
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 19 May 2022
Sec. Public Mental Health
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.869326
This article is part of the Research TopicMental Illness, Culture, and Society: Dealing with the COVID-19 PandemicView all 44 articles
 Giulia Menculini1†
Giulia Menculini1† Giorgio Pomili1†
Giorgio Pomili1† Francesca Brufani1Agnese Minuti1Niccolò Mancini1Martina D’Angelo2Sonia Biscontini3Enrico Mancini4Andrea Savini4
Francesca Brufani1Agnese Minuti1Niccolò Mancini1Martina D’Angelo2Sonia Biscontini3Enrico Mancini4Andrea Savini4 Laura Orsolini5
Laura Orsolini5 Umberto Volpe5Alfonso Tortorella1
Umberto Volpe5Alfonso Tortorella1 Luca Steardo Jr.2*
Luca Steardo Jr.2*Introduction: Adolescents and young adults represent a vulnerable population in the context of the Coronavirus disease 2019 (COVID-19) pandemic. The present retrospective study aims to investigate the pandemic’s psychological impact on adolescents and young adults by analyzing data from an outpatient mental health service dedicated to youths in Umbria, central Italy.
Materials and Methods: The clinical charts of subjects aged 14–24 who first accessed the service in the timeframe between March 1st, 2019, and February 28th, 2021, were reviewed. Subjects were divided into two subgroups according to the period of time when they accessed the service (pre-COVID-19 vs. during- COVID-19 outbreak). Bivariate analyses were performed using the Chi-square test and the Welch’s t-test. A secondary analysis was performed considering only subjects suffering from psychiatric disorders. Furthermore, data concerning individuals who were already followed by the service before the pandemic were analyzed by the McNemar’s test and the t-paired test to assess changes in treatment features.
Results: The number of new accesses during the pandemic period remained stable. After the emergency onset, youths accessing the service showed a higher prevalence of anxiety disorders (p = 0.022). During the COVID-19 period, services were more frequently delivered by using a digital mental health approach (p = 0.001). Psychopharmacological treatment was more frequently prescribed among subjects that were referred to the service after the pandemic onset (p = 0.033). As for substance use, a highly significant reduction in opioid use was observed (p = 0.003). Family therapy was delivered less frequently in the during-COVID-19 subgroup, especially in the subpopulation of subjects suffering from psychiatric disorders (p = 0.013). When considering subjects referred to the service in the pre-COVID-19 period, the number of interventions provided to this population increased after the pandemic outbreak (p = 0.038).
Conclusion: In the context of the COVID-19-related public health crisis, youths represent an at-risk population for which pathways to care should be reinforced, and targeted interventions, including psychosocial treatments, should be implemented.
The Coronavirus disease 2019 (COVID-19) pandemic represents an unprecedented health emergency affecting healthcare systems worldwide, with serious socioeconomic consequences (1). In the complex scenario that arose from the infection spread, mental health was prioritized because of the high psychological distress caused by social distancing and isolation (2, 3). Indeed, an increasing prevalence of anxiety, depression, irritability, and insomnia has been documented among the general population after the COVID-19 outbreak (4). The COVID-19 pandemic hit Italy consistently, and data from the epidemiological register of the Umbria region, in the center of the country, also reported a dramatic increase in the curve since the beginning of the pandemic spread (5). The rise in contagions forced the regional council to adopt severe restrictive measures to preserve the proper functioning of the hospital and healthcare network, with high psychopathological distress for the population. Indeed, previous reports underlined that the mental health of the general population in central Italy was significantly impacted by the pandemic, as also demonstrated by the increase of psychiatric consultations in emergency services (6).
However, the risk of developing COVID-19-related psychological distress was particularly high in vulnerable populations, such as in subjects aged 16–24 years old, who represented one of the groups most affected by the pandemic emergency (7–10). Lockdown measures had an unfavorable impact on adolescents and young adults, and a large amount of literature highlighted a greater risk for the occurrence of psychiatric symptoms due to a change in their lifestyles and habits (11) as well as lower levels of post-traumatic growth (12). For instance, the closure of schools has imposed distance learning as an alternative to maintain continuity in the education of children and adolescents (13). The subsequent prolonged social isolation threatened the psycho-physical wellbeing of youths, worsening or unmasking psychopathology (14). During the pandemic, there has been a widespread increase in depression, anxiety, irritability among children, and adolescents, and suicidal behaviors (8, 15, 16). Studies conducted in Italy already demonstrated a high prevalence of moderate or severe anxiety among youths (17), as well as a higher risk for developing problematic internet use in this population during the pandemic (18).
Furthermore, limitations due to infection imposed an adaptation in the availability of psychiatric and psychosocial interventions in dedicated settings, which were pointed out as critical needs for this population (19–21). For this reason, implementing telepsychiatry and integrating interventions to maintain regular and emergency child and adolescent psychiatric treatment during the pandemic was identified as a significant challenge that could be necessary for limiting long-term consequences on mental health (22). In fact, integrated intervention programs (medical intervention, psychotherapy, psychoeducation to family members, social intervention) seem to have a considerably better impact than treatment-as-usual in the youth population, especially at disease onset (23).
Several countries had already allocated tailored funding for the mental health of adolescents and young adults before the pandemic (24) and conducted specific campaigns to address children and young people’s mental health in the COVID-19 era (25). To this end, the European Year of Youth 2022 presents an opportunity for countries and organizations to enhance health promotion initiatives and focus on mitigating mental health problems in this population (26).
Within this scenario, the Italian Umbria region had already decided to allocate specific funds to widen the possibility of mental health departments supporting youths with psychopathological distress. The Addiction Service (SerD) of Local Mental Health 2 (USL Umbria 2) in Foligno agreed with the Umbria region to expand its curative offer by implementing an outpatient service dedicated to adolescents and young adults who present psychological distress.
Based on these premises, the present study aimed to investigate the pandemic’s impact on adolescents and young adults, analyzing data from the abovementioned outpatient youth mental health service. Notably, changes in access to mental health care, clinical and treatment features of patients in charge of the service before the pandemic were furtherly analyzed. A secondary analysis was performed to evaluate access to care and changes in clinical and treatment features of subjects suffering from psychiatric disorders. Particularly, we expect to detect significant changes in diagnostic and treatment (both psychopharmacological and psychosocial) features after the COVID-19 outbreak, possibly reflecting differences in pathways to care and patterns of care for this population.
The present study was performed by carrying out a retrospective chart review analysis of clinical data collected during the time period between March 1st, 2019 and February 28th, 2021, at the Addiction Service (SerD) of Local Mental Health 2 (USL Umbria 2) in Foligno, Umbria, Italy. Clinical charts of subjects aged 14–24 who first accessed the service between March 1st, 2019, and February 28th, 2021, were retrospectively reviewed. In the study, we included both subjects who had a personal history of substance use disorders (SUD) and subjects who reported no history of SUD. Indeed, SUD can also be considered an early sign of psychological distress in youths and may represent a “red flag” for the later development of clear-cut psychiatric symptoms (27).
Information concerning the personal and clinical history of the included subjects was extracted from the electronic medical charts achieved from the online platform PoInT GeDi (28). Data were inserted in two electronic datasets created ad hoc for the current project. In the first dataset, subjects who first accessed the service between March 1st, 2019, and February 28th, 2021, were entered. This population was then divided in two subgroups, namely subjects who had accessed the service for the first time in the period March 1st, 2019, and February 28th, 2020 (pre-COVID-19 period) and those who referred to the service for the first time in the period March 1st, 2020 and February 28th, 2021 (during-COVID-19 period). Indeed, the national lockdown was established in Italy on March 9th, 2020, which also concerned the Umbria region. Furthermore, the first case of COVID-19 was confirmed in Italy at the end of February 2020, and an increase in COVID-19 cases and related hospitalizations registered in Umbria at the beginning of March (29). This dataset was used to compare socio-demographic, clinical, and treatment characteristics among the two populations to evaluate significant differences between subjects who accessed the service before and after the pandemic outbreak and between the treatments provided in the two populations in the two different periods. Socio-demographic data collected for the included subjects were age, gender, nationality, marital status, scholarity, working status, and living status. As for clinical information, data concerning medical comorbidities, SUD (alcohol, amphetamines, cannabinoids, cocaine, and heroin), psychiatric diagnosis, suicide attempts, and non-suicidal self-injurious behavior was collected. Moreover, we extracted the following treatment-related features: current psychopharmacological treatment (antidepressants, antipsychotics, benzodiazepines, mood stabilizers), replacement treatment for addiction, other pharmacological treatments, psychosocial interventions (individual psychotherapy, family therapy, social, and educational interventions), and treatment in a residential facility.
Only subjects who first accessed the service in the pre-COVID-19 period were considered in the second dataset. Information concerning treatments provided before and after the pandemic was collected to analyze significant changes in treatment features possibly related to the COVID-19 pandemic. Data concerning clinical characteristics and treatment features (see above) was collected for both pre- and during-pandemic periods.
To address the secondary aim of the study, a further analysis was performed on a subsample of subjects suffering from psychiatric disorders. The following nosographic entities were considered: schizophrenia spectrum disorders, depressive disorders, bipolar disorders, anxiety disorders, impulse control disorders, neurodevelopmental disorders, substance-related disorders, personality disorders, and adjustment disorders. Trained psychiatrists and psychologists with specific expertise on youth mental health carried out the diagnostic evaluation by using the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) (30). Subjects affected by neurocognitive disorders or medical illnesses that might significantly influence mental health status were excluded. The analysis was then repeated following the aforementioned procedure, focusing on this subsample.
According to the study’s observational nature, all the included subjects underwent treatment as usual. The study was conducted in accordance with Declaration of Helsinki and followed the Good Clinical Practice Guidelines. All the included subjects signed their informed consent for having their data used for research purposes. In the case of minors, informed consent was also obtained by parents or those who exercised parental authority. The study protocol was approved by the Ethics Committee of Umbria Region (protocol N° 23369/21/ON).
The facility where the study was carried out is a multidisciplinary service aimed at providing health promotion, prevention, and treatment of people with problems of addiction to legal or illegal psychoactive substances (drugs, alcohol, smoking), or addiction without the use of substances (e.g., gambling and video addiction). The service is equipped with specific facilities dedicated to youth suffering from psychological distress, with separate pathways for those who report SUD, including alcohol, and those who do not. Indeed, despite the service itself being dedicated to addiction problems, the growing number of youths reporting mental health problems led to the institution of a specific project addressed to young people with psychological distress without SUD comorbidity. This path of care is part of two specific projects, named “Girovento” and “Giovani 2.0.” These projects attempt to address the need for new clinical-organizational responses concerning increasingly complex requests coming from youths in the fourteen-twenty-four age group; all these treatment pathways operate in close integration with the services of child and adolescent psychiatry, inpatient, and outpatient community mental health services for adults, and with the school psychologists consulting service, as well as with social services.
The multidisciplinary team discusses weekly the clinical cases of subjects who access these projects, identifying and elaborating individualized therapeutic projects, e.g., individual psychotherapy, family therapy, social and educational interventions, peer groups and support groups addressed to parents. Psychiatric evaluation and treatment are also provided whenever needed.
A descriptive analysis of socio-demographic, clinical, diagnostic, and treatment features was performed to evaluate the distributional properties of the variables in the study sample. Categorical variables were expressed as frequencies, while continuous variables were expressed as mean and standard deviation (SD) or median and interquartile range (IQR) according to the normality of the distribution. The normality of continuous variables was verified by using the Kolmogorov-Smirnov test.
Bivariate analyses were carried out to compare the subgroups of subjects who accessed the service before and after the pandemic outbreak. We performed the Chi-Square test for categorical variables since levels of the variables were mutually exclusive and the compared groups were independent. All tests were performed for 2 × 2 cross tabs. The assumption according to which the expected cell count should be ≥ 5 in at least 80% of the cells was verified for all tests, and when this assumption was not met the Fisher’s exact test was carried out (31, 32). The Welch’s t-test was used for continuous variables due to the presence of outliers. The analysis was conducted using a parametric test due to the sensitivity of this technique, which guarantees sufficient robustness in case of normality assumption violation in sample sizes like the one we considered (33–35). In order to assess differences concerning the pre- and during-COVID-19 period for subjects who first accessed the service before the pandemic break, the Mc Nemar’s test was used for categorical variables since we attempted to find statistically significant differences in paired variables categorized as dichotomous. The sample consisted of all youths accessing the service, and since no restrictions in access to the service were established (e.g., presentation modalities, area of residence), the sample could be considered as representative of the population of interest (youths accessing to care in the Umbria region). The Student’s t-test for paired samples was employed for continuous variables. We chose not to apply a p-value correction (e.g., Bonferroni correction) to avoid type II errors. Indeed, we conducted exploratory analyses for testing a hypothesis mainly concerning two groups of variables, namely diagnostic and treatment features, and thus did not want to miss possible significant association worthy of being further explored (36). All p-values were two-tailed. Since the reporting of results according to a continuous approach rather than to a fixed threshold (e.g., p < 0.05) has been largely advocated (37, 38), findings from the present study will be presented in terms of high (p < 0.01), medium (p < 0.05 and ≥ 0.01), and low (p < 0.1 and ≥ 0.05) significance. All analyses were performed using the Statistical Package for Social Sciences (SPSS) version 26 for Windows Inc. (Chicago, IL, United States).
The overall study population consisted of 110 subjects, with a higher prevalence of male gender (n = 77, 70%) and a median age of 19 ± years old (IQR 5, range 14–24). Most subjects in the sample were Italian (n = 97, 88.2%). None of the included subjects was married, and the majority lived with their family of origin (n = 77, 70%). As for working status, 56 (50.9%) were current students, whilst 19 (17.3%) did not study or work. In the sample, 57 (51.8%) youths were referred to the service before the COVID-19 pandemic outbreak and 53 (48.2%) had their first contact after the pandemic spread. The most frequently reported addictive behavior was alcohol use (n = 35, 31.8%), followed by cannabis use (n = 31, 28.2%).
Subjects suffering from a psychiatric disorder were 79 (71.8%), among which 48 (60.8%) were males. The median age in the sample was 18 (IQR 4) years old, ranging from 14 to 24. When analyzing the period when youths referred to the service, 42 (53.2%) accessed the outpatient facility before the COVID-19 outbreak. Most subjects in this subsample lived with their family of origin (n = 65, 82.3%), while a minority of them lived in residential facilities (n = 7, 8.9%) or on their own (n = 6, 7.6%). At the time of clinical assessment, 53 subjects (67.1%) were students, while 14 (17.7%) did not study or work. In this subsample, the most common psychiatric disorders were represented by anxiety disorders (n = 37, 46.8%) and adjustment disorders (n = 22, 27.8%). Concerning addictive behaviors, most subjects reported cannabis use (n = 29, 36.7%) (see Tables 1, 2). Six (7.6%) subjects presented self-aggressive behaviors, and one attempted suicide. Psychopharmacological treatment was prescribed in 21 (19.9%) subjects in the overall sample. Particularly, antipsychotics were prescribed to 10 (9.1%) subjects, while five (4.5%) received antidepressants, 10 (9.1%) took mood stabilizers, and seven (6.4%) underwent anxiolytics prescription. As for psychosocial interventions, individual psychotherapy was delivered to 72 (65.5%) subjects, and family therapy was provided in 17 (15.5%) cases. Moreover, 49 (44.5%) and 20 (18.2%) subjects underwent social-educational interventions.
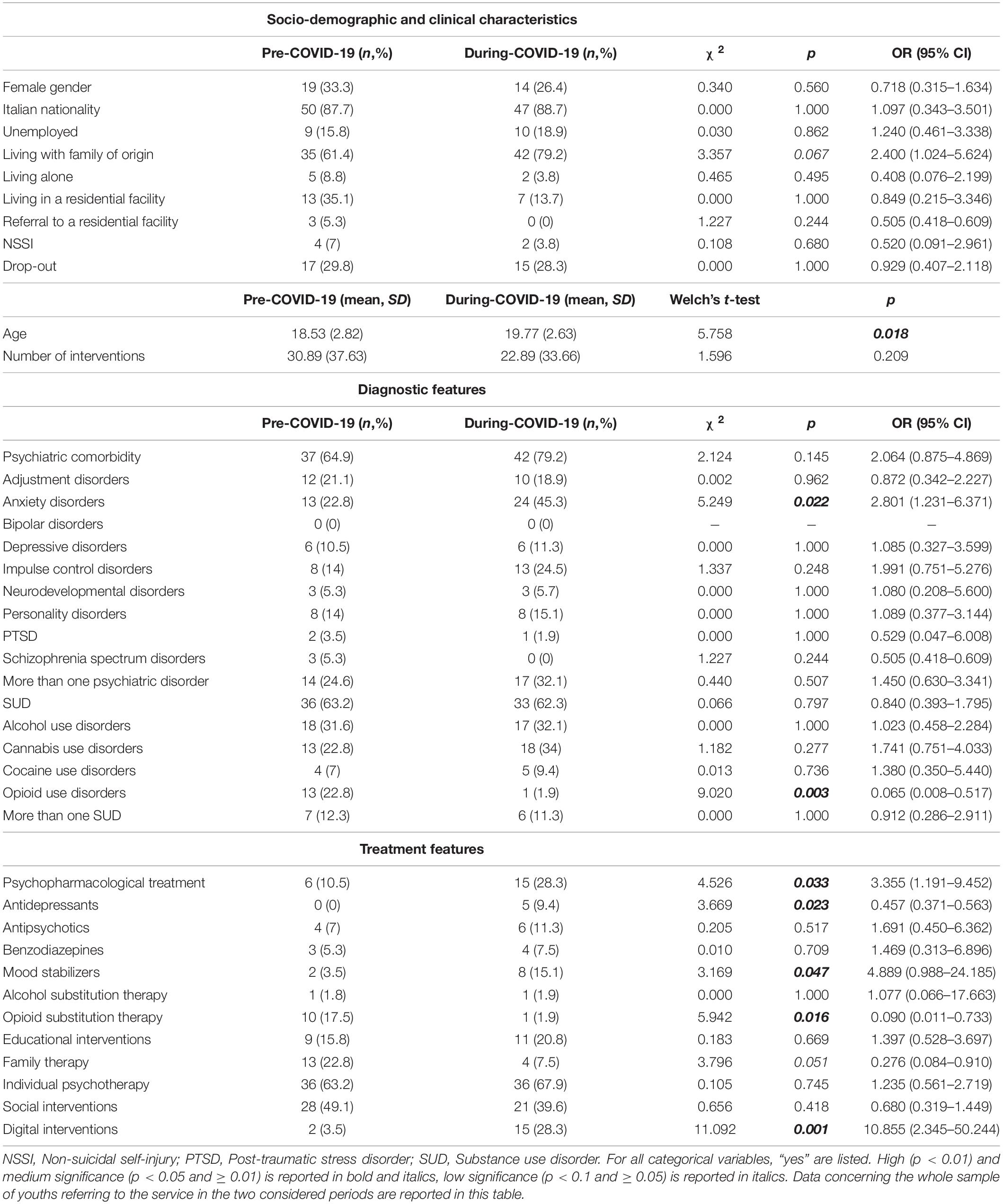
Table 1. Comparison of socio-demographic and clinical characteristics of subjects accessing the service before (pre-COVID-19; n = 57, 51.8%) and after the COVID-19 pandemic outbreak (during-COVID-19; n = 53, 48.2%).
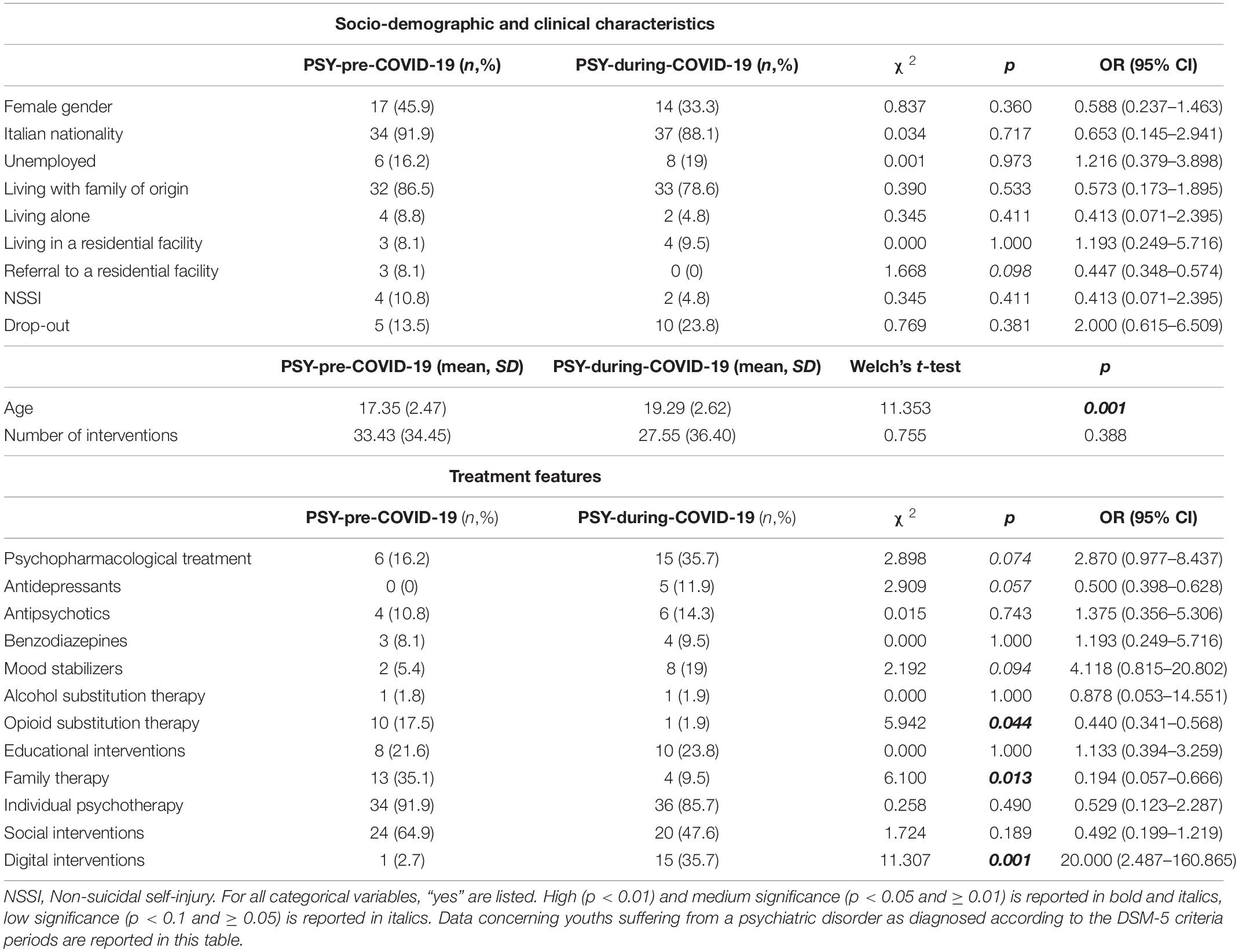
Table 2. Comparison of socio-demographic and clinical characteristics of subjects accessing the service before (PSY-pre-COVID-19; n = 37, 46.8%) and after the COVID-19 pandemic outbreak (PSY-during-COVID-19; n = 42, 53.2%).
When comparing subjects accessing the service before (n = 57, 51.8%) and during the COVID-19 pandemic (n = 53, 48.2%), no differences in socio-demographic characteristics were found regarding gender and occupation. Subjects accessing the service after the pandemic started were older than those referred before the COVID-19 outbreak (mean age 19.77 ± 2.63 vs. 18.53 ± 2.82), and more often lived with their family of origin (79.2% vs. 61.4%), respectively with a medium (p = 0.018) and low (p = 0.067) significance.
When assessing addictive behaviors in the two subgroups, no differences were detected between subjects accessing the service before and during the COVID-19 pandemic except for opioid use, which was highly more prevalent in the pre-pandemic sample (22.8% vs. 1.9%, p = 0.003). Furthermore, youths accessing the service after the emergency onset showed a higher prevalence of anxiety disorders (45.3% vs. 22.8%, p = 0.022).
The two subgroups did not differ in the number of psychiatric visits and psychosocial interventions supplied. After the COVID-19 outbreak, services were more frequently delivered using a digital mental health approach (28.3% vs. 3.5%), with a high significance of the result (p = 0.001). No significant differences were detected in terms of drop-out rates.
A medium significance was found for differences in the prescrition of psychopharmacological treatment, which was more frequently prescribed among subjects that were referred to the service after the pandemic (28.3% vs. 10.5%, p = 0.033). Particularly, antidepressant and mood stabilizer prescription rates were higher after the COVID-19 outbreak (9.4% vs. 0%, p = 0.023; 15.1% vs. 3.5%, p = 0.047). When assessing changes in the delivery of psychosocial interventions, we evidenced a reduction in family therapy in the during-COVID-19 group (7.5% vs. 22.8%), with a low significance (p = 0.051). For comparison between subjects accessing the service before and after the pandemic spread, see Table 1.
When analyzing the secondary outcome of the study, by comparing subjects affected by psychiatric disorders referring to the service before (n = 37, 46.8%) and during (n = 42, 53.2%) the- COVID-19 pandemic (see Table 2), the only socio-demographic characteristic that differed among the two subgroups with a high significance was the age. Indeed, subjects accessing psychiatric services after the pandemic were older than those who were referred to the service before the infection outbreak (19.29 ± 2.62 vs. 17.35 ± 2.47, p = 0.001). Diagnostic features did not differ between the two subgroups, nor did the other clinical characteristics investigated in the present study.
Digital social and educational interventions and telepsychiatry interventions were significantly more frequent in the during-COVID-19 subgroup (35.7% vs. 2.7%, p = 0.001). Treatment prescription varied among the two populations with a low significance. Particularly, higher psychopharmacological prescription rates (35.7% vs. 16.2%, p = 0.074), especially for what concerned antidepressants (11.9% vs. 0%, p = 0.057) and mood stabilizers (19% vs. 5.4%, p = 0.094), were highlighted in the during-COVID-19 population.
Family therapies were less frequently administered to subjects who accessed the service after the pandemic spread when evaluating psychosocial interventions (9.5% vs. 35.1%), with a medium significance (p = 0.013). Moreover, none of the subjects accessing the service after the COVID-19 outbreak was referred to residential facilities, with a low significance when compared to those accessing the service before (0% vs. 8.1%, p = 0.098).
Among subjects referred to the service before the pandemic, 18 (31%) dropped out of the therapeutic program before the COVID-19 spread. Only subjects who did not drop-out before the pandemic outbreak were considered for this sub-analysis (n = 39).
Medium significance was found in the difference between the number of interventions supplied before and during the COVID-19 pandemic (70.80 ± 107.117 vs. 34.55 ± 39.08, p = 0.038). Digital mental health services demonstrated a highly significant increase in the considered population (5.1% vs. 56.4%, p < 0.001). The rates of psychosocial interventions did not differ when comparing the period before and after the pandemic spread, and neither did psychopharmacological treatment features.
After the COVID-19 outbreak, there was a significant increase in the number of interventions supplied to subjects who first accessed the service in the “pre-COVID-19” period. We found an increase in the mean age of subjects who accessed the service in the “during-COVID-19” period, a higher prevalence of anxiety disorders, and an increase in the use of anxiolytics and mood stabilizers. A reduction in the prevalence of opioids use disorder and in the use of substitution therapy for opioid dependence was also observed. Furthermore, we observed a highly significant increase in digital mental health interventions in the “during-COVID-19” period, as well as a decrease in family therapies, both provided by digital tools and in-person, with a high significance of the difference in the subpopulation of subjects suffering from psychiatric disorders. Treatment features of people who were already followed by the service before the COVID-19 outbreak did not significantly change, except for the number of supplied interventions and the already mentioned increase of digital interventions.
New accesses to the service after the COVID-19 outbreak were stable, which is in line with the literature on the topic. Indeed, previous studies highlighted that the number of admissions to psychiatric care facilities showed trends similar to the pre-COVID-19 outbreak period (39). This result could be due to an adaptation of mental services to give help during the pandemic, especially implementing digital mental health services (40), while it is in contrast with other findings, e.g., those concerning the decrease of new accesses to psychiatric emergency units (41–43). Based on the stated above, access to care during the COVID-19 emergency should be further investigated since it represents a complex issue that relies on several possible determinants (44). Future research on the topic should thus consider these determinants, such as socio-economic factors (45, 46).
Our study also observed a significant increase in the number of follow-up interventions of subjects that were already being treated in the “pre-COVID-19” period. This has been made possible by the highly significant increase of digital mental health interventions (47–51). Indeed, digital mental health interventions, such as those delivered via mobile and web-based platforms, offer the potential to improve access to care while avoiding many existing barriers to receiving face-to-face intervention, including stigma and time (52–54). The evidence base for digital mental health interventions in the general population is rapidly accumulating (55, 56), and many studies on the topic reported that such interventions were either effective or partially effective in producing beneficial changes in the main psychological outcome variables, also among youngsters (50, 57, 58).
Dropouts from the therapeutic project did not face a statistically significant increase and were similar to those detected in studies conducted on similar populations before the pandemic spread (59). Despite this, an increasing trend in dropouts was evidenced after the COVID-19 outbreak and a positive, strong association was highlighted in the psychiatric disorders’ subgroup. To our best knowledge, literature concerning drop-out rates from outpatient psychiatric services during the pandemic is scant, especially for the youth population. Data from the present research are thus expected to be further clarified by future prospective studies, since adequate access to care represents a crucial issue in the field of early intervention (60).
The results have shown an increase of medium significance in the mean age of subjects accessing the service in the “during-COVID-19” period. We hypothesized that this finding could be due to better social support given by belonging to a group, such as schoolmates for adolescents, representing a protective factor against loneliness that can lead to anxiety and depressive symptomatology (61). Therefore, having finished school, with a consequent reduction in the sense of belongingness, may have a synergistic effect with the isolation linked to the pandemic and lockdown measures themselves. Many studies reported that loneliness threatens mental health (7, 62), leading to sleep disturbances and increased inactivity (63, 64). Greater severity of depressive symptomatology may also had been caused by loneliness, along with poor self-perceived overall health quality, impaired functional status, and a perceived negative change in the quality of life (65).
Concerning people who first sought help to the service after the COVID-19 outbreak, we found a higher prevalence of anxiety disorders in this population when compared to those referred before the pandemic spread. An increase in prescriptions of antidepressants and mood stabilizers was also highlighted, both for subjects suffering from psychiatric disorders and those who did not. Interestingly, the significance of the phenomenon was higher in the second group. Several studies confirmed our findings by detecting the increase in the prevalence of anxiety and depressive disorders in young adults during the COVID-19 pandemic (66, 67). Scientific papers that have evaluated the differences in the prescriptions of psychopharmacological treatments during the pandemic are scant. However, some studies showed an increasing trend (68). It should also be noted that the choice of pharmacological treatments in youth populations represents a critical issue, as demonstrated by the high prescription rates of off-label treatments in this population (69). In our sample, when a clear-cut diagnosis according to the DSM-5 criteria was not possible to be performed, pharmacological treatments were based on symptom dimensions. Indeed, the absence of a full-blown diagnosis does not necessarily mean the absence of an at-risk state, namely a totipotent condition that could hesitate in different exit syndromes (70–72). This could also explain higher rates of mood stabilizer prescription in the sample, even though the diagnosis of bipolar disorders did not significantly change. To this extent, it should be noted that the emergence of SUD or anxiety symptoms during youth may be the expression of a bipolar diathesis in young people, and this may partially explain the higher mood stabilizer prescription rate (73). Furthermore, we should consider that adjustment disorders may also manifest with disturbed conduct, which may more frequently benefit from mood stabilizers or antipsychotics in youths (74, 75). Due to the risk of dependence associated with benzodiazepines assumption, especially in a population of subjects accessing an addiction service, low-dose atypical antipsychotics and mood stabilizers were preferred for anxiety symptoms or anxiety disorders (76, 77).
As demonstrated by some reviews (10, 78), the COVID-19 pandemic and the lockdown measures may have negatively impacted youths’ mental health. First, school closure may have significantly impacted children and adolescents, particularly those aged between 5 and 18 (79). Lack of regular contact with friends may more frequently result in loneliness during adolescence and is not necessarily mitigated using phones or other communication forms (80). This context predisposes adolescents to psychopathological vulnerability, leading to an increasing trend in diagnoses of depressive and anxiety disorders (81). Accordingly, the prevalence of depression in young people across studies conducted in this period ranged from 22.6% to 43.7%, according to previous studies (66, 67), and an increase in the severity of pre-existing depression was detected (82). A survey conducted in China among 8,079 adolescents aged 12–18 revealed a high prevalence of symptoms of depression (43%), anxiety (37%), and combined depression and anxiety (31%) during the COVID-19 pandemic (83). Several risk factors, such as relatives suffering from COVID-19, were identified for the development of affective symptoms (84). These findings are considerable since youths suffering from psychiatric disorders represent an extremely vulnerable population, among which significant consequences could also emerge after the pandemic outbreak (85).
As expected, we observed a highly significant increase in telepsychiatry interventions in line with a large amount of literature. Several papers highlighted an increase in the prevalence of digital mental health interventions in young adults during the COVID-19 pandemic, and different psychological interventions were adapted to the online form (86, 87). We highlighted a decreasing trend in family therapies, with higher significance in the subgroup of subjects suffering from psychiatric disorders. Family therapies are psychotherapy interventions provided by a trained mental health professional (in our service, usually a psychologist) and oriented toward communication improvement and conflict solution in familiar contexts. This data is relevant since scientific literature demonstrated how the pandemic impacted the whole familiar system. Indeed, previous reports underlined that quarantine measures might influence depressive symptom severity among students and their family members (88). Studies focusing on the mental health of children, young adults and their parents showed considerable stressors that these populations perceived during the pandemic period. Children and adolescents were mainly stressed by the disruption of social life and important activities/events, whereas their parents were stressed by the uncertainty of the pandemic and the disease itself (89). These changes in habits suggest that specific risk factors for the development of psychological distress should be identified for both youths and their families in order to act on potentially modifiable stressors. Despite this, the readaptation of family therapy models to digital mental health settings, which was needed due to physical distancing protocols, required a huge effort, and several challenges were faced by both professionals and users (90). Indeed, the lack of adequate technology could represent a concern for families already coping with socio-economic problems before the pandemic due to the worsening of such problems in most cases (91).
Furthermore, the engagement with the therapist could become a concern for families that were not already in contact with the service in the “pre-COVID-19” period. This issue could explain the decrease in such interventions, possibly due to one or more members’ difficulties trusting the therapist and establishing a therapeutic alliance (92). A decreasing trend was not evidenced for social and educational interventions, usually requiring one-to-one relationships between social workers/professional educators and the user. This relationship does not happen in the context of a therapeutic process and does not undergo the rules of a psychotherapeutic setting, making it easier to adapt the intervention for a digital setting.
These considerations reinforce the need for integrated interventions in adolescents showing the onset of psychiatric symptoms during the pandemic (93). Integrated psychosocial interventions could avoid the detriments of more extended home-schooling periods, the loss of opportunities to meet peers, and the disruption of familiar daily routines (89). Accordingly, the finding concerning the reduction in access to residential facilities should be considered, even though the significance was low. This could be interpreted in consideration of significant challenges faced in youth residential care, where social distancing measures and the interruption of contacts with families of origin critically affected the possibility of providing integrative care (94).
Regarding substance use, in our study, we observed a reduction in opioid use in the “during-COVID-19” period of medium significance and, consequently, a reduction in the use of substitution therapy for drug addiction. This evidence could be related to the limitations produced by the lockdown measures during the pandemic period and confirms data from previous studies (95, 96).
However, our sample’s decrease in opioid consumption should be considered a part of a more complex, multi-facet situation. Indeed, due to reduced access to treatment and replacement pharmacology therapies and the lack of continuity in the intake of opioids, emergencies occurred more frequently in the pandemic period, as demonstrated by the increase in cases of opioid overdose (97).
Our study has limitations: first, the relatively small sample size may limit the generalizability of the findings. The issue is also due to the choice of a real-world setting relying on data from one service, since outpatient facilities dedicated to adolescents and young adults suffering from mental health problems are limited in our region. The sample size also hindered the possibility to perform further sub-analyses, e.g., stratifying subjects based on psychiatric diagnoses. Furthermore, it should be considered that data concerning the “during-COVID-19” period were collected during different pandemic phases, without, e.g., specifying whether new accesses happened during lockdown periods or not. To note, we could not analyze any increasing trends in the considered variables during the years preceding the COVID-19 outbreak, and the comparison between the pre-COVID-19 and the during-COVID-19 period assumed no increasing trends in the variables of interest.
Moreover, a specific psychopathological assessment was not systematically administered, and data collected in the usual clinical practice were instead used. This issue may limit the possibility to evaluate treatment response in the considered population. To this end, further studies should evaluate the outcomes of the administered interventions in youths suffering from psychological distress, particularly focusing on telepsychiatry and psychosocial treatments.
Data from the present study suggest that health professionals should accurately screen youths for the presence of psychological distress, both those that already suffered from a psychiatric disorder and those manifesting such distress for the first time. Youths represent a high-risk population for the development of mental disorders, and these were demonstrated to increase during the COVID-19 pandemic and could be expected to rise in the post-pandemic era. The increase of specific psychopathological features in this vulnerable group after the COVID-19 outbreak suggests that pathways to care should be reinforced, and targeted interventions should be proposed to improve the mental health of adolescents and young adults. Particularly, clinicians should further promote the adaptation of mental health services to the emerging historical and social context, e.g., extensively rethinking services under a digital mental health perspective. Furthermore, the proposed interventions should include tailored pharmacological treatments that could help achieve symptomatologic remission and psychosocial interventions that would progressively lead youths toward a full-functional recovery.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of Umbria Region (protocol N° 23369/21/ON). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
GM and GP conceived the idea and designed the study. GP and AS collected the data. GM performed the statistical analysis. GM, GP, FB, AM, NM, and MD’A wrote the original draft. SB, EM, LO, UV, and AT revised the whole manuscript. LS supervised the study during all its phases. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Lundbeck for indirectly supporting this study by the research support provided to GP.
1. Holmes EA, O’Connor RC, Perry VH, Tracey I, Wessely S, Arseneault L, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. (2020) 7:547–60. doi: 10.1016/S2215-0366(20)30168-1
2. Adhanom Ghebreyesus T. Addressing mental health needs: an integral part of COVID-19 response. World Psychiatry. (2020) 19:129–30. doi: 10.1002/wps.20768
3. Kuzman MR, Curkovic M, Wasserman D. Principles of mental health care during the COVID-19 pandemic. Eur Psychiatry. (2020) 63:e45. doi: 10.1192/j.eurpsy.2020.54
4. Fiorillo A, Sampogna G, Giallonardo V, Del Vecchio V, Luciano M, Albert U, et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: results from the COMET collaborative network. Eur Psychiatry. (2020) 63:e87. doi: 10.1192/j.eurpsy.2020.89
5. Umbria R. COVID-19 dati generali sui casi della Regione Umbria. (2022). Available online at: https://coronavirus.regione.umbria.it/casi (accessed March 25, 2022).
6. Beghi M, Ferrari S, Biondi L, Brandolini R, Corsini C, De Paoli G, et al. Mid-term psychiatric consequences of the COVID-19 pandemic: a 4 months observational study on emergency room admissions for psychiatric evaluation after the (first) lockdown period in Italy. Soc Psychiatry Psychiatr Epidemiol. (2022) 2022:1–7. doi: 10.1007/s00127-022-02262-6
7. Sampogna G, Giallonardo V, Del Vecchio V, Luciano M, Albert U, Carmassi C, et al. Loneliness in young adults during the first wave of COVID-19 lockdown: results from the multicentric COMET study. Front Psychiatry. (2021) 12:788139. doi: 10.3389/FPSYT.2021.788139
8. Loades ME, Chatburn E, Higson-Sweeney N, Reynolds S, Shafran R, Brigden A, et al. Rapid systematic review: the impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. J Am Acad Child Adolesc Psychiatry. (2020) 59:1218.e–39.e. doi: 10.1016/j.jaac.2020.05.009
9. Duan L, Shao X, Wang Y, Huang Y, Miao J, Yang X, et al. An investigation of mental health status of children and adolescents in china during the outbreak of COVID-19. J Affect Disord. (2020) 275:112–8. doi: 10.1016/j.jad.2020.06.029
10. Singh S, Roy D, Sinha K, Parveen S, Sharma G, Joshi G. Impact of COVID-19 and lockdown on mental health of children and adolescents: a narrative review with recommendations. Psychiatry Res. (2020) 293:113429. doi: 10.1016/J.PSYCHRES.2020.113429
11. Moreno C, Wykes T, Galderisi S, Nordentoft M, Crossley N, Jones N, et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry. (2020) 7:813–24. doi: 10.1016/S2215-0366(20)30307-2
12. Menculini G, Albert U, Bianchini V, Carmassi C, Carrà G, Cirulli F, et al. Did we learn something positive out of the COVID-19 pandemic? Post-traumatic growth and mental health in the general population. Eur Psychiatry. (2022) 64:e79. doi: 10.1192/J.EURPSY.2021.2263
13. Oliva S, Russo G, Gili R, Russo L, Di Mauro A, Spagnoli A, et al. Risks and protective factors associated with mental health symptoms during COVID-19 home confinement in italian children and adolescents: the #understandingkids study. Front Pediatr. (2021) 9:664702. doi: 10.3389/fped.2021.664702
14. Golberstein E, Wen H, Miller BF. Coronavirus disease 2019 (COVID-19) and mental health for children and adolescents. JAMA Pediatr. (2020) 174:819–20. doi: 10.1001/jamapediatrics.2020.1456
15. Jefsen OH, Rohde C, Nørremark B, Østergaard SD. Editorial Perspective: COVID-19 pandemic-related psychopathology in children and adolescents with mental illness. J Child Psychol Psychiatry Allied Discip. (2021) 62:798–800. doi: 10.1111/jcpp.13292
16. Raballo A, Poletti M, Valmaggia L, McGorry PD. Editorial perspective: rethinking child and adolescent mental health care after COVID-19. J Child Psychol Psychiatry Allied Discip. (2020) 62:1067–9. doi: 10.1111/jcpp.13371
17. Germani A, Buratta L, Delvecchio E, Gizzi G, Mazzeschi C. Anxiety severity, perceived risk of COVID-19 and individual functioning in emerging adults facing the pandemic. Front Psychol. (2020) 11:567505. doi: 10.3389/FPSYG.2020.567505
18. Volpe U, Orsolini L, Salvi V, Albert U, Carmassi C, Carrà G, et al. COVID-19-Related Social Isolation Predispose to Problematic Internet and Online Video Gaming Use in Italy. Int J Environ Res Public Health. (2022) 19:1539. doi: 10.3390/IJERPH19031539
19. Prisco V, Prisco L, Donnarumma B. [Telepsychiatry in adults and adolescents: a useful tool against CoViD-19]. Recenti Prog Med. (2020) 111:411–4. doi: 10.1701/3407.33923
20. Deolmi M, Pisani F. Psychological and psychiatric impact of COVID-19 pandemic among children and adolescents. Acta Biomed. (2020) 91:1–5. doi: 10.23750/ABM.V91I4.10870
21. Alivernini F, Manganelli S, Girelli L, Cozzolino M, Lucidi F, Cavicchiolo E. Physical distancing behavior: the role of emotions, personality, motivations, and moral decision-making. J Pediatr Psychol. (2021) 46:15–26. doi: 10.1093/JPEPSY/JSAA122
22. Fegert JM, Vitiello B, Plener PL, Clemens V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: a narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc Psychiatry Ment Health. (2020) 14:20. doi: 10.1186/S13034-020-00329-3
23. Torresani S, Doimo S, Furlato K, Naika F, Conca A, Lasalvia A. [Continuity of care and therapeutic adherence in young people at psychosis onset: the integrated intervention model of the Psychiatric Service of Bolzano]. Riv Psichiatr. (2021) 56:93–9. doi: 10.1708/3594.35767
24. Liese BH, Gribble RSF, Wickremsinhe MN. International funding for mental health: a review of the last decade. Int Health. (2019) 11:361–9. doi: 10.1093/INTHEALTH/IHZ040
25. National Health Service.Funding boost for young people’s mental health services. (2021). Available online at: https://www.england.nhs.uk/2021/06/funding-boost-for-young-peoples-mental-health-services/ (accessed December 31, 2021)
26. Lancet Regional Health– Europe T. Protecting the mental health of youth. Lancet Reg Heal. (2022) 12:100306. doi: 10.1016/j.lanepe.2021.100306
27. Robinson ZD, Riggs PD. Cooccurring Psychiatric and Substance Use Disorders. Child Adolesc Psychiatr Clin N Am. (2016) 25:713–22. doi: 10.1016/J.CHC.2016.05.005
28. Ciditech. PoInT GeDi. Ciditech (2016). Available online at: http://www.ciditech.it/gedi
29. Regione Umbria.Umbria: Evoluzione Della Pandemia e Interventi Adottati in Fase 1. (2020). Available online at: https://webstat.regione.umbria.it/covid19_monitorumbria/ (accessed February 22, 2022).
30. American Psychiatric Association (APA).Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed. Washington, DC: American Psychiatric Association (2013).
31. McHugh ML. The Chi-square test of independence. Biochem Medica. (2013) 23:143. doi: 10.11613/BM.2013.018
32. Bewick V, Cheek L, Ball J. Statistics review 8: qualitative data – tests of association. Crit Care. (2004) 8:46. doi: 10.1186/CC2428
33. Altman DG, Bland JM. Statistics notes: the normal distribution. BMJ. (1995) 310:298. doi: 10.1136/bmj.310.6975.298
34. Fagerland MW. T-tests, non-parametric tests, and large studiesa paradox of statistical practice? BMC Med Res Methodol. (2012) 12:78. doi: 10.1186/1471-2288-12-78
35. Ghasemi A, Zahediasl S. Normality tests for statistical analysis: a guide for non-statisticians. Int J Endocrinol Metab. (2012) 10:486–9. doi: 10.5812/ijem.3505
36. Armstrong RA. When to use the Bonferroni correction. Ophthalmic Physiol Opt. (2014) 34:502–8. doi: 10.1111/OPO.12131
37. Amrhein V, Korner-Nievergelt F, Roth T. The earth is flat (p > 0:05): significance thresholds and the crisis of unreplicable research. PeerJ. (2017) 5:e3544. doi: 10.7717/peerj.3544
38. Greenland S, Senn SJ, Rothman KJ, Carlin JB, Poole C, Goodman SN, et al. Statistical tests, P values, confidence intervals, and power: a guide to misinterpretations. Eur J Epidemiol. (2016) 31:337. doi: 10.1007/S10654-016-0149-3
39. Columb D, Hussain R, O’Gara C. Addiction psychiatry and COVID-19: impact on patients and service provision. Ir J Psychol Med. (2020) 37:164–8. doi: 10.1017/IPM.2020.47
40. Carpiniello B, Tusconi M, Zanalda E, Di Sciascio G, Di Giannantonio M, Di Giannantonio M, et al. Psychiatry during the Covid-19 pandemic: a survey on mental health departments in Italy. BMC Psychiatry. (2020) 20:593. doi: 10.1186/s12888-020-02997-z
41. Simpson SA, Loh RM, Cabrera M, Cahn M, Gross A, Hadley A, et al. The Impact of the COVID-19 Pandemic on Psychiatric Emergency Service Volume and Hospital Admissions. J Acad Consult Psychiatry. (2021) 62:588–94. doi: 10.1016/j.jaclp.2021.05.005
42. Fasshauer JM, Bollmann A, Hohenstein S, Mouratis K, Hindricks G, Meier-Hellmann A, et al. Impact of COVID-19 pandemic on involuntary and urgent inpatient admissions for psychiatric disorders in a German-wide hospital network. J Psychiatr Res. (2021) 142:140–3. doi: 10.1016/J.JPSYCHIRES.2021.07.052
43. Kim HK, Carvalho AF, Gratzer D, Wong AHC, Gutzin S, Husain MI, et al. The Impact of COVID-19 on Psychiatric Emergency and Inpatient Services in the First Month of the Pandemic in a Large Urban Mental Health Hospital in Ontario, Canada. Front Psychiatry. (2021) 12:563906. doi: 10.3389/FPSYT.2021.563906
44. Menculini G, Tortorella A, Albert U, Carmassi C, Carrà G, Cirulli F, et al. Access to mental health care during the first wave of the COVID-19 pandemic in Italy: results from the COMET multicentric study. Brain Sci. (2021) 11:1413. doi: 10.3390/BRAINSCI11111413
45. Penner F, Rajesh A, Kinney KL, Mabus KL, Barajas KG, McKenna KR, et al. Racial and demographic disparities in emergency department utilization for mental health concerns before and during the COVID-19 pandemic. Psychiatry Res. (2022) 310:114442. doi: 10.1016/J.PSYCHRES.2022.114442
46. Roulston C, McKetta S, Price M, Fox KR, Schleider JL. Structural Correlates of Mental Health Support Access among Sexual Minority Youth of Color during COVID-19. J Clin Child Adolesc Psychol. (2022) 2022:2034633. doi: 10.1080/15374416.2022.2034633
47. Torous J, Choudhury T, Barnett I, Keshavan M, Kane J. Smartphone relapse prediction in serious mental illness: a pathway towards personalized preventive care. World Psychiatry. (2020) 19:308–9. doi: 10.1002/wps.20805
48. Ramalho R, Adiukwu F, Gashi Bytyçi D, El Hayek S, Gonzalez-Diaz JM, Larnaout A, et al. Telepsychiatry and healthcare access inequities during the COVID-19 pandemic. Asian J Psychiatr. (2020) 53:102234. doi: 10.1016/j.ajp.2020.102234
49. Ramalho R, Adiukwu F, Gashi Bytyçi D, El Hayek S, Gonzalez-Diaz JM, Larnaout A, et al. Telepsychiatry During the COVID-19 Pandemic: Development of a Protocol for Telemental Health Care. Front Psychiatry. (2020) 11:552450. doi: 10.3389/FPSYT.2020.552450
50. Orsolini L, Pompili S, Salvi V, Volpe U. A systematic review on telemental health in youth mental health: focus on anxiety, depression and obsessive-compulsive disorder. Medicina. (2021) 57:793. doi: 10.3390/MEDICINA57080793
51. Adiukwu F, de Filippis R, Orsolini L, Gashi Bytyçi D, Shoib S, Ransing R, et al. Scaling Up Global Mental Health Services During the COVID-19 Pandemic and Beyond. Psychiatr Serv. (2021) 73:231–4. doi: 10.1176/APPI.PS.202000774
52. Kass AE, Balantekin KN, Fitzsimmons-Craft EE, Jacobi C, Wilfley DE, Taylor CB. The economic case for digital interventions for eating disorders among United States college students. Int J Eat Disord. (2017) 50:250–8. doi: 10.1002/EAT.22680
53. Lattie EG, Adkins EC, Winquist N, Stiles-Shields C, Wafford QE, Graham AK. Digital mental health interventions for depression, anxiety, and enhancement of psychological well-being among college students: systematic review. J Med Internet Res. (2019) 21:e12869. doi: 10.2196/12869
54. Rai M, Vigod SN, Hensel JM. Barriers to office-based mental health care and interest in E-communication with providers: a survey study. JMIR Ment Heal. (2016) 3:e35. doi: 10.2196/MENTAL.6068
55. Karyotaki E, Riper H, Twisk J, Hoogendoorn A, Kleiboer A, Mira A, et al. Efficacy of self-guided internet-based cognitive behavioral therapy in the treatment of depressive symptoms: a meta-analysis of individual participant data. JAMA Psychiatry. (2017) 74:351–9. doi: 10.1001/JAMAPSYCHIATRY.2017.0044
56. Firth J, Torous J, Nicholas J, Carney R, Pratap A, Rosenbaum S, et al. The efficacy of smartphone-based mental health interventions for depressive symptoms: a meta-analysis of randomized controlled trials. World Psychiatry. (2017) 16:287–98. doi: 10.1002/WPS.20472
57. Andrews G, Basu A, Cuijpers P, Craske MG, McEvoy P, English CL, et al. Computer therapy for the anxiety and depression disorders is effective, acceptable and practical health care: an updated meta-analysis. J Anxiety Disord. (2018) 55:70–8. doi: 10.1016/J.JANXDIS.2018.01.001
58. Ebert DD, Zarski AC, Christensen H, Stikkelbroek Y, Cuijpers P, Berking M, et al. Internet and computer-based cognitive behavioral therapy for anxiety and depression in youth: a meta-analysis of randomized controlled outcome trials. PLoS One. (2015) 10:e0119895. doi: 10.1371/JOURNAL.PONE.0119895
59. Wells JE, Browne MO, Aguilar-Gaxiola S, Al-Hamzawi A, Alonso J, Angermeyer MC, et al. Drop out from out-patient mental healthcare in the World Health Organization’s World Mental Health Survey initiative. Br J Psychiatry. (2013) 202:42–9. doi: 10.1192/BJP.BP.112.113134
60. Lambert M, Schöttle D, Ruppelt F, Rohenkohl A, Sengutta M, Luedecke D, et al. Early detection and integrated care for adolescents and young adults with psychotic disorders: the ACCESS III study. Acta Psychiatr Scand. (2017) 136:188–200. doi: 10.1111/a.12762
61. Baskin TW, Wampold BE, Quintana SM, Enright RD. Belongingness as a Protective Factor Against Loneliness and Potential Depression in a Multicultural Middle School. Couns Psychol. (2010) 38:626–51. doi: 10.1177/0011000009358459
62. Hwang TJ, Rabheru K, Peisah C, Reichman W, Ikeda M. Loneliness and social isolation during the COVID-19 pandemic. Int Psychogeriatr. (2020) 32:1. doi: 10.1017/S1041610220000988
63. Cacioppo JT, Hawkley LC, Berntson GG, Ernst JM, Gibbs AC, Stickgold R, et al. Do lonely days invade the nights? Potential social modulation of sleep efficiency. Psychol Sci. (2002) 13:384–7. doi: 10.1111/1467-9280.00469
64. Fässberg MM, van Orden KA, Duberstein P, Erlangsen A, Lapierre S, Bodner E, et al. A systematic review of social factors and suicidal behavior in older adulthood. Int J Environ Res Public Health. (2012) 9:722–45. doi: 10.3390/IJERPH9030722
65. Lee EE, Depp C, Palmer BW, Glorioso D, Daly R, Liu J, et al. High prevalence and adverse health effects of loneliness in community-dwelling adults across the lifespan: role of wisdom as a protective factor. Int Psychogeriatr. (2019) 31:1447–62. doi: 10.1017/S1041610218002120
66. Xie X, Xue Q, Zhou Y, Zhu K, Liu Q, Zhang J, et al. Mental Health Status Among Children in Home Confinement During the Coronavirus Disease 2019 Outbreak in Hubei Province, China. JAMA Pediatr. (2020) 174:898–900. doi: 10.1001/JAMAPEDIATRICS.2020.1619
67. Liu X, Luo WT, Li Y, Li CN, Hong ZS, Chen HL, et al. Psychological status and behavior changes of the public during the COVID-19 epidemic in China. Infect Dis Poverty. (2020) 9:58. doi: 10.1186/S40249-020-00678-3
68. Diez-Quevedo C, Iglesias-González M, Giralt-López M, Rangil T, Sanagustin D, Moreira M, et al. Mental disorders, psychopharmacological treatments, and mortality in 2150 COVID-19 Spanish inpatients. Acta Psychiatr Scand. (2021) 143:526–34. doi: 10.1111/ACPS.13304
69. Hoekstra PJ, Dietrich A. First do no harm: use off-label antipsychotic medication in children and adolescents with great caution. Eur Child Adolesc Psychiatry. (2022) 31:1–3. doi: 10.1007/S00787-022-01950-7
70. Raballo A, Mechelli A, Menculini G, Tortorella A. Risk syndromes in psychiatry: a state-of-the-art overview. Arch Psychiatry Psychother. (2019) 2:7–14. doi: 10.12740/APP/109506
71. McGorry PD, Hartmann JA, Spooner R, Nelson B. Beyond the “at risk mental state” concept: transitioning to transdiagnostic psychiatry. World Psychiatry. (2018) 17:133–42. doi: 10.1002/wps.20514
72. Hartmann JA, Nelson B, Spooner R, Paul Amminger G, Chanen A, Davey CG, et al. Broad clinical high-risk mental state (CHARMS): methodology of a cohort study validating criteria for pluripotent risk. Early Interv Psychiatry. (2019) 13:379–86. doi: 10.1111/eip.12483
73. Menculini G, Steardo L, Verdolini N, Cirimbilli F, Moretti P, Tortorella A. Substance use disorders in bipolar disorders: clinical correlates and treatment response to mood stabilizers. J Affect Disord. (2022) 300:326–33. doi: 10.1016/J.JAD.2022.01.001
74. Khan S, Down J, Aouira N, Bor W, Haywood A, Littlewood R, et al. Current pharmacotherapy options for conduct disorders in adolescents and children. Expert Opin Pharmacother. (2019) 20:571–83. doi: 10.1080/14656566.2018.1561862
75. Pringsheim T, Hirsch L, Gardner D, Gorman DA. The pharmacological management of oppositional behaviour, conduct problems, and aggression in children and adolescents with attention-deficit hyperactivity disorder, oppositional defiant disorder, and conduct disorder: a systematic review and meta-analysis. Part 2: antipsychotics and traditional mood stabilizers. Can J Psychiatry. (2015) 60:52–61. doi: 10.1177/070674371506000203
76. Bushnell GA, Crystal S, Olfson M. Prescription Benzodiazepine Use in Privately Insured U.S. Children and Adolescents. Am J Prev Med. (2019) 57:775–85. doi: 10.1016/J.AMEPRE.2019.07.006
77. Kurtz SP, Buttram ME, Surratt HL. Benzodiazepine Dependence among Young Adult Participants in the Club Scene Who Use Drugs. J Psychoactive Drugs. (2017) 49:39–46. doi: 10.1080/02791072.2016.1269978
78. Guessoum SB, Lachal J, Radjack R, Carretier E, Minassian S, Benoit L, et al. Adolescent psychiatric disorders during the COVID-19 pandemic and lockdown. Psychiatry Res. (2020) 291:113264. doi: 10.1016/J.PSYCHRES.2020.113264
79. Nearchou F, Hennessy E, Flinn C, Niland R, Subramaniam SS. Exploring the impact of COVID-19 on mental health outcomes in children and adolescents: a systematic review. Int J Environ Res Public Health. (2020) 17:1–19. doi: 10.3390/IJERPH17228479
80. Ghosh R, Dubey MJ, Chatterjee S, Dubey S. Impact of COVID -19 on children: special focus on the psychosocial aspect. Minerva Pediatr. (2020) 72:226–35. doi: 10.23736/S0026-4946.20.05887-9
81. Seçer I, Ulaş S. An Investigation of the Effect of COVID-19 on OCD in Youth in the Context of Emotional Reactivity, Experiential Avoidance, Depression and Anxiety. Int J Ment Health Addict. (2020) 19:2306–19. doi: 10.1007/S11469-020-00322-Z
82. Hawes MT, Szenczy AK, Klein DN, Hajcak G, Nelson BD. Increases in depression and anxiety symptoms in adolescents and young adults during the COVID-19 pandemic. Psychol Med. (2021) 13:1–9. doi: 10.1017/S0033291720005358
83. Zhou SJ, Zhang LG, Wang LL, Guo ZC, Wang JQ, Chen JC, et al. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur Child Adolesc Psychiatry. (2020) 29:749–58. doi: 10.1007/S00787-020-01541-4
84. Cao W, Fang Z, Hou G, Han M, Xu X, Dong J, et al. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. (2020) 287:112934. doi: 10.1016/j.psychres.2020.112934
85. Roy D, Ghosh R, Dubey S, Dubey MJ, Benito-Leon J, Kanti Ray B. Neurological and Neuropsychiatric Impacts of COVID-19 Pandemic. Can J Neurol Sci. (2021) 48:9–24. doi: 10.1017/CJN.2020.173
86. Dave S, Abraham S, Ramkisson R, Matheiken S, Pillai AS, Reza H, et al. Digital psychiatry and COVID-19: the Big Bang effect for the NHS? BJPsych Bull. (2021) 45:259–63. doi: 10.1192/BJB.2020.114
87. Gentile A, De Berardis D, Tomasetti C, Ventriglio A. Digital psychiatry in COVID-19 pandemic: an Italian perspective. Psychiatry Res. (2020) 292:113316. doi: 10.1016/j.psychres.2020.113316
88. Mechili EA, Saliaj A, Kamberi F, Girvalaki C, Peto E, Patelarou AE, et al. Is the mental health of young students and their family members affected during the quarantine period? Evidence from the COVID-19 pandemic in Albania. J Psychiatr Ment Health Nurs. (2021) 28:317–25. doi: 10.1111/JPM.12672
89. Mohler-kuo M, Dzemaili S, Foster S, Werlen L, Walitza S. Stress and Mental Health among Children/Adolescents, Their Parents, and Young Adults during the First COVID-19 Lockdown in Switzerland. Int J Environ Res Public Health. (2021) 18:4668. doi: 10.3390/IJERPH18094668
90. Fraenkel P, Cho WL. Reaching up, down, in, and around: couple and family coping during the coronavirus pandemic. Fam Process. (2020) 59:847–64. doi: 10.1111/FAMP.12570
91. Inchausti F, MacBeth A, Hasson-Ohayon I, Dimaggio G. Psychological intervention and COVID-19: what we know so far and what we can do. J Contemp Psychother. (2020) 50:1. doi: 10.1007/S10879-020-09460-W
92. Brothwood PL, Baudinet J, Stewart CS, Simic M. Moving online: young people and parents’ experiences of adolescent eating disorder day programme treatment during the COVID-19 pandemic. J Eat Disord. (2021) 9:62. doi: 10.1186/S40337-021-00418-4
93. Fusar-Poli P, Correll CU, Arango C, Berk M, Patel V, Ioannidis JPA. Preventive psychiatry: a blueprint for improving the mental health of young people. World Psychiatry. (2021) 20:200–21. doi: 10.1002/wps.20869
94. Carvalho HM, Mota CP, Santos B, Costa M, Matos PM. From chaos to normalization and deconfinement: what did the pandemic unveil in youth residential care. Child Adolesc Social Work J. (2022) 2022:1–13. doi: 10.1007/s10560-021-00808-2
95. Been F, Emke E, Matias J, Baz-Lomba JA, Boogaerts T, Castiglioni S, et al. Changes in drug use in European cities during early COVID-19 lockdowns - A snapshot from wastewater analysis. Environ Int. (2021) 153:106540. doi: 10.1016/J.ENVINT.2021.106540
96. Reinstadler V, Ausweger V, Grabher AL, Kreidl M, Huber S, Grander J, et al. Monitoring drug consumption in Innsbruck during coronavirus disease 2019 (COVID-19) lockdown by wastewater analysis. Sci Total Environ. (2021) 757:144006. doi: 10.1016/J.SCITOTENV.2020.144006
Keywords: adolescents, COVID-19, psychopathological distress, psychiatric disorders, young adults, youth mental health
Citation: Menculini G, Pomili G, Brufani F, Minuti A, Mancini N, D’Angelo M, Biscontini S, Mancini E, Savini A, Orsolini L, Volpe U, Tortorella A and Steardo L Jr (2022) COVID-19 and Youth Psychopathological Distress in Umbria, Central Italy: A 2-Year Observational Study in a Real-World Setting. Front. Psychiatry 13:869326. doi: 10.3389/fpsyt.2022.869326
Received: 04 February 2022; Accepted: 29 March 2022;
Published: 19 May 2022.
Edited by:
Samer El Hayek, University of Miami Health System, United StatesReviewed by:
Andrea Amerio, University of Genoa, ItalyCopyright © 2022 Menculini, Pomili, Brufani, Minuti, Mancini, D’Angelo, Biscontini, Mancini, Savini, Orsolini, Volpe, Tortorella and Steardo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luca Steardo Jr., c3RlYXJkb0B1bmljei5pdA==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.