 Clarisse de Azambuja Farias1,2
Clarisse de Azambuja Farias1,2 Taiane de Azevedo Cardoso2,3Marielle Moro da Silva4
Taiane de Azevedo Cardoso2,3Marielle Moro da Silva4 Francesca D’Angelo3Thaise Campos Mondin2
Francesca D’Angelo3Thaise Campos Mondin2 Luciano Dias de Mattos Souza2Ricardo Azevedo da Silva2
Luciano Dias de Mattos Souza2Ricardo Azevedo da Silva2 Flavio Kapczinski1,3,4Karen Jansen2
Flavio Kapczinski1,3,4Karen Jansen2 Pedro V. S. Magalhães1*
Pedro V. S. Magalhães1*- 1Graduate Program in Psychiatry and Behavioral Sciences, Hospital de Clínicas de Porto Alegre, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil
- 2Graduate Program in Health and Behavior, Universidade Católica de Pelotas, Pelotas, Brazil
- 3Department of Psychiatry and Behavioral Neurosciences, McMaster University, Hamilton, ON, Canada
- 4Faculty of Medicine, Hospital de Clínicas de Porto Alegre, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil
In this report, we aim to assess the interaction of bipolar disorder and major depressive disorder with the evolution of social roles, economic classification, and substance misuse in emerging adults. This is a longitudinal population-based study (n = 231 at baseline), in which participants were reassessed at a mean of 5 years after baseline. A structured clinical interview was used to diagnose the participants with bipolar disorder and major depression; a control group without mood disorders was included. Men with mood disorders were less likely to be married in the beginning of the study and less likely to work in the follow-up. Women with major depression were less likely to study and more likely to be in a lower economic class at the beginning of the study. In comparison, women with bipolar disorder were less likely to live with their parents and more likely to live with their children in the first wave of the study. Substance misuse was more likely in people with mood disorders, especially in men, and women with bipolar disorder had the highest likelihood in the follow-up. Albeit longitudinal analyses were limited by a possibly insufficient sample size and mediating mechanisms for change, such as stigma, were not explored, the study suggests sex-related specificities regarding the change in social roles and substance use in people with mood disorders. Emerging adults, especially those with mood disorders, are in a period of change and instability and at a greater risk for substance use and abuse.
Introduction
The way people live the period of their lives between 18 and 29 years old has changed substantially in the last 50 years. Demographic trends of a longer period of education and an older age to get married and have children have led to the proposal for a new developmental period, emerging adulthood (18–29 years old) (1, 2). This proposal arises as an attempt to describe what it means to be an adult and what defines the transition to adulthood, with cultural influences that change over time. This period is not just a brief transition, but a period of many changes and instabilities in different areas of life, a long phase before achieving stable adulthood (2). As a result, specific characteristics, even if not exclusive to the period, have been proposed for the emerging adult life, such as identity explorations, instability (romantic relationships, work, residence), focus on oneself (less daily social roles and obligations to others), “feeling in-between” (neither teenager nor adult) and possibilities or optimism (about the future; work and economic conditions) (1, 2). While the important experiences that make up this phase can be exciting, they can also be confusing and challenging. Involuntary changes, reduced social support, and high self-demand can all be associated with depressive and anxious symptoms in emerging adults (2).
Thus, some more prominent developmental challenges for the emerging adult age, such as the transition process from living with parents to no longer living with them, starting the journey to higher education, following a professional path, seeking financial autonomy, and finding a life partner, may be associated with the incidence of mental health problems at this stage (2). There are also aspects of brain development that make emerging adults especially vulnerable to mental disorders, such as the excessively rapid synaptic pruning (3), possibly having an interaction with the environment (4). As a result, the very fast synaptic reduction can increase the sensitivity to stress and turn the individual vulnerable to mental disorders (4). Multiple mental disorders are more prevalent during the emerging adult stage, especially mood disorders (5, 6). The onset of mental illness during emerging adulthood has the potential of adversely impacting development and identity formation (7).
Considering the impairments associated with major depressive disorder and bipolar disorder, such as functional impairment (family, social and occupational areas) (8–13), cognitive impairment (12, 14–17), poor quality of life (10), and the changes and uncertainties of the emerging adult phase, it is of extreme importance to monitor emerging adults with mental disorders. It is in this stage of life that there is the highest probability for the onset of bipolar disorder (18). This period can impose multiple challenges, from symptom management to maintaining functioning and relationships (19). In addition, recent evidence suggests that most subjects diagnosed with bipolar disorder transition to multiple episodes within 5 years of the onset of the disorder (20, 21).
Another point of convergence between the onset of certain mental disorders and this stage of life is substance use and misuse. Emerging adults are more likely to present substance abuse or dependence when compared to young adults (22). People with mood disorders have a high prevalence of comorbidity with substance use disorder (23–27). Post and Kalivas (28), postulated that cross-sensitization between stressors, episodes, and inadequate use of substances contribute to the progression of bipolar disorder (28).
The few longitudinal studies that have investigated the evolution of emerging adults with mental disorders tend to be based on clinical samples or of limited population generalizability (29, 30). In addition, there is a trend in the mood disorder literature to investigate only clinical outcomes, such as symptoms, mood episodes, and relapses. The investigation of the broader biopsychosocial development, such as leaving the parent’s house, the transition from study to work, and the constitution of new families has been less often investigated. Thus, the objective of the present study was to assess the interaction of bipolar disorder and major depressive disorder with social roles, economic classification, and substance misuse in emerging adults, in a longitudinal population-based study.
Materials and methods
Design and participants
In this cohort, we followed up matched cases and controls nested in a population-based sample. Full descriptions of the original study have been published elsewhere (31–33). Briefly, initially, 1,560 participants aged between 18 and 24 were assessed in the period from 2007 to 2009; sample selection was performed by clusters. Eighty-nine census-based urban sectors were randomly selected from the city of Pelotas, in South Brazil (34). For this nested sample, every participant with a past or current history of a manic or hypomanic episode from the population-based study was included at baseline. Ninety-three individuals met this criterion by Mini International Neuropsychiatric Interview (MINI) (35, 36). Two comparison groups were recruited. People without any history of mood episodes were randomly selected and frequency-matched for sex, age, and economic situation, i.e., a healthy control sample. We also recruited a group with a current depression but no past history of (hypo) mania. Other mental disorders or clinical morbidity, including substance use, were not a reason for exclusion. We were able to obtain data on 231 subjects (83% of the intended sample) at baseline. The whole matched sample of cases and controls further underwent the Structured Clinical Interview for DSM-IV (SCID) (37, 38) to confirm diagnoses and improve reliability, and this is the group-defining criterion for this study. After SCID diagnoses, the final baseline sample consisted of 93 participants without any history of mood episodes, 83 participants with major depression, and 55 with bipolar disorder (33 type I and 22 type II) (31, 33).
Second wave data were collected between 2012 and 2014. The 231 participants were invited to return for a follow-up assessment after a mean of 5 years post-baseline (39, 40). Master’s or Ph.D. level psychologists again evaluated current mood status using the Mini International Neuropsychiatric Interview (MINI-PLUS) (35, 36), and in cases of diagnostic doubt, reassessments were conducted with the SCID (37, 38). Those who consented to participate in the study signed an informed consent form. Participants who had a psychiatric disorder at baseline, as well as at the 5-year follow-up, were referred for treatment at the Clinic of Research and Extension in Mental Health of the Universidade Católica de Pelotas. The Research Ethics Committees of the Universidade Católica de Pelotas and Hospital de Clínicas de Porto Alegre approved the study.
Instruments
Participants answered a questionnaire with sociodemographic variables, including age, sex, having a partner, living with offspring, and occupational status (work and study). Economic status was defined according to the criteria of the Brazilian Association of Research Companies (41). This instrument measures economic classification through the accumulation of material goods (color television, radio, bathroom, automobiles, monthly employee, washing machine, VCR/DVD, refrigerator, freezer—independent appliance or part of the duplex refrigerator) and the level of schooling of the householder. The sum of the points results in a total score, classified into five groups (A, B, C, D, and E), where “A” refers to the highest economic classification and “E” to the lowest, consistent with previous research, we dichotomize participants into two categories, A/B/C (high) and D/E (low). Substance use disorders (tobacco, alcohol, and other substances) were assessed with the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) (42, 43), with a cutoff of four. The ASSIST was used at baseline and follow-up assessment (39, 44, 45).
Statistical analysis
We use chi-squared statistics to investigate differences in proportions. A generalized estimating equations (GEE) model with Poisson distribution and robust standard errors was used to investigate differences in proportions between diagnostic groups and from baseline to endpoint. The model includes diagnosis, sex, follow-up wave, and interactions between group and sex and group and wave.
Results
Two hundred and seven (89.6%) out of the 231 individuals assessed at baseline were re-assessed at follow-up. The baseline sample consisted of 158 (68.4%) women. More than half of the sample identified themselves as having white skin color (153; 66.2%). The average age at baseline was 22.04 (s.d. 2.18), and the average time between the two assessments was 5 years (Table 1).

Table 1. Sample characteristics according to baseline diagnosis.
Considering the entire sample in the follow-up assessment, there were significantly more people working (OR = 4.46; 95%CI: 2.97–6.70; p < 0.001), living with a partner (OR = 2.29; 95%CI: 1.54–3.40; p < 0.001), who were living with their children (OR = 2.51; 95%CI: 1.68–3.74; p < 0.001), and fewer people studying (OR 0.41;95%CI: 0.27–0.63; p < 0.001) or living with their parents (OR = 0.26; 95%CI: 0.17–0.38; p < 0.001). In addition, there were fewer people in the economic classes D or E (lowest classes) (OR = 0.30; 95%CI: 0.15–0.60; p < 0.001).
Several differences were observed between baseline and the 5-year follow-up, as well as between the diagnostic groups. There were changes in working and living, and the explanatory analysis suggested different patterns of change associated with group and sex (Figure 1). Men with mood disorders were less likely to be working at follow-up and to be married at baseline; for substance use disorders, men already had differences in mood disorder groups at baseline. Women with mood disorders had a lower chance of being currently studying at baseline and a higher chance of already having children of their own and not living with their parents at baseline; they were also more likely to present substance use disorders in the 5-year follow-up. All the people in the control group left the lower economic classes, which did not happen in the mood disorders groups.
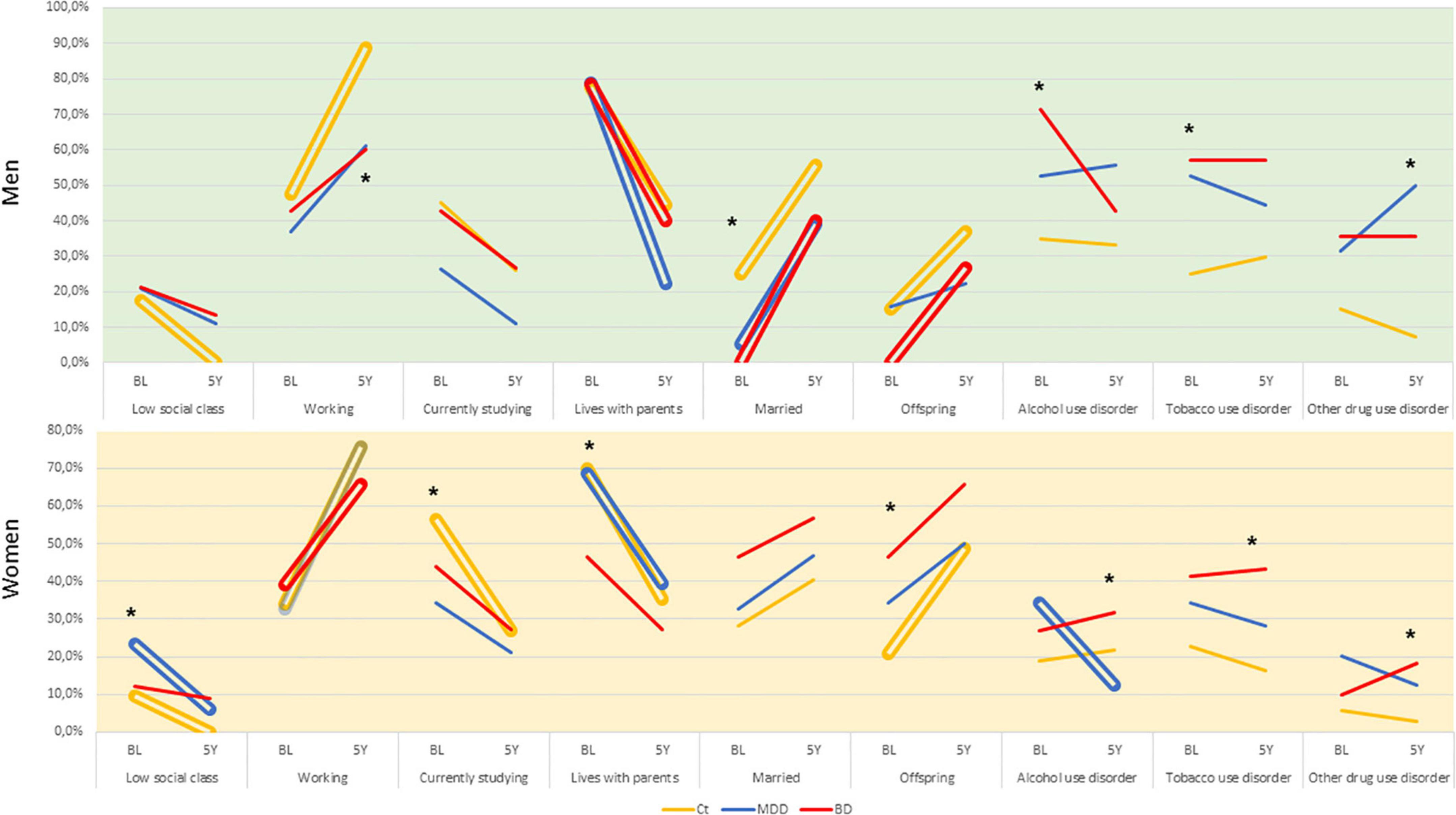
Figure 1. Changes in socioeconomic variables and substance abuse/dependence according sex at baseline and 5-year follow-up in emerging adults with and without mood disorders. Double bars indicate significant within-group changes (p < 0.05) and asterisks indicate significant between-group changes (p < 0.05).
The GEE models, however, tended to retain only the main effects of time and diagnostic group, with a few interesting exceptions. Having a partner was significantly more likely for women in both mood disorder groups and living with their children was more likely for women with bipolar disorder (Table 2).
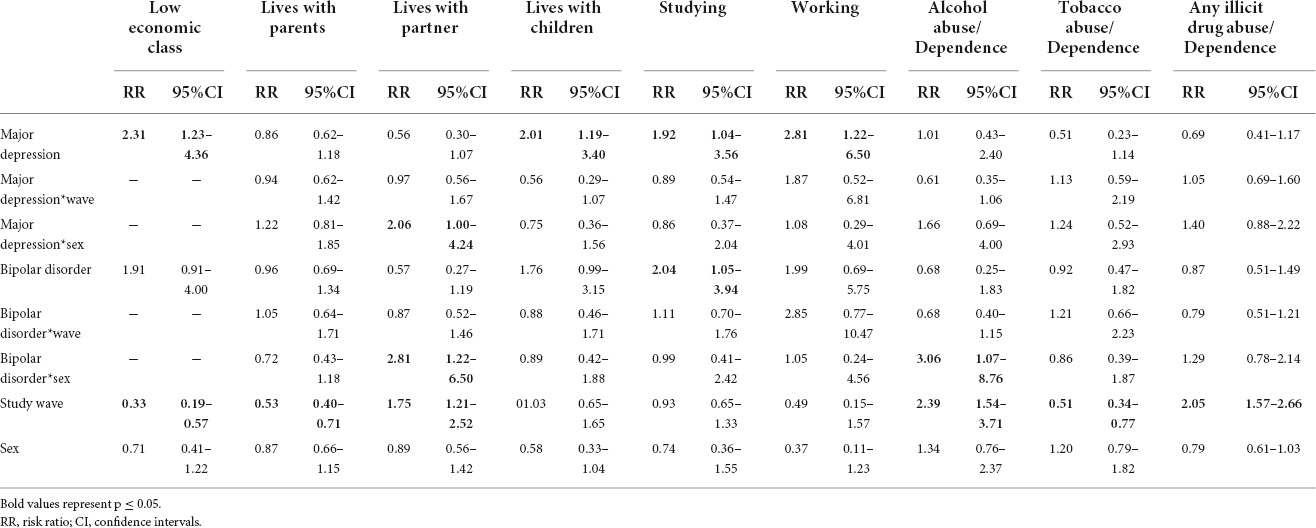
Table 2. Effects of diagnosis, sex, and study wave on socioeconomic variables and substance abuse/dependence in the final model (n = 231).
Discussion
This study explored psychosocial changes over an average period of 5 years in a population-based sample of emerging adults. In general, the changes tended to follow an expected pattern—young people left home, many stopped studying and started working, got married, and started a new family. In groups diagnosed with a mood disorder, exploratory analyses suggested some potentially relevant deviations. Many differences were already present at baseline, especially in men regarding substance misuse. Women, especially with bipolar disorder, at baseline were already more likely to have left their parents’ house, to be married, and be living with their own children. For both sexes, there was a significant change in economic class, and none of the controls were in the lower classes at follow-up, which was not true for the groups with mood disorders.
According to Arnett et al. (2), emerging adults, unlike teenagers, have reached physical and sexual maturity, are legally responsible for their actions, and present diversities in their combinations of educational and occupational trajectories. In contrast with young adults in their thirties, most emerging adults have not yet established a stable structure in adult life, with long-term commitments in love and work relationships (2). Even when considering this instability and variability common to the emerging adulthood phase, the changes found between the groups studied here suggest the possibility of significantly different courses for emerging adults with mood disorders. Some findings from the exploratory analyses suggest that women with mood disorders already have more characteristics of young adults at this stage, married and living with children. Men with mood disorders, on the other hand, seemed to be much less likely to be working at follow-up, which possibly already reflects some degree of impairment associated with the disorder.
In this period of so many new challenges, family relationships can have a significant impact on this important journey of emerging adults. In a study conducted with 1,502 undergraduate students, it was found that family plays a fundamental role in the psychological wellbeing of emerging adults. Parental support for autonomy, low levels of behavioral and psychological control were found to be important factors for having a higher level of psychological adjustment among emerging adults (46). In contrast, there is also the impact of a dysfunctional family dynamic, as well as a family history of psychiatric illness. A cross-sectional population-based study found that a family history of mood disorders was associated with mood disorders in emerging adults and childhood traumas. In that study, it was also found that childhood trauma was a mediating factor for the association between a family history of mood disorder and mood disorder in emerging adulthood (47). The phenomenon characterized here may be related to our finding and the history of mental illness in the family is an additional complicating factor in the transition, causing, for example, emerging adults with bipolar disorder to leave their parents’ home earlier to avoid abusive relationships.
In the present study, we found that women at baseline, especially those with bipolar disorder, were already more likely to have left their parents’ home, to be married, and living with children. The literature shows that among subjects with bipolar disorder, women are more likely to marry than men. Lieberman et al. (48) found in their study that among men with bipolar disorder, those who were never married were more likely to have bipolar disorder I and earlier onset of illness compared to married men. Furthermore, it was observed that among women with bipolar disorder, those who were married showed an improvement in the course of the disease, with a reduction in depressive episodes over a 2-year period and a lower cumulative depression severity when compared to those who were not married. However, marriage was not associated with a difference in the course of the disorder among married men, suggesting that women may be more sensitive to the positive effects of social support available in a stable marital relationship (48). In addition, men with mood disorders may present a lower chance of being married, as they are at the beginning of the disorder and face symptoms differently compared to women.
The problematic use of substances may be one of the responsible factors for these trajectories. Emerging adults are in a period of many changes and instabilities, and at a greater risk for substance use and abuse (49, 50). In addition to emerging adults (18–25 years) presenting a higher prevalence of mental health problems and substance use disorders, they also present lower treatment rates (51). In the present study, the prevalence of substance use disorders was greater in participants with mood disorders. We also found that, in addition to the higher prevalence of substance use disorders among men with mood disorders, an increase was observed among women with bipolar disorder at follow-up. According to the literature, there is a higher prevalence of substance use disorders in men in this period, compared to women (22, 51). Men with major depressive episodes are more likely to report alcohol abuse/dependence (22).
Overall, women start using drugs at lower doses than men, but drug use evolves more quickly into addiction, and they face a higher risk of negative health consequences and relapse after abstinence (52). This could be one of the explanations as to why the prevalence of substance use disorders in women with bipolar disorder increased at follow-up. Another possible explanation is that substance use may be less socially acceptable for women than for men. In this case, women who develop a substance use disorder may represent the more severely affected people with a higher risk of psychiatric comorbidity, as mentioned in another study (53). The fact that substance misuse is already installed at this stage implies additional difficulties for the development of emerging adults. These relationships are complex, and substance use can also be related to the onset of mood disorders or to a complicated course of illness (54). It can also be an additional burden that makes it difficult to adapt to new stages of development.
It is in the emerging adult phase that many people first enter into the labor market and face the challenges of being admitted to desired jobs (1), and paid work can be a marker of social inclusion and status (55). In addition, there is a relationship between mental disorders and unemployment, underemployment, temporary leave, and retirement (30, 56–58). Butterworth et al. (59), observed in a longitudinal study that impairments in the mental health state of individuals assessed at baseline, for example, symptoms of depression, were predictors of underemployment in subsequent years. In the present study, we found that men with mood disorders seemed to be less likely to be working in the follow-up. According to the systematic review of Marwaha et al. (55), people with bipolar disorder early in the course of the illness tend to have higher employment rates than later in the course of illness and that employment patterns may differ depending on the stage of the disorder. For people with mental illness, work is perceived as an important component for their recovery (60). As found by Luo et al. (61), the relationship between work and the course of the illness possibly has effects to a greater degree for men than for women with major depressive disorder (61). We can also think that the duration of unemployment is possibly greater for men with mood disorders than for women (59).
Despite possibly being an unstable journey (2), individuals in the emerging adult age tend to initiate a movement toward financial autonomy. However, people with mental disorders often have impairments in their functioning, including in the workplace (8–10, 13, 62–64). This will possibly have an impact on their economic conditions. Hakulinen et al. (57) found in a cohort study (measured years 1988–2015) that earnings for individuals with severe mental disorders were considerably low and that the mean total annual income remained stable between 25 and 52 years for most groups of mental disorders (57). Recently, Cao et al. (65) found a unidirectional effect from depression to financial stress on emerging adults. In addition, a case-control study carried out from records from all individuals (N = 50,551) who were hospitalized for severe mental disorders, including bipolar disorder, between 1988 and 2015 in Finland found that, on average, during the year when the first inpatient diagnosis was given, individuals with bipolar disorder were earning 76% of the total income earned by the control group. Five years later they were earning 67% and 10 years later they were earning 66% (30). Similar findings were observed in a longitudinal study conducted in Taiwan, showing that the probability of switching to a person without income is significantly higher in patients with bipolar disorder than in controls over time (29).
In the present study, differences in economic class change may have occurred due to a series of factors related to the mental illness. Mood disorders are associated with impairment of occupational functioning, possibly associated with cognitive difficulties directly resulting from the illness or its treatment (12, 14, 16, 17, 66–68). Furthermore, depression has been associated with an increased risk of unemployment, particularly for those with less education (69). Educational level is an additional predictor of future employment in mood disorders (70). The early onset of mood disorders can have a negative impact on the educational process, often leading to interruption of studies in youth (55). Mental illness can also impair social skills directly relevant to functioning. Close to 30–60% of people with bipolar disorder fail to regain full functioning in the occupational and social domains (71). Another area that can cause harm is the stigma associated with mental disorders (72). Substance use can also play a role in limiting youth performance and opportunities. Due to the low rate of functional recovery in individuals with severe mental disorders, they have a great likelihood of receiving a permanent or temporary disability pension after they are diagnosed. In Finland, after the onset of a severe mental disorder, the disability pension is the main source of income for most individuals with severe mental disorder and their long-term economic wellbeing depends largely on this pension (30). In Brazil, a multicenter study carried out with 2,475 patients with mental disorders, found that 35.6% of the sample received disability benefits or retirement, and 46.6% of the patients had no individual source of income or obtained income that was not related to work activity, such as assistance from the State, pension, assistance from family members (56, 62). Few studies have assessed economic status prospectively.
Arnett’s theory of emerging adulthood has been based mainly on subjects living in developed countries (1). In Brazil, economic and cultural issues can be quite different when compared to developed countries, and this may influence the characteristics of this stage of life, which may be a conceptual limitation to link our findings with a context of this stage. Here, we could not assess the self-stigma and social stigma of the disease, a possible mechanism underlying some of the findings. It is also possible that the study was underpowered to detect some relevant differences between time and sex interactions. Here we also only assessed two time points within this sensitive period. Future cohort assessments should be able to clarify some effects found. Longitudinal studies that monitor the periods of change during this phase may also contribute to the improvement of preventive and treatment actions, especially when it comes to substance misuse. The effect of early treatment was also not assessed here. Future studies with a qualitative approach may also contribute to a greater understanding of the facilitators and barriers present in the development of this phase. Despite these limitations, a major difference of the present study is that it included a community sample of emerging adults and analyzed several social aspects in a longitudinal design.
The trajectories of emerging adulthood in young people with mood disorders that we examined here may suggest pathways potentially associated with impairment, with relevant consequences. In this sensitive period, the acquisition of certain skills is expected, and significant deviations here can lead to impairments in functioning associated with difficulties in the ability to work and develop interpersonal relationships. A marker of emerging adulthood, substance use, can have significant interactions with mood disorders and should be a focus of investigation associated with these impairments. These findings also reinforce the probable impacts that early diagnosis and interventions may have on social, occupational, and education skills and also on the risks of substance misuse during this period.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Comitê de Ética e Pesquisa do Hospital de Clínicas de Porto Alegre. The patients/participants provided their written informed consent to participate in this study.
Author contributions
All authors made substantial contributions to the conception or design of the work, the acquisition, analysis, and interpretation of data for the work, and drafting of the work, revised it critically for important intellectual content, approved the version to be published, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This work was supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (KJ, #422500/2016-0), the Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (RS, #17/2551-0001433-2 and #19/2551-0000689-6), and the Instituto Nacional de Ciência e Tecnologia Translacional em Medicina [FK, Fundação de Amparo à Pesquisa do Estado de São Paulo (#2014/50891-1), and the Conselho Nacional de Desenvolvimento Científico e Tecnológico (#465458/2014-9)]. Also financed in part by Fundo de Incentivo á Pesquisa (FIPE/HCPA) and the Coordenação de Aperfeiaçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001 and received financial support from Conselho Nacional de Desenvolvimento Científico e Tecnológico (Brasil).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Arnett JJ. Emerging adulthood: a theory of development from the late teens through the twenties. Am Psychol. (2000) 55:469–80. doi: 10.1037/0003-066X.55.5.469
2. Arnett JJ, Žukauskiene R, Sugimura K. The new life stage of emerging adulthood at ages 18-29 years: implications for mental health. Lancet Psychiatry. (2014) 1:569–76. doi: 10.1016/S2215-0366(14)00080-7
3. Taber-Thomas B, Peréz-Edgar K. Emerging adulthood brain development. In: JJ Arnett editor. Oxford Handbook of Emerging Adulthood. New York, NY: Oxford University Press (2015).
4. Rapoport JL, Giedd JN, Gogtay N. Neurodevelopmental model of schizophrenia: update 2012. Mol Psychiatry. (2012) 17:1228–38. doi: 10.1038/mp.2012.23
5. Kessler RC, Amminger GP, Aguilar-Gaxiola S, Alonso J, Lee S, Ustün TB. Age of onset of mental disorders: a review of recent literature. Curr Opin Psychiatry. (2007) 20:359–64. doi: 10.1097/YCO.0b013e32816ebc8c
6. Solmi M, Radua J, Olivola M, Croce E, Soardo L, Salazar de Pablo G II, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. (2021) 27:281–95. doi: 10.1038/s41380-021-01161-7
7. Potterton R, Austin A, Robinson L, Webb H, Allen KL, Schmidt U. Identity development and social-emotional disorders during adolescence and emerging adulthood: a systematic review and meta-analysis. J Youth Adolesc. (2022) 51:16–29. doi: 10.1007/s10964-021-01536-7
8. Fleck MP, Lima AF, Louzada S, Schestasky G, Henriques A, Borges VR, et al. Association of depressive symptoms and social functioning in primary care service. Brazil. Rev Saude Publica. (2002) 36:431–8. doi: 10.1590/s0034-89102002000400008
9. Hilty DM, Brady KT, Hales RE. A review of bipolar disorder among adults. Psychiatr Serv. (1999) 50:201–13. doi: 10.1176/ps.50.2.201
10. Magalhães PVS, Dodd S, Nierenberg AA, Berk M. Cumulative morbidity and prognostic staging of illness in the systematic treatment enhancement program for bipolar disorder (STEP-BD). Aust N Z J Psychiatry. (2012) 46:1058–67. doi: 10.1177/0004867412460593
11. Martinez-Aran A, Vieta E, Torrent C, Sanchez-Moreno J, Goikolea JM, Salamero M, et al. Functional outcome in bipolar disorder: the role of clinical and cognitive factors. Bipolar Disord. (2007) 9:103–13. doi: 10.1111/j.1399-5618.2007.00327.x
12. Martínez-Arán A, Vieta E, Reinares M, Colom F, Torrent C, Sánchez-Moreno J, et al. Cognitive function across manic or hypomanic, depressed, and euthymic states in bipolar disorder. Am J Psychiatry. (2004) 161:262–70. doi: 10.1176/appi.ajp.161.2.262
13. Rosa AR, Reinares M, Michalak EE, Bonnin CM, Sole B, Franco C, et al. Functional impairment and disability across mood states in bipolar disorder. Value Heal. (2010) 13:984–8. doi: 10.1111/j.1524-4733.2010.00768.x
14. Godard J, Baruch P, Grondin S, Lafleur MF. Psychosocial and neurocognitive functioning in unipolar and bipolar depression: a 12-month prospective study. Psychiatry Res. (2012) 196:145–53. doi: 10.1016/j.psychres.2011.09.013
15. Hellvin T, Sundet K, Simonsen C, Aminoff SR, Lagerberg TV, Andreassen OA, et al. Neurocognitive functioning in patients recently diagnosed with bipolar disorder. Bipolar Disord. (2012) 14:227–38. doi: 10.1111/j.1399-5618.2012.01004.x
16. Kozicky JM, Torres IJ, Silveira LE, Bond DJ, Lam RW, Yatham LN. Cognitive change in the year after a first manic episode: association between clinical outcome and cognitive performance early in the course of bipolar I disorder. J Clin Psychiatry. (2014) 75:e587–93. doi: 10.4088/JCP.13m08928
17. Malhi GS, Ivanovski B, Hadzi-Pavlovic D, Mitchell PB, Vieta E, Sachdev P. Neuropsychological deficits and functional impairment in bipolar depression, hypomania and euthymia. Bipolar Disord. (2007) 9:114–25. doi: 10.1111/j.1399-5618.2007.00324.x
18. Dell’Osso B, Grancini B, Vismara M, De Cagna F, Maggi M, Molle M, et al. Age at onset in patients with bipolar I and II disorder: a comparison of large sample studies. J Affect Disord. (2016) 201:57–63. doi: 10.1016/j.jad.2016.04.009
19. Smyth K, Salloum A, Herring J. Interpersonal functioning, support, and change in early-onset bipolar disorder: a transcendental phenomenological study of emerging adults. J Ment Health. (2021) 30:121–8. doi: 10.1080/09638237.2020.1713997
20. Martinez-Aran A, Bonnin C, Torrent C, Soleì B, Torres I, Jimeìnez E. Cognition and illness progression in bipolar disorder. In: F Kapczinski editor. Neuroprogression and Staging in Bipolar Disorder. Oxford: Oxford University Press (2015). p. 99–113.
21. van der Markt A, Klumpers UM, Draisma S, Dols A, Nolen WA, Post RM, et al. Testing a clinical staging model for bipolar disorder using longitudinal life chart data. Bipolar Disord. (2019) 21:228–34. doi: 10.1111/bdi.12727
22. Qadeer RA, Georgiades K, Boyle MH, Ferro MA. An epidemiological study of substance use disorders among emerging and young adults. Can J Psychiatry. (2019) 64:313–22. doi: 10.1177/0706743718792189
23. Lasser K, Boyd JW, Woolhandler S, Himmelstein DU, McCormick D, Bor DH. Smoking and mental illness: a population-based prevalence study. JAMA. (2000) 284:2606–10. doi: 10.1001/jama.284.20.2606
24. Merikangas KR, Herrell R, Swendsen J, Rössler W, Ajdacic-Gross V, Angst J. Specificity of bipolar spectrum conditions in the comorbidity of mood and substance use disorders: results from the Zurich cohort study. Arch Gen Psychiatry. (2008) 65:47–52. doi: 10.1001/archgenpsychiatry.2007.18
25. Perlis RH, Miyahara S, Marangell LB, Wisniewski SR, Ostacher M, DelBello MP, et al. Long-term implications of early onset in bipolar disorder: data from the first 1000 participants in the systematic treatment enhancement program for bipolar disorder (STEP-BD). Biol Psychiatry. (2004) 55:875–81. doi: 10.1016/j.biopsych.2004.01.022
26. Regier DA, Farmer ME, Rae DS, Locke BZ, Keith SJ, Judd LL, et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the epidemiologic catchment area (ECA) study. JAMA. (1990) 264:2511–8.
27. Subramaniam M, Abdin E, Vaingankar JA, Chong SA. Prevalence, correlates, comorbidity and severity of bipolar disorder: results from Singapore mental health study. J Affect Disord. (2013) 146:189–96. doi: 10.1016/j.jad.2012.09.002
28. Post RM, Kalivas P. Bipolar disorder and substance misuse: pathological and therapeutic implications of their comorbidity and cross-sensitisation. Br J Psychiatry. (2013) 202:172–6. doi: 10.1192/bjp.bp.112.116855
29. Chang HC, Huang KC, Chiu WC, Huang KC, Tang CH, Su KP. Change in employment status in bipolar disorder: a longitudinal study using national claims data. J Clin Psychiatry. (2016) 77:e429–35. doi: 10.4088/JCP.14m09
30. Hakulinen C, Elovainio M, Arffman M, Lumme S, Suokas K, Pirkola S, et al. Employment status and personal income before and after onset of a severe mental disorder: a case-control study. Psychiatr Serv. (2020) 71:250–5. doi: 10.1176/appi.ps.201900239
31. Jansen K, Magalhães PVS, Pinheiro RT, Kapczinski F, Silva RA. Early functional impairment in bipolar youth: a nested population-based case-control study. J Affect Disord. (2012) 142:208–12. doi: 10.1016/j.jad.2012.04.028
32. Jansen K, Ores LC, Cardoso TA, Lima RC, Souza LDM, Magalhães PVS, et al. Prevalence of episodes of mania and hypomania and associated comorbidities among young adults. J Affect Disord. (2011) 130:328–33. doi: 10.1016/j.jad.2010.10.007
33. Magalhães PVS, Jansen K, Pinheiro RT, Colpo GD, Da Motta LL, Klamt F, et al. Peripheral oxidative damage in early-stage mood disorders: a nested population-based case-control study. Int J Neuropsychopharmacol. (2012) 15:1043–50. doi: 10.1017/S1461145711001532
34. Jansen K, Mondin TC, Cardoso TA, Ores LC, Souza LDM, Pinheiro RT, et al. Quality of life and mood disorder episodes: community sample. J Affect Disord. (2013) 147:123–7. doi: 10.1016/j.jad.2012.10.021
35. Amorim P. Mini international neuropsychiatric interview (MINI): validação de entrevista breve para diagnóstico de transtornos mentais. Rev Bras Psiquiatr. (2000) 22:106–15. doi: 10.1590/s1516-44462000000300003
36. Sheehan D, Lecrubier Y, Sheehan K, Amorim P, Janavs J, Weiller E, et al. The mini-international neuropsychiatric interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. (1998) 59(Suppl. 20):22–33.
37. Del-Ben CM, Vilela JAA, Crippa JA, de S, Hallak JEC, Labate CM, et al. Confiabilidade da “entrevista clínica estruturada para o dsm-iv - versão clínica” traduzida para o Português. Rev Bras Psiquiatr. (2001) 23:156–9. doi: 10.1590/s1516-44462001000300008
38. First M, Spitzer R, Gibbon M, Williams J. Structured Clinical Interview for DSM-IV axis I Disorders: Clinician Version (SCID-CV). Washington. DC: American Psychiatric Press (1996).
39. Cardoso TDA, Mondin TC, Souza LDDM, Da Silva RA, Magalhães PVS, Kapczinski F, et al. Functioning in bipolar disorder with substance abuse/dependence in a community sample of young adults. J Affect Disord. (2015) 187:179–82. doi: 10.1016/j.jad.2015.08.046
40. Vieira DC, Cardoso TA, Mondin TC, Jansen K, Silva RA, Souza LDM, et al. Mood disorders and prospective suicidality in young adults: a population-based cohort study. Acta Psychiatr Scand. (2018) 137:109–15. doi: 10.1111/acps.12846
41. ABEP. Classificação Econômica Brasil. (2008). Available online at: http://www.abep.org (accessed June 4, 2014)
42. Henrique IFS, De Micheli D, Lacerda RB, Lacerda LA, Formigoni ML. Validation of the Brazilian version of alcohol, smoking and substance involvement screening test (ASSIST). Rev Assoc Med Bras. (2004) 50:199–206. doi: 10.1590/S0104-42302004000200039
43. Who Assist Working Group. The alcohol, smoking and substance involvement screening test (ASSIST): development, reliability and feasibility. Addiction. (2002) 97:1183–94. doi: 10.1046/j.1360-0443.2002.00185.x
44. Narvaez JC, Pechansky F, Jansen K, Pinheiro RT, Silva RA, Kapczinski F, et al. Quality of life, social functioning, family structure, and treatment history associated with crack cocaine use in youth from the general population. Braz J Psychiatry. (2015) 37:211–8. doi: 10.1590/1516-4446-2014-1494
45. Narvaez JC, Jansen K, Pinheiro RT, Kapczinski F, Silva RA, Pechansky F, et al. Psychiatric and substance-use comorbidities associated with lifetime crack cocaine use in young adults in the general population. Compr Psychiatry. (2014) 55:1369–76. doi: 10.1016/j.comppsych.2014.04.021
46. Mendoza MCG, Queija IS, Jiménez ÁP. The role of parents in emerging adults’ psychological well-being: a person-oriented approach. Fam Process. (2019) 58:954–71. doi: 10.1111/famp.12388
47. Jansen K, Cardoso TA, Fries GR, Branco JC, Silva RA, Kauer-Sant’Anna M, et al. Childhood trauma, family history, and their association with mood disorders in early adulthood. Acta Psychiatr Scand. (2016) 134:281–6. doi: 10.1111/acps.12551
48. Lieberman DZ, Massey SH, Goodwin FK. The role of gender in single vs married individuals with bipolar disorder. Compr Psychiatry. (2010) 51:380–5. doi: 10.1016/j.comppsych.2009.10.004
49. Skidmore CR, Kaufman EA, Crowell SE. Substance use among college students. Child Adolesc Psychiatr Clin N Am. (2016) 25:735–53. doi: 10.1016/j.chc.2016.06.004
50. Stone AL, Becker LG, Huber AM, Catalano RF. Review of risk and protective factors of substance use and problem use in emerging adulthood. Addict Behav. (2012) 37:747–75. doi: 10.1016/j.addbeh.2012.02.014
51. Adams SH, Knopf DK, Jane Park M. Prevalence and treatment of mental health and substance use problems in the early emerging adult years in the United States: findings from the 2010 national survey on drug use and health. Emerg Adult. (2014) 2:163–72. doi: 10.1177/2167696813513563
52. Ait-Daoud N, Blevins D, Khanna S, Sharma S, Holstege CP, Amin P. Women and addiction: an update. Med Clin. (2019) 103:699–711. doi: 10.1016/j.mcna.2019.03.002
53. Zilberman ML, Tavares H, Blume SB, El-Guebaly N. Substance use disorders: sex differences and psychiatric comorbidities. Can J Psychiatry. (2003) 48:5–13. doi: 10.1177/070674370304800103
54. Lalli M, Brouillette K, Kapczinski F, Cardoso TA. Substance use as a risk factor for bipolar disorder: a systematic review. J Psychiatr Res. (2021) 144:285–95. doi: 10.1016/j.jpsychires.2021.10.012
55. Marwaha S, Durrani A, Singh S. Employment outcomes in people with bipolar disorder: a systematic review. Acta Psychiatr Scand. (2013) 128:179–93. doi: 10.1111/acps.12087
56. Assunção AA, Lima EP, Guimarães MDC. Transtornos mentais e inserção no mercado de trabalho no Brasil: um estudo multicêntrico nacional. Cad Saúde Pública. (2017) 33:e00166815. doi: 10.1590/0102-311X00166815
57. Hakulinen C, Elovainio M, Arffman M, Lumme S, Pirkola S, Keskimäki I, et al. Mental disorders and long-term labour market outcomes: nationwide cohort study of 2 055 720 individuals. Acta Psychiatr Scand. (2019) 140:371–81. doi: 10.1111/acps.13067
58. Silva EBF, Tomé LAO, Costa T, de JG, Santana M, da CCP. Transtornos mentais e comportamentais: perfil dos afastamentos de servidores públicos estaduais em Alagoas, 2009. Epidemiol Serv Saúde. (2012) 21:505–14. doi: 10.5123/S1679-49742012000300016
59. Butterworth P, Leach LS, Pirkis J, Kelaher M. Poor mental health influences risk and duration of unemployment: a prospective study. Soc Psychiatry Psychiatr Epidemiol. (2012) 47:1013–21. doi: 10.1007/s00127-011-0409-1
60. Dunn EC, Wewiorski NJ, Rogers ES. The meaning and importance of employment to people in recovery from serious mental illness: results of a qualitative study. Psychiatr Rehabil J. (2008) 32:59–62. doi: 10.2975/32.1.2008.59.62
61. Luo Z, Cowell AJ, Musuda YJ, Novak SP, Johnson EO. Course of major depressive disorder and labor market outcome disruption. J Ment Health Policy Econ. (2010) 13:135–49.
62. Frey BN, Vigod S, de Azevedo Cardoso T, Librenza-Garcia D, Favotto L, Perez R, et al. The early burden of disability in individuals with mood and other common mental disorders in Ontario, Canada. JAMA Netw Open. (2020) 3:e2020213. doi: 10.1001/jamanetworkopen.2020.20213
63. Martinez-Aran A, Vieta E, Torrent C, Sanchez-Moreno J, Goikolea JM, Salamero M, et al. Functional outcome in bipolar disorder: the role of clinical and cognitive factors. Bipolar Disord. (2007) 9:103–13. doi: 10.1111/j.1399-5618.2007.00327.x
64. Martínez-Arán A, Vieta E, Colom F, Torrent C, Sánchez-Moreno J, Reinares M, et al. Cognitive impairment in euthymic bipolar patients: implications for clinical and functional outcome. Bipolar Disord. (2004) 6:224–32. doi: 10.1111/j.1399-5618.2004.00111.x
65. Cao H, Zhou N, Li X, Serido J, Shim S. Temporal dynamics of the association between financial stress and depressive symptoms throughout the emerging adulthood. J Affect Disord. (2021) 282:211–8. doi: 10.1016/j.jad.2020.12.166
66. Hellvin T, Sundet K, Simonsen C, Aminoff SR, Lagerberg TV, Andreassen OA, et al. Neurocognitive functioning in patients recently diagnosed with bipolar disorder. Bipolar Disord. (2012) 14:227238. doi: 10.1111/j.1399-5618.2012.01004.x
67. Simonsen C, Sundet K, Vaskinn A, Birkenaes AB, Engh JA, Hansen CF, et al. Neurocognitive profiles in bipolar I and bipolar II disorder: differences in pattern and magnitude of dysfunction. Bipolar Disord. (2008) 10:245–55. doi: 10.1111/j.1399-5618.2007.00492.x
68. Solé B, Bonnin CM, Torrent C, Balanzá-Martínez V, Tabarés-Seisdedos R, Popovic D, et al. Neurocognitive impairment and psychosocial functioning in bipolar II disorder. Acta Psychiatr Scand. (2012) 125:309–17. doi: 10.1111/j.1600-0447.2011.01759.x
69. Dooley D, Prause J, Ham-Rowbottom KA. Underemployment and depression: longitudinal relationships. J Health Soc Behav. (2000) 41:421–36.
70. Gilbert E, Marwaha S. Predictors of employment in bipolar disorder: a systematic review. J Affect Disord. (2013) 145:156–64. doi: 10.1016/j.jad.2012.07.009
71. MacQueen GM, Young LT, Joffe RT. A review of psychosocial outcome in patients with bipolar disorder. Acta Psychiatr Scand. (2001) 103:163–70. doi: 10.1034/j.1600-0447.2001.00059.x
Keywords: emerging adults, mood disorder, substance use disorder, social roles, economic status, longitudinal studies
Citation: Farias CdA, Cardoso TdA, Silva MMd, D’Angelo F, Mondin TC, Souza LDdM, Silva RAd, Kapczinski F, Jansen K and Magalhães PVS (2022) Socioeconomic and substance use changes in emerging adults and their relationship with mood disorders in a population-based cohort. Front. Psychiatry 13:932484. doi: 10.3389/fpsyt.2022.932484
Received: 29 April 2022; Accepted: 04 August 2022;
Published: 24 August 2022.
Edited by:
Carlos Roncero, University of Salamanca, SpainReviewed by:
Lucas França Garcia, University Center of Maringá (UniCesumar), BrazilCélia Costa Franco, Coimbra Hospital and University Center, Portugal
Copyright © 2022 Farias, Cardoso, Silva, D’Angelo, Mondin, Souza, Silva, Kapczinski, Jansen and Magalhães. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pedro V. S. Magalhães, cGVkcm9tYWdhMkBnbWFpbC5jb20=