
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry , 16 September 2022
Sec. Digital Mental Health
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.913213
This article is part of the Research Topic Role of Assistive Technologies to Offer Diagnosis, Intervention and Rehabilitation for individuals with Neurological or Neurodevelopmental Disorder View all 5 articles
 James Chung-Wai Cheung1,2
James Chung-Wai Cheung1,2 Bryan Pak-Hei So1
Bryan Pak-Hei So1 Ken Hok Man Ho3
Ken Hok Man Ho3 Duo Wai-Chi Wong1
Duo Wai-Chi Wong1 Alan Hiu-Fung Lam4
Alan Hiu-Fung Lam4 Daphne Sze Ki Cheung2,5*
Daphne Sze Ki Cheung2,5*Agitated behaviour among elderly people with dementia is a challenge in clinical management. Wrist accelerometry could be a versatile tool for making objective, quantitative, and long-term assessments. The objective of this review was to summarise the clinical application of wrist accelerometry to agitation assessments and ways of analysing the data. Two authors independently searched the electronic databases CINAHL, PubMed, PsycInfo, EMBASE, and Web of Science. Nine (n = 9) articles were eligible for a review. Our review found a significant association between the activity levels (frequency and entropy) measured by accelerometers and the benchmark instrument of agitated behaviour. However, the performance of wrist accelerometry in identifying the occurrence of agitation episodes was unsatisfactory. Elderly people with dementia have also been monitored in existing studies by investigating the at-risk time for their agitation episodes (daytime and evening). Consideration may be given in future studies on wrist accelerometry to unifying the parameters of interest and the cut-off and measurement periods, and to using a sampling window to standardise the protocol for assessing agitated behaviour through wrist accelerometry.
Agitation is highly prevalent among older adults with dementia, ranging from 24.8 to 71% depending on the severity of the dementia (1–4). Individuals have exhibited subsyndromes of dementia, including agitation, psychosis, affective symptoms, and apathy, with the level of agitation increasing with the severity of the dementia (5). Healthcare providers may find it challenging in caring agitated people with dementia in places such as homes, hospitals, residential care homes, and elderly day centres (6). Safety issues are significant considerations in elderly care. Agitation-induced wandering behaviour or physical aggression increases the fall and injury risks for the agitated individuals, the people around them, and caregivers, and are associated with an increased use of restraints, both physical (e.g., bedside rails, alarm pads) and chemical (e.g., antipsychotic and hypnotic drugs). These restraints might in turn aggravate psychosocial and agitation problems among older adults (7), precipitating stress, embarrassment, and safety risks among informal caregivers and reducing their quality of life (8, 9). Family caregivers might then send their relatives to residential care homes, increasing the healthcare burden.
Agitated behaviour is broadly classified as excessive motor activity, verbal aggression, or physical aggression by patients with cognitive impairment and emotional distress, which may cause excess disability (10). Agitated behaviour is not solely attributable to the care environment, other disorders, or to the effects of taking a substance (10). It could also be found in individuals without cognitive impairment (11). Non-aggressive physical behaviours include wandering, hiding things, and repetitive mannerisms. Individuals may present verbally, through such behaviours as complaining, asking repetitive questions, and making unwarranted requests. Aggressive behaviours include screaming noises, which could advance to aggressive physical actions such as throwing things, hitting, and hurting oneself or others.
Traditionally, agitation is identified via informant rating and observation. Informant ratings are based on the frequency and severity of the agitated behaviours reported by caregivers, although these are subjective, prone to bias, and blended with the ratings for other dementia symptoms (12, 13). An observational method has been proposed, involving videotaping an individual's behaviour at a given time and having trained personnel watch the videotape (12). Apart from observer bias, a long duration of observation is required to detect low-frequency agitated behaviours, making continuous monitoring infeasible (6, 12).
Technological assessments enable objective, manpower-saving, and continuous monitoring of agitated behaviours, while traditional observational approaches or questionnaires are generally subjective. Actigraphy or accelerometry is increasingly being applied to monitor agitation through the measurement of physical activity among older adults (14). Actigraphy and accelerometry are often used interchangeably (15). While accelerometers refer to the sensors that measure acceleration of body segments (16), actigraphy is a process that involves applying accelerometer data to quantify and infer motor or behavioural activities, such as sleeping and waking, often through a wrist-worn accelerometric measurement device (17). Accelerometers detect movement by the acceleration and deceleration signals induced by the initialisation and termination of movements. There is no acceleration when the movement of the body is steady or stationary. The principle of assessment lies in the characteristics of repetitive movements when agitated, such as restlessness and pacing (18). Accelerometers, some integrated with gyroscopes, can detect movements and changes of velocity at a wide range of frequencies. The collected data can be used to classify different postures, activities, postural transitions, and walking patterns (19, 20), and has been used to evaluate wandering behaviour (21), restlessness during sleep (22), physical exercise levels (23), walking instability (24), and falling events (25). Moreover, the validity of accelerometry in agitation assessments has been demonstrated through correlation with other instruments, including the Cohen-Mansfield Agitation Inventory (CMAI) and the Neuropsychiatric Inventory (NPI) (26). However, its application and analytical methods have varied across studies, which may have hindered its usage and the development of related research.
Healthcare assessments and management for older adults in clinical settings remain one of the greatest challenges in public health, especially for those with dementia or other chronic diseases. Common behavioural symptoms associated with dementia, such as agitation and wandering, impose significant psychological distress on caregivers and fall or injury risks to older people. The coronavirus disease 2019 (COVID-19) pandemic has led to pressure on healthcare workers and staff shortages. In addition, social distancing and mask-wearing measures have negatively impacted older people and potentially exaggerated the behavioural problems of those with dementia (27–29). Healthcare technology, such as wrist accelerometry for agitation monitoring, provides a versatile platform for real-time and prolonged assessments to facilitate better clinical management and relieve the staffing and hospitalisation burden (30). Moreover, traditional screening or assessment methods rely on subjective observations from professionals or data from questionnaires. Wrist accelerometry may provide an objective way to evaluate and quantify levels of agitated behaviour.
There have been some similar reviews of this topic. Camargos et al. (31) focused on the application of wrist accelerometry in night-time agitation and sleep disturbances in comparison to polysomnography, while Cheung et al. (19) reported on the application of accelerometry in determining daily activities. Khan et al. (6) endeavoured to summarise platforms for automatic detection and generalised predictive models for sensors in detecting agitation and aggression. The objectives of this review are to supplement previous reviews by: (1) reviewing the application of wrist accelerometry for monitoring agitated behaviours among people with dementia in clinical settings; (2) understanding the analytical approach of wrist accelerometry in assessing agitated behaviours; and (3) commenting on the potential weaknesses of current applications.
This scoping review was based on the approach of Arksey and O'Malley (32), which includes five steps: (i) identifying the research question; (ii) searching for relevant studies; (iii) selecting the studies; (iv) charting the data; and (v) collating, summarising, and reporting the results. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines were followed in reporting the study (33).
1. How was the wrist accelerometry/actigraphy applied in the clinical settings to monitor agitation for individuals with dementia?
2. How was wrist accelerometry/actigraphy evaluated by comparing the results to those obtained with a benchmarked instrument or by comparing the results of individuals with and without agitation?
3. How were the collected data analysed?
Eligibility was limited to original research articles published in peer-reviewed academic journals in English from the year 2000 onwards, a time during which the application of accelerometry for agitation monitoring had gained acceptance (14). The inclusion criteria included: (1) studies in which the participants had been diagnosed with any type of dementia (such as Alzheimer's disease or vascular dementia); (2) a study design that included the application of a wrist accelerometer/actigraph for monitoring agitation, an investigation of those with agitated and non-agitated dementia, and validation against/association with benchmarked instruments for measuring agitation; (3) studies conducted in non-laboratory clinical field settings, such as communities, hospitals, or residential care homes.
Exclusion criteria included: (1) non-original research (e.g., reviews or perspective articles); (2) articles not from academic journals (e.g., conference papers, patents); (3) articles with insufficient content on the setting and results of the accelerometry on dementia agitation: (4) studies where the accelerometry/actigraph was not on a wrist configuration; (5) studies not primarily dedicated to or measuring agitation (e.g., measuring rest and activity levels without addressing agitation); (6) intervention studies (e.g., those evaluating the influence of a medication or therapy).
A systematic literature search was performed to identify studies reporting on the application of wrist accelerometry in monitoring the agitated behaviour of people with dementia. The literature search was performed on databases including Web of Science, PubMed, PsycInfo, EMBASE, and CINAHL. The first and second author ran the independent searches on 20 March 2022. The search was conducted using MeSH or natural language keywords in the title and abstract of articles related to dementia, accelerometry/actigraphy, and agitation. The full search strategy is set out in Supplementary Table 1.
Titles and abstracts were screened first, followed by a full-text screening according to the eligibility criteria. The two-step screening process was conducted by the first and second authors working independently. Any disagreements were resolved by seeking a consensus with the corresponding author. To ensure the consistency between two reviewers, they had pilot reviewed 10% of the retrieved articles at both stages according to the selection criteria and got a consensus before reviewing separately.
A data charting form was designed based on the research questions. Information on the studies was extracted, including a summary of background information on the study, accelerometer/actigraph measurements, data analyses, and findings. The data charting results were cross-checked to ensure accuracy.
A descriptive summary was developed to collate and summarise the results.
An initial search yielded 333 articles, from which 49 duplicates were removed. A preliminary screening of titles and abstracts was conducted on 284 records, and 186 of them were excluded because the articles were irrelevant (n = 2), of the wrong type (e.g., review articles, conference papers) (n = 20), not in English (n = 1), unrelated to accelerometer/actigraph (n = 107), agitation (n = 20), or dementia (n = 35), or not a human study (n = 1). Ninety-eight articles remaining after the preliminary screening, the full texts of which were then screened. Eighty-nine of them were excluded, the reasons being that the article did not appear in a journal (n = 1), was of the wrong type (n = 8), contained insufficient data (n = 2), was an intervention study (n = 17), not conducted in a clinical settings (n = 5), the study design was ineligible (n = 7), the study was not related to or did not measure agitation (n = 29), was not related to or did not measure agitation by accelerometer/actigraph (n = 16), and the accelerometer/actigraph was not at a wrist setting (n = 4). In the end, nine articles were eligible for the review. Figure 1 shows the flowchart of this selection process.
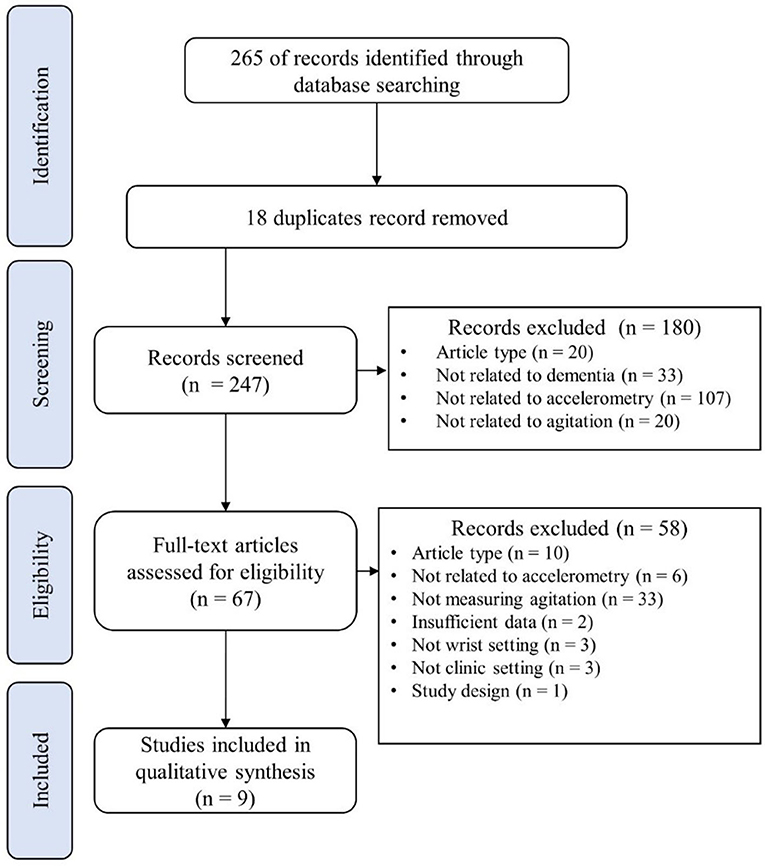
Figure 1. Flowchart of the systematic search and screening.
Although the parameters of the literature search included articles published as early as 2000, the earliest article found was published in 2006. Among the nine articles, five were on studies conducted in the Americas, three in Europe, and one in Asia. As shown in Table 1, the articles involved 373 individuals (134 males and 239 females), with sample sizes ranging from 1 to 183. Six out of nine articles had a sample size of <20. Nearly all of the participants were older, with a pooled weighted average age of 82. Most of the studies involved participants with Alzheimer's disease or other types of dementia. They were diagnosed using the National Institute of Neurological Disorders and Stroke-Alzheimer Disease and Related Disorders (NINCDS-ADRDA) criteria (42), measurements drawn from the Diagnostic and Statistical Manual of Mental Disorders (43) or by the Clinical Dementia Rating Scale (44).
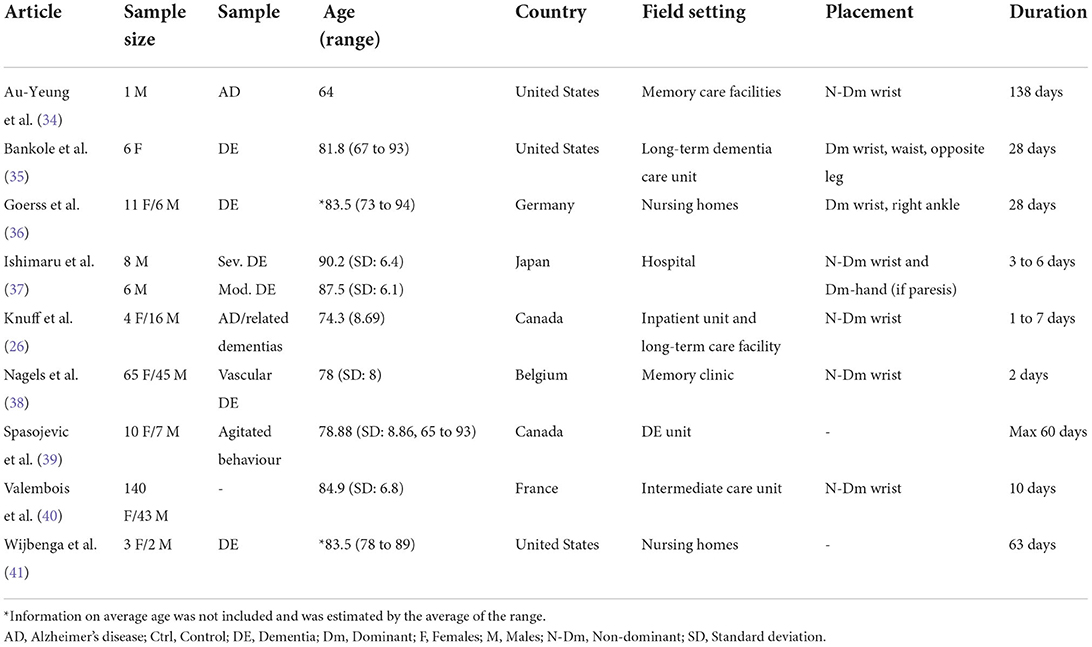
Table 1. Basic information on the eligible articles.
Most of the work took place in specialised care units, in addition to nursing homes and inpatient wards. The measurement periods ranged from 2 days to 138 days and five out of nine studies had a measurement period of more than 28 days (i.e., 4 weeks). Some studies did not employ a unified measurement time for their participants (26, 37, 39). Six included studies placed the accelerometer device on the non-dominant wrist, while two studies placed it on the dominant wrist. One study emphasised that the accelerometer device was switched to the dominant wrist if a participant had paresis on the non-dominant wrist (37). Another study mentioned that an ankle accelerometer was used during the night so that the battery could be recharged on the wrist accelerometer during the daytime (36). Two articles also included accelerometer measurements of the ankle or waist (35, 36).
Regarding the objectives or design of the studies, two articles implemented a descriptive approach to dementia with agitation samples, and then investigated the relationship between agitated episodes and some risk factors (34, 41). Six studies correlated the accelerometric data to a benchmarked instrument and one of them further evaluated the differences between individuals with different levels of agitation (26). Valembois et al. (40) compared the accelerometry between individuals with and without agitation, whilst Spasojevic et al. (39) evaluated the internal validity of different classifiers on identifying agitation episodes.
The accelerometric devices that were used in the studies covered in the review articles differed (see Table 2). All but one study applied commercially available accelerometric or actigraphic devices. These included Actiwatch Spectrums (Philips Respironics, Murrysville, United States), Grey Innovation Sensors (Grey Innovation, Melbourne, Australia), Micro Motionlogger WatchWare (Ambulatory Monitoring Inc., New York, United States), wGT3x+ (ActiGraph LLC, Pensacola, United States), Actiwatch (Neurotechnology Co., Cambridge, United Kingdom), Empatica E4 wristband (Empatica Inc., Boston, United States), Vivago (Vivago Oy, Espoo, Finland), and MotionWatch 8 (CamNtech, Cambridgeshire, UK). It should be noted that some of these devices incorporated gyroscopes and could be called inertial measurement units (IMUs). On the other hand, Bankole et al. (35) utilised the concept of the body sensor network using a collection of wearable sensor nodes (45), processing and integrating the data through technology-enabled medical precision observation (TEMPO) technology.
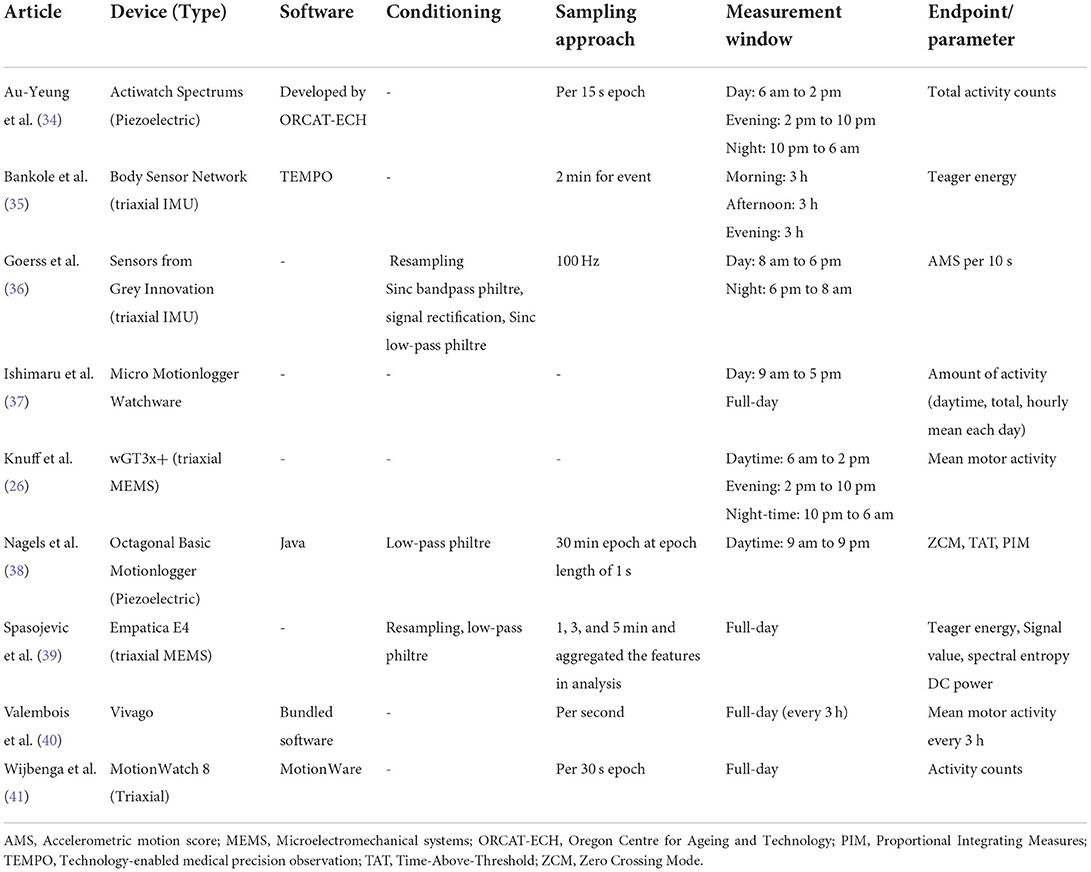
Table 2. Accelerometer specification, data conditioning, and endpoints.
Some studies employed an accelerometer with fewer than three axes (34, 38). Cheung et al. (19) recommended against this practise because the movements associated with agitation are not always in two dimensions. In addition, some of the devices employed in the included studies incorporated IMU, which is more desirable. This is because static acceleration, such as gravity, makes it impossible for an accelerometer to differentiate between dynamic translation and rotational motion (46). An accelerometer with a gyroscope and a magnetometer as an IMU can fully interpret motion signals. The integrated sensors demonstrate better reliability and accuracy and also enable the intensity of movements to be determined and thus allow activities to be classified (19). Two studies (34, 38) employed piezoelectric accelerometers in contrast to the ordinary accelerometers based on Microelectromechanical systems (MEMS) used in other studies. A piezoelectric accelerometer consists of a seismic mass hanged by a piezoelectric beam, which has undergone bending and has displaced charges upon acceleration (47).
Two-thirds of the studies did not provide adequate information on the data processing or filtering methods that were used, but some studies reported that they had utilised the stipulated bundled software for processing the data. While Goerss et al. (36) and Spasojevic et al. (39) resampled the data before processing it, three studies utilised different signal filtering strategies, including a low-pass filter at 2 to 3 Hz (38), a Butterworth low-pass filter at the 6 Hz cut-off point (39), and a Sinc bandpass and low pass philtre with signal rectification (36). Goerss et al. (36) defined the Accelerometric Motion Score (AMS) as the average activity count after data conditioning.
Nevertheless, the endpoint parameters for all studies were different. Therefore, comparing outcomes was difficult, especially when the sampling, measurement, and selection of averaging sums differed. The total amount and average amount of activity over a period were intuitive estimation and commonly used for evaluation (26, 34, 36, 37, 39–41). With the Zero Crossing Mode (ZCM) and the Time-Above-Threshold (TAT), the occurrence and time of the activity are taken into consideration only when the accelerometer signal is above the threshold value (38). Some other analyses recommended that at least 3 days of measurements are needed to accurately estimate physical activity levels (48). Relevant information is needed for assessing dementia agitation. In addition, two studies endeavoured to identify the occurrence of agitation episodes from labelled data, instead of recognising individuals with agitated behaviour in general (35, 39).
Apart from the time domain signal analytics (i.e., the number of counts), the frequency response of the triaxial accelerometer signals can also be analysed using the Fourier transform, Laplace transform, or other similar ways of identifying the peak of the amplitude and its frequency with regard to the 3-axis acceleration signal (49). On the other hand, by using power spectrum density (PSD), the power level of 3-axis acceleration signals and the resultant acceleration can be shown (50). The change in power level from a calm state to an agitated state may provide further data to shed light on the nature of the agitated behaviours.
Entropy-related parameters were also applied in some analyses. For example, the Proportional Integrating Measure (PIM) was calculated based on the area under the rectified accelerometer signal (38). The Teager energy score, which appeared in two articles, is a measure of aggregated movement energy and was calculated by the sum of the amplitude squared and the frequency squared of the signal (35, 39). Spasojevic et al. (39) integrated many parameters for detecting agitation, including the maximum, minimum, mean, and simple square integral of the Teager energy; and the mean, minimum, standard deviation, interquartile range, spectral entropy, and DC power of the accelerometer signal. A Pearson correlation analysis was conducted, with a cut-off point of 0.9 to avoid multicollinearity.
The protocol for measuring activity differed among studies according to their research objectives. Three articles considered a global association of activity counts with agitation (e.g., summing the activity count over 24 h) (26, 37, 41), while Valembois et al. (40) also took measurements over 24 h but analysed the data every 3 h. Au-Yeung et al. (34) stratified the full-day measurement into days (6 am to 2 pm), evenings (2 pm to 10 pm), and nights (10 pm to 6 am). Two articles defined the daytime activities differently, from 9 am to 5 pm (37), and from 9 am to 9 pm (38), respectively. Goerss et al. (36) monitored a morning and an afternoon section, while Bankole et al. (35) picked three sets of 3-h sections at different times of the day.
Nearly all studies investigated the association between accelerometric-measured activity and measures of agitated behaviour, particularly using parametric tests (e.g., t-test, ANOVA) or non-parametric tests (e.g., Wilcoxon's signed-rank test, the Mann-Whitney U test) to compare groups with or without agitation; and correlation tests (e.g., Spearman or Pearson tests) between the level of agitation and accelerometry readings (see Table 3). Spasojevic et al. (39) constructed several classifiers to segregate agitation episodes with accelerometer signals, but all produced poor performance, with the Area under the Receiver Operating Characteristics (AUC) being <0.65.
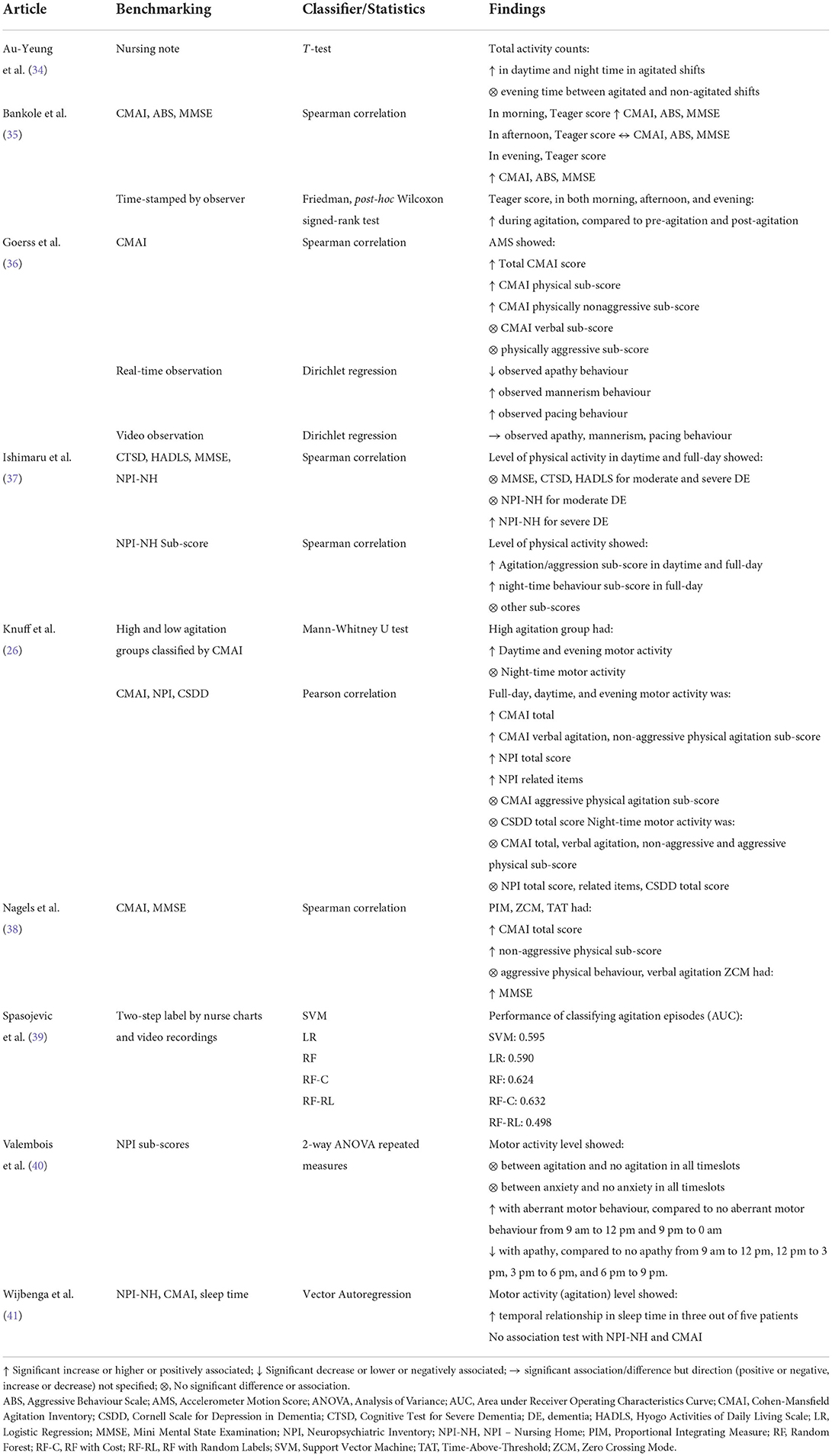
Table 3. Data analysis and key findings.
The Cohen-Mansfield Agitation Inventory (CMAI) and the Neuropsychiatric Inventory (NPI) were benchmarks for labelling the class or severity of the agitated behaviour completed by a proxy (51, 52). The CMAI is a 29-item questionnaire on agitated behaviour, on a seven-point scale of frequency. Its subgroup constructs or sub-scores are also commonly used, including the aggressive behaviour sub-score, the physical non-aggressive behaviour sub-score, and the verbally agitated behaviour sub-score (51). Both Knuff et al. (26) and Nagels et al. (38) divided the participants into those exhibiting high and low levels of agitation at a cut-off point of 50 for the CMAI total score. The NPI was developed to assess neuropsychiatric syndromes for patients with a score system calculated by multiplying the frequency (1 to 4 points) and severity (1 to 3 points) of each item on 10 domains. The instrument has been translated into different versions and languages (53), including a nursing home version (NPI–NH) used by Ishimaru et al. (37). The original version encompassed domains that could be broadly classified as depression-related or delusion-related items, while the sub-scores on anxiety, agitation, aberrant motor disturbance, apathy, and night-time disturbances appeared in our review. Other related instruments included the Aggressive Behaviour Scale (ABS) (54) and the Mini Mental State Examination (MMSE) (55).
In general, the application of wrist accelerometry (or movement measurements) in recognising potentially agitated individuals was supported by the significant association with the benchmark instrument CMAI (26, 35, 36, 38). In addition, during the occurrence of agitation episodes an increase in motor activity level was also reported by the wrist accelerometer (35). Interestingly, in a few studies a correlation with the non-aggressive agitation sub-score was demonstrated, but not with the aggressive agitation and verbal agitation sub-scores (26, 36, 38). In other words, high levels of motion were associated with non-aggressive manoeuvres, such as restlessness, mannerisms, pacing, and hiding, instead of with aggressive manoeuvres, such as hitting, grabbing, and kicking. The findings were also confirmed by real-time and video-recorded observations (36).
Six articles analysed the level of activity at different times. Some studies divided the day into daytime and night-time, while some split the day into morning, afternoon, evening, and night-time. During daytime, all studies reported significant associations between agitation and level of activity, while three out of four studies supported the association during evening. Mixed results were found in the afternoon and night-time. One reason for this could be the heterogeneity in time-splitting, measurement time, sampling, wearing time, and compliance, while confounding factors such as the environment and co-residence with other people could have influenced the level of activity during the night-time. In the afternoon, individuals in residential care homes may have some physical activities or entertainment arranged for them, while those in inpatient wards may have limited activities. These scheduled activities may have positive or negative impacts on people with dementia with agitation and other related behavioural constructs (56).
Our review showed that the frequency or entropy (aggregated energy) of activity levels as measured by wrist accelerometers was associated with agitated behaviour in clinical settings despite differences in accelerometer devices and research protocols (26, 35, 36, 38). Nevertheless, one study reported poor discriminative performance from actigraphy in identifying agitation episodes (39). The objective, quantitative, real-time and prolonged nature of accelerometry could also complement the weaknesses of benchmark questionnaires or observations. However, improvement is required if accelerometers are to be used to identify or measure agitated behaviour episodes. Yet evaluations of the discriminating power of accelerometry on agitation or not are lacking, for example using sensitivity, specificity, or receiver-operating characteristic curves.
The time when behavioural disturbances were exhibited by agitated persons with dementia was commonly examined in clinical settings, with daytime and evening likely to be the most likely times. Au-Yeung et al. (34) also investigated the influence of environmental light, noise, temperature, humidity, and level of pollutants, in a study that employed wearable devices that monitored the skin temperature and heart rate of individuals (36). In one review, it was suggested that integrating accelerometers with other sensors may improve the accuracy with which agitation and aggressive behaviours are detected, and that more field validation is required (6). In short, multi-modal sensor platforms could provide clinical management with information that could be used to modify the environment and design entertainment programmes and activities, such as music interventions, to alleviate agitation and promote well-being among agitated individuals (57).
There are some drawbacks to wrist accelerometry. Accelerometry can only measure physical signals, and therefore cannot be used conduct an assessment of verbal agitation (58). Our review also found that the level of physical activity was not correlated with the verbal agitation construct in the questionnaire (26, 36, 38). The maintenance and power of the wearable devices could be another problem for 24-h surveillance. In fact, Bankole et al. (35) reported critical incidents that occurred in the study due to device break-down, albeit at a low rate. Discomfort in wearing the wrist accelerometers presented another notable problem, contributing to drop-outs, poor skin contact, and other compliance issues that were reported in the articles that we reviewed (37, 40). Some studies proposed using a depth-channel camera and machine learning model for behavioural surveillance as a compromise between privacy and the need to carry out monitoring (59, 60), and this has been successfully implemented in clinical settings (61). We also discovered some potential biases in the studies. For example, only records with high-quality data and sufficient time and days were analysed (39, 40). Agitated individuals might wear the devices less often and exhibit poorer compliance (26), while some agitated behaviour may result in poor contact with the wrist accelerometers and therefore lead to poor-quality data. Therefore, it is possible that only “obedient” agitated individuals or moments were included in the data.
There were some limitations to this review. First of all, selection bias could have resulted from the inclusion criteria, with only original articles and journal papers in English eligible for inclusion. Second, our review targeted clinical settings and discarded some studies with home-based or laboratory settings (62, 63). Those laboratory studies contributed more to the development of systems and classification models with more technical specifications than those studies that used secondary datasets or created data by instructing participants to perform agitated and non-agitated acts (64, 65). There were other data analysis methods, such as the inter-daily stability and intra-daily variability on actigraphic rest-and-activity rhythms (66). Some studies were also excluded because they were not focused on agitation, although they assessed the motor activity or rest patterns of the patients. In future studies, consideration may be given to investigating the application of accelerometry to evaluate interventions such as those involving medications (67, 68), electrical stimulation (69), and light therapy (70).
Given that agitation is common among people with dementia, employing technology for assessing the agitated behaviour may be beneficial for both patients and caregivers. In the future, we recommended standardising the protocol for assessing agitated behaviour by unifying the parameter-of-interest, cut-offs, measurement period, and sampling window for wrist accelerometry/actigraphy. Validating multi-modal sensors, which measure different parameters may be the next step to increase the accuracy of agitated behaviours assessment.
DC and KH designed the study. JC, BS, and DW searched for and screened studies. JC and BS extracted data from the selected studies. JC, DW, DC, and AL wrote the manuscript. KH critically reviewed it. All authors reviewed and edited the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.913213/full#supplementary-material
1. Hendriks SA, Smalbrugge M, Galindo-Garre F, Hertogh CM, Van Der Steen JT. From admission to death: prevalence and course of pain, agitation, and shortness of breath, and treatment of these symptoms in nursing home residents with dementia. J Am Med Dir Assoc. (2015) 16:475–81. doi: 10.1016/j.jamda.2014.12.016
2. Sampson EL, White N, Lord K, Leurent B, Vickerstaff V, Scott S, et al. Pain, agitation, and behavioural problems in people with dementia admitted to general hospital wards: a longitudinal cohort study. Pain. (2015) 156:675–83. doi: 10.1097/j.pain.0000000000000095
3. Tanaka H, Hashimoto M, Fukuhara R, Ishikawa T, Yatabe Y, Kaneda K, et al. Relationship between dementia severity and behavioural and psychological symptoms in early-onset Alzheimer's disease. Psychogeriatrics. (2015) 15:242–7. doi: 10.1111/psyg.12108
4. Halpern R, Seare J, Tong J, Hartry A, Olaoye A, Aigbogun MS. Using electronic health records to estimate the prevalence of agitation in Alzheimer disease/dementia. Int J Geriatr Psychiatry. (2019) 34:420–31. doi: 10.1002/gps.5030
5. Selbæk G, Engedal K, Benth JŠ, Bergh S. The course of neuropsychiatric symptoms in nursing-home patients with dementia over a 53-month follow-up period. Int Psychogeriatr. (2014) 26:81–91. doi: 10.1017/S1041610213001609
6. Khan SS, Ye B, Taati B, Mihailidis A. Detecting agitation and aggression in people with dementia using sensors—a systematic review. Alzheimers Dement. (2018) 14:824–32. doi: 10.1016/j.jalz.2018.02.004
7. Cipriani G, Lucetti C, Carlesi C, Danti S, Nuti A. Sundown syndrome and dementia. Eur Geriatr Med. (2015) 6:375–80. doi: 10.1016/j.eurger.2015.03.006
8. Cohen-Mansfield J. Agitated behavior in persons with dementia: the relationship between type of behavior, its frequency, and its disruptiveness. J Psychiatr Res. (2008) 43:64–9. doi: 10.1016/j.jpsychires.2008.02.003
9. Sampson EL, Stringer A, La Frenais F, Higgins S, Doyle M-J, Laybourne A, et al. Agitation near the end of life with dementia: an ethnographic study of care. PLoS ONE. (2019) 14:1–19. doi: 10.1371/journal.pone.0224043
10. Cummings J, Mintzer J, Brodaty H, Sano M, Banerjee S, Devanand D, et al. Agitation in cognitive disorders: International Psychogeriatric Association provisional consensus clinical and research definition. Int Psychogeriatr. (2015) 27:7–17. doi: 10.1017/S1041610214001963
11. Brown DT, Westbury JL, Schüz B. Sleep and agitation in nursing home residents with and without dementia. Int Psychogeriatr. (2015) 27:1945–55. doi: 10.1017/S1041610215001568
12. Cohen-Mansfield J, Martin LS. Assessment of agitation in older adults. In: Lichtenberg PA, editor. Handbook of Assessment in Clinical Gerontology. Cambridge, Massachusetts: Academic Press (2010). p. 381–403. doi: 10.1016/B978-0-12-374961-1.10015-6
13. Reverdink I. The state of the art of the technologies that monitor disease progression in dementia patients: A scoping review. Psychology BSc, University of Twente (2019).
14. André PSDB, Varum H. Accelerometers: Principles, Structure and Applications. New York: Nova Publishers (2013).
15. Quante M, Kaplan ER, Rueschman M, Cailler M, Buxton OM, Redline S. Practical considerations in using accelerometers to assess physical activity, sedentary behavior, and sleep. Sleep Health. (2015) 1:275–84. doi: 10.1016/j.sleh.2015.09.002
16. Migueles JH, Cadenas-Sanchez C, Ekelund U, Delisle Nyström C, Mora-Gonzalez J, Löf M, et al. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: a systematic review and practical considerations. Sports Med. (2017) 47:1821–45. doi: 10.1007/s40279-017-0716-0
17. Reiterer V, Sauter C, Klösch G, Lalouschek W, Zeitlhofer J. Actigraphy–a useful tool for motor activity monitoring in stroke patients. Eur Neurol. (2008) 60:285–91. doi: 10.1159/000157882
18. Volicer L, Frijters DH, Van Der Steen JT. Relationship between symptoms of depression and agitation in nursing home residents with dementia. Int J Geriatr Psychiatry. (2012) 27:749–54. doi: 10.1002/gps.2800
19. Cheung VH, Gray L, Karunanithi M. Review of accelerometry for determining daily activity among elderly patients. Arch Phys Med Rehabil. (2011) 92:998–1014. doi: 10.1016/j.apmr.2010.12.040
20. Hong TT-H, Wang Y, Tan Q, Zhang G, Wong DW-C, Zhang M. Measurement of covered curvature based on a tape of integrated accelerometers. Measurement. (2022) 193:1–13. doi: 10.1016/j.measurement.2022.110959
21. Díaz-Ramírez A, Miranda-Vega JE, Ramos-Rivera D, Rodríguez DA, Flores-Fuentes W, Sergiyenko O. Time series data processing for classifying wandering patterns in people with dementia. IEEE Sens J. (2021) 22:10196–206. doi: 10.1109/JSEN.2021.3123543
22. Reimers A, Heidenreich V, Bittermann H, Knapp G, Reimers C. Accelerometer-measured physical activity and its impact on sleep quality in patients suffering from restless legs syndrome. BMC Neurol. (2021) 21:1–10. doi: 10.1186/s12883-021-02115-w
23. Liu JYW, Kor PPK, Chan CPY, Kwan RYC, Cheung DSK. The effectiveness of a wearable activity tracker (WAT)-based intervention to improve physical activity levels in sedentary older adults: A systematic review and meta-analysis. Arch Gerontol Geriatr. (2020) 91:1–17. doi: 10.1016/j.archger.2020.104211
24. Zhang G, Wong IK-K, Chen TL-W, Hong TT-H, Wong DW-C, Peng Y, et al. Identifying fatigue indicators using gait variability measures: a longitudinal study on elderly brisk walking. Sensors. (2020) 20:1–12. doi: 10.3390/s20236983
25. Cheung C-WJ, Chan W-HR, Chiu M-W, Law S-Y, Lee T-H, Zheng Y-P. A three-month study of fall and physical activity levels of intellectual disability using a transfer belt-based motion recording sensor. In: IFMBE Proceedings. Springer. p. 1393–6. doi: 10.1007/978-3-642-14515-5_355
26. Knuff A, Leung RH, Seitz DP, Pallaveshi L, Burhan AM. Use of actigraphy to measure symptoms of agitation in dementia. Am J Geriatr Psychiatry. (2019) 27:865–9. doi: 10.1016/j.jagp.2019.02.013
27. Kwan RYC, Lee PH, Cheung DSK, Lam SC. Face mask wearing behaviors, depressive symptoms, and health beliefs among older people during the COVID-19 pandemic. Front Med. (2021) 8:1–8. doi: 10.3389/fmed.2021.590936
28. Ho KHM, Mak AKP, Chung RWM, Leung DYL, Chiang VCL, Cheung DSK. Implications of COVID-19 on the loneliness of older adults in residential care homes. Qual Health Res. (2022) 32:279–90. doi: 10.1177/10497323211050910
29. Lo SKL, Liu JYW, Cheung DSK, Yin Y, Ng SY, Kor PPK, et al. “How are you doing?” on the healthy aging of the community-dwelling oldest-old in the shadow of the COVID-19 pandemic. Res Aging. (2022). doi: 10.1177/01640275221100949
30. Kales HC, Gitlin LN, Lyketsos CG. Assessment and management of behavioral and psychological symptoms of dementia. BMJ. (2015) 350:h369. doi: 10.1136/bmj.h369
31. Camargos EF, Louzada FM, Nóbrega OT. Wrist actigraphy for measuring sleep in intervention studies with Alzheimer's disease patients: application, usefulness, and challenges. Sleep Med Rev. (2013) 17:475–88. doi: 10.1016/j.smrv.2013.01.006
32. Arksey H, O'malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
33. Tricco AC, Lillie E, Zarin W, O'brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
34. Au-Yeung WTM, Miller L, Beattie Z, Dodge HH, Reynolds C, Vahia I, et al. Sensing a problem: Proof of concept for characterizing and predicting agitation. Alzheimers Dement. (2020) 6:1–10. doi: 10.1002/trc2.12079
35. Bankole A, Anderson M, Smith-Jackson T, Knight A, Oh K, Brantley J, et al. Validation of noninvasive body sensor network technology in the detection of agitation in dementia. Am J Alzheimers Dis Other Demen. (2012) 27:346–54. doi: 10.1177/1533317512452036
36. Goerss D, Hein A, Bader S, Halek M, Kernebeck S, Kutschke A, et al. Automated sensor-based detection of challenging behaviors in advanced stages of dementia in nursing homes. Alzheimers Dement. (2020) 16:672–80. doi: 10.1016/j.jalz.2019.08.193
37. Ishimaru D, Tanaka H, Nagata Y, Takabatake S, Nishikawa T. Physical activity in severe dementia is associated with agitation rather than cognitive function. Am J Alzheimers Dis Other Demen. (2020) 35:1–7. doi: 10.1177/1533317519871397
38. Nagels G, Engelborghs S, Vloeberghs E, Van Dam D, Pickut BA, De Deyn PP. Actigraphic measurement of agitated behaviour in dementia. Int J Geriatr Psychiatry. (2006) 21:388–93. doi: 10.1002/gps.1483
39. Spasojevic S, Nogas J, Iaboni A, Ye B, Mihailidis A, Wang A, et al. A pilot study to detect agitation in people living with dementia using multi-modal sensors. J Healthc Inform Res. (2021) 5:342–58. doi: 10.1007/s41666-021-00095-7
40. Valembois L, Oasi C, Pariel S, Jarzebowski W, Lafuente-Lafuente C, Belmin J. Wrist actigraphy: a simple way to record motor activity in elderly patients with dementia and apathy or aberrant motor behavior. J Nutr Health Aging. (2015) 19:759–64. doi: 10.1007/s12603-015-0530-z
41. Wijbenga RA, Blaauw FJ, Janus SIM, Tibben C, Smits AE, Voshaar RCO, et al. Individual differences in the temporal relationship between sleep and agitation: a single-subject study in nursing home residents with dementia experiencing sleep disturbance and agitation. Aging and Mental Health. (2022) 26:1669–77. doi: 10.1080/13607863.2021.1935464
42. Dubois B, Feldman HH, Jacova C, Dekosky ST, Barberger-Gateau P, Cummings J, et al. Research criteria for the diagnosis of Alzheimer's disease: revising the NINCDS–ADRDA criteria. Lancet Neurol. (2007) 6:734–46. doi: 10.1016/S1474-4422(07)70178-3
43. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Washington, DC: American Psychiatric Association (2013). doi: 10.1176/appi.books.9780890425596
44. Huang HC, Tseng YM, Chen YC, Chen PY, Chiu HY. Diagnostic accuracy of the clinical dementia rating scale for detecting mild cognitive impairment and dementia: a bivariate meta-analysis. Int J Geriatr Psychiatry. (2021) 36:239–51. doi: 10.1002/gps.5436
46. Van Hees VT, Gorzelniak L, Dean León EC, Eder M, Pias M, Taherian S, et al. Separating movement and gravity components in an acceleration signal and implications for the assessment of human daily physical activity. PLoS ONE. (2013) 8:1–10. doi: 10.1371/journal.pone.0061691
47. Chen KY, Bassett DR. The technology of accelerometry-based activity monitors: current and future. Med Sci Sports Exerc. (2005) 37:S490. doi: 10.1249/01.mss.0000185571.49104.82
48. Hart TL, Swartz AM, Cashin SE, Strath SJ. How many days of monitoring predict physical activity and sedentary behaviour in older adults? Int J Behav Nutr Phys Act. (2011) 8:1–7. doi: 10.1186/1479-5868-8-62
49. Fourati H, Manamanni N, Afilal L, Handrich Y. Complementary observer for body segments motion capturing by inertial and magnetic sensors. IEEE/ASME Trans Mechatron. (2014) 19:149–57. doi: 10.1109/TMECH.2012.2225151
50. Attal F, Mohammed S, Dedabrishvili M, Chamroukhi F, Oukhellou L, Amirat Y. Physical human activity recognition using wearable sensors. Sensors. (2015) 15:31314–38. doi: 10.3390/s151229858
51. Cohen-Mansfield J,. Instruction manual for the Cohen-Mansfield agitation inventory (CMAI). Australia: Research Institute of the Hebrew Home of Greater Washington (1991). Available online at: https://dementiaresearch.org.au/wp-content/uploads/2016/06/CMAI_Manual.pdf (accessed March 23, 2022).
52. Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology. (1994) 44:2308–14. doi: 10.1212/WNL.44.12.2308
53. Cummings J. The neuropsychiatric inventory: development and applications. J Geriatr Psychiatry Neurol. (2020) 33:73–84. doi: 10.1177/0891988719882102
54. Perlman CM, Hirdes JP. The aggressive behavior scale: a new scale to measure aggression based on the minimum data set. J Am Geriatr Soc. (2008) 56:2298–303. doi: 10.1111/j.1532-5415.2008.02048.x
55. Folstein MF, Folstein SE, Mchugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
56. Ayalon L, Bornfeld H, Gum AM, Areán PA. The use of problem-solving therapy and restraint-free environment for the management of depression and agitation in long-term care. Clin Gerontol. (2008) 32:77–90. doi: 10.1080/07317110802468728
57. Cheung DSK, Lai CKY, Wong FKY, Leung MCP. Is music-with-movement intervention better than music listening and social activities in alleviating agitation of people with moderate dementia? A randomized controlled trial. Dementia. (2020) 19:1413–25. doi: 10.1177/1471301218800195
58. Rose KM, Lach J, Perkhounkova Y, Gong J, Dandu SR, Dickerson R, et al. Use of body sensors to examine nocturnal agitation, sleep, and urinary incontinence in individuals with Alzheimer's disease. J Gerontol Nurs. (2018) 44:19–26. doi: 10.3928/00989134-20180626-03
59. Cheung JC-W, Tam EW-C, Mak AH-Y, Chan TT-C, Lai WP-Y, Zheng Y-P. Night-time monitoring system (eNightLog) for elderly wandering behavior. Sensors. (2021) 21:704. doi: 10.3390/s21030704
60. Tam AY-C, So BP-H, Chan TT-C, Cheung AK-Y, Wong DW-C, Cheung JC-W. A blanket accommodative sleep posture classification system using an infrared depth camera: A deep learning approach with synthetic augmentation of blanket conditions. Sensors. (2021) 21:1–13. doi: 10.3390/s21165553
61. Cheung JC-W, Tam EW-C, Mak AH-Y, Chan TT-C, Zheng Y-P. A night-time monitoring system (eNightLog) to prevent elderly wandering in hostels: a three-month field study. Int J Environ Res Public Health. (2022) 19:2103. doi: 10.3390/ijerph19042103
62. Kirste T, Hoffmeyer A, Koldrack P, Bauer A, Schubert S, Schröder S, et al. Detecting the effect of Alzheimer's disease on everyday motion behavior. J Alzheimers Dis. (2014) 38:121–32. doi: 10.3233/JAD-130272
63. Bankole A, Anderson MS, Homdee N, Alam R, Lofton A, Fyffe N, et al. BESI: Behavioral and environmental sensing and intervention for dementia caregiver empowerment—Phases 1 and 2. Am J Alzheimer's Dis other Dement. (2020) 35:1–15. doi: 10.1177/1533317520906686
64. Chikhaoui B, Ye B, Mihailidis A. Aggressive and agitated behavior recognition from accelerometer data using non-negative matrix factorization. J Ambient Intell Humaniz Comput. (2018) 9:1375–89. doi: 10.1007/s12652-017-0537-x
65. Tchuente F, Baddour N, Lemaire ED. Classification of aggressive movements using smartwatches. Sensors. (2020) 20:6377. doi: 10.3390/s20216377
66. Spira AP, Zipunnikov V, Raman R, Choi J, Di J, Bai J, et al. Brain amyloid burden, sleep, and 24-hour rest/activity rhythms: screening findings from the anti-amyloid treatment in asymptomatic Alzheimer's and longitudinal evaluation of amyloid risk and neurodegeneration studies. Sleep Advances. (2021) 2:zpab015. doi: 10.1093/sleepadvances/zpab015
67. Mahlberg R, Kunz D, Sutej I, Kuhl KP, Hellweg R. Melatonin treatment of day-night rhythm disturbances and sundowning in Alzheimer disease-an open-label pilot study using actigraphy. J Clin Psychopharmacol. (2004) 24:456–9. doi: 10.1097/01.jcp.0000132443.12607.fd
68. Mahlberg R, Walther S, Eichmann U, Tracik F, Kunz D. Effects of rivastigmine on actigraphically monitored motor activity in severe agitation related to Alzheimer's disease: a placebo-controlled pilot study. Arch Gerontol Geriatr. (2007) 45:19–26. doi: 10.1016/j.archger.2006.07.006
69. Scherder E, Knol D, Van Tol MJ, Van Someren E, Deijen JB, Swaab D, et al. Effects of high-frequency cranial electrostimulation on the rest-activity rhythm and salivary cortisol in Alzheimer's disease: a pilot study. Dement Geriatr Cogn Disord. (2006) 22:267–72. doi: 10.1159/000095108
Keywords: Alzheimer's disease, agitation, wearable device, dementia, wandering, wristband, mild cognitive impairment, aggression
Citation: Cheung JC-W, So BP-H, Ho KHM, Wong DW-C, Lam AH-F and Cheung DSK (2022) Wrist accelerometry for monitoring dementia agitation behaviour in clinical settings: A scoping review. Front. Psychiatry 13:913213. doi: 10.3389/fpsyt.2022.913213
Received: 05 April 2022; Accepted: 22 August 2022;
Published: 16 September 2022.
Edited by:
Kazunori Miyata, Japan Advanced Institute of Science and Technology, JapanReviewed by:
Elisabeth Flo, University of Bergen, NorwayCopyright © 2022 Cheung, So, Ho, Wong, Lam and Cheung. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daphne Sze Ki Cheung, ZGFwaG5lLmNoZXVuZ0Bwb2x5dS5lZHUuaGs=; ZGFwaG5lLnMuay5jaGV1bmdAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.