
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 13 July 2022
Sec. Anxiety and Stress Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.917299
 Tiia Ståhlberg1*
Tiia Ståhlberg1* Subina Upadhyaya1
Subina Upadhyaya1 Päivi Polo-Kantola2Prakash Khanal1
Päivi Polo-Kantola2Prakash Khanal1 Terhi Luntamo1,3Susanna Hinkka-Yli-Salomäki1
Terhi Luntamo1,3Susanna Hinkka-Yli-Salomäki1 Andre Sourander1,3
Andre Sourander1,3Objective: Mode of delivery and well-being markers for newborn infants have been associated with later psychiatric problems in children and adolescents. However, only few studies have examined the association between birth outcomes and anxiety disorders and the results have been contradictory.
Methods: This study was a Finnish population-based register study, which comprised 22,181 children and adolescents with anxiety disorders and 74,726 controls. Three national registers were used to collect the data on exposures, confounders and outcomes. Mode of delivery, the 1-min Apgar score, umbilical artery pH and neonatal monitoring were studied as exposure variables for anxiety disorders and for specific anxiety disorders. Conditional logistic regression was used to examine these associations.
Results: Unplanned and planned cesarean sections increased the odds for anxiety disorders in children and adolescents (adjusted OR 1.08, 95% CI 1.02–1.15 and aOR 1.12, 95% CI 1.05–1.19, respectively). After an additional adjustment for maternal diagnoses, unplanned cesarean sections remained statistically significant (aOR 1.11, 95% CI 1.04–1.18). For specific anxiety disorders, planned cesarean sections and the need for neonatal monitoring increased the odds for specific phobia (aOR 1.21, 95% CI 1.01–1.44 and aOR 1.28, 95% CI 1.07–1.52, respectively).
Conclusions: Birth by cesarean section increased the odds for later anxiety disorders in children and adolescents and unplanned cesarean sections showed an independent association. Further studies are needed to examine the mechanisms behind these associations.
Anxiety disorders are the most common psychiatric disorders (1) and among the earliest to manifest during life (2). They may be prolonged, lead to secondary diagnoses and cause notable impairment (1, 3). The etiological risk factors include some genetic and childhood environmental factors (4), but the role of perinatal factors is less clear, especially those during birth. Obstetrical adversities have been associated with various neurodevelopmental and psychiatric disorders (5–8). For example, perinatal hypoxemia, ischemia, infections, inflammation and stress may alter neurodevelopment and the hypothalamus-pituitary-adrenal axis (9, 10). These serve as potential mechanisms in the association between perinatal factors and later psychiatric problems (11). Maternal stress, due to perinatal adversities, may also have a negative impact on parenting styles and interaction, which could contribute to anxiety disorders in their offspring (12).
Large register-based studies are ideal for studying perinatal factors, because they can include whole birth cohorts, detailed confounders and also eliminate recall bias. Five register-based studies have examined birth outcomes and anxiety disorders (13–17). Four found that cesarean sections increased the risk for anxiety disorders (13–16). However, the associations with planned and unplanned cesarean sections disappeared in one study when they were adjusted for specific indications for cesarean section (13). The fifth did not find any associations (17). Low Apgar scores increased the risk for anxiety disorders in one study (17), but not in two other studies (15, 16) (Supplementary Table 1, available online). The definition of anxiety disorders varied, as four studies also included obsessive-compulsive disorder or stress-related disorders (13–15, 17). These are no longer included in the anxiety disorder category in the fifth version of Diagnostic and Statistical Manual of Mental disorders, as they stem from a slightly different etiology (18). It is notable that only two studies included childhood anxiety disorders (15, 17). In addition, planned and unplanned cesarean sections were only separated in one study (13). No register studies examined specific anxiety disorders separately. One small cohort study found that treatment in a neonatal intensive care unit (NICU) was associated with specific phobias (19) and two identified it to associate with separation anxiety disorders (19, 20).
The main aim of this study was to examine the associations between mode of delivery, birth outcomes and anxiety disorders using a large nationwide register-sample of children and adolescents. The exposure variables were mode of delivery, Apgar score, umbilical artery pH and neonatal monitoring and the confounders included various other perinatal events. The second aim was to examine the associations between mode of delivery, birth outcomes and specific anxiety disorders.
This register-based study was part of the Finnish Prenatal Study of Anxiety, an ongoing nested case-control study that uses data from three national registers (Figure 1). The use of this data was approved by the Finnish Data Protection Ombudsman.
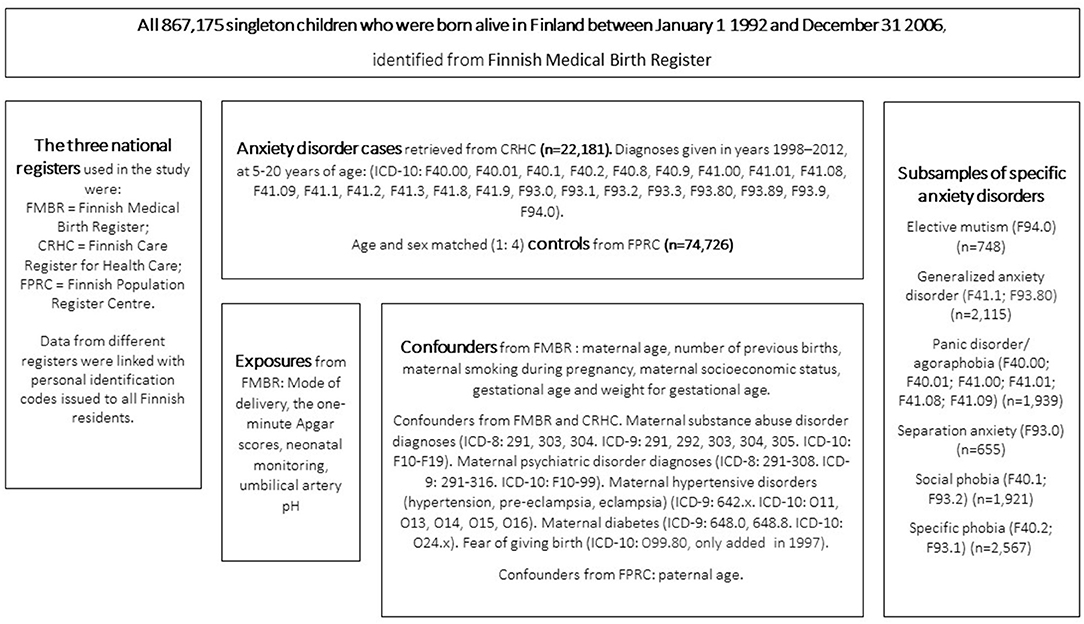
Figure 1. Study design.
The data from each register are described in Figure 1. The Finnish Care Register for Health Care was established in 1969 (21) and provides diagnostic information from specialized healthcare services. The Finnish Medical Birth Register, established in 1987, contains a great variety of prenatal and perinatal information about infants born alive or stillborn in Finland, with gestational ages of ≥22 weeks or birth weights of ≥500 grams (22). The Finnish Population Register Centre provides information on permanent Finnish residents. The data on these registers can be linked by the personal identification codes, which are unique codes issued to all Finnish residents. The linkage enabled to collect the data accurately for exposures and confounders for each case and control subject of this study.
The study sample was a birth cohort of all 867,175 singletons born alive in Finland in 1992–2006. We identified those diagnosed with an anxiety disorder between 1998 and 2012. The births were collected from the Finnish Medical Birth Register and the diagnoses from the Finnish Care Register for Health Care. Four sex and age matched controls without anxiety disorders were identified for each case. Controls were excluded if they received an anxiety disorder diagnosis during the 2012–2016 follow-up period or if they had missing data. Cases and controls with severe of profound intellectual disabilities, with the International Classification of Diseases, Tenth Revision (ICD-10) codes of F72 and F73 (23), were excluded. The final cohort comprised 22,181 cases with an anxiety disorder diagnosis and 74,726 controls.
The outcome was any anxiety disorder diagnosis in the Finnish Care Register for Health Care from 1998–2012. The Register has provided inpatient data from 1969, but only started recording outpatient data in 1998. Physicians used the ICD-10 anxiety disorder diagnoses (23). The incident diagnoses for the cases were included from the year the subjects turned 6 years. Following ICD-10 anxiety disorder diagnoses were included: F40, F41, F93, and F94.0. Additionally, the following specific anxiety disorders were examined separately: elective mutism (n = 748), generalized anxiety disorder (n = 2,115), panic disorder and/or agoraphobia (n = 1,939), separation anxiety disorder (n = 655), social phobia (n = 1,921), and specific phobia (n = 2,567). Detailed diagnostic information is presented in Figure 1.
Four exposure variables were selected from the Birth Register: mode of delivery, the 1-min Apgar score, umbilical artery pH and neonatal monitoring. There were four categories for delivery. Vaginal deliveries were split into spontaneous, unassisted vaginal cephalic deliveries and other types, which included induced delivery, vacuum or forceps and breech. Cesarean deliveries were split into planned and unplanned, which included urgent, emergency or other. The 1-min Apgar score was categorized as ≥7 or <7. Low Apgar score indicates disturbances in color, pulse, reflexes, muscle tone or respiratory function (24). The more feasible 5-min Apgar score was not available bit for 2.9% of the cases and therefore not utilizable. The umbilical artery pH was both a categorical (≥7.15 or <7.15) and continuous variable. Low pH values indicate asphyxia (25). Routinely measuring umbilical artery pH only began during the study period and was only available for 43.1% of the sample. Neonatal monitoring was defined as “no” referring to normal neonatal treatment or “yes” referring to enhanced monitoring, admitted by a pediatrician and carried out in a NICU or maternal postpartum ward.
The confounder variables were based on our previous studies (6, 7, 26) and literature (15–17) and obtained from the three national registers (Figure 1). These were tested for relevance before being added to the multivariate model. They were: maternal and paternal age, number of previous births, maternal and paternal psychiatric disorders (maternal substance use disorders excluded), maternal substance abuse, smoking during pregnancy and socioeconomic class (SES), gestational age and weight for gestational age. Three additional cofounders were chosen for the supplementary mode of delivery analysis, based on the literature and availability in the registers. These were: maternal hypertensive disorders (27, 28), diabetes (29, 30) and fear of giving birth (31, 32).
The missing data for the confounders was relatively small. Maternal SES was missing for 4.8% of the subjects and handled as a missing category. Smoking was missing for 2.2% and paternal age for 1.2% (Supplementary Table 2). There was no collinearity between maternal SES and smoking. The ICD-10-diagnosis O99.80, fear of giving birth was only established in 1997 (26, 32) and therefore not available for the oldest subjects.
The odds ratios (OR) and the 95% confidence intervals (95% CI) were obtained by fitting conditional logistic regression models for matched sets. The chi-square test was used to examine the association between each potential confounder and each exposure in the controls. We also used conditional logistic regression to test the associations between possible confounders and diagnosed anxiety disorders in the case-control model. Confounders were included in the final conditional logistic regression model if both of these analyses yielded significant associations (p < 0.05) with at least one exposure. We included all exposures with significant associations in the unadjusted model. An additional conditional logistic regression model was created for mode of delivery, with additional confounders that indicate the need for a cesarean section. These models were used also to analyze specific anxiety disorders. Statistical significance was p < 0.05. SAS version 9.4 was used for the statistical analyses (SAS Institute, Inc., Cary, NC, USA).
Table 1 describes the frequencies for the 22,181 cases (56.4% female) and 74,726 controls by each exposure and confounder. The mean age for anxiety disorder diagnoses was 12.7 ± 3.7 years (range 5–20 years).
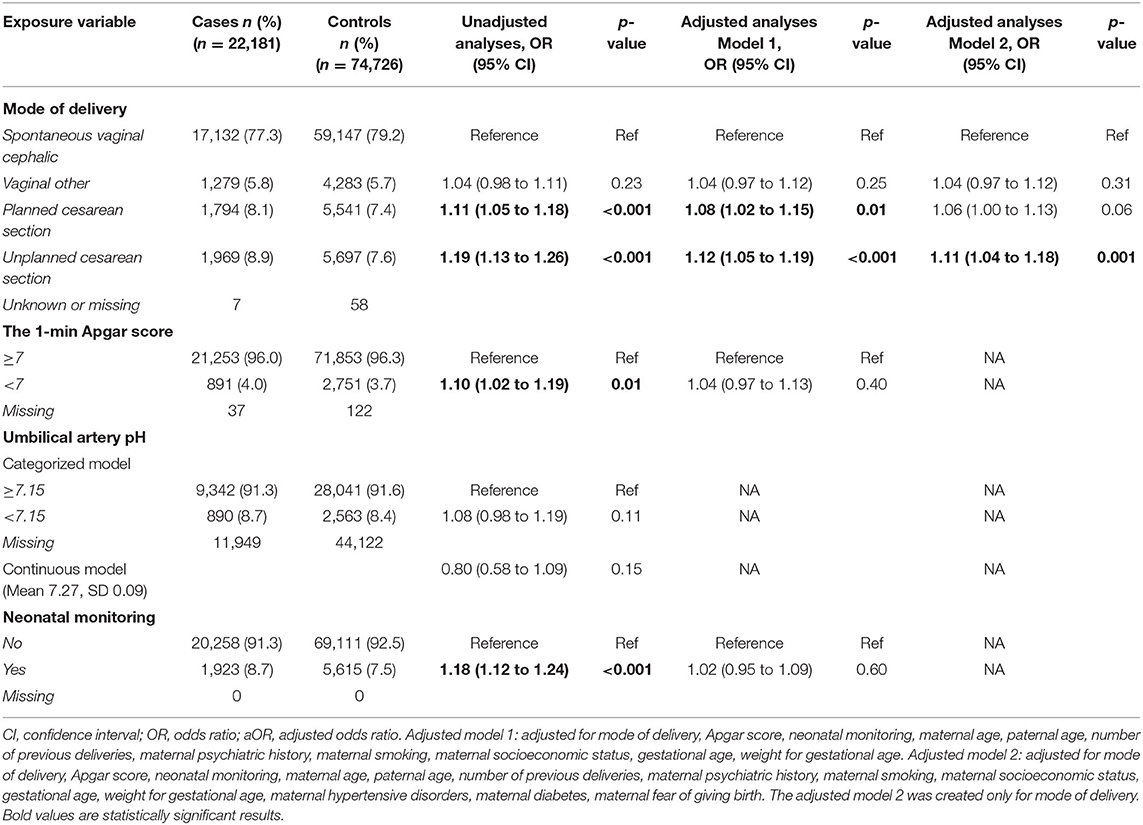
Table 1. Associations between exposures and anxiety disorders in the unadjusted and adjusted analyses.
Table 1 and Figure 2 show the unadjusted and adjusted data. All exposures, but umbilical artery pH, were associated with increased odds for anxiety disorders and therefore included in the adjusted model. Umbilical artery pH was excluded because it was unavailable for 56.9% of the sample and showed no associations in the categorized or continuous unadjusted models. Offspring born by planned and unplanned cesarean sections were more likely to have anxiety disorders, with adjusted ORs (aORs) of 1.08 (95% CI 1.02–1.15) and 1.12 (95% CI 1.05–1.19), respectively. No associations were observed for any vaginal birth categories, Apgar score and neonatal monitoring.
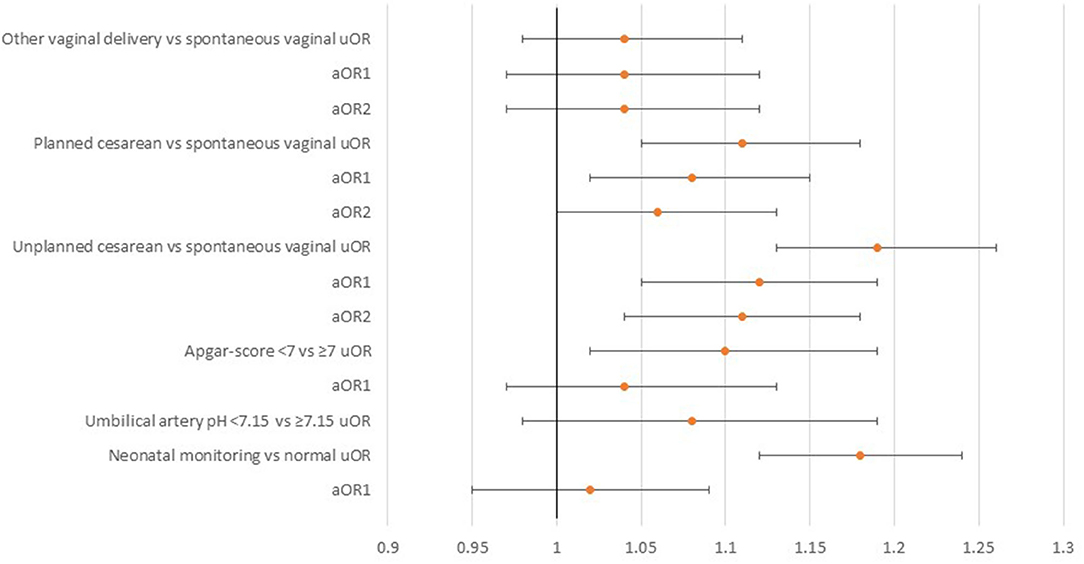
Figure 2. The associations between mode of delivery, birth outcomes, and anxiety disorders.
Table 2A shows the frequencies of each exposure in the specific anxiety disorder groups and Table 2B shows the associations between the exposures and specific anxiety disorders in the unadjusted and adjusted models. Several associations emerged in the unadjusted analyses. Birth by planned cesarean sections were associated with increased odds for generalized anxiety disorder, social phobia and specific phobia. Birth by unplanned cesarean sections were associated with increased odds for generalized anxiety disorder, separation anxiety disorder, social phobia and specific phobia. Low Apgar scores were associated with increased odds for specific phobia and neonatal monitoring was associated with increased odds for elective mutism, separation anxiety disorder and specific phobia. No associations were found for umbilical artery pH. In the adjusted analyses, birth by planned cesarean section and neonatal monitoring were only associated with increased odds for specific phobias, aOR 1.24 (95% CI 1.04–1.48), and aOR 1.28 (95% CI 1.07–1.52), respectively.
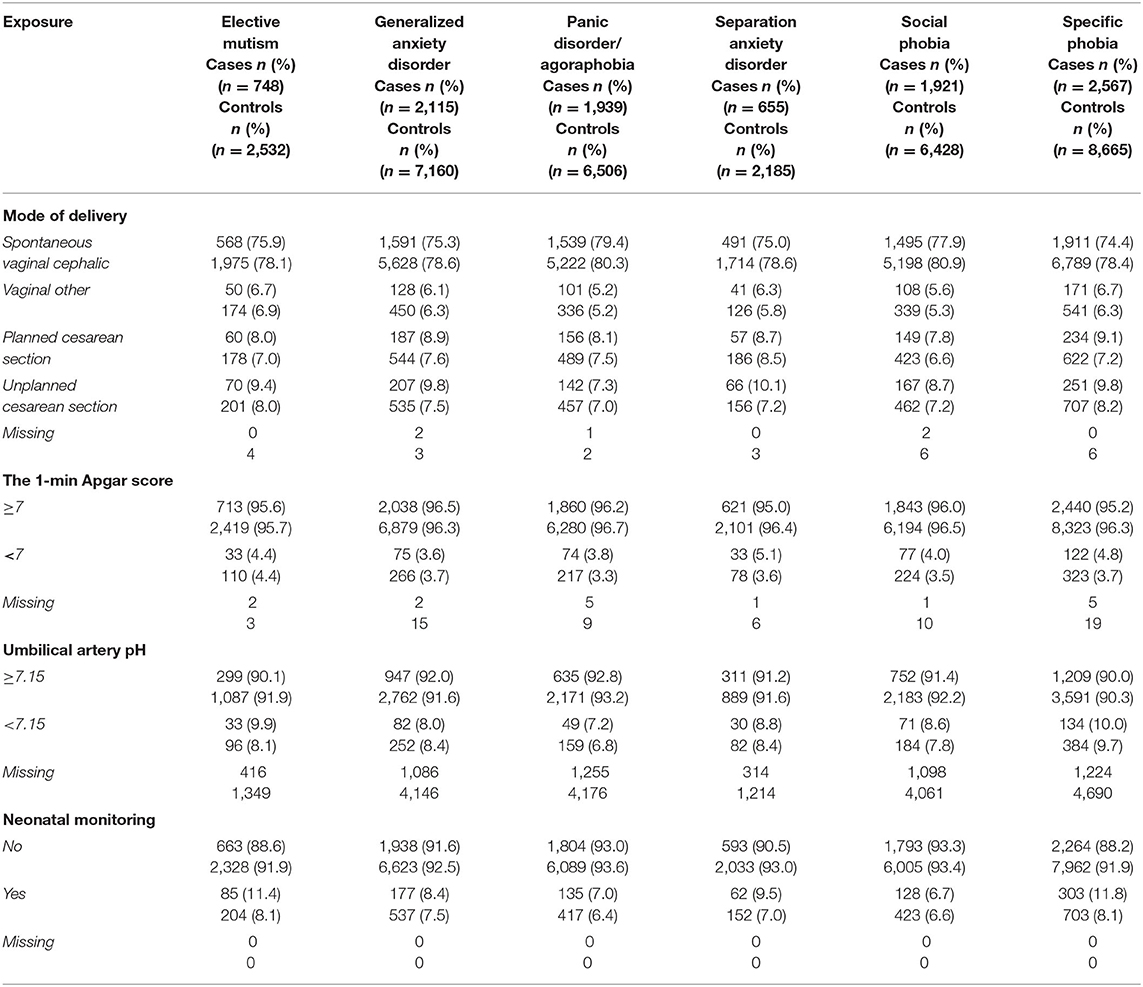
Table 2A. Frequencies of the exposure variables in the cases with specific anxiety disorders and the controls.
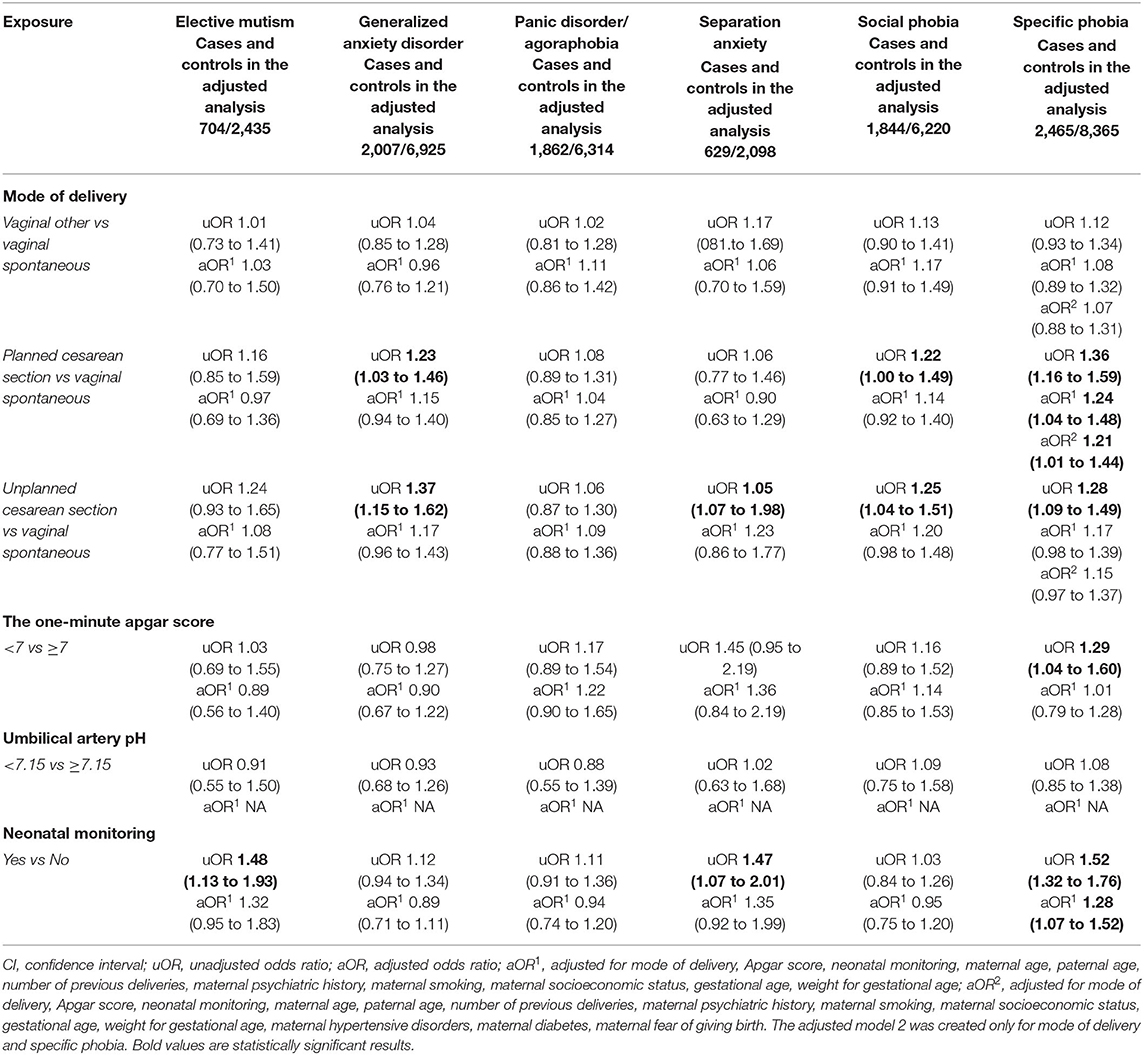
Table 2B. ORs (95% CIs) for the associations between the exposures and specific anxiety disorders in the unadjusted and adjusted analyses.
An additional conditional logistic regression model was created for delivery mode, with further adjustments (Tables 1, 2B). Birth by unplanned cesarean section was associated with increased odds for anxiety disorders, aOR 1.11 (95% CI 1.04–1.18) and planned cesarean section with increased odds for specific phobia, aOR 1.21 (95% CI 1.01–1.44). The association between birth by planned cesarean section and anxiety disorders became insignificant in the adjusted analyses, but showed a tendency for statistical significance, aOR 1.06 (95% CI 1.00–1.13).
This was the largest study to examine whether mode of delivery and birth outcomes were associated with anxiety disorders in childhood and adolescence and the first study to use national register data to identify associations with specific anxiety disorders. Children born by cesarean section were more likely to be diagnosed with child and adolescent anxiety disorders and specific phobias were more common if cesarean section was planned and neonatal monitoring was required after delivery.
Birth by planned and unplanned cesarean section showed increased odds for later anxiety disorders in the adjusted model. However, when maternal diagnoses of hypertensive disorders, diabetes and fear of giving birth were included, the association between birth by unplanned cesarean section and anxiety disorders remained, but birth by planned cesarean section only showed a tendency. The continuous increase in cesarean sections highlight the importance of these findings (33). Previous register-based studies that reported associations between cesarean sections and anxiety disorders later in life did not consider planned and unplanned cesarean sections separately and include comprehensive cofounders, such as indications for cesarean sections (14–16). A Swedish register-based study showed no such associations after full adjustment, unlike our study (13). These differences in the findings may be due to the definitions of anxiety disorders that were used. For example, Zhang et al. (13) included stress-related disorders, but not childhood onset disorders. In contrast, our study concentrated more precisely on child and adolescent anxiety disorders. Furthermore, Zhang et al. (13) included numerous perinatal confounders for cesarean sections (Supplementary Table 1) and the adjustment for maternal somatic problems, amniotic fluid and placental disorders, pelvic disproportion, malpresentation, dystocia, failed induction and fetal distress made their associations insignificant. We only included such confounders that were previously shown to be associated with the studied exposures and anxiety disorders (5–7, 15–17, 26–31). Although we did not include all the possible perinatal adversities, we did include indicators for fetal distress by studying Apgar scores and umbilical artery pH.
Several factors could explain the associations with cesarean sections. These include immunological mechanisms that influence neuronal development, prenatal or perinatal complications and maternal emotional factors. In animal models gut microbiome has related to altered neurodevelopment and emotional behavior (34). Similar mechanisms could contribute to anxiety disorders in humans. Immunological changes due to the disrupted transfer of microbiota from mother to child are likely to occur in cesarean sections (35). The microbiome can also be altered by antibiotics (36), which are typically administered during cesarean sections. Both planned and unplanned cesarean sections can follow prenatal or perinatal complications, such as pre-eclampsia, diabetes, fetal distress or infections (37) and these prenatal factors could contribute to the development of anxiety disorders (13, 16, 28, 30). Mothers who undergo cesarean sections may experience emotional distress and perceived loss of control and this can have impact their attachment to their child and parental behavior (38).
When we analyzed specific anxiety disorders, planned cesarean sections were associated with increased odds of specific phobias, but unplanned cesarean section was not. Studies have reported that women with psychiatric disorders are more likely to ask for cesarean sections (39). Maternal request for cesarean section can be derived from various fearful or anxious concepts (31). Phobic disorders run in families, with genetics playing a notable role (40). Our study was controlled for maternal psychiatric disorders diagnosed by specialized services and fear of giving birth. However, mothers with undiagnosed anxiety and less severe phobias could have contributed to the findings. Although we adjusted for the most common perinatal conditions, some residual confounding factors may have existed. Residual confounding factors have been suggested as plausible explanations for the associations between birth by cesarean sections and neurodevelopmental disorders in offspring, as the associations were attenuated in sibling analyses (13, 41).
Low Apgar score was associated with increased odds ratios for any anxiety disorder and for specific phobia in the unadjusted analyses. However, no significant results emerged in the adjusted analyses. Previously, one study has examined the 1-min Apgar score and anxiety disorders with no association (15). For the 5-min Apgar score, a significant association for increased odds of child anxiety disorders was found in one study (17), but not in the other (16). Apgar score is an unspecific measurement of infant's color, heart rate, reflexes, muscle tone and respiration, and it is ideally used for describing newborn infant's well-being and resuscitation response (24). The measurement time, as well as the unspecific nature of the score, could contribute to the discrepancies in the findings. Low Apgar score does not seem to be independently associated with increased odds for anxiety disorders but the found associations are explained by other factors.
Children who needed neonatal monitoring were more likely to be diagnosed with specific phobias. A relatively small cohort study, found that NICU treatment was associated with specific phobia and separation anxiety in children, based on specific anxiety disorder diagnoses reported by the children and their parents (19). The association between neonatal monitoring and specific phobia could be explained by residual perinatal adversities, similar to those for cesarean sections, as discussed above. In addition, NICU treatment notably increases newborn stress (42). Some infants treated in NICU have severe conditions and hence require multiple, painful and frightening procedures even after they are discharged. These potentially traumatizing experiences could predispose these children to later specific phobia (43). Painful NICU procedures have been associated with alterations in early brain development (44) and with stress responses (45). Newborn stress may also be increased by parental separation, as fewer parental NICU visits have been associated with later behavioral problems in offspring (46). Parental NICU visits have only increased in recent decades (47). Furthermore, NICU treatment increases parental stress, which could have an impact on parent-child interactions (12) and attachment (7). Neonatal adversities may also lead to parents being more sensitive to their child's conditions and problems (48).
Certain limitations should be considered. The anxiety disorder diagnoses were from specialized healthcare and less severe anxiety disorders were not included. Umbilical artery pH was only available for less than half the sample, which limited its use, and may have contained incorrect recordings, such as venous samples reported as arterial values. The ICD-10 diagnostic code for fear of giving birth was only added in in 1997 (23, 32) and was not available for the oldest subjects. The 1-min Apgar score was well recorded. The 5-min score would have been preferable, but it was only available for 2.9% of the sample. The specific anxiety disorder groups were relatively small, as most diagnoses were non-specific anxiety disorders. The anxiety disorder diagnoses had not been validated, except for elective mutism (49). However, the psychiatric diagnoses in the Health Care register had been validated as accurate (7, 50). We were unable to address all the possible residual confounders, as the data in the registers was not comprehensive for all perinatal events. We did not have data on the later life events for cases and controls, such as childhood adversities, which could contribute to the development of anxiety disorders. Globally varying rates of cesarean sections and focusing on singleton pregnancies may influence the generalizability of the results.
Children and adolescents born by cesarean section were more likely to have anxiety disorders later in childhood and adolescence, especially if cesarean section was unplanned. However, we were unable to show whether these associations were affected by residual confounding factors, such as additional perinatal adversities or maternal stress and anxiety. The constantly increasing rate of cesarean sections underlines the importance of our results.
The datasets presented in this article are not readily available because the data are available on Finnish Social and Health Data Permit Authority (FINDATA) and were used under a license for this study. Data are available from the authors upon reasonable request and with permission of FINDATA. Requests to access the datasets should be directed to aW5mb0BmaW5kYXRhLmZp, dHRodWh0QHV0dS5maQ==.
TS drafted the initial manuscript and contributed to the study design, data analysis, data interpretation, and literature search. SU and PP-K contributed to the study design, data analysis, data interpretation, and reviewed and revised the manuscript. PK and TL contributed to the study design, data interpretation, and reviewed and revised the manuscript. SH-Y-S contributed to the study design, conducted the statistical analyses, and reviewed and revised the manuscript. AS conceptualized the study, contributed to the study design, data collection and data interpretation, organized the funding of the study, and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
AS received funding from the Academy of Finland Flagship Programme (decision number 320162), the Strategic Research Council at the Academy of Finland (decision number 303581), and the Academy of Finland Health from Cohorts and Biobanks Programme (decision number 308552). TS received funding from Finnish Brain Foundation. The funders played no role in any aspect of the study or manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank Emmi Heinonen and Joonas Laitinen from Research Centre for Child Psychiatry, the INVEST Flagship, University of Turku, for their support in managing the data.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.917299/full#supplementary-material
1. Yang X, Fang Y, Chen H, Zhang T, Yin X, Man J, et al. Global, regional and national burden of anxiety disorders from 1990 to 2019: results from the Global Burden of Disease Study 2019. Epidemiol Psychiatr Sci. (2021) 30:1–11. doi: 10.1017/S2045796021000275
2. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. (2005) 62:593–602. doi: 10.1001/archpsyc.62.6.593
3. Steinsbekk S, Ranum B, Wichstrøm L. Prevalence and course of anxiety disorders and symptoms from preschool to adolescence: a 6-wave community study. J Child Psychol Psychiatry Allied Discip. (2021) 63:527–34. doi: 10.1111/jcpp.13487
4. Beesdo-Baum K, Knappe S. Developmental epidemiology of anxiety disorders. Child Adolesc Psychiatr Clin N Am. (2012) 21:457–78. doi: 10.1016/j.chc.2012.05.001
5. Sucksdorff M, Lehtonen L, Chudal R, Suominen A, Gissler M, Sourander A. Lower Apgar scores and Caesarean sections are related to attention-deficit/hyperactivity disorder. Acta Paediatr Int J Paediatr. (2018) 107:1750–8. doi: 10.1111/apa.14349
6. Polo-Kantola P, Lampi KM, Hinkka-Yli-Salomäki S, Gissler M, Brown AS, Sourander A. Obstetric risk factors and autism spectrum disorders in Finland. J Pediatr. (2014) 164:358–65. doi: 10.1016/j.jpeds.2013.09.044
7. Upadhyaya S, Chudal R, Luntamo T, Hinkka-Yli-Salomäki S, Sucksdorff M, Lehtonen L, et al. Perinatal risk factors and reactive attachment disorder: a nationwide population-based study. Acta Paediatr Int J Paediatr. (2020) 109:1603–11. doi: 10.1111/apa.15156
8. Zhang T, Sidorchuk A, Sevilla-Cermeño L, Vilaplana-Pérez A, Chang Z, Larsson H, et al. Association of cesarean delivery with risk of neurodevelopmental and psychiatric disorders in the offspring: a systematic review and meta-analysis. JAMA Netw Open. (2019) 2:1–19. doi: 10.1001/jamanetworkopen.2019.10236
9. Rees S, Inder T. Fetal and neonatal origins of altered brain development. Early Hum Dev. (2005) 81:753–61. doi: 10.1016/j.earlhumdev.2005.07.004
10. Seckl JR. Prenatal glucocorticoids and long-term programming. Eur J Endocrinol Suppl. (2004) 151:49–62. doi: 10.1530/eje.0.151u049
11. Amgalan A, Andescavage N, Limperopoulos C. Prenatal origins of neuropsychiatric diseases. Acta Paediatr Int J Paediatr. (2021) 110:1741–9. doi: 10.1111/apa.15766
12. Grunberg VA, Geller PA, Bonacquisti A, Patterson CA. NICU infant health severity and family outcomes: a systematic review of assessments and findings in psychosocial research. J. Perinatol. (2019) 39:156–72. doi: 10.1038/s41372-018-0282-9
13. Zhang T, Brander G, Mantel A, Kuja-Halkola R, Stephansson O, Chang Z, et al. Assessment of cesarean delivery and neurodevelopmental and psychiatric disorders in the children of a population-based swedish birth cohort. JAMA Netw Open. (2021) 4:1–15. doi: 10.1001/jamanetworkopen.2021.0837
14. Chen X, Kong L, Piltonen TT, Gissler M, Lavebratt C. Association of polycystic ovary syndrome or anovulatory infertility with offspring psychiatric and mild neurodevelopmental disorders: a Finnish population-based cohort study. Hum Reprod. (2020) 35:2336–47. doi: 10.1093/humrep/deaa192
15. Guhn M, Emerson SD, Mahdaviani D, Gadermann AM. Associations of birth factors and socio-economic status with indicators of early emotional development and mental health in childhood: a population-based linkage study. Child Psychiatry Hum Dev. (2020) 51:80–93. doi: 10.1007/s10578-019-00912-6
16. Larsen JT, Bulik CM, Thornton LM, Koch SV, Petersen L. Prenatal and perinatal factors and risk of eating disorders. Psychol Med. (2021) 51:870–80. doi: 10.1017/S0033291719003945
17. Kingston D, Heaman M, Brownell M, Ekuma O. Predictors of childhood anxiety: a population-based cohort study. PLoS ONE. (2015) 10:1–13. doi: 10.1371/journal.pone.0129339
18. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Publishing (2013).
19. Chiorean A, Savoy C, Beattie K, El Helou S, Silmi M, Van Lieshout RJ. Childhood and adolescent mental health of NICU graduates: an observational study. Arch Dis Child. (2020) 105:684–9. doi: 10.1136/archdischild-2019-318284
20. Karabel M, Tan S, Tatli MM, Yilmaz AE, Tonbul A, Karadag A. Separation anxiety disorder increases among neonatal intensive care unit graduates. J Matern Neonatal Med. (2012) 25:783–8. doi: 10.3109/14767058.2011.592876
21. THL: Finnish Institute for Health and Welfare (2021). Available online at: https://www.thl.fi/en/web/thlfi-en/statistics-and-data/data-and-services/register-descriptions/care-register-for-healthcare (accessed November 09, 2021).
22. THL: Finnish Institute for Health and Welfare (2017). Available online at: https://www.thl.fi/en/web/thlfi-en/statistics-and-data/data-and-services/register-descriptions/newborns (accessed November 09, 2021).
23. World Health Organization. International Classification of Diseases, Tenth Revision (ICD-10). Geneva: World Health Organization (1992).
24. Watterberg KL, Aucott S, Benitz WE, Cummings JJ, Eichenwald EC, Goldsmith J, et al. The apgar score. Pediatrics. (2015) 136:819–22. doi: 10.1542/peds.2015-2651
25. Vandenbussche FP, Oepkes D, Keirse MJ. The merit of routine cord blood pH measurement at birth. J Perinat Med. (1999) 27:158–65. doi: 10.1515/JPM.1999.021
26. Khanal P, Ståhlberg T, Luntamo T, Gyllenberg D, Kronström K, Suominen A, et al. Time trends in treated incidence, sociodemographic risk factors and comorbidities: a Finnish nationwide study on anxiety disorders. BMC Psychiatry. (2022) 22:144. doi: 10.1186/s12888-022-03743-3
27. Agrawal A, Wenger NK. Hypertension during pregnancy. Card Probl Pregn. (2019) 1:339–348. doi: 10.1002/9781119409861.ch24
28. Dachew BA, Scott JG, Mamun A, Alati R. Hypertensive disorders of pregnancy and the risk of anxiety disorders in adolescence: findings from the Avon Longitudinal Study of Parents and Children. J Psychiatr Res. (2019) 110:159–65. doi: 10.1016/j.jpsychires.2019.01.001
29. Scavini M, Secchi A. Diabetes in pregnancy. Acta Diabetol. (2019) 56:719–21. doi: 10.1007/s00592-019-01364-z
30. Kong L, Chen X, Gissler M, Lavebratt C. Relationship of prenatal maternal obesity and diabetes to offspring neurodevelopmental and psychiatric disorders: a narrative review. Int J Obes. (2020) 44:1981–2000. doi: 10.1038/s41366-020-0609-4
31. Jenabi E, Khazaei S, Bashirian S, Aghababaei S, Matinnia N. Reasons for elective cesarean section on maternal request: a systematic review. J Matern Neonatal Med. (2020) 33:3867–72. doi: 10.1080/14767058.2019.1587407
32. Saisto T, Halmesmäki E. Fear of childbirth: a neglected dilemma. Acta Obstet Gynecol Scand. (2003) 82:201–8. doi: 10.1034/j.1600-0412.2003.00114.x
33. Betran AP, Ye J, Moller AB, Souza JP, Zhang J. Trends and projections of caesarean section rates: global and regional estimates. BMJ Global Health. (2021) 6:e005671. doi: 10.1136/bmjgh-2021-005671
34. Mayer EA, Tillisch K, Gupta A. Gut/brain axis and the microbiota. J Clin Invest. (2015) 125:926–938. doi: 10.1172/JCI76304
35. Wampach L, Heintz-Buschart A, Fritz JV, Ramiro-Garcia J, Habier J, Herold M, et al. Birth mode is associated with earliest strain-conferred gut microbiome functions and immunostimulatory potential. Nat Commun. (2018) 9:5091. doi: 10.1038/s41467-018-07631-x
36. Yassour M, Vatanen T, Siljander H, Hämäläinen AM, Härkönen T, Ryhänen SJ, et al. Natural history of the infant gut microbiome and impact of antibiotic treatments on strain-level diversity and stability. Sci Transl Med. (2016) 8:343ra81. doi: 10.1126/scitranslmed.aad0917
37. Mylonas I, Friese K. The indications for and risks of elective cesarean section. Dtsch Arztebl Int. (2015) 112:489–95. doi: 10.3238/arztebl.2015.0489
38. Lobel M, DeLuca RS. Psychosocial sequelae of cesarean delivery: review and analysis of their causes and implications. Soc Sci Med. (2007) 64:2272–84. doi: 10.1016/j.socscimed.2007.02.028
39. Sydsjö G, Möller L, Lilliecreutz C, Bladh M, Andolf E, Josefsson A. Psychiatric illness in women requesting caesarean section. BJOG An Int J Obstet Gynaecol. (2015) 122:351–8. doi: 10.1111/1471-0528.12714
40. Hettema JM, Neale MC, Kendler KS. A review and meta-analysis of the genetic epidemiology of anxiety disorders. Am J Psychiatry. (2001) 158:1568–78. doi: 10.1176/appi.ajp.158.10.1568
41. Curran EA, Khashan AS, Dalman C, Kenny LC, Cryan JF, Dinan TG, et al. Obstetric mode of delivery and attention-deficit/hyperactivity disorder: a sibling-matched study. Int J Epidemiol. (2016) 45:532–42. doi: 10.1093/ije/dyw001
42. D'Agata AL, Young EE, Cong X, Grasso DJ, McGrath JM, Forsythe PL. Infant medical trauma in the neonatal intensive care unit (IMTN). Adv Neonatal Care. (2016) 16:289–97. doi: 10.1097/ANC.0000000000000309
43. LeBeau RT, Glenn D, Liao B, Wittchen HU, Beesdo-Baum K, Ollendick T, et al. Specific phobia: a review of DSM-IV specific phobia and preliminary recommendations for DSM-V. Depress Anxiety. (2010) 27:148–67. doi: 10.1002/da.20655
44. Brummelte S, Grunau RE, Chau V, Poskitt KJ, Brant R, Vinall J, et al. Procedural pain and brain development in premature newborns. Ann Neurol. (2012) 71:385–96. doi: 10.1002/ana.22267
45. Provenzi L, Giusti L, Fumagalli M, Tasca H, Ciceri F, Menozzi G, et al. Pain-related stress in the neonatal intensive care unit and salivary cortisol reactivity to socio-emotional stress in 3-month-old very preterm infants. Psychoneuroendocrinology. (2016) 72:161–5. doi: 10.1016/j.psyneuen.2016.07.010
46. Latva R, Lehtonen L, Salmelin RK, Tamminen T. Visiting less than every day. Arch Pediatr Adolesc Med. (2004) 158:1153. doi: 10.1001/archpedi.158.12.1153
47. Latva R, Lehtonen L, Salmelin RK, Tamminen T. Visits by the family to the neonatal intensive care unit. Acta Paediatr Int J Paediatr. (2007) 96:215–20. doi: 10.1111/j.1651-2227.2007.00053.x
48. Tallandini MA, Morsan V, Gronchi G, Macagno F. Systematic and meta-analytic review: triggering agents of parental perception of child's vulnerability in instances of preterm birth. J Pediatr Psychol. (2014) 40:545–53. doi: 10.1093/jpepsy/jsv010
49. Koskela M, Chudal R, Luntamo T, Suominen A, Steinhausen HC, Sourander A. The impact of parental psychopathology and sociodemographic factors in selective mutism- A nationwide population-based study. BMC Psychiatry. (2020) 20:221. doi: 10.1186/s12888-020-02637-6
Keywords: cesarean section, perinatal care, epidemiology, anxiety disorders, child psychiatry, adolescent psychiatry, registries
Citation: Ståhlberg T, Upadhyaya S, Polo-Kantola P, Khanal P, Luntamo T, Hinkka-Yli-Salomäki S and Sourander A (2022) Associations Between Delivery Modes, Birth Outcomes and Offspring Anxiety Disorders in a Population-Based Birth Cohort of Children and Adolescents. Front. Psychiatry 13:917299. doi: 10.3389/fpsyt.2022.917299
Received: 11 April 2022; Accepted: 06 June 2022;
Published: 13 July 2022.
Edited by:
Idan Menashe, Ben-Gurion University of the Negev, IsraelReviewed by:
Michał Pomorski, Wroclaw Medical University, PolandCopyright © 2022 Ståhlberg, Upadhyaya, Polo-Kantola, Khanal, Luntamo, Hinkka-Yli-Salomäki and Sourander. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tiia Ståhlberg, dHRodWh0QHV0dS5maQ==; orcid.org/0000-0003-0536-3057
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.