
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 14 June 2022
Sec. Psychological Therapy and Psychosomatics
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.914358
This article is part of the Research Topic Community Series in Extreme Eating Behaviors, volume II View all 12 articles
 Felix S. Hussenoeder1*†
Felix S. Hussenoeder1*† Alexander Pabst1*†
Alexander Pabst1*† Ines Conrad1
Ines Conrad1 Margrit Löbner1
Margrit Löbner1 Christoph Engel2,3Samira Zeynalova2Nigar Reyes2
Christoph Engel2,3Samira Zeynalova2Nigar Reyes2 Heide Glaesmer4
Heide Glaesmer4 Andreas Hinz4
Andreas Hinz4 Veronica Witte5Matthias L. Schroeter5,6Kerstin Wirkner3Toralf Kirsten2,7Markus Löffler2Arno Villringer5
Veronica Witte5Matthias L. Schroeter5,6Kerstin Wirkner3Toralf Kirsten2,7Markus Löffler2Arno Villringer5 Steffi G. Riedel-Heller1
Steffi G. Riedel-Heller1Background: Anxiety is a widespread phenomenon, and it is connected to disordered eating and obesity. We want to analyze the connection between anxiety and food addiction (FA) over two points in time to better understand the directionality of the association. Since there are gender differences with regard to anxiety and eating, we are also interested in differences between men and women.
Methods: We used data from the population-based LIFE-Adult-Study (N = 1,474) at time 1 (baseline) and time 2 (first follow-up) to analyze the connections between anxiety (GAD-7) and FA (YFAS) using a multiple group latent cross-lagged panel model with female and male participants as groups. We controlled for age, marital status, socioeconomic status and social support.
Results: Anxiety (women: β = 0.50, p ≤ 0.001; men: β = 0.59, p ≤ 0.001) as well as FA (women: β = 0.37, p ≤ 0.001; men: β = 0.58, p ≤ 0.001) exhibited stability over time for both genders. We found a significant association between anxiety at time 1 and FA at time 2 for women (β = 0.25, p ≤ 0.001) but not for men (β = 0.04, p = 0.10), and significant associations between FA at time 1 and anxiety at time 2 for women (β = 0.23, p ≤ 0.001) as well as men (β = 0.21, p ≤ 0.001).
Conclusion: Food addiction longitudinally affects anxiety, independent of gender and other sociodemographic variables. In addition, anxiety affects subsequent FA as well, but only in women. Interventions that address FA could reduce anxiety in men and women, while interventions that mitigate anxiety could help prevent FA in women.
Anxiety and anxiety symptoms are a widespread phenomenon (1, 2). For example, studies report a lifetime prevalence of generalized anxiety disorder (GAD) of around 3.7% (3), and of sub-threshold GAD of around 12.4% (4).
Anxiety is associated with eating-related health outcomes, as research links it to disordered, emotional, uncontrolled, and binge eating behaviors (5–8). In addition, studies show associations with obesity (9, 10) as well as bulimia, binge eating disorder and night eating syndrome that all involve excessive forms of eating behavior and food consumption (8, 11, 12).
While cross-sectional studies suggest an empirical connection between anxiety and eating, the direction of the connection is not clear to date, due to the lack of longitudinal studies in the field. Do increased levels of anxiety contribute to problematic eating behaviors, e.g., as a way of coping, or do problematic forms of eating longitudinally increase anxiety, e.g., via disturbing physiological homeostasis? It may also be that both phenomena are mutually dependent on each other in a longitudinal perspective.
In our study, we want to add to the literature by applying a cross-lagged design with two time points in order to evaluate the direction of the effects of the associations between anxiety and food addiction (FA). We chose FA for our analysis since, compared to eating disorders and obesity, it is more common in the general population and more accessible in terms of prevention measures. A current review shows a clear empirical connection between FA and binge eating disorder, bulimia nervosa, and obesity (13). FA has been validated in multiple international studies (14–16), and it is associated with typical addiction phenomena, i.e., brain reward dysfunction, preoccupation, risky use, impaired control, tolerance/withdrawal, social impairment, chronicity, and relapse (17). FA has already been connected to anxiety in cross-sectional research (18–20).
Since the literature shows that women are more likely than men to exhibit anxiety (21, 22) and FA (23, 24) and that the connection between anxiety and disordered eating could be moderated by gender (25, 26), we will further analyze whether the cross-lagged effects between anxiety and FA differ by gender.
The Adult Study of the Leipzig Research Centre for Civilization Diseases (LIFE) is a population-based cohort study in the city of Leipzig, Germany. It is a collaboration of several clinical and epidemiological research teams, for which 10,000 participants between 18 and 80 years were recruited through age- and gender-stratified random selection by the local residents’ registry office. The only exclusion criterion was being pregnant. The majority of participants (84.9%) were above 40 years of age. The LIFE-Adult baseline examination was carried out between 2011 and 2014, when every participant provided written informed consent prior to participation. Participants underwent a set of assessments, including interviews, questionnaires, and medical examinations. Details on study design, methods and assessments can be found elsewhere (27). The follow up examination took place between 2017 and 2021 with a total of 5,665 individuals completing the postal questionnaires.
For our analyses we included those 1,934 participants that were asked for their eating behaviors and took part in the baseline assessment (time 1) as well as in the follow-up (time 2). We excluded participants who were living in retirement/nursing homes, with relatives or in some form of supported living because we assumed that this would affect their eating behaviors (N = 60). In addition, we excluded individuals with diabetes, and those that stated they were treated for a disease, when treatment or disease were likely to have an impact on eating behavior, like ulcer or cancer (N = 361). In addition, another 39 individuals had to be excluded due to missing information on covariates, resulting in a final analytical sample size of N = 1,474. There was no significant age difference between our sample and the other participants from the LIFE study at baseline, but our sample contained slightly less female participants (53.0% vs. 48.2%).
The LIFE-Adult-Study complies with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The study was approved by the ethics committee of the University of Leipzig.
In order to measure anxiety, we used the Generalized Anxiety Disorder Scale-7 (GAD-7), (28, 29) which contains seven items that can be answered on a scale from “0” (=never) to “3” (=almost every day). The items refer to typical anxiety symptoms, like worrying, nervousness, and irritability, and higher scores represent higher levels of anxiety.
We used the Yale Food Addiction Scale (YFAS); (30, 31) to assess FA. The scale contains 25 items with mixed response categories (dichotomous and Likert-type). The seven subscales of the YFAS represent the criteria for an eating addiction in line with the guidelines for substance dependence according to DSM-IV, like control over consumption and withdrawal. They were computed using the algorithm proposed in Gearhardt et al. (30). The eighth item (clinical significance) was excluded, so that the YFAS measurement resembles a symptom count without diagnosis at both times. Scores range from 0 to 7 with higher scores representing higher levels of FA.
Participants were asked for information on age, gender, marital status, and medical history in standardized interviews by trained study personnel. They also provided information on education, equivalent household income, and occupational status that was used to compute socioeconomic status (low, medium, and high); (32). We assessed social support via the 5-item ENRICHD Social Support Scale (33). We decided to include social support as a covariate based on our own theoretical considerations as well as on the literature (34).
Descriptive statistics of the analytical sample were estimated using Stata version 16 SE (Stata Corp., College Station, TX, United States). In particular, gender-stratified means with SDs and numbers of cases with percentages were reported for quantitative and qualitative measures, respectively.
The bidirectional relationships between FA and anxiety were examined using a latent autoregressive cross-lagged panel model with multiple groups, estimated in Mplus 8.6 (35). The model consists of three parts: the autoregressive paths a1 and a2 indicate the intraindividual stability of FA and anxiety over time (Figure 1). The two cross-lagged paths b1 and b2 represent the reciprocal effect of FA at time 1 on anxiety at time 2 and vice versa. Finally, the cross-sectional paths c1 and c2 model the covariance between FA and anxiety within each wave of assessment. The multiple-group option in Mplus allows estimating and comparing the depicted cross-lagged path model between men and women simultaneously.
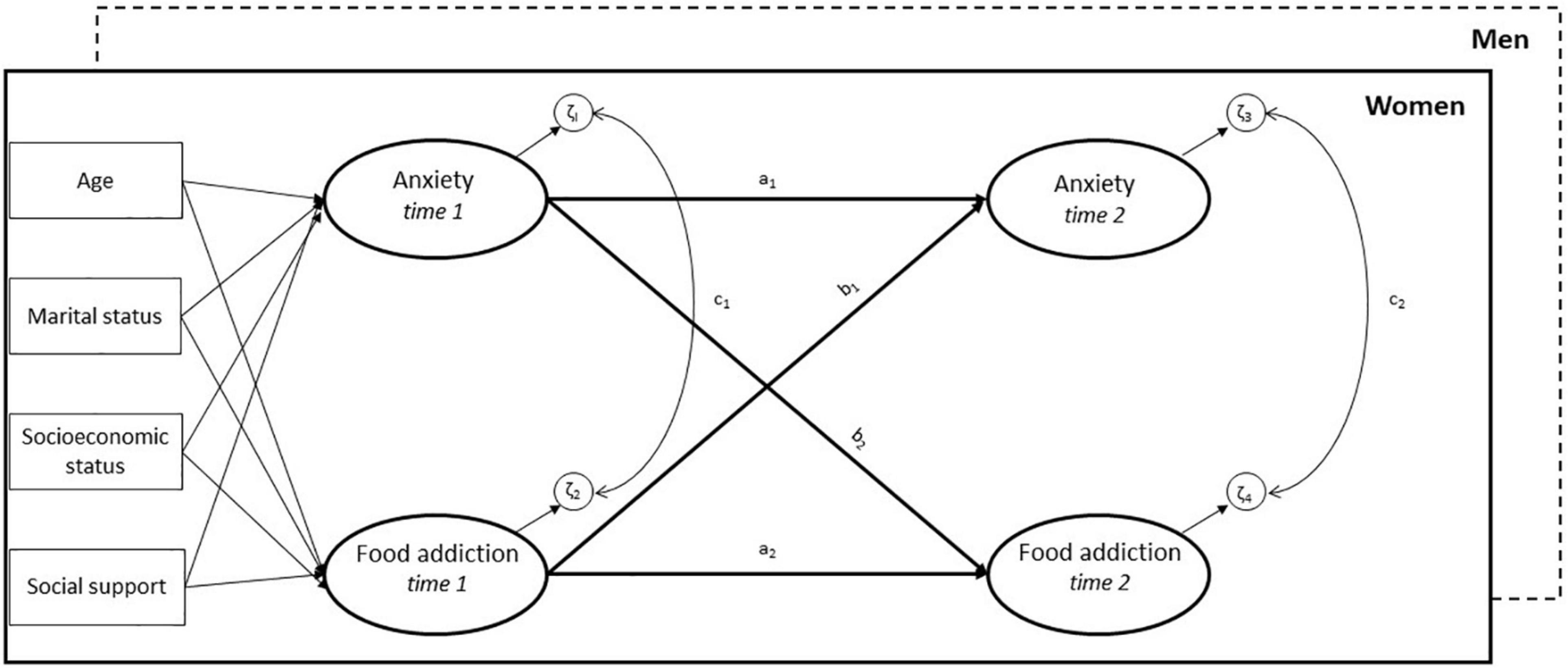
Figure 1. Multiple-group latent autoregressive cross-lagged panel model of the association between anxiety and food addiction. a1, a2: autoregressive paths, b1, b2: cross-lagged paths; c1, c2: cross-sectional paths. The measurement models for the latent variables with pairwise correlated errors over time are not shown. Model adjusted for age, marital status, socioeconomic status and social support at time 1.
Individual items of the GAD-7 and the subscale scores of the YFAS were entered as ordered categorical in Mplus and the constructs were modeled as latent variables. First, both constructs were evaluated separately using confirmatory factor analysis (CFA). With regard to the YFAS, the subscale “attempts” did not significantly predict the latent variable at time 1 (β = 0.197, p = 0.056) and time 2 (β = 0.010, p = 0.937) and was subsequently excluded from the analyses. Second, measurement invariance across time (i.e., time 1 and time 2) and across groups (i.e., men and women) was evaluated by introducing equality constraints on model parameters (e.g., factor loadings, intercepts, and variances) in a series of models with increasingly restrictive hypotheses. Parameters that proved not invariant, as indicated by model fit indices and chi-square difference tests in Mplus, were allowed to vary across time and groups. Error terms of the GAD-7 items and the YFAS subscales were set to be pairwise correlated over time, and factor means of the latent variables were allowed to vary by gender. Next, the partially invariant measurement models for FA and anxiety were combined to estimate the cross-lagged panel model shown in Figure 1. The model was finally adjusted for age, marital status, SES and social support at time 1. Results are presented as fully standardized (STDYX) regression coefficients with 95% confidence intervals for the paths a1 to c2 in the final cross-lagged model.
Since items of the GAD-7 and the computed subscale scores of the YFAS were ordered categorical, the WLSMV estimator in Mplus was used for the estimation of effects. Missingness on single indicators of the GAD-7 and the YFAS were handled using Full Information Maximum Likelihood (FIML) estimation, as implemented in Mplus. As indices of goodness-of-fit, the Tucker-Lewis fit index (TLI), the comparative fit index (CLI) and the root mean square error of approximation (RSMEA) were computed, with values below 0.06 for the RMSEA, and values above 0.95 for the TLI and CFI indicating a good model fit (36). All tests were two-tailed with p < 0.05 indicating statistical significance.
Our sample included 711 (48.2%) female and 763 (51.8%) male participants with an average age of 57.6 (female) and 58.4 (male) years. Table 1 gives an overview of the general characteristics of our sample.
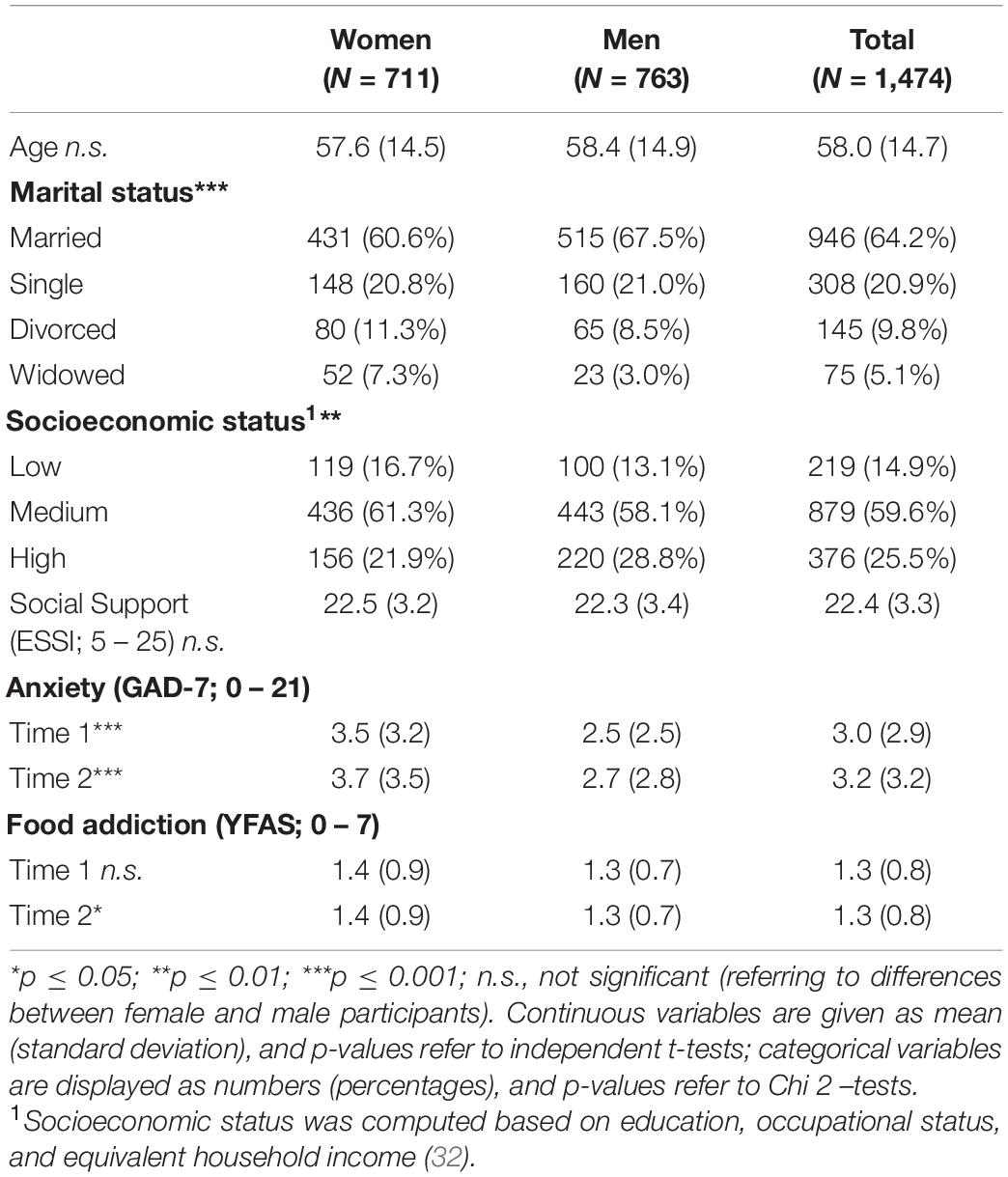
Table 1. General characteristics of the study population.
Table 2 depicts the correlations between key variables of our analysis, and shows that all of them are significantly correlated.
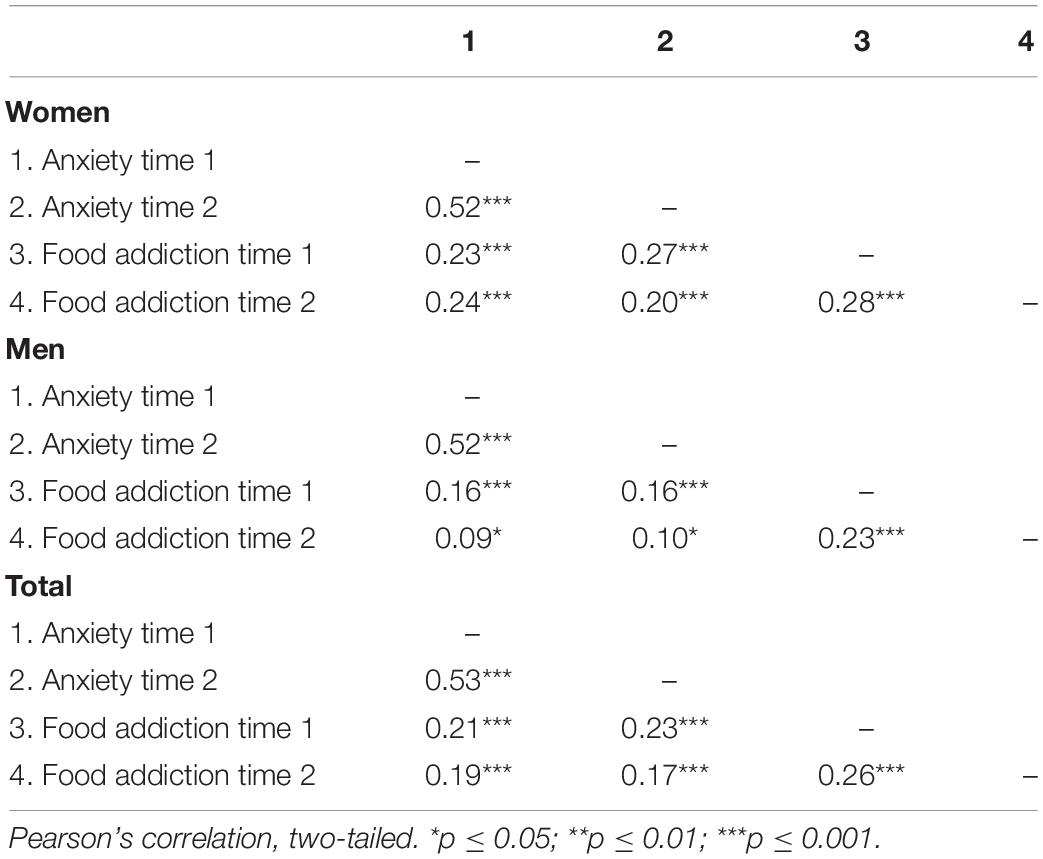
Table 2. Correlations of key variables for women and men.
After adjustment for covariates, the final multiple-group cross-lagged panel model with partial measurement invariance yielded an excellent fit of the data (χ2(988) = 1,372.07, p > 0.001; CFI = 0.971; TLI = 0.970; RMSEA = 0.023). This model with gender-specific paths for the autoregressive, cross-sectional and cross-lagged effects fitted the data statistically better than a model with each of the effects constrained across gender (χ2(4) = 17.33, p = 0.002). Standardized coefficients and standard errors of the significant paths obtained from the final model are shown for both genders in Figure 2.
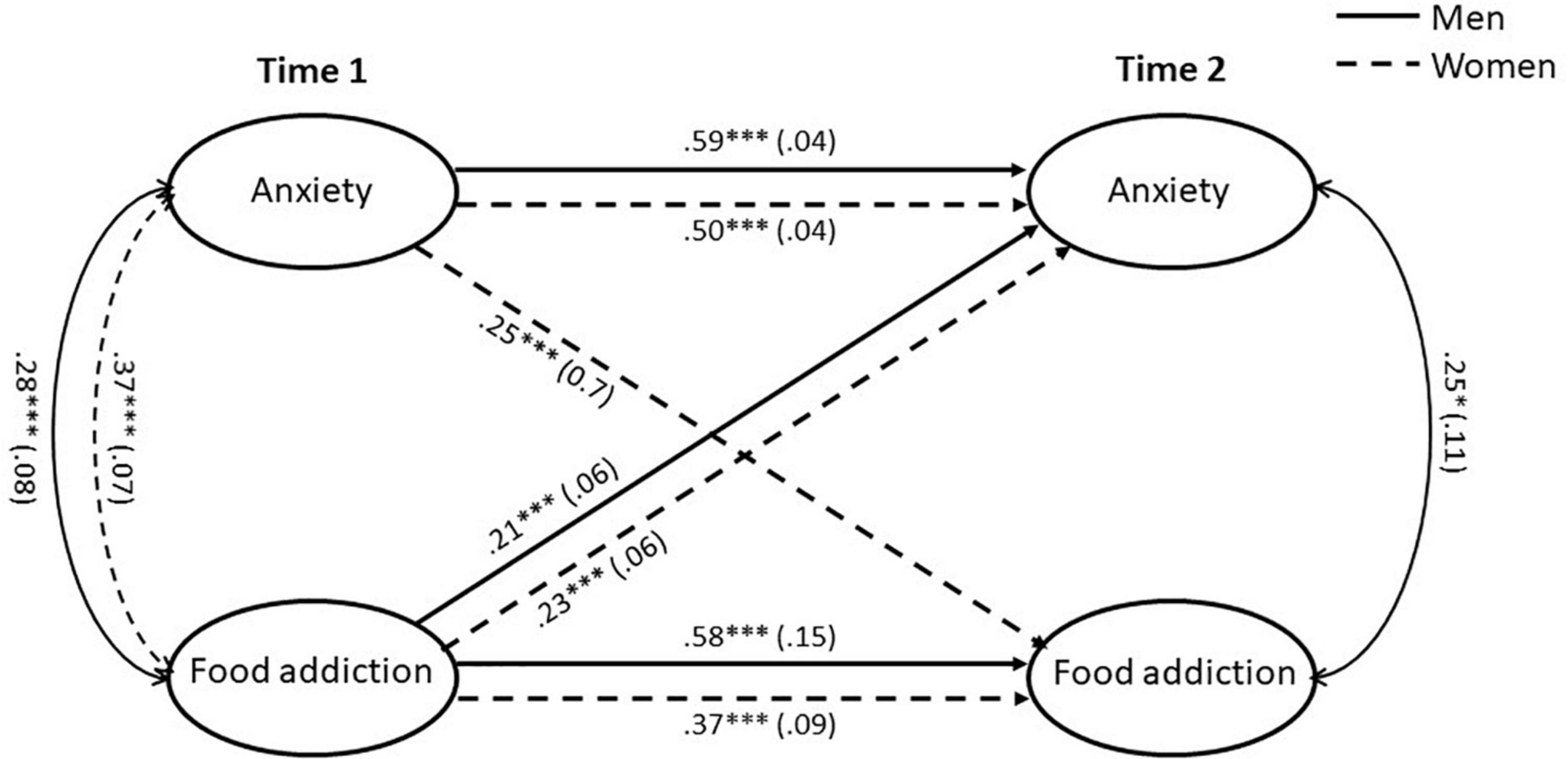
Figure 2. Multiple-group latent autoregressive cross-lagged panel model with standardized beta coefficients and standard errors in parentheses. The model only displays the significant paths for men and women. The effects of control variables (age, marital status, socioeconomic status, social support) on anxiety and food addiction at time 1 were included in the estimation but not shown for ease of presentation. Sample size: 1,474 (48.2% female). *p ≤ 0.05; ***p ≤ 0.001.
Autoregressive paths (a1, a2) represent the stability of a concept over time. Both autoregressive effects for anxiety (women: β = 0.50, p ≤ 0.001; men: β = 0.59, p ≤ 0.001) as well as for FA (women: β = 0.37, p ≤ 0.001; men: β = 0.58, p ≤ 0.001) were statistically significant for both genders.
Cross-sectional paths (c1, c2) represent correlations between concepts at either time 1 or time 2. Female participants showed a significant correlation between anxiety and FA at time 1 (r = 0.37, p ≤ 0.001) but no significant correlation at time 2 (r = −0.02, p = 0.78), while male participants exhibited significant correlations at time 1 (r = 0.28, p ≤ 0.001) and time 2 (r = 0.25, p ≤ 0.05).
Cross-lagged paths (b1, b2) represent prospective bidirectional associations between one concept and the other over the two points of time. We found an association between anxiety at time 1 and FA at time 2 for women (β = 0.25, p ≤ 0.001) but not for men (β = 0.04, p = 0.69). In addition, there were significant associations between FA at time 1 and anxiety at time 2 for women (β = 0.23, p ≤ 0.001) as well as men (β = 0.21, p ≤ 0.001).
Our study addressed the associations between anxiety and FA in a longitudinal design, showing the significant stability of both constructs over time. There was a significant effect of FA at time 1 on anxiety at time 2 for both genders. Vice versa, only women showed a significant effect of anxiety at time 1 on FA at time 2.
The stability of anxiety (37, 38) and FA (39, 40) over time that we have obtained from our data is also reflected in the literature. In addition, the higher levels of anxiety in women at both times of measurement resonate with other international studies (41, 42). With regard to FA, we found no gender difference at time 1 but a significantly yet only slightly higher score for women at time 2. These results are in line with the literature that suggest either no gender effects (43, 44) or higher values for women (24, 45).
We found a cross-sectional association between anxiety and FA for women as well as men at time 1 and for men at time 2, which matches with other studies that suggest associations between FA and a higher prevalence of anxiety disorders in obese patients seeking bariatric surgery (46) and between FA and anxiety in general (19). The results indicate that both concepts are interrelated, and the lack of a significant association for women at time 2 that is not reflected in the correlational analysis (Table 2) can be seen as a consequence of the inclusion of control variables.
We also found evidence for cross-lagged effects. There is a significant effect of anxiety at time 1 on FA at time 2 for women, indicating that anxiety has different implications depending on gender. This gender-specific effect could be explained by rumination, a cognitive process and maladaptive strategy for emotion regulation that involves repetitive thoughts about negative experiences and emotions. Rumination is empirically associated with both, anxiety and pathological forms of eating (47–49), and it has been connected to a variety of addictive behaviors, e.g., related to alcohol, work, or social media use (50–52). Furthermore, a current study suggests that targeting rumination could be important for reducing disinhibited eating patterns in women with normal body weight (53). Since women are more likely to ruminate than men (54), when men and women experience the same level of anxiety, women will be much more affected by rumination that then contributes to FA. This interpretation is in line with research that suggests that rumination mediated the connection between gender and food craving, binge eating, and eating pathology (55), that rumination can increase problematic alcohol and substance abuse, especially in women (56), and that women are more likely to exhibit emotional eating as a reaction to negative emotions (5, 57). Rumination has repeatedly been associated with exacerbating and maintaining psychopathology and physiological stress responses, prolonging negative emotional states, increasing negative emotional reactivity, interfering with problem solving, and acting as a transdiagnostic mental vulnerability (56). In that way, rumination that is associated with anxiety at time 1 could, in addition to maintaining anxiety over time as it is reflected in significant and substantial autocorrelations, set the stage for FA at time 2. On an applied level, our results indicate that interventions that mitigate anxiety could help prevent FA in women, who are more often affected by anxiety than men (58, 59). Meta-analyses show that measures based on cognitive behavioral therapy, delivered both online and offline (60, 61), are effective against anxiety, and a current study suggests that irrational beliefs could be a source of anxiety and a potential target for treatment in FA (62). By addressing anxiety, mental health professionals could not only mitigate FA in women, but they could also reduce the likelihood of a variety of negative health behaviors and outcomes that are related to FA, from unhealthy lifestyle habits (63) to eating disorders, mental illnesses, and obesity (19, 45, 64). Overweight and obesity are major risk factors for a variety of disorders, and they bear enormous costs for societies worldwide (65).
Our results further indicate a cross-lagged effect of FA at time 1 on anxiety at time 2 in both men and women. This could be a consequence of the fact that the overconsumption of food that is a central element of FA alters brain functioning and physiology, which then affects anxiety. Accordingly, there is a plethora of neurobiological studies that link the consumption of food that is high in calories, sugar, or fat to anxiety-like behaviors in rats and that emphasize the roles of certain brain circuits, neurobiological processes, and the immune system (66–68). In addition, research with human participants links disordered eating to subsequent increased anxiety and anxiety disorders (69, 70). Hence, interventions that address FA behaviors and food consumption could mitigate anxiety in men and women. Studies that address overeating and binge eating behaviors suggest that cognitive interventions that address internal food-related biases and response inhibition training, mindfulness-based interventions, and increasing physical activity could be promising avenues to address FA (71–73). A current study suggests that the treatment of FA could also benefit weight-related self-stigma and binge eating (74).
While this study has several advantages, e.g., the large dataset and a longitudinal design, there are also certain limitations. First, FA was assessed via self-report, therefore we cannot rule out that there is a certain bias. Second, while we included established control variables in our model, there could be other variables that affect both anxiety and FA, e.g., specific personality traits, and future research may benefit from including them.
Our results show that FA longitudinally affected anxiety in both men and women, and that anxiety affected subsequent FA only in women. Hence, interventions that address FA could reduce anxiety in both genders, while interventions that mitigate anxiety could help prevent FA in women.
The data analyzed in this study is subject to the following licenses/restrictions: The data that support the findings of this study are available from the corresponding author upon reasonable request. Requests to access these datasets should be directed to FH, RmVsaXguSHVzc2Vub2VkZXJAbWVkaXppbi51bmktbGVpcHppZy5kZQ==.
The LIFE-Adult-Study complies with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The study was approved by the Ethics Committee of the University of Leipzig. The patients/participants provided their written informed consent to participate in this study.
FH, AP, IC, and SR-H designed the study. FH and AP conducted the statistical analysis and literature searches. FH wrote the first draft of the manuscript. MGL, CE, SZ, NR, HG, AH, VW, MS, KW, TK, MKL, and AV contributed to the data and/or expertise. All authors contributed to and have approved the final manuscript.
LIFE was funded by means of the European Union, by the European Regional Development Fund (ERDF) and by funds of the Free State of Saxony within the framework of the excellence initiative (project numbers 713-241202, 14505/2470, and 14575/2470). MGL was funded by the @ktivPLUS study (German Federal Ministry of Education and Research, grant number 01GY2108). We acknowledge support from the German Research Foundation (DFG) and Universität Leipzig within the program of Open Access Publishing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the research teams and the participants of the LIFE-Adult-Study.
1. Duffy ME, Twenge JM, Joiner TE. Trends in mood and anxiety symptoms and suicide-related outcomes among U.S. undergraduates, 2007–2018: evidence from two national surveys. J Adolesc Health. (2019) 65:590–8. doi: 10.1016/j.jadohealth.2019.04.033
2. Remes O, Brayne C, van der Linde R, Lafortune L. A systematic review of reviews on the prevalence of anxiety disorders in adult populations. Brain Behav. (2016) 6:e00497. doi: 10.1002/brb3.497
3. Ruscio AM, Hallion LS, Lim CC, Aguilar-Gaxiola S, Al-Hamzawi A, Alonso J, et al. Cross-sectional comparison of the epidemiology of DSM-5 generalized anxiety disorder across the globe. JAMA Psychiatry. (2017) 74:465–75. doi: 10.1001/jamapsychiatry.2017.0056
4. Haller H, Cramer H, Lauche R, Gass F, Dobos GJ. The prevalence and burden of subthreshold generalized anxiety disorder: a systematic review. BMC Psychiatry. (2014) 14:128. doi: 10.1186/1471-244X-14-128
5. Hussenoeder FS, Conrad I, Engel C, Zachariae S, Zeynalova S, Glaesmer H, et al. Analyzing the link between anxiety and eating behavior as a potential pathway to eating-related health outcomes. Scie Rep. (2021) 11:14717. doi: 10.1038/s41598-021-94279-1
6. Lee KS, Vaillancourt TA. Four-year prospective study of bullying, anxiety, and disordered eating behavior across early adolescence. Child Psychiatry Hum Dev. (2019) 50:815–25. doi: 10.1007/s10578-019-00884-7
7. Janjetic MA, Rossi ML, Acquavía C, Denevi J, Marcolini C, Torresani ME. Association between anxiety level, eating behavior, and nutritional status in adult women. J Am Coll Nutr. (2020) 39:200–5. doi: 10.1080/07315724.2019.1633970
8. Rosenbaum DL, White KS. The relation of anxiety, depression, and stress to binge eating behavior. J Health Psychol. (2015) 20:887–98. doi: 10.1177/1359105315580212
9. Amiri S, Behnezhad S. Obesity and anxiety symptoms: a systematic review and meta-analysis. Neuropsychiatrie. (2019) 33:72–89. doi: 10.1007/s40211-019-0302-9
10. Sharafi SE, Garmaroudi G, Ghafouri M, Bafghi SA, Ghafouri M, Tabesh MR, et al. Prevalence of anxiety and depression in patients with overweight and obesity. Obes Med. (2020) 17:100169. doi: 10.1016/j.obmed.2019.100169
11. Pineda-García G, Ochoa-Ruiz E, Gómez-Peresmitré G, Platas-Acevedo S. Assessment of alcohol consumption and anxiety as predictors of risk of anorexia and bulimia in non-clinicals samples. Int J Environ Res Public Health. (2020) 17:6293.
12. Sevincer GM, Ince E, Taymur I, Konuk N. Night eating syndrome frequency in university students: association with impulsivity, depression, and anxiety. Bull Clin Psychopharmacol. (2016) 26:238–47. doi: 10.5455/bcp.20160322093750
13. Oliveira J, Colombarolli MS, Cordás TA. Prevalence and correlates of food addiction: systematic review of studies with the YFAS 2.0. Obes Res Clin Pract. (2021) 15:191–204. doi: 10.1016/j.orcp.2021.03.014
14. Chen G, Tang Z, Guo G, Liu X, Xiao S. The Chinese version of the Yale food addiction scale: an examination of its validation in a sample of female adolescents. Eat Behav. (2015) 18:97–102. doi: 10.1016/j.eatbeh.2015.05.002
15. Granero R, Jiménez-Murcia S, Gearhardt AN, Agüera Z, Aymamí N, Gómez-Peña M, et al. Validation of the Spanish version of the Yale food addiction scale 2.0 (YFAS 2.0) and clinical correlates in a sample of eating disorder, gambling disorder, and healthy control participants. Front Psychiatry. (2018) 9:208. doi: 10.3389/fpsyt.2018.00208
16. Meule A, Vögele C, Kübler A. deutsche übersetzung und validierung der yale food addiction scale-German translation and validation of the Yale food addiction scale. Diagnostica. (2012) 58:115–26.
17. Gordon EL, Ariel-Donges AH, Bauman V, Merlo LJ. What Is the evidence for “food addiction?” A systematic review. Nutrients. (2018) 10:477.
18. da Silva Júnior AE, de Lima Macena M, de Oliveira ADS, Praxedes DR, de Oliveira Maranhão Pureza IR, de Menezes Toledo Florêncio TM, et al. Prevalence of food addiction and its association with anxiety, depression, and adherence to social distancing measures in Brazilian university students during the COVID-19 pandemic: a nationwide study. Eat Weight Disord. (2022):1–9.
19. Burrows T, Kay-Lambkin F, Pursey K, Skinner J, Dayas C. Food addiction and associations with mental health symptoms: a systematic review with meta-analysis. J Hum Nutr Diet. (2018) 31:544–72. doi: 10.1111/jhn.12532
20. Mutlu HH, Sargın M. Food addiction prevalence and related factors among people with obesity: a hospital-based study. Ankara Med J. (2021) 21:22–34. doi: 10.5505/amj.2021.59862
21. Byrd-Bredbenner C, Eck K, Quick V. GAD-7, GAD-2, and GAD-mini: psychometric properties and norms of university students in the United States. Gen Hosp Psychiatry. (2021) 69:61–6. doi: 10.1016/j.genhosppsych.2021.01.002
22. Sun J, Liang K, Chi X, Chen S. Psychometric properties of the generalized anxiety disorder scale-7 item (GAD-7) in a large sample of Chinese adolescents. Healthcare (Basel). (2021) 9:1709.
23. Yu Z, Indelicato NA, Fuglestad P, Tan M, Bane L, Stice C. Sex differences in disordered eating and food addiction among college students. Appetite. (2018) 129:12–8. doi: 10.1016/j.appet.2018.06.028
24. Pursey KM, Stanwell P, Gearhardt AN, Collins CE, Burrows TL. The prevalence of food addiction as assessed by the Yale food addiction scale: a systematic review. Nutrients. (2014) 6:4552–90.
25. Turel T, Jameson M, Gitimu P, Rowlands Z, Mincher J, Pohle-Krauza R, et al. Disordered eating: influence of body image, sociocultural attitudes, appearance anxiety and depression – a focus on college males and a gender comparison. Cogent Psychol. (2018) 5:1483062. doi: 10.1080/23311908.2018.1483062
26. Zimmer-Gembeck MJ, Webb HJ, Kerin J, Waters AM, Farrell LJ. Risk factors and temporal patterns of disordered eating differ in adolescent boys and girls: testing gender-specific appearance anxiety models. Dev Psychopathol. (2021) 33:856–67. doi: 10.1017/S0954579420000188
27. Loeffler M, Engel C, Ahnert P, Alfermann D, Arelin K, Baber R, et al. The LIFE-Adult-Study: objectives and design of a population-based cohort study with 10,000 deeply phenotyped adults in Germany. BMC Public Health. (2015) 15:691. doi: 10.1186/s12889-015-1983-z
28. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7.
29. Hinz A, Klein AM, Brähler E, Glaesmer H, Luck T, Riedel-Heller SG, et al. Psychometric evaluation of the generalized anxiety disorder screener GAD-7, based on a large German general population sample. J Affect Disord. (2017) 210:338–44.
30. Gearhardt AN, Corbin WR, Brownell KD. Preliminary validation of the Yale food addiction scale. Appetite. (2009) 52:430–6. doi: 10.1016/j.appet.2008.12.003
31. Gearhardt AN, White MA, Masheb RM, Morgan PT, Crosby RD, Grilo CM. An examination of the food addiction construct in obese patients with binge eating disorder. Int J Eat Disord. (2012) 45:657–63. doi: 10.1002/eat.20957
32. Lampert T, Kroll L, Müters S, Stolzenberg H. Measurement of socioeconomic status in the German health interview and examination survey for adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. (2013) 56:631–6. doi: 10.1007/s00103-012-1663-4
33. Berkman LF, Blumenthal J, Burg M, Carney RM, Catellier D, Cowan MJ, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the enhancing recovery in coronary heart disease patients (ENRICHD) randomized trial. JAMA. (2003) 289:3106–16.
34. Conceição EM, Fernandes M, de Lourdes M, Pinto-Bastos A, Vaz AR, Ramalho S. Perceived social support before and after bariatric surgery: association with depression, problematic eating behaviors, and weight outcomes. Eat Weight Disord. (2020) 25:679–92. doi: 10.1007/s40519-019-00671-2
36. Hu L-T, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. (1999) 6:1–55.
37. Peter RS, Meyer ML, Mons U, Schöttker B, Keller F, Schmucker R, et al. Long-term trajectories of anxiety and depression in patients with stable coronary heart disease and risk of subsequent cardiovascular events. Depress Anxiety. (2020) 37:784–92. doi: 10.1002/da.23011
38. Ivanova E, Burns RJ, Deschênes SS, Knäuper B, Schmitz NA. Longitudinal investigation of anxiety and depressive symptomatology and exercise behaviour among adults with type 2 diabetes mellitus. Can J Diabetes. (2017) 41:73–81. doi: 10.1016/j.jcjd.2016.07.006
39. Pursey KM, Collins CE, Stanwell P, Burrows TL. The stability of ‘food addiction’ as assessed by the Yale food addiction scale in a non-clinical population over 18-months. Appetite. (2016) 96:533–8. doi: 10.1016/j.appet.2015.10.015
40. Meadows A, Higgs S. Internalized weight stigma and the progression of food addiction over time. Body Image. (2020) 34:67–71. doi: 10.1016/j.bodyim.2020.05.002
41. Luo Z, Li Y, Hou Y, Liu X, Jiang J, Wang Y, et al. Gender-specific prevalence and associated factors of major depressive disorder and generalized anxiety disorder in a Chinese rural population: the Henan rural cohort study. BMC Public Health. (2019) 19:1744. doi: 10.1186/s12889-019-8086-1
42. Tiirikainen K, Haravuori H, Ranta K, Kaltiala-Heino R, Marttunen M. Psychometric properties of the 7-item generalized anxiety disorder scale (GAD-7) in a large representative sample of Finnish adolescents. Psychiatry Res. (2019) 272:30–5. doi: 10.1016/j.psychres.2018.12.004
43. Hauck C, Weiß A, Schulte EM, Meule A, Ellrott T. Prevalence of ‘food addiction’ as measured with the Yale food addiction scale 2.0 in a representative German sample and its association with sex, age and weight categories. Obes Facts. (2017) 10:12–24. doi: 10.1159/000456013
44. Schulte EM, Gearhardt AN. Associations of food addiction in a sample recruited to be nationally representative of the United States. Eur. Eat. Disord Rev. (2018) 26:112–9. doi: 10.1002/erv.2575
45. Gearhardt AN, Corbin WR, Brownell KD. Development of the Yale food addiction scale version 2.0. Psychol Addict Behav. (2016) 30:113–21. doi: 10.1037/adb0000136
46. Benzerouk F, Gierski F, Ducluzeau P-H, Bourbao-Tournois C, Gaubil-Kaladjian I, Bertin É, et al. Food addiction, in obese patients seeking bariatric surgery, is associated with higher prevalence of current mood and anxiety disorders and past mood disorders. Psychiatry Res. (2018) 267:473–9. doi: 10.1016/j.psychres.2018.05.087
47. Olatunji BO, Naragon-Gainey K, Wolitzky-Taylor KB. Specificity of rumination in anxiety and depression: a multimodal meta-analysis. Clin Psychol Sci Pract. (2013) 20:225–57. doi: 10.1037/h0101719
48. Dar KA, Iqbal N. Worry and rumination in generalized anxiety disorder and obsessive compulsive disorder. J Psychol. (2015) 149:866–80. doi: 10.1080/00223980.2014.986430
49. Smith KE, Mason TB, Lavender JM. Rumination and eating disorder psychopathology: a meta-analysis. Clin Psychol Rev. (2018) 61:9–23. doi: 10.1016/j.cpr.2018.03.004
50. Caselli G, Gemelli A, Querci S, Lugli AM, Canfora F, Annovi C, et al. The effect of rumination on craving across the continuum of drinking behaviour. Addict Behav. (2013) 38:2879–83. doi: 10.1016/j.addbeh.2013.08.023
51. Kun B, Urbán R, Bõthe B, Griffiths MD, Demetrovics Z, Kökönyei G. Maladaptive rumination mediates the relationship between self-esteem, perfectionism, and work addiction: a largescale survey study. Int J Environ Res Public Health. (2020) 17:7332.
52. Wang P, Wang X, Wu Y, Xie X, Wang X, Zhao F, et al. Social networking sites addiction and adolescent depression: a moderated mediation model of rumination and self-esteem. Pers Individ Differ. (2018) 127:162–7. doi: 10.1016/j.paid.2018.02.008
53. Waliłko J, Bronowicka P, He J, Brytek-Matera A. Dieting and disinhibited eating patterns in adult women with normal body weight: does rumination matter? Nutrients. (2021) 13:2475.
54. Johnson DP, Whisman MA. Gender differences in rumination: a meta-analysis. Pers Individ Differ. (2013) 55:367–74. doi: 10.1016/j.paid.2013.03.019
55. Opwis M, Schmidt J, Martin A, Salewski C. Gender differences in eating behavior and eating pathology: the mediating role of rumination. Appetite. (2017) 110:103–7. doi: 10.1016/j.appet.2016.12.020
56. Watkins ER, Roberts H. Reflecting on rumination: consequences, causes, mechanisms and treatment of rumination. Behav Res Ther. (2020) 127:103573. doi: 10.1016/j.brat.2020.103573
57. Rosenqvist E, Kiviruusu O, Konttinen H. The associations of socioeconomic status and financial strain with restrained and emotional eating among 42-year-old women and men. Appetite. (2022) 169:105795. doi: 10.1016/j.appet.2021.105795
58. Guo X, Meng Z, Huang G, Fan J, Zhou W, Ling W, et al. Meta-analysis of the prevalence of anxiety disorders in mainland China from 2000 to 2015. Sci Rep. (2016) 6:28033. doi: 10.1038/srep28033
59. Grenier S, Payette M-C, Gunther B, Askari S, Desjardins FF, Raymond B, et al. Association of age and gender with anxiety disorders in older adults: a systematic review and meta-analysis. Int J Geriatr Psychiatry. (2019) 34:397–407. doi: 10.1002/gps.5035
60. Andrews G, Basu A, Cuijpers P, Craske MG, McEvoy P, English CL, et al. Computer therapy for the anxiety and depression disorders is effective, acceptable and practical health care: an updated meta-analysis. J Anxiety Disord. (2018) 55:70–8. doi: 10.1016/j.janxdis.2018.01.001
61. Carpenter JK, Andrews LA, Witcraft SM, Powers MB, Smits JA, Hofmann SG. Cognitive behavioral therapy for anxiety and related disorders: a meta-analysis of randomized placebo-controlled trials. Depress Anxiety. (2018) 35:502–14. doi: 10.1002/da.22728
62. Nolan LJ, Jenkins SM. Food addiction is associated with irrational beliefs via trait anxiety and emotional eating. Nutrients. (2019) 11:1711.
63. Romero-Blanco C, Hernández-Martínez A, Parra-Fernández ML, Onieva-Zafra MD, Prado-Laguna MD, Rodríguez-Almagro J. Food addiction and lifestyle habits among university students. Nutrients. (2021) 13:1352.
64. Borisenkov MF, Tserne TA, Bakutova LA. Food addiction in Russian adolescents: associations with age, sex, weight, and depression. Eur Eat Disord Rev. (2018) 26:671–6. doi: 10.1002/erv.2644
65. Okunogbe A, Nugent R, Spencer G, Ralston J, Wilding J. Economic impacts of overweight and obesity: current and future estimates for eight countries. BMJ Glob Health. (2021) 6:e006351. doi: 10.1136/bmjgh-2021-006351
66. Jacques A, Chaaya N, Beecher K, Ali SA, Belmer A, Bartlett S. The impact of sugar consumption on stress driven, emotional and addictive behaviors. Neurosci Biobehav Rev. (2019) 103:178–99. doi: 10.1016/j.neubiorev.2019.05.021
67. Dutheil S, Ota KT, Wohleb ES, Rasmussen K, Duman RS. High-fat diet induced anxiety and anhedonia: impact on brain homeostasis and inflammation. Neuropsychopharmacology. (2016) 41:1874–87. doi: 10.1038/npp.2015.357
68. Sivanathan S, Thavartnam K, Arif S, Elegino T, McGowan PO. Chronic high fat feeding increases anxiety-like behaviour and reduces transcript abundance of glucocorticoid signalling genes in the hippocampus of female rats. Behav Brain Res. (2015) 286:265–70. doi: 10.1016/j.bbr.2015.02.036
69. Puccio F, Fuller-Tyszkiewicz M, Youssef G, Mitchell S, Byrne M, Allen N, et al. Longitudinal Bi-directional effects of disordered eating, depression and anxiety. Eur Eat Disord Rev. (2017) 25:351–8. doi: 10.1002/erv.2525
70. Micali N, Solmi F, Horton NJ, Crosby RD, Eddy KT, Calzo JP, et al. Adolescent eating disorders predict psychiatric, high-risk behaviors and weight outcomes in young adulthood. J Am Acad Child Adolesc Psychiatry. (2015) 54:652.e–9.e. doi: 10.1016/j.jaac.2015.05.009
71. Adams RC, Sedgmond J, Maizey L, Chambers CD, Lawrence NS. Food addiction: implications for the diagnosis and treatment of overeating. Nutrients. (2019) 11:2086.
72. Godfrey KM, Gallo LC, Afari N. Mindfulness-based interventions for binge eating: a systematic review and meta-analysis. J Behav Med. (2015) 38:348–62. doi: 10.1007/s10865-014-9610-5
73. Blanchet C, Mathieu M-È, St-Laurent A, Fecteau S, St-Amour N, Drapeau V. A systematic review of physical activity interventions in individuals with binge eating disorders. Curr Obes Rep. (2018) 7:76–88. doi: 10.1007/s13679-018-0295-x
Keywords: gender, GAD-7, YFAS, anxiety, longitudinal, food addiction
Citation: Hussenoeder FS, Pabst A, Conrad I, Löbner M, Engel C, Zeynalova S, Reyes N, Glaesmer H, Hinz A, Witte V, Schroeter ML, Wirkner K, Kirsten T, Löffler M, Villringer A and Riedel-Heller SG (2022) Anxiety and Food Addiction in Men and Women: Results From the Longitudinal LIFE-Adult-Study. Front. Psychiatry 13:914358. doi: 10.3389/fpsyt.2022.914358
Received: 06 April 2022; Accepted: 25 May 2022;
Published: 14 June 2022.
Edited by:
Hubertus Himmerich, King’s College London, United KingdomReviewed by:
Ashley Nicole Gearhardt, University of Michigan, United StatesCopyright © 2022 Hussenoeder, Pabst, Conrad, Löbner, Engel, Zeynalova, Reyes, Glaesmer, Hinz, Witte, Schroeter, Wirkner, Kirsten, Löffler, Villringer and Riedel-Heller. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Felix S. Hussenoeder, RmVsaXguSHVzc2Vub2VkZXJAbWVkaXppbi51bmktbGVpcHppZy5kZQ==; Alexander Pabst, QWxleGFuZGVyLlBhYnN0QG1lZGl6aW4udW5pLWxlaXB6aWcuZGU=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.