
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry, 08 July 2022
Sec. Psychopharmacology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.865466
This article is part of the Research TopicTherapeutic Use of Ketamine in Psychiatric DisordersView all 12 articles
 Maud Rothärmel1*
Maud Rothärmel1* Cherifa Benosman1
Cherifa Benosman1 Wissam El-Hage2,3Caroline Berjamin1
Wissam El-Hage2,3Caroline Berjamin1 Diane Ribayrol1Olivier Guillin1,4,5Raphaël Gaillard6Lucie Berkovitch6,7
Diane Ribayrol1Olivier Guillin1,4,5Raphaël Gaillard6Lucie Berkovitch6,7 Virginie Moulier1,8
Virginie Moulier1,8Introduction: Major depressive disorder (MDD) is more likely to resist to usual treatment when it is associated with post-traumatic stress disorder (PTSD). Capitalizing on the effect of ketamine in both treatment-resistant depression (TRD) and PTSD, we conducted a study in order to assess the efficacy of intranasal (IN) Esketamine in patients having TRD with comorbid PTSD.
Materials and Methods: In this open-label, single arm, retrospective pilot study, 11 patients were treated with IN Esketamine (56 or 84 mg) with a longitudinal follow-up of 6 months. IN Esketamine was administered twice weekly during the first month, once weekly during the second month, and then once every 1 or 2 weeks. Patients were assessed with Montgomery-Åsberg Depression Rating Scale (MADRS), Patient Health Questionnaire 9 items, Global Assessment of Functioning (GAF), and Clinical Global Impression-Suicide Scale (CGI-SS).
Results: We included 9 women and 2 men (mean age 47.3 ± 11.1 years). The mean (SD) MADRS scores decreased significantly from 38.6 (6.4) at baseline to 18.2 (10.03) after 6 months of IN Esketamine; 7 patients were responders and 3 patients were in remission. The percentage of patients who were moderately to severely suicidal declined from 63.6% at baseline to 27.3% after 1 month of IN Esketamine sessions. No serious adverse reactions were observed.
Conclusion: This study reports the outcomes of 11 severely ill patients with comorbid TRD and PTSD after IN Esketamine treatment. Esketamine significantly improved depression symptoms, suggesting that it is likely to be a treatment of choice in this specific population.
Major depressive disorder (MDD) is a common psychiatric disorder and is considered as one of the leading causes of disability worldwide (1). More than one third of depressed patients fail to fully respond to antidepressant treatments at adequate doses and duration, and are regarded as treatment-resistant depression (TRD) patients (2). Treatment resistance is characterized by an absence of symptomatic remission after the use of two successive trials of antidepressants of different pharmacological classes, well conducted in terms of dosage and duration while ensuring quality compliance (3, 4). A wide range of sociodemographic (female sex, age, financial insecurity, low level of education, etc.) and clinical factors, such as psychiatric and somatic comorbidities, are associated with treatment resistance (3). Post-traumatic Stress Disorder (PTSD) is one of those comorbidities (5, 6). It is a chronic and disabling condition arising after exposure to a severe traumatic event, characterized by persistent reexperiencing, avoidance, and hyperarousal symptoms. Risk for PTSD depends on trauma exposure severity, cumulative number of traumas, and trauma type; interpersonal traumas (physical and sexual assault in the context of relationship) carrying the highest risk (7). Patients with comorbid depression and PTSD have greater functional impairment (8) and their likelihood of suicidality is increased by more than three times compared to individuals with only one of these disorders (9).
Treatment strategies for TRD include antidepressants [e.g., selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclics and monoamine oxidase inhibitors], psychotherapy and brain stimulation techniques [e.g., electroconvulsive therapy (ECT) and repetitive transcranial magnetic stimulation (rTMS)] (10). Because some patients do not respond to those treatments, additional therapeutic strategies are strongly needed (11). In recent years, a growing body of evidence has implicated the glutamatergic system in the pathogenesis of depression, N-methyl-D-aspartate (NMDA) glutamate receptors being identified as a potential pharmacotherapeutic target for MDD, including TRD (12–14). Intravenous ketamine, a non-competitive receptor antagonist of NMDA glutamate receptors, was found to exhibit a robust and rapid onset of efficacy in patients with TRD when administered at subanesthetic doses (0.5 mg/kg) (15–19). Glutamate is also involved in stress responsivity, the formation of traumatic memories, and the pathophysiology of PTSD (20). So ketamine was proposed as a potential treatment for chronic PTSD (21–23) or for comorbid PTSD with TRD (24), although the results regarding ketamine efficacy in this indication are contradictory (25).
Nevertheless, ketamine is known for its abuse potential and profound adverse effects, such as psychotomimetic symptoms, neurotoxicity, cognitive impairment, and hypertension. These effects appear to be less frequent with its S-enantiomer or Esketamine, making it preferable to use (26). Oral Esketamine administration yields a low bioavailability of around 20%, which stimulated the development of its intranasal (IN) form (27). Indeed, the bioavailability and the kinetics of effects of ketamine vary considerably according to the route of administration (e.g., bioavailability: oral: 20%; intramuscular: 90%; rectal: 25%; intranasal: 50%; epidural: 77%; kinetics of effects: oral: delay 15–30 min, duration: 60–90 min; intramuscular: delay: 10–15 min, duration: 30–120 min; intravenous: delay: 1–2 min, duration: 20–60 min) (28). Granted marketing authorization by the European Medicines Agency (EMA) for the treatment of TRD in December 2019 (29), Esketamine nasal spray is used as an antidepressant for TRD. It delivers a 28 mg Esketamine dose via two sprays (one per nostril) (29, 30). Phase-3 short-term trials of Esketamine nasal spray (28, 56, or 84 mg) plus an oral antidepressant have demonstrated a statistically significant reduction in depressive symptoms [reduction from baseline Montgomery–Åsberg Depression Rating Scale (MADRS) total score] in patients with TRD compared with an oral antidepressant plus placebo nasal spray (31), and a sustained decreased risk of relapse among stable remitters and responders in long-term trials (29, 32, 33). Long-term safety data showed that most treatment-emergent adverse events (AEs) were mild or moderate in intensity, and resolved on the same day (33). However, the optimum dose, duration, and frequency of use are not fully understood yet (34) and potential indications still need to be clarified. There is no head-to-head data to compare ketamine or Esketamine formulation in terms of tolerance or efficacy. Nevertheless, a recent case series demonstrated that 10 consecutive patients who had responded to IV racemic ketamine for TRD successfully maintained their antidepressant response when switched to IN Esketamine (35).
On the basis of the reported efficacy of intravenous ketamine on PTSD and TRD, we hypothesized that IN Esketamine could be effective in TRD patients with comorbid PTSD. This study is the first one to examine the efficacy and the safety of repeated IN Esketamine administration over a 6-month period on symptoms of depression in this specific population. We further discuss the possible mechanisms of action and the potential synergistic effect with psychotherapeutic intervention.
We have led an open-label, single arm, retrospective pilot study on 11 adult patients (aged 18–65 years) who have received from Esketamine nasal spray between February 2020 and November 2021 in one psychiatric department specialized in TRD. Patients underwent a psychiatric evaluation by a board-certified psychiatrist (MR or CB) to confirm diagnosis of major depression and comorbid PTSD according to the criteria in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). All participants met the criteria for TRD (3) and PTSD (DSM-5). Written informed consent was obtained from all participants before participation. Under French ethical law (public Health code), retrospective studies based on the exploitation of routine care data do not have to be submitted to an ethics committee. This research was performed in accordance with the Declaration of Helsinki.
All participants received Esketamine nasal spray co-administered with a newly initiated oral antidepressant in either a full or partial hospitalization setting, as recommended by the Summary of Product Characteristics (SmPC) approved by ANSM [European Medicines Agency (36)]. All patients had baseline blood tests and an electrocardiogram to determine medical stability before the initiation of Esketamine. Post-administration monitoring was undertaken by a healthcare professional for ≥120 min. Throughout their treatment with Esketamine, the patients benefited from individualized follow-up by the same referring nurse. Esketamine was initiated at 56 mg and adjusted on an individual basis during the treatment period in accordance with the following treatment guidelines (29, 36): Weeks 1–4: 56 or 84 mg twice weekly; Weeks 5–8: 56 or 84 mg once weekly; and Week 9 and onward: 56 or 84 mg once every 1 or 2 weeks (Supplementary Figure 1). However, psychiatrists were free to adjust treatment dosage and frequency on an individual basis, depending on the patient’s response and tolerance to treatment. During Esketamine treatment, voluntary patients were offered trauma-focused psychotherapy [cognitive behavioral therapy (CBT) or eye movement desensitization and reprocessing (EMDR)] once every 1 or 2 weeks. Psychotherapy sessions took place within one week of Esketamine administration.
Scores were collected every month. The primary outcome was changes in depression score, assessed with the MADRS, between treatment initiation at baseline (Day 1) and 6 months of treatment (M6). A MADRS score of 30 is considered a definition of severe depression (37). At 6 months, patients who achieved a 50% or greater reduction in their MADRS scores were considered as responders, while patients who obtained a MADRS score inferior to 12 were remitters. Secondary outcomes included changes in scores on Patient Health Questionnaire-9 (PHQ-9), Global Assessment of Functioning (GAF) and Clinical Global Impression-Suicide Scale (CGI-SS) between baseline, and M6. Side effects and tolerability were assessed after each Esketamine administration. We also assessed PTSD symptoms as an exploratory variable in patients who were undergoing psychotherapy using the PTSD Checklist for DSM-5 (PCL-5) between psychotherapy initiation and the 6th month of psychotherapy (38). A PCL-5 score of 32 was deemed to have the greatest likelihood of correctly categorizing a participant as having PTSD as per the DSM-5 guidelines (38).
Changes in quantitative outcome measures from the baseline to 6 months after Esketamine initiation were examined using non-parametric Friedman tests, due to the small sample size. Statistical analyses were conducted using SPSS, version 28 (IBM, Armonk, NY, United States).
As shown in Supplementary Table 1, we included 9 female and 2 male patients with comorbid TRD and PTSD (mean age 47.27 ± 11.07 years, range 24–59). The majority of patients were in a relationship (n = 8), on sick leave (n = 5) or unemployed (n = 4). Nine patients (82%) have already attempted suicide in their lifetime. Patients suffered from chronic PTSD related to rape (n = 2), sexual abuse in childhood (n = 4) or other traumatic experiences (one suicide of family member, one brutal love breakup, and three workplace bullying). Nine patients also had other comorbidities, namely, anxiety disorders (n = 4), chronic pain (n = 3), addiction (n = 1), and eating disorder (n = 1).
Treatment with IN Esketamine was initiated at 56 mg, followed by a titration up to a target dose of 84 mg. At 6 months, all patients were still receiving a dose of 84 mg per session except for one patient who was receiving 56 mg due to poor tolerance (nausea). However, the rhythm of the sessions was conducted in accordance with the recommended Esketamine administration protocol for all patients. The mean number of Esketamine sessions administered in 6 months were 25.0 (5.3) ranging from 13 to 28. Concomitant medication prescriptions included SSRIs (n = 2), serotonin/norepinephrine reuptake inhibitors (n = 7), α2 antagonists (n = 1), tricyclics (n = 1), atypical antipsychotics (n = 9), mood stabilizers (n = 10), and benzodiazepines (n = 6). Treatment (other than Esketamine) was not changed during the follow-up period.
To test the effect of concomitant antidepressant treatments on our primary outcome (change in MADRS between baseline and 6 months of Esketamine treatment), we converted antidepressant treatments into fluoxetine equivalent (39). No significant correlation (ρ = –0.598, p = 0.068) was found between relative improvement (between baseline and 6 months of esketamine) and antidepressants dose (fluoxetine-equivalents).
At the baseline, the mean Maudsley staging score was 10.4 (1.6) (range: 7–12), with moderate (n = 5) to severe (n = 6) level of resistance (40). The evolution of depressive symptoms (through MADRS and PHQ-9) and global functioning (through GAF) are illustrated in Figure 1. The mean MADRS score significantly decreased during the treatment period (–13.5 points at 3 months and –20.4 at 6 months, p < 0.001, see Table 1). As reported in Table 1, the PHQ-9 scores significantly decreased over the treatment period (p = 0.012), whereas the GAF scores significantly increased (p = 0.001). The number of patients who achieved response (defined by a reduction of at least 50.0% of the MADRS total score) increased with time from one (9.1%) after one month of treatment, to five (45.5%) after 3 months and seven (63.6%) after 6 months. Regarding remission (defined as a MADRS total score ≤ 12), three patients (27.3%) reached remission at 3 and 6 months [including one (9.1%) who achieved remission one month after treatment initiation]. One patient did not respond to treatment and stopped after 25 sessions.
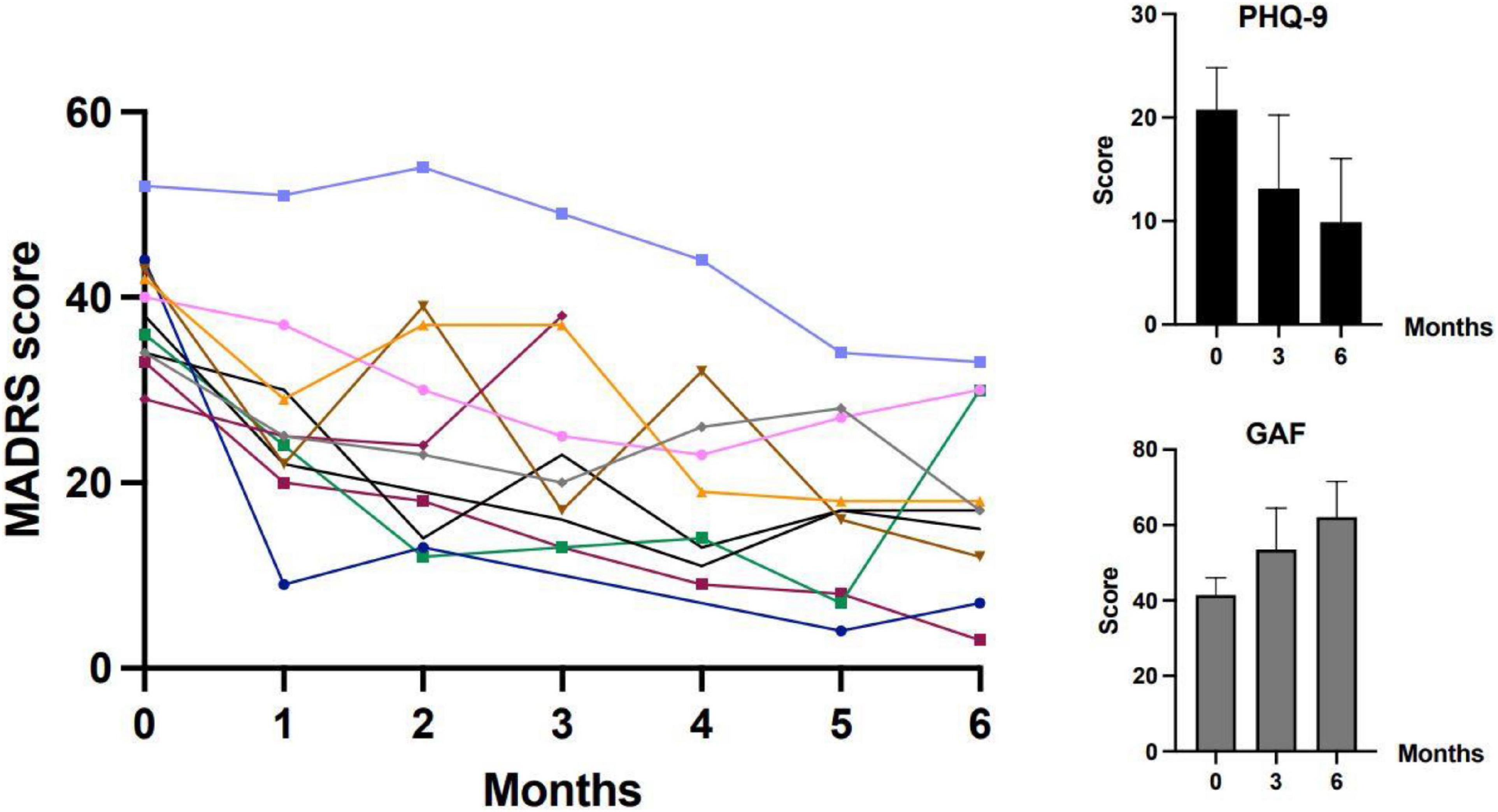
Figure 1. The evolution of depressive symptoms (through MADRS and PHQ-9) and global functioning (through GAF) during treatment. MADRS, Montgomery-Åsberg Depression Rating Scale; PHQ-9, Patient Health Questionnaire-9; GAF, Global Assessment of Functioning. The main figure (on the left) shows MADRS scores for individual participants. The two figures on the right report means and standard deviations for PHQ-9 and GAF.
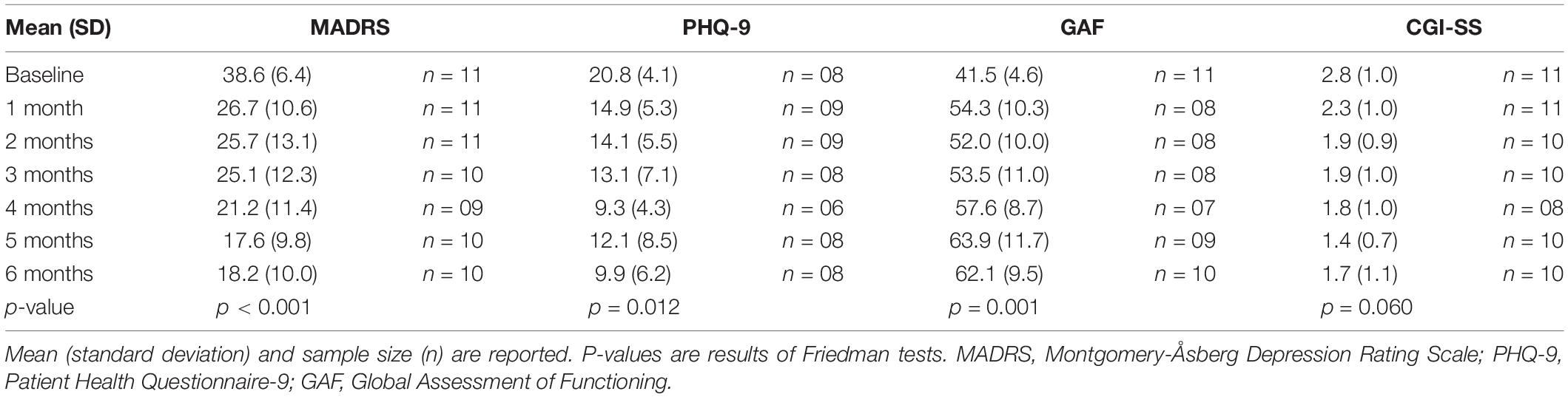
Table 1. Evolution of mood and functioning outcomes during treatment.
As for suicidality, the percentage of patients who were at least moderately to severely suicidal (CGI-SS score ≥ 3) went from 63.6% before treatment to 27.3% after 1 month of Esketamine treatment, and then to 20% after 3 months. However, the decrease was not statistically significant (Table 1).
Seven patients received psychotherapy in parallel with the administration of IN Esketamine: either cognitive and behavioral therapy focused on trauma (n = 3), or EMDR (n = 1) or both (n = 3). Psychotherapy occurred on average (SD) 3.6 (2.8) months after starting Esketamine treatment. Their post-traumatic symptoms were assessed through the PCL-5 before and after psychotherapy with a mean interval of 5.6 (5.5) months. The mean score went from 58.6 (3.9) before treatment to 32.7 (16.0) after treatment. The mean (SD) relative improvement was 45.3% (25.5).
Among the eleven patients included in the analyses, three patients stopped IN Esketamine before 6 months: one patient stopped 2 months after Esketamine initiation (i.e., 13 sessions) because of remission, one patient stopped after 4 months (16 sessions) due to travel difficulties and a third patient stopped due to lack of efficacy of IN Esketamine (25 sessions) and started treatment with a non-selective monoamine oxidase inhibitor.
The most frequent AEs were dissociation (n = 7), somnolence (n = 4), nausea (n = 4), sedation (n = 3), dizziness (n = 3), anxiety (n = 2), and increased blood pressure or hypertension (n = 1). Most side effects were moderate and did not require discontinuation of treatment. One patient had nausea and required anti-emetic treatment before sessions. For this patient, the increase of Esketamine dosage to 84 mg had to be delayed. The dissociative effects consisted of disinhibition with verbalization of traumatic events (n = 4) or derealization (n = 3). We did not observe any serious adverse effects throughout the study. In particular, no safety issue due to repeated Esketamine administration occurred in our study.
This pilot study provides the first data evaluating IN Esketamine treatment in patients with dual diagnosis of TRD and PTSD, suggesting that this treatment, in association with antidepressants and with psychotherapy, could rapidly reduce depressive symptoms in this population with a long-lasting effect up to 6 months. In our sample, two thirds of TRD patients achieved response and one third reached remission after 6 months of IN Esketamine treatment. The risk of suicide was importantly reduced, although not statistically significant: the percentage of moderately to severely suicidal patients was divided by 3 in 6 months of treatment. PTSD symptoms have also importantly improved for patients that had both Esketamine and trauma-focused therapy, with a mean (SD) reduction of 45.3% (25.5) of PCL-5 after 6 months of therapy. This latter result is exploratory and only concerns a sub-group of patients but seems clinically meaningful considering the severity, the resistance and the functional outcome of the disease presented by our population.
In previous studies, Esketamine has been shown to be effective in TRD. In our study, we found that patients with comorbid TRD and PTSD have similar to higher rates of response than patients with TRD alone in previous studies [63.6% in our study versus 45.6, 52.2, and 61.4% in TRANSFORM-1 (41) and TRANSFORM-2 (31) studies]. However, they have lower rates of remission (27.3% in our study versus 33.3, 34.8, and 46.5% in TRANSFORM-1 and TRANSFORM-2 studies). This difference may be explained by the persistence of residual symptoms that could be specific to the PTSD comorbidity. Several studies found that racemic ketamine could decrease PTSD symptoms (21–23, 42) but this effect was recently challenged (25). Still, the only study that previously explored the efficacy of racemic ketamine on comorbid TRD and PTSD found a quick and significant reduction of symptoms, but with a limited effect over time (median time to relapse of 41 days) (24). Our study therefore confirms these results with IN Esketamine.
This action of Esketamine in patients with both depressive and PTSD symptoms might be explained by common pathophysiological features. Indeed, in both depression and PTSD, patients are more sensitive to negative emotional stimuli which trigger an increased activation of amygdala and anterior cingulate cortex and a decreased activation of the prefrontal cortex (43, 44). Interestingly, low doses of ketamine have been shown to reverse that pattern in patients with MDD (45). On the other hand, PTSD is a risk factor for TRD (5, 6) and patients with TRD perceive their onset-related events as serious psychological distress symptoms (46). It was also shown that patients with TRD who have experienced traumatic events are relieved by trauma-focused psychotherapy (47), so one could postulate that part of the efficacy of ketamine on TRD may be related to a beneficial action on underlying traumas. Finally, ketamine facilitates fear memory extinction (48, 49) which could help patients with PTSD to have less avoidance behaviors and to enter in a psychotherapeutic process. The main mechanism of action of Esketamine is to block NMDA receptors on GABA interneurons and to activate the alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptors. This action might increase neurotrophic signaling, thereby restoring synaptic function and improving neural plasticity and synaptogenesis (50) in particular in the prefrontal cortex (51, 52). Ketamine reverses structural and functional deficits induced by chronic stress exposure (53), which could help both patients with PTSD and with depression. Indeed, in individuals with chronic PTSD, persistent, recurrent intrusions could represent a form of chronic stress that prolongs and worsens maladaptive biological changes, including synaptic atrophy, dysregulation of glutamatergic transmission, and disrupted connectivity in corticolimbic circuitry (54, 55). Finally, ketamine normalizes the disrupted connectivity between the prefrontal cortex, the default mode network and other key brain regions, that is observed in depression (56, 57) and could similarly restore cerebral connectivity in these regions in PTSD (58).
Importantly, the present study also demonstrated that repeated IN Esketamine sessions were safe and well-tolerated, with transient dissociative symptoms that disappeared within 2 h. Indeed, over 6 months, we did not observe any serious adverse effects. These data are consistent with previous ecological observations which did not identify new safety signals (59) compared to the initial data that allowed Esketamine approval. This is a crucial result since previous studies suggested that Esketamine could trigger higher dissociative symptoms than racemic ketamine when administered in acute trauma phases (60). On the contrary, the dissociative effects could induce a surprisingly positive impact. Indeed a trance state, as described during ketamine-assisted psychotherapy (61) was observed in our study for 6 patients (54.5%). It promoted communication and allowed some of them to verbalize their traumatic experience for the first time. Therapists then observed that these patients were getting rid of fear more easily, enabling them to create new positive associations. Such an effect could have directly emerged from the disinhibition and the fear extinction induced by ketamine (48, 49) or from an increased neuroplasticity (51, 52) that could have reduced the rigidity of traumatic memories, making them finally accessible to psychotherapy. Ketamine-assisted psychotherapy has shown to be a relevant approach in other chronic, severe or resistant diseases, e.g., in alcohol use disorder (62), heroin addiction (63), and TRD without comorbid PTSD (64). Previous articles developed clinical guides of ketamine-assisted psychotherapy (65, 66). However, its modalities, notably in the treatment of PTSD, remain to be better defined. More specifically, the optimal moment to start psychotherapy and how it should be articulated with Esketamine sessions in order to have the most benefit should be specified. Here we tentatively suggest that the first sessions may allow the patients to get used to subjective changes induced by Esketamine and to benefit from early anxiolytic and antidepressant effects. In this sense, it could be more appropriate to start trauma-focused psychotherapy a bit later. In contrast, patients could be accompanied before and during the first Esketamine sessions with techniques that have been developed to improve tolerance and avoid “bad-trip” during psychotropic-assisted therapy (67).
Despite encouraging results, our study had several limitations, notably the small number of patients included and the absence of sample size calculation. The open-label design and the absence of placebo control does not allow us to firmly conclude in terms of efficacy. In addition, there is an overlap between depressive symptoms and some PTSD symptoms and our study cannot accurately describe the respective effect of Esketamine on each of them or tease apart the respective contributions of the pharmacological and the psychotherapeutic treatment in the observed improvement. Moreover, we cannot eliminate a confounding effect of different drugs or other comorbid disorders since there was no control group. Quantitative measures of the intensity of dissociation during Esketamine administration would have allowed us to explore whether it was predictive of response or remission of PTSD symptoms. In the future, the efficacy of Esketamine-assisted therapy may be further assessed with a more structured protocol including a control group.
This pilot study is the first one to assess Esketamine efficacy on comorbid TRD and PTSD. Our results suggest rapid and sustained effects of Esketamine both on depressive and PTSD symptoms at 6 months even if patients were severely ill and importantly disabled by their disorders. The properties of Esketamine seem to combine particularly well with trauma-focused therapies and those two approaches probably have a synergistic effect. Esketamine could therefore be a treatment of choice in TRD patients with comorbid PTSD.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
MR, WE-H, OG, RG, VM, and LB conceived and conceptualized the study. MR, ChB, CaB, and DR collected data. VM and DR performed formal analysis of data collected. MR and VM wrote the preliminary draft. WE-H and LB revised and edited the final draft. All authors reviewed and approved the final draft of the manuscript and made substantial contributions to this study.
MR has received honoraria or consulting fees from Janssen-Cilag and Lundbeck-Otsuka. WE-H reports personal fees from Air Liquide, Chugai, Lundbeck, Janssen-Cilag, Otsuka, and UCB. LB has participated to a Medical Education Steering Committee for Janssen-Cilag. OG has received honoraria or consulting fees from EISAI, Lundbeck, Otsuka/Lundbeck, Janssen-Cilag, MAGPREP, and Bioprojet. RG has received compensation as a member of the scientific advisory board of Janssen, Lundbeck, Roche, SOBI, and Takeda. He has consulted and/or served as speaker for Astra Zeneca, Boehringer-Ingelheim, Pierre Fabre, Lilly, Lundbeck, MAPREG, Otsuka, Pileje, SANOFI, Servier, LVMH, and has received research support from Servier. Co-founder and stock shareholder: Regstem.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all the participants. We also thank Sandrine Philippe, a pharmacist, Corinne Lagniez, Carine Kerninon, Gérald Adler, Graziella Guesdon, and Christine Fichaux for assistance in Esketamine administration.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.865466/full#supplementary-material
1. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1789–858. doi: 10.1016/S0140-6736(18)32279-7
2. Fava M, Davidson KG. Definition and epidemiology of treatment-resistant depression. Psychiatr Clin North Am. (1996) 19:179–200. doi: 10.1016/S0193-953X(05)70283-5
3. Rush AJ, Thase ME, Dubé S. Research issues in the study of difficult-to-treat depression. Biol Psychiatry. (2003) 53:743–53. doi: 10.1016/s0006-3223(03)00088-x
4. Holtzmann J, Richieri R, Saba G, Allaïli N, Bation R, Moliere F, et al. [How to define treatment-resistant depression?]. Presse Med. (2016) 45:323–8. doi: 10.1016/j.lpm.2016.02.002
5. Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the national comorbidity survey. Arch Gen Psychiatry. (1995) 52:1048–60. doi: 10.1001/archpsyc.1995.03950240066012
6. Kaplan MJ, Klinetob NA. Childhood emotional trauma and chronic posttraumatic stress disorder in adult outpatients with treatment-resistant depression. J Nerv Ment Dis. (2000) 188:596–601. doi: 10.1097/00005053-200009000-00006
7. Kessler RC, Aguilar-Gaxiola S, Alonso J, Benjet C, Bromet EJ, Cardoso G, et al. Trauma and PTSD in the WHO world mental health surveys. Eur J Psychotraumatol. (2017) 8(Suppl. 5):1353383. doi: 10.1080/20008198.2017.1353383
8. Post LM, Zoellner LA, Youngstrom E, Feeny NC. Understanding the relationship between co-occurring PTSD and MDD: symptom severity and affect. J Anxiety Disord. (2011) 25:1123–30. doi: 10.1016/j.janxdis.2011.08.003
9. Karatzias T, Hyland P, Bradley A, Cloitre M, Roberts NP, Bisson JI, et al. Risk factors and comorbidity of ICD-11 PTSD and complex PTSD: findings from a trauma-exposed population based sample of adults in the United Kingdom. Depress Anxiety. (2019) 36:887–94. doi: 10.1002/da.22934
10. Bennabi D, Charpeaud T, Yrondi A, Genty JB, Destouches S, Lancrenon S, et al. Clinical guidelines for the management of treatment-resistant depression: French recommendations from experts, the French association for biological psychiatry and neuropsychopharmacology and the fondation FondaMental. BMC Psychiatry. (2019) 19:262. doi: 10.1186/s12888-019-2237-x
11. Johnston KM, Powell LC, Anderson IM, Szabo S, Cline S. The burden of treatment-resistant depression: a systematic review of the economic and quality of life literature. J Affect Disord. (2019) 242:195–210. doi: 10.1016/j.jad.2018.06.045
12. Kadriu B, Musazzi L, Henter ID, Graves M, Popoli M, Zarate CA. Glutamatergic neurotransmission: pathway to developing novel rapid-acting antidepressant treatments. Int J Neuropsychopharmacol. (2019) 22:119–35. doi: 10.1093/ijnp/pyy094
13. Mathews DC, Henter ID, Zarate CA. Targeting the glutamatergic system to treat major depressive disorder. Drugs. (2012) 72:1313–33. doi: 10.2165/11633130-000000000-00000
14. Li CT, Yang KC, Lin WC. Glutamatergic dysfunction and glutamatergic compounds for major psychiatric disorders: evidence from clinical neuroimaging studies. Front Psychiatry. (2019) 9:767. doi: 10.3389/fpsyt.2018.00767
15. Zarate CA, Singh JB, Carlson PJ, Brutsche NE, Ameli R, Luckenbaugh DA, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry. (2006) 63:856–64. doi: 10.1001/archpsyc.63.8.856
16. Schwenk ES, Viscusi ER, Buvanendran A, Hurley RW, Wasan AD, Narouze S, et al. Consensus guidelines on the use of intravenous ketamine infusions for acute pain management from the American society of regional anesthesia and pain medicine, the American academy of pain medicine, and the American society of anesthesiologists. Reg Anesth Pain Med. (2018) 43:456–66. doi: 10.1097/AAP.0000000000000806
17. Zheng W, Gu LM, Sun CH, Zhou YL, Wang CY, Lan XF, et al. Comparative effectiveness of repeated ketamine infusions in treating anhedonia in bipolar and unipolar depression. J Affect Disord. (2022) 300:109–13. doi: 10.1016/j.jad.2021.12.105
18. Zheng W, Zhou YL, Liu WJ, Wang CY, Zhan YN, Li HQ, et al. Rapid and longer-term antidepressant effects of repeated-dose intravenous ketamine for patients with unipolar and bipolar depression. J Psychiatr Res. (2018) 106:61–8. doi: 10.1016/j.jpsychires.2018.09.013
19. Li Z, Ruan M, Chen J, Fang Y. Major depressive disorder: advances in neuroscience research and translational applications. Neurosci Bull. 2021 37(6):863-880. Erratum Neurosci Bull. (2021).
20. Nair J, Singh Ajit S. The role of the glutamatergic system in posttraumatic stress disorder. CNS Spectr. (2008) 13:585–91.
21. Feder A, Parides MK, Murrough JW, Perez AM, Morgan JE, Saxena S, et al. Efficacy of intravenous ketamine for treatment of chronic posttraumatic stress disorder: a randomized clinical trial. JAMA Psychiatry. (2014) 71:681–8.
22. Feder A, Costi S, Rutter SB, Collins AB, Govindarajulu U, Jha MK, et al. A randomized controlled trial of repeated ketamine administration for chronic posttraumatic stress disorder. Am J Psychiatry. (2021) 178:193–202.
23. Duek O, Li Y, Kelmendi B, Amen S, Gordon C, Milne M, et al. Modulating amygdala activation to traumatic memories with a single ketamine infusion. medRxiv[Preprint]. (2021). doi: 10.1101/2021.07.07.21260166
24. Albott CS, Lim KO, Forbes MK, Erbes C, Tye SJ, Grabowski JG, et al. Efficacy, safety, and durability of repeated ketamine infusions for comorbid posttraumatic stress disorder and treatment-resistant depression. J Clin Psychiatry. (2018) 79:17m11634.
25. Abdallah CG, Roache JD, Gueorguieva R, Averill LA, Young-McCaughan S, Shiroma PR, et al. Dose-related effects of ketamine for antidepressant-resistant symptoms of posttraumatic stress disorder in veterans and active duty military: a double-blind, randomized, placebo-controlled multi-center clinical trial. Neuropsychopharmacology. (2022) 47:1574–81.
26. Muller J, Pentyala S, Dilger J, Pentyala S. Ketamine enantiomers in the rapid and sustained antidepressant effects. Ther Adv Psychopharmacol. (2016) 6:185–92.
27. Li L, Vlisides PE. Ketamine: 50 years of modulating the mind. Front Hum Neurosci. (2016) 10:612. doi: 10.3389/fnhum.2016.00612
28. Dinis-Oliveira RJ. Metabolism and metabolomics of ketamine: a toxicological approach. Forensic Sci Res. (2017) 2:2–10. doi: 10.1080/20961790.2017.1285219
29. European Medicines Agency. Spravato 28 mg Nasal Spray (Esketamine), Solution. Summary of Product Characteristics. (2021). Available online at: https://www.ema.europa.eu/en/documents/product-information/spravato-epar-product-information_en.pdf (accessed June 23, 2021).
30. U.S. Food and Drug Administration. SPRAVATO® (Esketamine) Nasal Spray, CIII. Prescribing Information. (2020). Available online at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/211243lbl.pdf (accessed June 23, 2021).
31. Popova V, Daly EJ, Trivedi M, Cooper K, Lane R, Lim P, et al. Efficacy and safety of flexibly dosed esketamine nasal spray combined with a newly initiated oral antidepressant in treatment-resistant depression: a randomized double-blind active-controlled study. Am J Psychiatry. (2019) 176:428–38. doi: 10.1176/appi.ajp.2019.19020172
32. Daly EJ, Trivedi MH, Janik A, Li H, Zhang Y, Li X, et al. Efficacy of esketamine nasal spray plus oral antidepressant treatment for relapse prevention in patients with treatment-resistant depression: a randomized clinical trial. JAMA Psychiatry. (2019) 76:893–903. doi: 10.1001/jamapsychiatry.2019.1189
33. Wajs E, Aluisio L, Holder R, Daly EJ, Lane R, Lim P, et al. Esketamine nasal spray plus oral antidepressant in patients with treatment-resistant depression: assessment of long-term safety in a phase 3, open-label study (SUSTAIN-2). J Clin Psychiatry. (2020) 81:19m12891. doi: 10.4088/JCP.19m12891
34. Salahudeen MS, Wright CM, Peterson GM. Esketamine: new hope for the treatment of treatment-resistant depression? A narrative review. Ther Adv Drug Saf. (2020) 11:2042098620937899. doi: 10.1177/2042098620937899
35. Banov MD, Landrum RE, Moore MB, Szabo ST. Switching to intranasal esketamine maintains the antidepressant response to intravenous racemic ketamine administration: a case series of 10 patients. J Clin Psychopharmacol. (2021) 41:594–9. doi: 10.1097/JCP.0000000000001456
36. European Medicines Agency. SPRAVATO 28 mg, Solution Pour Pulvérisation Nasale. Résumé des Caractéristiques Produit. (2017). Available online at: https://www.ema.europa.eu/en/documents/product-information/spravato-epar-product-information_fr.pdf (accessed June 23, 2021).
37. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. (1979) 134:382–9.
38. Ashbaugh AR, Houle-Johnson S, Herbert C, El-Hage W, Brunet A. Psychometric validation of the English and French versions of the posttraumatic stress disorder checklist for DSM-5 (PCL-5). PLoS One. (2016) 11:e0161645. doi: 10.1371/journal.pone.0161645
39. Hayasaka Y, Purgato M, Magni LR, Ogawa Y, Takeshima N, Cipriani A, et al. Dose equivalents of antidepressants: evidence-based recommendations from randomized controlled trials. J Affect Disord. (2015) 180:179–84. doi: 10.1016/j.jad.2015.03.021
40. Fekadu A, Donocik JG, Cleare AJ. Standardisation framework for the Maudsley staging method for treatment resistance in depression. BMC Psychiatry. (2018) 18:100. doi: 10.1186/s12888-018-1679-x
41. Fedgchin M, Trivedi M, Daly EJ, Melkote R, Lane R, Lim P, et al. Efficacy and safety of fixed-dose esketamine nasal spray combined with a new oral antidepressant in treatment-resistant depression: results of a randomized, double-blind, active-controlled study (TRANSFORM-1). Int J Neuropsychopharmacol. (2019) 22:616–30. doi: 10.1093/ijnp/pyz039
42. McGhee LL, Maani CV, Garza TH, Gaylord KM, Black IH. The correlation between ketamine and posttraumatic stress disorder in burned service members. J Trauma. (2008) 64(2 Suppl.):S195–8; discussion S197–8. doi: 10.1097/TA.0b013e318160ba1d
43. Hayes JP, Vanelzakker MB, Shin LM. Emotion and cognition interactions in PTSD: a review of neurocognitive and neuroimaging studies. Front Integr Neurosci. (2012) 6:89. doi: 10.3389/fnint.2012.00089
44. Groenewold NA, Opmeer EM, de Jonge P, Aleman A, Costafreda SG. Emotional valence modulates brain functional abnormalities in depression: evidence from a meta-analysis of fMRI studies. Neurosci Biobehav Rev. (2013) 37:152–63. doi: 10.1016/j.neubiorev.2012.11.015
45. Li C-T, Chen M-H, Lin W-C, Hong C-J, Yang B-H, Liu R-S, et al. The effects of low-dose ketamine on the prefrontal cortex and amygdala in treatment-resistant depression: a randomized controlled study. Hum Brain Mapp. (2016) 37:1080–90. doi: 10.1002/hbm.23085
46. Kimura A, Hashimoto T, Niitsu T, Iyo M. Presence of psychological distress symptoms associated with onset-related life events in patients with treatment-refractory depression. J Affect Disord. (2015) 175:303–9. doi: 10.1016/j.jad.2015.01.027
47. Minelli A, Zampieri E, Sacco C, Bazzanella R, Mezzetti N, Tessari E, et al. Clinical efficacy of trauma-focused psychotherapies in treatment-resistant depression (TRD) in-patients: a randomized, controlled pilot-study. Psychiatry Res. (2019) 273:567–74. doi: 10.1016/j.psychres.2019.01.070
48. Wei M-D, Wang Y-H, Lu K, Lv B-J, Wang Y, Chen W-Y. Ketamine reverses the impaired fear memory extinction and accompanied depressive-like behaviors in adolescent mice. Behav Brain Res. (2020) 379:112342. doi: 10.1016/j.bbr.2019.112342
49. Philippens IHCHM, Draaisma L, Baarends G, Krugers HJ, Vermetten E. Ketamine treatment upon memory retrieval reduces fear memory in marmoset monkeys. Eur Neuropsychopharmacol. (2021) 50:1–11. doi: 10.1016/j.euroneuro.2021.04.004
50. Duman RS, Aghajanian GK, Sanacora G, Krystal JH. Synaptic plasticity and depression: new insights from stress and rapid-acting antidepressants. Nat Med. (2016) 22:238–49.
51. Li N, Lee B, Liu R-J, Banasr M, Dwyer JM, Iwata M, et al. mTOR-dependent synapse formation underlies the rapid antidepressant effects of NMDA antagonists. Science. (2010) 329:959–64. doi: 10.1126/science.1190287
52. Pham TH, Gardier AM. Fast-acting antidepressant activity of ketamine: highlights on brain serotonin, glutamate, and GABA neurotransmission in preclinical studies. Pharmacol Ther. (2019) 199:58–90. doi: 10.1016/j.pharmthera.2019.02.017
53. Li N, Liu R-J, Dwyer JM, Banasr M, Lee B, Son H, et al. Glutamate N-methyl-D-aspartate receptor antagonists rapidly reverse behavioral and synaptic deficits caused by chronic stress exposure. Biol Psychiatry. (2011) 69:754–61. doi: 10.1016/j.biopsych.2010.12.015
54. Averill LA, Purohit P, Averill CL, Boesl MA, Krystal JH, Abdallah CG. Glutamate dysregulation and glutamatergic therapeutics for PTSD: evidence from human studies. Neurosci Lett. (2017) 649:147–55. doi: 10.1016/j.neulet.2016.11.064
55. Krystal JH, Abdallah CG, Averill LA, Kelmendi B, Harpaz-Rotem I, Sanacora G, et al. Synaptic loss and the pathophysiology of PTSD: implications for ketamine as a prototype novel therapeutic. Curr Psychiatry Rep. (2017) 19:74. doi: 10.1007/s11920-017-0829-z
56. Abdallah CG, Roache JD, Averill LA, Young-McCaughan S, Martini B, Gueorguieva R, et al. Repeated ketamine infusions for antidepressant-resistant PTSD: methods of a multicenter, randomized, placebo-controlled clinical trial. Contemp Clin Trials. (2019) 81:11–8.
57. Evans JW, Szczepanik J, Brutsché N, Park LT, Nugent AC, Zarate CA. Default mode connectivity in major depressive disorder measured up to 10 days after ketamine administration. Biol Psychiatry. (2018) 84:582–90. doi: 10.1016/j.biopsych.2018.01.027
58. Akiki TJ, Averill CL, Abdallah CG. A network-based neurobiological model of PTSD: evidence from structural and functional neuroimaging studies. Curr Psychiatry Rep. (2017) 19:81. doi: 10.1007/s11920-017-0840-4
59. Samalin L, Rothärmel M, Mekaoui L, Gaudré-Wattinne E, Codet MA, Bouju S, et al. Esketamine nasal spray in patients with treatment-resistant depression: the real-world experience in the French cohort early-access programme. Int J Psychiatry Clin Pract. (2022) 1–11. doi: 10.1080/13651501.2022.2030757
60. Schönenberg M, Reichwald U, Domes G, Badke A, Hautzinger M. Effects of peritraumatic ketamine medication on early and sustained posttraumatic stress symptoms in moderately injured accident victims. Psychopharmacology (Berl). (2005) 182:420–5. doi: 10.1007/s00213-005-0094-4
61. Dore J, Turnipseed B, Dwyer S, Turnipseed A, Andries J, Ascani G, et al. Ketamine assisted psychotherapy (KAP): patient demographics, clinical data and outcomes in three large practices administering ketamine with psychotherapy. J Psychoactive Drugs. (2019) 51:189–98. doi: 10.1080/02791072.2019.1587556
62. Grabski M, McAndrew A, Lawn W, Marsh B, Raymen L, Stevens T, et al. Adjunctive ketamine with relapse prevention-based psychological therapy in the treatment of alcohol use disorder. Am J Psychiatry. (2022) 179:152–62. doi: 10.1176/appi.ajp.2021.21030277
63. Krupitsky E, Burakov A, Romanova T, Dunaevsky I, Strassman R, Grinenko A. Ketamine psychotherapy for heroin addiction: immediate effects and two-year follow-up. J Subst Abuse Treat. (2002) 23:273–83. doi: 10.1016/s0740-5472(02)00275-1
64. Wilkinson ST, Rhee TG, Joormann J, Webler R, Ortiz Lopez M, Kitay B, et al. Cognitive behavioral therapy to sustain the antidepressant effects of ketamine in treatment-resistant depression: a randomized clinical trial. Psychother Psychosom. (2021) 90:318–27.
65. Bottemanne H, Baldacci A, Muller C, Boyreau A, Claret A. [Ketamine augmented psychotherapy (KAP) in mood disorder: user guide]. Encephale. (2021) 48:304–12. doi: 10.1016/j.encep.2021.08.011
66. Kolp E, Friedman HL, Krupitsky E, Jansen K, Sylvester M, Young MS, et al. Ketamine psychedelic psychotherapy: focus on its pharmacology, phenomenology, and clinical applications. Int J Transpers Stud. (2014) 33:84–140. doi: 10.24972/ijts.2014.33.2.84
Keywords: Esketamine, treatment-resistant depression, post-traumatic stress disorder, assisted-therapy, trauma-focused psychotherapy
Citation: Rothärmel M, Benosman C, El-Hage W, Berjamin C, Ribayrol D, Guillin O, Gaillard R, Berkovitch L and Moulier V (2022) Efficacy and Safety of Intranasal Esketamine in Patients With Treatment-Resistant Depression and Comorbid Chronic Post-traumatic Stress Disorder: Open-Label Single-Arm Pilot Study. Front. Psychiatry 13:865466. doi: 10.3389/fpsyt.2022.865466
Received: 29 January 2022; Accepted: 20 June 2022;
Published: 08 July 2022.
Edited by:
Celia J. A. Morgan, University of Exeter, United KingdomReviewed by:
Zezhi Li, Guangzhou Medical University, ChinaCopyright © 2022 Rothärmel, Benosman, El-Hage, Berjamin, Ribayrol, Guillin, Gaillard, Berkovitch and Moulier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maud Rothärmel, bWF1ZC5yb3RoYXJtZWxAY2gtbGVyb3V2cmF5LmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.