 Veronica Nisticò1,2,3†
Veronica Nisticò1,2,3† Adriano Iacono1†
Adriano Iacono1† Diana Goeta4Roberta Tedesco1Barbara Giordano5Raffaella Faggioli5
Diana Goeta4Roberta Tedesco1Barbara Giordano5Raffaella Faggioli5 Alberto Priori1,2,6
Alberto Priori1,2,6 Orsola Gambini1,2,5
Orsola Gambini1,2,5 Benedetta Demartini1,2,5*
Benedetta Demartini1,2,5*- 1Dipartimento di Scienze della Salute, Università degli Studi di Milano, Milan, Italy
- 2“Aldo Ravelli” Research Center for Neurotechnology and Experimental Brain Therapeutics, University of Milan, Milan, Italy
- 3Dipartimento di Psicologia, Università degli Studi di Milano-Bicocca, Milan, Italy
- 4Unità di Psichiatria, Presidio San Carlo, Azienda Socio-Sanitaria Territoriale (ASST) Santi Paolo e Carlo, Milan, Italy
- 5Unità di Psichiatria 52, Presidio San Paolo, Azienda Socio-Sanitaria Territoriale (ASST) Santi Paolo e Carlo, Milan, Italy
- 6III Clinica Neurologica, Presidio San Paolo, Azienda Socio-Sanitaria Territoriale (ASST) Santi Paolo e Carlo, Milan, Italy
Autism spectrum disorders (ASDs) and functional neurological disorders (FNDs) share some clinical characteristics such as alexithymia, sensory sensitivity and interoceptive issues. Recent evidence shows that both the disorders present symptoms compatible with a diagnosis of hypermobile Ehlers-Danlos Syndrome and hypermobile spectrum disorders (hEDS/HSD), a heterogeneous group of heritable connective tissue disorders characterized by joint hypermobility, skin hyperextensibility, and tissue fragility. Here we compared the prevalence of hEDS/HSD-related symptoms in a group of patients with FNDs, of people with ASDs without intellectual disabilities, and a non-clinical comparison group (NC). Twenty patients with FNDs, 27 individuals with ASDs without intellectual disabilities and 26 NC were recruited and completed the Self-reported screening questionnaire for the assessment of hEDS/HSD-related symptoms (SQ-CH). We found that 55% of the patients with FNDs, 44.4% of the individuals with ASDs and 30.8% of NC scored above the cut-off at the SQ-CH; SQ-CH scores of both FNDs and ASDs group were significantly higher than the NC group's ones. In conclusion, both ASDs and FNDs individuals present hEDS/HSD-related symptoms in a higher number than the general population. Imputable mechanisms include (i) overwhelming of executive functions with consequent motor competence impairment for ASDs individuals, and (ii) exacerbation of FNDs symptoms by physical injury and chronic pain due to abnormal range of joint mobility. Moreover, we speculated that the amygdala and the anterior cingulate cortex circuitry might be responsible for the imbalances at the proprioceptive, interoceptive, and emotional levels.
Introduction
Autism spectrum disorders (ASDs) and functional neurological disorders (FNDs) are two relatively common neuropsychiatric conditions, both affecting childhood and adulthood. ASDs refer to a group of neurodevelopmental disorders whose core features concern persistent deficits in social communication and social interaction, and restricted, repetitive patterns of behavior, interests, or activities (1); FNDs consist of symptoms of altered voluntary motor or sensory function that cannot be explained by recognized neurological or medical conditions (1). Despite being apparently separate clinical entities, previous studies showed that ASDs and FNDs share some common clinical and psychopathological features, in terms of alexithymia (difficulties in recognizing one's own emotion at a cognitive level) (2, 3), interoception (the perception of the states and signals coming from within the body) (4–7), and sensory over-responsivity (the excessive or protracted negative response to sensory stimuli), which is known to be a key trait of ASDs (1, 8) and has been recently described also in individuals with a diagnosis of FNDs (9). In a recent paper, we discussed the literature assessing the comorbidity between FNDs and ASDs and showed that the incidence of functional neurological symptoms in a group of adults with ASDs without intellectual disabilities was significantly higher than in a group of healthy neurotypical adults (10). Previous studies also suggest that both the disorders display increased evidence of symptoms compatible with a diagnosis of hypermobile Ehlers-Danlos Syndrome and hypermobile spectrum disorders (hEDS/HSD), (formerly known as Joint Hypermobility Syndrome—JHS) (11–14). The Ehlers–Danlos syndromes (EDS) represent a clinically and genetically heterogeneous group of heritable connective tissue diseases sharing some common features such as joint hypermobility, skin hyperextensibility, and tissue fragility. Since collagen is thoroughly distributed through the body, the manifestations of EDS are multi-systemic and often accompanied by painful sensations. The International EDS consortium now recognizes thirteen subtypes of EDS/HSD (15). Concerning hypermobile EDS (hEDS), despite being the most common EDS subtype, a genetic cause has not been verified yet. Patients with symptomatic joint hypermobility not fulfilling the diagnostic criteria for hEDS are now considered under the umbrella of “hypermobility spectrum disorders” (HSD) (16). Both hEDS and HSD can be associated with functional, extra-musculoskeletal manifestations, such as chronic fatigue, various dysautonomic features, immune system alterations, cognitive disturbances (such as “brain fog”), and psychological distress (17). The case-control study by Bulbena et al. (18) paved the way to several studies investigating the association between EDS and psychiatric disorders. They found that a clinical group composed by hypermobile individuals (i.e., with a positive Beighton Score, a widely used screening test for hEDS) presented a significantly higher rate of panic disorder, agoraphobia, and simple phobia than a group of non-hypermobile individuals (i.e., negative Beighton Score). It is currently known that individuals with hypermobility are up to seven times overrepresented among those with panic or anxiety disorders and exhibited a four times greater probability of manifesting anxiety (19). Moreover, women with hypermobility present higher levels of anxiety than hypermobile men. Other disorders found to be associated with generalized joint hypermobility were depression, schizophrenia, attention deficit hyperactivity disorder, and personality disorders (20).
Aim of this study was to evaluate the prevalence of hEDS/HSD-related symptoms in patients with FNDs, individuals with ASDs without intellectual disabilities, and in a non-clinical comparison group (NC).
Methods
Participants
Twenty consecutive patients affected by FNDs and 27 consecutive individuals with ASDs without intellectual disabilities were recruited at the tertiary level neuropsychiatric outpatient clinic of our hospital. Diagnosis of FNDs was made according to DSM-5 diagnostic criteria by a neurologist and a psychiatrist. Diagnosis of ASDs was formulated by a psychiatrist and a psychologist according to DSM-5 criteria (1) and the Module 4 of the Autism Diagnostic Observation Schedule-−2nd version (ADOS-2) (21). The control group was composed by 26 NC individuals, recruited via word-of-mouth amongst hospital staff and their acquaintances; their “health state” was assessed through a detailed clinical interview, although they did not undergo any official screening for neuropsychiatric conditions. Exclusion criteria were: (i) age below 18 years; (ii) inability to understand the researcher's instruction or to complete questionnaires because of language difficulties, cognitive disabilities (I.Q. < 70) or dementia; (iii) presence of other severe neurological or medical conditions. The study was approved by the local Ethics Committee. All participants signed an online-written informed consent form.
Materials
First, demographic and clinical information was obtained by an online questionnaire. Thereafter, each participant completed the Self-reported screening questionnaire for the assessment of Joint Hypermobility Syndrome (SQ-CH) (22), a seven-item instrument including the Hakim and Grahame's five criteria (23) and two additional ones. Each item is presented in a dichotomy format (i.e., participants can only answer “yes” or “no”) and one point is given for each criteria answered affirmatively, hence the Total Score can range from 0 to 7 points. The items consider the entire life of the patient, such as: “As a child you could, or have you ever been able (even now) to place your palms on the ground without bending your knees?”; for this reason, in this study we analyzed possible differences between groups controlling for gender only, and not for age. The SQ-CH has been created as a screening tool to facilitate the HSD diagnosis, which requires a high sensitivity and temporal stability. The SQ-CH is validated only in Spanish: the Italian translation was done by means of a forward and back-translation by an independent translator, blind to the aim of our study. Correlation between the instrument and the widely used Beighton's criteria is high (r = 0.9; p < 0.001); the cut-off point is established at 3, with a sensitivity of 0.78 and a specificity of 0.24 (22).
Statistical analysis
Power analysis was conducted with G.Power 3.1.
Statistical analysis was conducted with SPSS 27 (Statistical Package for Social Sciences). Significance level was set at p ≤ 0.05, all tests were 2-tailed. First, descriptive statistics were calculated for each group. To assess whether groups were balanced for age and gender, univariate ANOVA and χ2 analysis were run, respectively. Second, univariate ANOVA with “Group” and “Gender” as factors and the Total Score of the SQ-CH questionnaire as dependent variable was run; to investigate specific differences between the three groups, Tukey's post-hoc analyses were implemented.
Results
Samples were matched for gender [χ(2) = 5.73; p = 0.057] and age [F(2, 70) = 2.73; p = 0.072]. FND symptoms included: 3 functional weakness; 2 jerks; 1 functional weakness with jerks; 1 functional tremor; 1 functional dystonia; 2 functional gait disorder; 10 Psychogenic non-epileptic seizures (PNES) (Table 1 for further demographic and clinical details about FND group). Psychiatric comorbidity for the ASD group included: 1 Major Depressive Disorder (MDD); 1 MDD and obsessive-compulsive disorder (OCD); 1 MDD and eating disorder; 1 bipolar disorder; 2 anxious-depressive syndrome; 1 Anorexia Nervosa and OCD; 1 dyslexia.

Table 1. Demographic and clinical information for patients with FNDs.
Eleven participants with FNDs, 14 with ASDs, and 8 NC scored above the cut-off for the SQ-CH (Table 2 for further details). At the SQ-CH total score, a significant main effect of group emerged [F(2, 67) = 4.03, p = 0.022], with both FNDs (p = 0.039) and ASDs (p = 0.043) patients showing more hEDS/HSD-related symptoms than NC, but no difference between FNDs and ASDs participants (p = 0.970; Figure 1). Moreover, a significant main effect of gender emerged [F(1, 67) = 5.12, p = 0.027], with females (mean score = 2.85, SD = 1.35) scoring significantly higher than males (mean score = 1.63, SD = 1.57) at the JHS questionnaire. No significant interaction effect existed between group and gender [F(2, 67) = 1.62; p = 0.21].

Table 2. Demographic and clinical information for FNDs, ASDs and NC groups.
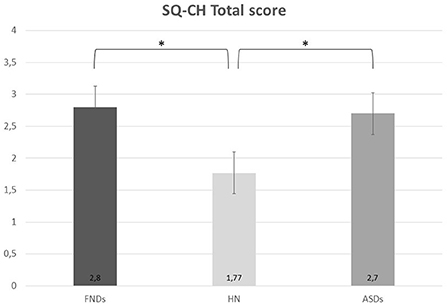
Figure 1. Scores of FNDs, ASDs, and NC groups at the SQ-CH questionnaire. ASDs, autism spectrum disorders; FNDs, functional neurological disorders; NC, non-clinical comparison group. *p < 0.05.
Discussion
The purpose of the study was to assess the presence of hEDS/HSD-related symptoms in a sample of patient with FNDs and a group of individuals diagnosed with ASDs. Results showed that both FNDs and ASDs group scored significantly higher than the NC group at the SQ-CH, hence presenting a higher number of hEDS/HSD-related symptoms; no difference emerged between FNDs and ASDs.
A significant main effect of gender was noted as well, with females scoring significantly higher than males. The latter finding is consistent with the current literature: as previously stated, the incidence of HSD is significantly higher in women than men, although the reason remains poorly understood (16, 17).
With respect to the relationship between ASDs and HSD, Cederlöf et al. (12) performed a population study investigating a possible association between EDS and psychiatric disorders: hypermobile disorders individuals (including EDS) showed a 1.4 increase in relative likelihood for ASDs occurrence; strikingly, EDS alone individuals had a 7-fold higher chance to co-manifest ASDs. Baeza-Velasco et al. (13) found that some features of hEDS/HSD embraced some peculiar traits of the ASD spectrum in terms of social skills, internalizing difficulties, and behaviors. Neurodevelopmental comorbidities frequently co-occur in EDS, especially impaired proprioception (24). Baeza-Velasco et al. (13) claim that, to maintain motor competence despite proprioceptive impairment, executive function may result overwhelmed, leading to some symptoms of ADHD, which is the most common co-occurring psychiatric disorder in ASDs (1). Moreover, pain and dysautonomia, frequently experienced by patients with EDS/HSD, have also been associated with cognitive deficits in attention and concentration. Thus, some characteristics present in EDS/HSD, such as hypermobility, dysautonomia, chronic pain, and proprioceptive impairment, may have consequences in terms of motor, cognitive, and behavioral skills, and may ultimately affect neurodevelopment.
Little is known about the association between FNDs and hEDS/HSD. Kassavetis et al. (11) were amongst the first postulating it, starting from the concept that HSD was linked with psychiatric disorders and other medical conditions whose pathogenesis has not been completely elucidated, including panic disorder, anxiety, irritable bowel syndrome, chronic fatigue syndrome, and fibromyalgia; moreover, they found a 2-fold increase in the incidence of HSD in their cohort of patients with functional movement disorders (FMD) suffering from dystonia. Delgado et al. (14) described the clinical and demographic characteristics of patients with FMD: among other findings, 21% of patients had clinical features suggestive of joint hypermobility, especially those with fixed limb dystonia. It was suggested that aberrant range of joint mobility can lead to physical injury, chronic pain and maladaptive maneuvers, and thus joint hypermobility may be a significant factor in the pathophysiology of fixed dystonia (14, 25). In a recent study by Koreki et al. (26), joint hypermobility was significantly associated with Functional Seizures, also known as psychogenic non-epileptic seizures (PNES), and the association was independent of their anxiety, depression, and other demographic factors such as age, sex, education, and BMI.
Neuroimaging comes into play in ideally explaining these different associations. Neural correlates found to be implicated in HSD are similar to those reported in the above-mentioned psychiatric disturbances, especially in the field of anxiety, alexithymia, and interoception abnormalities: Eccles et al., in a neuroimaging study (27) have found that bilateral amygdala volume was significantly greater in a group of hypermobile patient compared to a group of non-hypermobile individuals; additionally, the same hypermobility group scored higher for interoceptive sensitivity, suggesting a more finely tuned sensory representation of internal bodily signals, and showed a trend toward significantly higher levels of anxiety. These findings suggest amygdala as a likely neural substrate mediating the association between hypermobility, anxiety, and psychosomatic conditions. The hypermobility group showed structural differences within anterior cingulate cortex, a central driver of autonomic arousal and a region implicated in the cognitive control of pain and negative emotions. Mallorquí-Bagué et al. (28) suggest that interoceptive sensitivity mediates the relationship between state anxiety and generalized joint hypermobility. Also, these subjects show increased neural reactivity to sad and angry scenes within brain regions implicated in emotional processing, compared to non-hypermobile subjects, especially in the insular cortex as the common substrate between interoception and emotions. Hence, we might speculate that abnormal signal integration at the level of the circuit involving amygdala, insula, and anterior cingulate cortex might be responsible for the proprioceptive, interoceptive, and emotional imbalances present in the condition, leading to its manifestations. Such speculations, in line with those postulated by Koreki et al. (26), who proposed differences in autonomic control, interoception, and brain structure, associated with joint hypermobility, may predispose patients to Functional Seizures.
Studies on the psychiatric correlates of HSD are in their infancy; this study adds a further piece of evidence to the general framework of the issue, though preliminarily. The major limitations of this study are: the limited sample size; the fact that our control group was not thoroughly screened for neuropsychiatric conditions, but only undergo a detailed clinical interview; the fact that the SQ-CH is not validated in Italian yet; the fact that all data are self-reported and need additional confirmation; further studies should confirm these preliminary data to rule out a chance association. Moreover, future studies with a larger sample size might take into account ASDs comorbidities, to understand whether hEDS/HSD is associated with ASDs subtypes.
Conclusion
In conclusion, this study provides preliminary evidence that both FNDs and ASDs patients present hEDS/HSD-related symptoms more frequently than the general population; a significant main effect of gender, with women scoring higher than men, has also been noticed. Since the reason underlying the association between hEDS/HSD and psychiatric disorders remains poorly substantiated, future studies are needed to elucidate the potential mechanisms underlying it.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by ASST Santi Paolo e Carlo. The patients/participants provided their written informed consent to participate in this study.
Author contributions
VN, AI, DG, RF, and BD contributed to conception and design of the study. VN, AI, RT, and BG collected the data and organized the database. VN and AI performed the statistical analysis. VN, AI, and DG wrote the first draft of the manuscript. RF, AP, OG, and BD revised the manuscript for intellectual content. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
This work was partially supported by “Aldo Ravelli” Research Center for Neurotechnology and Experimental Brain Therapeutics, Università degli Studi di Milano, Milano, Italy.
Acknowledgments
The authors acknowledge support from the University of Milan through the APC initiative.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th ed. Washington, DC: American Psychiatric Association (2013).
2. Demartini B, Petrochilos P, Ricciardi L, Price G, Edwards MJ, Joyce E. The role of alexithymia in the development of functional motor symptoms (conversion disorder). J Neurol Neurosurg Psychiatry. (2014) 85:1132–7. doi: 10.1136/jnnp-2013-307203
3. Kinnaird E, Stewart C, Tchanturia K. Investigating alexithymia in autism: a systematic review and meta-analysis. Eur Psychiatry. (2019) 55:80–9. doi: 10.1016/j.eurpsy.2018.09.004
4. Quattrocki E, Friston K. Autism, oxytocin and interoception. Neurosci Biobehav Rev. (2014) 47:410–30. doi: 10.1016/j.neubiorev.2014.09.012
5. DuBois D, Ameis SH, Lai MC, Casanova MF, Desarkar P. Interoception in autism spectrum disorder: a review. Int J Dev Neurosci. (2016) 52:104–11. doi: 10.1016/j.ijdevneu.2016.05.001
6. Ricciardi L, Demartini B, Crucianelli L, Krahé C, Edwards MJ, Fotopoulou A. Interoceptive awareness in patients with functional neurological symptoms. Biol Psychol. (2016) 113:68–74. doi: 10.1016/j.biopsycho.2015.10.009
7. Ricciardi L, Nisticò V, Andrenelli E, Cunha JM, Demartini B, Kirsch LP, et al. Exploring three levels of interoception in people with functional motor disorders. Parkinsonism Relat Disord. (2021) 86:15–8. doi: 10.1016/j.parkreldis.2021.03.029
8. Green SA, Hernandez L, Tottenham N, Krasileva K, Bookheimer SY, Dapretto M. Neurobiology of sensory overresponsivity in youth with autism spectrum disorders. JAMA psychiatry. (2015) 72:778–86. doi: 10.1001/jamapsychiatry.2015.0737
9. Ranford J, MacLean J, Alluri PR, Comeau O, Godena E, LaFrance WC Jr, et al. Perez DL. Sensory processing difficulties in functional neurological disorder: a possible predisposing vulnerability? Psychosomatics. (2020) 61:343–52. doi: 10.1016/j.psym.2020.02.003
10. Nisticò V, Goeta D, Iacono A, Tedesco R, Giordano B, Faggioli R, et al. Clinical overlap between functional neurological disorders and autism spectrum disorders: a preliminary study. Neurol Sci. (2022) 5:1–7. doi: 10.1007/s10072-022-06048-1
11. Kassavetis P, Batla A, Pareés I, Saifee TA, Schrag A, Cordivari C, et al. Edwards MJ. Joint hypermobility syndrome: a risk factor for fixed dystonia? Mov Disord. (2012) 27:1070. doi: 10.1002/mds.25004
12. Cederlöf M, Larsson H, Lichtenstein P, Almqvist C, Serlachius E, Ludvigsson JF. Nationwide population-based cohort study of psychiatric disorders in individuals with Ehlers–Danlos syndrome or hypermobility syndrome and their siblings. BMC Psychiatry. (2016) 16:1–7. doi: 10.1186/s12888-016-0922-6
13. Baeza-Velasco C, Cohen D, Hamonet C, Vlamynck E, Diaz L, Cravero C, et al. Autism, joint hypermobility-related disorders and pain. Front Psychiatry. (2018) 9:656. doi: 10.3389/fpsyt.2018.00656
14. Delgado C, Kurtis M, Martin B, Rada P, Martinez L, Sanz M, et al. Clinical and demographic characteristics of patients with functional movement disorders: a consecutive cohort study from a specialized clinic. Acta Neurol Belg. (2022) 122:97–103. doi: 10.1007/s13760-021-01648-8
15. Malfait F, Francomano C, Byers P, Belmont J, Berglund B, Black J, et al. The 2017 international classification of the Ehlers–Danlos syndromes. Am J Med Genet C Semin Med Genet. (2017) 175:8–26. doi: 10.1002/ajmg.c.31547
16. Castori M, Tinkle B, Levy H, Grahame R, Malfait F, Hakim A, et al. framework for the classification of joint hypermobility and related conditions. Am J Med Genet C Semin Med Genet. (2017) 175:148–57. doi: 10.1002/ajmg.c.31539
17. Malfait F, Castori M, Francomano CA, Giunta C, Tomoki K, Byers P H. The Ehlers-Danlos syndromes. Nat Rev Dis Prim. (2020) 6:64. doi: 10.1038/s41572-020-0194-9
18. Bulbena A, Duró JC, Porta M, Martín-Santos R, Mateo A, Molina L, et al. Anxiety disorders in the joint hypermobility syndrome. Psychiatry Res. (1993) 46:59–68. doi: 10.1016/0165-1781(93)90008-5
19. Smith TO, Easton V, Bacon H, Jerman E, Armon K, Poland F, et al. Original article The relationship between benign joint hypermobility syndrome and psychological distress: a systematic review and meta-analysis. Rheumatology. (2014) 53:114–22. doi: 10.1093/rheumatology/ket317
20. Sinibaldi L, Ursini G, Castori M. Psychopathological manifestations of joint hypermobility and joint hypermobility syndrome/ Ehlers-Danlos syndrome, hypermobility type: the link between connective tissue and psychological distress revised. Am J Med Genet C Semin Med Genet. (2015) 169:97–106. doi: 10.1002/ajmg.c.31430
21. Hus V, Lord C. The autism diagnostic observation schedule, module 4: revised algorithm and standardized severity scores. J Autism Dev Disord. (2014) 44:1996–2012. doi: 10.1007/s10803-014-2080-3
22. Bulbena A, Mallorquí-Bagué N, Pailhez G, Rosado S, González I, Blanch-Rubió J, Carbonell J. Self-reported screening questionnaire for the assessment of Joint Hypermobility Syndrome (SQ-CH), a collagen condition, in Spanish population. Eur J Psychiat. (2014) 28:17–26. doi: 10.4321/S0213-61632014000100002
23. Hakim A, Grahame R. Joint hypermobility. Musculoskeletal Care. (2007) 5:4–19. doi: 10.1002/msc.91
24. Clayton HA, Jones SA, Henriques DY. Proprioceptive precision is impaired in Ehlers–Danlos syndrome. Springerplus. (2015) 4:1–8. doi: 10.1186/s40064-015-1089-1
25. Rubio-Agusti I, Kojovic M, Chandrashekar HS, Edwards MJ, Bhatia KP. Cervical dystonia and joint hypermobility syndrome: a dangerous combination. Mov Disord. (2012) 27:203–4. doi: 10.1002/mds.24013
26. Koreki A, Eccles J, Garfinkel S, Critchley H, Cope S, Agrawal N, et al. Epilepsy & Behavior Hypermobility in patients with functional seizures: toward a pathobiological understanding of complex conditions. Epilepsy Behav. (2022) 132:108710. doi: 10.1016/j.yebeh.2022.108710
27. Eccles JA, Beacher FD, Gray MA, Jones CL, Minati L, Harrison NA, Critchley HD. Brain structure and joint hypermobility: relevance to the expression of psychiatric symptoms. Br J Psychiatry. (2012) 200:508–9. doi: 10.1192/bjp.bp.111.092460
28. Mallorquí-Bagué N, Garfinkel SN, Engels M, Eccles JA, Pailhez G, Bulbena A, et al. Neuroimaging and psychophysiological investigation of the link between anxiety, enhanced affective reactivity and interoception in people with joint hypermobility. Front Psychol. (2014) 5:1162. doi: 10.3389/fpsyg.2014.01162
Keywords: autism spectrum disorders, functional neurological disorders, conversion disorder, Joint Hypermobility Syndrome, Ehlers-Danlos Syndrome, connective tissue disorder
Citation: Nisticò V, Iacono A, Goeta D, Tedesco R, Giordano B, Faggioli R, Priori A, Gambini O and Demartini B (2022) Hypermobile spectrum disorders symptoms in patients with functional neurological disorders and autism spectrum disorders: A preliminary study. Front. Psychiatry 13:943098. doi: 10.3389/fpsyt.2022.943098
Received: 13 May 2022; Accepted: 04 August 2022;
Published: 24 August 2022.
Edited by:
Thomas Nickl-Jockschat, The University of Iowa, United StatesReviewed by:
Jessica Eccles, Brighton and Sussex Medical School, United KingdomRita Barone, University of Catania, Italy
Copyright © 2022 Nisticò, Iacono, Goeta, Tedesco, Giordano, Faggioli, Priori, Gambini and Demartini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Benedetta Demartini, YmVuZWRldHRhLmRlbWFydGluaUB1bmltaS5pdA==
†These authors share first authorship