 Antonio Del Casale
Antonio Del Casale Martina Nicole Modesti
Martina Nicole Modesti Ludovica Rapisarda
Ludovica Rapisarda Paolo Girardi1
Paolo Girardi1 Renata Tambelli
Renata Tambelli- 1Department of Dynamic and Clinical Psychology, and Health Studies, Faculty of Medicine and Psychology, Sapienza University, Rome, Italy
- 2Unit of Psychiatry, ‘Sant'Andrea' University Hospital, Rome, Italy
- 3Faculty of Medicine and Psychology, Sapienza University, Rome, Italy
As COVID-19 pandemic spread all over the world, it brought serious health consequences in every medical field, including mental health. Not only healthcare professionals were more prone to develop anxiety, depression, and stress, but the general population suffered as well. Some of those who had no prior history of a psychiatric disease developed peculiar symptoms following infection with SARS-CoV-2, mostly because of psychological and social issues triggered by the pandemic. People developed traumatic memories, and hypochondria, probably triggered by social isolation and stress. Infection with SARS-CoV-2 has influenced the mental health of psychiatric patients as well, exacerbating prior psychiatric conditions. In this review, we focus on analyzing those cases of mania in the context of bipolar disorder (BD) reported after COVID-19 disease, both in people with no prior psychiatric history and in psychiatric patients who suffered an exacerbation of the disease. Results have shown that COVID-19 may trigger a pre-existing BD or unmask an unknown BD, due to social and psychological influences (decreased social interaction, change in sleep patterns) and through biological pathways both (neuroinflammation and neuroinvasion through ACE-2 receptors expressed in the peripheral and central nervous systems (PNS and CNS respectively). No direct correlation was found between the severity of COVID-19 disease and manic symptoms. All cases presenting severe symptoms of both diseases needed specific medical treatment, meaning that they concur but are separate in the treatment strategy needed. This review highlights the importance of a now widespread viral disease as a potential agent unmasking and exacerbating bipolar mood disorder, and it can hopefully help physicians in establishing a rapid diagnosis and treatment, and pave the road for future research on neuroinflammation triggered by SARS-CoV-2.
Introduction
On December 31st, 2019, several cases of atypical pneumonia arose in Wuhan, China, later found as being caused by a novel coronavirus called Severe Acute Respiratory Syndrome CoronaVirus-2 (SARS-CoV-2) (1). The World Health Organization classified the epidemic as a global pandemic on March 11th, 2020. As the pandemic was spreading, several important consequences on the mental health of the world population were emerging (2–4). Among these consequences, high rates of depression and anxiety among health professionals need to be highlighted (5), as well as anxiety, depression, and stress-related disorders in the general population (6, 7), psychological symptoms related to social isolation, especially in the elderly, poor, and subjects with difficulties in accessing or handling technology, such as telephone or Internet connections (7). Other symptoms that could arise in the general population are related to social isolation and quarantine (3, 8, 9), unemployment and financial difficulties (3, 9). Some of the psychological issues triggered by the pandemic are specific to infected patients and may include hypochondriac ideas, stigma-related concerns, amnesia, and traumatic memories of severe illness (4). Nevertheless, mental conditions have witnessed a change in paradigm, as the environment played a certain role in triggering some diseases, as previously stated, but the virus itself has the potential to influence the development of some neurological and psychiatric sequelae, as a direct effect of the coronavirus infection of the CNS and PNS, or an indirect effect of medical therapy or abnormal immune response, or a combination of these factors. Patients admitted to the hospital for severe SARS-CoV-2 infection can show different neurological symptoms, more commonly delirium. Different mental disorders may manifest in the subsequent months, including post-traumatic stress disorder, depression, anxiety, and fatigue. COVID-19 can be associated with delirium, agitation, and symptoms of depression, anxiety, and insomnia (4). The reason why this happens finds its roots in microbiological processes: the access of SARS-CoV-2 into human host cells is mediated by the angiotensin-converting enzyme II (ACE-2) receptor, mainly expressed in the lungs and gastrointestinal tract. This is also expressed in brain endothelial cells, which are a hypothetical route of entry into the CNS for coronaviruses (10, 11). Even if severe neurological and psychiatric direct consequences of SARS-CoV-2 appear to be rare, considering the prevalence of the pandemic, many people worldwide may have been affected (4, 12). Most of all, there is evidence of an overall increased vulnerability of patients with a primary diagnosis of bipolar disorder (BD) compared to the general population, despite some studies report a lower degree of distress in this population during the first month of the pandemic compared to a previous baseline (13, 14) Different COVID-19-related stressors can impact BD, mainly including social isolation, restrictive measures, lifestyle, biological circadian rhythms changes, and infection-related concerns (15). Furthermore, the access to mental health services among BD patients had become more difficult during some phases of the pandemic. Conversely, BD might indirectly worsen the risk of acquiring SARS-CoV-2 infection (15, 16). Neuroinvasion of the virus may represent a potential etiology for BD in absence of any other biological, psychological, and social precipitating factors. Nevertheless, some citokines appear to be involved in the development of psychiatric symptoms: it has been suggested that some may be specific for manic state (IL-2,4,6), and for depression (IL-6) (17, 18). Some authors have indeed suggested the particular need to develop standardized laboratory panels that include inflammatory markers (IL-6, TNF-α), cerebrospinal fluid (CSF) testing, and SARS-CoV-2 antibody assays to entirely understand the etiology of neuropsychiatric complications of SARS-CoV-2 infections and the pandemic itself (19). Neuroinflammation might be related to BD symptoms and is infrequently an etiological factor. An aberrant neuroglial function may be responsible for some neuronal miswiring that is consistent with psychotic symptoms frequently observed in BD (20). Manic episodes manifested during or after Covid-19 can arise both as an onset of BD and as a relapse. The main purpose of this article is to provide a review of the scientific literature focused on the clinical and biological correlates of cases of mania manifested in conjunction with or after SARS-CoV-2 infection.
Methods
On April the 18th, 2022, we conducted a first research on PubMed with the title/abstract specification, using the terms “(mania OR manic) AND (COVID OR SARS-CoV-2)” in the search bar. For eligibility, we included randomized controlled studies, case-control studies, and case reports focused on the issue. We excluded reviews, other types of articles and other studies that did not focus on the main topic, such as BD following another medical condition. The system provided 51 articles, of which we excluded 22 for low relevance. Hence, we assessed 29 articles for eligibility, excluding 12 articles for not respecting the inclusion criteria (4 reviews, 4 unrelated to the topic, and 4 focused on other diagnoses). We finally included 17 articles in the qualitative analysis (see PRISMA flow diagram in Figure 1).
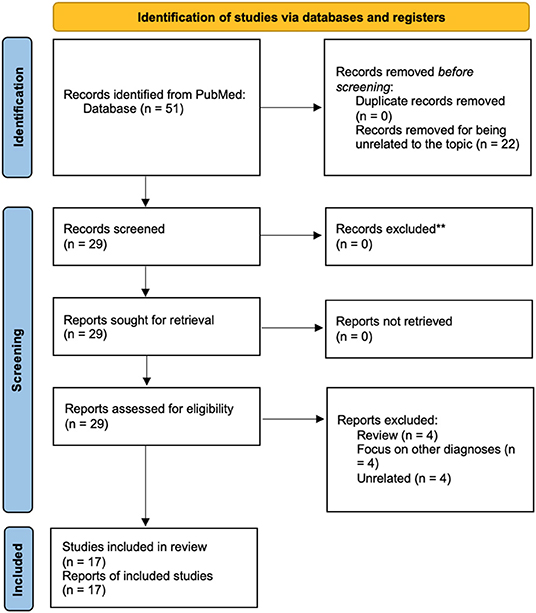
Figure 1. PRISMA 2020 flow diagram of the systematic review. For more information visit: http://www.prisma-statement.org/.
Results
The main results are summarized as follows in Table 1 below.
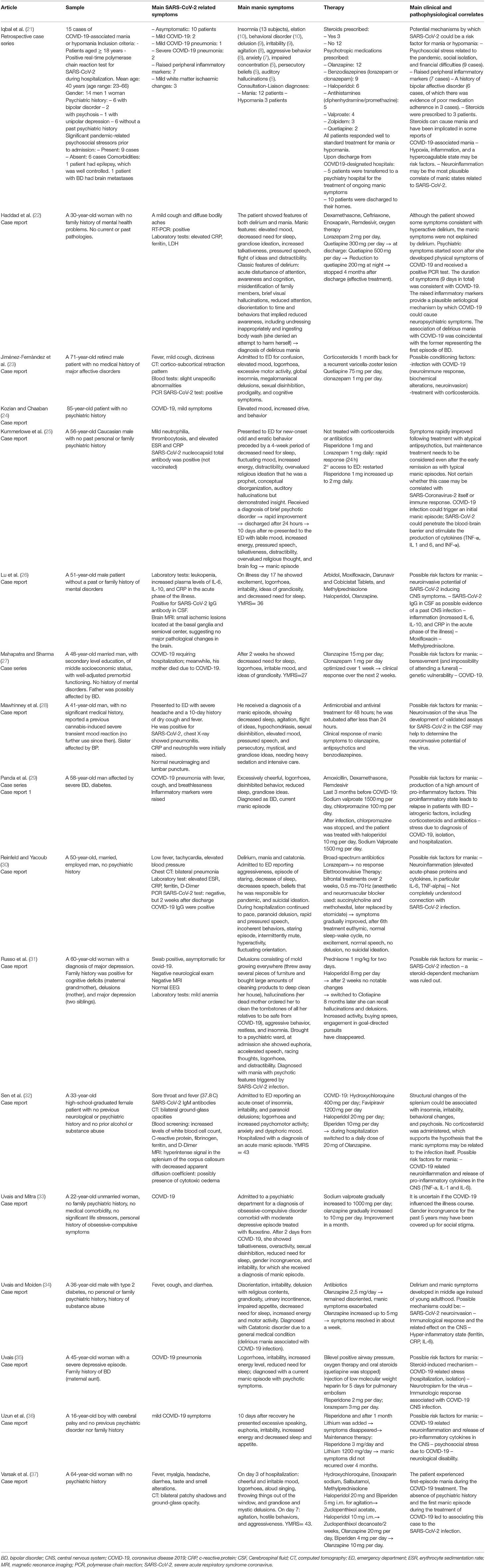
Table 1. Studies of manic episodes comorbid with ymrsSARS-CoV-2.
All studies are observational, being case-reports/case-series. Only traditional medical treatments were employed for the diseases. All studies regarded mania manifestations in different scenarios, and patients from cases analyzed shared a diagnosis of mania plus SARS-CoV-2 infection. Seven patients had a preexisting diagnosis of BD (21, 29); two patients had a preexisting diagnosis of major depressive disorder/unipolar depression (21, 31) 1 patient had a preexisting diagnosis of OCD (33), 2 of psychosis (21). Some cases, despite having a negative psychiatric history, had a positive psychiatric family history: 3 for BD (27, 28, 35) 1 for cognitive deficits, major depressive disorder and delirium (31). Since the aim of the review was to identify episodes of mania in the context of Covid-19, single patient outcome (resolution of the disease, remission, etc.) were not taken into consideration. Different and common clinical aspects were included in the main table in the symptoms column. Not all articles mentioned lab results of the case presented. Whenever mentioned, the mostly involved inflammatory markers were fibrinogen, ferritin, LDH, d-dimer, PCR, ESR, IL-6, IL-10.
Discussion
There is increasing evidence in literature regarding patients infected with SARS-CoV-2 which developed manic symptoms, possibly correlating with the infection itself, due to a cascade triggered by SARS-CoV-2 neuroinvasion, increased neuroinflammatory and inflammatory response in general, hypoxia, iatrogenic factors including antibiotics and steroidal therapy. Results of our research raise questions regarding the possibility that SARS-CoV-2 infection can be a trigger for a manic/hypomanic episode. On the basis that COVID-19 is still under many investigations regarding all consequences of the disease, the study can be enlightening in helping clinicians to suspect a psychiatric correlate of COVID-19 when specific symptoms of mania arise.
Iqbal et al. (21) have highlighted how mania can both be caused by psychosocial stress in susceptible individuals, and by an inflammatory mechanism as well, as has been hypothesized by Park et al. (25) as well: COVID-19 infection could trigger an initial manic episode, SARS-CoV-2 could penetrate blood–brain barriers and stimulate the production of cytokines (TNF-α, IL 1 and 6, and INF-α). Nonetheless, DSM-5 (38) and ICD-10 (39) permit a diagnosis of manic episode even in the background of a medical disorder or substance use, and this could be the case with COVID-19, but knowing how widespread the virus has become, this could influence the incidence of manic episodes across all countries.
The main mania symptoms experienced in the cases analyzed include classical presentations of mania: insomnia (22, 26) abnormal behavior (23, 24, 27), delusions (30, 31), irritability (34, 36), agitation (35), aggressive behavior (33, 37), anxiety (37), impaired concentration (21), persecutory beliefs (30), auditory hallucinations (21, 25), grandiose ideas (21, 28, 29). These findings support the hypothesis that the psychiatric condition experienced is no other than a manic episode, therefore not representing a separate diagnostic entity. The fact that remission of the mood swing occurred after appropriate medical treatment (mostly thanks to Atypical and Typical Anti-psychotics) further supports this statement.
The elevated peripheral inflammatory markers support neuroinflammation as a possible mechanism for COVID-19 causing the patients' neuropsychiatric symptoms (22, 26, 29). Furthermore, the included studies showed that the severity of COVID-19 did not correlate with manic symptoms, suggesting hidden neuroinflammatory mechanisms are strongly present. A discrepancy between pro-inflammatory and anti-inflammatory cytokines has been observed in bipolar patients, the former being more elevated and the latter being less expressed, in particular during mania. (40) Inflammation may act as a triggering factor by disrupting the blood brain barrier mostly, allowing SARS-CoV-2 entrance in the CNS (41), although the neurotropism of SARS-CoV-2 is still under investigation (42). SARS-CoV-2 apparently enters human cells through ACE-2, which is mostly expressed in the respiratory and gastrointestinal system, although being present in the endothelial system as well, also in the brain (10, 11). Invasion of the Central Nervous and of the Peripheral Nervous System as well (43) may explain a potential psychiatric clinical presentation of COVID-19. More specifically, in animal models there is evidence of the expression of ACE-2 in the amygdala, i.e., a site in which the spike proteins of the virus may bind (44). Neuronal and endothelial cells are potential targets for SARS-CoV-2 infection, which may cause their dysregulation after contact with the Spike viral protein (45). Viral invasion of the CNS may occur through several routes, including transsynaptic transfer across infected neurons, entry via the olfactory nerve, vascular endothelium infection, and leukocyte migration across the blood-brain barrier (46). Furthermore, SARS-CoV-2 can replicate in in-vitro neuronal cells, although confirmatory in vivo studies are required (47).
Worth of mention is that behavioral and mood disorders following infectious disorders have been observed previously as far as other coronaviruses are concerned (48). Studies have shown that individuals affected by BD may show an increased inflammatory status (49), therefore neuroinvasion may act as a trigger for the disease in those with a certain predisposition, culminating with the well-known manifestations of mania. Knowing the role played by the inflammatory cascade in the development of BD (50, 51), the hypothesis that COVID-19 may be a co-protagonist in unmasking a latent BD, as has happened in some cases analyzed (27, 28, 31, 35, 36) is gaining importance, yet needing further investigation.
Regarding the hypothesis that the pandemic social consequences themselves can be triggering factors for a previously unknown BD [as happened in some case reports analyzed: Uzun et al. (36), Varsak et al. (37), Meltem et al. (32)] or an exacerbating factor for those who had already been diagnosed with BD (52, 53), this appears to be relevant, as previous studies have already shown that social disasters can exacerbate BD mania symptoms but no other psychiatric disorders (54). Lockdown measures adopted to embank the pandemic influenced some of those factors which are crucial in mood maintenance in BD, such as sleep and social interactions, therefore possibly causing exacerbation of the mood disorder (55). In fact, studies have shown how the current pandemic has led to more depressive episodes in individuals affected by BD (56) compared to controls and patients affected by unipolar depression (57).
Limits
Our investigation was based on a low sample population and evidence mainly comes from single case reports and case series. Hence, further investigation is needed as a direct correlation between mania and SARS-CoV-2 neuroinvasion cannot be stated with certainty, although having some clue.
Conclusions
Manic episodes occurring in the context of COVID-19 are becoming more and more frequent. Knowing that biopsychological factors and environmental factors all concur in the development and/or exacerbation of BD, already well known to be of multifactorial etiology, raises alarm because of the high incidence of SARS-CoV-2 infections throughout the world. Awareness should be raised in physicians witnessing symptoms of mania in patients affected by COVID-19, even if asymptomatic from the organic point of view, and even if the patient has no prior psychiatric history. Results have shown that COVID-19 may trigger a pre-existing bipolar disorder or unmask an unknown BD, due to social and psychological influences and through biological pathways both. Further research is needed to understand the precise mechanisms of neurotropism of SARS-CoV-2 and, hopefully, prevent it at least in those patients who already received a diagnosis of BD. These, in particular, need a certain clinical focus, as they are more prone to re-exacerbation of the disease due to the stress which followed the pandemic, social isolation, difficulties in receiving appropriate medical attention and follow-up, therapy changes due to Covid-19 disease, increased inflammatory response and SARS-CoV-2 neuroinvasion of the CNS.
Author Contributions
AD, RT, and MNM: conceptualization. AD and LR: data curation. AD, LR, MNM, and PG: investigation. AD: methodology. AD, PG, and RT: supervision. AD, MNM, and LR: roles/writing—original draft. AD and MNM: writing—review and editing. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. 2019 Novel Coronavirus (2019nCoV): Strategic Preparedness and Response Plan. (2020). Available online at: https://www.who.int/docs/default-source/coronaviruse/srp-04022020.pdf?sfvrsn=7ff55ec0_4&download=true (cited April 16, 2022).
2. World Health Organization. Mental Health and Psychosocial Considerations During the COVID-19 Outbreak. (2020). Available online at: https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf (cited April 16, 2020).
3. Girardi P, Bonanni L, Kotzalidis GD, Fiaschè F, Del Casale A. Evolution of International Psychiatry. Psychiatry Int. (2020) 1:27–30. doi: 10.3390/psychiatryint1010004
4. Rogers JP, Chesney E, Oliver D, Pollak TA, McGuire P, Fusar-Poli P, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. The lancet Psychiatry. (2020) 7:611–27. doi: 10.1016/S2215-0366(20)30203-0
5. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw open. (2020) 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
6. Asmundson GJG, Taylor S. Coronaphobia: Fear and the 2019-nCoV outbreak. J Anxiety Disord. (2020) 70:102196. doi: 10.1016/j.janxdis.2020.102196
7. Xiong J, Lipsitz O, Nasri F, Lui LMW, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. (2020) 277:55–64. doi: 10.1016/j.jad.2020.08.001
8. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet (London, England). (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
9. Chaves C, Castellanos T, Abrams M, Vazquez C. The impact of economic recessions on depression and individual and social well-being: the case of Spain (2006-2013). Soc Psychiatry Psychiatr Epidemiol. (2018) 53:977–86. doi: 10.1007/s00127-018-1558-2
10. Hamming I, Timens W, Bulthuis MLC, Lely AT, Navis GJ, van Goor H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol. (2004) 203:631–7. doi: 10.1002/path.1570
11. Baig AM, Khaleeq A, Ali U, Syeda H. Evidence of the COVID-19 virus targeting the CNS: tissue distribution, host-virus interaction, and proposed neurotropic mechanisms. ACS Chem Neurosci. (2020) 11:995–8. doi: 10.1021/acschemneuro.0c00122
12. Pleasure SJ, Green AJ, Josephson SA. The spectrum of neurologic disease in the severe acute respiratory syndrome coronavirus 2 pandemic infection: neurologists move to the frontlines. JAMA Neurol. (2020) 77:679–80. doi: 10.1001/jamaneurol.2020.1065
13. Orhan M, Korten N, Paans N, de Walle B, Kupka R, van Oppen P, et al. Psychiatric symptoms during the COVID-19 outbreak in older adults with bipolar disorder. Int J Geriatr Psychiatry. (2021) 36:892–900. doi: 10.1002/gps.5489
14. Pinkham AE, Ackerman RA, Depp CA, Harvey PD, Moore RC. A Longitudinal Investigation of the Effects of the COVID-19 Pandemic on the Mental Health of Individuals with Pre-existing Severe Mental Illnesses. Psychiatry Res. (2020) 294:113493. doi: 10.1016/j.psychres.2020.113493
15. Fornaro M, De Prisco M, Billeci M, Ermini E, Young AH, Lafer B, et al. Implications of the COVID-19 pandemic for people with bipolar disorders: a scoping review. J Affect Disord. (2021) 295:740–51. doi: 10.1016/j.jad.2021.08.091
16. Wang Q, Xu R, Volkow ND. Increased risk of COVID-19 infection and mortality in people with mental disorders: analysis from electronic health records in the United States. World Psychiatry. (2021) 20:124–30. doi: 10.1002/wps.20806
17. Najjar S, Pearlman DM, Alper K, Najjar A, Devinsky O. Neuroinflammation and psychiatric illness. J Neuroinflamm. (2013) 10:816. doi: 10.1186/1742-2094-10-43
18. Lorkiewicz P, Waszkiewicz N. Biomarkers of Post-COVID Depression. J Clin Med. (2021) 10:4142. doi: 10.3390/jcm10184142
19. Łoś K, Kulikowska J, Waszkiewicz N. The Impact of the COVID-19 Virus Pandemic on the Incidence of First Psychotic Spectrum Disorders. Int J Environ Res Public Health. (2022) 19:3781. doi: 10.3390/ijerph19073781
20. Kotzalidis G, Ambrosi E, Simonetti A, Cuomo I, Del Casale A, Caloro M, et al. Neuroinflammation in bipolar disorders. Neuroimmunol Neuroinflamm. (2015) 2:252. doi: 10.4103/2347-8659.167309
21. Iqbal Y, Alabdulla M, Latoo J, Kumar R, Albrahim S, Wadoo O, et al. Mania and hypomania associated with COVID-19: a series of 15 cases seen by the consultation-liaison psychiatry service in Qatar. Qatar Med J. (2021) 2021:65. doi: 10.5339/qmj.2021.65
22. Haddad PM, Alabdulla M, Latoo J, Iqbal Y. Delirious mania in a patient with COVID-19 pneumonia. BMJ Case Rep. (2021) 14:e243816. doi: 10.1136/bcr-2021-243816
23. Jiménez-Fernández S, Solis MO, Martínez-Reyes I, Alvarado-Dafonte A, Soldado-Rodríguez L, Rodríguez-Natal MI. Secondary Mania in an Elderly Patient during SARS-CoV-2 Infection with Complete Remission) A 1-Year Follow-Up. Psychiatr Danub. (2021) 33:418–20. doi: 10.24869/psyd.2021.418
24. Kozian R, Chaaban A., (Mania after COVID-19 Infection). Psychiatr Prax. (2022) 49:51–3. doi: 10.1055/a-1642-7701
25. Park JH, Kummerlowe M, Gardea Resendez M, Nuñez NA, Almorsy A, Frye MA. First manic episode following COVID-19 infection. Bipolar Disord. (2021) 23:847–9. doi: 10.1111/bdi.13123
26. Lu S, Wei N, Jiang J, Wu L, Sheng J, Zhou J, et al. First report of manic-like symptoms in a COVID-19 patient with no previous history of a psychiatric disorder. J Affect Disord. (2020) 277:337–40. doi: 10.1016/j.jad.2020.08.031
27. Mahapatra A, Sharma P. Case series associated with COVID-19 pandemic in causing psychiatric morbidity. Gen psychiatry. (2021) 34:e100343. doi: 10.1136/gpsych-2020-100343
28. Mawhinney JA, Wilcock C, Haboubi H, Roshanzamir S. Neurotropism of SARS-CoV-2: COVID-19 presenting with an acute manic episode. BMJ Case Rep. (2020) 13:e236123. doi: 10.1136/bcr-2020-236123
29. Panda TK, Nebhinani N, Suthar N, Choudhary S, Singhai K. Relapse in bipolar disorder in hospitalized patients with COVID-19: a case series and key recommendations. Indian J Psychiatry. 63:610–2. doi: 10.4103/indianjpsychiatry.indianjpsychiatry_1433_20
30. Reinfeld S, Yacoub A. A Case of Delirious Mania Induced by COVID-19 Treated With Electroconvulsive Therapy. J ECT. (2021) 37:e38–9. doi: 10.1097/YCT.0000000000000789
31. Russo M, Consoli S, De Rosa MA, Calisi D, Dono F, Carrarini C, et al. A case of Sars-Cov-2-related mania with prominent psychosis. Psychiatry Res. (2021) 306:114266. doi: 10.1016/j.psychres.2021.114266
32. Sen M, Yesilkaya UH, Balcioglu YH. SARS-CoV-2-associated first episode of acute mania with psychotic features. J Clin Neurosci. (2021) 87:29–31. doi: 10.1016/j.jocn.2021.02.012
33. Uvais NA, Mitra S. Gender Incongruence Unmasked by Manic Switch During COVID-19 Infection. Prim care companion CNS Disord. (2022) 24:21cr03129. doi: 10.4088/PCC.21cr03129
34. Uvais NA, Moideen S. COVID-19 presenting with delirious mania: a case report. Bipolar Disord. (2022) doi: 10.1111/bdi.13180. [Epub ahead of print].
35. Uvais NA. Manic Switch in a Patient With Depression in the Setting of COVID-19 Treatment. Prim care companion CNS Disord. (2021) 23:21cr02984. doi: 10.4088/PCC.21cr02984
36. Uzun N, Kiliç AO, Akinci MA, Özgül-Katircioglu D, Erden S. Could COVID-19 be a trigger for manic attack in an adolescent? Neurol Sci. (2021) 42:3521–2. doi: 10.1007/s10072-021-05390-0
37. Varsak N, Topaloglu M, Özdemir E. First Manic Attack During COVID-19 Treatment: a Case Report. Clin Psychopharmacol Neurosci. (2021) 19:786–8. doi: 10.9758/cpn.2021.19.4.786
38. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th editio. American Psychiatric Association, editor. Arlington, VA (2013).
39. World Health Organization. The ICD-10 Classification of mental and Behavioural Disorders. 10th ed. Geneve, Switzerland (1993).
40. Sayana P, Colpo GD, Simões LR, Giridharan VV, Teixeira AL, Quevedo J, et al. A systematic review of evidence for the role of inflammatory biomarkers in bipolar patients. J Psychiatr Res. (2017) 92:160–82. doi: 10.1016/j.jpsychires.2017.03.018
41. Amruta N, Chastain WH, Paz M, Solch RJ, Murray-Brown IC, Befeler JB, et al. SARS-CoV-2 mediated neuroinflammation and the impact of COVID-19 in neurological disorders. Cytokine Growth Factor Rev. (2021) 58:1–15. doi: 10.1016/j.cytogfr.2021.02.002
42. Zhou Z, Kang H, Li S, Zhao X. Understanding the neurotropic characteristics of SARS-CoV-2: from neurological manifestations of COVID-19 to potential neurotropic mechanisms. J Neurol. (2020) 267:2179–84. doi: 10.1007/s00415-020-09929-7
43. Li Y-C, Bai W-Z, Hashikawa T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J Med Virol. (2020) 92:552–5. doi: 10.1002/jmv.25728
44. Wang L, de Kloet AD, Pati D, Hiller H, Smith JA, Pioquinto DJ, et al. Increasing brain angiotensin converting enzyme 2 activity decreases anxiety-like behavior in male mice by activating central Mas receptors. Neuropharmacology. (2016) 105:114–23. doi: 10.1016/j.neuropharm.2015.12.026
45. Benedetti F, Silvestri G, Mavian C, Weichseldorfer M, Munawwar A, Cash MN, et al. Comparison of SARS-CoV-2 receptors expression in primary endothelial cells and retinoic acid-differentiated human neuronal cells. Viruses. (2021) 13:2193. doi: 10.3390/v13112193
46. Zubair AS, McAlpine LS, Gardin T, Farhadian S, Kuruvilla DE, Spudich S. Neuropathogenesis and neurologic manifestations of the coronaviruses in the age of coronavirus disease 2019: a review. JAMA Neurol. (2020) 77:1018–27. doi: 10.1001/jamaneurol.2020.2065
47. Chu H, Chan JF-W, Yuen TT-T, Shuai H, Yuan S, Wang Y, et al. Comparative tropism, replication kinetics, and cell damage profiling of SARS-CoV-2 and SARS-CoV with implications for clinical manifestations, transmissibility, and laboratory studies of COVID-19: an observational study. Lancet Microbe. (2020) 1:e14–23. doi: 10.1016/S2666-5247(20)30004-5
48. Okusaga O, Yolken RH, Langenberg P, Lapidus M, Arling TA, Dickerson FB, et al. Association of seropositivity for influenza and coronaviruses with history of mood disorders and suicide attempts. J Affect Disord. (2011) 130:220–5. doi: 10.1016/j.jad.2010.09.029
49. Stich O, Andres TA, Gross CM, Gerber SI, Rauer S, Langosch JM. An observational study of inflammation in the central nervous system in patients with bipolar disorder. Bipolar Disord. (2015) 17:291–302. doi: 10.1111/bdi.12244
50. Benros ME, Waltoft BL, Nordentoft M, Ostergaard SD, Eaton WW, Krogh J, et al. Autoimmune diseases and severe infections as risk factors for mood disorders: a nationwide study. JAMA psychiatry. (2013) 70:812–20. doi: 10.1001/jamapsychiatry.2013.1111
51. Réus GZ, Fries GR, Stertz L, Badawy M, Passos IC, Barichello T, et al. The role of inflammation and microglial activation in the pathophysiology of psychiatric disorders. Neuroscience. (2015) 300:141–54. doi: 10.1016/j.neuroscience.2015.05.018
52. Koenders M, Mesbah R, Spijker A, Boere E, de Leeuw M, van Hemert B, et al. Effects of the COVID-19 pandemic in a preexisting longitudinal study of patients with recently diagnosed bipolar disorder: Indications for increases in manic symptoms. Brain Behav. (2021) 11:e2326. doi: 10.1002/brb3.2326
53. Uvais NA. Mania Precipitated by COVID-19 Pandemic-Related Stress. Prim Care Companion CNS Disord. (2020) 22:20l02641. doi: 10.4088/PCC.20l02641
54. Matsumoto J, Kunii Y, Wada A, Mashiko H, Yabe H, Niwa S. Mental disorders that exacerbated due to the Fukushima disaster, a complex radioactive contamination disaster. Psychiatry Clin Neurosci. (2014) 68:182–7. doi: 10.1111/pcn.12112
55. Takaesu Y. Circadian rhythm in bipolar disorder: a review of the literature. Psychiatry Clin Neurosci. (2018) 72:673–82. doi: 10.1111/pcn.12688
56. Karantonis JA, Rossell SL, Berk M, Van Rheenen TE. The mental health and lifestyle impacts of COVID-19 on bipolar disorder. J Affect Disord. (2021) 282:442–7. doi: 10.1016/j.jad.2020.12.186
Keywords: COVID-19, SARS-CoV-2, manic episode, bipolar disorder, neuroinflammation, neuroinvasion
Citation: Del Casale A, Modesti MN, Rapisarda L, Girardi P and Tambelli R (2022) Clinical Aspects of Manic Episodes After SARS-CoV-2 Contagion or COVID-19. Front. Psychiatry 13:926084. doi: 10.3389/fpsyt.2022.926084
Received: 22 April 2022; Accepted: 24 May 2022;
Published: 15 June 2022.
Edited by:
Domenico De Berardis, Mental Health Center (CSM) and Psychiatric Service of Diagnosis and Treatment (SPDC), ItalyReviewed by:
Napoleon Waszkiewicz, Medical University of Białystok, PolandMichele De Prisco, Federico II University Hospital, Italy
Copyright © 2022 Del Casale, Modesti, Rapisarda, Girardi and Tambelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Del Casale, YW50b25pby5kZWxjYXNhbGVAdW5pcm9tYTEuaXQ=