
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 10 June 2022
Sec. Aging Psychiatry
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.898990
This article is part of the Research Topic The Medium and Long-Term Effect of the COVID-19 Pandemic and Public Health Measures on modifiable Risk Factors for Dementia and Cognitive Decline: a Global Perspective View all 10 articles
 Nanae Matsumoto1
Nanae Matsumoto1 Taiki Sugimoto1,2
Taiki Sugimoto1,2 Yujiro Kuroda2
Yujiro Kuroda2 Kazuaki Uchida1,3
Kazuaki Uchida1,3 Yoshinobu Kishino1,4Hidenori Arai5Takashi Sakurai1,2,4*
Yoshinobu Kishino1,4Hidenori Arai5Takashi Sakurai1,2,4*Psychological resilience refers to the ability to cope with adversities, and deficits in resilience might lead to mental illness. The COVID-19 pandemic has had impact on psychological resilience for older adults, but there are as yet no data on its impacts on the mental health of older adults who were living with mild cognitive impairment (MCI). Therefore, the aim of this study was to investigate the impact of the COVID-19 pandemic on psychological resilience in older adults with MCI and to explore associated physical and psychosocial factors. In this cross-sectional study of 268 older adults aged 65–85, we defined MCI as age- and education-adjusted cognitive decline with a standard deviation of 1.0 or more from the reference threshold. During December 2020 to April 2021, we carried out to all participants the 10-item version of the Connor-Davidson Resilience Scale (CD-RISC-10) to measure psychological resilience. We also conducted a comprehensive geriatric assessment including sleep quality and depressive symptoms (Pittsburgh Sleep Quality Index and 15-item Geriatric Depression Scale, respectively). To identify factors associated with CD-RISC-10 scores (mean: 23.3 ± 0.4), multiple regression analysis revealed that older age [coefficient = 0.23, 95% confidence interval (CI) = 0.06–0.39] was significantly correlated with higher scores, whereas poor sleep quality (coefficient = −2.06, 95% CI = −3.93 to −0.19) and depressive symptoms (coefficient = −2.95, 95% CI = −5.70 to −0.21) were significantly correlated with lower scores. In this study, older adults with MCI showed low psychological resilience during the COVID-19 pandemic, and people with low psychological resilience indicated poor sleep quality and depressive symptoms. Our findings suggest directions for devising interventions to maintain mental health and psychological resilience among the vulnerable population of older adults with MCI living under the socially isolated conditions of COVID-19 pandemic restrictions. Our recommendation includes continuous assessment of this population and appropriate care for poor sleep quality and depressive symptoms.
The coronavirus disease 2019 (COVID-19) pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) began spreading in Japan in January 2020. Prevention measures such as social distancing effectively reduced new infections (1), but these measures severely restricted older adults' participation in physical, social, and community activities (2, 3). Although the number of participants was limited, the agitation, depression and anxiety of older adults with mild cognitive impairment (MCI) increased during lockdown (4). MCI or subjective cognitive decline showed decreased physical activity (43.4%) since the start of the lockdown, and there was an increase of 69.6% in the time spent sitting or lying down (5). These reports suggest that older adults with MCI have faced problems in mental health and physical activity during the COVID-19 pandemic.
Researchers found that isolation caused by infection prevention measures was linked to depression, anxiety, and cognitive decline as well as lower self-worth, which are factors involved in the concept of resilience (6).
Resilience is the ability to adapt positively in the face of adversity and maintain mental health (7), and it derives from a combination of genetic, biological, psychological, social, and cultural factors (8, 9). In one study before COVID-19, older adults showed higher psychological resilience than did young adults (10), although older adults with MCI showed lower resilience than did healthy older adults (11). High resilience is useful for recovering from stress (12), but some researchers found lower psychological resilience among adults during the pandemic compared with before (13–16). Given that older adults with MCI frequently showed mental health problems during the pandemic such as fear, anxiety, and frustration (17, 18), it is understandable that their psychological resilience would be affected as well. However, no researchers have yet investigated psychological resilience in older adults with MCI during the COVID-19 pandemic including factors related to their resilience. Therefore, we aimed with the present study to investigate these factors and the psychological resilience of older adults with MCI during the COVID-19 pandemic. Our identifying psychological resilience and these associated factors should help with developing effective mental health interventions for older adults with MCI.
We conducted this cross-sectional study as part of the World-Wide FINGERS SARS-CoV-2 survey (19) in World-Wide FINGERS (20), the global network of lifestyle intervention trials for dementia risk reduction and prevention. The 10-item version of the Connor-Davidson Resilience Scale (CD-RISC-10) (21) was used in the survey, which was conducted between December 2020 and April 2021, and a comprehensive geriatric assessment (CGA) in the present study was conducted between February 2020 and March 2021.
We recruited all participants from the Japan-multimodal intervention trial for prevention of dementia (J-MINT) conducted by the National Center for Geriatrics and Gerontology (NCGG) in Aichi Prefecture (22). The inclusion criterion of this study was older adults with MCI in the age group of 65–85 years. The diagnosis of MCI was made using the NCGG Functional Assessment Tool (FAT), which has been established as a screening tool for older adults at high risk of incident dementia (23, 24). All participants had age- and education-adjusted cognitive decline with a standard deviation (SD) of 1.0 or more from the reference threshold on at least one of the four cognitive domains of memory, attention, executive function, and processing speed as measured by the NCGG-FAT. The exclusion criteria were older adults diagnosed with dementia and having a Mini-Mental State Examination (MMSE) (25) score of < 24 points at baseline; respondents who self-reported a diagnosis of depression and those who had missing data on the CD-RISC-10 were excluded. Of 361 J-MINT participants at the NCGG, 298 took part in the present study. This study was approved by the NCGG Ethics Committee, and all participants underwent informed consent procedures prior to enrolling in the study, all participants gave their consent for participation in the study.
We collected participants' demographic information (age, sex, marital status, living status, years of education, employment status, household income, absolute alcohol consumption per day, smoking status, polypharmacy, and self-reported medical history) by questionnaire. The response options for household income were in increments of JPY 2,000,000, and for self-reported medical history, we asked about the following diseases: diabetes, hypertension, dyslipidemia, atrial fibrillation, congestive heart failure, chronic kidney disease, liver disease, cerebrovascular disease, malignant tumor, thyroid disease, coronary artery disease, neurodegenerative disease, depression and insomnia. For our analyses, the self-reported medical history was divided no medical condition or one or more.
We used the CD-RISC-10 score to evaluate respondents' psychological resilience. Respondents rate each item on a scale from 0 (not true at all) to 4 (true nearly all the time), so that the total score ranges from 0 to 40. Higher scores reflect greater psychological resilience.
To explore factors related to the older adults' psychological resilience in this study, we conducted a CGA, a inclusive method of assessing psychological and functional capability of older adults (26). For all participants, the CGA consisted of measuring physical performance, lifestyle, social participation, mental health, and cognitive function with the following full test battery: (1) We used the frailty phenotype proposed by Fried et al. (27), in the Cardiovascular Health Study to measure physical frailty (not frail, prefrail, or frail). (2) We used the Barthel Index (28) to assess basic activities of daily living (ADLs); this scale ranges from 0 to 100, with 100 points indicating complete independence. (3) We measured instrumental ADLs using the Lawton Index, for which perfect scores are 5 for men and 8 for women (29). (4) We used the EuroQol 5-Dimension (EQ−5D) to measure health-related quality of life. The scores for the five EQ-5D dimensions are combined to obtain up to 3,125 possible health states, from which a signal index (utility) score is computed; one score indicates better health status (30). (5) We measured the older adults' nutritional status with the Mini-Nutritional Assessment Short-Form (MNA-SF) (31), which consists of six items (score range: 0–14 points, normal ≥ 12). (6) Sleep quality was evaluated by the Pittsburgh Sleep Quality Index (PSQI); the score ranges from 0 to 21, and a score of 6 or higher indicates poor sleep quality (32). (7) We used the Lubben Social Network Scale-6 (LSNS-6) to measure participants' social networks and connections (33); the LSNS-6 consists of six items, the score ranges from 0 to 30, and scores of 11 or lower indicate social isolation. (8) We measured social participation by asking participants if they belonged to any of eight types of organizations presented in a list (34). (9) We based global cognitive functioning on the MMSE scores, which ranged from 0 to 30. (10) We conducted the 15-item Geriatric Depression Scale (GDS) to measure depression; the score ranges from 0 to 15, and higher scores indicate depressive symptoms (35). For the Japanese version of the GDS, 7 or more points indicates depressive symptoms (36).
All participants' demographic information is expressed as mean ± SD, median and interquartile range (IQR) or number of people and percentage. We used simple regression to analyze the associations between the CD-RISC-10 and each CGA variable, and we used multiple regression to analyze the CD-RISC-10-variable relationships that were statistically significant in the simple regressions, with the CD-RISC-10 score as the response variable and the statistically significant variables as explanatory variables. Moreover, we entered sex and education, which were related to psychological resilience in a previous study (16), as confounding variables. We conducted all analyses in Stata 16.1 (Stata Corp, College Station, TX, United States) and set P < 0.05 as statistically significant.
Of 298 original participants, 279 responded to the questionnaire of the CD-RISC-10 between December 2020 and April 2021 (response rate: 93.6%). From those 279, we excluded six respondents who self-reported depression and five whose CD-RISC-10 responses were incomplete, which left the data on 268 participants for the analysis. Table 1 shows the demographic characteristics of the participants in this study. The mean CD-RISC-10 score was 23.3 points.
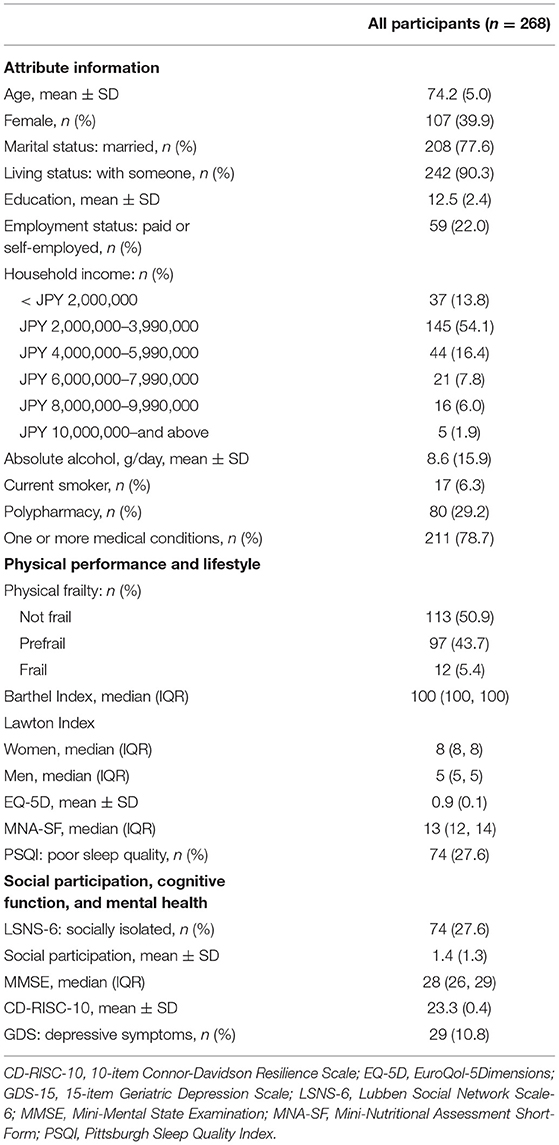
Table 1. Demographic characteristics and comprehensive geriatric assessment results.
Simple regression analysis showed that higher CD-RISC-10 score was significantly associated with older age and higher household income and lower score was related to social isolation, depressive symptoms, and poor sleep quality (Table 2). The CD-RISC-10 score was not associated with sex, marital status, living status, years of education, employment status, absolute alcohol consumption per day, smoking status, polypharmacy, or one or more medical conditions. In the multiple regression analysis of all statistically significant variables from the simple regressions, older age (coefficient = 0.23, 95% CI = 0.06–0.39) was related to higher CD-RISC-10 score, and depressive symptoms (coefficient = −2.95, 95% CI = −5.70 to −0.21) and poor sleep quality (coefficient = −2.06, 95% CI = −3.93 to −0.19) were associated with lower score (Table 2). The CD-RISC-10 score was not associated with sex, years of education, household income, or LSNS-6 scores.
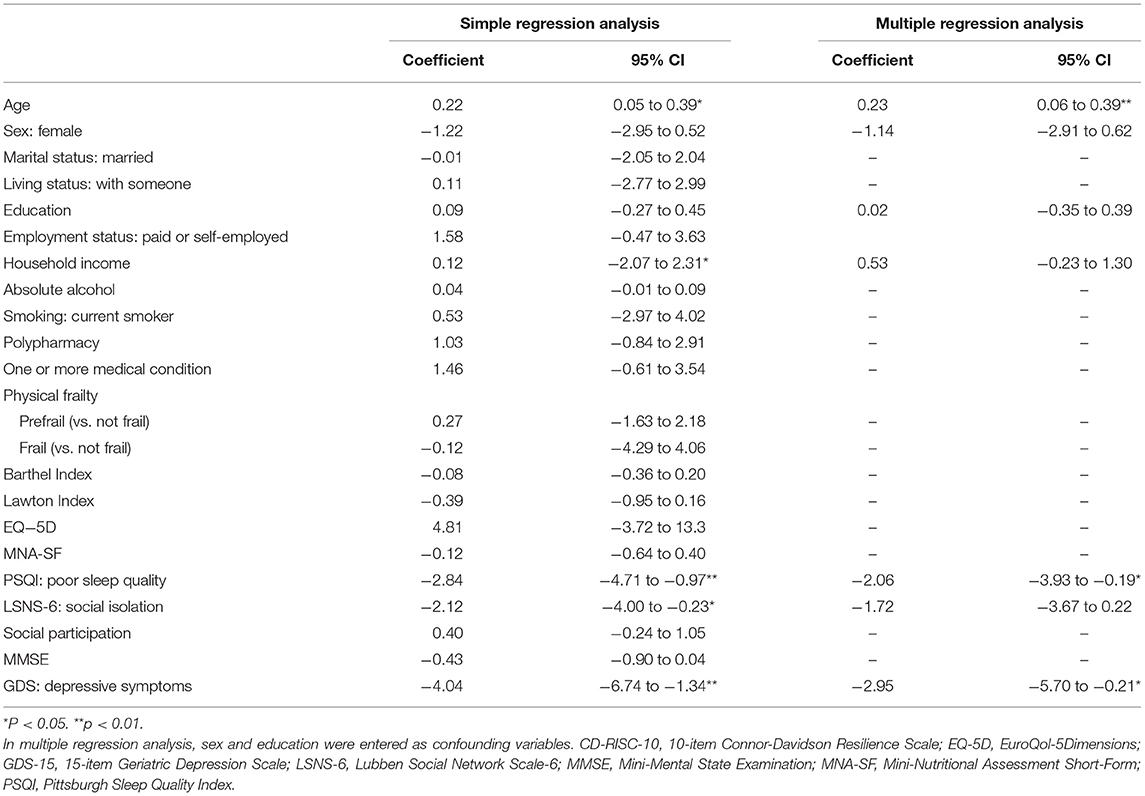
Table 2. Simple and multiple regression analysis results for psychological resilience.
Older adults with MCI had frequent mental health problems during the COVID-19 pandemic (17, 18), psychological resilience is also possibility to be affected, but no previous researchers have investigated the psychological resilience during COVID-19 of older adults who were living with MCI. With the present study, therefore, we clarified psychological resilience in this population, and we identified a number of relevant correlations as below.
The older adults in this study showed a mean CD-RISC-10 score of 23.3 points, which contrasted with scores of 31.7 and 31.1 points in, respectively, adults age 18 or older and older adults who had good cognitive function (16, 37). Researchers who measured resilience with a different test from the CD-RISC-10 found low resilience among older adults with cognitive impairment (11). Moreover, in a previous study during the COVID-19 pandemic, the mean CD-RISC-10 score for older adults was 28.4 points (14). Although we cannot directly compare the mean CD-RISC-10 score from the present study with the scores from previous studies, our findings do suggest lower psychological resilience among older adults with MCI during the pandemic; the mean score in the present study was similar to the mean of 23.6 points that other researchers found for veterans with post-traumatic stress disorder and depression (38). Owing to the nature of cross-sectional studies, we could not describe the pandemic's specific impacts on psychological resilience. However, given that resilience indicates stress coping ability (15, 16), our findings suggest that the major stress from the COVID-19 infection prevention and control measures in Japan put older adults with MCI at high risk for adverse health outcomes.
Many previous researchers reported that psychological resilience was related to age, sex, education level, financial situation, sleep quality, and depressive symptoms (10, 16, 37, 39–41), but we did not find associations with sex or education level. Researchers have reported conflicting results of higher resilience among men, higher resilience among women, and no gender differences (42–44), and other scholars found that higher levels of education were related to higher resilience (16). In our study, participants had a mean education level of 12.5 ± 2.4 years, and the group differences were small, which is likely why we did not find the association between education level and psychological resilience. We also found in the present study an association between high CD-RISC-10 score and older age, which supported earlier findings from reports on psychological resilience and age of higher psychological resilience among older adults than among adults who were middle-aged and younger (10, 39).
Some investigators found significant associations between good sleep quality and high resilience among adults aged 60 years or younger (40, 41), and we also found this significant association. Researchers identified poor sleep quality in respondents with a mean age of 35 during the COVID-19 pandemic (45), and there was another report of increased sleep latency, a component of sleep quality, during the pandemic compared with before (46). It was suggested that people with low psychological resilience are at risk of poor quality during the pandemic.
We also found in the present study a correlation between lower psychological resilience and depressive symptoms, which supported Gerino et al.'s (47), reporting that high resilience contributed to less anxiety and depression. Some people who experience prolonged stress develop psychiatric disorders such as depression, whereas many people can maintain normal psychological functioning through stress, and resilience might be a factor in this normal functioning (48). Researchers found higher prevalence of depressive symptoms among adults during COVID-19 than before (49), and in our study, older adults with depressive symptoms also had low psychological resilience, which would interfere with their coping capacities.
In simple regression analysis in this study, higher household income was related to higher psychological resilience, and social isolation was related to lower resilience. Higher incomes allow for more comfortable and secure lives (50), social ties play a beneficial role in maintaining psychological wellbeing (51), those could be related to higher resilience.
There were some limitations in the present study. First, we collected the data of the CD-RISC-10 for this study between December 2020 and April 2021, but Aichi Prefecture, where NCGG is located, was under a state of emergency from mid-January to February 2021; participants responded to our study questionnaire in different infection statuses, and our analyses did not reflect these differences. In addition, we did not include a control group in the present study, and sampling was not random; therefore, our results have limited generalizability to broader populations. To our advantage, however, we were able to collect data on many older adults with MCI in a short period of time because we recruited from individuals who were already participating in the ongoing J-MINT study. In an additional limitation, we conducted a cross-sectional study, and thus, we could not measure changes in psychological resilience over the course of the pandemic; future study needs to conduct longitudinal investigations of changes in psychological resilience over the course of and following the COVID-19 pandemic.
The World Health Organization declared COVID-19 a pandemic in March 2020, and it is ongoing as of this writing. Because it shows signs that its abatement will be slow, it is and will be necessary for involved stakeholders to attempt to minimize long-range impacts on populations affected. This study suggested particularly impact of psychological resilience on older adults with MCI. We found correlations in this study between sleep quality, depressive symptoms, older age, and psychological resilience, and we expect these findings to be useful in developing interventions to provide ongoing support to older adults with MCI who are at risk of poor mental health outcomes. We also recommend continuous assessment of these older adults to help them maintain optimal sleep quality and minimize their depressive symptoms during COVID-19 pandemic restrictions.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by the NCGG Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
NM and TSu designed the study. NM performed statistical analyses and wrote first draft. NM, TSu, YKu, KU, YKi, HA, and TSa contributed to the interpretation and discussion of results and reviewed the manuscript. All authors contributed to the article and approved the submitted version.
This study was funded by a Hori Sciences and Arts Foundation and Longevity Sciences Grant (Grant Number 22-23) from the NCGG. The funders had no role in the preparation of this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all participants in this study and J-MINT staff for collecting the questionnaires.
1. Nussbaumer-Streit B, Mayr V, Dobrescu AI, Chapman A, Persad E, Klerings I, et al. Quarantine alone or in combination with other public health measures to control Covid-19: a rapid review. Cochrane Database Syst Rev. (2020) 4:CD013574. doi: 10.1002/14651858.CD013574
2. Yamada M, Kimura Y, Ishiyama D, Otobe Y, Suzuki M, Koyama S, et al. effect of the Covid-19 epidemic on physical activity in community-dwelling older adults in Japan: a cross-sectional online survey. J Nutr Health Aging. (2020) 24:948–50. doi: 10.1007/s12603-020-1501-6
3. Noguchi T, Hayashi T, Kubo Y, Tomiyama N, Ochi A, Hayashi H. Association between decreased social participation and depressive symptom onset among community-dwelling older adults: a longitudinal study during the Covid-19 pandemic. J Nutr Health Aging. (2021) 25:1070–5. doi: 10.1007/s12603-021-1674-7
4. Barguilla A, Fernandez-Lebrero A, Estragues-Gazquez I, Garcia-Escobar G, Navalpotro-Gomez I, Manero RM, et al. Effects of Covid-19 pandemic confinement in patients with cognitive impairment. Front Neurol. (2020) 11:589901. doi: 10.3389/fneur.2020.589901
5. Di Santo SG, Franchini F, Filiputti B, Martone A, Sannino S. The effects of Covid-19 and quarantine measures on the lifestyles and mental health of people over 60 at increased risk of dementia. Front Psychiatry. (2020) 11:578628. doi: 10.3389/fpsyt.2020.578628
6. Webb L. Covid-19 lockdown: a perfect storm for older people's mental health. J Psychiatr Ment Health Nurs. (2021) 28:300 doi: 10.1111/jpm.12644
7. Okuyama J, Funakoshi S, Tomita H, Yamaguchi T, Matsuoka H. Longitudinal characteristics of resilience among adolescents: a high school student cohort study to assess the psychological impact of the Great East Japan earthquake. Psychiatry Clin Neurosci. (2018) 72:821–35. doi: 10.1111/pcn.12772
8. Luthar SS, Brown PJ. Maximizing resilience through diverse levels of inquiry: prevailing paradigms, possibilities, and priorities for the future. Dev Psychopathol. (2007) 19:931–55. doi: 10.1017/S0954579407000454
9. Southwick SM, Bonanno GA, Masten AS, Panter-Brick C, Yehuda R. Resilience definitions, theory, and challenges: interdisciplinary perspectives. Eur J Psychotraumatol. (2014) 5:25338. doi: 10.3402/ejpt.v5.25338
10. Gooding PA, Hurst A, Johnson J, Tarrier N. Psychological resilience in young and older adults. Int J Geriatr Psychiatry. (2012) 27:262–70. doi: 10.1002/gps.2712
11. Melendez JC, Satorres E, Redondo R, Escudero J, Pitarque A. Wellbeing, resilience, and coping: are there differences between healthy older adults, adults with mild cognitive impairment, and adults with alzheimer-type dementia? Arch Gerontol Geriatr. (2018) 77:38–43. doi: 10.1016/j.archger.2018.04.004
12. Davydov DM, Stewart R, Ritchie K, Chaudieu I. Resilience and mental health. Clin Psychol Rev. (2010) 30:479–95. doi: 10.1016/j.cpr.2010.03.003
13. Killgore WDS, Taylor EC, Cloonan SA, Dailey NS. Psychological resilience during the Covid-19 lockdown. Psychiatry Res. (2020) 291:113216. doi: 10.1016/j.psychres.2020.113216
14. Shen X, Li Y, Feng J, Lu Z, Tian K, Gan Y. Current status and associated factors of psychological resilience among the Chinese residents during the Coronavirus disease 2019 pandemic. Int J Soc Psychiatry. (2022) 68:34–43. doi: 10.1177/0020764020980779
15. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience scale (CD-RISC). Depress Anxiety. (2003) 18:76–82. doi: 10.1002/da.10113
16. Campbell-Sills L, Forde DR, Stein MB. Demographic and childhood environmental predictors of resilience in a community sample. J Psychiatr Res. (2009) 43:1007–12. doi: 10.1016/j.jpsychires.2009.01.013
17. Tsapanou A, Papatriantafyllou JD, Yiannopoulou K, Sali D, Kalligerou F, Ntanasi E, et al. The impact of Covid-19 pandemic on people with mild cognitive impairment/dementia and on their caregivers. Int J Geriatr Psychiatry. (2021) 36:583–7. doi: 10.1002/gps.5457
18. Goodman-Casanova JM, Dura-Perez E, Guzman-Parra J, Cuesta-Vargas A, Mayoral-Cleries F. Telehealth home support during Covid-19 confinement for community-dwelling older adults with mild cognitive impairment or mild dementia: survey study. J Med Internet Res. (2020) 22:e19434. doi: 10.2196/19434
19. Lehtisalo J, Palmer K, Mangialasche F, Solomon A, Kivipelto M, Ngandu T. Changes in lifestyle, behaviors, and risk factors for cognitive impairment in older persons during the first wave of the coronavirus disease 2019 pandemic in Finland: results from the finger study. Front Psychiatry. (2021) 12:624125. doi: 10.3389/fpsyt.2021.624125
20. Kivipelto M, Mangialasche F, Snyder HM, Allegri R, Andrieu S, Arai H, et al. World-wide fingers network: a global approach to risk reduction and prevention of dementia. Alzheimers Dement. (2020) 16:1078–94. doi: 10.1002/alz.12123
21. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-Davidson Resilience scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. (2007) 20:1019–28. doi: 10.1002/jts.20271
22. Sugimoto T, Sakurai T, Akatsu H, Doi T, Fujiwara Y, Hirakawa A, et al. The Japan-Multimodal intervention trial for prevention of dementia (J-MINT): the study protocol for an 18-month, multicenter, randomized, controlled trial. J Prev Alzheimers Dis. (2021) 8:465–76. doi: 10.14283/jpad.2021.29
23. Makizako H, Shimada H, Park H, Doi T, Yoshida D, Uemura K, et al. Evaluation of multidimensional neurocognitive function using a tablet personal computer: test-retest reliability and validity in community-dwelling older adults. Geriatr Gerontol Int. (2013) 13:860–6. doi: 10.1111/ggi.12014
24. Shimada H, Makizako H, Park H, Doi T, Lee S. Validity of the national center for geriatrics and gerontology-functional assessment tool and mini-mental state examination for detecting the incidence of dementia in older Japanese adults. Geriatr Gerontol Int. (2017) 17:2383–8. doi: 10.1111/ggi.13079
25. Folstein MF, Folstein SE, McHugh PR. “Mini-Mental State”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-395690026-6
26. Palmer K, Onder G. Comprehensive geriatric assessment: benefits and limitations. Eur J Intern Med. (2018) 54:e8–9. doi: 10.1016/j/ejim.2018.02.016
27. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. (2001) 56:M146–56. doi: 10.1093/gerona/56.3.m146
28. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. (1965) 14:61–5. doi: 10.1037/t02366-000
29. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. (1969) 9:179–86. doi: 10.1093/geront/9.3_Part_1.179
30. Kunz S. Psychometric properties of the EQ-5D in a study of people with mild to moderate dementia. Qual Life Res. (2010) 19:425–34. doi: 10.1007/s11136-010-9600-1
31. Rubenstein LZ, Harker JO, Salvà A, Guigoz Y, Vellas B. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol A Biol Sci Med Sci. (2001) 56:M366–72. doi: 10.1093/gerona/56.6.m366
32. Buysse DJ, Reynolds CF. 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric. practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
33. Lubben J, Blozik E, Gillmann G, Iliffe S, von Renteln Kruse W, Beck JC, et al. Performance of an abbreviated version of the lubben social network scale among three European community-dwelling older adult populations. Gerontologist. (2006) 46:503–13. doi: 10.1093/geront/46.4.503
34. Kanamori S, Kai Y, Aida J, Kondo K, Kawachi I, Hirai H, et al. Social participation and the prevention of functional disability in older Japanese: the JAGES cohort study. PLoS ONE. (2014) 9:e99638. doi: 10.1371/journal.pone.0099638
35. Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. (1982) 17:37–49. doi: 10.1016/0022-3956(82)90033-4
36. Sugishita K, Sugishita M, Hemmi I, Asada T, Tanigawa T, A. Validity and reliability study of the Japanese version of the geriatric depression scale 15 (GDS-15-J). Clin Gerontol. (2017) 40:233–40. doi: 10.1080/07317115.2016.1199452
37. Tourunen A, Siltanen S, Saajanaho M, Koivunen K, Kokko K, Rantanen T. Psychometric properties of the 10-item Connor-Davidson resilience scale among Finnish older adults. Aging Ment Health. (2021) 25:99–106. doi: 10.1080/13607863.2019.1683812
38. Wingo AP, Briscione M, Norrholm SD, Jovanovic T, McCullough SA, Skelton K, et al. Psychological resilience is associated with more intact social functioning in veterans with post-traumatic stress disorder and depression. Psychiatry Res. (2017) 249:206–11. doi: 10.1016/j.psychres.2017.01.022
39. Terrill AL, Molton IR, Ehde DM, Amtmann D, Bombardier CH, Smith AE, et al. Resilience, age, and perceived symptoms in persons with long-term physical disabilities. J Health Psychol. (2016) 21:640–9. doi: 10.1177/1359105314532973
40. Liu X, Liu C, Tian X, Zou G, Li G, Kong L, et al. Associations of perceived stress, resilience and social support with sleep disturbance among community-dwelling adults. Stress Health. (2016) 32:578–86. doi: 10.1002/smi.2664
41. Lee SJ, Park CS, Kim BJ, Lee CS, Cha B, Lee YJ, et al. Association between morningness and resilience in Korean college students. Chronobiol Int. (2016) 33:1391–9. doi: 10.1080/07420528.2016.1220387
42. Hardy SE, Concato J, Gill TM. Resilience of community-dwelling older persons. J Am Geriatr Soc. (2004) 52:257–62. doi: 10.1111/j.1532-5415.2004.52065.x
43. MacLeod S, Musich S, Hawkins K, Alsgaard K, Wicker ER. The impact of resilience among older adults. Geriatr Nurs. (2016) 37:266–72. doi: 10.1016/j.gerinurse.2016.02.014
44. Wells M. Resilience in rural community-dwelling older adults. J Rural Health. (2009) 25:415–9. doi: 10.1111/j.1748-0361.2009.00253.x
45. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during Covid-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. (2020) 288:112954. doi: 10.1016/j.psychres.2020.112954
46. Targa ADS, Benitez ID, Moncusi-Moix A, Arguimbau M, de Batlle J, Dalmases M, et al. Decrease in sleep quality during Covid-19 outbreak. Sleep Breath. (2021) 25:1055–61. doi: 10.1007/s11325-020-02202-1
47. Gerino E, Rolle L, Sechi C, Brustia P. Loneliness, resilience, mental health, and quality of life in old age: a structural equation model. Front Psychol. (2017) 8:2003. doi: 10.3389/fpsyg.2017.02003
48. Han MH, Nestler EJ. Neural substrates of depression and resilience. Neurotherapeutics. (2017) 14:677–86. doi: 10.1007/s13311-017-0527-x
49. Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM, Galea S. Prevalence of depression symptoms in US adults before and during the Covid-19 pandemic. JAMA Netw Open. (2020) 3:e2019686. doi: 10.1001/jamanetworkopen.2020.19686
50. Wagnild G. Resilience and successful aging. comparison among low and high income older adults. J Gerontol Nurs. (2003) 29:42–9. doi: 10.3928/0098-9134-20031201-09
Keywords: older adults, mild cognitive impairment, psychological resilience, CD-RISC-10, COVID-19, sleep quality, depressive symptoms
Citation: Matsumoto N, Sugimoto T, Kuroda Y, Uchida K, Kishino Y, Arai H and Sakurai T (2022) Psychological Resilience Among Older Japanese Adults With Mild Cognitive Impairment During the COVID-19 Pandemic. Front. Psychiatry 13:898990. doi: 10.3389/fpsyt.2022.898990
Received: 18 March 2022; Accepted: 19 May 2022;
Published: 10 June 2022.
Edited by:
Gustavo Sevlever, Fundación Para la Lucha Contra las Enfermedades Neurológicas de la Infancia (FLENI), ArgentinaReviewed by:
Prateek Varshney, National Institute of Mental Health and Neurosciences (NIMHANS), IndiaCopyright © 2022 Matsumoto, Sugimoto, Kuroda, Uchida, Kishino, Arai and Sakurai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Takashi Sakurai, dHNha3VyYWlAbmNnZy5nby5qcA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.