 Navdeep Kaur1†
Navdeep Kaur1† Gabriel Bastien1,2†
Gabriel Bastien1,2† Lea Gagnon1†Johann Graham2,3Violaine Mongeau-Pérusse2†Hamzah Bakouni1†
Lea Gagnon1†Johann Graham2,3Violaine Mongeau-Pérusse2†Hamzah Bakouni1† Florence Morissette2†Camille Theriault2Benedikt Fischer4,5,6,7†
Florence Morissette2†Camille Theriault2Benedikt Fischer4,5,6,7† Didier Jutras-Aswad1,2*†
Didier Jutras-Aswad1,2*†- 1Centre de Recherche du Centre Hospitalier de l’Université de Montréal (CRCHUM), Montréal, QC, Canada
- 2Department of Psychiatry and Addiction, Faculty of Medicine, Université de Montréal, Montréal, QC, Canada
- 3Faculty of Medicine, Université Laval, Quebec City, QC, Canada
- 4School of Population Health, Faculty of Medical and Health Sciences, University of Auckland, Auckland, New Zealand
- 5Department of Psychiatry, University of Toronto, Toronto, ON, Canada
- 6Centre for Applied Research in Mental Health and Addiction, Faculty of Health Sciences, Simon Fraser University, Vancouver, BC, Canada
- 7Department of Psychiatry, Universidade Federal de São Paulo (UNIFESP), São Paulo, Brazil
Introduction: Evidence supporting associations between cannabis use and many health outcomes is growing, however it remains unclear how such associations vary across the lifespan. We therefore aim to answer the following questions: (1) Are the risks of cannabis’s adverse effects on mental health and addiction-related outcomes different in adolescents than in adults? (2) What are the relationships between these cannabis’s adverse effects and (a) an individual’s age at first cannabis use, (b) age at assessment, and (c) duration of cannabis use?
Methods: We searched Medline, Embase, CINAHL, and PsychINFO from inception to 18 October 2021. Two reviewers independently screened studies and descriptively synthesized results.
Results: We included 140 studies. Cannabis effects on mental health and addiction-related outcomes were worse in adolescents, early cannabis initiators and cannabis users who consumed for longest periods. Evidence of worse long-term adverse effects in adolescents was substantial for psychosis, cannabis, and nicotine use disorders; mixed for depression, suicidality, other substance use and disorders; and limited for anxiety. Additionally, acute cannabis exposure had the opposite trend with adults more often reporting adverse effects than adolescents.
Conclusion: The available evidence suggests that cannabis use should be delayed as late as possible in adulthood and shortened in duration across the lifespan to decrease the risk of negative outcomes, while emphasizing the need for adapted harm reduction approaches. This scoping review provides evidence on the role of age and duration of exposure as determinants of cannabis-related adverse effects, which may inform prevention and harm reduction strategies.
Systematic review registration: https://doi.org/10.17605/OSF.IO/BYG72
Introduction
Around the world, almost 200 million people consumed cannabis in the past year, making it the most used psychoactive substance after nicotine and alcohol (1–3). Cannabis use prevalence is particularly high among adolescents and young adults (3). Consumed for recreational purposes and its therapeutic properties, cannabis can also adversely impact users’ health (4, 5). Cannabis exposure has been associated with a myriad of physical, mental, and psychosocial adverse health outcomes affecting all age groups (5). Notably, early cannabis initiation while the brain is still developing has been hypothesized to distinctly predispose adolescents to detrimental effects and increase risks specifically for mental health, cognitive and addiction problems (6). For example, adolescent cannabis use has been associated with psychiatric disorders such as schizophrenia (7–12), depression, and suicidal behavior (13). The probability for cannabis users to transition to cannabis use disorder (CUD) range between 9 and 27%, depending on the sample population, diagnosis definition and age of exposure onset (14, 15). Some evidence also suggests that early cannabis consumption may lead to the use of other substances (16, 17).
With the prevalence of cannabis use on the rise in many contexts and some jurisdictions liberalizing controls (including legalization) for recreational use (18), the establishment of a strong evidence base is needed to guide best public health strategies, harm reduction interventions, and policies. Existing initiatives have traditionally employed a precautionary approach assuming higher risks of harms in youth than in adults, thus suggesting broadly to avoid early and generally delay exposure to cannabis. While the body of evidence on associations between cannabis use and health outcomes is progressing, however, most of the existing literature reviews on cannabis harms on mental health and addiction in humans focused on a narrow set of mental health outcomes (7, 19) or on specific age groups (20). Consequently, it remains unclear how such associations may vary across the lifespan and whether they do similarly for all outcomes. To map the existing evidence as well as to identify any knowledge gap, we conducted a scoping review to answer these research questions (RQs): (1) Are the risks of cannabis’s adverse effects on mental health and addiction-related outcomes different between adolescents and adults? (2) What are the relationships between these cannabis’s adverse effects and (a) the user’s age at first cannabis use (b) participant’s age at assessment, and (c) duration of cannabis use?
Methods
We followed the Joanna Briggs Institute (21) scoping review methodology and the Preferred Reporting Items for Systematic Reviews and Meta-Analyzes extension for Scoping Reviews (PRISMA-ScR) guidelines (22) to prepare our prospectively published protocol (23).
Eligibility criteria
Human studies were included if they: (i) reported adverse mental health or addiction outcome(s) related to cannabis use, (ii) reported relationship(s) between cannabis’s adverse mental health or addiction outcome(s) and cannabis use onset or duration, (iii) included adolescents (<18 years old) and adults (≥18 years old), (iv) were published in peer-reviewed journals, and (v) were available in English, French, or Spanish. Editorials, letters, research protocols, and commentaries were excluded. To retrieve a full text that could not be obtained through institutional holdings, a librarian, the author, or the journal editor was contacted.
Data sources and search strategy
We searched for publications in three main electronic databases (MEDLINE, Embase, and PsychINFO) from inception to 27 October 2020. However, due to unforeseen circumstances caused by the COVID-19 pandemic, our scoping review got bit delayed therefore, to ensure inclusion of latest publications, we updated our search strategy on 18 October 2021. We consulted a specialized librarian to develop and execute a specific search strategy for each database. The search concepts were: (i) cannabis, (ii) adolescents and adults OR age of onset or initiation, and (iii) adverse or negative effects OR mental health OR addiction. Supplementary Appendix 1 presents our first and updated search strategies for Medline that were adapted for other databases. Furthermore, we manually searched through the reference lists of all identified records for retrieving additional relevant studies.
Study selection process
All citations were imported into the EndNote X9 software. A screening form was developed a priori. Distiller SR® was used for data extraction and study selection. We followed a three-step study selection process. First, all duplicate publications were removed. Second, two reviewers (GB and VM, JG and CT/NK, FM and LG, NK, and HB) screened titles and abstracts with the screening form. Third, full texts meeting the inclusion criteria were reviewed and relevant studies were selected. Two independent reviewers (GB and VM, FM/JG and LG, NK, and HB) screened and extracted data from the full texts and a third reviewer (DJ-A/NK) resolved discrepancies between reviewers.
Data charting and synthesis
From each study, the following information was extracted: first author’s name, publication year, country of study, study design, sample size, and cannabis use definition and findings. The main outcomes of interest were mental health, addiction and addictive behaviors related to cannabis use among adults and adolescents, relationships between cannabis’s adverse mental health and addiction effects AND (a) participant’s age at first cannabis use OR (b) participant’s age at assessment OR (c) duration of cannabis use. In this scoping review, the “participant’s age at assessment” is defined as the participant’s age at study participation. Data were synthesized descriptively, and study characteristics were presented in a tabular form including structured summaries of the study characteristics and findings.
Results
Search findings
In total, 1986 studies (Medline n = 933; Embase n = 876; PsychINFO n = 110; and manual sources n = 67) were identified. After removing duplicates, 1,679 remained. Of these, 1,354 ineligible studies were excluded, and the remaining 325 full texts were reviewed. Finally, 185 studies were excluded leaving a total of 140 studies included in this scoping review (Figure 1).
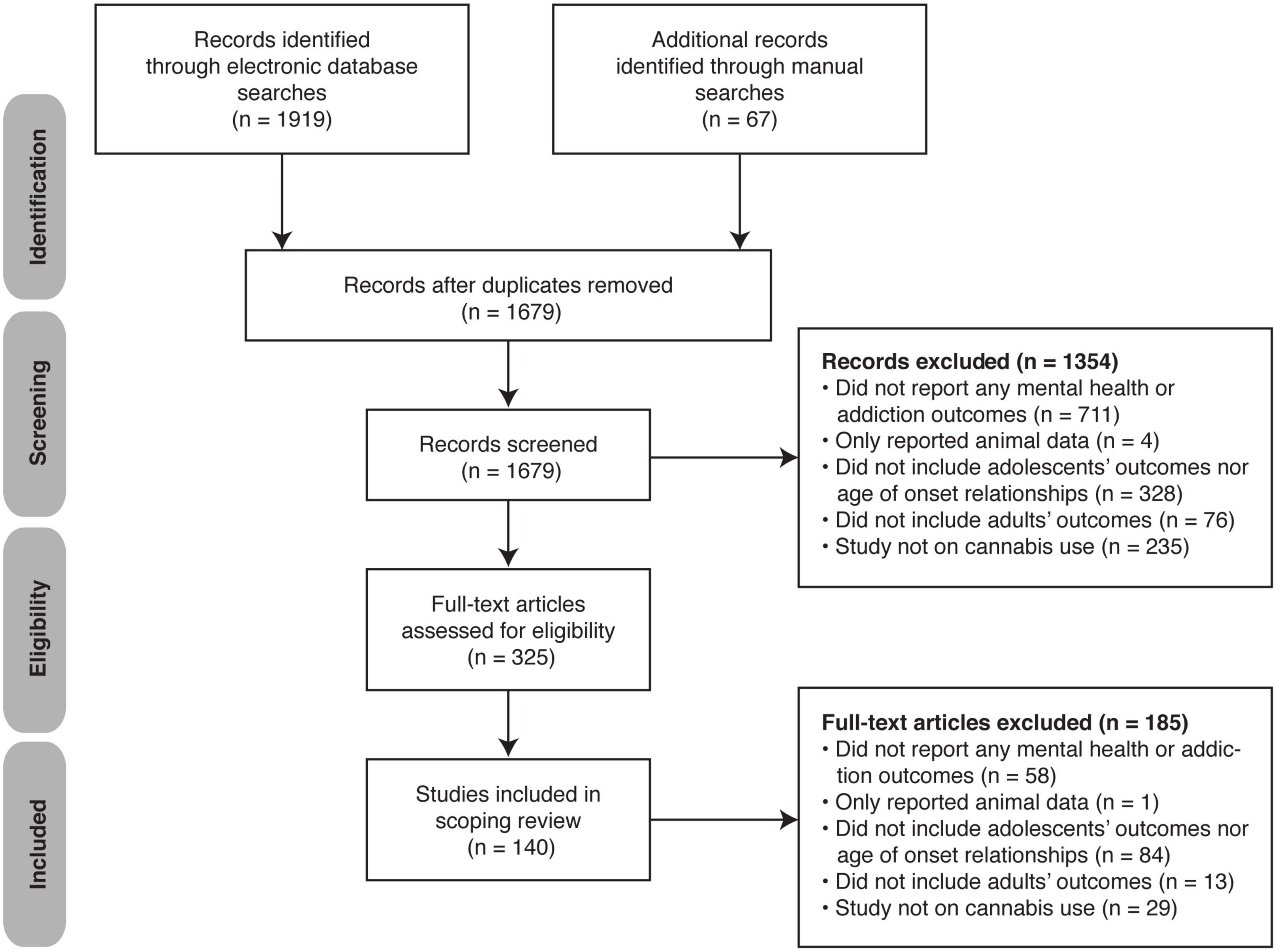
Figure 1. PRISMA flow diagram of the search and study selection process.
Characteristics of included studies
Among the 140 included studies, 135 were in English (9–13, 16, 20, 24–151) three in French (152–154), one in Spanish (155) and one was available both in French and English (7). There was one meta-analysis (88), one systematic review (7), two combined meta-analyses and systematic reviews (13, 20), 11 literature reviews (33, 61, 76, 86, 87, 90, 95, 110, 124, 136, 152), four randomized controlled trials (79, 100, 112, 134), 61 cohort studies (10, 16, 26, 28, 29, 32, 35, 36, 40–45, 47–50, 55, 60, 62, 64, 68, 69, 71, 74, 78, 80, 83, 92, 96, 98, 104, 106–109, 111, 116, 118, 119, 123, 125, 128, 130, 132, 133, 135, 138–147, 149–151), 52 cross-sectional studies (11, 12, 24, 25, 27, 30, 31, 34, 37–39, 46, 51–54, 57–59, 66, 67, 70, 72, 73, 75, 77, 81, 82, 84, 85, 89, 91, 94, 97, 99, 101–103, 105, 113, 115, 117, 120, 121, 126, 127, 131, 137, 148, 153–155), three repeated cross-sectional studies (93, 122, 129), one naturalistic study (56), two retrospective cohort studies (65, 114), and two case-control studies (9, 63). Characteristics of the included studies are presented in Supplementary Tables 1–4 and the main findings are described below.
Main findings
Research question 1: Are the risks of cannabis’s adverse effects on mental health and addiction higher in adolescents compared with adults?
Supplementary Table 1 summarizes the 12 studies comparing cannabis’s adverse mental health and addiction effects between adolescents and adults.
(i) Psychotic symptoms
Two studies by Mokrysz et al. (100, 134) reported that adults acutely exposed to cannabis experienced more psychotic-like effects than adolescents. Kelley et al. (99) found that daily cannabis use in adolescents tripled and in adults doubled the rate of onset of psychosis. Albertella et al. (10) reported that younger frequent cannabis users showed increased negative schizotypy while older frequent users showed reduced negative schizotypy.
(ii) Anxiety
Mokrysz et al. (100) observed that adults acutely exposed to cannabis rated their anxiety higher than when exposed to placebo while adolescents reported no such difference.
(iii) Suicidality
Levine et al. (110) concluded adolescent cannabis users are at higher risk of later suicidality.
(iv) Cannabis use and cannabis use disorder
Adolescents reported using cannabis more often than adults (115). Four studies (24, 31, 91, 105) reported 1.3–2.5 increased odds of developing a CUD in adolescent compared with adult cannabis users. Mokrysz et al. found that adolescents felt less stoned, felt the drug less, wanted more cannabis following exposure (100) and scored lower on negative experience (77) compared with adults.
(v) Other substance use disorders
Wang et al. (102) concluded that the odds of co-occurring nicotine dependence greatly varied with age of cannabis use, reaching peak values during adolescence and late adulthood. Levine et al. (110) reported that adolescent cannabis users were at increased risk of addiction to several substances.
(vi) Other adverse effects on mental health
Hawke et al. (115) found that adolescent cannabis users were more likely to have an externalizing disorder such as attention deficit hyperactivity disorder than adult users. Levine et al. (110) indicated that adolescent cannabis users are at increased risk of psychiatric morbidity.
Research question 2: What are the relationships between cannabis’s adverse effects and (a) participant’s age at first cannabis use, (b) participant’s age at assessment, and (c) duration of cannabis use?
(a) Supplementary Table 2 summarizes the 115 studies on relationships between cannabis’s adverse mental health and addiction effects and participant’s age at first cannabis use.
(i) Psychosis and related disorders
Forty-four studies reported that early cannabis initiation was associated with psychotic outcomes, including earlier age of onset of psychosis (7, 9, 53, 61, 64, 65, 73, 75, 82, 97, 99, 101, 138), higher risks of psychotic symptoms (12, 38, 56, 66–68, 70, 71, 75, 94, 95, 103, 111, 116, 127, 131, 150) and greater severity of these symptoms (20, 61, 89), higher risks of psychosis (61, 86, 90, 131, 147), and higher risk of psychotic disorder (7, 59, 87, 95, 136, 152) compared with later initiation or non-use of cannabis. Two studies (73, 82) revealed that the onset of psychosis followed cannabis initiation on average 7–8 years after. Two studies (59, 89) associated the risk of cocaine-induced psychosis to an earlier age of cannabis use. A review (86) suggested that the higher risk of psychosis in early cannabis users was dose dependent. Eight studies (63, 80, 92, 97, 112, 116, 125, 128) found no association between psychosis outcomes and the age of cannabis initiation. Curran et al. (121) reported opposite results with older age of cannabis initiation associated with more psychotic symptoms.
(ii) Anxiety
Five studies (87, 106, 128, 142, 143) reported that early-age cannabis users had between two and three times the odds of anxiety disorders compared with non-users, while five studies (13, 68, 92, 132, 149) including a meta-analysis (13) and a cohort study (149) found no such association after adjusting for demographics and childhood adversities. Another study indicated that such increased risk was limited to early and frequent cannabis users (78). Late cannabis initiation was associated with a fourfold increase in odds of developing an anxiety disorder as compared with non-users (128) a finding supported by another team reporting similar probability (92). Of the four studies comparing the risk or incidence of anxiety disorders between early and late cannabis users, only one (96) found a fourfold increased odds while the other three (92, 107, 132) found no difference. Dragt et al. (71) reported that age at first cannabis use positively correlated with age of onset of anxiety symptoms while two other studies (67, 112) found no such correlation. Two studies (61, 87) concluded that early cannabis initiation is a risk factor for anxiety disorders for frequent cannabis users. Hosseini et al. (7) indicated that too low quality of evidence exists on anxiety for recommending a minimum age for cannabis use for preventing this outcome.
(iii) Depression
Fifteen studies (13, 29, 33, 37, 61, 68, 72, 87, 88, 98, 119, 139, 142, 143, 152) reported that early cannabis initiators had between 1.1 and 8.8 times the odds of depression compared with non-users, while eight studies (37, 48, 50, 67, 78, 98, 128, 149) reported similar odds, incidence or no association. Four studies (72, 128, 139, 150) found that late cannabis initiators had between 1.6 and 3.3 times the odds of depression compared with non-users while two studies (29, 119) reported similar odds. These increased odds of depression disappeared after covariates adjustment in three studies (37, 142, 143). Lynskey et al. (37) revealed that depression risk was increased only in dizygotic twins discordant for early cannabis use, but not in monozygotic twins, before confounders adjustment, indicating a genetic modulatory effect. Harder et al. (48) found 2.6 times increased odds of depression only in males with problematic cannabis use in adolescence compared with those without problematic cannabis use. Three studies (54, 96, 132) showed that early cannabis initiators were between 1.2 and 1.9 times more likely to develop depression compared with late initiators, while another study (26) found similar likelihood. Out of three studies (37, 67, 71, 112) assessing correlations, one (71) found a positive correlation between age of cannabis initiation and age of onset of depressed mood.
(iv) Suicidality
Five studies (13, 37, 104, 128, 142) including a meta-analysis (13) reported that early cannabis initiators had 1.5–4.2 times the odds of considering suicide and 1.7–8.7 times the odds of attempting suicide compared with non-users (13, 37, 88, 104). However, these relationships in some instances became non-significant after covariates adjustment (37, 128, 142) and two studies (50, 106) reported no association. Silins et al. (88) found that the higher risk of suicide attempts in early cannabis users depended on cannabis use frequency, with daily cannabis use having the highest odds. Late cannabis users had a similar risk of suicide ideation (104, 128) and suicide attempts (104) compared with never users. When comparing early with late cannabis users, the suicidality risk was increased twofold in the early users (132). Savage et al. (112) reported that age of cannabis initiation negatively correlated with suicide risk rating.
(v) Other cannabis use outcomes
Baggio et al. (83) reported higher proportions of early compared with late cannabis users who felt high, relaxed, laughed a lot, and did crazy things the first time they tried cannabis. Ellickson et al. (40) indicated that a younger age at cannabis initiation was associated with negative consequences such as concentration problems. A cross-sectional study (39) found that early-age cannabis users (<16 years old) had increased odds of problematic cannabis use than later-age users. Bravo et al. (120) observed that younger age at first cannabis use was associated with less reliance on cannabis protective behavioral strategies. A cohort study (144) reported that early cannabis use increased the likelihood of continued cannabis use in adulthood.
(vi) Cannabis use disorder
Five studies (34, 88, 108, 123, 128) found that, depending on use frequency, cannabis users starting in adolescence had between two and 300 times the odds of subsequent cannabis dependence compared with non-users. When controlling for covariates, these odds ratios remained significant and varied between two and 253 (34, 55, 88, 108, 128). Furthermore, rates of dependence were between four and 14 times higher in early-age cannabis users compared with never users (143). Two cohort studies (36, 107) and two cross-sectional studies (25, 85) reported similar risk of dependence in early-age compared with later-age cannabis initiators. Three cross-sectional studies (34, 85, 131) and three cohort studies (32, 69, 151) found 2.0–2.7 times increased risk of developing cannabis abuse or dependence in early compared with later-age cannabis initiators. Interestingly, each year older at first cannabis use reduced the odds of developing dependence by 11% (84). People who develop cannabis dependence are more likely to have a younger age of initiation than non-problematic cannabis users (46). The time from first cannabis use to cannabis dependence diagnosis increased from 28 years in cannabis initiators starting before age 13, to 47 years in initiators starting after age 19 (57). The increased risk of dependence among young cannabis initiators was further supported by three narrative reviews (95, 124, 152) and a cohort study (145). Four studies further associated early initiation with risky cannabis use (81), severe cannabis dependence (126), and CUD (148).
(vii) Other substances use
Four studies found that early cannabis users were more likely to consume tobacco than non-users (68) or late cannabis users (49, 103, 130). Three studies (44, 85, 96) supported this finding but only for daily tobacco use, and this association was non-significant after covariates adjustment in another study (149). Moore and Budney (27) reported a younger age at first cannabis use among tobacco smokers compared with non-smokers. Mixed evidence was found among the three studies (85, 93, 96) measuring alcohol use. Moss et al. (85) found no difference between early cannabis users and non-users for monthly and yearly alcohol use, while Buu et al. (93) noted an increased risk of heavy alcohol use for both early and late cannabis users compared with non-users. Few et al. (96) revealed that early cannabis users had twice the odds of regularly using alcohol compared with their late using co-twin. Stanley et al. (137) reported that while late cannabis users had 16 times the odds of misusing prescription drugs compared with non-users, early cannabis users had 47 times these odds. Early cannabis initiators had twice the odds of misusing prescription opioids compared with non-users (135), and nearly twice the risk of prescription opioid misuse compared with late users (129). This contrasts with Moss et al. (85) findings of similar prevalence of pain reliever misuse between early cannabis users and non-users. Hall et al. (95) reported that majority of the 17 studies reviewed associated early cannabis use with other illicit substance use. Early cannabis users had between two and 14 times the odds of using other drugs compared with non-users (34, 41, 42, 68, 88, 135). After covariates adjustment, these odds were increased to between two and 17 times (34, 62, 88, 135), or became non-significant (149). These results are in line with increased prevalence of a range of illicit drug uses among early cannabis users compared with non-users (47, 85), especially in frequent cannabis users (143). Early cannabis users were sometimes as likely (39, 79) and sometimes more likely (96, 103) to use illicit substances than late users. Finally, the age of cannabis initiation negatively correlates (medium effect size) with illicit drug use frequency (40).
(viii) Other substance use disorders
Early cannabis users were more likely to develop nicotine dependence than non-users (45, 55, 128) or late users (44, 45, 131). However, two studies reported no difference either in this risk between early cannabis users and non-users (85) or in the incidence of nicotine use disorder in early versus late cannabis initiators (107). The risk of developing an alcohol dependence was also higher for early cannabis users compared with non-users (55, 128, 143) or late users (36). However, this relationship sometimes became non-significant after covariates adjustment (55, 143). Another study (107) found similar incidence of alcohol use disorder in early- and later-age cannabis users. When controlling for confounders, early cannabis initiators had between 2 and 66 times the odds of illicit substance use disorder (SUD) (29, 128) or drug abuse (62) and twice the prevalence of illegal drug dependence (85) compared with non-users. The review by Dervaux et al. (152) further supported these results. Four studies (34, 118, 131, 145) found that the risk of illicit drug use or dependence depended on the age at first cannabis use and the type of other drug involved. For example, it was the highest in cannabis initiators starting before age 13 and became non-significant after age 15 (118). Moreover, it was higher for cocaine/stimulants, and opioids (34) but similar for methamphetamines (131) and sedatives (34).
(ix) Other mental health outcomes
As reviewed by Rubino et al. (76) three studies reported that early cannabis initiation increased the odds of psychological distress (103), subclinical psychotic experience (66), or non-suicidal injury (96) compared with later cannabis initiation. When compared with non-users, early and frequent cannabis use increased the odds of anxiety and depression two to threefold while late and frequent cannabis use increased it twofold (43). Estrada et al. (11) reported a positive correlation between age at first use and age of onset for psychiatric illness. Shah et al. (114) found that early cannabis initiation predicted progression to a cannabis-induced psychotic or mood disorder. Eight studies (35, 36, 40, 67, 92, 113, 149, 155) found no relationship between age of cannabis initiation and psychiatric disorders.
(b) Supplementary Table 3 summarizes the 12 studies on relationships between cannabis’s adverse mental health and addiction effects and participant’s age at assessment.
(i) Depression and anxiety
The associations between cannabis use and depression symptoms differed with age (133). When depression and anxiety were measured together, however, Meier et al. (133) found no evidence of an association with age. When assessed separately, one cohort study (74) confirmed that cannabis use at younger age was associated with increased depressive symptoms compared with older age. Conversely, although Patton et al. (146) did not directly compare age groups in their cohort, the association between daily cannabis use and depression and anxiety during adulthood was stronger for past-year adult use than for adolescent use in women only (similar in males).
(ii) Suicidality
Fergusson et al. (141) showed that the strength of association between cannabis use frequency and suicidal ideations and attempts decreased with increasing age (14–21 years old).
(iii) Cannabis use and cannabis use disorder
Fergusson et al. (140) indicated that the cumulative risk of cannabis dependence increased gradually from 0% at age 16 to 9% at age 21. Wagner et al. (30) showed a moderate risk for developing CUD following early cannabis use. Madruga et al. (148) indicated that odds of current or past-year cannabis use decreased with progressing age. Chen et al. (144) reported that early age is a predictor of ongoing cannabis use. Padovano et al. (117) reported that adolescents experienced a greater subjective high experience than young adults.
(iv) Other substances use and substance use disorders
Two studies (16, 62) indicated that the odds of other illicit substance use following cannabis use declined with increasing age. One study (16) confirmed similar significant associations for other substance use. Another study (155) reported that younger age is associated with SUD among cannabis users. Finally, Fergusson et al. (141) showed that the strength of association between cannabis use frequency and illicit drug use decreased gradually with increasing age (between ages 14 and 21).
(v) Other mental health outcomes
A cross-sectional study (155) showed that age was associated with the presence of Axis I psychiatric disorders other than SUD but not with Axis II disorders among cannabis users.
(c) Supplementary Table 4 summarizes the 18 studies on relationships between cannabis’s mental health and addiction adverse effects and duration of cannabis use.
(i) Psychosis and related disorders
Two studies (52, 60) found that a cannabis use duration of more than 5 or 6 years increased the odds of experiencing psychosis twofold compared with a shorter duration or no cannabis use. Two studies (97, 147) found no correlation between cannabis use duration and age of onset of psychotic disorder (97) nor transition to psychosis (147).
(ii) Anxiety
Four (58, 94, 128, 133) out of the five studies (58, 94, 128, 133, 153) focusing on anxiety found a positive relationship with cannabis use duration. Cannabis users consuming for at least 11 years, between 2 and 10 years, and for 1 year or less had respectively 2.8, 2.3, and 1.6 times the odds of anxiety compared with non-users (58). Similarly, weekly cannabis users consuming for 16 years had 2.1 (2.5) times the (adjusted) odds of anxiety compared with non-users whereas those who weekly used for 8 years had 2.3 (2.8) times these odds (128). Although Cloak et al. (94) did not measure cannabis use duration per se, they found positive small-effect size correlations between cumulative lifetime quantity of cannabis and anxiety symptoms or phobic anxiety. Furthermore, Meier et al. (133) indicated that each additional year of weekly cannabis use increased the risk of anxiety and depression problems, when measured together. Another cross-sectional study (153) found no correlation between cannabis use duration and anxiety.
(iii) Depression and suicidality
Four studies associated a higher risk of depression (58, 72, 122, 133), one study associated depressive symptoms (153) and one study associated suicidal ideation (128) with long cannabis use duration. Two studies (58, 72) indicated that cannabis users who consumed cannabis for more than 11 years had nearly three times the odds of depression compared with non-users, whereas those who used between 2 and 10 years had twice these odds. Chabrol et al. (153) also reported a positive correlation between the depression score and cannabis use duration. Similarly, Meier et al. (133) indicated that each additional year of weekly cannabis use slightly increased the risk of depression. Conversely, Han et al. (122) reported a decreased depression prevalence for longer cannabis use duration (>3 years) than shorter duration (1–2 years) among adolescents.
(iv) Cannabis use disorder
Five (24, 84, 128, 154, 156) studies found an increased prevalence or risk with longer cannabis use duration. Von Sydow et al. (28) indicated that cannabis users develop cannabis abuse and dependence on average 2.0- and 2.4-years following initiation, respectively. Han et al. (122) reported an increased prevalence of CUD among adolescents and adults (adjusted prevalence of CUD in adolescents increased from 10.9 to 20.6% and in adults from 5.6 to 10.5% between the first and the fourth year of cannabis use).
(v) Other substance use disorders
Two cross-sectional studies (155, 156) and two cohort studies (128, 149) confirmed an increased prevalence or risk of SUD with longer cannabis use duration whereas Degenhardt et al. (51) found the opposite association. Han et al. (122) reported that after long cannabis use periods, both adults and adolescents developed other SUDs related to nicotine, alcohol, cocaine, hallucinogen, tranquilizers/sedatives, and opioids.
(vi) Other mental health outcomes
Three studies found positive small-effect size correlations between cannabis use duration and borderline personality disorder (153), and obsessive-compulsive scores (94). Cuenca-Royo et al. (155) found similar odds of psychiatric diagnosis in cannabis users consuming for 5–7 years compared with those consuming from 1 to 4 years.
Discussion
Our scoping review’s results indicate that cannabis use is overall associated with higher likelihood of adverse mental health and substance use outcomes among adolescents, early cannabis initiators and cannabis users who consumed for longest periods. The strength of evidence varied based on the types of mental health and addiction outcomes. Substantial evidence was found for psychotic disorders, as well as cannabis and nicotine use disorders. Mixed evidence was obtained for depression and suicidality, other substance use, and other SUDs while it was limited for anxiety. Acute cannabis exposure led to the opposite trend with adults more often reporting adverse effects compared with adolescents. While our findings are overall consistent with three other recent reviews (7, 13, 95) on specific outcomes (i.e., psychosis, depression, other substance use, and suicidality) of cannabis exposure, we identified several knowledge gaps in the literature with some inherent limits and strengths in this scoping review.
Nearly half of the studies evaluating the effect of age of use initiation on cannabis-related harms compared early cannabis users with non-users instead of later-age users. Consequently, it was impossible to disentangle the effects of cannabis use from age at first use other than by comparing results with those obtained in similar studies conducted in older samples. Moreover, studies divided their age groups using different age categories, and most of the included studies measured cannabis consumption using self-report data. This type of measurement may be prone to recall and social desirability biases. More importantly, it prevents from accurately identifying exposure to specific cannabinoids (i.e., tetrahydrocannabinol and cannabidiol) and the level of such exposure. Future research should use complementary biological sampling to improve measurement of cannabis and cannabinoid exposure, like did few authors (11, 100, 113, 114, 131, 134). This is even more important with the continuously changing concentrations of tetrahydrocannabinol and cannabidiol especially in cannabis products obtained from the unregulated market (157–159). These ongoing changes in cannabis composition and potency also highlight the need for repeated assessments of the risks of cannabis use, which may fluctuate over time, as different products are made available to consumers across all age groups.
Age of cannabis use initiation and duration of cannabis use were main factors influencing the magnitude of cannabis-related harms. Other important contributors and potential effect moderators include cannabis potency (160), use frequency (161), familial medical history (162), and peer influence (163, 164). However, not all studies controlled for these potential confounders and among those who did, the associations were sometimes non-significant. This suggests that young age, early initiation, and longer duration of cannabis use represent only some of a complex array of risk factors that contribute to potential adverse outcomes of cannabis exposure. Overall, there was no clear evidence of a specific age of use at which cannabis-related harms could be avoided; such threshold would likely vary according to specific outcomes of interest. This prevents us from advising an age limit for “safe” cannabis consumption and highlights the challenging nature of such efforts. Notwithstanding the limitations of the available literature, it is reasonable to suggest that delaying cannabis consumption as late as possible and limiting the duration of use could decrease the risk of both short- and long-term adverse effects, aligned with the recommendations of the Lower Risk Cannabis Use Guidelines (165). Equally important, and as has been proposed by others, efforts are required to further standardize measurement of cannabis exposure, outcomes to prioritize, and potential confounders to facilitate knowledge synthesis.
Beyond the restrictions of the available literature as described above, this scoping review has its very own strengths and limitations. One of the key strengths of the present scoping review is that we used a broad search strategy and included highly heterogeneous study designs and measurement methods. This allowed us to obtain a wide overview of cannabis harms on mental health and addiction. Other outcomes related to mental health such as cognitive function, however, were outside the scope of this review and merit further attention. Also, we limited our selection to studies published in English, French, and Spanish. This could have introduced a small language bias that, however, seems to be unlikely to change our conclusions. Finally, in this review we broadly used the term “adulthood,” which, at least in theory, included “senior age.” Future research and knowledge synthesis efforts should pay specific attention to that age group to determine if and how some outcomes may specifically vary among older adults.
Conclusion
In conclusion, age of exposure seems likely to modulate cannabis use-related mental health and addiction outcomes. Cannabis’ adverse effects on the long-term outcomes tended to be generally worse in adolescents, early cannabis use initiators and cannabis users who consumed for long periods. Thus, delaying cannabis use initiation to as late as possible in young adulthood and limiting cannabis use to short periods could decrease the risk of adverse cannabis use consequences. Using a harm reduction perspective, we advocate for providing youth with nuanced and accurate information on potential effects of cannabis use and develop interventions to promote safer cannabis consumption practices, taking into consideration specific risks associated with early-age cannabis use, which are not the same for all outcomes. Finally, we recommend that future research efforts on age-specific cannabis harms account for important confounding factors such as frequency and potency of cannabis consumed, and other key individual and environmental factors.
Data availability statement
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
DJ-A and NK: study conceptualization and supervision. NK: methodology. GB, LG, JG, VM-P, NK, HB, FM, and CT: study selection. GB, LG, JG, NK, HB, and VM-P: data charting and synthesis. NK, JG, LG, and GB: original manuscript draft writing. LG, GB, HB, NK, DJ-A, and BF: data interpretation. NK, GB, LG, JG, VM-P, HB, FM, CT, BF, and DJ-A: reviewing and editing of the manuscript. DJ-A: funding acquisition. All authors contributed to the article and approved the submitted version.
Funding
This work was financially supported by the Institut Universitaire sur les Dépendances and Quebec’s Ministère de la Santé et des Services Sociaux. The funders had no role in the study design, data collection and analysis, manuscript writing or decision to publish. DJ-A holds a clinical research award from the Fonds de Recherche du Québec en Santé. GB had received a Ph.D. scholarship from Université de Montréal. FM holds a scholarship from the Canadian Institutes of Health Research.
Acknowledgments
We thank Benedicte Nauche and Caroline Sauvé, librarians at the Centre Hospitalier de l’Université de Montréal (CHUM) for refining, adapting, and updating the search strategy.
Conflict of interest
LG was now employed by AbbVie Corporation who does not support any of the author’s views and declares that this is the author’s independent work. VM was currently employed by Indivior who had no input, control or review of this article and confirms it is the author’s own independent work. DJ-A receives study materials from Tetra BioPharma and Cardiol Therapeutics for clinical trials funded by the Quebec’s Ministère de la Santé et des Services Sociaux.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.973988/full#supplementary-material
References
1. World Health Organization. Mental Health and Substance Abuse. Geneva: World Health Organization (2020).
2. Degenhardt L, Hall W. Extent of illicit drug use and dependence, and their contribution to the global burden of disease. Lancet. (2012) 379:55–70. doi: 10.1016/S0140-6736(11)61138-0
3. United Nations Office on Drugs and Crime. World Drug Report 2020. New York, NY: United Nations Publications (2021).
4. Cohen K, Weizman A, Weinstein A. Positive and negative effects of Cannabis and cannabinoids on health. Clin Pharmacol Ther. (2019) 105:1139–47.
5. National Academies of Sciences, Engineering and Medicine. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington, DC: The National Academies Press (2017). p. 486.
6. Blest-Hopley G, Colizzi M, Giampietro V, Bhattacharyya S. Is the adolescent brain at greater vulnerability to the effects of Cannabis? A narrative review of the evidence. Front Psychiatry. (2020) 11:859. doi: 10.3389/fpsyt.2020.00859
7. Hosseini S, Oremus M. The effect of age of initiation of Cannabis use on psychosis, depression, and anxiety among youth under 25 years. Can J Psychiatry. (2019) 64:304–12. doi: 10.1177/0706743718809339
8. Arseneault L, Cannon M, Witton J, Murray RM. Causal association between Cannabis and psychosis: examination of the evidence. Br J Psychiatry. (2004) 184:110–7.
9. Di Forti M, Sallis H, Allegri F, Trotta A, Ferraro L, Stilo SA, et al. Daily use, especially of high-potency Cannabis, drives the earlier onset of psychosis in Cannabis users. Schizophr Bull. (2014) 40:1509–17. doi: 10.1093/schbul/sbt181
10. Albertella L, Le Pelley ME, Yucel M, Copeland J. Age moderates the association between frequent Cannabis use and negative schizotypy over time. Addict Behav. (2018) 87:183–9. doi: 10.1016/j.addbeh.2018.07.016
11. Estrada G, Fatjo-Vilas M, Munoz MJ, Pulido G, Minano MJ, Toledo E, et al. Cannabis use and age at onset of psychosis: further evidence of interaction with COMT Val158Met polymorphism. Acta Psychiatr Scand. (2011) 123:485–92. doi: 10.1111/j.1600-0447.2010.01665.x
12. Konings M, Henquet C, Maharajh HD, Hutchinson G, Van Os J. Early exposure to Cannabis and risk for psychosis in young adolescents in Trinidad. Acta Psychiatr Scand. (2008) 118:209–13. doi: 10.1111/j.1600-0447.2008.01202.x
13. Gobbi G, Atkin T, Zytynski T, Wang S, Askari S, Boruff J, et al. Association of Cannabis use in adolescence and risk of depression, anxiety, and suicidality in young adulthood: a systematic review and meta-analysis. JAMA Psychiatry. (2019) 76:426–34. doi: 10.1001/jamapsychiatry.2018.4500
14. Lopez-Quintero C, Perez de los Cobos J, Hasin DS, Okuda M, Wang S, Grant BF, et al. Probability and predictors of transition from first use to dependence on nicotine, alcohol, Cannabis, and cocaine: results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Drug Alcohol Depend. (2011) 115:120–30. doi: 10.1016/j.drugalcdep.2010.11.004
15. Feingold D, Livne O, Rehm J, Lev-Ran S. Probability and correlates of transition from Cannabis use to DSM-5 Cannabis use disorder: results from a large-scale nationally representative study. Drug Alcohol Rev. (2020) 39:142–51. doi: 10.1111/dar.13031
16. Fergusson DM, Boden JM, Horwood LJ. Cannabis use and other illicit drug use: testing the Cannabis gateway hypothesis. Addiction. (2006) 101:556–69. doi: 10.1111/j.1360-0443.2005.01322.x
17. Wells J, McGee MA. Violations of the usual sequence of drug initiation: prevalence and associations with the development of dependence in the New Zealand Mental Health Survey. J Stud Alcohol Drugs. (2008) 69:789–95. doi: 10.15288/jsad.2008.69.789
18. Carliner H, Brown QL, Sarvet AL, Hasin DS. Cannabis use, attitudes, and legal status in the U.S.: a review. Prev Med. (2017) 104:13–23. doi: 10.1016/j.ypmed.2017.07.008
19. Moore THM, Zammit S, Lingford-Hughes A, Barnes TRE, Jones PB, Burke M, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet. (2007) 370:319–28.
20. Kiburi SK, Molebatsi K, Ntlantsana V, Lynskey MT. Cannabis use in adolescence and risk of psychosis: are there factors that moderate this relationship? A systematic review and meta-analysis. Subst Abus. (2021) 42:527–42. doi: 10.1080/08897077.2021.1876200
21. Peters M, Godfrey C, McInerney P, Soares C, Khalil H, Parker D. The Joanna Briggs Institute Reviewers’ Manual 2015: Methodology for JBI Scoping Reviews. Adelaide, SA: Joanna Briggs Institute (2015).
22. Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73.
23. Kaur, N, Bastien G, Mongeau-Pérusse V, Johann G, Thériault C, Jutras-Aswad D. Comparing mental health outcomes of Cannabis use among adolescents and adults: a scoping review. Open Sci Framework. (2020).
24. Chen K, Kandel DB, Davies M. Relationships between frequency and quantity of marijuana use and last year proxy dependence among adolescents and adults in the United States. Drug Alcohol Depend. (1997) 46:53–67. doi: 10.1016/s0376-8716(97)00047-1
25. DeWit DJ, Hance J, Offord DR, Ogborne A. The influence of early and frequent use of marijuana on the risk of desistance and of progression to marijuana-related harm. Prev Med. (2000) 31:455–64. doi: 10.1006/pmed.2000.0738
26. Kandel DB, Chen K. Types of marijuana users by longitudinal course. J Stud Alcohol. (2000) 61:367–78.
27. Moore BA, Budney AJ. Tobacco smoking in marijuana-dependent outpatients. J Subst Abuse. (2001) 13:583–96. doi: 10.1016/s0899-3289(01)00093-1
28. Von Sydow K, Lieb R, Pfister H, Hofler M, Sonntag H, Wittchen HU. The natural course of Cannabis use, abuse and dependence over four years: a longitudinal community study of adolescents and young adults. Drug Alcohol Depend. (2001) 64:347–61. doi: 10.1016/s0376-8716(01)00137-5
29. Brook DW, Brook JS, Zhang C, Cohen P, Whiteman M. Drug use and the risk of major depressive disorder, alcohol dependence, and substance use disorders. Arch Gen Psychiatry. (2002) 59:1039–44.
30. Wagner FA, Anthony JC. From first drug use to drug dependence: developmental periods of risk for dependence upon marijuana, cocaine, and alcohol. Neuropsychopharmacology. (2002) 26:479–88.
31. Chen CY, Anthony JC. Possible age-associated bias in reporting of clinical features of drug dependence: epidemiological evidence on adolescent-onset marijuana use. Addiction. (2003) 98:71–82. doi: 10.1046/j.1360-0443.2003.00237.x
32. Coffey C, Carlin JB, Lynskey M, Li N, Patton GC. Adolescent precursors of Cannabis dependence: findings from the Victorian adolescent health cohort study. Br J Psychiatry. (2003) 182:330–6. doi: 10.1192/bjp.182.4.330
33. Degenhardt L, Hall W, Lynskey M. Exploring the association between Cannabis use and depression. Addiction. (2003) 98:1493–504.
34. Lynskey MT, Heath AC, Bucholz KK, Slutske WS, Madden PAF, Nelson EC, et al. Escalation of drug use in early-onset Cannabis users vs co-twin controls. J Am Med Assoc. (2003) 289:427–33. doi: 10.1001/jama.289.4.427
35. Ellickson PL, Martino SC, Collins RL. Marijuana use from adolescence to young adulthood: multiple developmental trajectories and their associated outcomes. Health Psychol. (2004) 23:299–307.
36. Flory K, Lynam D, Milich R, Leukefeld C, Clayton R. Early adolescent through young adult alcohol and marijuana use trajectories: early predictors, young adult outcomes, and predictive utility. Dev Psychopathol. (2004) 16:193–213. doi: 10.1017/s0954579404044475
37. Lynskey MT, Glowinski AL, Todorov AA, Bucholz KK, Madden PAF, Nelson EC, et al. Major depressive disorder, suicidal ideation, and suicide attempt in twins discordant for Cannabis dependence and early-onset Cannabis use. Arch Gen Psychiatry. (2004) 61:1026–32. doi: 10.1001/archpsyc.61.10.1026
38. Stefanis NC, Delespaul P, Henquet C, Bakoula C, Stefanis CN, Van Os J. Early adolescent Cannabis exposure and positive and negative dimensions of psychosis. Addiction. (2004) 99:1333–41. doi: 10.1111/j.1360-0443.2004.00806.x
39. Baumeister SE, Tossmann P. Association between early onset of cigarette, alcohol and Cannabis use and later drug use patterns: an analysis of a survey in European metropolises. Eur Addict Res. (2005) 11:92–8. doi: 10.1159/000083038
40. Ellickson PL, D’Amico EJ, Collins RL, Klein DJ. Marijuana use and later problems: when frequency of recent use explains age of initiation effects (and when it does not). Subst Use Misuse. (2005) 40:343–59. doi: 10.1081/ja-200049356
41. Lessem JM, Hopfer CJ, Haberstick BC, Timberlake D, Ehringer MA, Smolen A, et al. Relationship between adolescent marijuana use and young adult illicit drug use. Behav Genet. (2006) 36:498–506. doi: 10.1007/s10519-006-9064-9
42. Lynskey MT, Vink JM, Boomsma DI. Early onset Cannabis use and progression to other drug use in a sample of Dutch twins. Behav Genet. (2006) 36:195–200. doi: 10.1007/s10519-005-9023-x
43. Hayatbakhsh MR, Najman JM, Jamrozik K, Mamun AA, Alati R, Bor W. Cannabis and anxiety and depression in young adults: a large prospective study. J Am Acad Child Adolesc Psychiatry. (2007) 46:408–17.
44. Timberlake DS, Haberstick BC, Hopfer CJ, Bricker J, Sakai JT, Lessem JM, et al. Progression from marijuana use to daily smoking and nicotine dependence in a national sample of U.S. adolescents. Drug Alcohol Depend. (2007) 88:272–81. doi: 10.1016/j.drugalcdep.2006.11.005
45. Agrawal A, Lynskey MT, Pergadia ML, Bucholz KK, Heath AC, Martin NG, et al. Early Cannabis use and DSM-IV nicotine dependence: a twin study. Addiction. (2008) 103:1896–904. doi: 10.1111/j.1360-0443.2008.02354.x
46. Caldeira KM, Arria AM, O’Grady KE, Vincent KB, Wish ED. The occurrence of Cannabis use disorders and other Cannabis-related problems among first-year college students. Addict Behav. (2008) 33:397–411.
47. Cleveland HH, Wiebe RP. Understanding the association between adolescent marijuana use and later serious drug use: gateway effect or developmental trajectory? Dev Psychopathol. (2008) 20:615–32.
48. Harder VS, Stuart EA, Anthony JC. Adolescent Cannabis problems and young adult depression: male-female stratified propensity score analyses. Am J Epidemiol. (2008) 168:592–601. doi: 10.1093/aje/kwn184
49. Heffner JL, DelBello MP, Fleck DE, Anthenelli RM, Strakowski SM. Cigarette smoking in the early course of bipolar disorder: association with ages-at-onset of alcohol and marijuana use. Bipolar Disord. (2008) 10:838–45. doi: 10.1111/j.1399-5618.2008.00630.x
50. Pedersen W. Does Cannabis use lead to depression and suicidal behaviours? A population-based longitudinal study. Acta Psychiatr Scand. (2008) 118:395–403. doi: 10.1111/j.1600-0447.2008.01259.x
51. Degenhardt L, Chiu WT, Conway K, Dierker L, Glantz M, Kalaydjian A, et al. Does the gateway matter? Associations between the order of drug use initiation and the development of drug dependence in the National Comorbidity Study Replication. Psychol Med. (2009) 39:157–67. doi: 10.1017/S0033291708003425
52. Di Forti M, Morgan C, Dazzan P, Pariante C, Mondelli V, Marques TR, et al. High-potency Cannabis and the risk of psychosis. Br J Psychiatry. (2009) 195:488–91.
53. Barrigon ML, Gurpegui M, Ruiz-Veguilla M, Diaz FJ, Anguita M, Sarramea F, et al. Temporal relationship of first-episode non-affective psychosis with Cannabis use: a clinical verification of an epidemiological hypothesis. J Psychiatr Res. (2010) 44:413–20. doi: 10.1016/j.jpsychires.2009.10.004
54. de Graaf R, Radovanovic M, van Laar M, Fairman B, Degenhardt L, Aguilar-Gaxiola S, et al. Early Cannabis use and estimated risk of later onset of depression spells: epidemiologic evidence from the population-based World Health Organization World Mental Health Survey Initiative. Am J Epidemiol. (2010) 172:149–59. doi: 10.1093/aje/kwq096
55. Degenhardt L, Coffey C, Carlin JB, Swift W, Moore E, Patton GC. Outcomes of occasional Cannabis use in adolescence: 10-year follow-up study in Victoria, Australia. Br J Psychiatry. (2010) 196:290–5. doi: 10.1192/bjp.bp.108.056952
56. Dragt S, Nieman DH, Becker HE, van de Fliert R, Dingemans PM, de Haan L, et al. Age of onset of Cannabis use is associated with age of onset of high-risk symptoms for psychosis. Can J Psychiatry. (2010) 55:165–71.
57. Ehlers CL, Gizer IR, Vieten C, Gilder DA, Stouffer GM, Lau P, et al. Cannabis dependence in the San Francisco family study: age of onset of use, DSM-IV symptoms, withdrawal, and heritability. Addict Behav. (2010) 35:102–10. doi: 10.1016/j.addbeh.2009.09.009
58. Han B, Gfroerer JC, Colliver JD. Associations between duration of illicit drug use and health conditions: results from the 2005-2007 national surveys on drug use and health. Ann Epidemiol. (2010) 20:289–97. doi: 10.1016/j.annepidem.2010.01.003
59. Kalayasiri R, Gelernter J, Farrer L, Weiss R, Brady K, Gueorguieva R, et al. Adolescent Cannabis use increases risk for cocaine-induced paranoia. Drug Alcohol Depend. (2010) 107:196–201. doi: 10.1016/j.drugalcdep.2009.10.006
60. McGrath J, Welham J, Scott J, Varghese D, Degenhardt L, Hayatbakhsh MR, et al. Association between Cannabis use and psychosis-related outcomes using sibling pair analysis in a cohort of young adults. Arch Gen Psychiatry. (2010) 67:440–7. doi: 10.1001/archgenpsychiatry.2010.6
61. Richardson TH. Cannabis use and mental health: a review of recent epidemiological research. Int J Pharmacol. (2010) 6:796–807.
62. Van Gundy K, Rebellon CJA. Life-course perspective on the “gateway hypothesis”. J Health Soc Behav. (2010) 51:244–59. doi: 10.1177/0022146510378238
63. Agrawal A, Nurnberger JI, Lynskey MT. Cannabis involvement in individuals with bipolar disorder. Psychiatry Res. (2011) 185:459–61. doi: 10.1016/j.psychres.2010.07.007
64. Decoster J, van Os J, Kenis G, Henquet C, Peuskens J, De Hert M, et al. Age at onset of psychotic disorder: Cannabis, BDNF Val66Met, and sex-specific models of gene-environment interaction. Am J Med Genet B Neuropsychiatr Genet. (2011) 156B:363–9. doi: 10.1002/ajmg.b.31174
65. Schimmelmann BG, Conus P, Cotton SM, Kupferschmid S, Karow A, Schultze-Lutter F, et al. Cannabis use disorder and age at onset of psychosis – A study in first-episode patients. Schizophr Res. (2011) 129:52–6. doi: 10.1016/j.schres.2011.03.023
66. Schubart CD, van Gastel WA, Breetvelt EJ, Beetz SL, Ophoff RA, Sommer IE, et al. Cannabis use at a young age is associated with psychotic experiences. Psychol Med. (2011) 41:1301–10. doi: 10.1017/S003329171000187X
67. Skinner R, Conlon L, Gibbons D, McDonald C. Cannabis use and non-clinical dimensions of psychosis in university students presenting to primary care. Acta Psychiatr Scand. (2011) 123:21–7. doi: 10.1111/j.1600-0447.2010.01546.x
68. Anglin DM, Corcoran CM, Brown AS, Chen H, Lighty Q, Brook JS, et al. Early Cannabis use and schizotypal personality disorder symptoms from adolescence to middle adulthood. Schizophr Res. (2012) 137:45–9. doi: 10.1016/j.schres.2012.01.019
69. Behrendt S, Beesdo-Baum K, Hofler M, Perkonigg A, Buhringer G, Lieb R, et al. The relevance of age at first alcohol and nicotine use for initiation of Cannabis use and progression to Cannabis use disorders. Drug Alcohol Depend. (2012) 123):48–56. doi: 10.1016/j.drugalcdep.2011.10.013
70. Camera AA, Tomaselli V, Fleming J, Jabbar GA, Trachtenberg M, Galvez-Buccollini JA, et al. Correlates to the variable effects of Cannabis in young adults: a preliminary study. Harm Reduct J. (2012) 9:15.
71. Dragt S, Nieman DH, Schultze-Lutter F, van der Meer F, Becker H, de Haan L, et al. Cannabis use and age at onset of symptoms in subjects at clinical high risk for psychosis. Acta Psychiatr Scand. (2012) 125:45–53. doi: 10.1111/j.1600-0447.2011.01763.x
72. Fairman BJ, Anthony JC. Are early-onset Cannabis smokers at an increased risk of depression spells? J Affect Disord. (2012) 138:54–62. doi: 10.1016/j.jad.2011.12.031
73. Galvez-Buccollini JA, Proal AC, Tomaselli V, Trachtenberg M, Coconcea C, Chun J, et al. Association between age at onset of psychosis and age at onset of Cannabis use in non-affective psychosis. Schizophr Res. (2012) 139:157–60.
74. Horwood LJ, Fergusson DM, Coffey C, Patton GC, Tait R, Smart D, et al. Cannabis and depression: an integrative data analysis of four Australasian cohorts. Drug Alcohol Depend. (2012) 126:369–78. doi: 10.1016/j.drugalcdep.2012.06.002
75. Leeson VC, Harrison I, Ron MA, Barnes TR, Joyce EM. The effect of Cannabis use and cognitive reserve on age at onset and psychosis outcomes in first-episode schizophrenia. Schizophr Bull. (2012) 38:873–80. doi: 10.1093/schbul/sbq153
76. Rubino T, Zamberletti E, Parolaro D. Adolescent exposure to Cannabis as a risk factor for psychiatric disorders. J Psychopharmacol. (2012) 26:177–88.
77. Zeiger JS, Haberstick BC, Corley RP, Ehringer MA, Crowley TJ, Hewitt JK, et al. Subjective effects for alcohol, tobacco, and marijuana association with cross-drug outcomes. Drug Alcohol Depend. (2012) 123(Suppl. 1):S52–8. doi: 10.1016/j.drugalcdep.2012.02.014
78. Degenhardt L, Coffey C, Romaniuk H, Swift W, Carlin JB, Hall WD, et al. The persistence of the association between adolescent Cannabis use and common mental disorders into young adulthood. Addiction. (2013) 108:124–33. doi: 10.1111/j.1360-0443.2012.04015.x
79. Hill KP, Bennett HE, Griffin ML, Connery HS, Fitzmaurice GM, Subramaniam G, et al. Association of Cannabis use with opioid outcomes among opioid-dependent youth. Drug Alcohol Depend. (2013) 132:342–5. doi: 10.1016/j.drugalcdep.2013.02.030
80. Mackie CJ, O’Leary-Barrett M, Al-Khudhairy N, Castellanos-Ryan N, Struve M, Topper L, et al. Adolescent bullying, Cannabis use and emerging psychotic experiences: a longitudinal general population study. Psychol Med. (2013) 43:1033–44. doi: 10.1017/S003329171200205X
81. Osuch E, Vingilis E, Ross E, Forster C, Summerhurst C. Cannabis use, addiction risk and functional impairment in youth seeking treatment for primary mood or anxiety concerns. Int J Adolesc Med Health. (2013) 25:309–14.
82. Stefanis NC, Dragovic M, Power BD, Jablensky A, Castle D, Morgan VA. Age at initiation of Cannabis use predicts age at onset of psychosis: the 7-to 8-year trend. Schizophr Bull. (2013) 39:251–4. doi: 10.1093/schbul/sbs188
83. Baggio S, Studer J, Deline S, Mohler-Kuo M, Daeppen JB, Gmel G. The relationship between subjective experiences during first use of tobacco and Cannabis and the effect of the substance experienced first. Nicotine Tob Res. (2014) 16:84–92. doi: 10.1093/ntr/ntt116
84. Butterworth P, Slade T, Degenhardt L. Factors associated with the timing and onset of Cannabis use and Cannabis use disorder: results from the 2007 Australian National Survey of Mental Health and Well-Being. Drug Alcohol Rev. (2014) 33:555–64. doi: 10.1111/dar.12183
85. Moss HB, Chen CM, Yi HY. Early adolescent patterns of alcohol, cigarettes, and marijuana polysubstance use and young adult substance use outcomes in a nationally representative sample. Drug Alcohol Depend. (2014) 136:51–62. doi: 10.1016/j.drugalcdep.2013.12.011
86. Radhakrishnan R, Wilkinson ST, D’Souza DC. Gone to pot – A review of the association between Cannabis and psychosis. Front Psychiatry. (2014) 5:54. doi: 10.3389/fpsyt.2014.00054
87. Renard J, Krebs MO, Le Pen G, Jay TM. Long-term consequences of adolescent cannabinoid exposure in adult psychopathology. Front Neurosci. (2014) 8:361. doi: 10.3389/fnins.2014.00361
88. Silins E, Horwood LJ, Patton GC, Fergusson DM, Olsson CA, Hutchinson DM, et al. Young adult sequelae of adolescent Cannabis use: an integrative analysis. Lancet Psychiatry. (2014) 1:286–93. doi: 10.1016/S2215-0366(14)70307-4
89. Trape S, Charles-Nicolas A, Jehel L, Lacoste J. Early Cannabis use is associated with severity of cocaine-induced psychosis among cocaine smokers in Martinique, French West Indies. J Addict Med. (2014) 8:33–9. doi: 10.1097/ADM.0000000000000003
90. Wilkinson ST, Radhakrishnan R, D’Souza DC. Impact of Cannabis use on the development of psychotic disorders. Curr Addict Rep. (2014) 1:115–28.
91. Wu LT, Brady KT, Mannelli P, Killeen TK. Cannabis use disorders are comparatively prevalent among nonwhite racial/ethnic groups and adolescents: a national study. J Psychiatr Res. (2014) 50:26–35. doi: 10.1016/j.jpsychires.2013.11.010
92. Bechtold J, Simpson T, White HR, Pardini D. Chronic adolescent marijuana use as a risk factor for physical and mental health problems in young adult men. Psychol Addict Behav. (2015) 29:552–63.
93. Buu A, Dabrowska A, Heinze JE, Hsieh HF, Zimmerman MA. Gender differences in the developmental trajectories of multiple substance use and the effect of nicotine and marijuana use on heavy drinking in a high-risk sample. Addict Behav. (2015) 50:6–12. doi: 10.1016/j.addbeh.2015.06.015
94. Cloak CC, Alicata D, Ernst TM, Chang L. Psychiatric symptoms, salivary cortisol and cytokine levels in young marijuana users. J Neuroimmune Pharmacol. (2015) 10:380–90. doi: 10.1007/s11481-015-9606-0
95. Hall W. What has research over the past two decades revealed about the adverse health effects of recreational Cannabis use? Addiction. (2015) 110:19–35. doi: 10.1111/add.12703
96. Few LR, Grant JD, Nelson EC, Trull TJ, Grucza RA, Bucholz KK, et al. Cannabis involvement and nonsuicidal self-injury: a discordant twin approach. J Stud Alcohol Drugs. (2016) 77:873–80. doi: 10.15288/jsad.2016.77.873
97. Frascarelli M, Quartini A, Tomassini L, Russo P, Zullo D, Manuali G, et al. Cannabis use related to early psychotic onset: role of premorbid function. Neurosci Lett. (2016) 633:55–61. doi: 10.1016/j.neulet.2016.08.061
98. Henchoz Y, N’Goran AA, Baggio S, Deline S, Studer J, Gmel G. Associations of age at Cannabis first use and later substance abuse with mental health and depression in young men. J Subst Use. (2016) 21:85–91.
99. Kelley ME, Wan CR, Broussard B, Crisafio A, Cristofaro S, Johnson S, et al. Marijuana use in the immediate 5-year premorbid period is associated with increased risk of onset of schizophrenia and related psychotic disorders. Schizophr Res. (2016) 171:62–7. doi: 10.1016/j.schres.2016.01.015
100. Mokrysz C, Freeman TP, Korkki S, Griffiths K, Curran HV. Are adolescents more vulnerable to the harmful effects of Cannabis than adults? A placebo-controlled study in human males. Transl Psychiatry. (2016) 6:e961. doi: 10.1038/tp.2016.225
101. Ringen PA, Nesvag R, Helle S, Lagerberg TV, Lange EH, Loberg EM, et al. Premorbid Cannabis use is associated with more symptoms and poorer functioning in schizophrenia spectrum disorder. Psychol Med. (2016) 46:3127–36. doi: 10.1017/S0033291716001999
102. Wang JB, Ramo DE, Lisha NE, Cataldo JK. Medical marijuana legalization and cigarette and marijuana co-use in adolescents and adults. Drug Alcohol Depend. (2016) 166:32–8.
103. Albertella L, Le Pelley ME, Copeland J. Cannabis use in early adolescence is associated with higher negative schizotypy in females. Eur Psychiatry. (2017) 45:235–41. doi: 10.1016/j.eurpsy.2017.07.009
104. Borges G, Benjet C, Orozco R, Medina-Mora ME, Menendez D. Alcohol, Cannabis and other drugs and subsequent suicide ideation and attempt among young Mexicans. J Psychiatr Res. (2017) 91:74–82. doi: 10.1016/j.jpsychires.2017.02.025
105. Dierker L, Mendoza W, Goodwin R, Selya A, Rose J. Marijuana use disorder symptoms among recent onset marijuana users. Addict Behav. (2017) 68:6–13.
106. Green KM, Doherty EE, Ensminger ME. Long-term consequences of adolescent Cannabis use: examining intermediary processes. Am J Drug Alcohol Abuse. (2017) 43:567–75. doi: 10.1080/00952990.2016.1258706
107. Guttmannova K, Kosterman R, White HR, Bailey JA, Lee JO, Epstein M, et al. The association between regular marijuana use and adult mental health outcomes. Drug Alcohol Depend. (2017) 179:109–16.
108. Henry KL, Augustyn MB. Intergenerational continuity in Cannabis use: the role of parent’s early onset and lifetime disorder on child’s early onset. J Adolesc Health. (2017) 60:87–92. doi: 10.1016/j.jadohealth.2016.09.005
109. Jones JD, Calkins ME, Scott JC, Bach EC, Gur RE. Cannabis use, polysubstance use, and psychosis spectrum symptoms in a community-based sample of U.S. youth. J Adolesc Health. (2017) 60:653–9. doi: 10.1016/j.jadohealth.2017.01.006
110. Levine A, Clemenza K, Rynn M, Lieberman J. Evidence for the risks and consequences of adolescent Cannabis exposure. J Am Acad Child Adolesc Psychiatry. (2017) 56:214–25.
111. McHugh MJ, McGorry PD, Yung AR, Lin A, Wood SJ, Hartmann JA, et al. Cannabis-induced attenuated psychotic symptoms: implications for prognosis in young people at ultra-high risk for psychosis. Psychol Med. (2017) 47:616–26. doi: 10.1017/S0033291716002671
112. Savage RJ, King VL, Clark CB, Cropsey KL. Factors associated with early marijuana initiation in a criminal justice population. Addict Behav. (2017) 64:82–8. doi: 10.1016/j.addbeh.2016.08.005
113. Schuster RM, Fontaine M, Nip E, Zhang H, Hanly A, Evins A. Prolonged Cannabis withdrawal in young adults with lifetime psychiatric illness. Prev Med. (2017) 104:40–5. doi: 10.1016/j.ypmed.2017.02.019
114. Shah D, Chand P, Bandawar M, Benegal V, Murthy P. Cannabis induced psychosis and subsequent psychiatric disorders. Asian J Psychiatry. (2017) 30:180–4. doi: 10.1016/j.ajp.2017.10.003
115. Hawke LD, Koyama E, Henderson J. Cannabis use, other substance use, and co-occurring mental health concerns among youth presenting for substance use treatment services: sex and age differences. J Subst Abuse Treat. (2018) 91:12–9. doi: 10.1016/j.jsat.2018.05.001
116. Jones HJ, Gage SH, Heron J, Hickman M, Lewis G, Munafo MR, et al. Association of combined patterns of tobacco and Cannabis use in adolescence with psychotic experiences. JAMA Psychiatry. (2018) 75:240–6. doi: 10.1001/jamapsychiatry.2017.4271
117. Padovano HT, Miranda R. Subjective Cannabis effects as part of a developing disorder in adolescents and emerging adults. J Abnorm Psychol. (2018) 127:282–93. doi: 10.1037/abn0000342
118. Rioux C, Castellanos-Ryan N, Parent S, Vitaro F, Tremblay RE, Seguin JR. Age of Cannabis use onset and adult drug abuse symptoms: a prospective study of common risk factors and indirect effects. Can J Psychiatry. (2018) 63:457–64. doi: 10.1177/0706743718760289
119. Schoeler T, Theobald D, Pingault JB, Farrington DP, Coid JW, Bhattacharyya S. Developmental sensitivity to Cannabis use patterns and risk for major depressive disorder in mid-life: findings from 40 years of follow-up. Psychol Med. (2018) 48:2169–76. doi: 10.1017/S0033291717003658
120. Bravo AJ, Weinstein AP, Pearson MR, Protective Strategies Study Team. The relationship between risk factors and alcohol and marijuana use outcomes among concurrent users: a comprehensive examination of protective behavioral strategies. J Stud Alcohol Drugs. (2019) 80:102–8. doi: 10.15288/jsad.2019.80.102
121. Curran HV, Hindocha C, Morgan CJA, Shaban N, Das RK, Freeman TP. Which biological and self-report measures of Cannabis use predict Cannabis dependency and acute psychotic-like effects? Psychol Med. (2019) 49:1574–80.
122. Han B, Compton WM, Blanco C, Jones CM. Time since first Cannabis use and 12-month prevalence of Cannabis use disorder among youth and emerging adults in the United States. Addiction. (2019) 114:698–707.
123. Johnson EC, Tillman R, Aliev F, Meyers JL, Salvatore JE, Anokhin AP, et al. Exploring the relationship between polygenic risk for Cannabis use, peer Cannabis use and the longitudinal course of Cannabis involvement. Addiction. (2019) 114:687–97. doi: 10.1111/add.14512
124. Krebs MO, Kebir O, Jay TM. Exposure to cannabinoids can lead to persistent cognitive and psychiatric disorders. Eur J Pain. (2019) 23:1225–33.
125. Leadbeater BJ, Ames ME, Linden-Carmichael AN. Age-varying effects of Cannabis use frequency and disorder on symptoms of psychosis, depression and anxiety in adolescents and adults. Addiction. (2019) 114:278–93. doi: 10.1111/add.14459
126. Mader J, Smith JM, Afzal AR, Szeto ACH, Winters KC. Correlates of lifetime Cannabis use and Cannabis use severity in a Canadian university sample. Addict Behav. (2019) 98:106015.
127. Yucens B, Kotan VO, Okay IT, Goka E. The severity of dissociative symptoms among patients with Cannabis and synthetic cannabinoid use disorder: association with substance use characteristics and suicide. Psychiatry Clin Psychopharmacol. (2019) 29:603–8.
128. Boden JM, Dhakal B, Foulds JA, Horwood LJ. Life-course trajectories of Cannabis use: a latent class analysis of a New Zealand birth cohort. Addiction. (2020) 115:279–90.
129. Choi NG, DiNitto DM, Choi BY. Prescription pain reliever use and misuse among Cannabis users aged 50+ years. Clin Gerontol. (2020) 44:53–65. doi: 10.1080/07317115.2020.1757540
130. Dunbar MS, Davis JP, Tucker JS, Seelam R, Shih RA, D’Amico EJ. Developmental trajectories of tobacco/nicotine and Cannabis use and patterns of product co-use in young adulthood. Tob Use Insights. (2020) 13:1179173X20949271 doi: 10.1177/1179173X20949271
131. Gicas KM, Cheng A, Panenka WJ, Kim DD, Yau JC, Procyshyn RM, et al. Differential effects of Cannabis exposure during early versus later adolescence on the expression of psychosis in homeless and precariously housed adults. Prog Neuropsychopharmacol Biol Psychiatry. (2020) 106:110084. doi: 10.1016/j.pnpbp.2020.110084
132. Hengartner MP, Angst J, Ajdacic-Gross V, Rossler W. Cannabis use during adolescence and the occurrence of depression, suicidality and anxiety disorder across adulthood: findings from a longitudinal cohort study over 30 years. J Affect Disord. (2020) 272:98–103. doi: 10.1016/j.jad.2020.03.126
133. Meier MH, Beardslee J, Pardini D. Associations between recent and cumulative Cannabis use and internalizing problems in boys from adolescence to young adulthood. J Abnorm Child Psychol. (2020) 48:771–82. doi: 10.1007/s10802-020-00641-8
134. Mokrysz C, Shaban NDC, Freeman TP, Lawn W, Pope RA, Hindocha C, et al. Acute effects of Cannabis on speech illusions and psychotic-like symptoms: two studies testing the moderating effects of cannabidiol and adolescence. Psychol Med. (2020) 51:2134–42. doi: 10.1017/S0033291720001038
135. Reboussin BA, Rabinowitz JA, Thrul J, Maher B, Green KM, Ialongo NS. Trajectories of Cannabis use and risk for opioid misuse in a young adult urban cohort. Drug Alcohol Depend. (2020) 215:108182. doi: 10.1016/j.drugalcdep.2020.108182
136. Scheier LM, Griffin KW. Youth marijuana use: a review of causes and consequences. Curr Opin Psychol. (2020) 38:11–8.
137. Stanley LR, Swaim RC, Smith JK, Conner BT. Early onset of Cannabis use and alcohol intoxication predicts prescription drug misuse in American Indian and non-American Indian adolescents living on or near reservations. Am J Drug Alcohol Abuse. (2020) 46:447–53.
138. Mane A, Berge D, Penzol MJ, Parellada M, Bioque M, Lobo A, et al. Cannabis use, COMT, BDNF and age at first-episode psychosis. Psychiatry Res. (2017) 250:38–43. doi: 10.1016/j.psychres.2017.01.045
140. Fergusson DM, Horwood LJ. Cannabis use and dependence in a New Zealand birth cohort. N Z Med J. (2000) 113:156–8.
141. Fergusson DM, Horwood LJ, Swain-Campbell N. Cannabis use and psychosocial adjustment in adolescence and young adulthood. Addiction. (2002) 97:1123–35. doi: 10.1046/j.1360-0443.2002.00103.x
142. Fergusson DM, Lynskey MT, Horwood LJ. The short-term consequences of early onset Cannabis use. J Abnorm Child Psychol. (1996) 24:499–512. doi: 10.1007/BF01441571
143. Fergusson DM, Horwood LJ. Early onset Cannabis use and psychosocial adjustment in young adults. Addiction. (1997) 92:279–96.
144. Chen K, Kandel DB. Predictors of cessation of marijuana use: an event history analysis. Drug Alcohol Depend. (1998) 50:109–21. doi: 10.1016/s0376-8716(98)00021-0
145. Lynskey MT, Agrawal A, Henders A, Nelson EC, Madden PAF, Martin NG. An Australian twin study of Cannabis and other illicit drug use and misuse, and other psychopathology. Twin Res Hum Genet. (2012) 15:631–41. doi: 10.1017/thg.2012.41
146. Patton GC, Coffey C, Carlin JB, Degenhardt L, Lynskey M, Hall W. Cannabis use and mental health in young people: cohort study. BMJ. (2002) 325:1195. doi: 10.1136/bmj.325.7374.1195
147. Valmaggia LR, Day FL, Jones C, Bissoli S, Pugh C, Hall D, et al. Cannabis use and transition to psychosis in people at ultra-high risk. Psychol Med. (2014) 44:2503–12. doi: 10.1017/S0033291714000117
148. Madruga CS, Miguel AQC, Massaro LTDS, Caetano R, Laranjeira R. Cannabis consumption onset and addiction: data from the second Brazilian Drugs and Alcohol Survey (BNADS). J Psychoactive Drugs. (2021) 54:140–8. doi: 10.1080/02791072.2021.1936700
149. Copeland WE, Hill SN, Shanahan L. Adult psychiatric, substance, and functional outcomes of different definitions of early Cannabis use. J Am Acad Child Adolesc Psychiatry. (2021) 17:17. doi: 10.1016/j.jaac.2021.07.824
150. Arseneault L, Cannon M, Poulton R, Murray R, Caspi A, Moffitt TE. Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study. BMJ. (2002) 325:1212–3. doi: 10.1136/bmj.325.7374.1212
151. Swift W, Coffey C, Carlin JB, Degenhardt L, Patton GC. Adolescent Cannabis users at 24 years: trajectories to regular weekly use and dependence in young adulthood. Addiction. (2008) 103:1361–70.
152. Dervaux A, Krebs MO, Laqueille X. [Cannabis-induced cognitive and psychiatric disorders]. Bull Acad Natl Med. (2014) 198:559–74; discussion75–7.
153. Chabrol H, Duconge E, Roura C, Casas C. Relations between anxious, depressive and borderline symptomatology and frequency of Cannabis use and dependence. Encephale. (2004) 30:141–6. doi: 10.1016/s0013-7006(04)95424-3
154. Chabrol H, Fredaigue N, Callahan S. Epidemiological study of Cannabis abuse and dependence among 256 adolescents. [French]. Encephale. (2000) 26:47–9.
155. Cuenca-Royo AM, Torrens M, Sanchez-Niubo A, Suelves JM, Domingo-Salvany A. Psychiatric morbidity among young-adults Cannabis users. Adicciones. (2013) 25:45–54.
156. Han BH, Palamar JJ. Marijuana use by middle-aged and older adults in the United States, 2015-2016. Drug Alcohol Depend. (2018) 191:374–81.
157. Burgdorf JRKB, Pacula RL. Heterogeneity in the composition of marijuana seized in California. Drug Alcohol Depend. (2011) 117:59–61. doi: 10.1016/j.drugalcdep.2010.11.031
158. Dujourdy LBF. A study of Cannabis potency in France over a 25 years period (1992-2016). Forensic Sci Int. (2017) 272:72–80. doi: 10.1016/j.forsciint.2017.01.007
159. ElSohly MAMZ, Foster S, Gon C, Chandra S, Church JC. Changes in Cannabis potency over the last 2 decades (1995-2014): analysis of current data in the United States. Biol Psychiatry. (2016) 79: 613–9.
160. Wilson JFT, Mackie CJ. Effects of increasing Cannabis potency on adolescent health. Lancet Child Adolesc Health. (2019) 3:121–8.
161. Hudson AHP. Risk factors for Cannabis-related mental health harms in older adults: a review. Clin Gerontol. (2021) 44:3–15. doi: 10.1080/07317115.2020.1808134
162. Hurd YL, Manzoni OJ, Pletnikov MV, Lee FS, Bhattacharyya S, Melis M. Cannabis and the developing brain: insights into its long-lasting effects. J Neurosci. (2019) 39:8250–8. doi: 10.1523/JNEUROSCI.1165-19.2019
163. Guxens MNM, Ariza C, Ochoa D. Factors associated with the onset of Cannabis use: a systematic review of cohort studies. Gac Sanit. (2007) 21:252–60. doi: 10.1157/13106811
164. Kohn LKF, Piette D. Peer, family integration and other determinants of Cannabis use among teenagers. Int J Adolesc Med Health. (2004) 16:359–70. doi: 10.1515/ijamh.2004.16.4.359
165. Fischer B, Robinson T, Bullen C, Curran V, Jutras-Aswad D, Medina-Mora ME, et al. Lower-risk Cannabis use guidelines (LRCUG) for reducing health harms from non-medical Cannabis use: a comprehensive evidence and recommendations update. Int J Drug Policy. (2022) 99:103381. doi: 10.1016/j.drugpo.2021.103381
Keywords: addictive behavior, adolescent, adult, cannabis, mental health
Citation: Kaur N, Bastien G, Gagnon L, Graham J, Mongeau-Pérusse V, Bakouni H, Morissette F, Theriault C, Fischer B and Jutras-Aswad D (2022) Variations of cannabis-related adverse mental health and addiction outcomes across adolescence and adulthood: A scoping review. Front. Psychiatry 13:973988. doi: 10.3389/fpsyt.2022.973988
Received: 20 June 2022; Accepted: 20 September 2022;
Published: 10 October 2022.
Edited by:
Yasser Khazaal, Université de Lausanne, SwitzerlandReviewed by:
Ulrich W. Preuss, Martin Luther University of Halle-Wittenberg, GermanyUdo Bonnet, Castrop-Rauxel Evangelical Hospital, Germany
Copyright © 2022 Kaur, Bastien, Gagnon, Graham, Mongeau-Pérusse, Bakouni, Morissette, Theriault, Fischer and Jutras-Aswad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Didier Jutras-Aswad, ZGlkaWVyLmp1dHJhcy1hc3dhZEB1bW9udHJlYWwuY2E=
†ORCID: Navdeep Kaur, orcid.org/0000-0002-3448-7633; Gabriel Bastien, orcid.org/0000-0002-7969-9998; Lea Gagnon, orcid.org/0000-0002-5300-7578; Violaine Mongeau-Pérusse, orcid.org/0000-0001-8516-2620; Hamzah Bakouni, orcid.org/0000-0001-5403-380X; Florence Morissette, orcid.org/0000-0002-9535-2353; Benedikt Fischer, orcid.org/0000-0002-2186-4030; Didier Jutras-Aswad, orcid.org/0000-0002-8474-508X