 Virve Marionneau
Virve Marionneau Janne Nikkinen
Janne Nikkinen
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry , 26 October 2022
Sec. Addictive Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.980303
This article is part of the Research Topic Gambling, Stigma, Suicidality, and the Internalization of the ‘Responsible Gambling’ Mantra View all 6 articles
The relationship between gambling and suicides or suicidality has received much research attention in recent years. Review studies have already mapped the quantitative occurrence of suicide attempts, suicides, and self-harm among gamblers, and found a positive association. Related comorbidities and conditions have also been charted in previous reviews. However, there is still a gap in knowledge regarding the actual processes that connect gambling and suicidal behavior. To understand these processes, the current paper conducts a systematic review of qualitative evidence on gambling-related suicides and suicidality. The aim was to identify the role of gambling as well as of confounding factors in suicidality, and what kind of support suicidal individuals have received or would need. We searched for relevant literature in seven scientific databases. We included all studies that presented empirical qualitative evidence on gambling-related suicide, suicidality and/or self-harm (N = 20). The results show two main processes that connect gambling and suicidal behavior: indebtedness and shame. At the same time, suicide is a multifactorial phenomenon, and related to other confounding factors. These include psychiatric conditions, personality traits, and life conditions. In many cases, these appear to emerge as a consequence of gambling. Treatment for suicidality has been effective in some cases, but indebtedness and shame may also function as barriers to help-seeking. We conclude that effective prevention is needed by adapting a more comprehensive public health approach and population-level interventions.
Gambling is a serious public health issue that is connected to a multitude of harms to individuals, communities, and societies. Suicide is among the most severe harmful consequences that have been connected to gambling (1–3). The relationship between gambling and suicide has evoked ample research interests recently, with several reviews published on the topic. Two recent scoping reviews (1, 4) as well as earlier reviews (5, 6) have mapped the quantitative occurrence of suicide attempts, suicides, and other self-harm among gamblers. These have found a positive association between gambling and suicidality. Related comorbidities or conditions have also been systematically mapped in young people (7) and gamblers more generally (2, 4). While knowledge on the prevalence of gambling-related suicides has increased, the existing reviews have also identified a gap in understanding the actual process that connects gambling and suicidality (2, 4, 8). To better understand this connection, the current paper conducts a review of qualitative evidence on gambling-related suicides and suicidality.
Quantitative evidence suggests that suicidality is high among those who gamble at harmful levels. In clinical populations and in treatment services for problem gambling, between 22 and 81 percent of individuals have been found to have suicidal ideations, while between 7 and 30 percent of individuals have had suicide attempts (9–16). In other reporting, approximately 40 percent of help-seekers have been identified as presenting a risk of suicide (17). In community samples, between 17 and 39 percent of those who gamble problematically have been reported to have suicide ideation and between 2 and 57 percent have reported suicide attempts (18–22). Suicidality also appears to increase alongside the severity of gambling-related problems (11, 14, 23, 24).
Suicidality amongst those who gamble at problematic levels is notably higher than in the general population. In Italy, the incidence rate ratio for suicide among those diagnosed with gambling disorder was 93.72 compared to the general population (18). In Sweden, individuals with diagnosed gambling disorder have been shown to have a 1.8-fold increase in mortality and a 15-fold increase in suicide mortality compared to the general population (25). Based on another Swedish population-based study, suicidal attempts were twice as common among those who gamble problematically (6.6 percent) compared to controls (3.3 percent). Suicidal ideations were almost twice as common among those who gamble problematically (21.2 percent) compared to controls (11.2 percent) (26). In a UK population study, 19.2 percent of problem gamblers had thought about suicide in the past year, in comparison to 4.1 percent among those with no signs of problem gambling. In the same study, 4.7 percent of problem gamblers had made a suicide attempt in the past year, in comparison to 0.6 percent of those with no problem gambling (24). Some population groups, such as the young, are particularly vulnerable (3, 27). In the UK, the adjusted odds ratio for attempted suicide for young men with problem gambling was 9.0, and 4.9 for young women with problem gambling (27).
The connection between gambling and suicidality has also been studied using coroner’s files as well as comparative statistics between casino and non-casino communities. Research utilizing coroner’s court files in Hong Kong has shown that approximately 20 percent of cases show evidence of gambling prior to death (28). Many of these have been connected to gambling-related indebtedness (28, 29). In comparative statistical work, Phillips et al. (30) has shown that Las Vegas displays the highest levels of suicide in the United States, for both residents and visitors. In Atlantic City, suicide levels also increased after casinos were opened. However, others have argued that gambling is not the most likely reason for the suicide in most cases even in Las Vegas (31) and that statistically suicide rates do not differ between casino and control communities (32). Any increases in suicidality within casino areas have rather been attributed to tourism (33).
The causal link between gambling and suicide has also been challenged by some authors. It has for example been suggested that suicide may not be directly linked to the severity of gambling, but to related depression, indebtedness, or to the stress and anxiety resulting from gambling (34, 35). Blaszczynski and Farrell (36) have also suggested that research on gambling-related suicide is burdened with problems of definition and confusion between suicidality and non-suicidal self-inflicted injuries and passive thoughts of escape.
The close association between suicidal risk and diagnosed pathological or disordered gambling may at least partly be explained by common underlying risk factors or diagnoses. Personality characteristics, such as impulsivity or poor coping skills (17, 37) or life situations such as trauma (17), loss of family relationships or home (38), family conflict (39), or a family history of addiction (40) have each been connected to the co-occurrence of gambling and suicidality. Furthermore, mood disorders, anxiety, and substance use disorders have been associated with suicidal ideation among diagnosed pathological gamblers (10, 17, 25, 38, 41–44).
In Sweden, a register-based study of individuals diagnosed with disordered gambling found that suicidal behavior was significantly associated with mood disorders (OR 2.65), anxiety disorders (OR 1.78), alcohol use disorder (OR 1.95), and drug use disorder (OR 3.6) (42). Co-occurring substance use has also been shown to distinguish between individuals who had suicide attempts instead of ideation only (22) and to increase the odds of suicidality (42, 45). It must be noted, however, that the co-occurrence of other diagnoses does not conclusively negate the role of gambling in suicidal behavior because the temporal sequencing between for example depression and gambling is also not evident (46). It is also possible that gambling is at the root of mood disorders. Other research also indicates that rates of suicidality are higher among problem and pathological gamblers also when levels of depression or alcohol dependence are controlled (3, 35).
Quantitative approaches to study gambling-related suicidality are important from an epidemiological perspective but leave gaps in our knowledge regarding qualitative insight into the processes that connect gambling and suicidality (44, 47). These gaps are not only characteristic of gambling literature, but a more general trend in suicide research. Research on suicide has for long been dominated by quantitative approaches focusing on risk factors and prevalence estimates. Hjelmeland and Knizek (48) have found that between 2005 and 2008, only three percent of studies published in leading international suicide research journals used a qualitative methodology.
In the current study, we focus on determining how gambling contributes to suicides and suicidality based on a systematic review of qualitative evidence on the relationship between gambling and suicide or suicidality. A qualitative systematic review methodology [e.g., Seers (49)] sheds light on what the role of gambling as well as confounding factors are in suicides and what kind of needs suicidal individuals would have for treatment and support.
We conducted a systematic review of qualitative studies addressing gambling-related suicidality and suicides. Following the qualitative systematic review methodology as described by Seers (49), the aim was to synthesize qualitative evidence and to understand and interpret the “why” and “how” behind the association between gambling and suicidality or suicide. The research question informing the analysis process was how gambling contributes to suicides and suicidality and what is the relationship between the two.
First, we identified relevant studies by conducting a literature search in eight scientific databases: Scopus, PubMed, Ebscohost, ProQuest, Core, OpenAire, Web of Science, and Google Scholar. The search focused on academic, peer-reviewed research articles and books that mainly focused on qualitative research and case study reports on gambling-related suicides and suicidality. This excluded gray literature such as reports as well as anecdotal evidence and quantitative research. The keywords used to conduct the searches were gambling AND suicide AND qualitative OR case study. Articles in any language were included at this stage. We did not limit the search to specific years, but included all references published by May 2022.
We then moved on to study selection. Figure 1 is adapted from the PRISMA guidelines of the inclusion process (50, 51). Our search yielded a total of 1,224 records. Based on the titles of references, we first removed the duplicates and unrelated hits (N = 918). We then screened the remaining 306 records for their relevance based on their abstracts, resulting in the exclusion of a further 259 papers. The inclusion criteria for this study were that the study would present empirical qualitative evidence on gambling-related suicide, suicidality, or self-harm. Due to the scarcity of qualitative research on the topic, we also included studies that were not mainly focused on gambling-related suicides or suicidality but did include empirical evidence on this topic. These included studies focusing more generally on suicidality or on gambling harms. The corresponding exclusion criteria at this stage were: (1) papers that only included quantitative evidence (N = 66); (2) papers that did not include empirical evidence, including reviews and protocols (N = 24); (3) papers written in a language we could not understand (not applicable as all records were in English, French, or Spanish); (4) papers with a topic not related to gambling-related suicide, suicidality, and self-harm (N = 163); (5) papers focusing on the suicidality of concerned significant others of gamblers instead of gamblers (N = 2); and (6) unfound papers (N = 4).
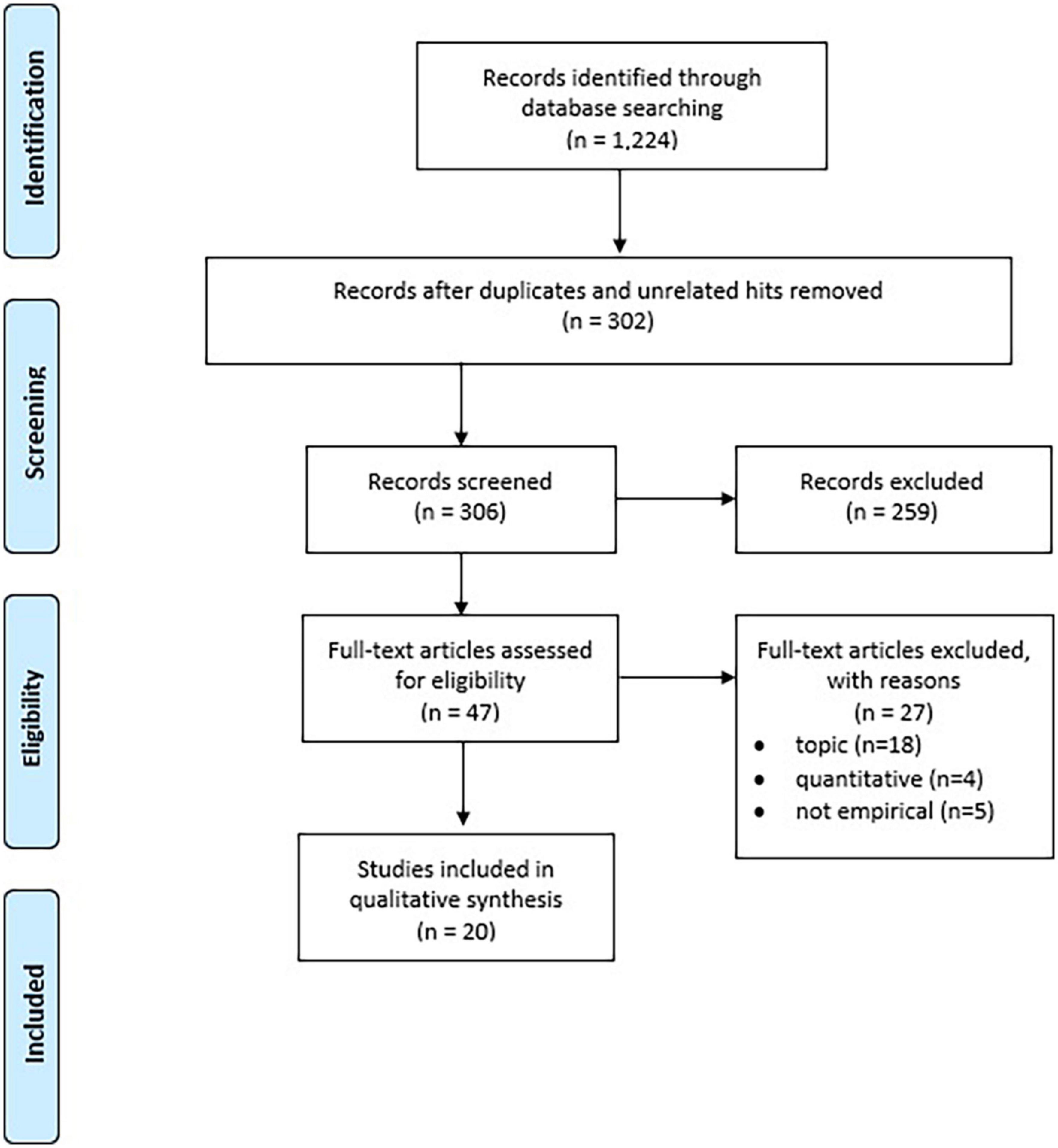
Figure 1. Prisma flow chart.
The remaining 47 papers were then read through to determine whether they qualified based on our inclusion criteria. A further 27 papers were excluded at this stage either because their focus was not on gambling-related suicidality (N = 18), they only included quantitative evidence (N = 4), or they did not include empirical evidence (N = 5). The final sample consists of 20 empirical research papers. The final sample, including reference, data, and funding source, is described in Table 1.
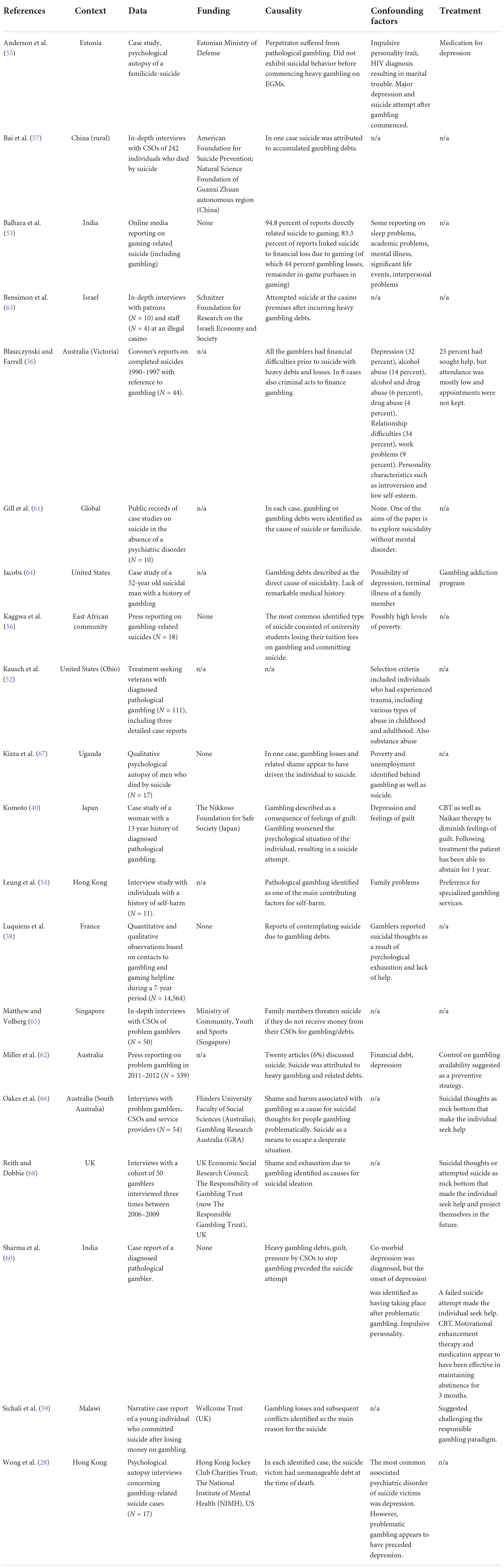
Table 1. Studies included in the review.
The relationship between gambling and suicide or suicidality, as well as how gambling contributes to suicide was charted using three analytical categories: (1) contribution of gambling to suicide or suicidality; (2) confounding factors; (3) support or recovery. We also noted additional observations. To limit the impact of individual bias in interpretation, two separate researchers reviewed the original studies and agreed on the topics and results of the analysis. Ethics approval was not required for the study as it based on existent and publicly available research evidence.
Overall, the quantity of papers included in this study show that there is a scarcity of qualitative research on gambling-related suicides and suicidality. However, geographically this type of research is quite well-spread. The studies included in this review represented a wide geographical distribution, including several contexts in Europe, Asia, Africa, Australia, and North America.
In line with the PRISMA guidelines (51) we also noted the funding sources for all the included studies. In the case of eight (8) studies, the information was not available (n/a). Given that industry funding has been an issue for example in the case of tobacco research, funding declarations would be important.
As per the inclusion criteria, all the included studies (N = 20) discussed how gambling contributed to suicides or suicidality. In the vast majority of these studies (19/20), gambling or gambling-related harms were seen as the main reason for a suicide. In only one study (52), gambling was rather seen as a coping mechanism to deal with other trauma in life that was also identified as the main reason for suicidality. However, the aim of the study in question was to investigate individuals with trauma which may explain the diverging perspective.
In some studies (53–55), gambling itself was described as the generic cause of suicide. Leung et al. (54) interviewed suicidal or self-harming individuals and found that pathological gambling was identified as one of the main contributing factors for self-harm. A case study of an individual in Estonia having committed familicide (55) found that the person had not exhibited suicidal behavior before commencing heavy gambling on electronic gambling machines (EGMs).
Other research identified two main processes through which gambling appears to contribute to suicidality.
The first, and most prevalent, of these processes related to indebtedness and money loss. Gambling-related debt or significant losses of capital were identified as a cause or at least an important contributor to suicide or suicidality in several studies (28, 36, 53, 56–64). This was true of both studies focusing on suicide victims more generally and of studies focusing on gambling specifically. For example, Miller et al. (62) studied press items on pathological gambling in Australia and found that in articles discussing suicide (N = 20), it was attributed to heavy gambling and related debts. Another study using press reporting on gambling and gaming related suicides in India (53) found that 83 percent of all reporting linked suicide to financial loss due to gambling or gaming. A study using press reporting on gambling-related suicides in East Africa (56) similarly found that in the most typical case, the victim was a university student having lost their tuition fees on gambling prior to committing suicide.
Psychological autopsy studies or research using coroner’s reports on completed suicides have similarly found indebtedness and heavy losses prior to death. For example, a study on gambling-related suicides in Hong Kong (28) found that in each identified case, the suicide victim had unmanageable debt at the time of death. Another study on completed suicides in Victoria, Australia (36) found that all the gamblers had heavy debts and losses before committing suicide. Some had also resorted to criminal acts to finance their gambling. Case studies from Malawi (59) and India (60) similarly show that gambling losses and subsequent family conflicts were the main reason behind the described suicide or suicide attempt.
Besides completed suicides, indebtedness is also often reported as a reason for contemplating suicide. As described by Luquiens et al. (58) based on data collected from contacts to a gambling helpline, heavy debts can make the individual feel like suicide is the only solution. If the debts have been incurred due to illegal gambling, this may put further stress on the individual to seek a desperate solution as described by Bensimon et al. (63) in a study of gamblers at an illegal casino in Israel or (64) in a case report of a suicidal individual in the United States. In some cases, suicide can also be used as a threat. Matthew and Volberg (65) interviewed concerned significant others of gamblers in Singapore and found that gambling family members may threaten suicide if they do not receive money from their family members for gambling or gambling-related debts.
The second process by which gambling appears to be connected to suicidality relates to shame. Several studies described how gambling either created or worsened feelings of shame and guilt, eventually leading to suicide or a suicide attempt (40, 60, 66–68). In one case study from Japan (40), the individual was described to have already fostered feelings of shame and guilt before commencing gambling. However, gambling worsened the psychological situation, resulting eventually in a suicide attempt. In other studies, the feelings of shame have rather resulted from excessive gambling or gambling losses (67, 68). One study, based on interviews with gamblers, their significant others, and service providers (66), found that shame associated with gambling was seen as an important contributing cause for suicidal thoughts for people gambling problematically. Suicide then becomes a means to escape the difficult feelings as well as a desperate situation.
In our material, 14 out of the 20 studies included discussion on confounding factors or co-occurring diagnoses that may have also contributed to suicidal behavior. Based on the data, these factors can be divided into three main categories related to psychiatric comorbidities, personality types, and life situation.
Regarding psychiatric comorbidities, depression (or more generic mental disorder) was cited in several studies (28, 36, 40, 53, 55, 60, 62, 64). Alcohol or drug abuse was also cited in some studies (52); Blaszczynski and Farrell (36) found in their study of coroner’s reports in Australia that 32 percent of gambling-related suicide victims had depression. Fourteen percent had alcohol abuse, six percent abused both alcohol and drugs, and four percent abused drugs only. However, in three studies in which the temporal order between depression and gambling was investigated, the analysis found that both depression and suicidality had emerged only after gambling-related problems (28, 55, 60). Luquiens et al. (58) also found that gamblers reported suicidal thoughts as a result of psychological exhaustion and lack of help for gambling problems.
Not all studies found other co-morbid psychiatric diagnoses. For example, a historical collection of case studies presented by Gill et al. (61) showed that gambling-related suicide can and does also occur without mental disorders.
Personality characteristics were mentioned as possible confounding factors in a few studies. Notably, impulsive personality traits were mentioned in case studies of suicide victims (55, 60). Blaszczynski and Farrell (36) also found references to introversion and low self-esteem in Australian coroner’s reporting.
The most often mentioned confounding factors were related to other trouble or hardship in life and life situation. Some of these problems had preceded gambling. Notably studies describing gambling-related suicides in Africa showed that high levels of poverty as well as unemployment had contributed to gambling (56, 59, 67). Kizza et al. (67) describe in their psychological autopsy study of suicides in post-conflict Uganda that many individuals started gambling due to otherwise limited opportunities of income. In other research, family history of suicide, or trauma, such as various types of abuse in childhood and adulthood, were identified as triggering factors to gambling and eventually suicidality (52, 64).
Other life situation related issues appear to have rather stemmed from gambling or emerged after gambling had commenced. These related notably to interpersonal problems and relationship difficulties (36, 53, 54) or to problems at study or work (36, 53). These are typically related to gambling debts and losses [also Blaszczynski and Farrell (36)].
We also noted any mentions of treatment for and recovery from suicidality. However, only eight studies discussed these issues. Based on the observations, the main motivation for individuals to seek help appears to have been “hitting a rock bottom”; Suicidal thoughts or suicide attempts were described as such a low point in several studies (64, 66, 68, 69). For example, Kizza et al. (67) describe a case in which suicidality allowed the individual to start projecting themselves in the future and therefore to finally seek help for their gambling.
The types of treatment received were also discussed in a few of the included studies (36, 40, 54, 55, 69). Although observations are not many, findings suggest that the more comprehensive and specialized the treatment and support approach, the better the results. Notably, a case study from Japan shows that cognitive behavioral therapy (CBT) combined with Naikan therapy to diminish feelings of guilt had resulted in abstinence from gambling for a year. In a case study from India (60), CBT combined with motivational enhancement therapy and medication had been effective in maintaining abstinence from gambling and suicidality for 3 months. Elsewhere, approaches based on only medication (55) or appointments that were often not kept (36) were not effective.
In addition to treatment and support, some studies also discussed how suicidal behavior could be prevented in the first place. For example, Miller et al. (62) noted based on their study on gambling-related problems in Australian press reporting, that there needs to be a better control of gambling availability and better controls on gambling to prevent excessive engagement in gambling and related suicidality. The case study of a suicide in Malawi (59) also concluded that the so-called responsible gambling paradigm puts blame for gambling problems on individuals and functions as a barrier to seek help. Challenging this paradigm would therefore be helpful in preventing individuals from committing suicides due to gambling and related harms.
Based on the results of the current review, gambling can be identified as an important contributor to suicide. The qualitative research evidence summarized in this study indicates that the two main processes that connect gambling to suicide or suicidality are indebtedness and shame. These two processes have also been identified in previous research literature, and gambling has been found to be a significant contributing factor to unmanageable indebtedness as well as to crippling shame (4, 29, 70).
The results of the current study are in line with the interpersonal theory of suicide (71). The theory has found that perceived burdensomeness and lack of belonging contribute to a desire for suicide. Both processes can also be linked to indebtedness and shame: Unmanageable debt and feelings of shame can be seen as hindrances for interpersonal interaction and belongingness.
At the same time, suicide is a complex and multifactorial phenomenon, limiting the determination of direct causality. Other confounding factors are also present for some, consisting notably of psychiatric comorbidities. In most cases, both comorbidities (notably depression) as well as other difficulties (relationship and work problems) appear to have emerged as consequences of gambling. There is also evidence that heavy indebtedness alone without other comorbidities appears to contribute to suicidality (29). This finding somewhat contrasts with evidence suggesting that depression rather than gambling is the causal reason behind suicide (34, 72). Quantitative suicide research on risk factors beyond the gambling field (73); also Hjelmeland and Knizek (48) has shown that a causal link between depression and suicide is typically accepted and implied. However, as argued by Hjelmeland and Knizek (48) this may also be due to methodological issues, lack of qualitative evidence, and publication bias. Furthermore, even in cases where a direct causality cannot be determined, it is fair to say that gambling has negatively affected the individual.
Treatment and support appear to have been effective in some cases, but there are also important barriers to seek and receive treatment. Resources and commitment to appointments may be one [cf. Blaszczynski and Farrell (36) and also Séguin et al. (74)], suggesting that additional engagement in treatment is necessary. At the same time, the processes of shame and indebtedness may also work as barriers. As also noted by Hing et al. (70) deep feelings of shame and self-stigma result in secrecy and unwillingness to seek help. Similarly, Dufour and Roy (5) have found that individuals may wish to conceal the extent of their indebtedness from others, and therefore do not seek help. Making the situation worse, particularly in the case of indebtedness, continued gambling is not only the cause but also the perceived solution to financial problems (5). The actual processes that connect gambling to suicide and suicidality therefore also appear to function as barriers to helping these individuals.
The only way to effectively prevent extreme gambling-related harms, such as suicidality, and the processes of indebtedness and shame that connect to it, appears to be shifting perspective in regulation toward a more comprehensive public health approach and prevention at a population level to relieve the blame on individuals. Gambling has become widely accessible across the world. Growing gambling markets in the global south, such as Africa (75), are also visible in the increasing attention that has been paid to gambling-related suicides in these contexts in recent years. In the more mature gambling markets of the global north, issues such as the responsible gambling mantra has been argued to increase shame for those who are supposedly irresponsible with their gambling (76). The normalization of gambling, easy accessibility, and individual responsibility rather than controls on industry actors increase total consumption on gambling and therefore also total harms. These harms are not limited to problem gambling prevalence, but to a wide array of intertwined harms to individuals, communities, and societies (77, 78).
The current study has been limited to a restricted sample of studies, due to the overall lack in qualitative evidence on gambling-related suicides and suicidality. The complexity of the suicide phenomenon also limits the possibilities to draw linear cause and effect conclusions. While we have identified two key processes that connect gambling and suicide, there is still need for more research to ascertain these processes and to investigate other possible “pathways.” Notably, there is need for more research on how individuals understand the meaning of suicide, and how suicidality can be placed within a person’s lived experience (48). For example, socio-cultural contexts and gender differences may impact lived experience and risk for suicidal behavior (47, 48). Due to the limited number of studies analyzed in the current review, these types of issues could not be systematically analyzed but should be addressed in future studies.
To prevent gambling-related suicidality in the future, a public health approach is needed to shift the blame for gambling-related harms and indebtedness from often vulnerable individuals to the societal and commercial conditions (79–81). At the same time, it is crucial to target the speed of gambling products, advertisement of gambling particularly to the young (82), but also put an end to easy and fast access to credit that enables debt-driven gambling.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
VM conducted the analysis and wrote the first draft of the manuscript. Both authors were in charge of data collection and the conception of this manuscript, revised the draft, and gave their final approval.
This study had been funded via a co-operation contract between the University of Helsinki and the Finnish Institute for Health and Welfare based of the Finnish Lotteries Act (1048/2011, section 52). The section 52 of the Act stated that harms caused by gambling shall be monitored and researched, and that the Ministry of Social Affairs and Health held the overall responsibility for these tasks. The section 52 funding scheme served to protect research integrity and detachment from the gambling monopoly company Veikkaus, which was billed for the monitoring and research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gray H, Edson T, Nelson S, Grossman A, LaPlante D. Association between gambling and self-harm: a scoping review. Addict Res Theory. (2021) 29:183–95.
2. Giovanni M, Fabiola S, Federica F, Mariangela C, Nicola P, Ilaria T, et al. Gambling disorder and suicide: an overview of the associated co-morbidity and clinical characteristics. Int J High Risk Behav Addict. (2017) 3:e30827. doi: 10.5812/ijhrba.30827
3. Nower L, Gupta R, Blaszczynski A, Derevensky J. Suicidality and depression among youth gamblers: a preliminary examination of three studies. Int Gambl Stud. (2004) 4:69–80. doi: 10.1080/1445979042000224412
4. Andreeva M, Audette-Chapdelaine S, Brodeur M. Gambling-related completed suicides: a scoping review. Addict Res Theory. (2022):1–12. doi: 10.1080/16066359.2022.2055001
5. Dufour M, Roy É. La crise chez les joueurs de jeux de hasard et d’argent: au-delà de l’appel de détresse, les services novateurs qui y répondent. Drogues Santé Soc. (2009) 8:109–39. doi: 10.7202/044473ar
6. Pfuhlmann B, Schmidtke A. Pathological gambling and suicidal behavior. Arch Suicide Res. (2002) 6:257–67. doi: 10.1080/13811110214145
7. Gifuni A, Perret L, Lacourse E, Geoffroy M, Mbekou V, Jollant F, et al. Decision-making and cognitive control in adolescent suicidal behaviors: a qualitative systematic review of the literature. Eur Child Adolesc Psychiatry. (2021) 12:1839–55. doi: 10.1007/s00787-020-01550-3
8. John A, Wardle H, McManus S, Dymond S. Scoping Current Evidence and Evidence-Gaps in Research on Gambling-Related Suicide. Report 3 Prepared for GambleAware. (2019). Birmingham: Gambling Commission.
9. Valenciano-Mendoza E, Fernández-Aranda F, Granero R, Gómez-Peña M, Moragas L, del Pino-Gutierrez A, et al. Suicidal behavior in patients with gambling disorder and their response to psychological treatment: the roles of gender and gambling preference. J Psych Res. (2021) 143:317–26. doi: 10.1016/j.jpsychires.2021.09.027
10. Roberts K, Smith N, Bowden-Jones H, Cheeta S. Gambling disorder and suicidality within the UK: an analysis investigating mental health and gambling severity as risk factors to suicidality. Int Gambl Stud. (2017) 17:51–64. doi: 10.1080/14459795.2016.1257648
11. Ronzitti S, Soldini E, Smith N, Potenza M, Clerici M, Bowden-Jones H. Current suicidal ideation in treatment-seeking individuals in the United Kingdom with gambling problems. Addict Behav. (2017) 74:33–40. doi: 10.1016/j.addbeh.2017.05.032
12. Wong P, Kwok N, Tang J, Blaszczynski A, Tse S. Suicidal ideation and familicidal-suicidal ideation among individuals presenting to problem gambling services. Crisis. (2014) 35:219–32. doi: 10.1027/0227-5910/a000256
13. Battersby M, Tolchard B, Scurrah M, Thomas L. Suicide ideation and behaviour in people with pathological gambling attending a treatment service. Int J Mental Health Addict. (2006) 4:233–46. doi: 10.1007/s11469-006-9022-z
14. Ledgerwood D, Steinberg M, Wu R, Potenza M. Self-reported gambling-related suicidality among gambling helpline callers. Psychol Addict Behav. (2005) 19:175. doi: 10.1037/0893-164X.19.2.175
15. Ledgerwood D, Petry N. Gambling and suicidality in treatment-seeking pathological gamblers. J Nerv Ment Dis. (2004) 192:711–4. doi: 10.1097/01.nmd.0000142021.71880.ce
16. Petry N, Kiluk B. Suicidal ideation and suicide attempts in treatment-seeking pathological gamblers. J Nerv Ment Dis. (2002) 190:462. doi: 10.1097/00005053-200207000-00007
17. Guillou-Landreat M, Guilleux A, Sauvaget A, Brisson L, Leboucher J, Remaud M, et al. Factors associated with suicidal risk among a French cohort of problem gamblers seeking treatment. Psychiatry Res. (2016) 240:11–8. doi: 10.1016/j.psychres.2016.04.008
18. Pavarin R, Fabbri C, Fioritti A, Marani S, De Ronchi D. Gambling disorder in an Italian population: risk of suicide attempts and associated demographic-clinical factors using electronic health records. J Gambl Stud. (2021):1–14. doi: 10.1007/s10899-021-10088-1
19. Darbeda S, Aubin H, Lejoyeux M, Luquiens A. Characteristics of gamblers who use the French national problem gambling helpline and real-time chat facility: longitudinal observational study. JMIR Form Res. (2020) 4:e13388. doi: 10.2196/13388
20. Hubert P, Griffiths M. A comparison of online versus offline gambling harm in Portuguese pathological gamblers: an empirical study. Int J Ment Health Addict. (2018) 16:1219–37. doi: 10.1007/s11469-017-9846-8
21. Haydock M, Cowlishaw S, Harvey C, Castle D. Prevalence and correlates of problem gambling in people with psychotic disorders. Compr Psychiatry. (2015) 58:122–9. doi: 10.1016/j.comppsych.2015.01.003
22. Hodgins D, Mansley C, Thygesen K. Risk factors for suicide ideation and attempts among pathological gamblers. Am J Addict. (2006) 15:303–10. doi: 10.1080/10550490600754366
23. Valenciano-Mendoza E, Fernández-Aranda F, Granero R, Gómez-Peña M, Moragas L, Mora-Maltas B, et al. Prevalence of suicidal behavior and associated clinical correlates in patients with behavioral addictions. Int J Environ Res Public Health. (2021) 18:11085. doi: 10.3390/ijerph182111085
24. Wardle H, Dymond S, John A, McManus S. Problem Gambling and Suicidal Thoughts, Suicide Attempts and Non-Suicidal Self-Harm in England: Evidence from the Adult Psychiatric Morbidity Survey 2007. Birmingham: Gambling Commission (2019).
25. Karlsson A, Håkansson A. Gambling disorder, increased mortality, suicidality, and associated comorbidity: a longitudinal nationwide register study. J Behav Addict. (2018) 7:1091–9. doi: 10.1556/2006.7.2018.112
26. Sundqvist K, Wennberg P. The association between problem gambling and suicidal ideations and attempts: a case control study in the General Swedish population. J Gambl Stud. (2021) 2:319–31. doi: 10.1007/s10899-020-09996-5
27. Wardle H, McManus S. Suicidality and gambling among young adults in Great Britain: results from a cross-sectional online survey. Lancet Public Health. (2021) 6:e39–49. doi: 10.1016/S2468-2667(20)30232-2
28. Wong P, Cheung D, Conner K, Conwell Y, Yip P. Gambling and completed suicide in Hong Kong: a review of coroner court files. Prim Care Companion CNS Disord. (2010) 12:27298. doi: 10.4088/PCC.09m00932blu
29. Yip P, Yang K, Ip B, Law Y, Watson R. Financial debt and suicide in Hong Kong SAR 1. J Appl Soc Psychol. (2007) 37:2788–99. doi: 10.1111/j.1559-1816.2007.00281.x
30. Phillips D, Welty W, Smith M. Elevated suicide levels associated with legalized gambling. Suicide Life Threat Behav. (1997) 27:373–8.
31. Marfels C. Gambling and suicide: evidence from the Las Vegas market. Gaming Law Rev. (2001) 5:33–41. doi: 10.1089/109218801750286822
32. Nichols M, Stitt B, Giacopassi D. Changes in suicide and divorce in new casino jurisdictions. J Gambl Stud. (2004) 20:391–404. doi: 10.1007/s10899-004-4581-z
33. Chew K, Mc Cleary R, Merrill V, Napolitano C. Visitor suicide risk in casino resort areas. Popul Res Policy Rev. (2000) 19:551–70. doi: 10.1023/A:1010696906473
34. Maccallum F, Blaszczynski A. Pathological gambling and suicidality: an analysis of severity and lethality. Suicide Life Threat Behav. (2003) 33:88–98. doi: 10.1521/suli.33.1.88.22781
35. Newman S, Thompson A. A population-based study of the association between pathological gambling and attempted suicide. Suicide Life Threat Behav. (2003) 33:80–7. doi: 10.1521/suli.33.1.80.22785
36. Blaszczynski A, Farrell E. A case series of 44 completed gambling-related suicides. J Gambl Stud. (1998) 14:93–109. doi: 10.1023/A:1023016224147
37. Blaszczynski A, Nower L. A pathways model of problem and pathological gambling. Addiction. (2002) 97:487–99. doi: 10.1046/j.1360-0443.2002.00015.x
38. Sharman S, Murphy R, Turner J, Roberts A. Predictors of suicide attempts in male UK gamblers seeking residential treatment. Addict Behav. (2022) 126:107171. doi: 10.1016/j.addbeh.2021.107171
39. Carr M, Ellis J, Ledgerwood D. Suicidality among gambling helpline callers: a consideration of the role of financial stress and conflict. Am J Addict. (2018) 27:531–7. doi: 10.1111/ajad.12787
40. Komoto Y. Factors associated with suicide and bankruptcy in Japanese pathological gamblers. Int J Ment Health Addict. (2014) 12:600–6. doi: 10.1007/s11469-014-9492-3
41. Karlsson A, Hedén O, Hansson H, Sandgren J, Håkansson A. Psychiatric comorbidity and economic hardship as risk factors for intentional self-harm in gambling disorder—a nationwide register study. Front Psychiatry. (2021) 12:688285. doi: 10.3389/fpsyt.2021.688285
42. Håkansson A, Karlsson A. Suicide attempt in patients with gambling disorder—associations with comorbidity including substance use disorders. Front Psychiatry. (2020) 11:593533. doi: 10.3389/fpsyt.2020.593533
43. Stein G, Pretorius A, Stein D, Sinclair H. The association between pathological gambling and suicidality in treatment-seeking pathological gamblers in South Africa. Ann Clin Psychiatry. (2016) 28:43–50.
44. Bischof A, Meyer C, Bischof G, John U, Wurst F, Thon N, et al. Suicidal events among pathological gamblers: the role of comorbidity of axis I and axis II disorders. Psychiatry Res. (2005) 225:413–9. doi: 10.1016/j.psychres.2014.11.074
45. Kim H, Salmon M, Wohl M, Young M. A dangerous cocktail: alcohol consumption increases suicidal ideations among problem gamblers in the general population. Addict Behav. (2016) 55:50–5. doi: 10.1016/j.addbeh.2015.12.017
46. Holdsworth L, Haw J, Hing N. The temporal sequencing of problem gambling and comorbid disorders. Int J Ment Health Addict. (2012) 10:197–209. doi: 10.1007/s11469-011-9324-7
47. Slutske W, Davis C, Lynskey M, Heath A, Martin N. An epidemiologic, longitudinal, and discordant-twin study of the association between gambling disorder and suicidal behaviors. Clin Psychol Sci. (2022) 10:901–19. doi: 10.1177/21677026211062599
48. Hjelmeland H, Knizek B. Qualitative evidence in suicide: findings from qualitative psychological autopsy studies. In: K Olson, R Young, I Schultz editors. Handbook of Qualitative Health Research for Evidence-Based Practice. New York, NY: Springer (2016). p. 355–71. doi: 10.1007/978-1-4939-2920-7_21
49. Seers K. Qualitative systematic reviews: their importance for our understanding of research relevant to pain. Br J Pain. (2015) 9:36–40. doi: 10.1177/2049463714549777
50. Moher D, Liberati A, Tetzlaff J, Altman DG, Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
51. Page M, McKenzie J, Bossuyt P, Boutron I, Hoffmann T, Mulrow C, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:89.
52. Kausch O, Rugle L, Rowland D. Lifetime histories of trauma among pathological gamblers. Am J Addict. (2006) 15:35–43. doi: 10.1080/10550490500419045
53. Balhara Y, Singh S, Yadav Z. Media reporting on deaths due to suicide attributed to gaming in digital news: a case of misrepresentation and missed opportunities. Asian J Psychiatr. (2022) 68:102955. doi: 10.1016/j.ajp.2021.102955
54. Leung M, Chow C, Ip P, Yip S. Self-harm attempters’ perception of community services and its implication on service provision. Int J Nurs Sci. (2019) 6:50–7. doi: 10.1016/j.ijnss.2018.12.003
55. Anderson A, Sisask M, Värnik A. Familicide and suicide in a case of gambling dependence. J Forens Psychiatry Psychol. (2011) 22:156–68. doi: 10.1080/14789949.2010.518244
56. Kaggwa M, Mamum M, Najjuka S, Muwanguzi M, Kule M, Nkola R, et al. Gambling-related suicide in East African community countries: evidence from press media reports. BMC Public Health. (2022) 22:158. doi: 10.1186/s12889-021-12306-2
57. Bai X, Zhou L, Mo Q, Jia C, Ma Z. Understanding the reasons for suicide among older adults in rural china using in-depth interviews. Crisis. (2021) 18:1–7. doi: 10.1027/0227-5910/a000799
58. Luquiens A, von Hammerstein C, Benyamina A, Perney P. Burden and help-seeking behaviors linked to problem gambling and gaming: observational quantitative and qualitative analysis. JMIR Ment Health. (2021) 8:e26521. doi: 10.2196/26521
59. Sichali J, Dube A, Kachiwanda L, Wardle H, Crampin A, Bunn C. Case Report: a gambling-related suicide in rural Malawi. Wellcome Open Res. (2021) 6:308. doi: 10.12688/wellcomeopenres.17333.1
60. Sharma N, Gupta A, Jane T. A case of pathological gambling. Indian J Psychiatry. (2019) 61:316. doi: 10.4103/psychiatry.IndianJPsychiatry_333_18
61. Gill D, Ahmadi J, Pridmore S. Suicide and gambling on the public record. Malaysian J Psychiatry. (2014) 23:81–8.
62. Miller H, Thomas S, Robinson P, Daube M. How the causes, consequences and solutions for problem gambling are reported in Australian newspapers: a qualitative content analysis. Aust N Z J Public Health. (2014) 38:529–35. doi: 10.1111/1753-6405.12251
63. Bensimon M, Baruch A, Ronel N. The experience of gambling in an illegal casino: the gambling spin process. Eur J Criminol. (2013) 10:3–21. doi: 10.1177/1477370812455124
64. Jacobs D. A 52-year-old suicidal man. J Am Med Assoc. (2000) 20:2693–9. doi: 10.1001/jama.283.20.2693
65. Matthew M, Volberg R. Impact of problem gambling on financial, emotional and social well-being of Singaporean families. Int Gambl Stud. (2013) 13:127–40. doi: 10.1080/14459795.2012.731422
66. Oakes J, Pols R, Lawn S. The ‘merry-go-round’of habitual relapse: a qualitative study of relapse in electronic gaming machine problem gambling. Int J Environ Res Public Health. (2019) 16:2858. doi: 10.3390/ijerph16162858
67. Kizza D, Knizek B, Kinyanda E, Hjelmeland H. An escape from agony: a qualitative psychological autopsy study of women’s suicide in a post-conflict northern Uganda. Int J Qual Stud Health Well. (2012) 7:18463. doi: 10.3402/qhw.v7i0.18463
68. Reith G, Dobbie F. Lost in the game: narratives of addiction and identity in recovery from problem gambling. Addict Res Theory. (2012) 20:511–21. doi: 10.3109/16066359.2012.672599
69. Sharman S, Murphy R, Turner J, Roberts A. Trends and patterns in UK treatment seeking gamblers: 2000–2015. Addict Behav. (2019) 89:51–6. doi: 10.1016/j.addbeh.2018.09.009
70. Hing N, Nuske E, Gainsbury S, Russell A. Perceived stigma and self-stigma of problem gambling: perspectives of people with gambling problems. Int Gambl Stud. (2016) 16:31–48. doi: 10.1080/14459795.2015.1092566
71. Chu C, Buchman-Schmitt JM, Stanley IH, Hom MA, Tucker RP, Hagan CR, et al. The interpersonal theory of suicide: a systematic review and meta-analysis of a decade of cross-national research. Psychol Bull. (2017) 12:1313–45. doi: 10.1037/bul0000123
72. Newman S, Thompson A. The association between pathological gambling and attempted suicide: findings from a national survey in Canada. Can J Psychiatry. (2007) 52:605–12. doi: 10.1177/070674370705200909
73. Cavanagh J, Carson A, Sharpe M, Lawrie S. Psychological autopsy studies of suicide: systematic review. Psychol Med. (2003) 33:395–405. doi: 10.1017/S0033291702006943
74. Séguin M, Boyer R, Lesage A, McGirr A, Suissa A, Tousignant M, et al. Suicide and gambling: psychopathology and treatment-seeking. Psychol Addict Behav. (2010) 24:541. doi: 10.1037/a0019041
75. Reith G, Wardle H, Gilmore I. Gambling harm: a global problem requiring global solutions. Lancet. (2019) 394:1212–4. doi: 10.1016/S0140-6736(19)31991-9
76. Livingstone C, Rintoul A. Gambling-related suicidality: stigma, shame, and neglect. Lancet Public Health. (2021) 6:E4–5. doi: 10.1016/S2468-2667(20)30257-7
77. Langham E, Thorne H, Browne M, Donaldson P, Rose J, Rockloff M. Understanding gambling related harm: a proposed definition, conceptual framework, and taxonomy of harms. BMC Public Health. (2016) 16:80. doi: 10.1186/s12889-016-2747-0
79. van Schalkwyk M, Petticrew M, Cassidy R, Adams P, McKee M, Reynolds J, et al. A public health approach to gambling regulation: countering powerful influences. Lancet Public Health. (2021) 8:E614–9. doi: 10.1016/S2468-2667(21)00098-0
80. Miller H, Thomas S. The problem with ‘responsible gambling’: impact of government and industry discourses on feelings felt and enacted stigma in people who experience problems with gambling. Addict Res Theory. (2018) 2:85–92. doi: 10.1080/16066359.2017.1332182
81. Wardle H, Reith G, Langham E, Rogers R. Gambling and public health: we need policy action to prevent harm. Br Med J. (2019) 365:l1807.
Keywords: gambling, suicide, qualitative, review, indebtedness, shame
Citation: Marionneau V and Nikkinen J (2022) Gambling-related suicides and suicidality: A systematic review of qualitative evidence. Front. Psychiatry 13:980303. doi: 10.3389/fpsyt.2022.980303
Received: 28 June 2022; Accepted: 07 October 2022;
Published: 26 October 2022.
Edited by:
Saeed Ahmed, Rutland Regional Medical Center, United StatesReviewed by:
Hilario Blasco-Fontecilla, Autonomous University of Madrid, SpainCopyright © 2022 Marionneau and Nikkinen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Virve Marionneau, dmlydmUubWFyaW9ubmVhdUBoZWxzaW5raS5maQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.