynd intervention (4). Moreover, children with ADHD showed the reorganization of the functional networks (e.g., decreased functional connectivity within the salience network), which was associated with the improvement of inattentive symptoms and the reduction of internalizing problems (72). ATENTIVmynd showed therapeutic effects of targeted attention deficits in children.
RECOGNeyes
Not adolescents but the majority of children, who were younger than 12 years, reported that playing RECOGNeyes was enjoyable and its levels of challenges were appropriate for them (63). While playing RECOGNeyes did not result in the change in the number of errors (i.e., commissions and omissions), the children and adolescents, who played RECOGNeyes by using their eyes as a controller, showed decreases in the level of impulsivity, made fewer fixations and fixated on the target for a longer duration than those who played RECOGNeyes by using the mouse as a controller (63). They also showed the improvement of impulsivity (63). That is, RECOGNeyes was found to improve the control of attention in children and adolescents with ADHD (63).
REThink
Compared to children who received REBE intervention, children, who played REThink, reported a higher level of satisfaction in the middle of REThik intervention that was an important factor to booster the therapeutic effects (11). Playing REThink was found not only to reduce overall negative emotional symptoms (e.g., anger and anxiety) but also to improve the emotional awareness and emotional control (11). That is, the risk of the development of problems decreased in children, who played REThink, but not in children, who received REBE intervention, and those in the waitlist group (11). Moreover, despite the overall decreases in anxiety symptoms in all groups of children, children, who played REThink, showed more inhibited activation in the frontal brain regions of the right hemisphere that was associated with negative affects and the motivation to withdraw (24). That is, it was found that the effectiveness of REThink on emotion regulation was associated with changes in irrational beliefs (73). The reports of emotional symptoms and depressive moods decreased in children, who played REThink, compared to those who received REBE intervention (73). These results suggested that REThink was an engaging and effective prevention intervention for children to learn emotional regulation skills.
Mightier
Mightier that was rated as a highly satisfactory, enjoyable and helpful intervention approach with a high level of adherence was found to be an acceptable intervention approach in children (66, 74). A case study that showed the feasibility of Mightier for the engagement and its effectiveness in coaching self-regulation skills suggested the potential that Mightier would have therapeutic effects in children and adolescents with anger and aggression (74). Compared to anger control therapy (ACT) that aimed to treat anger and aggression as one of CBT programs (75), Mightier that augmented ACT was found to significantly decrease symptoms of emotional arousal (e.g., anger) and to improve the maintenance of calm states in children and adolescents (66). As ACT did not show therapeutic effects on emotional arousal and the control of emotion (66), Mightier appeared to have the potential to be used as a standalone intervention for the emotion regulation. Moreover, as children whose primary diagnosis was a restrictive eating disorder showed improvement in anger after playing Mightier, Mightier appeared to have valuable therapeutic effects in children who showed some emotional problems regarding anger in addition to their primary mental health problems (66).
MindLight
MindLight that was rated to produce a higher level of anxiety by children compared to the commercial control game was reported to be less appealing than the control game (37) but more equally appealing like CBT interventions (76). The effectiveness of MindLight on the reduction of anxiety symptoms in children with the subclinical level of anxiety was found to be comparable to that of commercial control games (e.g., “Max” where players control the avatar in puzzle platform VG) (37, 77). Although children, who played MindLight, showed the similar extent of improvement of anxiety symptoms compared to those who played control games immediately after the intervention (37), not only children with more severe level of anxiety but also children with ASD in addition to subclinical anxiety symptoms showed improved anxiety symptoms after playing MindLight (37, 77). The therapeutic effect of MindLight on anxiety symptoms in children with elevated levels of anxiety was also comparable to that of CBT (76). MindLight was found to be an effective intervention for anxiety without the further addition of CBT elements in that including more CBT-related components in MindLight for children with ASD did not have additional therapeutic effects on anxiety (78). Moreover, compared to boys, girls, who showed higher levels of anxiety symptoms at the beginning of the intervention, showed greater decreases in their anxiety symptoms after playing MindLight (76). These results suggested that MindLight that provided the engaging context for children to practice their strategies for emotion regulation (37) showed the therapeutic effect on the subclinical level of anxiety that was comparable to the game- or CBT-relevant improvements (37, 76, 77).
SPARX
SPARX that was reported as a helpful and satisfactory intervention (8, 58) showed a high level of adherence in adolescents (58, 79) despite the relatively low adherence levels in the adolescent sample including transgender adolescents (69). The effectiveness of SPARX in the reduction of depressive symptoms was comparable to that of CBT in Dutch female adolescents with elevated depressive symptoms (8). Compared to usual treatments (e.g., counseling), SPARX was found to significantly reduce depressive symptoms in adolescents with mild to moderate depressive disorder (58) and adolescents who were excluded from mainstream education (79). The therapeutic effect of SPARX on depressive symptoms was greater in adolescents who showed more severe level of depression at the beginning of the intervention (58). However, SPARX did not show the improvement of depressive symptoms in transgender adolescents (69). Although SPARX did not effectively reduce depressive symptoms in some adolescents, it was suggested to have the therapeutic effect on depressive symptoms that was comparable to or better than the interventions for depression.
The identified seven game-based DTx are as effective as usual treatments (e.g., CBT) or show better therapeutic or preventive effects compared to some interventions (e.g., REBE interventions) (see Table 2). EndeavorRx, ATENTIVmynd and RECOGNeyes that target attention deficits show therapeutic effects in children and adolescents with ADHD (4, 44, 57, 63, 72). REThink and Mightier result in decreased symptoms of negative emotions (e.g., anger and depression) and improve emotional control compared to frequently used interventions (e.g., REBE interventions) (11, 24, 66, 73). While the therapeutic effect of MindLight on anxiety in children and adolescents is comparable to commercial VGs (37, 77) or CBT (76, 78), the extent of improvement of depression is found to be greater in adolescents who play SPARX than those who receive frequently used treatments (e.g., counseling) (58) and to be comparable to that of the CBT-based prevention approach (8).

Table 2. The summary of 21 studies that examined the therapeutic effects of DTx for children and adolescents.
The sustainability of therapeutic effects of DTx
Therapeutic effects of DTx were found to be sustained at follow-ups. The treatment effects of ATENTIVmynd, MindLight and SPARX on targeted mental health problems in children and adolescents were maintained for 3 months after the interventions (4, 20, 37, 58, 76, 77). The effectiveness of SPARX on depression was also maintained in children who were excluded from mainstream education at the 10-weeks follow-up (79). Moreover, the treatment effects of some DTx were maintained for longer durations. Larger decreases in anxiety symptoms that were reported by children who played MindLight were maintained at the 6-months follow-up and the sustained improvement in anxiety symptoms was reported by both children and their parents (76). Unlike the sustained improvement of anxiety symptoms in both children who played MindLight and those who played the control game, “Max”, at the follow-up (37), not parents of children, who played the control game (i.e., “Triple Town”), but parents of children, who played MindLight, reported the sustained decreases in their anxiety symptoms at the follow-up (77). In case of EndeavorRx, its therapeutic effects on attention function in children with SPD and inattentive-ADHD were sustained for 9 months after the intervention (60). Furthermore, receiving three booster training sessions of ATENTIVmynd during the 3-months follow-up did not show the further improvement of attention function at the follow-up (4). That is, the therapeutic effect of ATENTIVmynd on attention function was maintained without the additional training sessions (4). However, the extent of improvement of anxiety symptoms was lesser in children who played MindLight and reported the highest weekly engagement time in gaming (76). Taken together, although the sustainability of RECOGNeyes, REThink, and Mighter was not examined, EndeavorRx, ATENTIVmynd, MindLight, and SPARX were found to show sustained therapeutic effects on targeted mental health problems (i.e., attention function, anxiety and depressive symptoms) for at least 3 months outside the intervention period.
The transfer of cognitive functions in DTx
When the extent to which cognitive functions were improved in game-based DTx was investigated, they showed the near transfer of cognitive functions. Both children with ADHD and typically developing children showed improvement in spatial working memory (WM) after playing EndeavorRx (42). However, the significant improvement in WM and inhibition after EndeavorRx intervention was found not in typically developing children but in children with ADHD (42). Despite the trend of improvement in WM in children with ADHD, children with a more severe level of ADHD showed the significant improvement in WM and inhibition (42). Children, who played REThink, and those, who received REBE intervention, also showed the significant improvement in focused attention (11). However, the extent of improvement of cognitive functions was limited to the characteristics of game-based DTx. Children, who played ATENTIVmynd, showed the improvement in focused attention by staying on tasks, completing more questions in the time limit and correctly answering more questions compared to those in the control group but did not show improvements in reading and math fluency after playing ATENTIVmynd (20). That is, DTx that targeted attention deficit or aimed to prevent emotional problems through the development of emotion regulation showed the improvement in cognitive functions that were related to the targeted mental health problems.
Discussion
This study aimed to review whether there are therapeutic effects of game-based DTx that are developed to target mental health problems in children and adolescents by delivering treatment or prevention interventions through VGs. It also reviewed whether the therapeutic effects of game-based DTx are sustainable and/or show the transfer of cognitive functions. Based on the review of literatures for the seven game-based DTx, it is found that using VGs as a delivery tool for treatment or prevention interventions in children and adolescents have the potential for therapeutic effects on targeted mental health problems (i.e., attention deficit, anxiety symptoms, emotion regulation and depression). The therapeutic effects of game-based DTx on mental health problems for this age group are at least comparable to that of frequently used treatment interventions (e.g., CBT) or are greater than some of the treatment interventions (e.g., REBE intervention). Moreover, game-based DTx show the persistent therapeutic effect of mental health problems in children and adolescents in at least short term (e.g., 3 months) and the near transfer of cognitive functions.
Acceptability and feasibility
Implementing VGs in DTx that aim to treat or prevent mental health problems in children and adolescents appears to be acceptable and feasible. Among seven game-based DTx, EndeavorRx (42, 44, 57), ATRNTImynd (4), Mightier (66) and SPARX (58, 79) show a higher level of adherence to the interventions without the reports of serious adverse events that are related to the DTx intervention. The acceptability and feasibility of EndeavorRx are found in children with ADHD (42), children with ADHD and ASD (57) and children with SPD and inattentive symptoms (60). Mild adverse events (i.e., the frustration in 3% of children and the headache in 2% of the children) that were reported in EndeavorRx also do not result in the dropout of the study (44). In case of SPARX, although the lower adherence level of SPARX in the sample including transgender adolescents is found (69), the study that examined the feasibility and acceptability of SPARX in adolescents in inpatient settings suggests that SPARX is a feasible intervention for adolescent patients with a greater severity of mental health problems (70). Moreover, the positive evaluation for EndeavorRx, Recogneyes, REThink, and SPARX (e.g., the enjoyment, satisfaction and helpfulness) is reported (11, 45, 57, 58, 63, 66, 74). In case of RECOGNeyes, age influences the evaluation of the intervention (63). While children, who were younger than 12 years, reported that RECOGNeyes were enjoyable and challenging without difficulty, those, who were older than 12 years, reported that RECOGNeyes were not interesting to play (63). Furthermore, unlike the suggested potential of VGs as an attractive and immersive tool to deliver clinical interventions in children and adolescents (33, 34), MindLight and SPARX are found to be rated as interventions that are less relevant with daily lives and less useful than CBT or CBT-based interventions despite the comparable appealing or satisfaction level (8, 76). These results suggest the necessity of further studies to examine factors that could influence the acceptability and feasibility of game-based DTx (e.g., age). Taken together, as EndeavorRx is the firstly approved DTx that delivers the treatment for children and adolescents through VGs (56), more studies for the acceptability and feasibility of game-based DTx should be conducted.
Immediate therapeutic effects
Despite the difference in the focus of DTx on the way to implement VGs, such as the focus on structural characteristics such as storylines [e.g., (37, 42)] and/or the controller to play VGs [e.g., (63, 66)], identified seven game-based DTx are found to be effective in treating or preventing targeted mental health problems in children and adolescents as standalone DTx [i.e., DTx that could treat targeted disorders independently (29, 80)]. It was because not only behavioral improvement in targeted mental health symptoms but also the alterations in symptom-relevant brain regions are found. Consistent with the potential of digital interventions for the cognitive rehabilitation (32), EndeavorRx (60, 71), ATENTIVmynd (72), and REThink (24) show alterations in brain regions that are associated with the behavioral improvement. However, in case of MindLight, although the extent of improvement of anxiety symptoms through MindLight intervention does not significantly differ from the improvement of anxiety through control commercial games (37, 77), MindLight appears to be an effective intervention to improve anxiety symptoms in children by offering a more anxiety-inducing environment where children could learn and practice emotion regulation strategies in response to triggered anxiety (37). The burdens of time investment, one of the reasons for dropping out of CBT program, are also not reported in MindLight (76). Moreover, the therapeutic or preventive effects of game-based DTx on targeted mental health problems are greater in children who report more severe levels of mental health problems than in those with less severe mental health problems (4, 42, 58, 60, 77). That is, children and adolescents, who are more likely to fail in receiving frequently used treatments or to report lower remission rates [e.g., children with SPD (60) and children with ASD in addition to ADHD (57)], show the improvement of targeted mental health problems after playing game-based DTx. These results suggest that DTx offer more personalized intervention environments where children and adolescents could experience the optimal level of challenge for their mental health problems (36, 37), resulting in the successful intervention results for those who show limited therapeutic effects through frequently used treatments (37, 41). Furthermore, the therapeutic effects of EndeavorRx and Mightier are found in children without attention deficits (42, 60) and those whose primary mental health problem is not the difficulty to control anger (66). Taken together, game-based DTx are suggested to show therapeutic or preventive effects on mental health problems by overcoming limitations of frequently used interventions. The DTx are also suggested to have the potential to not only be applied to children with mental health conditions that are relevant with targeted mental health problems but also improve cognitive functions in the general population of children and adolescents.
Although delivering treatment or prevention interventions for targeted mental health problems through VGs in DTx enables more personalized interventions for children and adolescents, personal factors (e.g., gender) seem to have the potential influence on the therapeutic effects of DTx. In SPARX, the extent to which hopelessness decreases and the quality of life improves is different between different groups of children and adolescents. Unlike the improvement in these aspects in children with mild to moderate level of depression (58), adolescents, who were excluded from mainstream education, did not report significant reduction in their hopelessness and improvement in life quality after playing SPARX (79). Moreover, unlike male and female adolescents, transgender adolescents also did not show the improvement in depressive symptoms through SPARX intervention (69). The potential influence of personal factors on the therapeutic effects of DTx could hinder the objective understanding for the effectiveness of game-based DTx in targeted mental health problems or could provide useful information for designing game-based DTx in the future. Thus, further studies should be conducted.
The sustainability of therapeutic effects
Consistent with the potential that the implementation of VGs have for the generalization of learned skills (37), the improvement in targeted mental health problems (i.e., attention deficit, anxiety and depression) in children and adolescents are found to be sustained for more than 10 weeks after the interventions (4, 20, 37, 58, 60, 76, 77, 79). In case of MindLight, children showed greater improvement of anxiety symptoms than those, who received CBT, not at the 3-month follow-up but at the 6-month follow-up (76). That is, game-based DTx appear to have to potential to overcome the limited sustainable therapeutic effects of frequently used treatments outside the intervention period. The sustained therapeutic effects of DTx on mental health problems suggest the generalization of acquired knowledge or skills into daily lives (41) in that not only children but also their parents or clinicians report the improvement of targeted mental health problems (4, 37, 58, 76, 77). Moreover, as receiving additional training sessions of ATENTIVmynd outside the intervention period did not result in further improvement of attention function in children (4), offering the appropriate level of game-based DTx interventions is found to be sufficient to persistently improve targeted mental health problems in children and adolescents. However, the lesser extent of the sustained improvement in anxiety symptoms is found in children who played MindLight and reported the highest amount of gaming time per week (76). As the commercial game with structural characteristics that are similar to MindLight (e.g., controlling the avatar and requiring the overcoming of fear) show the sustained improvement of anxiety symptom at the follow-up (37), it seems that some structural characteristics of commercial VGs could help the improvement of anxiety symptoms or interfere with the sustainability of therapeutic effects of game-based DTx. In order to understand the interference between commercial game playing and game-based DTx, further studies examining the influence of structural characteristics of VGs on therapeutic effects of DTx should be conducted. Furthermore, gaming behavior is identified as one of factors that could influence the maintenance of therapeutic effects of DTx. The change and maintenance of anxiety symptoms through MindLight is found to be predicted by gaming behavior of children (68). While avoidant/safety behaviors predicted increased anxiety symptoms 3 months after the training, engaged gaming behaviors predicted the reduction in anxiety (68). That is, for the better understanding about the sustainability of game-based DTx, further studies should be conducted by investigating the types of engagement behavior and other plausible factors that could influence the sustainability of DTx.
Cognitive improvements
Along with alterations in brain activations related to targeted mental health problems of EndeavorRx, ATENTIVmynd and REThink [e.g., inhibited activation in right frontal brain regions (24), increased MFT activity power (60), and reorganized functional networks (72)], cognitive functions that are relevant with targeted mental health problems (e.g., spatial WM, inhibition and focused attention) are found to show the improvement in children after playing EndeavorRx, ATENTIVmynd, or REThink (11, 20, 42). However, despite the relevance of the focused attention with academic performance, playing ATENTIVmynd does not result in the improvement in academic performance (e.g., reading) (20). That is, consistent with the near transfer of cognitive improvements that was found in VG playing (54), game-based DTx show the near transfer effects for the cognitive improvement. Moreover, although the improvement in spatial WM and inhibition were found in children with and without attention deficits after playing EndeavorRx, those, who reported more severe levels of attention deficit, showed the significant improvement in related cognitive functions along with the greater immediate therapeutic effects of EndeavorRx (42). That is, game-based DTx seem to booster therapeutic effects by improving not only targeted mental health problems but also relevant cognitive functions in children who have more difficulties to learn targeted skills in frequently used treatments. Further studies should be conducted to examine whether the extent of therapeutic effects of DTx in children with more severe mental health problems is modulated by the improvement of relevant cognitive functions.
Limitations
Although both immediate and sustainable therapeutic effects of game-based DTx on targeted mental health problems in children and adolescents are found, four limitations are identified in this review. The first limitation is that the therapeutic effects of DTx are based on relatively small sample size. While more than 100 participants were included in some studies [e.g., (24, 37, 44, 58)], other studies in this review examined the therapeutic effects of DTx based on relatively small sample size. For example, the effectiveness of Mightier in the improvement of emotion regulation in children and adolescents was based on the study included 37 children (66) and one case study (74). As the results of the therapeutic effects of DTx based on small sample size showed the limited generalization of the findings (38), further studies with larger sample sizes should be conducted.
The second limitation is that the motivation of game playing and structural characteristics of VGs are not sufficiently considered. In order to ensure the therapeutic effects of MindLight on anxiety symptoms in children by controlling attention, motivation, behavioral activation and expectations (37, 81), commercial games were used as active control conditions (37, 77). However, game playing itself appears to provide children with the environment where they could train their anxiety reduction-related skills (e.g., resilience and self-efficacy) (35) and it is found that children, who report clinical level of mental health problems, are more likely to play games for the reduction of stress (82). As the motivation of game playing makes it difficult to understand the therapeutic effects of MindLight on anxiety, including additional control groups should be considered in future studies. Moreover, there are inconsistencies in the sustainability of improved anxiety between studies. While children, who played the commercial game, showed sustained improvement of anxiety at the follow-up like those who played MindLight (37), playing commercial games for longer time was found to decrease the extent of sustainability of therapeutic effects of MindLight (76). Thus, further studies that would explore the structural characteristics of VGs that could influence the immediate and/or sustained therapeutic effects of game-based DTx should be conducted.
The third limitation is that self-report measurements that ask children to explicitly indicate their suggestive states (83) are frequently used to examine therapeutic effects of game-based DTx in most studies. The explicit indication of subjective states could be challenging for them in that metacognitive insights are required (83). Although reports are also completed by their parents or clinicians in some studies [e.g., (58, 77)], physiological measurements (e.g., EEG) that are less sensitive to cognitive factors that could bias self-reports could offer more objective information (24) especially in studies where the blinding of conditions is limited. Among included research articles, only four studies [e.g., (24, 60)] are found to include the physiological measurements. As structural and functional alterations in brain regions were influenced by various experiences (e.g., physical activity and cognitive training) (84), investigating the alterations in brain regions after playing game-based DTx would provide valuable and objective information about their effectiveness in addition to behavioral evidence. That is, further studies that include physiological measurements should be conducted.
The last limitation is that the number of studies that examine the extent to which DTx are sustainable in short-term and long-term or show the transfer of cognitive functions is limited. Based on the short-term and long-term follow-ups for the investigation of the sustainability of game-based DTx, they are found to overcome the limited sustainability of frequently used treatments. However, most studies focus on the short-term maintenance of treatment effectiveness and the therapeutic or preventive effects of some DTx are not followed up. As the sustainability of the effectiveness of DTx outside the intervention period is one of important concerns that are reported in mental health interventions (43, 44), more studies that would follow up the therapeutic effects of DTx in long-terms should be conducted. Moreover, greater therapeutic effects of game-based DTx in children with more severe level of mental health problems and the significant improvement in cognitive functions that are related to targeted mental health problems (42) suggest the potential of cognitive remediation through game-based DTx that could result in greater therapeutic effects. Despite the potential of game-based DTx in cognitive remediation (32), only three studies that were included in this review [e.g., (46)] are found to examine the transfer of cognitive functions in game-based DTx. In order to ensure that game-based DTx show sustainable therapeutic effects and have additional effects on VG-related cognitive improvement, studies that would follow up the sustainability of therapeutic effects of DT in longer terms and that would investigate the extent of cognitive improvement after playing game-based DTx should be conducted in the future.
Conclusion
Game-based DTx that aims to treat or prevent targeted mental health problems in children and adolescents are found to be acceptable and feasible. They are also found to show therapeutic or preventive effects on attention function, emotional regulation, anxiety symptom and depression. The therapeutic effects of game-based DTx are sustained in at least short term outside the intervention period. Cognitive functions that are related to the targeted mental health problems also show the improvement. However, there are factors that have the potential to influence the therapeutic effects of DTx or the sustainability of therapeutic effects. Moreover, there are limitations that should be considered in understanding the evidence for the therapeutic effects of DTx. In order to investigate the therapeutic effects of game-based DTx in children and adolescents more objectively, studies that consider the identified factors and limitations should be conducted in the future.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
EC, EY, and MP contributed to data collection, literature review, and the writing of the manuscript. EC was a major contributor in writing the manuscript. MP contributed to the planning, analysis, and supervision of the study. All authors have read and approved the final manuscript.
Funding
This work was supported by the Technology Innovation Program (or Industrial Strategic Technology Development Program) (PC20ONDI0074, AI Driven Global PHR Pediatric Developmental Disability Management/Treatment Platform) funded by the Ministry of Trade, Industry and Energy (MOTIE, Korea) and by National Research Foundation of Korea (NRF) grant funded by the Korean Government (NRF- 2020R1F1A1070581). The funders did not have any role in study design, literature review, decision to publish, and preparation of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA, et al. Annual research review: a meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry. (2015) 56:345–65. doi: 10.1111/jcpp.12381
2. Elsabbagh M, Divan G, Koh Y-J, Kim YS, Kauchali S, Marcin C, et al. Global prevalence of autism and other pervasive developmental disorders. Autism Res. (2012) 5:160–79. doi: 10.1002/aur.239
3. Collishaw S. Annual research review: secular trends in child and adolescent mental health. J Child Psychol Psychiatry. (2015) 56:370–93. doi: 10.1111/jcpp.12372
4. Lim CG, Lee TS, Guan C, Fung DSS, Zhao Y, Teng SSW, et al. A brain-computer interface based attention training program for treating attention deficit hyperactivity disorder. PLoS ONE. (2012) 7:e46692. doi: 10.1371/journal.pone.0046692
5. Kim-Cohen J, Caspi A, Moffitt TE, Harrington H, Milne BJ, Poulton R, et al. Prior juvenile diagnoses in adults with mental disorder: developmental follow-back of a prospective-longitudinal cohort. Arch Gen Psychiatry. (2003) 60:709–17. doi: 10.1001/archpsyc.60.7.709
6. Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: a meta-analytic review. Clin Psychol Rev. (2010) 30:217–37. doi: 10.1016/j.cpr.2009.11.004
7. MCLaughlin KA, Hatzenbuehler ML, Mennin DS, Nolen-Hoesksema S. Emotion dysregulation and adolescent psychopathology: a prospective study. Behav Res Ther. (2011) 49:544–54. doi: 10.1016/j.brat.2011.06.003
8. Poppelaars M, Tak YR, Lichtwarck-Aschoff A, Engels RCME, Lobel A, Merry SN, et al. A randomized controlled trial comparing two cognitive-behavioral programs for adolescent girls with subclinical depression: a school-based program (Op Volle Kracht) and a computerized program (SPARX). Behav Res Therapy. (2016) 80:33–42. doi: 10.1016/j.brat.2016.03.005
9. Birmaher B, Williamson DE, Dahl RE, Axelson DA, Kaufman J, Dorn LD, et al. Clinical presentation and course of depression in youth: does onset in childhood differ from onset in adolescence? J Am Acad Child Adolesc Psychiatry. (2004) 43:63–70. doi: 10.1097/00004583-200401000-00015
10. Costello J, Mustillo S, Erkanli A, Keeeler G, Angold A. Prevalence and development of psychiatric disorders in childhood and adolescence. Arch Gen Psychiatry. (2003) 60:837–44. doi: 10.1001/archpsyc.60.8.837
11. David OA, Cardoş RA, Matu S. Is REThink therapeutic game effective in preventing emotional disorders in children and adolescents? Outcomes of a randomized clinical trial. Eur Child Adolesc Psychiatry. (2019) 28:111–22. doi: 10.1007/s00787-018-1192-2
12. Patulny R, Muir K, Powell S, Flaxman S, Oprea I. Are we reaching them yet? Service access patterns among attendees at the headspace youth mental health initiative. Child Adolesc Ment Health. (2013) 18:95–102. doi: 10.1111/j.1475-3588.2012.00662.x
13. Pliszka SR. Pharmacologic treatment of attention-deficit/hyperactivity disorder: efficacy, safety and mechanisms of action. Neuropsychol Rev. (2007) 17:61–72. doi: 10.1007/s11065-006-9017-3
14. Buitelaar J. Optimising treatment strategies for ADHD in adolescence to minimise ‘lost in transition'to adulthood. Epidemiol Psychiatr Sci. (2017) 26:448–52. doi: 10.1017/S2045796017000154
15. Toomey SL, Sox CM, Rusinak D, Finkelstein JA. Why do children with ADHD discontinue their medication? Clin Pediatr. (2012) 51:763–9. doi: 10.1177/0009922812446744
16. Thapar A, Collishaw S, Pine DS, Thapar AK. Depression in adolescence. Lancet. (2012) 379:1056–67. doi: 10.1016/S0140-6736(11)60871-4
17. Olfson M, Blanco C, Wang S, Laje G, Correll CU. National trends in the mental health care of children, adolescents, and adults by office-based physicians. JAMA Psychiatry. (2014) 71:81–90. doi: 10.1001/jamapsychiatry.2013.3074
18. Coates J, Taylor JA, Sayal K. Parenting interventions for ADHD: a systematic literature review and meta-analysis. J Atten Disord. (2015) 19:831–43. doi: 10.1177/1087054714535952
19. Schnyder N, Sawyer MG, Lawrence D, Panczak R, Burgess P, Harris MG, et al. Barriers to mental health care for Australian children and adolescents in 1998 and 2013–2014. Aus New Zealand J Psychiatry. (2020) 54:1007–19. doi: 10.1177/0004867420919158
20. McDermott AF, Rose M, Norris T, Gordon E. A novel feed-forward modeling system leads to sustained improvements in attention and academic performance. J Atten Disord. (2020) 24:1443–56. doi: 10.1177/1087054715623044
21. Simkin DR, Thatcher RW, Lubar J. Quantitative EEG and neurofeedback in children and adolescents: anxiety disorders, depressive disorders, comorbid addiction and attention-deficit/hyperactivity disorder, and brain injury. Child Adolesc Psychiatr Clin. (2014) 23:427–64. doi: 10.1016/j.chc.2014.03.001
22. Butnik SM. Neurofeedback in adolescents and adults with attention deficit hyperactivity disorder. J Clin Psychol. (2005) 61:621–5. doi: 10.1002/jclp.20124
23. Kola L. Global mental health and COVID-19. Lancet Psychiatry. (2020) 7:655–7. doi: 10.1016/S2215-0366(20)30235-2
24. David OA, Predatu R, Maffei A. REThink online video game for children and adolescents: effects on state anxiety and frontal alpha asymmetry. Int J Cogn Therapy. (2021) 14:388–416. doi: 10.1007/s41811-020-00077-4
25. Hollis C, Morriss R, Martin J, Amani S, Cotton R, DenisM, et al. Technological innovations in mental healthcare: harnessing the digital revolution. Br J Psychiatry. (2015) 206:263–5. doi: 10.1192/bjp.bp.113.142612
26. Dang A, Arora D, Rane P. Role of digital therapeutics and the changing future of healthcare. J Family Med Primary Care. (2020) 9:2207. doi: 10.4103/jfmpc.jfmpc_105_20
27. Bhavnani SP, Narula J, Sengupta PP. Mobile technology and the digitization of healthcare. Eur Heart J. (2016) 37:1428–38. doi: 10.1093/eurheartj/ehv770
28. Dallery J, Kurti A, Erb P. A new frontier: integrating behavioral and digital technology to promote health behavior. Behav Analyst. (2015) 38:19–49. doi: 10.1007/s40614-014-0017-y
29. An S. The Trend of Digital Therapeutics, in BIO ECONOMY BRIEF. KoreaBIO: Korea Bio-Economy Research Center. (2020)
30. Patel NA, Butte AJ. Characteristics and challenges of the clinical pipeline of digital therapeutics. NPJ Digital Med. (2020) 3:159. doi: 10.1038/s41746-020-00370-8
31. Recchia G, Capuano MR, Mistri N, Verna R. Digital therapeutics-what they are, what they will be. Acta Sci Med Sci. (2020) 4:1–9. doi: 10.31080/ASMS.2020.04.0575
32. Abbadessa G, BrigoF, Clerico M, Mercanti SD, Trojsi F, Tedeschi G, et al. Digital therapeutics in neurology. J Neurol. (2022) 269:1209–24. doi: 10.1007/s00415-021-10608-4
33. Craven MP, Groom MJ. Computer games for user engagement in Attention Deficit Hyperactivity Disorder (ADHD) monitoring and therapy. in 2015. Int Conf Interactive Technol Games. (2015). IEEE:34–40. doi: 10.1109/iTAG.2015.9
34. Shah A, Kraemer KR, Won CR, Black S, Hasenbein W. Developing digital intervention games for mental disorders: a review. Games Health J. (2018) 7:213–24. doi: 10.1089/g4h.2017.0150
35. Granic I, Lobel A, Engels RC. The benefits of playing video games. Am Psychol. (2014) 69:66. doi: 10.1037/a0034857
36. Barnes S, Prescott J. Empirical evidence for the outcomes of therapeutic video games for adolescents with anxiety disorders: systematic review. JMIR Serious Games. (2018) 6:e3. doi: 10.2196/games.9530
37. Schoneveld EA, Malmberg M, Lichtwarck-Aschoff A, Verheijen GP, Engels RCME, Granic I, et al. A neurofeedback video game (MindLight) to prevent anxiety in children: a randomized controlled trial. Comp Human Behav. (2016) 63:321–33. doi: 10.1016/j.chb.2016.05.005
38. Cardo R, Predatu R, David O. Development and validation of a cartoon based set of children's facial emotion stimuli for the REThink online therapeutic game. Cog Behav Coach. (2016) 39–43.
39. Fisak BJ, Richard D, Mann A. The prevention of child and adolescent anxiety: a meta-analytic review. Prev Sci. (2011) 12:255–68. doi: 10.1007/s11121-011-0210-0
40. Kazdin AE. Evidence-based treatment research: advances, limitations, and next steps. Am Psychol. (2011) 66:685. doi: 10.1037/a0024975
41. Zayeni D, Raynaud J-P, Revet A. Therapeutic and preventive use of video games in child and adolescent psychiatry: a systematic review. Front Psychiatry. (2020) 11:36. doi: 10.3389/fpsyt.2020.00036
42. Davis NO, Bower J, Kollins SH. Proof-of-concept study of an at-home, engaging, digital intervention for pediatric ADHD. PLoS ONE. (2018) 13:e0189749. doi: 10.1371/journal.pone.0189749
43. Weiss M, Childress A, Mattingly G, Nordbrock E, Kupper RJ, Adjei AL, et al. Relationship between symptomatic and functional improvement and remission in a treatment response to stimulant trial. J Child Adolesc Psychopharmacol. (2018) 28:521–9. doi: 10.1089/cap.2017.0166
44. Kollins SH, DeLoss DJ, Canadas E, Lutz J, Findling PRL, Keefe RL, et al. A novel digital intervention for actively reducing severity of paediatric ADHD (STARS-ADHD): a randomised controlled trial. Lancet Digital Health. (2020) 2:e168–78. doi: 10.1016/S2589-7500(20)30017-0
45. Kahn J, Ducharme P, Rotenberg A, Gonzalez-Heydrich J. “RAGE-control”: a game to build emotional strength. Games Health J. (2013) 2:53–7. doi: 10.1089/g4h.2013.0007
46. Colder Carras M, Van Rooji AJ, Spruijt-Metz D, Kvedar J, Griffiths MD, Carabas Y, et al. Commercial video games as therapy: a new research agenda to unlock the potential of a global pastime. Front Psychiatry. (2018) 8:300. doi: 10.3389/fpsyt.2017.00300
47. Hollis C, Falconer CJ, Martin JL, Whittington C, Stockton S, Glazebrook C, et al. Annual research review: digital health interventions for children and young people with mental health problems–a systematic and meta-review. J Child Psychol Psychiatry Invest. (2017) 58:474–503. doi: 10.1111/jcpp.12663
48. Wiederhold BK. Data-driven digital therapeutics: the path forward. Cyberpsychol Behav Soc Netw. (2021) 24:631–2. doi: 10.1089/cyber.2021.29227.editorial
49. Phirom K, Kamnardsiri T, Sungkarat S. Beneficial effects of interactive physical-cognitive game-based training on fall risk and cognitive performance of older adults. Int J Env Res Public Health. (2020) 17:6079. doi: 10.3390/ijerph17176079
50. Pichierri G, Murer K, de Bruin ED. A cognitive-motor intervention using a dance video game to enhance foot placement accuracy and gait under dual task conditions in older adults: a randomized controlled trial. BMC Geriatr. (2012) 12:1–14. doi: 10.1186/1471-2318-12-74
51. Wang G, Zhao M, Yang F, Cheng LJ, Lau Y. Game-based brain training for improving cognitive function in community-dwelling older adults: a systematic review and meta-regression. Arch Gerontol Geriatr. (2021) 92:104260. doi: 10.1016/j.archger.2020.104260
52. Toril P, Reales JM, Mayas J, Ballesteros S. Video game training enhances visuospatial working memory and episodic memory in older adults. Front Human Neurosci. (2016) 10:206. doi: 10.3389/fnhum.2016.00206
53. Anguera JA, Boccanfuso J, Rintoul JL, Al-Hashimi O, Faraji F, Janowich J, et al. Video game training enhances cognitive control in older adults. Nature. (2013) 501:97–101. doi: 10.1038/nature12486
54. Choi E, Shin S-H, Ryu J-K, Jung K-I, Kim S-Y, Park M-H, et al. Commercial video games and cognitive functions: video game genres and modulating factors of cognitive enhancement. Behav Brain Funct. (2020) 16:1–14. doi: 10.1186/s12993-020-0165-z
55. Oei AC, Patterson MD. Are videogame training gains specific or general? Front Syst Neurosci. (2014) 8:54. doi: 10.3389/fnsys.2014.00054
56. Akili_Interactive_Labs. Akili Announces FDA Clearance of EndeavorRx™ for Children with ADHD, the First Prescription Treatment Delivered Through a Video Game. (2020). Available online at: https://www.akiliinteractive.com/news-collection/akili-announces-endeavortm-attention-treatment-is-now-available-for-children-with-attention-deficit-hyperactivity-disorder-adhd-al3pw (accessed December 22, 2020).
57. Yerys BE, Bertollo JR, Kenworthy L, Dawson G, Marco EJ, Schultz RT, et al. Brief report: pilot study of a novel interactive digital treatment to improve cognitive control in children with autism spectrum disorder and co-occurring ADHD symptoms. J Autism Develop Disord. (2019) 49:1727–37. doi: 10.1007/s10803-018-3856-7
58. Merry SN, Stasiak K, Shepherd M, Frampton C, Fleming T, Lucassen MFG, et al. The effectiveness of SPARX, a computerised self help intervention for adolescents seeking help for depression: randomised controlled non-inferiority trial. BMJ. (2012) 344:e2598. doi: 10.1136/bmj.e2598
59. David OA, Predatu RM, Cardoş RA-I. A pilot study of the REThink online video game applied for coaching emotional understanding in children and adolescents in the therapeutic video game environment: the feeling better resources game. J Evid-Based Psychotherap. (2018) 18:57–67. doi: 10.24193/jebp.2018.1.5
60. Anguera JA, Brandes-Aitken AN, Antovich AD, Rolle CE, Desia SS, Marco EJ, et al. A pilot study to determine the feasibility of enhancing cognitive abilities in children with sensory processing dysfunction. PLoS ONE. (2017) 12:e0172616. doi: 10.1371/journal.pone.0172616
62. ATENTIVHealth. Products that Teach the Exective Fucntion Skills of Attention. Available online at: https://www.atentiv.com/products.html (accessed December 22, 2020).
63. García-Baos A, D'Amelio T, Oliveira I, Collins P, Echevarria C, Zapata LP, et al. Novel interactive eye-tracking game for training attention in children with attention-deficit/hyperactivity disorder. Prim Care Companion CNS Disord. (2019) 21:26348. doi: 10.4088/PCC.19m02428
64. Mightier. Available online at: https://www.mightier.com/science/ (accessed December 27, 2020).
65. Kahn J, Ducharme P, Travers B, Gonzalez-Heydrich J. RAGE control: regulate and gain emotional control. Strat Future Health. (2009) 3:335.
66. Ducharme P, Wharff EA, Kahn J, Hutchinson E, Logan G, Waber D, et al. Augmenting anger control therapy with a videogame requiring emotional control: a pilot study on an inpatient psychiatric unit. Adolesc Psychiatry. (2012) 2:323–32. doi: 10.2174/2210676611202040323
67. Wijnhoven LA, Creemers DHM, Engels RCM, Granic I. The effect of the video game Mindlight on anxiety symptoms in children with an Autism Spectrum Disorder. BMC Psychiatry. (2015) 15:1–9. doi: 10.1186/s12888-015-0522-x
68. Wols A, Lichtwarck-Aschoff A, Schoneveld EA, Granic I. In-game play behaviours during an applied video game for anxiety prevention predict successful intervention outcomes. J Psychopathol Behav Assess. (2018) 40:655–68. doi: 10.1007/s10862-018-9684-4
69. Lucassen MF, Stasiak K, Fleming T, Frampton C, Perry Y, Shepherd M, et al. Computerized cognitive behavioural therapy for gender minority adolescents: Analysis of the real-world implementation of SPARX in New Zealand. Aust New Zealand J Psychiatry. (2021) 55:874–82. doi: 10.1177/0004867420976846
70. Bobier C, Stasiak K, Mountford H, Merry S, Moor S. Examination of the utility of a self-help computerised cognitive behavioural therapy (cCBT) program (SPARX) in an acute adolescent inpatient unit. Adv Mental Health. (2013) 11:286–92. doi: 10.5172/jamh.2013.11.3.286
71. Gallen CL, Anguera JA, Gerdes MR, Simon AJ, Canadas E, Marco EJ, et al. Enhancing neural markers of attention in children with ADHD using a digital therapeutic. PLoS ONE. (2021) 16:e0261981. doi: 10.1371/journal.pone.0261981
72. Qian X, Loo BRY, Castellanos FX, Liu S, Koh HL, Poh XWW, et al. Brain-computer-interface-based intervention re-normalizes brain functional network topology in children with attention deficit/hyperactivity disorder. Transl Psychiatry. (2018) 8:1–11. doi: 10.1038/s41398-018-0213-8
73. David OA, Cardos RA, Matu S. Changes in irrational beliefs are responsible for the efficacy of the REThink therapeutic game in preventing emotional disorders in children and adolescents: mechanisms of change analysis of a randomized clinical trial. Euro Child Adoles Psych. (2019) 28:307–18. doi: 10.1007/s00787-846018-1195-z
74. Ducharme P, Wharff E, Hutchinson E, Kahn J, Logan G, Gonzalez-Heydrich J. Videogame assisted emotional regulation training: an ACT with RAGE-Control case illustration. Clin Soc Work J. (2012) 40:75–84. doi: 10.1007/s10615-011-0363-0
75. Sukhodolsky DG. Randomized trial of anger control training for adolescents with Tourette's syndrome and disruptive behavior. J Am Acad Child Adolesc Psychiatry. (2009) 48:413–21. doi: 10.1097/CHI.0b013e3181985050
76. Schoneveld EA, Lichtwarck-Aschoff A, Granic I. Preventing childhood anxiety disorders: is an applied game as effective as a cognitive behavioral therapy-based program? Prev Sci. (2018) 19:220–32. doi: 10.1007/s11121-017-0843-8
77. Wijnhoven LA, Creemers DHM, Vermulst AA, Lindauer RJL, Otten R, Engels RCME, et al. Effects of the video game ‘Mindlight'on anxiety of children with an autism spectrum disorder: a randomized controlled trial. J Behav Therapy Exp Psychiatry. (2020) 68:101548. doi: 10.1016/j.jbtep.2020.101548
78. Wijnhoven LA, Engels RCME, Onghena P, Otten R, Creemers DHM. The additive effect of CBT elements on the video game ‘mindlight'in decreasing anxiety symptoms of children with autism spectrum disorder. J Autism Develop Disord. (2022) 52:150–68. doi: 10.1007/s10803-021-04927-8
79. Fleming T, Dixon R, Frampton C, Merry S, et al. A pragmatic randomized controlled trial of computerized CBT (SPARX) for symptoms of depression among adolescents excluded from mainstream education. Behav Cogn Psychother. (2012) 40:529–41. doi: 10.1017/S1352465811000695
81. Boot WR, Simons DJ, Stothart C, Stutts C. The pervasive problem with placebos in psychology: why active control groups are not sufficient to rule out placebo effects. Perpect Psychol Sci. (2013) 8:445–54. doi: 10.1177/1745691613491271
82. Ferguson CJ, Olson CK. Friends, fun, frustration and fantasy: child motivations for video game play. Motivat Emot. (2013) 37:154–64. doi: 10.1007/s11031-012-9284-7
83. Deighton J, Croudace T, Fonagy P, Brown J, Patalay P, Wolpert M. Measuring mental health and wellbeing outcomes for children and adolescents to inform practice and policy: a review of child self-report measures. Child Adolesc Psychiatry Mental Health. (2014) 8:1–14. doi: 10.1186/1753-2000-8-14
Keywords: children and adolescents, mental health problem, digital therapeutics, therapeutic effects, transfer, sustainability, video games
Citation: Choi E, Yoon E-H and Park M-H (2022) Game-based digital therapeutics for children and adolescents: Their therapeutic effects on mental health problems, the sustainability of the therapeutic effects and the transfer of cognitive functions. Front. Psychiatry 13:986687. doi: 10.3389/fpsyt.2022.986687
Received: 05 July 2022; Accepted: 20 October 2022;
Published: 29 November 2022.
Edited by:
Natalia Szejko, Medical University of Warsaw, PolandReviewed by:
Michael Feldmeier, UCLA Health System, United StatesCourtney Gallen, University of California, San Francisco, United States
Luigi Lavorgna, University of Campania Luigi Vanvitelli, Italy
Copyright © 2022 Choi, Yoon and Park. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Min-Hyeon Park, bmVvbWlubmllMDBAaGFubWFpbC5uZXQ=