 Hunde Tarafa
Hunde Tarafa Yadeta Alemayehu
Yadeta Alemayehu Meskerem Nigussie
Meskerem Nigussie- Department of Psychiatry, College of Health Sciences, Metu University, Metu, Ethiopia
Pregnancy-related anxiety (PRA) is an anxiety related to the pregnancy, involving labor and delivery, the well-being of the fetus/infant and the mother, the availability of quality of healthcare resources, and the capacity to parent. There is scarcity of study conducted on magnitude of Pregnancy-related anxiety and its associated factors among pregnant women in Ethiopia. The main objective of this research was to assess factors associated with Pregnancy-related anxiety among pregnant women attending ANC follow-up at Bedelle general and Metu Karl comprehensive specialized hospitals, Southwest Ethiopia. A hospital-based cross-sectional study design was used among pregnant women attending ANC follow-up. Data were collected from 406 sampled pregnant women who were selected through a systematic random sampling technique. Pregnancy-Related Anxiety Questionnaire-Revised (PRAQ-R2) was used to measure the outcome variable. The collected data were analyzed using Statistical Package for Social Sciences (SPSS) version 26. Logistic regression analyses were done to identify factors associated with Pregnancy-related anxiety and significance level set at p < 0.05. The overall prevalence of PRA in this study was 32.7%. Unwanted pregnancy AOR = 2.77, 95% CI [1.71, 4.54], high perceived stress AOR = 2.39, 95% CI [1.54, 3.62], young age AOR = 2.14, 95% CI [1.49, 2.83], depression AOR = 2.09, 95% CI [1.39, 2.89], low income AOR = 2.01, 95% CI [1.29, 3.14], and poor social support AOR = 1.79, 95% CI [1.14, 3.37] were significantly associated with Pregnancy-related anxiety. The findings of this study showed that the prevalence of Pregnancy-related anxiety was high in the study area and positively associated with young age, low income, poor social support, high perceived stress, depression, and unwanted pregnancy. This finding suggests that clinicians should integrate screening for Pregnancy-related anxiety into clinical standards, more efforts should be made in the future to reduce the anxiety among pregnant women who had an unwanted pregnancy, young women, and poor social support. Also, it is good to encourage the pregnant mother to enhance their social connectedness by creating a self-help group, and increasing early identification of mental health problems throughout their daily ANC follow-up.
Introduction
Pregnancy is one of the most remarkable experiences in a woman's life. It is connected to a wide range of physical, enthusiastic, and social changes (1). Besides, pregnant women are preoccupied with fetal growth and future obligations, making them vulnerable to different psychological issues such as mood swings, exhaustion, mixed anxiety-depressive disorder, emotional disorders, and pregnancy-related anxiety (PRA) (2). PRA is a predominant issue for women both during and after pregnancy (3).
Pregnancy-related anxiety (PRA) is an anxiety related to the pregnancy, involving labor and delivery, the well-being of the fetus or infant, the well–being of the mother, the availability and quality of healthcare resources, and/or the capacity to parent (4–6). PRA is different from general anxiety that happens together with pregnancy (6) and has stronger associations to preterm birth (born at <37 weeks gestation) than more commonly researched general anxiety disorder or depressive disorders (4, 7–9). Preterm birth is thought to affect 85 percent of the world's population in Africa and Asia (10). Africa has the most prominent rate of preterm birth, with certain areas coming to 17.5%; generally 14.3% of births in Eastern Africa are preterm (10).
Untreated PRA may have a significant effect on the on the pregnant woman's and growing fetus' health (11). High levels of PRA have been connected to shorter gestation and duration of birth, miscarriage, and hypertension in pregnant women (4, 12, 13). Furthermore, high levels of PRA have been linked with preterm birth and low birth weight (4), as well as negative emotion (14, 15), attention-deficit hyperactivity disorder (ADHD), and delay in development (13, 16).
The prevalence of PRA has been reported to range from 6 to 29% in developed countries, with South Asia accounting for 32% (17–19). According to a systematic review study, the magnitude of PRA accounts from 1 percent to 26 percent in low- & middle-income nations (LMICs) (20). However, there appears to be a scarcity of published study on PRA in Ethiopia. Therefore, the purpose of this study was to determine the prevalence of PRA and its associated factors among pregnant women.
Methods and materials
Study setting and period
This study was conducted from September 14 to November 14 2021 at Bedelle general hospital and Metu Karl comprehensive specialized hospital. Bedelle general hospital is located in Bedelle town at a distance of 426 Km from Addis Ababa (see Figure 1). Bedelle general hospital was established in 2011GC. Bedelle general hospital has 8 gynecology bed rooms, three post-delivery rooms, and one Psychiatry outpatient department (OPD). It provides curative and rehabilitative services for about 1.5 million people living in Bunno Bedelle zone and people from different zones like east and west Wollega. Whereas Metu Karl comprehensive specialized hospital is found in Metu town, Ilu Abba Boor zone, Oromia region, Southwest Ethiopia (see Figure 1). Metu town is located 600 km far apart from the capital city of Ethiopia, Addis Ababa and 124 km away from Bedelle town. Its climatic condition is woynadega with full of forest and it is conducive environment for survival. Metu Karl comprehensive specialized hospital provides curative and rehabilitative services for about 2.1 million people living in Ilu Aba Bor zone and people from different regions like Gambella, Southern nation and nationalities peoples (SNNP) region and West Wollega. Also the hospital has four wards, 192 beds, two psychiatric OPD and giving different services as inpatient and outpatients and with different clinics.

Figure 1. Study area map.
Study design and population
A hospital-based cross-sectional study was conducted among all sampled pregnant women attending ANC follow-up at Bedelle general hospital and Metu Karl comprehensive specialized hospital. Individuals who were critically ill during the data collection period and pregnant women aged <18 were excluded from the study since family consent is needed for their participation in the study.
Sample size and sampling technique
The sample size was determined by the using single population proportion formula n = (21) by assuming the proportion of pregnancy-related anxiety of 50% since there are no published studies in the study area, a confidence interval of 95, and 5% margin of error. Then, adding a non-response rate of 10%. Thus, the total sample size required was 423.
A systematic random sampling technique was used to select representative samples of pregnant women from both hospitals. Averagely 1,120 pregnant women attend ANC follow-up at both hospitals in 2 months. The sampling fraction was calculated by dividing the total number of pregnant women attending ANC follow-up in 2 months (1,120) by the final sample size (423); k = N/n = 2.6 ≈ 2. The first woman was selected by lottery method and then continued every 2 intervals. The data were collected from every other pregnant woman attending ANC follow-up at Bedelle general hospital and Metu Karl Specialized hospital.
Variables of the study
The dependent variable in this study was pregnant-related anxiety. Independent variables included socio-demographic related variables (age, religion, marital status, ethnicity, level of education, educational status of the spouse, occupational status, occupational status of the spouse, family size, and income), psycho-social factors (family history of mental illness, social support, substance use history of the spouse, and marital satisfaction), health-related factors (current illness, depression, and perceived stress), pregnancy-related factors (duration of pregnancy, the woman's desire for pregnancy, and gravity), previous obstetrics factors (preterm history, stillbirth history, very low birth weight history, postnatal hemorrhage, abortion, and cesarean section), substance use-related factors (khat, alcohol, and tobacco).
Data collection instruments
Pregnancy-related anxiety questionnaire-revised (PRAQ-R2)
The 10-item Pregnancy-Related Anxiety Questionnaire-Revised (PRAQ-R2) is a commonly used tool for assessing and identifying pregnancy-related anxiety in all pregnant women, regardless of parity. It has high psychometric values and predicts birth and childhood outcomes. In this study PRAQ-R2 adopted to measure the outcome variable. PRAQ-R2 contains 10 items. Each item asks about current feelings, and responses are measured on a 5-point likert scale: absolutely not relevant, hardly relevant, sometimes relevant, reasonably relevant, and very relevant, coded as “0”, “1”, “2”, “3”, and “4”, respectively. When all of the items are added together, the final score ranges from 0 to 40. “It consisted of three subscales: fear of giving birth, worries about a disabled child, and concern about one's appearance”. Scores of 13 or greater on PRAQ-R2 were considered as having pregnancy-related anxiety (22). In the current study the internal consistency (Cronbach's alpha) of PRAQ-R2 was 0.87.
Edinburgh postnatal depression scale (EPDS)
EPDS was used to screen for depression in this study. The EPDS is constituted of ten short statements. A mother selects one of four possible responses that best describe how she has felt over the last week. Responses are assigned a score of 0, 1, 2, or 3 based on the severity of the symptom. “Items 3, 5 to 10 are reverse scored (i.e., 3, 2, 1, and 0)”. The overall score is calculated by adding the scores for each of the 10 items. Mothers with a score of more than 13 were considered as depressed (23). In the current study the internal consistency (Cronbach's alpha) of EPDS was 0.84.
Perceived stress scale (PSS-10)
A perceived stress scale (PSS-10) with 10 items was used to collect data on perceived stress. The tool uses a 5-point Likert scale. Each item was rated using a scale of 0 = Never, 1 = Almost Never, 2 = Sometimes, 3 = Fairly Often, and 4 = Very Often. “The sum score ranged from 0 to 40 with higher scores indicating higher perceived stress”. “Scores ranging from 0 to 13 would be regarded as low stress, 14 to 26 would be considered moderate stress, and 27–40 would be considered high perceived stress” (24). In the current study the internal consistency (Cronbach's alpha) of PSS-10 was 0.93.
Oslo 3-items social support scale
Social support was measured by using Oslo social support questionnaire which has a score range from 3–14 that was interpreted as 3–8 is poor support, 9–11 is moderate support, and 12–14 is strong support (25). In the current study the internal consistency (Cronbach's alpha) of Oslo 3-items social support scale was 0.79.
Data collection procedures and data quality control
Interviewer-administered questionnaires were used to collect the data. The data were collected by five BSc. Nurses and supervised by two BSc. Psychiatry nurses. The questionnaire consisted of structured questions that can be subdivided into eight different categories: socio-demographic characteristics, PRAQ-R2, substance use, EPDS, PSS 10, psycho-social, health-related factors, and Oslo 3-items social support scale, previous obstetrics factors, and pregnancy-related factors.
The questionnaires were pretested on 5% (n = 21) of the total sample size at Chora primary hospital 1 week before data collection. Based on the pretest results, questions that were unclear or ambiguous were reviewed and fixed. The data collectors were supervised regularly, and the completed questionnaires were verified by the supervisor and principal investigator daily basis. To ensure consistency, the questionnaire was developed in English, and then translated into the local language Afan Oromo then back-translated into English by language experts. The data has been collected using the Afan Oromo version questionnaire.
Data processing and analysis
Data were coded and reviewed for completeness. Epi-data management version 4.6 was used to enter data, which was then exported to SPSS Version 26.0 for analysis. Tables and charts were used to present descriptive statistics such as frequency, percentage, mean, and standard deviation. The logistic regression analysis model was utilized; first, a bivariate analysis was performed to determine the association between each independent variable and pregnancy-related anxiety. Variables with P < 0.25 in bivariate analysis were incorporated into a multivariate logistic regression model to determine the association of each independent variable with pregnancy-related anxiety. P-value (p < 0.05) was used to determine statistical significance.
Ethical considerations
Ethical clearance was obtained from the ethical review committee of Metu University. A formal letter of permission was obtained from Bedelle general hospital and Metu Karl comprehensive specialized hospital. The study's objectives were explicitly conveyed to data collectors and study participants. The study participants were given the option to refuse or cease participation at any time, as well as the opportunity to ask any questions they had concerning the study. Participants' written consents were obtained before data were gathered. Throughout the study, confidentiality was maintained.
Results
Socio-demographic characteristics of participants
Four hundred six (406) study participants freely participated in the study, yielding a 96.0 percent response rate out of a total of 423 study participants. The majority 392 (96.53 %) of the study participants were married. The mean age of the participants was 28.4 (±6.13) years. Regarding educational level, 225 (55.4%) of the study participants were not attended formal education. The majority of respondents 360 (88.6%) were from the Oromo ethnic group, and 189(46.5%) were Orthodox Christian religion followers. Two hundred one (49.5 %) participants were housewives (Table 1).
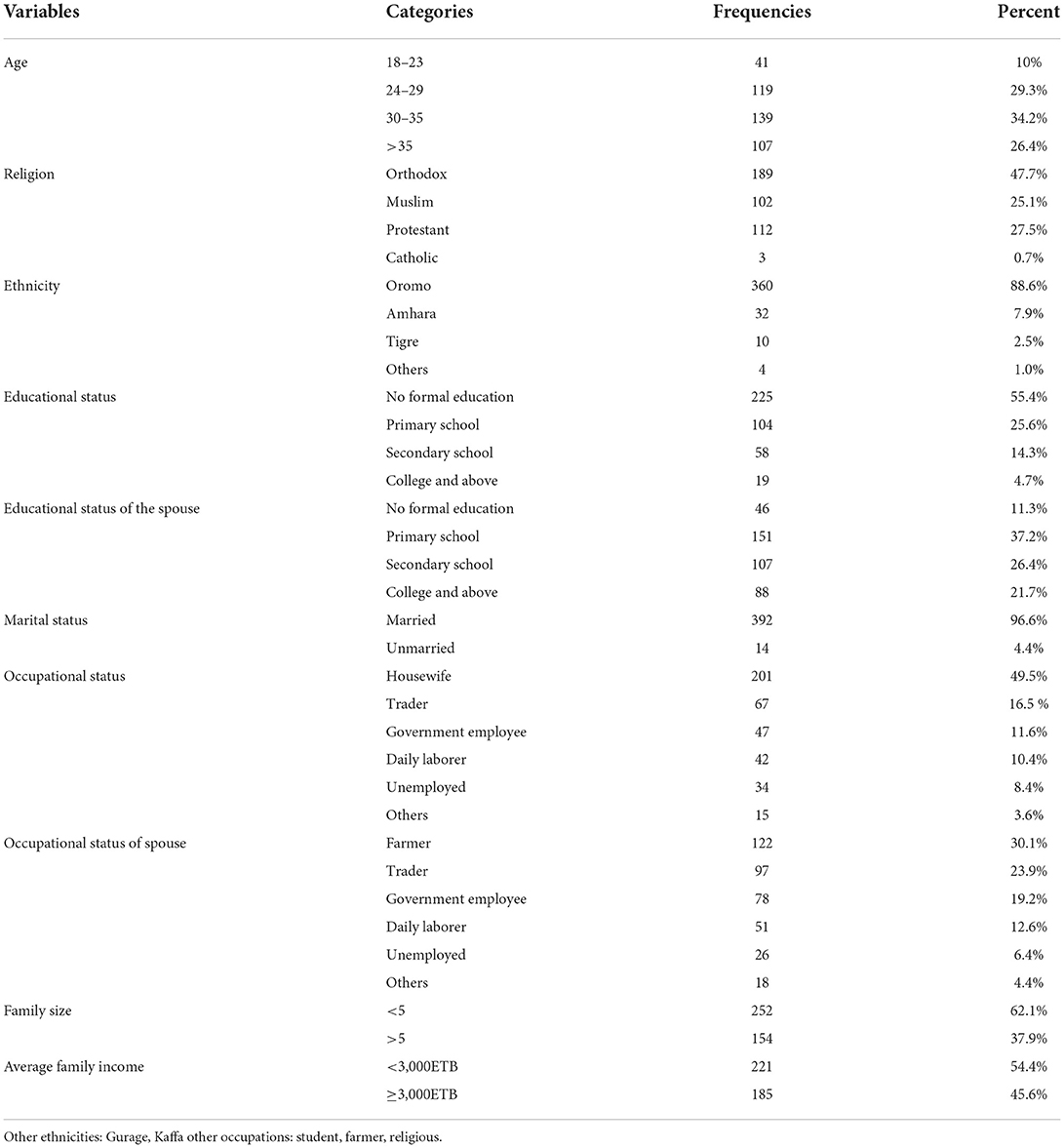
Table 1. Socio-demographic characteristics of pregnant women attending ANC follow-up at Bedelle general hospital and Metu Karl comprehensive specialized hospital, 2021 (N = 406).
Psychosocial, substance use, and health-related characteristics of respondents
About half of the participants 204 (50.2%) had moderate social support; the majority of participants were reported a satisfying marital relationship 316 (77.8%) and about three fourth of the participants 302 (74.4%) had low perceived stress (Figure 2). Only 4.7% of the participants had a family history of mental illness. About one-third 118 (29.1%) of the participants had a spouse with an alcohol drinking habit and 42 (10.3%) had a spouse who smoke cigarettes (Table 2).
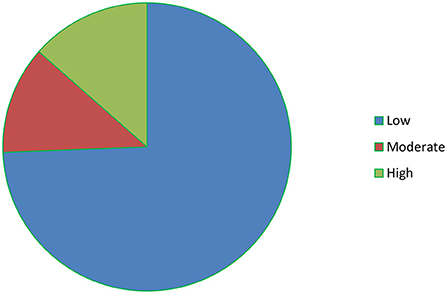
Figure 2. The level of perceived stress among respondents.
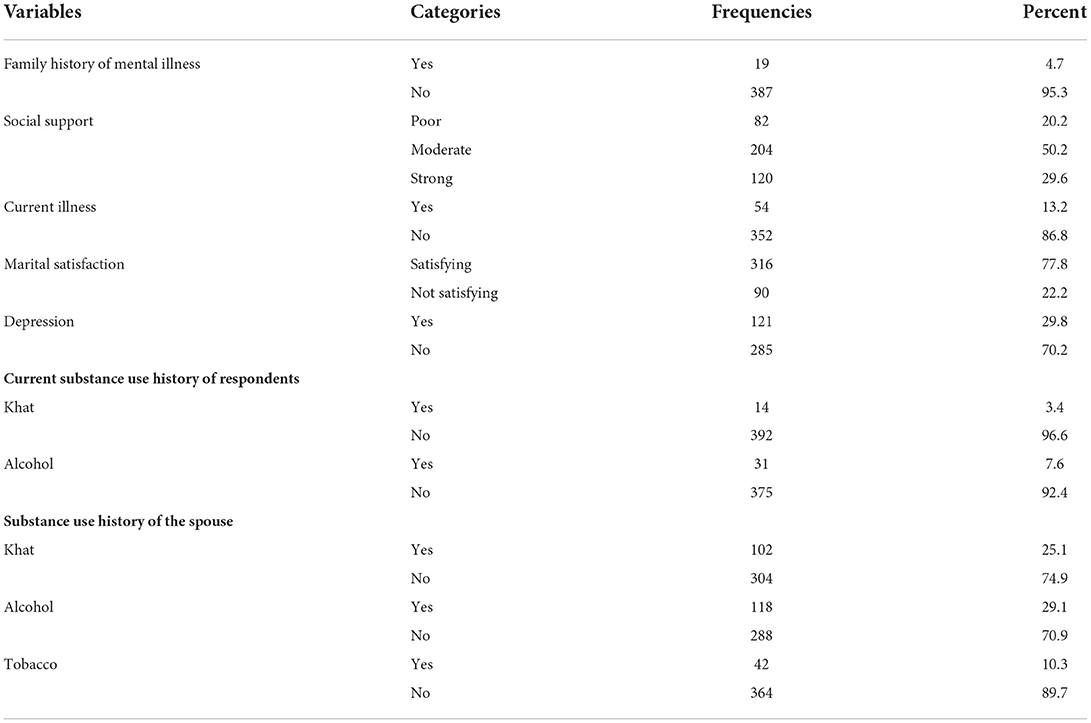
Table 2. Psychosocial, substance use, and health-related characteristics of pregnant women attending antenatal clinic follow-up at Bedelle general hospital and Metu Karl comprehensive specialized hospital, 2021 (N = 406).
Previous obstetrics and pregnancy-related characteristics
Nearly three-quarters of participants 294 (72.4%) were multiparous; the majority of participants were in the second trimester of pregnancy 198 (48.7%) and the majority of participants 378 (93.1%) reported that the pregnancy was wanted. About 37 (9.1%) of participants had a history of abortion in the past (Table 3).
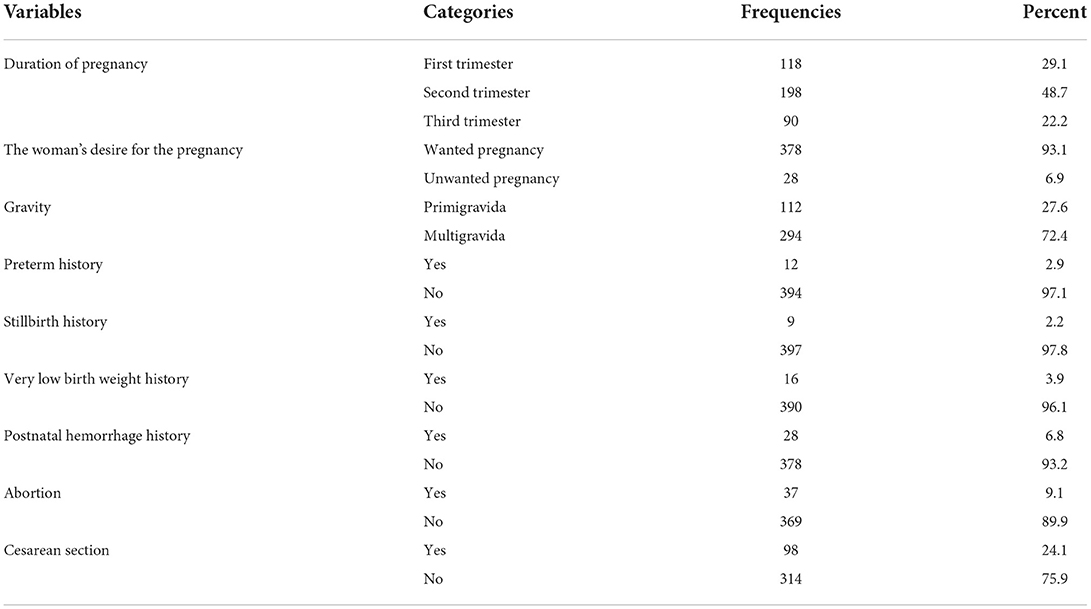
Table 3. Previous obstetrics and pregnancy-related characteristics of pregnant women attending antenatal clinic follow-up at Bedelle general hospital and Metu Karl comprehensive specialized hospital, 2021 (N = 406).
The prevalence of pregnancy-related anxiety among pregnant women
The overall prevalence of pregnancy-related anxiety in this study was 32.7 % with 95% CI (29.4, 36.3).
Factors associated with PRA
Association of PRA with socio-demographic characteristics
The socio-demographic variables, including age, marital status, occupational status, and income have shown an association with pregnancy-related anxiety in bivariate logistic regression analysis. However, young age and low income were the only socio-demographic variables associated with pregnancy-related anxiety in the final model. See Table 4 for detail.
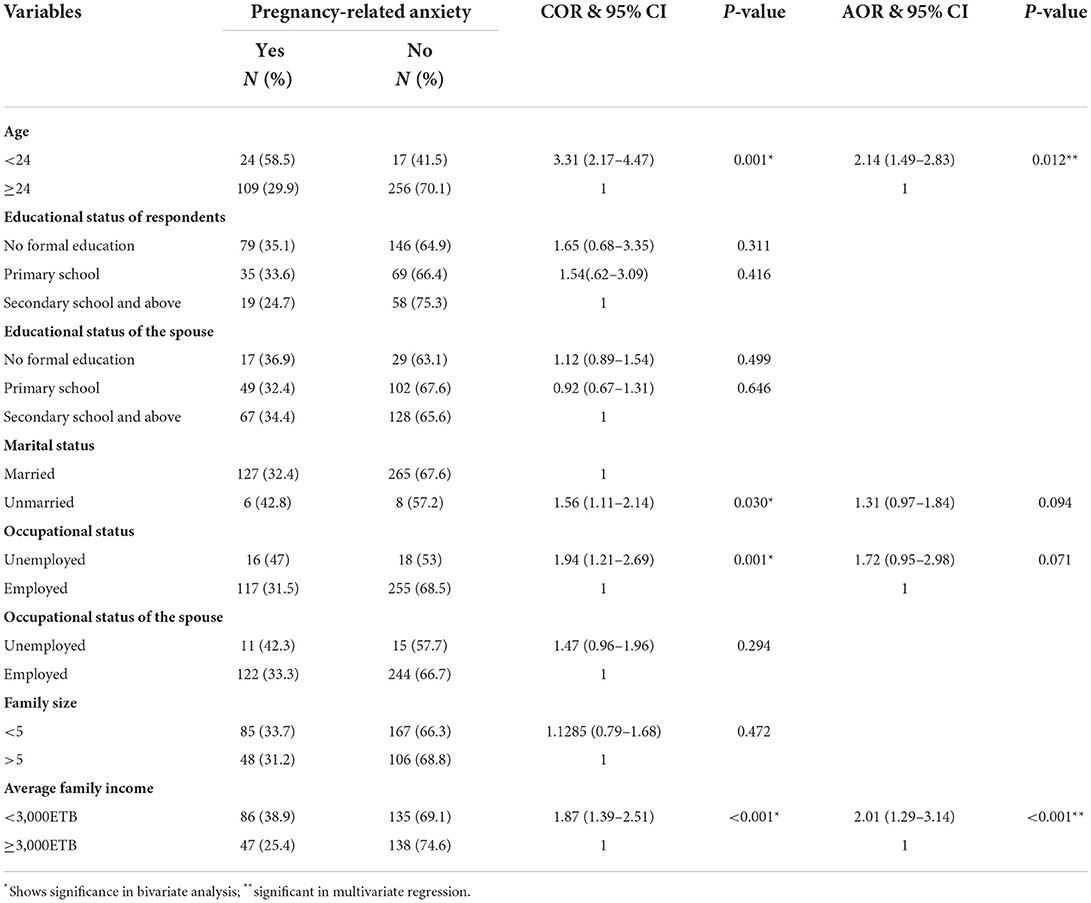
Table 4. Bivariate and Multivariate binary logistic regression analysis showing the association between pregnancy-related anxiety and socio-demographic variables among pregnant women attending ANC follow up Bedelle general hospital and Metu Karl comprehensive specialized hospital, 2021 (N = 406).
The odds of PRA were 2.14-times (AOR = 2.14, 95% CI = 1.49, 2.83) higher in pregnant women aged <24 compared to those aged 24 and above. Similarly, pregnant women who reported low family income were about 2-times more likely to have pregnant-related anxiety than pregnant women who have good family income AOR = 2.01, 95% CI (1.29, 3.14).
Association of pregnancy-related anxiety with psychosocial factors, substance use history, and health-related variables
From psychosocial factors, substance use history and health-related variables, family history of mental illness, social support, perceived stress, depression, current illness, khat use of the respondent, alcohol use of the respondent, alcohol use history of the spouse, and tobacco use history of the spouse were associated with pregnancy-related anxiety in bivariate logistic regression analysis. However, poor social support, high perceived stress, and depression were psychosocial and health related variables associated with pregnancy-related anxiety in the final model. See Table 5 for detail.
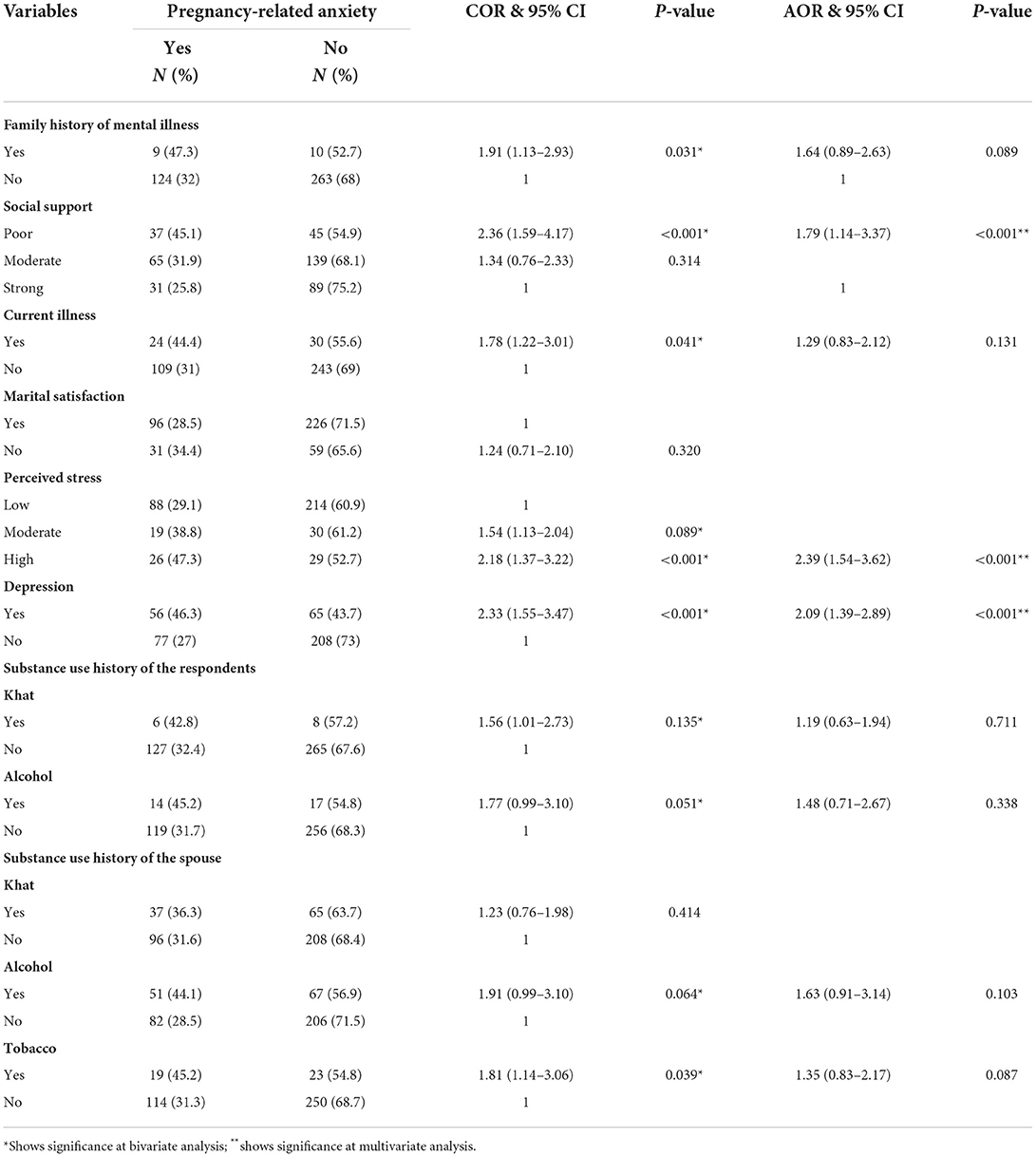
Table 5. Bivariate and Multivariate binary logistic regression analysis showing the association between PRA and psychosocial, substance use, and health-related variables among pregnant women attending ANC follow-up Bedelle general hospital and Metu Karl comprehensive specialized hospital, 2021 (N = 406).
In this study, the odds of having PRA among respondents who have poor social support were 1.79-times (AOR = 1.79, 95% CI = 1.14, 3.37) higher compared to those who have strong social support. Likewise high perceived stress increases the likelihood of pregnancy-related anxiety by 2.4-times as compared to low perceived stress, AOR = 2.39, 95% (1.54, 3.62). The odds of having pregnancy-related anxiety among respondents who have depression symptoms were 2.01-times higher than those without depression symptoms (AOR = 1.84, 95% CI = 1.01–3.35).
Association of pregnancy-related anxiety with previous obstetrics and pregnancy-related factors
From previous obstetrics and pregnancy related variables, unwanted pregnancy, preterm history, gravity, history of abortion, and history of cesarean section delivery were associated with pregnancy-related anxiety in bivariate logistic regression analysis. However, unwanted pregnancy was the only pregnancy-related variable associated with pregnancy-related anxiety in the final model.
In this study, the odds of having pregnancy-related anxiety among respondents who had reported unwanted pregnancy was 2.77-times (AOR = 2.77, 95% CI = 1.71, 4.54) higher as compared to those who reported the pregnancy is wanted. See Table 6 for detail.
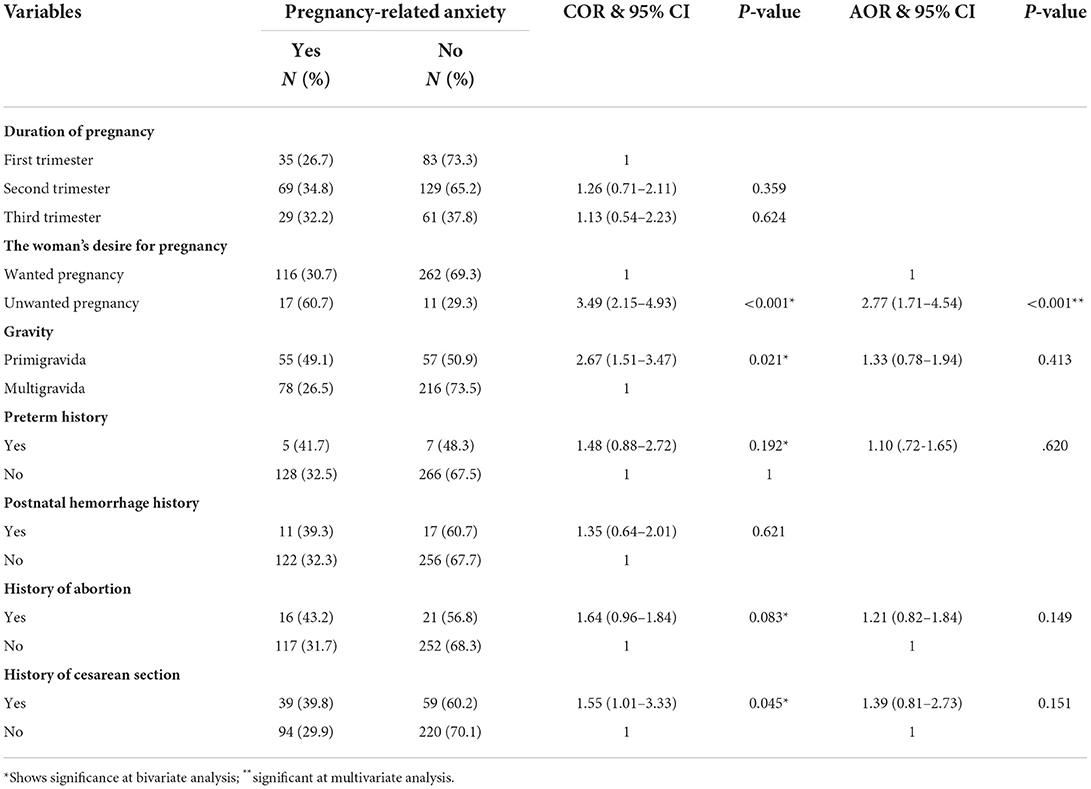
Table 6. Bivariate and Multivariate binary logistic regression analysis showing the association between PRA and previous obstetrics and pregnancy related variables among pregnant women attending ANC follow up Bedelle general hospital and Metu Karl comprehensive specialized hospital, 2021 (N = 406).
Discussion
The purpose of this study was to determine the prevalence of PRA and its associated factors among pregnant mothers receiving antenatal care at Bedelle general hospital and Metu Karl comprehensive specialized hospital. The magnitude of PRA among pregnant mothers in this research was 32.7% (95% CI 29.4, 36.3). The finding of our study was similar with the finding of the research that undertaken in Dilla university referral hospital where 32.2% of the study participants were screened positive for anxiety (26). However, The reported prevalence rates from other studies using different scales appear to be much lower than the finding of this study: 10.04 percent in Arba minch area district study by utilizing the General Anxiety Disorder 7-items to screen PRA (27), 25 percent in Tanzania study in which they used PRAQ to screen PRA (28), 23 percent in South Africa in which they utilized the Mini-International Neuropsychiatric Interview diagnostic interview to screen PRA, 23.6 percent in Saudi Arabia study using the State Anxiety scale (29), 26.6 percent in Qatar study using PRAQ-R2 (22), and 26.8 percent in Brazil study using the Hospital Anxiety Subscale (30). In contrast, the result of this study is lower than the result of the study that conducted in southern India (31) where 55.7% pregnant mothers have screened positive for PRA.
This variation in prevalence of PRA could be related to discrepancies in the psychometric qualities of the measuring tool utilized. In addition it might be related to demographic and sociocultural differences. Societal norms and beliefs can also influence views of what is “stressful” or “hazardous,” accounting for the diversity in prevalence across different study contexts. Moreover, other possible reasons for the difference in prevalence can be related to variation in sample size and sampling techniques.
Our study showed that being pregnant at young age was found to be a risk factor for PRA. The finding of this research is similar with the finding of a study conducted in in India (32), Hungary (33), and Sweden (19). This association might be attributed to an increased feeling about the fear of birth and approaching birth may leads to the development of pregnancy-related anxiety. The possible reason could be that at an early age, the pregnant mother might anxious the possibility of fetus loss and the viability of a developing fetus.
In this study, low income was significantly associated with pregnant-related anxiety. This is similar with the result of studies undertaken in United States (34) and Hungary (33). These findings show that low-income pregnant women may be obsessed with issues associated with parenting, such as higher financial expenses, availability to prenatal service, and maternity leave. For instance, the anticipated financial costs of maintaining a baby may be an extra pressure during the perinatal time, influencing the occurrences of anxiety. Additionally, pregnant mother with low financial income may be worried about their capability to provide for their child; as a result of this, they develop higher level of anxiety symptoms. Low income pregnant mother may be worried about their access to ANC service, which may be hindered by their family income. Pregnant mother with lower socioeconomic status receive limited prenatal service at higher rates than their middle and high socioeconomic status counterparts (35), and lower socioeconomic status has been linked with high risk of hypertension, diabetes, and other complications related to pregnancy (35).
Our study finding indicated that those pregnant mothers who have poor social support had higher chance of PRA compared to pregnant mothers who have strong social support. This is similar to the results of the researches that undertaken in Dilla university referral hospital (26), Hungary (33), and Australia (36). Pregnant mothers who have poor social support might not happy with their family and has no good interaction with their social environment, and due to this, they may develop social withdrawal, becoming less psychological and coping ability and eventually leads to more anxiety (37).
This research has indicated that depression is highly linked with pregnancy-related anxiety. The existing research supports the established association between depression and pregnancy-related anxiety (6,40). Pregnant mother have high chance of suffering anxiety and depression than non-pregnant women (38, 39). However, there appears to be a lack of knowledge as to why this comorbidity emerges and whether depression or anxiety develops first in this inquiry, stress, appraisal, and coping theory consideration (40), along with the intricacies of this sample's sociocultural circumstances, gives insight. According to Lazarus and Folkman (40), stress happened when an event is seen as a potential danger to one's well-being, and the assets to play down the occasion are respected as inaccessible. Furthermore, conditions such as uniqueness and closeness to the situation can influence perceptions of the severity of the danger happened (40). According to this concept, an inadequate basic health related knowledge, combined with constrained get to healthcare facilities and a destitute financial status, makes an environment in which pregnancy is frequently linked with stress or anxiety (41).
In the current study high level of perceived stress is strongly associated with pregnancy-related anxiety. This findings is similar with the finding of a study that conducted in Tanzania (28). Perceived stress is a person thought of the level of suffering posed by stressors, and their capability to cope with those stressors. Pregnant mothers usually develop a high level of perceived stress, due to the stress of approaching the delivery time; this may in turn leads to anxiety (41).
This research showed that unwanted pregnancy was a significant predictor of PRA. This finding is consistent with a findings of researches conducted in Nigeria (42), Spain (43), and China (44). This association is possible explained lack of financial preparation from women to have a new baby and lack of psychological preparedness for motherhood (44–46). Moreover, an unwanted pregnancy was linked to increased levels of anxiety during the delivery process.
This research has number of limitations. First, the cross-sectional design of our study limits the ability to draw conclusions about directions of the relationships. Second, since the study is limited to Bedelle general hospital and Metu Karl comprehensive specialized hospital, the findings of research may not inferred to health facilities. Some variables were assessed with only self-report such as family history of mental illness, pregnancy wanted or unwanted, and medical illness which may have influenced by social desirability bias. We attempt to minimize these limitations by giving training for the data collectors to explain the respondents the objective of the study and interviewing them in to the way their privacy is maintained and informing them as the information collected from them was anonymous and this may in turn increase the response rate.
Conclusion
The magnitude of pregnancy-related anxiety among pregnant mothers in the study setting was high. One in three pregnant women was found to have PRA in the study setting. Young age, low income, poor social support, high perceived stress, depression, and unwanted pregnancy were significantly associated with PRA. The clinicians working in ANC need to include mental health screening in their routine services and forward the right intervention to initiate and enhance access to mental health treatment, especially for vulnerable groups. Early treatment and integrating mental health services for co-morbid mental illness and ANC is essential, since PRA is notably common among pregnant mothers. It is better if interventions focus among the pregnant mothers who had a history of depression and mothers with unwanted pregnancy are implemented. In addition, it is better to encourage the pregnant women to increase their social network by establishing a self-help group, and strengthening early detection of mental health problems throughout their routine ANC follow-up. Based on the study findings, we recommend that the concerned public organizations like women and youth affair and other governmental organization (NGO) work on educating women on preventing unwanted pregnancy as well as policy makers consider stress management technique to ANC to curb the burden on pregnant women.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
HT conceived the study design, collected, analyzed, interpreted data, and drafted the manuscript for important intellectual content. YA and MN conceived the study design, interpreted data, and review the manuscript for important intellectual content. All authors contributed to the article and approved the submitted version.
Acknowledgments
We would like to thank the Metu University College of Health Sciences for providing research funding. We would like to thank all of the data collectors, supervisors, and study participants for their valuable contributions to this work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ANC, Antenatal Care; AOR, Adjusted odds ratio; COR, Crude odds ratio; EPDS, Edinburgh Postnatal Depression Scale; LMICs, Low-income and Middle-Income Countries; PRA, Pregnancy-related anxiety; PRAQ-R2, Pregnancy-Related Anxiety Questionnaire-Revised; PSS-10, Perceived Stress Scale; SPSS, Statistical Package for Social Sciences.
References
1. Ahmadi A, Moosavi Sahebalzamani S, Ghavami F, Shafiee YFA. Effects of psychological interventions on postpartum depression, anxiety and infants' weight in primipara women. Prev Care Nurs Midwifery J. (2014) 4:19–31.
2. Bjelica A, Cetkovic N, Trninic-Pjevic A M-SL. The phenomenon of pregnancy—a psychological view. Ginekol Pol. (2018) 89:102–6. doi: 10.5603/GP.a2018.0017
3. Chinchilla-Ochoa D, Peón PB-C, Farfán-Labonne BE, Garza-Morales S, Leff-Gelman P F-RM. Depressive symptoms in pregnant women with high trait and state anxiety during pregnancy and postpartum. Int J Women's Heal. (2019) 11:257–65. doi: 10.2147/IJWH.S194021
4. Dunkel Schetter C, Tanner L. Anxiety, depression and stress in pregnancy: implications for mothers, children, research, and practice. Curr Opin Psychiatry. (2012) 25:141–8. doi: 10.1097/YCO.0b013e3283503680
5. Schetter CD. Psychological science on pregnancy: stress processes, biopsychosocial models, and emerging research issues. Annu Rev Psychol. (2011) 62:531–58. doi: 10.1146/annurev.psych.031809.130727
6. Huizink AC, Mulder EJH, Robles De Medina PG, Visser GHA, Buitelaar JK. Is pregnancy anxiety a distinctive syndrome? Early Hum Dev. (2004) 79:81–91. doi: 10.1016/j.earlhumdev.2004.04.014
7. Rose MS, Pana G, Premji S. Prenatal maternal anxiety as a risk factor for preterm birth and the effects of heterogeneity on this relationship: a systematic review and meta-analysis. Biomed Res Int. (2016) 2016:8312158. doi: 10.1155/2016/8312158
8. Glynn LM, Schetter CD, Hobel CJ, Sandman CA. Pattern of perceived stress and anxiety in pregnancy predicts preterm birth. Heal Psychol. (2008) 27:43–51. doi: 10.1037/0278-6133.27.1.43
10. Beck S, Wojdyla D, Say L, Betran AP, Merialdi M, Requejo JH, et al. The worldwide incidence of preterm birth: a systematic review of maternal mortality and morbidity. Bull World Health Organ. (2010) 88:31–8. doi: 10.2471/BLT.08.062554
11. Huizink AC, Delforterie MJ, Scheinin NM, Tolvanen M, Karlsson L, Karlsson H. Adaption of pregnancy anxiety questionnaire–revised for all pregnant women regardless of parity: PRAQ-R2. Arch Womens Ment Health. (2016) 19:125–32. doi: 10.1007/s00737-015-0531-2
12. Tomfohr-Madsen L, Cameron EE, Dunkel Schetter C, Campbell T, O'Beirne M, Letourneau N, et al. Pregnancy anxiety and preterm birth: the moderating role of sleep. Health Psychol. (2019) 38:1025–35. doi: 10.1037/hea0000792
13. Field T. Prenatal anxiety effects: a review. Infant Behav Dev. (2017) 49:120–8. doi: 10.1016/j.infbeh.2017.08.008
14. Huizink AC, De Medina PGR, Mulder EJ, Visser GH, BJ. Psychological measures of prenatal stress as predictors of infant temperament. J Am Acad Child Adolesc Psychiatry. (2002) 41:1078–85. doi: 10.1097/00004583-200209000-00008
15. Gutteling BM, de Weerth C, Willemsen-Swinkels SHN, Huizink AC, Mulder EJH, Visser GHA, et al. The effects of prenatal stress on temperament and problem behavior of 27-month-old toddlers. Eur Child Adolesc Psychiatry. (2005) 14:41–51. doi: 10.1007/s00787-005-0435-1
16. Van den Bergh BR, Mennes M, Oosterlaan J, Stevens V, Stiers P, Marcoen A, et al. High antenatal maternal anxiety is related to impulsivity during performance on cognitive tasks in 14-and 15-year-olds. Neurosci Biobehav Rev. (2005) 29:259–69. doi: 10.1016/j.neubiorev.2004.10.010
17. Jill Fleuriet K, Sunil TS. Perceived social stress, pregnancy-related anxiety, depression and subjective social status among pregnant Mexican and Mexican American Women in South Texas. J Health Care Poor Underserved. (2014) 25:546–61. doi: 10.1353/hpu.2014.0092
18. Arch JJ. Pregnancy-specific anxiety: which women are highest and what are the alcohol-related risks? Compr Psychiatry. (2013) 54:217–28. doi: 10.1016/j.comppsych.2012.07.010
19. Rubertsson C, Hellström J. Cross M, Sydsjo G. Anxiety in early pregnancy: prevalence and contributing factors. Arch Womens Ment Health. (2014) 17:221–8. doi: 10.1007/s00737-013-0409-0
20. Jha S, Salve HR, Goswami K, Sagar R, Kant S. Burden of common mental disorders among pregnant women: a systematic review. Asian J Psychiatry. (2018) 36:46–53. doi: 10.1016/j.ajp.2018.06.020
21. Kethari C. Reasearch Methodology: Methods and Techniques. New Delhi: New Age International(P) Limited, Publishers. (2004).
22. Naja S, Al Kubaisi N, Singh R, Bougmiza I. Generalized and pregnancy-related anxiety prevalence and predictors among pregnant women attending primary health care in Qatar, 2018–2019. Heliyon. (2020) 6:e05264. doi: 10.1016/j.heliyon.2020.e05264
23. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10-item edinburgh postnatal depression scale. Br J Psychiatr. (1987) 150:3–6. doi: 10.1192/bjp.150.6.782
24. Chaaya M, Osman H, Naassan G. Ziyad M. “Validation of the Arabic version of the cohen perceived stress scale (PSS-10) among pregnant and postpartum women”. BMC Psychiatry. (2010) 10:1–7. doi: 10.1186/1471-244X-10-111
25. Abiola T, Udofia O, ZM. Psychometric properties of the 3-item oslo social support scale among clinical students of Bayero University Kano, Nigeria. Malaysian J Psychiatry. (2013) 22:32–41.
26. Chalachew Kassew PD. The prevalence of general anxiety diorder and its associated factors among women's attending at the prenatal service of Dilla university referral hospital, Dilla town, Ethiopia, April, 2020 in COVID pandemic. Heliyon. (2020) 6:e05593. doi: 10.1016/j.heliyon.2020.e05593
27. Bante A, Mersha A, Zerdo Z, Wassihun B, Yeheyis T. Comorbid anxiety and depression : Prevalence and associated factors among pregnant women in Arba Minch zuria district, Gamo zone, southern Ethiopia. PLoS ONE. (2021) 16:e0248331. doi: 10.1371/journal.pone.0248331
28. Wall V, Premji SS, Letourneau N, Mccaffrey G, Nyanza EC. Factors associated with pregnancy- related anxiety in Tanzanian women : a cross sectional study. BMJ Open. (2018) 8:e020056. doi: 10.1136/bmjopen-2017-020056
29. Alqahtani AH, Al Khedair K, Al-Jeheiman R, Al-Turki HA, Al Qahtani NH. Anxiety and depression during pregnancy in women attending clinics in a University Hospital in Eastern province of Saudi Arabia: prevalence and associated factors. Int J Womens Health. (2018) 10:101–8. doi: 10.2147/IJWH.S153273
30. Silva MM de J, Nogueira DA, Clapis MJ, Leite EPRC. Anxiety in pregnancy: prevalence and associated factors. Rev da Esc Enferm. (2017) 51:1–8. doi: 10.1590/s1980-220x2016048003253
31. Nath A, Venkatesh S, Balan S, Metgud CS, Krishna M, Murthy GVS. The prevalence and determinants of pregnancy-related anxiety amongst pregnant women at less than 24 weeks of pregnancy in Bangalore, Southern India. Int J Womens Health. (2019) 11:241–8. doi: 10.2147/IJWH.S193306
32. Madhavanprabhakaran GK, D'Souza MS, Nairy KS. Prevalence of pregnancy anxiety and associated factors. Int J Africa Nurs Sci. (2015) 3:1–7. doi: 10.1016/j.ijans.2015.06.002
33. Bödecs T, Szilágyi E, Cholnoky P, Sándor J, Gonda X, Rihmer Z, et al. Prevalence and psychosocial background of anxiety and depression emerging during the first trimester of pregnancy: data from a Hungarian population-based sample. Psychiatr Danub. (2013) 25:352–8.
34. Mandabach MK. Socioeconomic Status and Symptoms of Anxiety and Depression in Pregnant Women from the Southern United States. Univ Mississippi eGrove. 2020;
35. Kim MK, Lee SM, Bae SH, Kim HJ, Lim NG, Yoon SJ, et al. Socioeconomic status can affect pregnancy outcomes and complications, even with a universal healthcare system. Int J Equity Health. (2018) 17:2. doi: 10.1186/s12939-017-0715-7
36. Bedaso A, Adams J, Peng W, Sibbritt D. The association between social support and antenatal depressive and anxiety symptoms among Australian women. BMC Pregnancy Childbirth. (2021) 21:1–12. doi: 10.1186/s12884-021-04188-4
37. Thoits PA. Social support as coping assistance. J Consult Clin Psychol. (1986) 54:416–23. doi: 10.1037/0022-006X.54.4.416
38. Rwakarema M, Premji SS, Nyanza EC, Riziki P, Palacios-Derflingher L. Antenatal depression is associated with pregnancy-related anxiety, partner relations, and wealth in women in Northern Tanzania: a cross-sectional study. BMC Womens Health. (2015) 15:1–10. doi: 10.1186/s12905-015-0225-y
39. Field T, Diego M, Hernandez-Reif M, Figueiredo B, Deeds O, Ascencio A, et al. Comorbid depression and anxiety effects on pregnancy and neonatal outcome. Infant Behav Dev. (2010) 33:23–9. doi: 10.1016/j.infbeh.2009.10.004
40. Lazarus RS, Susan F. Stress, Appraisal, and Coping. Springer publishing company; NewYork, NY: Springer. (1984).
41. Rosario MK, Premji SS, Nyanza EC, Bouchal SR, Este D. A qualitative study of pregnancy-related anxiety among women in Tanzania. BMJ Open. (2017) 7:1–8. doi: 10.1136/bmjopen-2017-016072
42. Ajayi AI, Nwokocha EE, Adeniyi OV, Ter Goon D, Akpan W. Unplanned pregnancy-risks and use of emergency contraception: a survey of two Nigerian Universities. BMC Health Serv Res. (2017) 17:1–8. doi: 10.1186/s12913-017-2328-7
43. Roca A, Imaz ML, Torres A, Plaza A, Subirà S, Valdés M. Unplanned pregnancy and discontinuation of SSRIs in pregnant women with previously treated affective disorder. J Affect Disord. (2013) 150:807–13. doi: 10.1016/j.jad.2013.02.040
44. You Y, Yan SQ, Huang K, Mao LJ, Zhou SS, Ge X, et al. Pregnancy intention and pregnancy-related anxiety in the second and third trimester: a birth cohort study. Zhonghua Liu Xing Bing Xue Za Zhi. (2017) 38:1179–82. doi: 10.3760/cma.j.issn.0254–6450.2017.09.007
45. Mulder EJH, De Medina PGR, Huizink AC. Prenatal maternal stress: effects on pregnancy and the (unborn) child. Early Hum Dev. (2002) 70:3–14. doi: 10.1016/S0378-3782(02)00075-0
Keywords: pregnancy-related anxiety, pregnant women, Bedelle, Metu, Ethiopia
Citation: Tarafa H, Alemayehu Y and Nigussie M (2022) Factors associated with pregnancy-related anxiety among pregnant women attending antenatal care follow-up at Bedelle general hospital and Metu Karl comprehensive specialized hospital, Southwest Ethiopia. Front. Psychiatry 13:938277. doi: 10.3389/fpsyt.2022.938277
Received: 07 May 2022; Accepted: 29 August 2022;
Published: 23 September 2022.
Edited by:
S. M. Yasir Arafat, Enam Medical College, BangladeshReviewed by:
Tesfaye Dessu Geleta, Jimma University, EthiopiaWafaa Boraey, Mansoura University, Egypt
Copyright © 2022 Tarafa, Alemayehu and Nigussie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hunde Tarafa, aHVuZGV0YXJhZmFAZ21haWwuY29t