
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 08 September 2022
Sec. Anxiety and Stress Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.888234
This article is part of the Research Topic Monitoring Depression and Anxiety Symptoms: Scales and Measurements View all 17 articles
 Isabella Louise Morais de Sousa1
Isabella Louise Morais de Sousa1 Rodrigo Silveira2
Rodrigo Silveira2 Mônica Yuri Takito2
Mônica Yuri Takito2 Adenilson Leão Pereira1,3Dalberto Lucianelli-Júnior1Giselle Sousa Carmona4Ana Paula do Vale Viegas1
Adenilson Leão Pereira1,3Dalberto Lucianelli-Júnior1Giselle Sousa Carmona4Ana Paula do Vale Viegas1 Francisco Bruno Teixeira5Ozélia Sousa Santos1*†
Francisco Bruno Teixeira5Ozélia Sousa Santos1*† Fernanda Nogueira Valentin1,3*†
Fernanda Nogueira Valentin1,3*†The impact of social isolation in the pandemic context on elderly Brazilian mental health is little known, especially about the occurrence of depressive symptoms. In this study, we evaluated elderly people undergoing social isolation in order to identify factors associated with depression and which of these are more important to characterize elderly Brazilians with depression. In a cross-sectional, exploratory, and analytical study of a quantitative nature, the mental profile of elderly individuals subjected to social isolation during the COVID-19 pandemic period was used. A total of 450 participants was divided into normal and depressive groups, and a form covering sociodemographic data, opinions/perceptions about the pandemic, and a Reduced Geriatric Depression Scale was used to assess participants' mental health. To assess the statistical significance between the variables, chi-square test was applied, considering the p-value <0.05. The effect size was analyzed to identify the magnitude of the difference between groups. To identify the most important characteristics to define the groups Multilayer Perceptron algorithm were applied. We found that elderly people with a depressive profile are (in Multilayer Perceptron rank order) (1) showing signs of anxiety during the COVID-19 pandemic, (2) of low education, (3) being divorced, (4) having more than one mental disorder, (5) reading, watching, or listening to information about COVID-19, and (6) being previously diagnosed with depression. In conclusion, elderly Brazilians in social isolation tend to develop depressive disorders during quarantine. Thus, we can consider that the pandemic requires effective and safe gerontological care and monitoring, especially with regard to mental health.
The emergence and rapid increase in the number of cases of COVID-19, an infectious disease caused by the new coronavirus, which in most cases can lead the patient to the severe acute respiratory syndrome, presents complex challenges for health, economy, and society. COVID-19 is currently a public health emergency of international concern, as declared on 30 January 2020 by the World Health Organization. In early July of 2022, there were more than 552 million confirmed cases of COVID-19 worldwide and more than 6.34 million deaths (1).
The first confirmed case of COVID-19 in Brazil was announced on 26 February 2020. Currently, the number of cases exceeds 28 million and more than 670,000 victims, making Brazil the third country with more cases and is the second deaths by COVID-19 in the world (2).
The COVID-19 pandemic has been compared to catastrophic events such as earthquakes, tsunamis, conflicts, and wars. However, unlike these cases, the pandemic was and is still something unusual and obscure for world society, because until some time ago, it was not known what was ahead, and the possibility of contagion by the virus was everywhere and is still a threat (3). In addition, the excess of information transmitted and still may generate panic, favoring situations of stress and fear. Studies show that these factors can trigger traumatic stress, which may manifest itself in the main models of post-traumatic stress disorder (4, 5), which may have even more catastrophic impacts on vulnerable groups such as the elderly people (6, 7).
In the beginning of the confrontation of the COVID-19 pandemic, in 2020, Brazil adopted many public health measures, such as quarantine and mandatory social isolation, suspensions from school and non-essential services, in order to mitigate the risks and impact of the disease on the population. A study carried out in Hong Kong showed that sudden changes in daily life are risk factors that can substantially affect mental health, and this fact can be brought to the Brazilian context (8).
The elderly are more vulnerable to COVID-19 because they have a higher risk of developing the most severe form of the disease, especially those with preexisting comorbidities, such as heart, hypertension, diabetes, kidney, lung, cancer, and immunosuppression diseases (9). In Brazil, the mortality rate in 2020 among people with aged ≥80 years was higher (14.8% died), when compared to the elderly aged 70–79 years (8% died) and 60–69 years (8.8% died), in other words, a rate of 3.82 times higher than the general average, reinforcing the concerns regarding the elderly population (10). However, after the start of vaccination for the elderly in January 2021, these numbers have been reduced (11). Orellana and collaborators in 2022 (12) observed changes in the pattern of hospitalizations and deaths from COVID-19 after substantial vaccination of the elderly in Manaus, Amazonas, and Brazil. According to him, there was an overall reduction of approximately 62% in hospitalization and death rates, especially in the elderly aged 60–69 years.
Social distancing and isolation are among the recommended guidelines for the safety of the elderly during the pandemic. However, social isolation is a major danger to the health and wellbeing of the elderly as it is associated with an increased mortality risk and is linked to worsening mental health (13). The incidence and prevalence of the depressive disorder in the elderly population is high globally, and although it affects both sexes, the incidence is higher in women (14). Recently, Santini, Jose (15), observed that social disconnection exposes the elderly to a high risk of depression. In addition, it is believed that the health risks associated with the social isolation and loneliness are equivalent to the prejudicial effects caused by smoking and obesity (16).
The causes of depression can be genetic, brain biochemistry, or vital events. Events that cause stress and anxiety, also called vital events, are mostly triggering factors for depressive episodes, especially in those who already have a genetic predisposition to the development of the disorder. The imbalance of neurotransmitters such as serotonin, dopamine, and noradrenaline responsible for controlling appetite, mood, and motor activity are also closely associated with depression (17).
The situations of daily life trigger different reactions in individuals, among which depressive symptoms are present. In these situations, individuals demonstrate general or non-specific responses of a physiological and psychological nature of the body to a stressor or external and internal threats (18, 19).
The causes and symptoms that trigger the depressive disorder are well characterized; however, in elderly individuals, these symptoms are more difficult to diagnose and, consequently, to treat. Therefore, the main difficulty in the treatment of this clinical condition is the correct diagnosis, which is partly associated with the fact that many elderly people do not accept their depressive clinical condition and do not seek adequate psychiatric treatment (20). In this scenario, the context of the COVID-19 global pandemic can make this situation more aggravating, since the fear of the unknown can lead to depression, and social isolation measures limit people's daily activities, especially of the elderly (21). Therefore, due to the pandemic conditions to which the elderly are being subjected, the development or worsening of depressive conditions is expected, since these disorders are closely related to social isolation, affecting physical and mental health and aggravating underlying diseases (22).
The Brazilian population has a cultural and religious plurality that is very subjective (23, 24), and it is possible that it does not behave in the same way in relation to other population groups. In this context, the use of machine learning can be useful to create robust models that can provide more accurate data for this population.
Although there are previous works based on bibliographic reviews in Brazil (25–28), and some cross-sectional studies on mental health of the elderly in the pandemic in other countries such as China, Spain, and Italy (8, 29–33), in Brazil, cross-sectional studies have not yet been found, nor combined with k-means cluster analysis (an unsupervised machine learning algorithm) that explored the association of COVID-19 impacts and physical isolation on the mental health of elderly Brazilians, especially in terms of depression levels.
In this study, we aimed to identify whether there are distinct groups in the elderly population (with and without depression). We also analyzed the main characteristics of elderly Brazilian people with and without depression in the period of social isolation and we identified which of these characteristics are more important to characterize Brazilian elderly people with depression. Thus, based on the literature cited, it is believed that elderly Brazilians may develop or worsen depressive symptoms during the COVID-19 pandemic due to social isolation.
The study included 450 male and female subjects, over 60 years of age (67.2 ± 6.7 years), representing all Brazilian states. The form was in Portuguese and was available online from 26 June to 8 September 2020, through social networks and e-mail.
Data collection was performed after approval of the research project by the Ethics Committee of the Institute of Health Sciences of the Federal University of Pará (CAAE number: 32893620.8.0000.0018). All participants who agreed to participate in the research signed the Informed Consent Form.
In this study, only people who lived in Brazil at the time of data collection were included. The questionnaires were distributed mostly by e-mail to universities, institutes, and personal e-mails of project participants. In addition, another part of the participants, the application of the form, was carried out through the whatsapp application and/or telephone call. The elderly who could not answer the form alone were helped by someone close (family member, friends, or project participants) to whom the questions were dictated and the respective alternatives were answered verbally. Participants unable to answer verbally and/or provide decisions regarding the alternatives to the questions by cognitive or psychiatric disability were excluded. In addition, for all participants who filled it more than once, only the first participation was maintained, excluding the remaining.
To ensure better quality of the data obtained, a pilot study was conducted before starting the official form dissemination with a dataset of 100 participants (not counted in the sample) to evaluate the dissemination strategy, responses obtained, and the quality of the anchoring questions.
For the sample calculation, the G* Power 3.0.10 software was used to simulate all the analyses performed. The sample size was determined by the analysis that estimated the largest number of participants, being a Chi-square test with up to 6 degrees of freedom, assuming an intermediate effect size, a significance of p < 0.05 and a statistical power of 95%, estimating a minimum sample of n = 232. However, to ensure better representativeness of the Brazilian population, this minimum sample size was estimated to be increased by 90%. Thus, based on cultural plurality rooted in the great social and regional diversity in the set of 27 Brazilian states (34), the estimated minimum sample size increased by 186 (~80%) with an additional 22 (~10%) for possible sample loss, totaling a minimum sample size of n = 440.
The online form was structured with multiple choice questions and covering general demographic data such as age, gender, race, marital status, religion, having children, education, city and previous diagnosis of mental disorder. The questions on the opinions and perceptions of the elderly regarding the COVID-19 pandemic were as follows: (a) If the participants claim to know what the pandemic and COVID-19 are?; (b) What are the main ways to obtain information about the pandemic?; (c) How much time do you spend getting this information?; (d) Do you know what social isolation is?; (e) Do you agree with the imposed social isolation?; (f) How do you feel about the whole pandemic scenario?; and (g) Who are they with passing the period of social isolation?
To assess anxiety, the Brazilian version of the Geriatric Anxiety Inventory (GAI) with 20 objective questions was applied (34). The GAI is characterized by being a self-applicable instrument with dichotomous responses (agree/disagree) (35). The instrument has a cutoff score between 10/11 (non-case/case), where a score of 0–10 indicates no anxiety, 11–15 indicates mild or moderate anxiety, and 16–20 indicates severe anxiety. In this study, only the absence (score 0–10) or presence (score 11–20) of anxiety was considered.
To assess depression, the Brazilian version of the reduced Geriatric Depression Scale with 15 objective questions was applied (36). Its score ranges from 0 to 15 points, being divided into three categories. A score of 0–5 is considered normal, 6–10 mild depressive symptoms, and 11–15 severe depressive symptoms. We only considered the absence (score 0–5) or presence (score 6–15) of depression.
To avoid possible interpretation errors and potential sources of bias, a pilot study was conducted, which served to improve the form questions.
Continuous data were presented as the median and interquartile range, while categorical data as percentages. To analyze the significance between the proportions of the sample with and without depressive disorder, 95% confidence intervals were observed. To analyze the associations between the groups with and without depression and the different categorical variables, Pearson's chi-square test was applied. Correction by Fisher's exact test was applied when in any contingency table there was n < 6 in any cell. For all tests, the statistical significance adopted was p-value <0.05. In contingency tables >2 x 2 with statistical significance, adjusted residuals >2 were analyzed to identify which categories influenced the p-value <0.05.
To analyze the magnitude of differences between groups, effect sizes were observed using Φ (ϕ) in 2 x 2 tables, assuming “no effect” for ϕ < 0.10, “small effect” for ϕ < 0.30, “moderate effect” for ϕ < 0.50 and “large effect” for higher values. In >2 x 2 tables, the sizes were observed by Cramer's V, whose interpretations of null, small, moderate, and large effects were performed considering the variations according to an increase in degrees of freedom (37, 38).
To assess the characteristics that most influence the classification of the participants as depressive or non-depressive, the Multilayer Perceptron algorithm was used (p-value <0.05). This supervised machine learning algorithm, through an artificial neural network, identifies non-linear patterns among different variables in a dataset and, in response, provides a prediction of some predetermined variable of interest. When executed, this learning algorithm perform through the following steps: (1) the weights are initialized; (2) the flow and analysis of information flows through the input, hidden, and output layers; (3) error rate in output layer predictions is calculated and weights are adjusted; and (4) all previous steps are repeated until the error rate becomes as low as possible (39).
Quantitative variables were rescheduled at intervals between 0 and 1. The samples were randomly divided into two datasets, where 70% of the samples were used for training the algorithm and 30% for the test. For training and optimization, Minibatch and Descending Gradient methods were selected, respectively. Because Multilayer Perceptron can give different results each time it is run due to randomization of dataset partitions for cross validation and initialization of weights, the algorithm was run three times. The trial chosen was the one with the lowest mean value of cross-entropy error ([training error + test error]/2). Therefore, the chosen attempt was the second.
The ability of the predictors to determine the artificial neural network was tested by using sensitivity analysis, combining the training and test samples. In addition, a table that shows the degree of importance of each predictor was created. Data analyses were processed using the SPSS v.23.0 software.
The sample distribution (n = 450) across Brazilian states ranged from n = 3 in Acre to n = 69 in São Paulo (Figure 1). Of the 450 subjects, 31.1% showed depressive symptoms (IC: Normal = 64.6–73.2; IC: Depressive = 26.8–35.4).
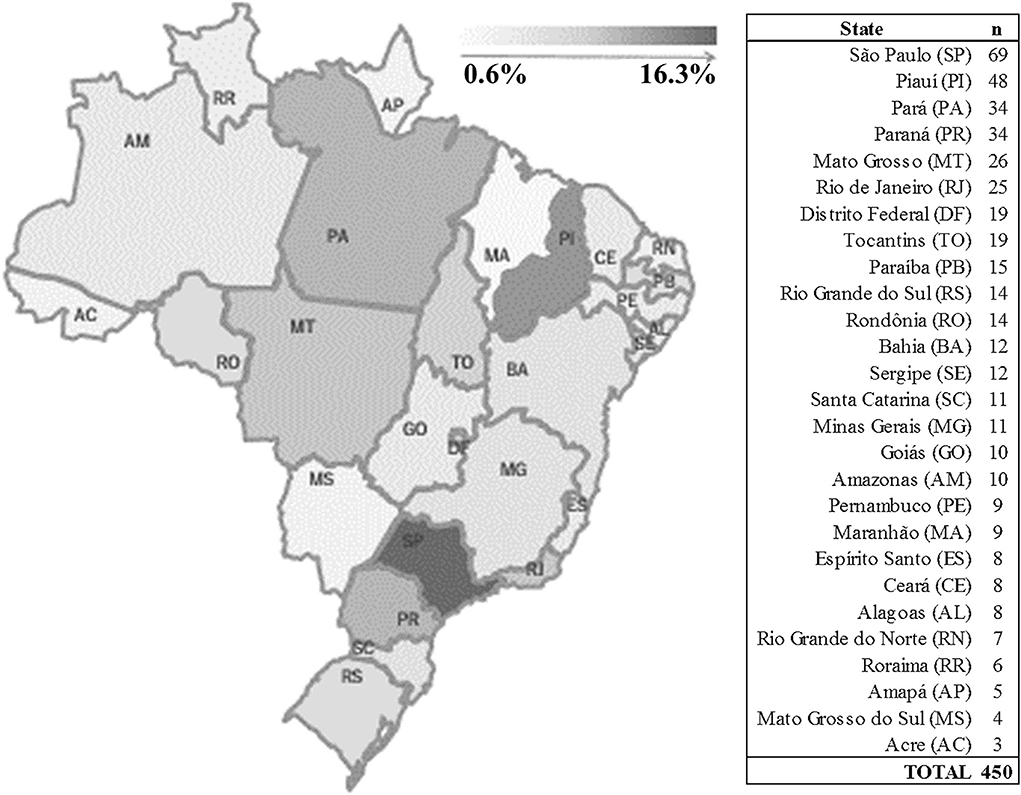
Figure 1. Sample divided by Brazilian states.
The sociodemographic characteristics between the groups are detailed in Supplementary Table S1. Individuals with depressive symptoms are characterized by having a higher proportion of women (80.7%), divorced (23.6%), and with low education (32.9%) (p < 0.01). Regarding the religion of the elderly without depressive symptoms, there was a higher proportion of individuals without religion (14.2%), while among the elderly with depressive symptoms, there was a higher proportion of subjects who adhere to Afro-Brazilian religions (2.1%) (p < 0.05). There was no statistical difference between the depressive and normal groups regarding ethnicity and whether they had children.
Table 1 shows the participants' psychological responses and perceptions about the COVID-19 pandemic. The elderly people were divided into groups with and without depression. On declaring themselves to have a mental disorder, it was observed that the elderly people who claimed to be anxious and those who already had a diagnosis of depressive disorder were present in the group with depression (p < 0.001). On declaring themselves to have a mental disorder, it was observed that the elderly who claimed to be anxious and those who already had a diagnosis of depressive disorder were present in the depressive group (p < 0.001). There is a direct relationship between the number of mental diseases and the group that has depression, while people without any mental disorder are mostly present in the non-depressive group.
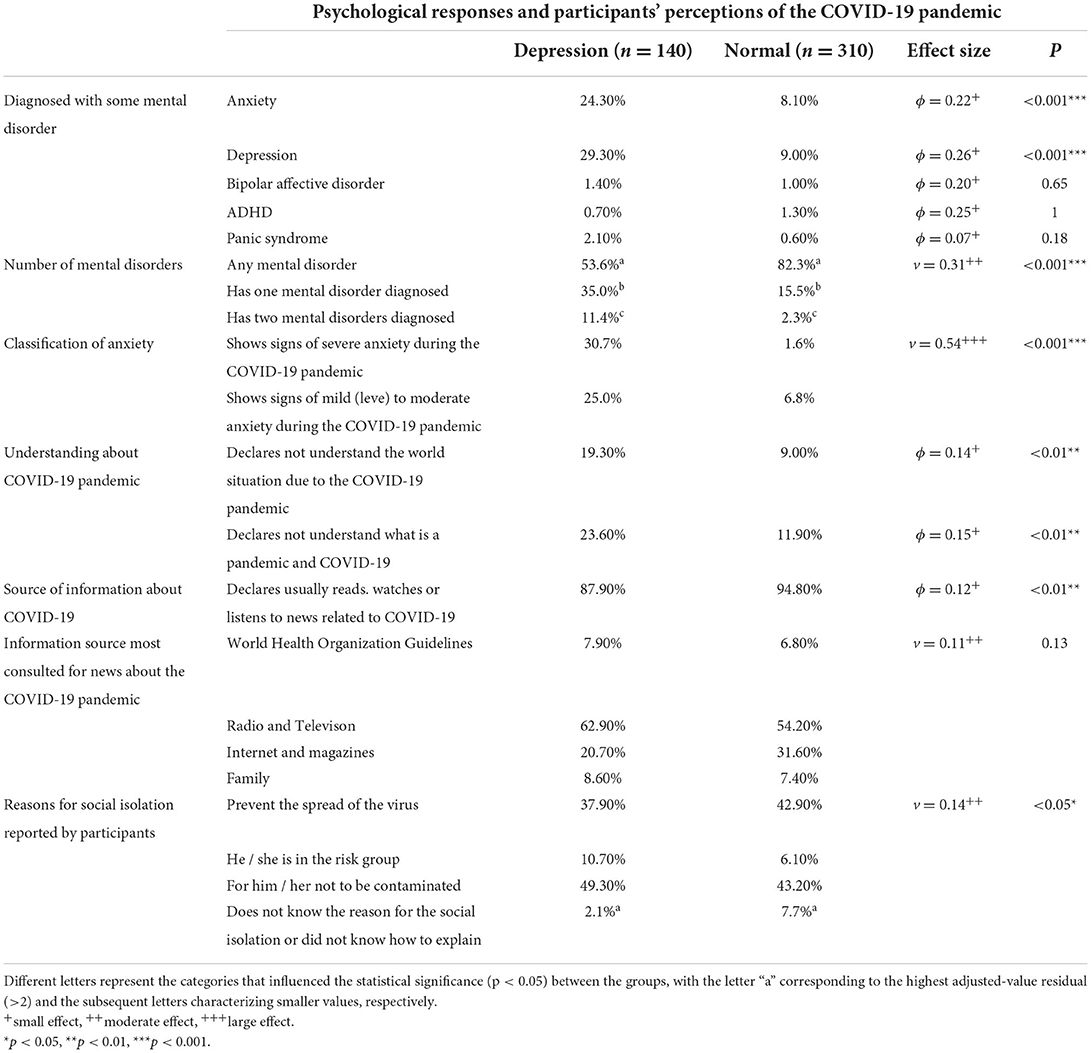
Table 1. Psychological responses and participants' perceptions about the COVID-19 pandemic.
Elderly with signs of severe (30.7%) and mild-to-moderate (25.0%) anxiety were predominant in depressive group (p < 0.001), having a large effect size (p < 0.001). Those who declared that they do not understand the situation that the world is going through, and who do not understand what a pandemic and COVID-19 is, most of them are present in the depressive group. Those who usually obtain information through reading, viewing, or listening to news about COVID-19 are present in the non-depressive group. There was no relevance among the sources of information used by the elderly to find out about the pandemic. As for the reason why the elderly person maintains social isolation, the elderly who declared not knowing or not understanding the reason for physical isolation predominated in the non-depressive group; this variable was the most influential (p < 0.05).
Of the characteristics with statistical value (p < 0.05), the most important to identify the groups is the presence or absence of anxiety symptoms, followed by education and civil status (Figure 2). In addition, the ranking showed that the importance of the other variables varies in a complex way among biological, psychological, and social factors.
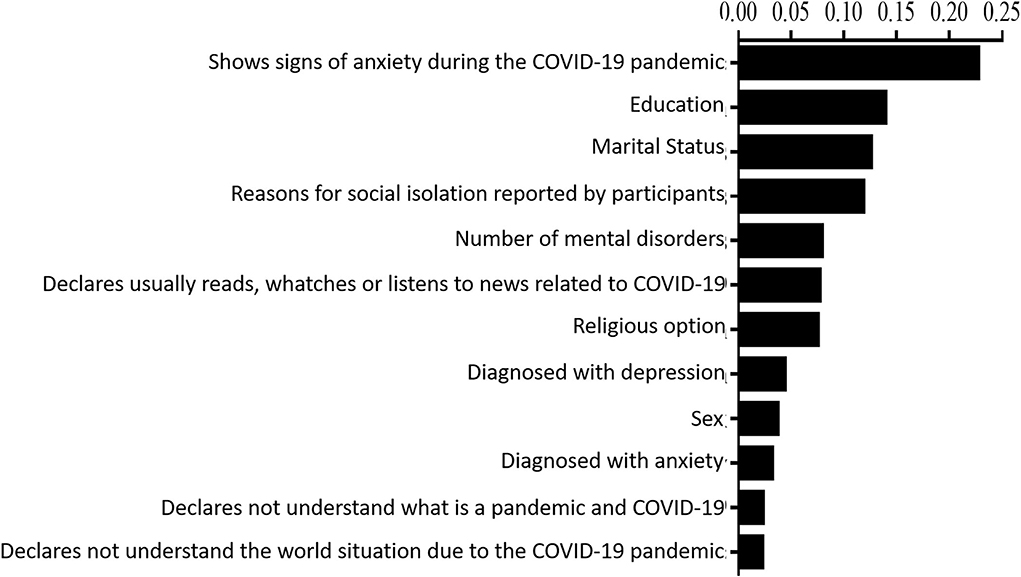
Figure 2. Importance of the variables for the characterization of the groups with and without depression. The figure shows the percentage importance of each variable that has statistical significance.
The COVID-19 pandemic was and is still considered an acute stressor for the general population (40). In addition, studies have shown that this event generated emotional deregulation that culminates in high psychological distress, triggering anxious and depressive symptoms, especially for older age groups (41, 42). Such an event contributed to a large number of people developing and exacerbating neurological disorders, which are determined by individual factors that affect the way each patient deals with a traumatic event, such as the pandemic (43).
In this study, we evaluated and identified the characteristics of Brazilian elderly people with and without depression in social isolation during the COVID-19 pandemic period, and which of them are more appropriate to characterize the elderly in depressive conditions. In general, the elderly in depressive conditions are mostly diagnosed with anxiety, have low education, and are widowed or unmarried.
We observed a predominance of women in the depressive group. This fact may be linked to the fact that women tend to be more vulnerable when subjected to stress and when developing post-traumatic symptoms, as a consequence of the intense routine required by the demands of work, child care, and daily routines (44). Our results corroborate previous studies (45, 46) that found an association between the female sex and psychological distress increasing.
Studies have observed that during social isolation there has been an increase in the number of cases of domestic violence against women in Brazil, in part, as a result of the longer time spent with couples or spouses (47, 48). The rise in this type of violence was an important factor for the development of depressive symptoms in women (47, 48).
We found that marital status is also associated with depression levels. In fact, widowed or divorced elderly people have a higher risk of feeling lonely and depressed (49). The loss of the spouse can cause an increase in depressive symptoms, and the absence of a partner is among the factors that lead the elderly to a state of social and emotional loneliness, favoring the onset of depressive symptoms (50).
Regarding religious conviction, the elderly of Afro-descendant religions belonged to the depressive group, while the elderly belonging to the non-depressive group and more informed about the pandemic declared not to have a religion. Therefore, we emphasize that new studies considering religious conviction among depressed elderly people need to be conducted to better investigate, characterize and understand the impact of this variable on the mental health of elderly people.
The fact of having or not having children was not statistically significant in determining the groups with and without depression. Nóbrega et al. (51) observed that the presence of depression in elderly Brazilians was independent of the fact of having children. Oliveira et al. (52) observed that elderly people who do not live with their children have a higher risk of feeling depressed, probably due to the feeling of loneliness. We emphasize that there is no consensus whether this variable is a factor directly related to the presence of depression in elderly.
The second most important variable to characterize depressed elderly people was their low educational level. These results corroborate previous studies that report that this condition influences the onset of anxiety and depression symptoms during old age (53, 54). The educational level is directly related to the economic level and quality of life, factors that are determinant for the index of depressive symptoms (55). It is recognized that the educational level is directly related to the economic level and quality of life, factors that are determinant for the index of depressive symptoms (44). These combined characteristics provide a state of pessimism that may result in the inability to confront these situations (56). In addition, the inability to read and interpret texts combined with limited access to information can be an obstacle for the elderly to obtain a minimum level of knowledge about protective measures against the coronavirus and to update themselves on their reality. Thus, this group may develop more concerns and, consequently, become more prone to the development of depressive symptoms (56).
Regarding the fact of having depression and previous diagnosis of other mental illnesses, the most elderly people with depressive disorders claimed to have another type of psychiatric disorder, mainly anxiety. We also identified that the most influential variable in determining elderly people with depressive disorder is the previous diagnosis of anxiety, since 55.7% of the elderly reported having symptoms of anxiety during the COVID-19 pandemic. These results corroborate the results of studies carried out in other countries during the pandemic (29). Anxiety is considered a possible risk factor for the onset of depression, and the simultaneous occurrence of these two psychopathologies among the elderly is frequent (57).
Elderly people in the non-depressive group stood out in terms of obtaining information about the pandemic and COVID-19 when compared to the depressive group. We emphasize that the individual in depression may develop feelings and thoughts of pessimism, helplessness, deep sadness, apathy, lack of initiative, physical discontent, difficulty in organizing and fluidity of ideas, impaired cognitive judgment, among other symptoms (58). Thus, such factors can compromise the ability of an individual affected by depression to obtain information, especially when related to COVID-19.
Participants who declared not knowing or not understanding the reason for physical isolation were predominant in the non-depressive elderly group. This result may be a consequence of data collection since the data were collected at the beginning of the pandemic, when the rigor of preventive measures imposed on the elderly population was lower and this group had no discernment of the COVID-19 complications. Thus, they probably became more prone to social isolation and, consequently, did not develop depressive symptoms.
We consider that the use of the electronic form could be a limitation for this study, since it could induce subjectivity in the interpretation of questions by the participants. To minimize this bias and before starting the study, we applied a pilot form with the aim of evaluating and improving the quality of the questions, alternative answers and avoiding possible misinterpretations. As a result of the adjustments, the final form is easier and clearer for elderly understanding.
Another limitation of this study was the impossibility of selecting, through “selection criteria,” only elderly people with the ability to handle electronic devices. This fact may have restricted the number of people who could have participated in the study, and consequently, may have been a bias. However, many of the elderly participants had the help of family members with such skill during the completion of the form, which may have reduced this bias. Although the study included participants from all Brazilian states, the predominance of women among the participants may have interfered with gender representation and may be a bias in terms of Brazilian population representation.
This study is important because it evaluated elderly people from all Brazilian states, which allowed the identification of the main mental characteristics of Brazilian elderly people affected by the pandemic period, considering the ethnic, social, and cultural plurality of this population (59). In additon, in this study, it was possible to recruit a large number of the participants and it was the only one to characterize the profile of mental health and the prevalence of depression associated with the pandemic period in the Brazilian elderly population.
With the results obtained in the study, which made it possible to know the characteristics of the elderly who developed or worsened symptoms of anxiety and depression, therapeutic strategies aimed at groups that are more likely to be anxious and depressive can be devised. People with mental illness or who share the characteristics found in the research may be unable or unwilling to protect themselves against COVID-19 due to apathy, depression, paranoia, or other psychiatric symptoms. Therefore, early identification of these symptoms is of fundamental importance for the resolution of the condition of these patients (60).
Overall, this study identified that for the sample of elderly people studied, the most important characteristics to identify the group with depression during the COVID-19 pandemic were (1) showing signs of anxiety during the COVID-19 pandemic; (2) of low education; (3) being divorced; (4) having more than one mental disorder; (5) reading, watching, or listening to information about COVID-19, and (6) being previously diagnosed with depression.
In conclusion, elderly Brazilians in social isolation tend to develop depressive disorders during quarantine. Having anxiety, low education, and marital status were the most important variables to characterize the depressive group. Thus, we can consider that the pandemic requires effective and safe gerontological care and monitoring, especially with regard to mental health.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Data collection was performed after approval of the Research Project by the Ethics Committee of the Institute of Health Sciences of the Federal University of Pará (CAAE number: 32893620.8.0000.0018). The patients/participants provided their written informed consent to participate in this study.
IS, OS, and FV: study conception and design. IS, RS, DL-J, AP, GC, AV, FT, OS, and FV: methodology and data collection. RS and MT: modeling and statistical analysis. IS, GC, AV, and FT: descriptive analysis. AP and DL-J: article editors. RS, MT, AP, DL-J, OS, and FV: scientific consultants and correction supervision. All authors contributed to the article and approved the submitted version.
We are grateful to PROPESP/UFPA (PAPQ) for funding the article publication fee. This study was partially funded by the Institutional Program for Scientific Initiation Scholarships (PIBIC) of the Federal University of Pará (UFPA), contemplating a scholarship (PRO4538-2020).
We thank the Study and Research Group on Health and Education in the Amazon – GEPSEA and the PIBIC of the Federal University of Pará (UFPA), which awarded a scientific initiation scholarship for the IS (PRO4538-2020).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.888234/full#supplementary-material
1. WHO. World Health Organization. Coronavirus (COVID-19) Dashboard. (2021). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance (accessed Sept 2, 2021),
2. Brasil MS. Coronavirus (covid-19) Panel in Brazil by the Ministry of Health. (2020). Available at: https://covid.saude.gov.br (accessed Aug 10, 2020).
3. Fiorillo A, Gorwood P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. J Eur Psychiatry.(2020) 63. doi: 10.1192/j.eurpsy.2020.35
4. Bridgland VM, Moeck EK, Green DM, Swain TL, Nayda DM, Matson LA, et al. Why the COVID-19 pandemic is a traumatic stressor. PloS ONE. (2021) 16:e0240146. doi: 10.1371/journal.pone.0240146
5. Unützer J, Kimmel RJ, Snowden M. Psychiatry in the age of COVID-19. World J Psychiatry. (2020) 19:130. doi: 10.1002/wps.20766
6. Perracini MR, De Amorim JSC, Lima CA, Da Silva A, Trombini-Souza F, Pereira DS, et al. Impact of COVID-19 pandemic on life-space mobility of older adults living in Brazil: REMOBILIZE study. J Front Public Health. (2021) 9:643640. doi: 10.3389/fpubh.2021.643640
7. Romero DE, Muzy J, Damacena GN, Souza NAd, Almeida WdSd, Szwarcwald CL, et al. Older adults in the context of the COVID-19 pandemic in Brazil: effects on health, income and work. J Cadernos de Saúde Pública. (2021) 37:e00216620. doi: 10.1590/0102-311x00216620
8. Choi EPH, Hui BPH, Wan EYF. Depression and anxiety in Hong Kong during COVID-19. Int J Environ Res Public Health. (2020) 17:3740. doi: 10.3390/ijerph17103740
9. Jordan RE, Adab P, Cheng K. Covid-19: risk factors for severe disease and death. BMJ. (2020) 368:m1198. doi: 10.1136/bmj.m1198
10. Barbosa IR, Galvão MHR, Souza TA, Gomes SM, Medeiros AdA, Lima KC. Incidence of and mortality from COVID-19 in the older Brazilian population and its relationship with contextual indicators: an ecological study. Rev Bras Geriatr Gerontol. (2020) 23:e200171. doi: 10.1590/1981-22562020023.200171
11. da Silva Marçal DF, Gaspar PAA. de Lima LT, Coelho DT, Reinaldo JZ, Dechen VM, et al. Mortality from COVID-19 and vaccination in the elderly: an ecological study in the city of Curitiba, Paraná, Brazil. J Infects Dis. (2022) 26:102039. doi: 10.1016/j.bjid.2021.102039
12. Orellana JDY. Cunha GMd, Marrero L, Leite IdC, Domingues CMAS, Horta BL. Changes in the pattern of hospitalizations and deaths from COVID-19 after substantial vaccination of the elderly in Manaus, Amazonas, Brazil. Cad Saude Publica. (2022) 38:PT192321. doi: 10.1590/0102-311xpt192321
13. Klinenberg E. Social isolation, loneliness, and living alone: identifying the risks for public health. Am J Public Health. (2016) 106:786–7. doi: 10.2105/AJPH.2016.303166
14. Armitage R, Nellums LB. COVID-19 and the consequences of isolating the elderly. J Lancet Public Health. (2020) 5:e256. doi: 10.1016/S2468-2667(20)30061-X
15. Santini ZI, Jose PE, Cornwell EY, Koyanagi A, Nielsen L, Hinrichsen C, et al. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): a longitudinal mediation analysis. J Lancet Public Health. (2020) 5:e62–70. doi: 10.1016/S2468-2667(19)30230-0
16. Lábadi B, Arató N, Budai T, Inhóf O, Stecina DT, Sík A, et al. Psychological wellbeing and coping strategies of elderly people during the COVID-19 pandemic in Hungary. J Aging Mental Health. (2022) 26:570–7. doi: 10.1080/13607863.2021.1902469
17. Aurélio SS. Physical Activity in Combating the Incidence of Depression and Anxiety in the COVID-19 Pandemic: A Literature Review. (2020). Available online at: https://repositorio.animaeducacao.com.br/handle/ANIMA/12635 (accessed May 20, 2021).
18. Kurebayashi LFS, Gnatta JR, Borges TP, da Silva MJP. Traditional Chinese Medicine diagnostic evaluation of stress symptoms treated by auriculotherapy: clinical trial. J Rev Eletr Enf . (2014) 16:68–76. doi: 10.5216/ree.v16i1.20167
19. Telles-Correia D, Barbosa A. Anxiety and depression in medicine: theoretical models and evaluation. J Acta Med Port. (2009) 22:89–98.
20. Drago SMMS, Martins RML. Depression in the elderly. Asia Pac Psychiatry. (2011) 3:46–53 doi: 10.1111/j.1758-5872.2011.00119.x
21. World Health Organization. The Injury Chart Book: A Graphical Overview of the Global Burden of Injuries. World Health Organization 2002 (2002).
22. Webb L. Covid-19 lockdown: a perfect storm for older people's mental health. J Psychiatr Ment Health Nurs. (2020) 28:300. doi: 10.1111/jpm.12644
23. Queiroz MIP. Cultural identity, national identity in Brazil. J Tempo soc. (1989) 1:29–46. doi: 10.1590/ts.v1i1.83318
24. Mendonça AG. Republic and religious plurality in Brazil. J Revista USP. (2003) 59:144–63. doi: 10.11606/issn.2316-9036.v0i59p144-163
25. Viana SAA, Lima Silva M, Lima PT. Impact on the mental health of the elderly during the period of social isolation due to the spread of the COVID-19 disease: a literary review. Diálogos Saúde. (2020) 3:1–16.
26. Lima Monteiro IV, Figueiredo JFC, Cayana EG. Elderly and mental health: impacts of the COVID-19 Pandemic. Braz J Med Biol Res. (2021) 4:6050–61. doi: 10.34119/bjhrv4n2-162
27. Almeida Costa F, Santos Silva AO. Caio Bismarck Silva, Costa LCS, Silva Paixão MÉ, Celestino MNS, et al. COVID-19: its clinical and psychological impacts on the elderly population. Braz Dev. (2020) 6:49811–24. doi: 10.34117/bjdv6n7-580
28. Oliveira VV, Oliveira LVV, Rocha MR, Leite IA, Lisboa RSA, Kelly CL. Impacts of social isolation on the mental health of the elderly during the COVID-19 pandemic. Braz J Health Rev. (2021) 4:3718–27. doi: 10.34119/bjhrv4n1-294
29. Wang Z, Qi S, Zhang H, Mao P, He Y, Li J, et al. Impact of the COVID-19 epidemic on anxiety among the elderly in community. J Zhonghua yi xue za zhi. (2020) 100:3179–85. doi: 10.3760/cma.j.cn112137-20200720-02167
30. Ozamiz NE, Dosil MS, Picaza MG, Idoiaga NM. Niveles de estrés, ansiedad y depresión en la primera fase del brote del COVID-19 en una muestra recogida en el norte de España. Cad Saude Publica. (2020) 36:e00054020. doi: 10.1590/0102-311x00054020
31. Gorrochategi MP, Munitis AE, Santamaria MD, Etxebarria NO. Stress, anxiety, and depression in people aged over 60 in the COVID-19 outbreak in a sample collected in Northern Spain. Am J Geriatr Psychiatry. (2020) 28:993–8. doi: 10.1016/j.jagp.2020.05.022
32. García-Fernández L, Romero-Ferreiro V, López-Roldán P, Padilla S, Rodriguez-Jimenez R. Mental health in elderly Spanish people in times of COVID-19 outbreak. Am J Geriatr Psychiatry. (2020) 28:1040–5. doi: 10.1016/j.jagp.2020.06.027
33. Iasevoli F, Fornaro M, D'Urso G, Galletta D, Casella C, Paternoster M, et al. Psychological distress in patients with serious mental illness during the COVID-19 outbreak and one-month mass quarantine in Italy. Psychol Med. (2021) 51:1054–6. doi: 10.1017/S0033291720001841
34. Martiny C, de Oliveira Silva AC, Nardi AE, Pachana NA. Translation and cross-cultural adaptation of the Brazilian version of the geriatric anxiety inventory (GAI)/Traducao e adaptacao transcultural da versao Brasileira do inventario de ansiedade geriatrica (GAI). Rev Psiquiatr Clin. (2011) 38:8–13. doi: 10.1590/S0101-60832011000100003
35. Pachana NA, Byrne GJ, Siddle H, Koloski N, Harley E, Arnold E. Development and validation of the geriatric anxiety inventory. Int Psychogeriatr. (2007) 19:103–14. doi: 10.1017/S1041610206003504
36. Almeida OP, Almeida SA. Short versions of the geriatric depression scale: a study of their validity for the diagnosis of a major depressive episode according to ICD-10 and DSM-IV. Int J Geriatr Psychiatry. (1999) 14:858–65. doi: 10.1002/(SICI)1099-1166(199910)14:10<858::AID-GPS35>3.0.CO;2-8
37. Fritz CO, Morris PE, Richler JJ. Effect size estimates: current use, calculations, and interpretation. J Exp Psychol Gen. (2012) 141:2–18. doi: 10.1037/a0024338
38. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Cambridge, MA: Academic press. (2013). doi: 10.4324/9780203771587
39. Russell Stuart J, Norvig P. Artificial Intelligence: A Modern Approach. Upper Saddle River, NJ: Prentice Hall Press. (2009).
40. Moccia L, Janiri D, Giuseppin G, Agrifoglio B, Monti L, Mazza M, et al. Reduced hedonic tone and emotion dysregulation predict depressive symptoms severity during the COVID-19 outbreak: an observational study on the Italian general population. Int J Environ Res Public Health. (2021) 18:255. doi: 10.3390/ijerph18010255
41. Janiri D, Kotzalidis G, Giuseppin G, Molinaro M, Modica M, Montanari S. Psychological distress after COVID-19 recovery: reciprocal effects with temperament and emotional dysregulation. An exploratory study of patients over 60 years of age assessed in a post-acute care service. Front Psychiatry. (2020) 11:590135. doi: 10.3389/fpsyt.2020.590135
42. Zaninotto P, Iob E, Demakakos P, Steptoe A. Immediate and longer-term changes in the mental health and wellbeing of older adults in England during the COVID-19 pandemic. J JAMA Psychiatry. (2022) 79:151–9. doi: 10.1001/jamapsychiatry.2021.3749
43. Piano C, Di Stasio E, Primiano G, Janiri D, Luigetti M, Frisullo G, et al. An Italian neurology outpatient clinic facing SARS-CoV-2 pandemic: data from 2,167 patients. Front Neurol. (2020) 11:564. doi: 10.3389/fneur.2020.00564
44. Sareen J, Erickson J, Medved MI, Asmundson GJ, Enns MW, Stein M, et al. Risk factors for post-injury mental health problems. Depress Anxiety. (2013) 30:321–7. doi: 10.1002/da.22077
45. Barros MBA, Lima MG. Malta DC, Szwarcwald CL, Azevedo RCSd, Romero D, et al. Report of sadness/depression, nervousness/anxiety and sleep problems in the Brazilian adult population during the COVID-19 pandemic. Epidemiol serv saude. (2020) 29:e2020427.
46. Meng H, Xu Y, Dai J, Zhang Y, Liu B, Yang H. Analyze the psychological impact of COVID-19 among the elderly population in China and make corresponding suggestions. J Psychiatry Res. (2020) 289:112983. doi: 10.1016/j.psychres.2020.112983
47. Barbosa TR. Confronting Domestic Violence Against Women in the Context of a Pandemic. (2020). Available online at: http://ri.ucsal.br:8080/jspui/handle/prefix/2729 (accessed Jun 2, 2021).
48. Morais AC. Depression in Women Victims of Domestic Violence. (2009). [Masters dissertation]. Available online at: https://repositorio.ufba.br/ri/bitstream/ri/11425/1/Disserta%C3%A7%C3%A3o_Enf_Ariane%20Cedraz%20Morais.pdf (Accessed May 12, 2021).
49. Oliveira LM, Abrantes GG, Ribeiro GS, Cunha NM, Pontes MLF, Vasconcelos SC. Loneliness in senescence and its relationship with depressive symptoms: an integrative review. Rev Bras Geriatr Gerontol. (2020) 22:e190241. doi: 10.1590/1981-22562019022.190241
50. Ramos M, Wilmoth J. Social relationships and depressive symptoms among older adults in southern Brazil. J Gerontol B Psychol Sci Soc Sci. (2003) 58:S253–S61. doi: 10.1093/geronb/58.4.S253
51. Nóbrega IRAP, Leal MCC. Marques APO, Vieira JCM. Factors associated with depression in institutionalized elderly: an integrative review. J Saúde em Debate. (2015) 39:536–50. doi: 10.1590/0103-110420151050002020
52. Oliveira MCGM, Salmazo-Silva H, Gomes L, Moraes CF, Alves VP. Elderly individuals in multigenerational households: Family composition, satisfaction with life and social involvement. Estud Psicol. (2020) 37:e180081. doi: 10.1590/1982-0275202037e180081
53. Almeida MASO, Lemes AG, do Nascimento VF, da Fonseca PIMN, da Rocha EM, Volpato RJ, et al. Risk factors associated with depression in the elderly in the interior of Mato Grosso. Rev Saude Publica. (2015) 39:627. doi: 10.22278/2318-2660.2015.v39.n3.a1895
54. Pardal A. Social Support, Symptoms of Anxiety and Depression and Life Satisfaction in the Elderly Under Social Response. (2011). Available online at http://repositorio.ismt.pt/jspui/handle/123456789/129 (accessed May 10, 2021).
55. Minghelli B, Tomé B, Nunes C, Neves A, Simões C. Comparison of anxiety and depression levels between active and sedentary elderly. Arch Clin Psychiatry. (2013) 40:71–6. doi: 10.1590/S0101-60832013000200004
56. Almeida-Filho N, Lessa I, Magalhães L, Araújo MJ, Aquino E, James SA, et al. Social inequality and depressive disorders in Bahia, Brazil: interactions of gender, ethnicity, and social class. Soc Sci Med. (2004) 59:1339–53. doi: 10.1016/j.socscimed.2003.11.037
57. Maximiano-Barreto MA, Oliveira Fermoseli AF. Prevalence of anxiety and depression in elderly people with low education in Maceió/Al. J Psicologia, Saúde e Doenças. (2017) 18:801–13. doi: 10.15309/17psd180314
58. Sougey EB, Del Porto JA. Brasil MA, Juruena MF. Guidelines of the Brazilian medical association for the treatment of depression. Braz J Psychiatry. (2003) 25:114–22. doi: 10.1590/S1516-44462003000200013
59. Canen A. Multicultural education, national identity and cultural plurality: tensions and curricular implications. Cad Pesqui. (2000) 111:135–49. doi: 10.1590/S0100-15742000000300007
Keywords: COVID-19, social isolation, elderly, mental health, anxiety, depression
Citation: Sousa ILMd, Silveira R, Takito MY, Pereira AL, Lucianelli-Júnior D, Carmona GS, Viegas APdV, Teixeira FB, Santos OS and Valentin FN (2022) The impact of the social isolation in elderly Brazilian mental health (anxiety and depression) during the COVID-19 pandemic. Front. Psychiatry 13:888234. doi: 10.3389/fpsyt.2022.888234
Received: 02 March 2022; Accepted: 05 August 2022;
Published: 08 September 2022.
Edited by:
Michael Noll-Hussong, Saarland University, GermanyReviewed by:
Gaia Sampogna, University of Campania L. Vanvitelli, ItalyCopyright © 2022 Sousa, Silveira, Takito, Pereira, Lucianelli-Júnior, Carmona, Viegas, Teixeira, Santos and Valentin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ozélia Sousa Santos, b3plbGlhc291c2FAdWZwYS5icg==; Fernanda Nogueira Valentin, ZmVyX3ZhbGVudGluQHlhaG9vLmNvbS5icg==
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.