 Dongyan Ding
Dongyan Ding Mengna Zheng
Mengna Zheng- School of Educational Science, Anhui Normal University, Wuhu, China
The previous research showed contradictions in the relationships between psychological flexibility processes and functioning. This meta-analysis is the first to provide a comprehensive meta-analysis of the associations between six core processes of psychological flexibility and functioning among chronic pain patients. Four databases were searched (PsycINFO; PubMed; CINAHL; Web of Science) along with reference lists. Thirty-six cross-sectional studies were included (7,812 chronic pain patients). A three-level meta-analytic model was used to examine the associations. The publication bias was assessed with the Egger test, funnel plot, and p-curve analysis. Significant associations were found between functioning and six processes of psychological flexibility (i.e., acceptance, defusion, present moment, committed action, self as context, and values). Except for the relationship between defusion and functioning, the relationships between the other five psychological flexibility processes and functioning were all moderated by domains of functioning. No moderators were found regarding age, percentage of females, country, or type of instrument used to measure functioning. These findings may carry significant implications for chronic pain patients and clinical workers. It might be more effective to focus on functioning-related psychological flexibility processes rather than all therapy packages if the relationships between functioning and specific processes of psychological flexibility were better informed. Limitations were also discussed.
Introduction
Chronic pain is one of the most common physical problems all over the world in the general population (1–3) and is a source of distress and disability that affects all aspects of a patient’s life (4, 5). Furthermore, individuals in a state of psychological distress experience more intense pain, leading to a reciprocal reinforcement between psychological distress and pain (5, 6). Chronic pain also costs economically higher than other diseases (4), leading to immense suffering for their families and high costs on our communities and healthcare systems (7).
Traditional pain management has been focused mainly on reducing pain and pain-related distress, with pain interference (i.e., functional impairment) being a neglected dimension (8). In treating chronic pain, recent research supports the view that a critical issue concerns the changes necessary to improve physical and psychological functioning (8, 9). One of these views comes from acceptance and commitment therapy (ACT), which defends a greater focus on functioning, and encourages patients to engage with valued activities and meaningful areas even when pain and distress persist (9, 10).
The expressed goal of ACT is to increase behaviors in the direction of functionality by increasing psychological flexibility (11, 12). Psychological flexibility refers to an individual’s ability to focus on the present moment, move toward their goals, and persist or change behaviors to serve valued ends (13–15). Actually, the psychological flexibility model of ACT can be seen as a basis for an integrated and progressive psychological approach to chronic pain management (16). This model fully integrates cognitive and environmental influences as the core processes of healthy and problem behaviors (16). As suggested by the psychological flexibility model, pain and suffering are inherent aspects of human life, and the psychological function of pain is central to the analysis (8). It means that a behavioral response is not directly related to the level of pain intensity but rather to its function or meaning for the individual in that particular context (8). Thus, individual functional behavior can be increased by improving psychological flexibility. Actually, many researchers suggested that ACT is more effective than controls (except CBT) in improving functional impairment or increasing values-congruent behaviors (17–19).
The previous studies with chronic pain patients have supported the role of the various components of psychological flexibility in reducing disability and functional impairment (20, 21). However, different results also appeared in different studies for the exact relationship between outcome variables. For example, some studies showed that the magnitude of the correlation coefficient between acceptance and functioning was small (22) or medium (23, 24), while in other studies, the effect sizes were large (25, 26). These discrepancies can also be found in the relationship between functioning and other psychological flexibility processes (27, 28). It is worth noting that most studies examining the relationship between psychological flexibility and functioning take psychological flexibility or functioning as a whole. However, the psychological flexibility model is comprised of six core ACT processes, i.e., acceptance, defusion, present moment, self as context, committed action, and values (15). All these six components may have a particular relationship with the functioning of patients with chronic pain. Specifically, acceptance is defined as acknowledging and experiencing unwanted thoughts and feelings without having to follow, reduce, or alter them and has been linked to better functioning in chronic pain patients (29, 30). For chronic pain patients, defusion involves learning to distance themself from pain and distress in order to reduce the influence of these experiences on behavior. The present moment entails flexible awareness and non-judgmental contact with ongoing events. Self as context entails an experience of taking a perspective from which to observe one’s psychological experiences without attachment to them or an investment in which particular experiences occur. Values are chosen qualities of purposive action that we want to achieve and reflect in our behavior. Committed action is the ability to flexibly persist in actions guided by values (15, 31). These six core processes can be fostered in the ACT by different exercises. From the view of the psychological flexibility model, chronic pain patients can relieve the psychological burden or improve their psychological functioning through accepting inner experiences, being mindful, and participating in actions that are aligned with individual goals and values (2, 32). Likewise, many researches have classified functioning into physical and psychological functioning (7, 33). Physical functioning is made up of independent ambulation, mobility, and body care and movement scales, while the psychosocial domain is made up of social interaction, alertness, emotional behavior, and communication (7, 33).
To date, no study makes a comprehensive meta-analysis of the relationship between specific mechanisms of psychological flexibility (e.g., acceptance, defusion, present moment, self as context, committed action, and values) and different domains of functioning. Many current researches examined the relationship between psychological flexibility and function without considering their sub-domains. Some researchers thought it is necessary to find which components of therapy work for which type of patient on which outcome/s and try to understand why (34). It would be hard to understand the mechanisms of psychological flexibility for functioning if we take psychological flexibility as a whole. The science and core clinical competencies of ACT also require the understanding of process-based therapy, which refers to contextually specific evidence-based processes associated with evidence-based procedures (35, 36). And the call for process-based therapy suggested that focusing on specific change processes could provide evidence-based methods and make the therapies person-centered to enhance particular people’s physical and psychological health more efficiently (35, 36). A meta-analysis of this subject is essential to understand the basic psychological processes underlying the functioning, which would consequentially form the basis for more robust testing of causal and manipulable relationships. Suppose we knew which process of psychological flexibility is more closely related to the domains of functioning. In that case, we could provide targeted intervention services to chronic pain patients to improve their functioning. Thus, it may have important implications for healthcare professionals, organizations, and patient care.
As suggested by the psychological flexibility model, increased psychological flexibility is not intended to reduce pain intensity, while the psychological function of pain is central to the analysis (8). Therefore, we hypothesize that the components of psychological flexibility may be more relevant to psychological functioning than to physical functioning. Besides, some studies suggested associations between psychological factors and functioning may be influenced by culture (37). Hence, we assumed that culture might be a moderating variable. We also considered age and the proportion of females as moderators.
The primary aim of this review was to identify and integrate all published findings on associations between different processes of psychological flexibility and domains of functioning, and address an analytic question about the magnitude and direction of the associations among chronic pain patients. A second aim is to determine which variables potentially moderate the relationships. We hypothesized that the following five moderators would systematically influence the effect: (1) the domain of functioning, (2) the age of the target sample, (3) the country, (4) the proportion of females, and (5) the type of measurements of functioning. A third research goal is to address descriptive questions about how these variables are being measured for chronic pain.
Materials and Methods
Selection of Studies
The meta-analysis was reported following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement (38).
The first author conducted a search using PsycINFO, PubMed, CINAHL, and Web of Science, all of which were searched on October 1, 2021, and updated on May 27, 2022. No date restrictions were applied to the search to maximize the search strategy. Because acceptance and value are wide-ranging, this study mainly uses instruments that measure them instead of these constructs. Other instruments commonly used to measure psychological flexibility processes were also used in order to minimize potential publication bias. The main search terms used included keywords and free words: [(Acceptance Questionnaire) OR (Valued Living Questionnaire) OR (Chronic Pain Values Inventory) OR (Valuing Questionnaire) OR (Personal Values Questionnaire) OR (Mindful Attention Awareness Scale) OR (Mindfulness) OR (Avoidance and Fusion Questionnaire) OR (Thought Suppression Inventory) OR (Automatic Thought Questionnaire) OR (present moment) OR (committed action) OR (self-as-context) OR (cognitive defusion) OR (psychological inflexibility) OR (psychological flexibility)] AND (functioning OR dysfunction OR (pain disability) OR (pain interference)] AND [(chronic pain) OR fibromyalgia). In addition, reference lists of eligible studies and relevant review articles, as well as relevant meta-analyses were manually searched to minimize potential publication bias.
Inclusion Criteria
(a) The sample population included chronic pain patients and fibromyalgia patients;
(b) One of six core processes of psychological flexibility was measured as well as the functioning (i.e., psychological functioning and/or physical functioning) of the patients.
(c) The relationship between processes of psychological flexibility and functioning was reported with Pearson’s r correlation coefficient.
Exclusion Criteria
(a) Review, meta-analysis, or theoretical articles;
(b) Without reporting Pearson’s r correlation coefficient.
Difficulties in deciding the selection were discussed between the two authors. According to the criteria, any ambiguity about studying eligibility was settled via discussion, and a full consensus was reached between the two authors.
Data Extraction and Coding
Data extraction was performed by the first author and checked by the second author. If there were disagreements, agreements would be reached through a full consultation. Extracted data include: authors and year of publication, country, instruments used to measure processes of psychological flexibility and functioning, study characteristics (e.g., sample size, mean age, and percentage of females), and effect sizes.
According to the authors’ definition, processes flexibility was coded as belonging to the six dimensions, i.e., acceptance, defusion, present moment, self as context, committed action, and values. Functioning was coded as three domains, i.e., psychological, physical, and overall functioning. When the total functioning score was used, and psychological or physical functioning was not reported, it would then be classified under the “overall functioning” heading. Besides psychological functioning, emotional and social functioning were also coded as psychological functioning. Physical functioning was coded as physical functioning.
We created three dummy variables for domains of functioning: psychological functioning, physical functioning, and overall functioning. The value 1 in these dummy variables is indicative of the specific type of functioning being applicable, whereas the value 0 indicates that the specific type of functioning is not applicable. We also created dummy variables for the type of the measurements of functioning. If the measurement was used only in one effect size, it would be coded as “other” to reduce the number of dummy variables. These dummy variables are mutually exclusive. Directions of these effects were adjusted accordingly within each study. For example, the direction of the relationship between acceptance and dysfunction would be reversely coded to represent the relationship between acceptance and functioning.
Data Analysis
In the present study, a three-level meta-analytic model was used to synthesize effect sizes and conduct moderator analyses to achieve maximum statistical power (39). The three-level model examined three sources of variance: sampling variance of the observed effect sizes (Level 1); variance between effect sizes from the same study (Level 2); and variance between studies (Level 3) (39, 40). Some scholars have noted that heterogeneity can be considered substantial if less than 75% of the total variance can be attributed to level 1 (41). Therefore, potential moderating effects that may impact the overall effect will be examined according to the 75% rule.
When a study reported multiple effect sizes due to the multiple instruments used to assess the same construct, all relevant effect sizes would be extracted so that we could control for within-study dependency without reducing the number of effect sizes available in the literature (39). All analyses were conducted in R version 4.1.2 (42), using the meta and metafor package (39). The R syntax was written following related tutorials (41, 43). All model parameters were estimated using the restricted maximum likelihood method.
Due to differences in measurement tools, the effect sizes were analyzed using the random-effects model. Individual study effect sizes (r and rs) and sample sizes were entered to calculate pooled effect size estimates (r). All extracted effects were converted to Fisher’s Z-values and weighted by sample size before analysis. These effects were then meta-analyzed, and the results were subsequently converted back to correlations for interpretation (44). In accordance with Cohen’s convention, the magnitude of effect for r is classified as small (0.10), medium (0.30), or large (0.50) with 95% CI.
The heterogeneity among the results was tested by the Q test and the I2 test (45, 46). If I2 > 50%, it is considered to have moderate-to-high heterogeneity. Egger test and funnel plot assessed the possibility of publication bias, with significant publication bias as p < 0.1 (45). When it revealed possible publication bias, trim and fill analyses were performed to provide an adjusted average effect size (47) to correct. P-curve analysis was also used to detect selective reporting (48, 49). The p-curve method is based on the distribution of significant p-values of a set of findings. If an actual effect exists, it will skew to the right or the left if selective reporting is prevalent (48, 49).
Results
Description of Studies
Studies Characteristics
Initially, 1,759 citations were identified through searches of electronic bibliographic databases and reference lists. After detecting duplicates and screening titles and abstracts for relevance, 134 articles were identified as potentially eligible for further assessment. After reading the full text of each article, 36 studies met the criteria and were included in this study (see Figure 1 for the details).
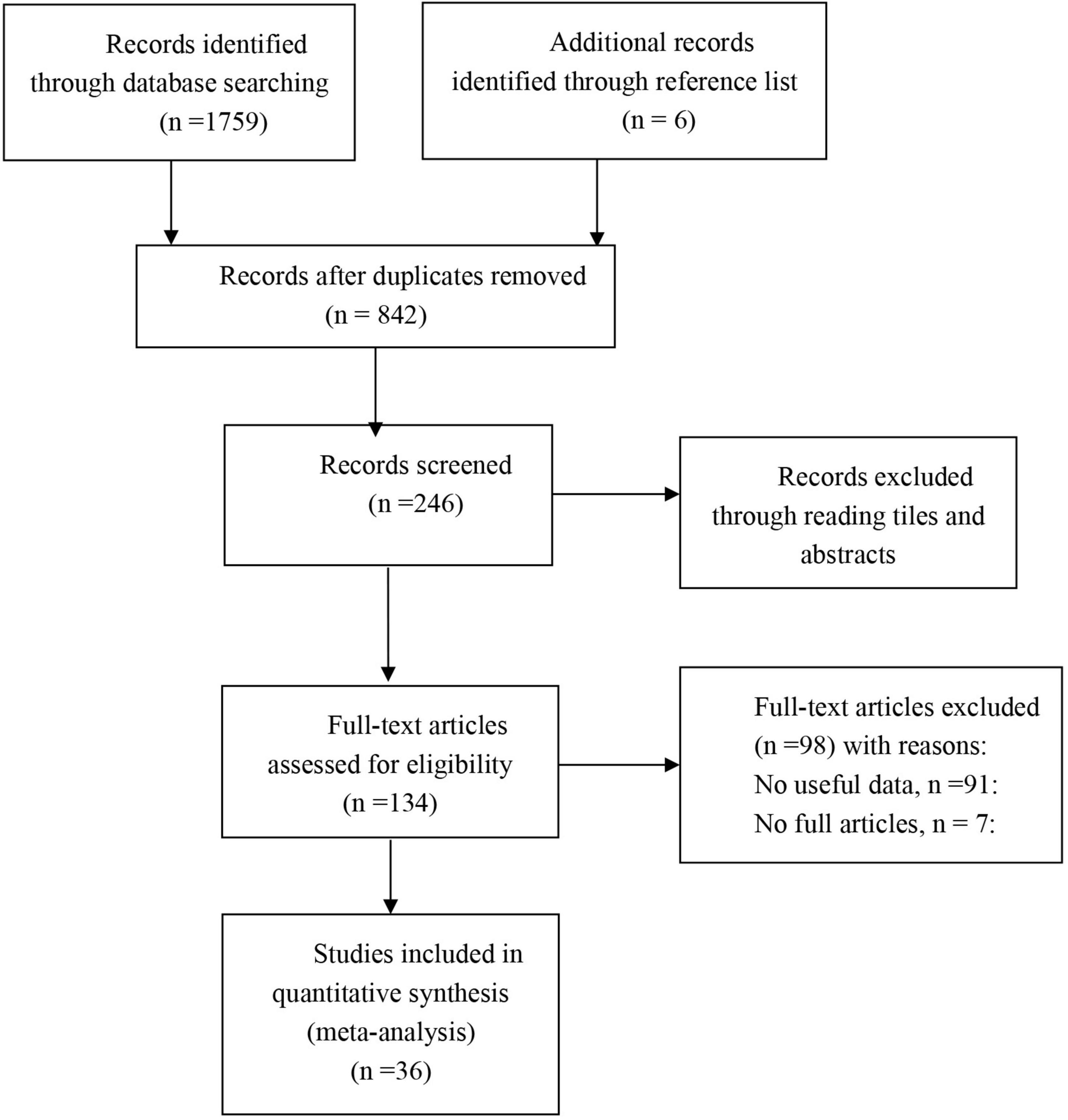
Figure 1. Study flow diagram.
The characteristics of the 36 included studies were summarized in Table 1, from which a total of 109 correlations could be extracted. Sample sizes for included studies ranged from 23 to 555 (total participants = 7,812). Among them, 15 studies were from the United Kingdom, six studies from the United States, four from Spain, Australia, and Sweden, one from Portugal, Singapore, Belgium, Republic of Cyprus, and multi-country (i.e., United States (30.1%), Ireland (30.1%), England (21.13%)]. The mean age of participants in these studies ranged from 14.44 to 69.3. There were 763 adolescents, and most participants were adults (97.67%). The proportion of females ranged from 39.2 to 100%.
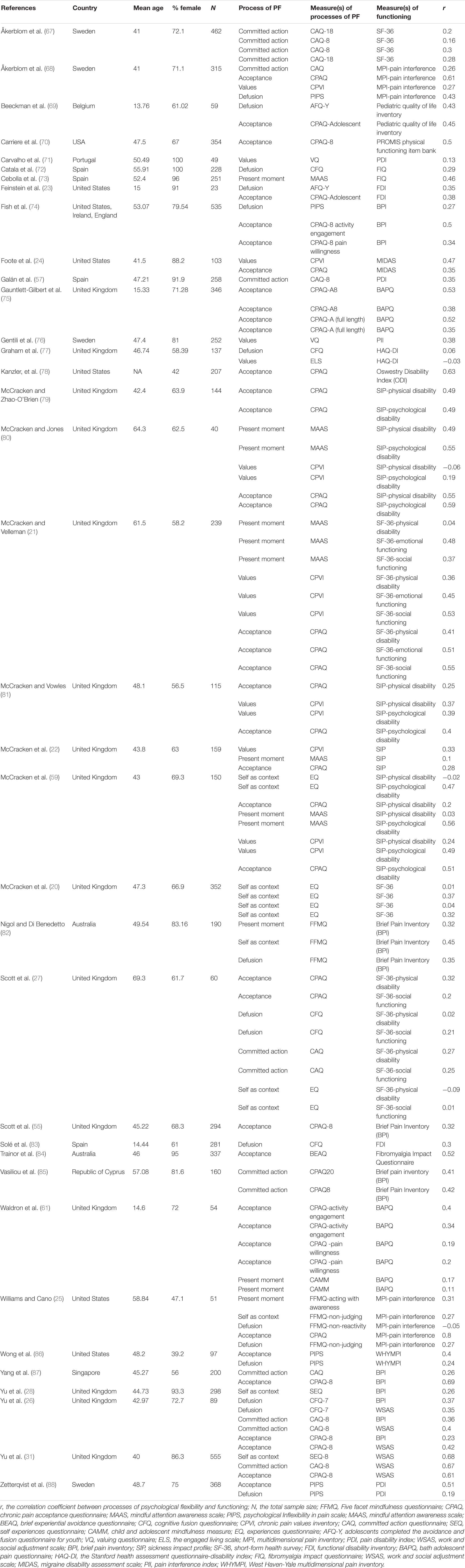
Table 1. Study characteristics and effect size.
The Measurements
Acceptance was measured with the Chronic Pain Acceptance Questionnaire (CPAQ) and Psychological Inflexibility in Pain Scale (PIPS). Committed action was measured with the Committed Action Questionnaire (CAQ). Cognitive defusion was measured with the Cognitive fusion questionnaire (CFQ), subscales of PIPS, the Avoidance and Fusion Questionnaire for Youth (AFQ-Y), and subscales of the Five Facet Mindfulness Questionnaire (FFMQ). The present moment was measured with the Mindful attention awareness scale (MAAS), the Child and Adolescent Mindfulness Measure (CAMM), and subscales of FFMQ (i.e., acting with awareness). Self as context was measured with Experiences Questionnaire (EQ), Self-experiences questionnaire (SEQ), and FFMQ-non-judgment (50). Values were measured with the Chronic Pain Values Inventory (CPVI), the Valuing Questionnaire (VQ), and the Engaged living scale (ELS).
Functional impairment mainly was measured with the Brief Pain Inventory-functional impairment subscale (BPI), Sickness Impact Profile (SIP), Short-Form Health Survey (SF-36), Pain Disability Index (PDI), Functional Disability Inventory (FDI), Fibromyalgia impact questionnaire (FIQ), and Multidimensional Pain Inventory (MPI).
Meta-Analyses
Acceptance and Functioning
Aggregating across 39 correlations in 24 studies that examined the relationship between acceptance and functioning, the overall effect size was statistically significant and medium to large (r = 0.48, 95% CI = 0.42, 0.54, p < 0.001; I2 = 83.89%, Q = 198.83, df = 38, p < 0.001). The results were presented in a forest plot in Figure 2.
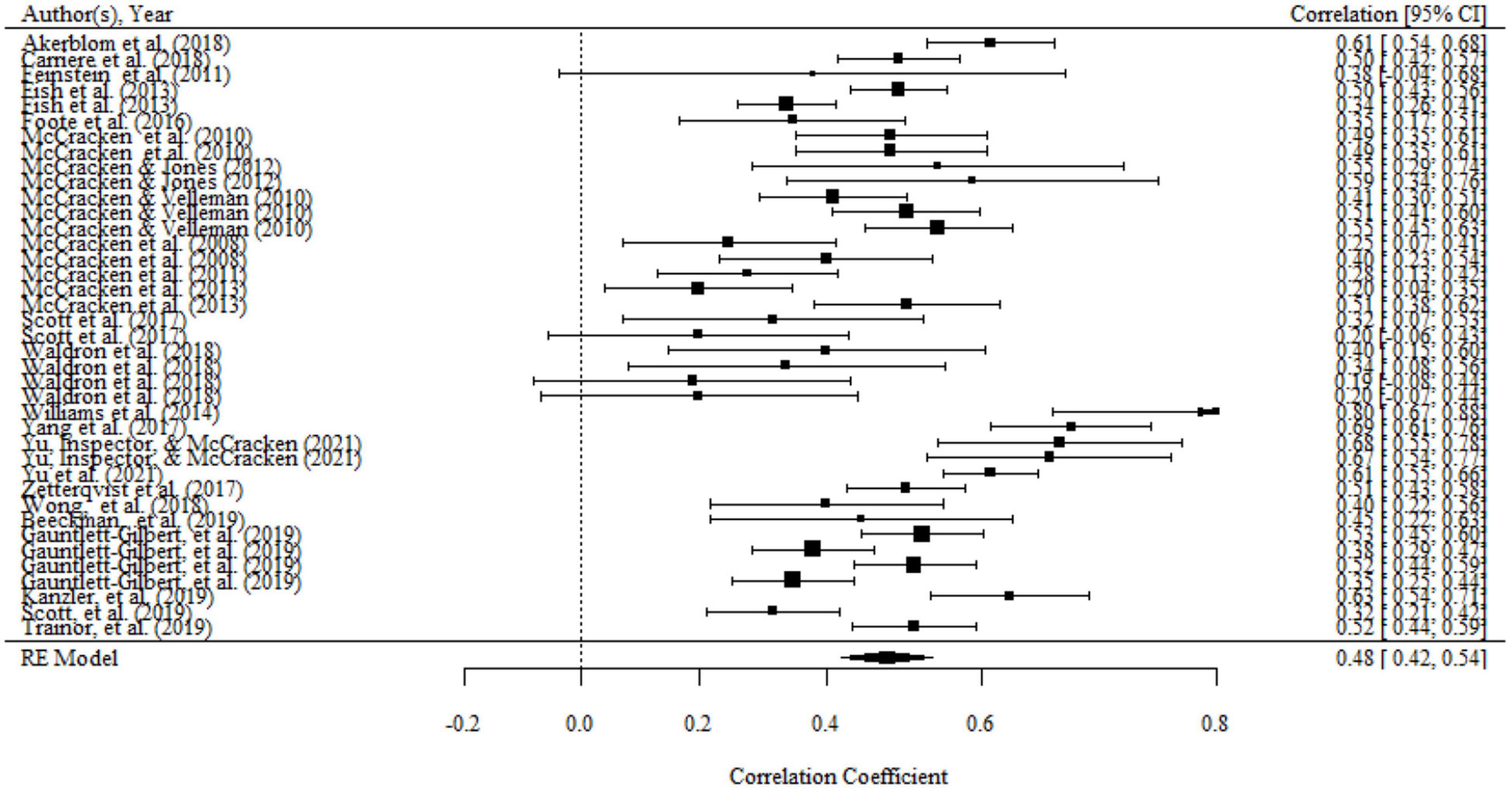
Figure 2. Forest plot of effect size (r) for the relationship between acceptance and functioning.
There were significant variances within the same studies (i.e., level 2 variance) and between studies (i.e., level 3 variance). The details can be seen in Table 2. Therefore, moderator analyses were conducted in order to determine variables that can explain level 2 and level 3 variance. Moderating effects of mean age, percentage of females, country, domains of functioning, and type of measurements of functioning have been evaluated separately in univariate models. We found a significant moderating effect of the domains of functioning on the association, as shown by the results of the omnibus test (F(2,36) = 6.63, p < 0.01). The mean effect of association between acceptance and overall functioning (r = 0.59, 95% CI = 0.49, 0.69, p < 0.001) and psychological functioning (r = 0.52, 95% CI = 0.40, 0.64, p < 0.001) were both significantly larger than that association of acceptance and physical functioning (r = 0.38, 95% CI = 0.22, 0.53, p < 0.01). However, there was no significant difference in the association between acceptance and psychological functioning and overall functioning. No significant moderating effects were found for the percentage of females, mean age, country, and type of functioning measurements.
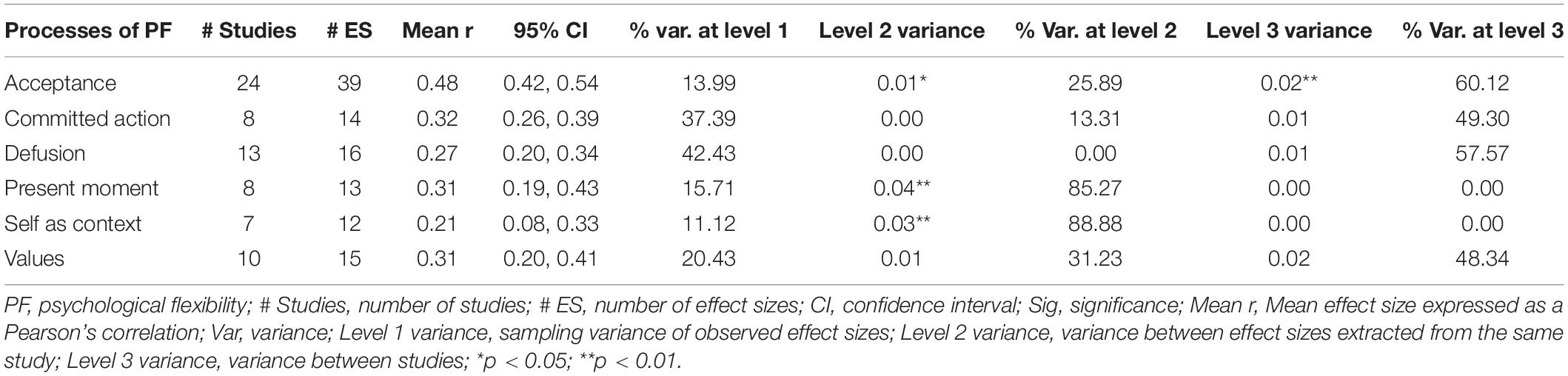
Table 2. Results for the overall mean effect sizes of the relationship between six processes and functioning.
There was no publication bias in Egger tests and Funnel plot (p > 0.1) on the relationship between acceptance and functioning. Both the full p-curve and the half p-curve test were significant with p < 0.0001 (Z = −31.74, Z = −30.62), which indicated that the distribution of p-values is significant right-skewed, as seen in Figure 3. Hence, the results further support the initial assessment that evidential value is present in the literature.
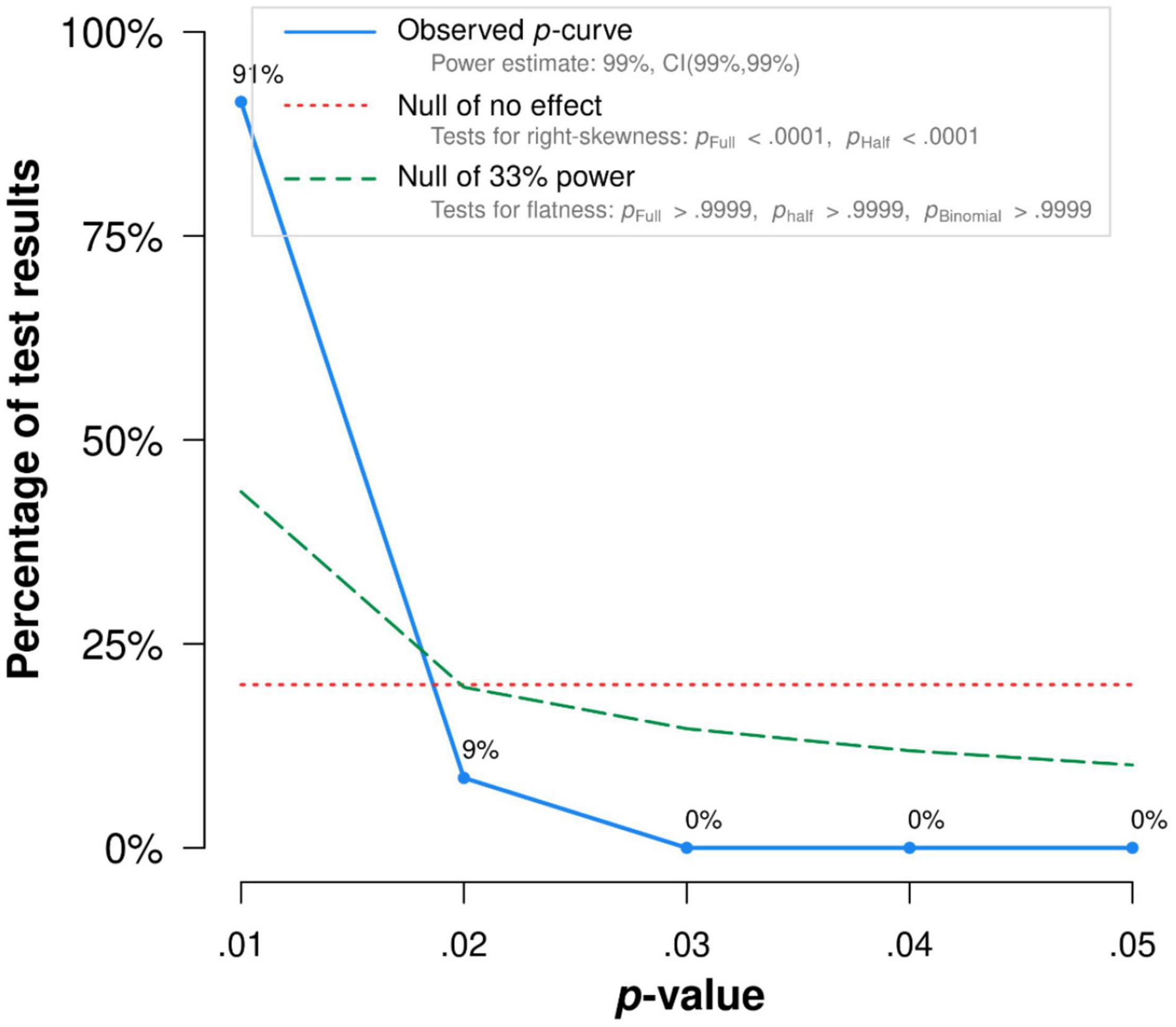
Figure 3. The p-Curve for statistically significant results on the relationship between acceptance and functioning. The observed p-curve includes 35 statistically significant (p < 0.05 results, of which 35 are p < 0.025. There were four additional results entered but excluded from p-curve because they were p > 0.05.
Committed Action and Functioning
Aggregating across 14 correlations that examined the relationship between committed action and functioning, the overall effect size was statistically significant and medium (r = 0.32, 95% CI = 0.26, 0.39, p < 0.001; I2 = 61.20%, Q = 35.04, df = 14, p < 0.01). The results were presented in a forest plot in Figure 4.
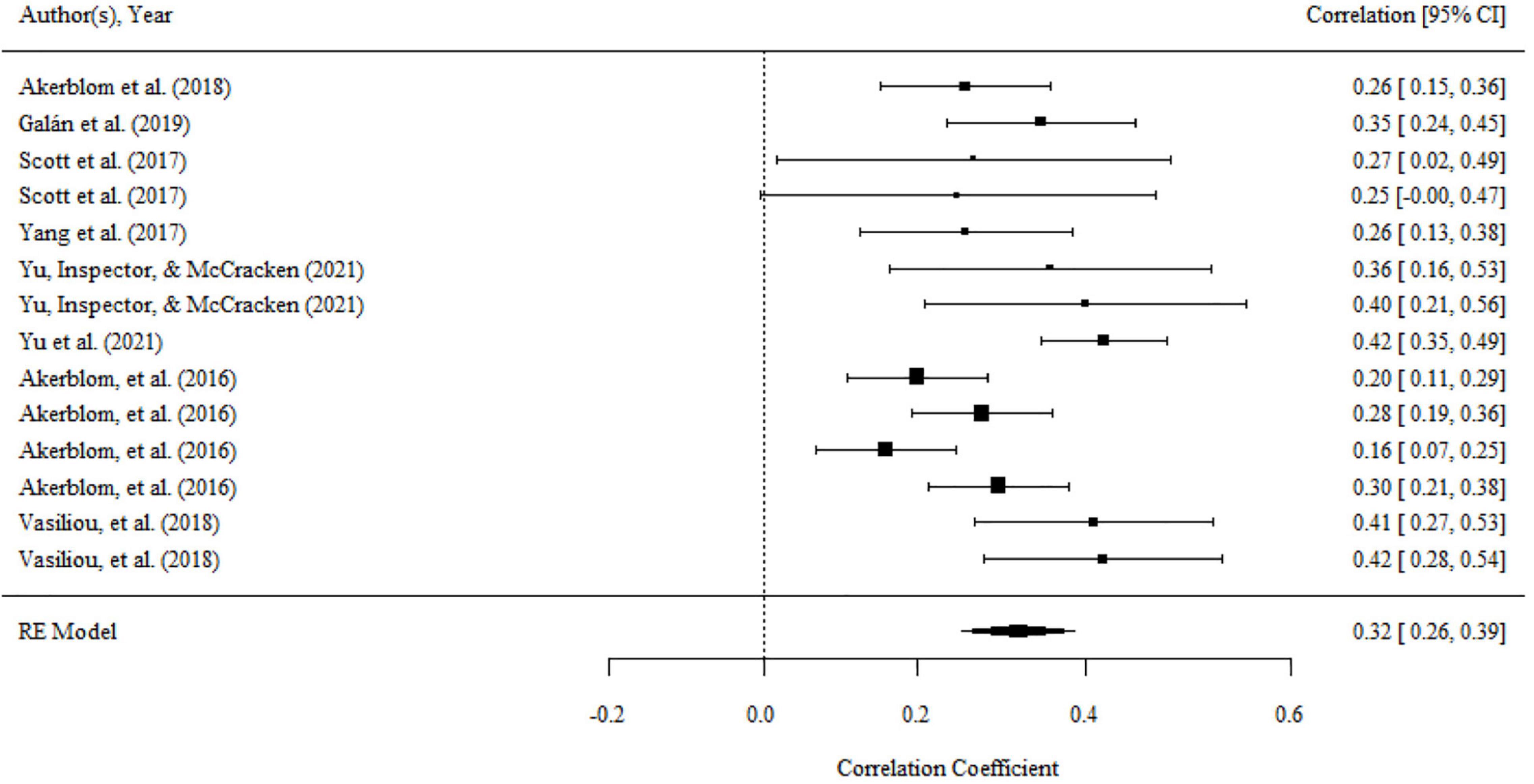
Figure 4. Forest plot of effect size (r) for the relationship between committed action and functioning.
There were no significant variances within level 2 and level 3. However, the variance within level 1 was less than 75% (i.e., 37.39), then moderator analyses were conducted. We found a significant moderating effect of the domains of functioning on the association, as shown by the results of the omnibus test (F(2,11) = 4.01, p < 0.05). The relationship of committed action with overall functioning (r = 0.38, 95% CI = 0.31, 0.45, p < 0.001) was significantly larger than that with psychological functioning (r = 0.24, 95% CI = 0.13, 0.34, p < 0.001). but there was no significant difference between the mean effect of overall functioning and physical functioning (r = 0.25, 95% CI = 0.14, 0.35, p < 0.001). The domain of functioning was the main source of heterogeneity. After it was included to analysis, the heterogeneity was significantly reduced (Q = 17.32, df = 11, p > 0.05).
There was no publication bias in Egger tests and Funnel plot (p > 0.1) on the relationship between acceptance and functioning. Both the full p-curve and the half p-curve test were significant with p < 0.0001 (Z = −14.19, Z = −14.29), which indicated that the distribution of p-values is significant right-skewed, as seen in Figure 5. Hence, the results further support the initial assessment that evidential value was present in the literature.
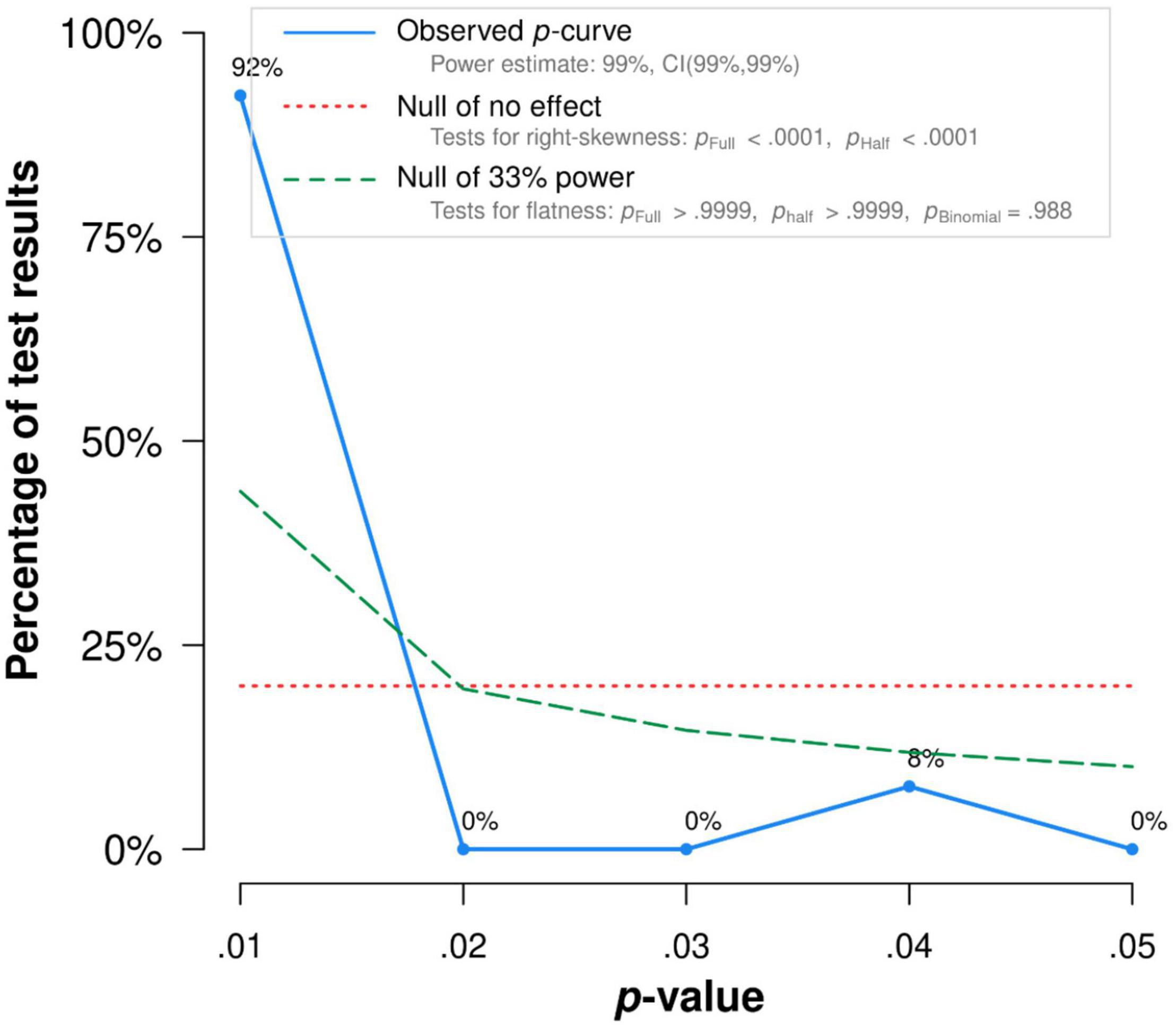
Figure 5. The p-Curve for statistically significant results on the relationship between committed action and functioning. The observed p-curve includes 13 statistically significant (p < 0.05) results, of which 12 are p < 0.025. There was one additional result entered but excluded from p-curve because it was p > 0.05.
Defusion and Functioning
Aggregating across 16 correlations in 13 studies that examined the relationship between defusion and functioning, the overall effect size was statistically significant and nearly medium (r = 0.27, 95% CI = 0.20, 0.34, p < 0.001; I2 = 57.66%, Q = 34.07, df = 15, p < 0.01). The results were presented in a forest plot in Figure 6.
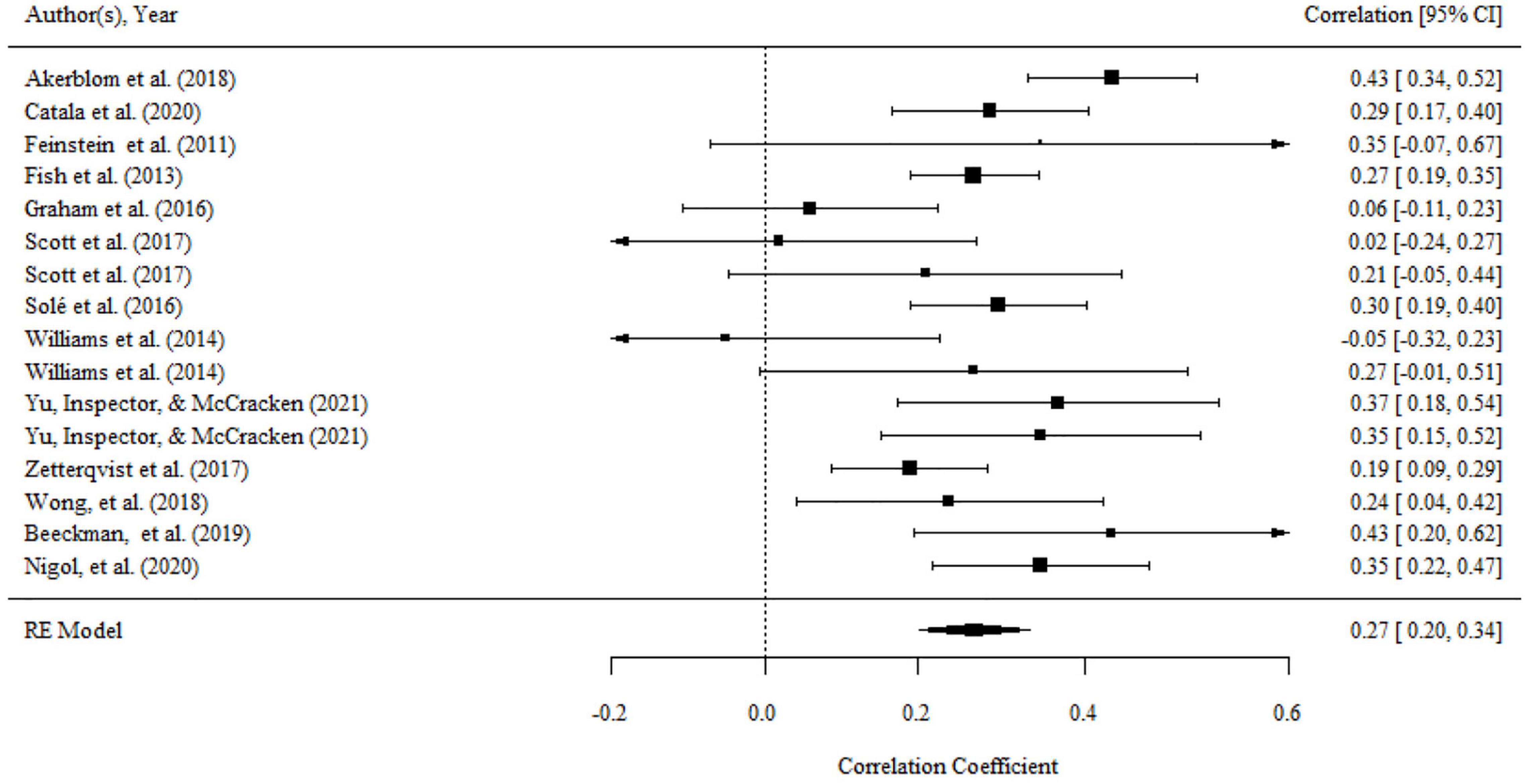
Figure 6. Forest plot of effect size (r) for the relationship between defusion and functioning.
There was no significant variance within level 2 and level 3. Moderating effects of mean age, percentage of females, country, domains of functioning, and type of functioning measurements did not exist for the relationship between defusion and functioning.
There was no publication bias in Egger tests and Funnel plot (p > 0.1) on the relationship between acceptance and functioning. Both the full p-curve and the half p-curve test were significant with p < 0.0001 (Z = −10.82, Z = −10.32), which indicated that the distribution of p-values is significant right-skewed as seen in Figure 7. Hence, the results further support the initial assessment that evidential value is present in the literature.
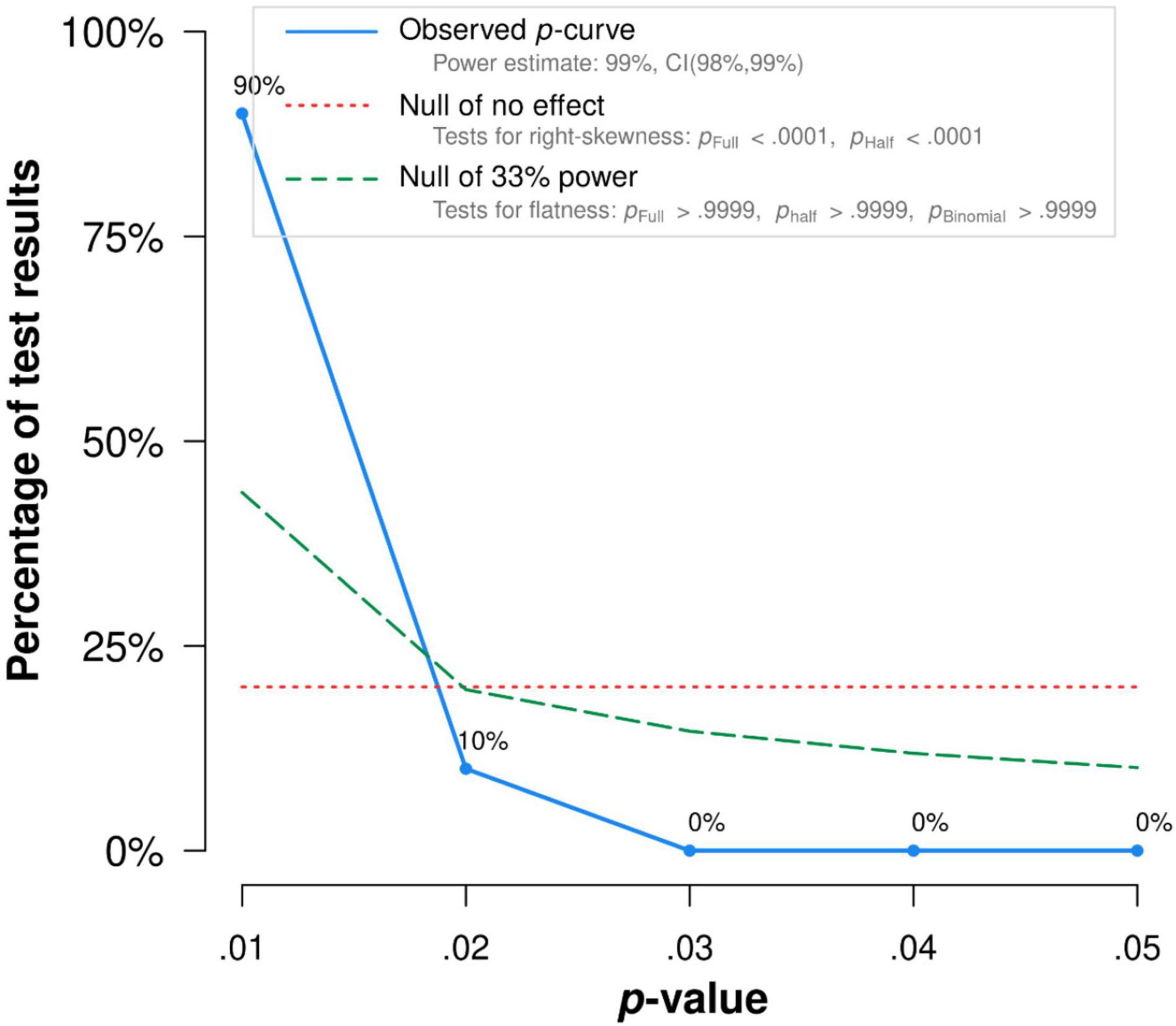
Figure 7. The p-Curve for statistically significant results on the relationship between defusion and functioning. The observed p-curve includes 10 statistically significant (p < 0.05) results, of which 10 are p < 0.025. There were 6 additional results entered but excluded from p-curve because they were p > 0.05.
Present Moment and Functioning
There were 13 correlations in seven studies that examined the relationship between present moment and functioning. The overall effect size was statistically significant and medium (r = 0.31, 95% CI = 0.19, 0.43, p < 0.001; I2 = 84.29%, Q = 79.70, df = 12, p < 0.001). The results were presented in a forest plot in Figure 8.
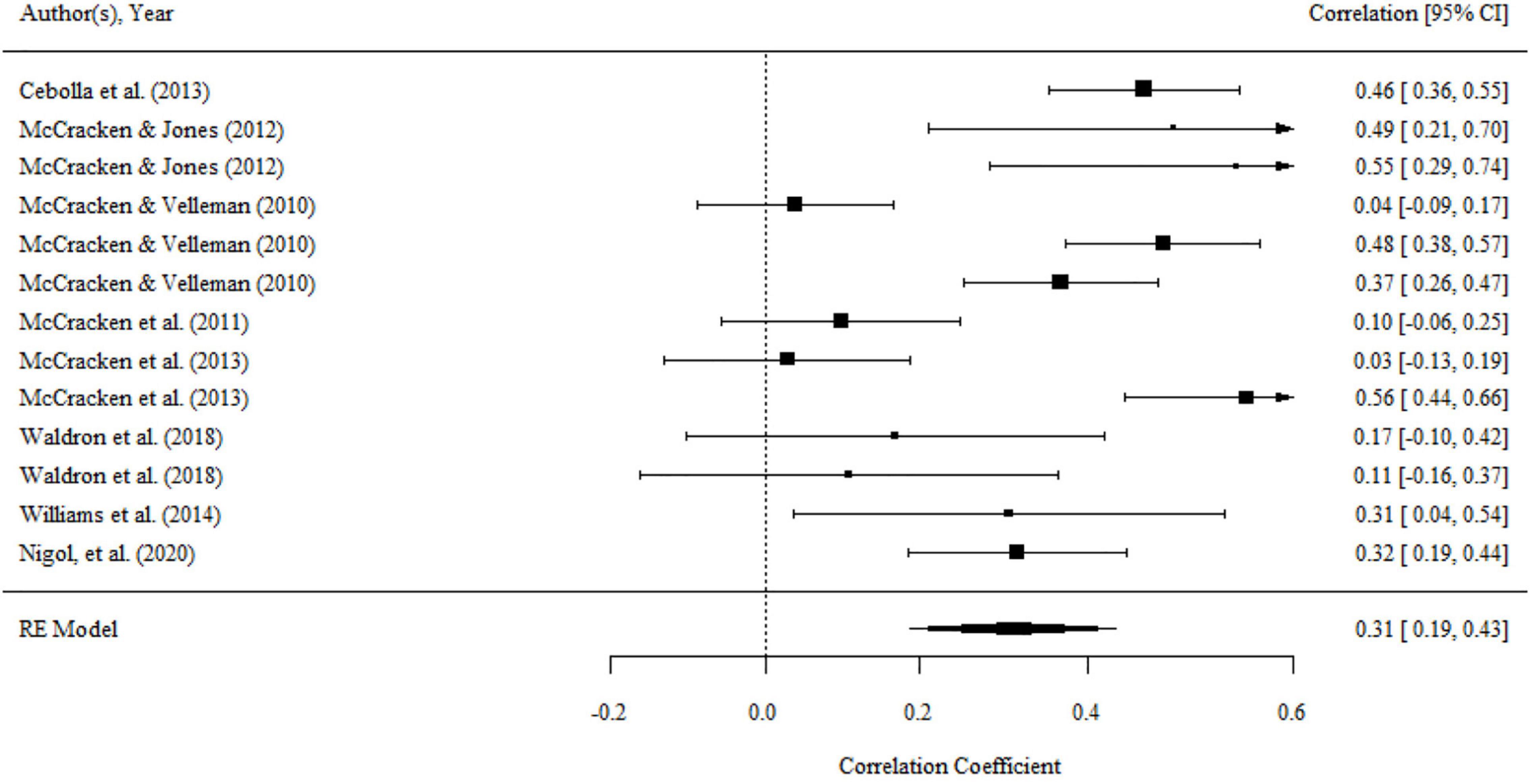
Figure 8. Forest plot of effect size (r) for the relationship between present moment and functioning.
There was significant variance within the same studies (i.e., level 2 variance), while there was no significant variance between studies (i.e., level 3 variance). The details can be seen in Table 2. Moderator analyses were conducted in order to determine variables that can explain level 2 variance. We found a significant moderating effect of the domains of functioning on the association, as shown by the results of the omnibus test (F(2,10) = 5.34, p < 0.05). The mean effect of the relationship between present moment and psychological functioning (r = 0.49, 95% CI = 0.29, 0.68, p < 0.001) was substantially larger than the association of present moment and physical functioning (r = 0.13, 95% CI = −0.08, 0.35, p > 0.05). No significant moderating effect was found for the percentage of females, mean age, country, and type of functioning measurements.
There was no publication bias in Egger tests and Funnel plot (p > 0.1) on the relationship between the present moment and functioning. Both the full p-curve and the half p-curve test were significant with p < 0.0001 (Z = −12.54, Z = −11.52), which indicated that the distribution of p-values is significant right-skewed, as seen in Figure 9. Hence, the results further support the initial assessment that evidential value is present in the literature.
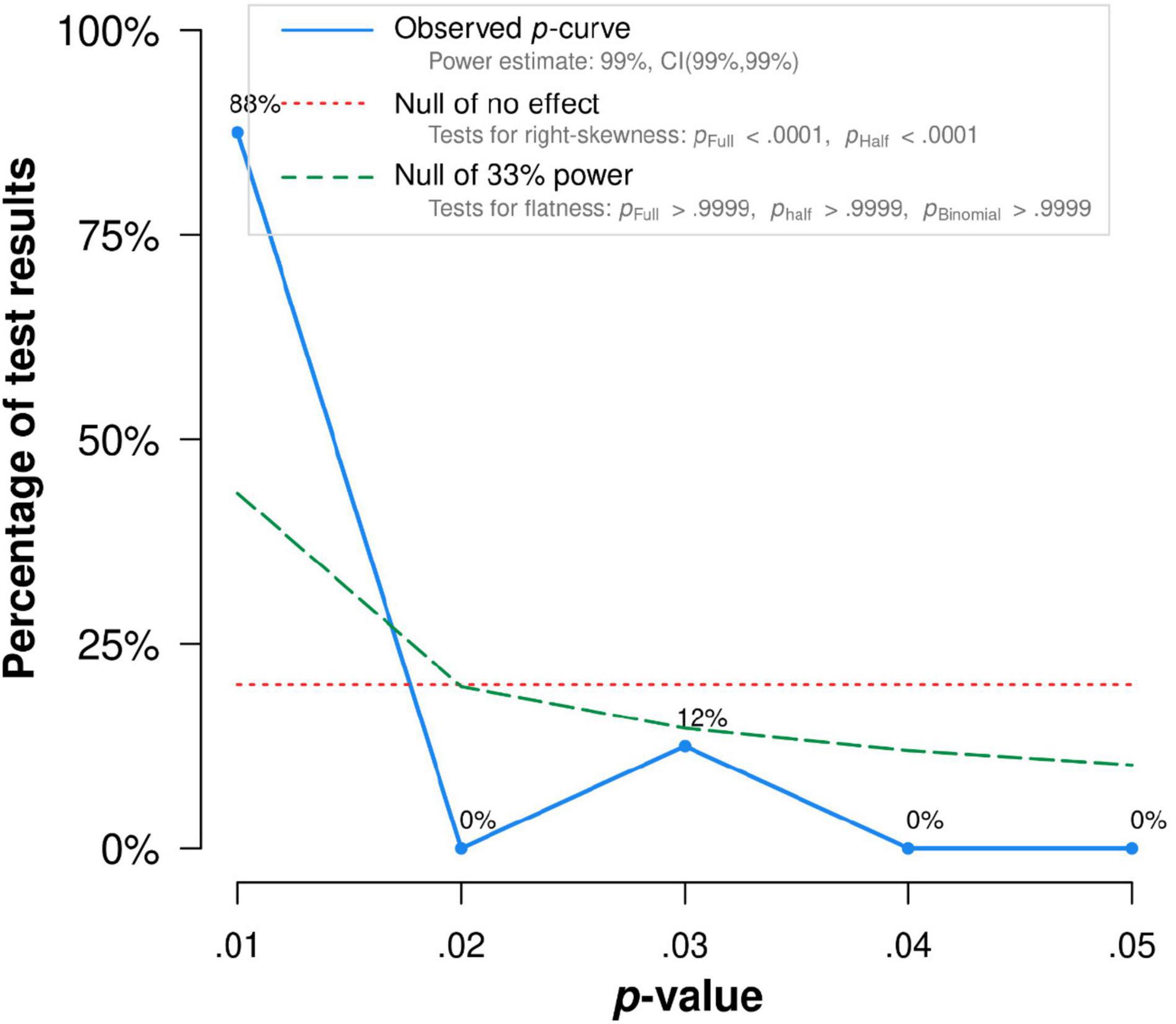
Figure 9. The p-Curve for statistically significant results on the relationship between present moment and functioning. The observed p-curve includes 8 statistically significant (p < 0.05) results, of which 8 are p < 0.025. There were five additional results entered but excluded from p-curve because they were p > 0.05.
Self as Context and Functioning
There were 12 correlations in seven studies that examined the relationship between self as context and functioning. The overall effect size was significant (r = 0.21, 95% CI = 0.08, 0.33, p < 0.01; I2 = 88.88%, Q = 83.72, df = 11, p < 0.001). The results were presented in a forest plot in Figure 10.
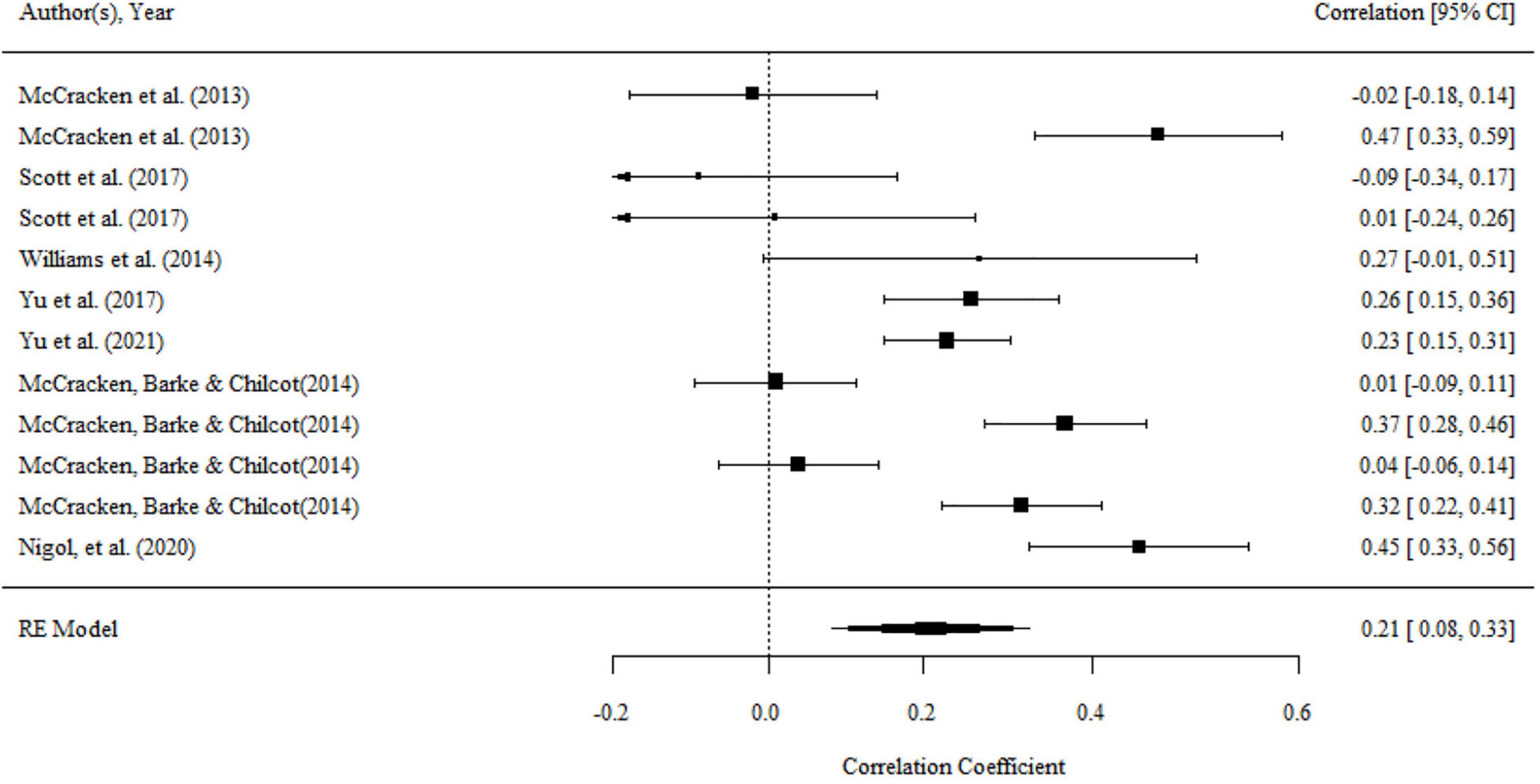
Figure 10. Forest plot of effect size (r) for the relationship between self as context and functioning.
There was significant variance within the same studies (i.e., level 2 variance), while there was no significant variance between studies (i.e., level 3 variance). The details can be seen in Table 2. There was a significant moderating effect of the domain of functioning on the association, as shown by the results of the omnibus test (F(2,10) = 29.56, p < 0.001). The mean effect of the relationship between self as context and overall functioning (r = 0.30, 95% CI = 0.19, 0.41, p < 0.001) and psychological functioning (r = 0.33, 95% CI = 0.19, 0.48, p < 0.001) was substantially larger than that association with physical functioning (r = −0.02, 95% CI = −0.17, 0.13, p > 0.05). No significant moderating effect was found for the percentage of females, mean age, country, type of functioning measurements.
There was no publication bias in Egger test, Funnel plot (p > 0.1), and trim-and-fill analyses. Both the full p-curve and the half p-curve test were significant with p < 0.0001 (Z = −13.15, Z = −12.83), which indicated that the distribution of p-values is significant right-skewed, as seen in Figure 11. Hence, the results further support the initial assessment that evidential value is present in the literature.
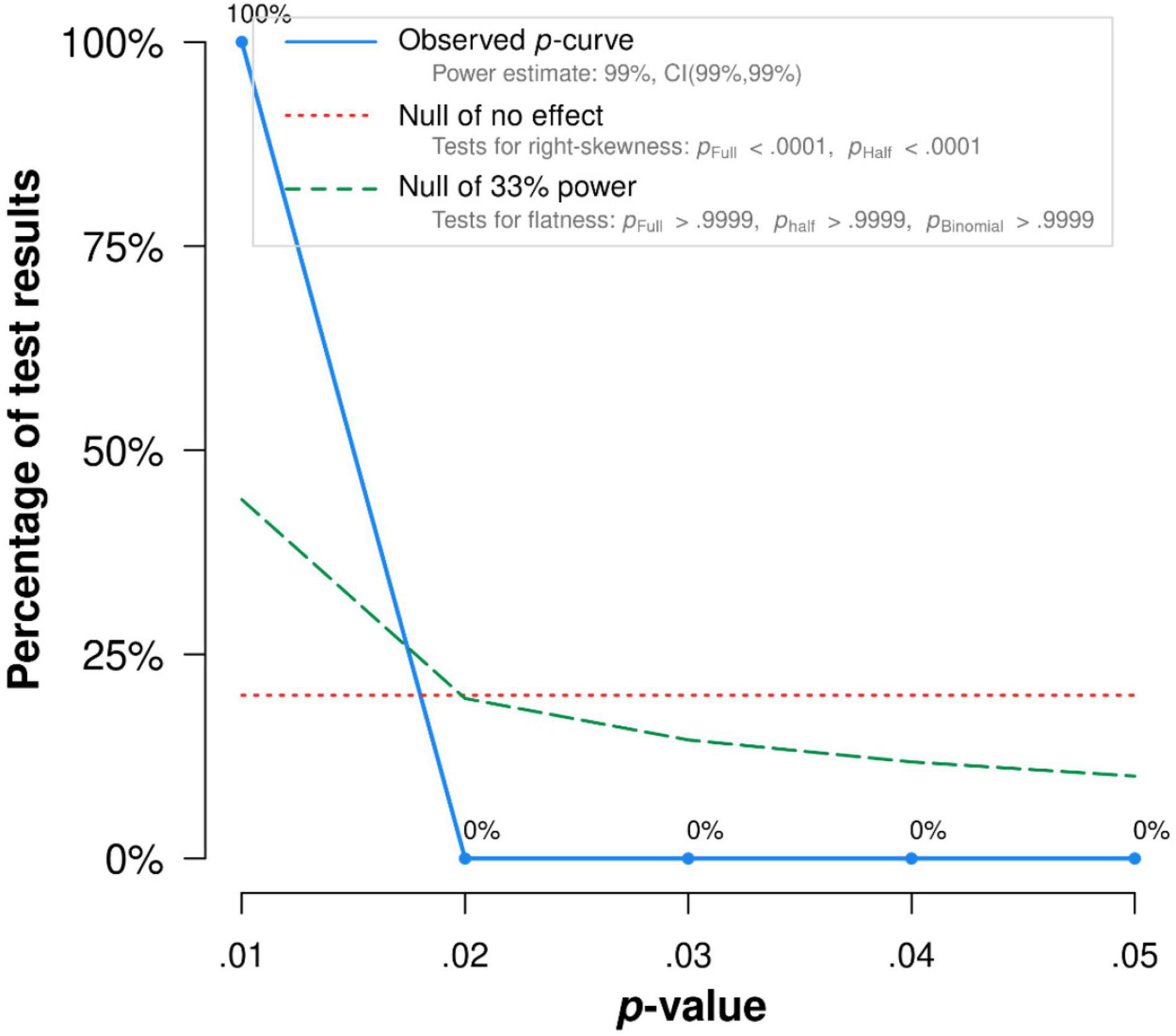
Figure 11. The p-Curve for statistically significant results on the relationship between self and context and functioning. The observed p-curve includes three statistically significant (p < 0.05) results, of which three are p < 0.025. There were four additional results entered but excluded from p-curve because they were p > 0.05.
Values and Functioning
There were fifteen correlations in ten studies that examined the relationship between values and functioning. The overall effect size was statistically significant and medium (r = 0.31, 95% CI = 0.20, 0.41, p < 0.01; I2 = 79.78%, Q = 58.23, df = 15, p < 0.001). The results were presented in a forest plot in Figure 12.
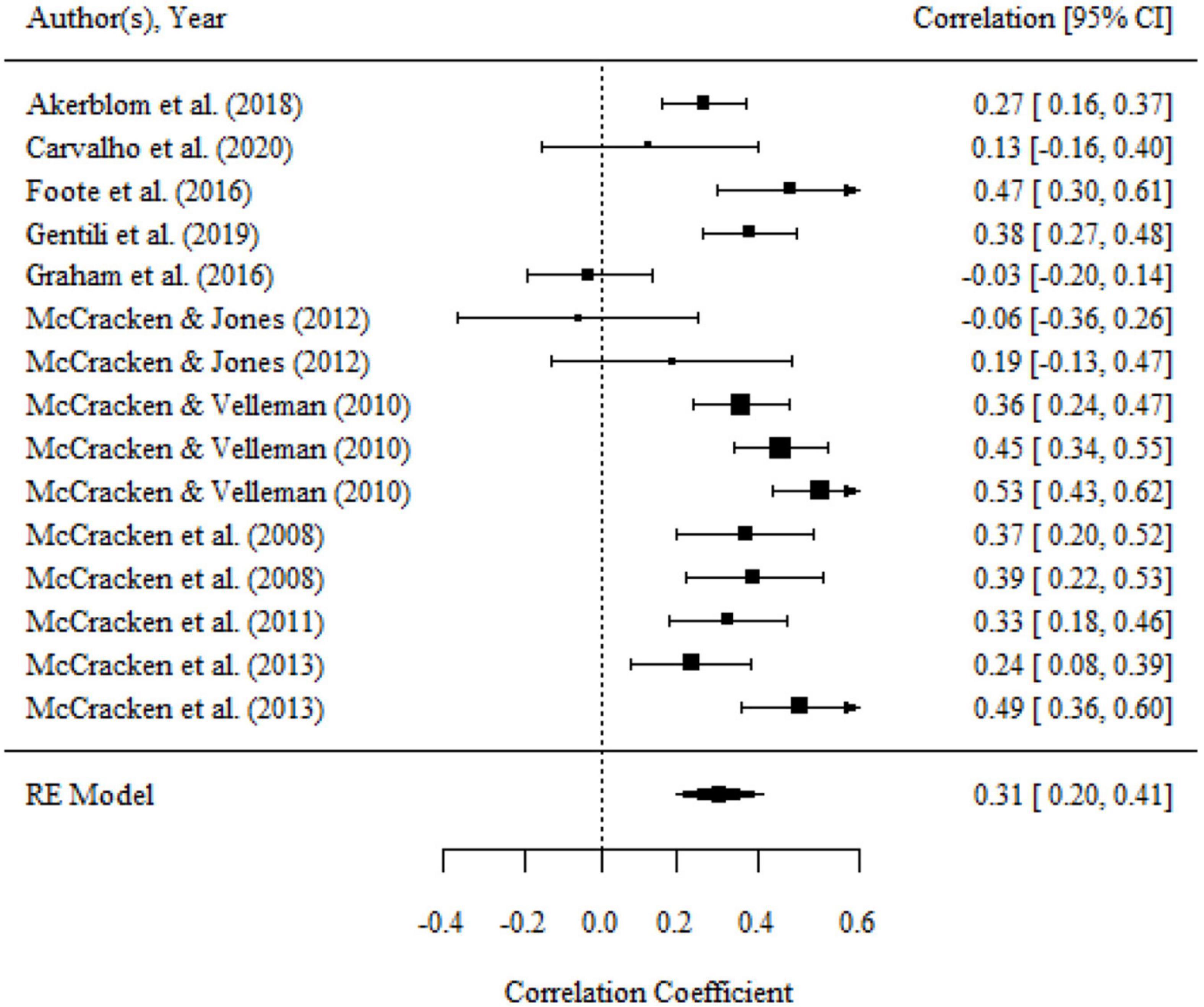
Figure 12. Forest plot of effect size (r) for the relationship between values and functioning.
There was no significant variance within the same studies (i.e., level 2 variance) and between studies (i.e., level 3 variance). The details can be seen in Table 2. We found a significant moderating effect of the domains of functioning on the association, as shown by the results of the omnibus test (F(2,12) = 4.66, p < 0.05). The relationship between values and psychological functioning (r = 0.45, 95% CI = 0.34, 0.55, p < 0.05) was substantially larger than the association of values and physical functioning (r = 0.27, 95% CI = 0.04, 0.48, p < 0.05). No significant moderating effects were found for the percentage of females, mean age, country, and type of functioning measurements.
There was no publication bias in Egger tests (p > 0.1) and the Funnel plot. Both the full p-curve and the half p-curve test were significant with p < 0.001 (Z = −15.41, Z = −14.85), which indicated that the distribution of p-values is significant right-skewed, as seen in Figure 13. Hence, the results further support the initial assessment that evidential value is present in the literature.

Figure 13. The p-Curve for statistically significant results on the relationship between values and functioning. The observed p-curve includes 11 statistically significant (p < 0.05) results, of which 11 are p < 0.025. There were four additional results entered but excluded from p-curve because they were p > 0.05.
Discussion
The present meta-analytic study aimed to estimate an overall association between functioning and six processes of psychological flexibility (i.e., acceptance, defusion, present moment, self as context, committed action, and values). A second aim was to assess whether the strength of these associations is influenced by domains of functioning, type of measurements of functioning, age of sample, country, and the proportion of females. In general, higher levels of psychological flexibility processes are significantly associated with higher levels of functioning. Except for the relationship between defusion and functioning, the relationships between the other five psychological flexibility processes and functioning were all moderated by domains of functioning. Specifically, the strength of the relationship between committed action and overall functioning exceeds its associations with psychological functioning. Also, the strength of the relationship between acceptance/self as context and overall functioning exceeds their associations with physical functioning. Besides, the mean effect of the relationship between acceptance/present moment/self as context/values and psychological functioning exceeds their associations with physical functioning. It was worth noting that the mean effect of the association between the present moment and physical functioning was not significant.
Acceptance is fostered as a behavioral response to pain and distress that cannot be directly changed to engage in meaningful but potentially painful activities (8). Thus, chronic pain patients with high acceptance could be more likely to accept their negative emotions and life events, and would not waste time on events or behaviors that are worthless, i.e., having high functioning. A prospective study found patients who reported greater acceptance at the base time would report better functioning in the future, which suggested that willingness to experience pain and accept it can lead to healthy functioning for chronic pain patients (51). In addition, acceptance is more related to overall and psychological functioning than physical functioning. It is not surprising, as there is a strong correlation between acceptance and an individual’s emotional or mental health (52, 53), and some scholars thought that acceptance alone is a better predictor of psychopathology and well-being than other variables (53). A randomized controlled trial found that acceptance and value clarification could improve participants’ social interaction after experiencing stressful social situations (54). The previous studies and present study both suggested that acceptance is strongly related to psychological functioning in patients with chronic pain. Enhancing personal acceptance may also mean enhancing individual psychological functioning. It may be due to the instruments used to measure overall functioning, such as the BPI (55), as the relationship between acceptance and overall functioning is also stronger than the association between acceptance and physical functioning. The BPI contains seven areas, including emotions and social and physical functioning, and emotions are closely associated with acceptance (52, 53).
Committed action is the ability to build and flexibly adhere to actions guided by values (56). As a behavior pattern oriented toward valued living, committed action may be important for the adaptive adjustment to pain in chronic pain patients (57, 58). Thus, if chronic pain patients have a high level of committed action, they may stay with the behavior or action that is useful to them (e.g., engaging in some recovery training or exercise) and would have a high level of physical functioning. In the present study, the relationship between committed action and physical functioning was higher than the association between committed action and psychological flexibility. However, there was no significant difference which may be due to the small number of studies included. Thus future studies should investigate whether there are differences between the two. The relationship between overall functioning and committed action was significantly higher than the association between psychological functioning and committed action, which may be due to the measurement of overall functioning aforementioned.
Also, cognitive defusion encourages patients to disengage or step back from thoughts and view them as what they are (i.e., merely cognitive events) rather than reality to reduce their impact on behavior (8). It was argued that defusion and acceptance loaded onto a single factor (58). Both processes relate to the willingness to deal with difficult experiences when attempts for change are ineffective or lead to further problems (58). Therefore, patients with greater defusion could lead to healthier functioning. Previous studies also suggested that chronic pain patients with a greater capacity to take a detached view of their own thoughts and emotional experiences (i.e., cognitive defusion) were more likely to suffer less and have better functioning (59).
McCracken and colleagues argued being more mindful or contacting the present moment can lead to a more “balanced, non-reactive and realistic” relationship to pain experiences (60). The present moment involves purposeful, non-judgmental, and fluid focus on present experiences (58, 61), which are not all directly related to pain but rather the processes of acceptance and the present moment play important roles in the suffering and functioning of chronic pain (60). Furthermore, chronic pain patients’ functioning can also be predicted by acceptance and present moment (60). Thus, the higher present moment is associated with higher functioning. However, in this study, we further found that physical functioning has a non-significant association with the present moment, while the present moment has a medium to large relationship with psychological functioning. A systematic review, which examined physical functioning and mindfulness skills training in chronic pain, suggested that contacting the present moment has no efficacy on physical functioning (62), while it has an important role in psychological functioning (63). These were consistent with our study.
In the present study, there was a small positive relationship between self as context and functioning. It should be noted that there was a small negative relationship between self as context and physiological function, but it was not significant. Self as context entails an experience of taking a perspective from their thoughts and feelings and distancing oneself from their thoughts and feelings, but it does not guide the patient’s behavior. Thus, self as context has a strong relationship with depression and can predict emotional functioning (28). And this may be the reason why the association between psychological/overall functioning and self as context were high than that with physical functioning.
Values can help chronic pain patients identify directions for meaningful activities essential to living (58). Treatment programs from ACT theoretical framework found that increased engagement in valued activities was significantly associated with greater improvement in psychological functioning but was not related to change in physical functioning at post-treatment (64). Thus, enhanced values orientation can have a more critical impact on psychological functioning than physical functioning. That may be why values have a higher relationship with psychological functioning in our analysis.
The hypothesized moderating effects (i.e., the percentage of females, mean age, country, and type of functioning measurements) were not found in this study, except for domains of functioning. The relatively narrow age range of participants in this study, which included only five studies that focused on adolescents, may limit detecting a real moderating effect of age on the associations. Also, most studies have focused on Europe and the United States, with very few studies on Asia (only one), so it would be difficult to identify the moderating role of culture. Therefore, future research in different cultural contexts is highly recommended, especially in Asia.
As no known studies have made a comprehensive meta-analysis of the relationship between specific processes of psychological flexibility (e.g., acceptance, defusion, present moment, self as context, committed action, and values) and different domains of functioning (i.e., physical functioning, psychological functioning, and overall functioning), the main strength of the current study lies in addressing this gap in the literature. The findings of this study produced more knowledge on the true associations between variables as well as contradictions or variances between studies. This study offers a possible explanation for why a particular therapy is more effective and can help researchers understand what is most important to pain patients and what might be more effective in improving their functioning. Knowing the relationship between the processes of psychological flexibility and functioning allows process-based therapy to be tailored to chronic pain patients. Patients can be better and more effectively served by emphasizing functioning-related psychological flexibility processes when designing intervention programs. The current study suggests that the ACT programs that focused on acceptance, committed action, the present moment, and values would be more recommendable or applicable to patients with chronic pain, because these processes have a medium to large relationship with functioning. Also, further study is needed to understand factors that influence functioning in attempting to mitigate functional impairment for chronic pain patients.
Although this study provided a conceptual and empirical basis for future work, there were some limitations. First, a major weakness of this meta-analysis is that the methodological quality of the studies was not rated. It was suggested that rating would be difficult due to the lack of clear methodological standards and relevant detail in the methods sections of these studies (56, 65). This study excluded unpublished studies, providing a general approach to ensure methodological quality, but also raising the risk of publication bias affecting the results. A more comprehensive search of the published and unpublished literature may be helpful for further research in this area. Second, the studies included were based on cross-sectional research, so the direction of causality remains unclear. Based on these findings, we cannot determine, for example, whether acceptance influences functioning, functioning influences acceptance, or (more likely) these factors have mutual influence. In addition, self-report data were used in included studies, which may lead to the inflationary effects of common method variance. Thus, the results need to be interpreted with caution. Longitudinal or experimental studies in which psychological flexibility processes are manipulated are needed to evaluate its potential causal impact on chronic pain patients’ functioning. Third, psychological flexibility and psychological inflexibility are two different concepts (50, 66) that were simplified in this study by reversing the results of measuring inflexibility to represent flexibility due to the limited number of available studies. Future research could explore the relationship between the different dimensions of psychological inflexibility and flexibility (i.e., the 12 dimensions) and domains of functioning. Besides, the current meta-analysis only examined gender, region, percentage of females, type of instruments, and domains of functioning as potential moderators. Other potential moderating variables (e.g., education level, family economic status) have not been analyzed and should be further explored in the future to investigate the role of other potential moderating variables in the relationship between functioning and psychological flexibility processes. Furthermore, region and culture are different, and the regional coding does not fully reflect the cultural context. Future research should explore a better way to code the cultural context. Finally, the number of some effect sizes of the moderation variables in the current meta-analytic studies are small, which may impact the results.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author Contributions
DD conceived and designed the analysis, collected the data, performed the analysis, and wrote the manuscript. MZ supported the data collecting, reviewed the included studies, and assisted in data analysis. Both authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank Wang for her help in reviewing the included literature.
References
1. Brooks JM, Iwanaga K, Chiu CY, Cotton BP, Deiches J, Morrison B, et al. Relationships between self-determination theory and theory of planned behavior applied to physical activity and exercise behavior in chronic pain. Psychol Health Med. (2017) 22:814–22. doi: 10.1080/13548506.2017.1282161
2. Rhodes A, Marks D, Block-Lerner J, Lomauro T. Psychological flexibility, pain characteristics and risk of opioid misuse in noncancerous chronic pain patients. J Clin Psychol Med Settings. (2021) 28:405–17. doi: 10.1007/s10880-020-09729-1
3. Si H, Wang C, Jin Y, Tian X, Qiao X, Liu N, et al. Prevalence, factors, and health impacts of chronic pain among community-dwelling older adults in China. Pain Manag Nurs. (2019) 20:365–72. doi: 10.1016/j.pmn.2019.01.006
4. Esteve R, Marcos E, Reyes-Pérez Á, López-Martínez AE, Ramírez-Maestre C. Pain acceptance creates an emotional context that protects against the misuse of prescription opioids: a study in a sample of patients with chronic noncancer pain. Int J Environ Res Public Health. (2021) 18:3054. doi: 10.3390/ijerph18063054
5. Goldbart A, Bodner E, Shrira A. The role of emotion covariation and psychological flexibility in coping with chronic physical pain: an integrative model. Psychol Health. (2020) 36:1299–313. doi: 10.1080/08870446.2020.1841766
6. Davis MC, Zautra AJ, Smith BW. Chronic pain, stress, and the dynamics of affective differentiation. J Pers. (2004) 72:1133–60. doi: 10.1111/j.1467-6494.2004.00293.x
7. McCracken LM, Vowles KE. Psychological flexibility and traditional pain management strategies in relation to patient functioning with chronic pain: an examination of a revised instrument. J Pain. (2007) 8:700–7. doi: 10.1016/j.jpain.2007.04.008
8. Wicksell RK, Vowles KE. The role and function of acceptance and commitment therapy and behavioral flexibility in pain management. Pain Manag. (2015) 5:319–22. doi: 10.2217/pmt.15.32
9. Vowles KE, Witkiewitz K, Levell J, Sowden G, Ashworth J. Are reductions in pain intensity and pain-related distress necessary? An analysis of within-treatment change trajectories in relation to improved functioning following interdisciplinary acceptance and commitment therapy for adults with chronic pain. J Consult Clin Psychol. (2017) 85:87–98. doi: 10.1037/ccp0000159
10. Hayes S, Hogan M, Dowd H, Doherty E, O’Higgins S, Gabhainn SN, et al. Comparing the clinical-effectiveness and cost-effectiveness of an internet-delivered Acceptance and Commitment Therapy (ACT) intervention with a waiting list control among adults with chronic pain: study protocol for a randomised controlled trial. BMJ Open. (2014) 4:e005092. doi: 10.1136/bmjopen-2014-005092
11. Ding D, Wang W. Psychological flexibility and job performance among it staff: a chained mediation model of workplace ostracism and perceived stress. Psychologia. (2022). doi: 10.2117/psysoc.2021-A154 [Epub ahead of print].
12. Kanstrup M, Wicksell RK, Kemani M, Lipsker CW, Lekander M, Holmstrom L. A clinical pilot study of individual and group treatment for adolescents with chronic pain and their parents: effects of acceptance and commitment therapy on functioning. Children. (2016) 3:30. doi: 10.3390/children3040030
13. Daks JS, Peltz JS, Rogge RD. Psychological flexibility and inflexibility as sources of resiliency and risk during a pandemic: modeling the cascade of COVID-19 stress on family systems with a contextual behavioral science lens. J Contextual Behav Sci. (2020) 18:16–27. doi: 10.1016/j.jcbs.2020.08.003
14. Fang S, Ding D. The efficacy of group-based acceptance and commitment therapy on psychological capital and school engagement: a pilot study among Chinese adolescents. J Contextual Behav Sci. (2020) 16:134–43. doi: 10.1016/j.jcbs.2020.04.005
15. Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Ther. (2006) 44:1–25. doi: 10.1016/j.brat.2005.06.006
16. McCracken LM, Morley S. The psychological flexibility model: a basis for integration and progress in psychological approaches to chronic pain management. J Pain. (2014) 15:221–34. doi: 10.1016/j.jpain.2013.10.014
17. Brown SL, Roush JF, Marshall AJ, Jones C, Key C. The intervening roles of psychological inflexibility and functional impairment in the relation between cancer-related pain and psychological distress. Int J Behav Med. (2020) 27:100–7. doi: 10.1007/s12529-019-09838-8
18. Hughes LS, Clark J, Colclough JA, Dale E, McMillan D. Acceptance and commitment therapy (ACT) for chronic pain: a systematic review and meta-analyses. Clin J Pain. (2017) 33:552–68. doi: 10.1097/ajp.0000000000000425
19. Trindade IA, Guiomar R, Carvalho SA, Duarte J, Lapa T, Menezes P, et al. Efficacy of online-based acceptance and commitment therapy for chronic pain: a systematic review and meta-analysis. J Pain. (2021) 22:1328–42. doi: 10.1016/j.jpain.2021.04.003
20. McCracken LM, Barker E, Chilcot J. Decentering, rumination, cognitive defusion, and psychological flexibility in people with chronic pain. J Behav Med. (2014) 37:1215–25. doi: 10.1007/s10865-014-9570-9
21. McCracken LM, Velleman SC. Psychological flexibility in adults with chronic pain: a study of acceptance, mindfulness, and values-based action in primary care. Pain. (2010) 148:141–7. doi: 10.1016/j.pain.2009.10.034
22. McCracken LM, Williams JL, Tang NK. Psychological flexibility may reduce insomnia in persons with chronic pain: a preliminary retrospective study. Pain Med. (2011) 12:904–12. doi: 10.1111/j.1526-4637.2011.01115.x
23. Feinstein AB, Forman EM, Masuda A, Cohen LL, Herbert JD, Moorthy LN, et al. Pain intensity, psychological inflexibility, and acceptance of pain as predictors of functioning in adolescents with juvenile idiopathic arthritis: a preliminary investigation. J Clin Psychol Med Settings. (2011) 18:291–8. doi: 10.1007/s10880-011-9243-6
24. Foote HW, Hamer JD, Roland MM, Landy SR, Smitherman TA. Psychological flexibility in migraine: a study of pain acceptance and values-based action. Cephalalgia. (2016) 36:317–24. doi: 10.1177/0333102415590238
25. Williams AM, Cano A. Spousal mindfulness and social support in couples with chronic pain. Clin J Pain. (2014) 30:528–35. doi: 10.1097/ajp.0000000000000009
26. Yu L, Kioskli K, McCracken LM. The psychological functioning in the COVID-19 pandemic and its association with psychological flexibility and broader functioning in people with chronic pain. J Pain. (2021) 22:926–39. doi: 10.1016/j.jpain.2021.02.011
27. Scott W, Daly A, Yu L, McCracken LM. Treatment of chronic pain for adults 65 and over: analyses of outcomes and changes in psychological flexibility following interdisciplinary acceptance and commitment therapy (ACT). Pain Med. (2017) 18:252–64. doi: 10.1093/pm/pnw073
28. Yu L, Norton S, Almarzooqi S, McCracken LM. Preliminary investigation of self-as-context in people with fibromyalgia. Br J Pain. (2017) 11:134–43. doi: 10.1177/2049463717708962
29. Wicksell RK, Ahlqvist J, Bring A, Melin L, Olsson GL. Can exposure and acceptance strategies improve functioning and life satisfaction in people with chronic pain and whiplash-associated disorders (WAD)? A randomized controlled trial. Cogn Behav Ther. (2008) 37:169–82. doi: 10.1080/16506070802078970
30. Wicksell RK, Melin L, Lekander M, Olsson GL. Evaluating the effectiveness of exposure and acceptance strategies to improve functioning and quality of life in longstanding pediatric pain–a randomized controlled trial. Pain. (2009) 141:248–57. doi: 10.1016/j.pain.2008.11.006
31. Yu L, Inspector Y, McCracken LM. Preliminary investigation of the associations between psychological flexibility, symptoms and daily functioning in people with chronic abdominal pain. Br J Pain. (2021) 15:175–86. doi: 10.1177/2049463720926559
32. Maathz P, Flink IK, Engman L, Ekdahl J. Psychological inflexibility as a predictor of sexual functioning among women with vulvovaginal pain: a prospective investigation. Pain Med. (2020) 21:3596–602. doi: 10.1093/pm/pnaa042
33. Bergner M, Bobbitt RA, Carter WB, Gilson BS. The sickness impact profile: development and final revision of a health status measure. Med Care. (1981) 19:787–805.
34. Gilpin HR, Keyes A, Stahl DR, Greig R, McCracken LM. Predictors of treatment outcome in contextual cognitive and behavioral therapies for chronic pain: a systematic review. J Pain. (2017) 18:1153–64. doi: 10.1016/j.jpain.2017.04.003
35. Hayes SC, Hofmann SG. Process-Based CBT: The Science and Core Clinical Competencies of Cognitive Behavioral Therapy. Oakland, CA: New Harbinger (2018).
36. Hofmann SG, Hayes SC. Modern CBT: moving toward process-based therapies. Rev Bras Ter Cogn. (2018) 14:77–84. doi: 10.5935/1808-5687.20180012
37. Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Associations between psychosocial factors and pain intensity, physical functioning, and psychological functioning in patients with chronic pain: a cross-cultural comparison. Clin J Pain. (2014) 30:713–23. doi: 10.1097/AJP.0000000000000027
38. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. (2021) 134:178–89. doi: 10.1016/j.jclinepi.2021.03.001
39. Cheung MW. Modeling dependent effect sizes with three-level meta-analyses: a structural equation modeling approach. Psychol Methods. (2014) 19:211–29. doi: 10.1037/a0032968
40. Gao S, Assink M, Cipriani A, Lin K. Associations between rejection sensitivity and mental health outcomes: a meta-analytic review. Clin Psychol Rev. (2017) 57:59–74. doi: 10.1016/j.cpr.2017.08.007
41. Assink M, Wibbelink CJM. Fitting three-level meta-analytic models in R: a step-by-step tutorial. Quant Method Psychol. (2016) 12:154–74. doi: 10.20982/tqmp.12.3.p154
42. R Core Team. R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing (2016). https://www.r-project.org/
43. Fernández-Castilla B. Chapter 5_Appendix Publication Bias Three-Level. (2019). Available online at: osf.io/2vkpz (accessed July 07, 2019).
45. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Hoboken, NJ: John Wiley & Sons Ltd (2008).
46. Leandro G. Meta-Analysis in Medical Research: The Handbook for the Understanding and Practice of Meta-Analysis. Hoboken, NJ: Blackwell Publishing Ltd (2007). doi: 10.1002/9780470994894
47. Duval S, Tweedie R. Trim and fill: a simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics. (2000) 56:455–63. doi: 10.1111/j.0006-341X.2000.00455.x
48. Simonsohn U, Nelson LD, Simmons JP. p-Curve and effect size: correcting for publication bias using only significant results. Perspect Psychol Sci. (2014) 9:666–81. doi: 10.1177/1745691614553988
49. Vogel D, Homberg F. P-Hacking, P-curves, and the PSM–performance relationship: Is there evidential value?. Public Adm Rev. (2020) 81:191–204. doi: 10.1111/puar.13273
50. Daks JS, Rogge RD. Examining the correlates of psychological flexibility in romantic relationship and family dynamics: a meta-analysis. J Contextual Behav Sci. (2020) 18:214–38. doi: 10.1016/j.jcbs.2020.09.010
51. McCracken LM, Eccleston C. A prospective study of acceptance of pain and patient functioning with chronic pain. Pain. (2005) 118:164–9. doi: 10.1016/j.pain.2005.08.015
52. Elices M, Tejedor R, Pascual JC, Carmona C, Soriano J, Soler J. Acceptance and present-moment awareness in psychiatric disorders: is mindfulness mood dependent?. Psychiatry Res. (2019) 273:363–8. doi: 10.1016/j.psychres.2019.01.041
53. Kotsou I, Leys C, Fossion P. Acceptance alone is a better predictor of psychopathology and well-being than emotional competence, emotion regulation and mindfulness. J Affect Disord. (2018) 226:142–5. doi: 10.1016/j.jad.2017.09.047
54. Hochard KD, Hulbert-Williams L, Ashcroft S, McLoughlin S. Acceptance and values clarification versus cognitive restructuring and relaxation: a randomized controlled trial of ultra-brief non-expert-delivered coaching interventions for social resilience. J Contextual Behav Sci. (2021) 21:12–21. doi: 10.1016/j.jcbs.2021.05.001
55. Scott W, Yu L, Patel S, McCracken LM. Measuring stigma in chronic pain: preliminary investigation of instrument psychometrics, correlates, and magnitude of change in a prospective cohort attending interdisciplinary treatment. J Pain. (2019) 20:1164–75. doi: 10.1016/j.jpain.2019.03.011
56. Levin ME, Hildebrandt MJ, Lillis J, Hayes SC. The impact of treatment components suggested by the psychological flexibility model: a meta-analysis of laboratory-based component studies. Behav Ther. (2012) 43:741–56. doi: 10.1016/j.beth.2012.05.003
57. Galán S, Roy R, Solé E, Racine M, de la Vega R, Jensen MP, et al. Committed action, disability and perceived health in individuals with fibromyalgia. Behav Med. (2019) 45:62–9. doi: 10.1080/08964289.2018.1467370
58. Vowles KE, Sowden G, Ashworth J. A comprehensive examination of the model underlying acceptance and commitment therapy for chronic pain. Behav Ther. (2014) 45:390–401. doi: 10.1016/j.beth.2013.12.009
59. McCracken LM, Gutiérrez-Martínez O, Smyth C. “Decentering” reflects psychological flexibility in people with chronic pain and correlates with their quality of functioning. Health Psychol. (2013) 32:820–3. doi: 10.1037/a0028093
60. McCracken LM, Gauntlett-Gilbert J, Vowles KE. The role of mindfulness in a contextual cognitive-behavioral analysis of chronic pain-related suffering and disability. Pain. (2007) 131:63–9. doi: 10.1016/j.pain.2006.12.013
61. Waldron SM, Gauntlett-Gilbert J, Marks E, Loades ME, Jacobs K. Dispositional mindfulness and its relationship with distress and functioning in adolescents with chronic pain and low-level pain. J Pediatr Psychol. (2018) 43:1038–46. doi: 10.1093/jpepsy/jsy036
62. Jackson W, Zale EL, Berman SJ, Malacarne A, Lapidow A, Schatman ME, et al. Physical functioning and mindfulness skills training in chronic pain: a systematic review. J Pain Res. (2019) 12:179–89. doi: 10.2147/JPR.S172733
63. Gu J, Strauss C, Bond R, Cavanagh K. How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clin Psychol Rev. (2015) 37:1–12. doi: 10.1016/j.cpr.2015.01.006
64. Vowles KE, Sowden G, Hickman J, Ashworth J. An analysis of within-treatment change trajectories in valued activity in relation to treatment outcomes following interdisciplinary Acceptance and Commitment Therapy for adults with chronic pain. Behav Res Ther. (2019) 115:46–54. doi: 10.1016/j.brat.2018.10.012
65. Low CA, Schauenburg H, Dinger U. Self-criticism and psychotherapy outcome: a systematic review and meta-analysis. Clin Psychol Rev. (2020) 75:101808. doi: 10.1016/j.cpr.2019.101808
66. Rolffs JL, Rogge RD, Wilson KG. Disentangling components of flexibility via the hexaflex model: development and validation of the multidimensional psychological flexibility inventory (MPFI). Assessment. (2016) 25:458–82. doi: 10.1177/1073191116645905
67. Åkerblom S, Perrin S, Fischer M, McCracken L. A validation and generality study of the committed action questionnaire in a Swedish sample with chronic pain. Int J Behav Med. (2016) 23:260–70. doi: 10.1007/s12529-016-9539-x
68. Åkerblom S, Perrin S, Rivano Fischer M, McCracken LM. The relationship between posttraumatic stress disorder and chronic pain in people seeking treatment for chronic pain: the mediating role of psychological flexibility. Clin J Pain. (2018) 34:487–96. doi: 10.1097/ajp.0000000000000561
69. Beeckman M, Hughes S, Ryckeghem DV, Hoecke EV, Dehoorne J, Joos R, et al. Resilience factors in children with juvenile idiopathic arthritis and their parents: the role of child and parent psychological flexibility. Pain Med. (2019) 20:1120–31. doi: 10.1093/pm/pny181
70. Carriere JS, Sturgeon JA, Yakobov E, Kao M-C, Mackey SC, Darnall BD. The impact of perceived injustice on pain-related outcomes: a combined model examining the mediating roles of pain acceptance and anger in a chronic pain sample. Clin J Pain. (2018) 34:739–47. doi: 10.1097/ajp.0000000000000602
71. Carvalho SA, Pinto-Gouveia J, Gillanders D, Lapa T, Valentim A, Santos E, et al. Above and beyond emotional suffering: the unique contribution of compassionate and uncompassionate self-responding in chronic pain. Scand J Pain. (2020) 20:853–7. doi: 10.1515/sjpain-2020-0082
72. Catala P, Suso-Ribera C, Gutierrez L, Perez S, Lopez-Roig S, Penacoba C. Is thought management a resource for functioning in women with fibromyalgia irrespective of pain levels? Pain Med. (2021) 22:1827–36. doi: 10.1093/pm/pnab073
73. Cebolla A, Luciano JV, DeMarzo MP, Navarro-Gil M, Campayo JG. Psychometric properties of the Spanish version of the Mindful Attention Awareness Scale (MAAS) in patients with fibromyalgia. Health Qual Life Outcomes. (2013) 11:6. doi: 10.1186/1477-7525-11-6
74. Fish RA, Hogan MJ, Morrison TG, Stewart I, McGuire BE. Willing and able: a closer look at pain Willingness and Activity Engagement on the Chronic Pain Acceptance Questionnaire (CPAQ-8). J Pain. (2013) 14:233–45. doi: 10.1016/j.jpain.2012.11.004
75. Gauntlett-Gilbert J, Alamire B, Duggan GB. Pain acceptance in adolescents: development of a short form of the CPAQ-A. J Pediatr Psychol. (2019) 44:453–62. doi: 10.1093/jpepsy/jsy090
76. Gentili C, Rickardsson J, Zetterqvist V, Simons LE, Lekander M, Wicksell RK. Psychological flexibility as a resilience factor in individuals with chronic pain. Front Psychol. (2019) 10:2016. doi: 10.3389/fpsyg.2019.02016
77. Graham CD, Gouick J, Ferreira N, Gillanders D. The influence of psychological flexibility on life satisfaction and mood in muscle disorders. Rehabil Psychol. (2016) 61:210–7. doi: 10.1037/rep0000092
78. Kanzler KE, Pugh JA, McGeary DD, Hale WJ, Mathias CW, Kilpela LS, et al. Mitigating the effect of pain severity on activity and disability in patients with chronic pain: the crucial context of acceptance. Pain Med. (2019) 20:1509–18. doi: 10.1093/pm/pny197
79. McCracken LM, Zhao-O’Brien J. General psychological acceptance and chronic pain: there is more to accept than the pain itself. Eur J Pain. (2010) 14:170–5. doi: 10.1016/j.ejpain.2009.03.004
80. McCracken LM, Jones R. Treatment for chronic pain for adults in the seventh and eighth decades of life: a preliminary study of Acceptance and Commitment Therapy (ACT). Pain Med. (2012) 13:860–7. doi: 10.1111/j.1526-4637.2012.01407.x
81. McCracken LM, Vowles KE. A prospective analysis of acceptance of pain and values-based action in patients with chronic pain. Health Psychol. (2008) 27:215–20. doi: 10.1037/0278-6133.27.2.215
82. Nigol SH, Di Benedetto M. The relationship between mindfulness facets, depression, pain severity and pain interference. Psychol Health Med. (2020) 25:53–63. doi: 10.1080/13548506.2019.1619786
83. Solé E, Tomé-Pires C, de la Vega R, Racine M, Castarlenas E, Jensen MP, et al. Cognitive fusion and pain experience in young people. Clin J Pain. (2016) 32:602–8. doi: 10.1097/ajp.0000000000000227
84. Trainor H, Henke M, Winefield H, Baranoff J. Functioning with fibromyalgia: the role of psychological flexibility and general psychological acceptance. Aust Psychol. (2019) 54:214–24. doi: 10.1111/ap.12363
85. Vasiliou VS, Karekla M, Michaelides MP, Kasinopoulos O. Construct validity of the G-CPAQ and its mediating role in pain interference and adjustment. Psychol Assess. (2018) 30:220–30. doi: 10.1037/pas0000467
86. Wong CCY, Paulus DJ, Lemaire C, Leonard A, Sharp C, Neighbors C, et al. Examining HIV-Related stigma in relation to pain interference and psychological inflexibility among persons living with HIV/AIDS: the role of anxiety sensitivity. J HIV AIDS Soc Serv. (2018) 17:1–15. doi: 10.1080/15381501.2017.1370680
87. Yang SY, McCracken LM, Moss-Morris R. Psychological treatment needs for chronic pain in singapore and the relevance of the psychological flexibility model. Pain Med. (2017) 18:1679–94. doi: 10.1093/pm/pnw175
Keywords: processes of psychological flexibility, physical functioning, psychological functioning, chronic pain, meta-analysis, acceptance, acceptance and commitment therapy
Citation: Ding D and Zheng M (2022) Associations Between Six Core Processes of Psychological Flexibility and Functioning for Chronic Pain Patients: A Three-Level Meta-Analysis. Front. Psychiatry 13:893150. doi: 10.3389/fpsyt.2022.893150
Received: 10 March 2022; Accepted: 02 June 2022;
Published: 11 July 2022.
Edited by:
Veena Kumari, Brunel University London, United KingdomReviewed by:
Dongfeng Zhang, Qingdao University, ChinaDongliang Jiao, Bengbu Medical College, China
Copyright © 2022 Ding and Zheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dongyan Ding, ZGR5MDU1OEAxMjYuY29t