 Adolfo Piñón-Blanco1,2
Adolfo Piñón-Blanco1,2 Esperanza Vergara-Moragues3Olga Gutiérrez-Martínez2,4Patricia Fernández-Palleiro2Sonia Rodrigues5
Esperanza Vergara-Moragues3Olga Gutiérrez-Martínez2,4Patricia Fernández-Palleiro2Sonia Rodrigues5 Daniela Rodrigues-Amorím6María Teresa Lage-López7Ana González-López7Teresa Velasquez8Mónica Amorim5Manuel Lloves-Moratinos9Isabel Viéitez-Fernández10Gerardo Sabio-Fernandez9Rebeca Graña-Torralba10Vanesa Vilar-Díaz10Indalecio Carrera-Machado7Jesús Cancelo-Martinez9Adelino Ferreira5Susana Cardoso5
Daniela Rodrigues-Amorím6María Teresa Lage-López7Ana González-López7Teresa Velasquez8Mónica Amorim5Manuel Lloves-Moratinos9Isabel Viéitez-Fernández10Gerardo Sabio-Fernandez9Rebeca Graña-Torralba10Vanesa Vilar-Díaz10Indalecio Carrera-Machado7Jesús Cancelo-Martinez9Adelino Ferreira5Susana Cardoso5 Tania Rivera-Baltanás2,11Francisco Otero-Lamas1,2
Tania Rivera-Baltanás2,11Francisco Otero-Lamas1,2 José Manuel Olivares2,4,11*
José Manuel Olivares2,4,11* Carlos Spuch2,11*
Carlos Spuch2,11*- 1Drug Dependency Assistance Unit of Vigo City Council (CEDRO), Vigo, Spain
- 2Translational Neuroscience Group, Galicia Sur Health Research Institute (IIS Galicia Sur), SERGAS-UVIGO, Vigo, Spain
- 3Departamento de Psicobiología y Metodología en Ciencias del Comportamiento, Universidad Complutense de Madrid (UCM), Madrid, Spain
- 4Department of Psychiatry, Hospital Álvaro Cunqueiro, SERGAS, Vigo, Spain
- 5Division for the Intervention of Addictive Behaviors and Dependencies (DICAD) of the Regional Health Administration-North of Portugal, Porto, Portugal
- 6Picower Institute for Learning and Memory, Massachusetts Institute of Technology, Cambridge, MA, United States
- 7Citizens’ Association for the Fight Against Drugs (Asociación Ciudadana de Lucha Contra la Droga), A Coruña, Spain
- 8Comunidade Terapêutica Clínica do Outeiro, Porto, Portugal
- 9Citizens’ Association for the Fight Against Drugs (Asociación Ciudadana de Lucha Contra la Droga), ACLAD-Alborada, Vigo, Spain
- 10Ferrol Association of Drug Addictions of Ferrol (ASFEDRO), Ferrol, Spain
- 11CIBERSAM, Centro Investigación Biomédica en Red Salud Mental, Madrid, Spain
Substance-related disorders (SRD) have been consistently associated with alterations both in cognitive and executive functions, which affect to patients’ quality of life. The main objective of this work was to test the beneficial cognitive effects on patients with SRD after the implementation of “Trisquel,” an intervention program in board game format. To check the effectiveness of Trisquel program, a group of people diagnosed with SRD was randomly assigned either to the experimental group or to the control group. The experimental group performed Trisquel structured sessions twice a week during 3 months, while the control group performed routinely conventional therapeutic activities with the same frequency and duration. Neuropsychological tests were done to both groups before and after the intervention. After the 3 months of intervention the experimental group showed the following statistically significant improvements for WAIS-III subtests: number key, symbol search, arithmetic, direct digits, inverse digits, total digits, letters-numbers in the processing speed index and in the working memory index. Regarding STROOP tests, statistically significant progress was observed in the phonetic fluency letter P, phonetic fluency letter M, phonetic fluency letter R subtests, word-reading and word-color subtests. The control group only obtained improvements for WAIS-III subtests of arithmetic, letters-numbers and in the working memory index. The results of this study confirm that “Trisquel” is an effective intervention program for people diagnosed with SRD, getting improvements in processing speed (psychomotor and reading), attentional subprocesses (focused and sustained) and executive functions (updating and inhibition).
Introduction
The Diagnostic and Statistical Manual of Mental Disorders DSM-5 (1) defines substance-related disorders (SRD) as those health problems caused by acute or chronic use of psychoactive substances. SRD are characterized by the association of cognitive, behavioral and physiological symptoms that lead a person to seek and use a substance despite its negative consequences. To date, SRD remains one of the most prevalent chronic diseases and there is evidence that the cost of treating Drug Use Disorders is much lower than not treating drug dependence. Despite the advancement in the knowledge of SRD and its treatments, relapse and therapeutic failure continue to be frequent problems (2).
Scientific evidence shows that drugs consumption has been consistently associated with the presence of alterations in different neuropsychological processes, such as memory, attention or executive functions (2–4), and these neuropsychological alterations are present even after prolonged periods of abstinence (5).
In Spain, 70% of people with SRD present cognitive impairment (2), which is considered a common feature in this type of patients (6). Literature highlights the relevance of cognitive rehabilitation in SRD and there is a growing number of studies proposing and evaluating different therapeutic interventions aimed at improving the cognitive domains in treatment outcomes (2, 7–9). Experience shows that psychotherapeutic interventions, such as psychotherapy or relapse prevention are failing in the goal of improve cognitive functions in SRD patients (10).
By other hand, an efficacy study of a Mindfulness and Goal Management Program carried out in Spain, has found an improvement in SRD patients regarding executive functioning, processes of reflection and goal achievement in daily activities (11).
Trisquel
Given the clinical and social need to implement, invigorate and improve therapeutic and neurorehabilitative interventions in SRD patients, it was decided to create a new intervention program, called “Trisquel,” designed following the reference framework of a “serious game.”
“Serious games” do not have entertainment or amusement as their primary goal as are designed to educate, train or change behavior while entertaining players (12). Them have been developed in different formats encompassing both interactive role-playing games and board games (8, 13–18). In just over a decade, there has been an increase in its use as a tool to improve specific skills or competencies in different areas such as outreach, education, training, human resource management and health (12, 19, 20). Different studies on their effectiveness demonstrated that this type of therapeutic games create dynamic and motivating learning environments (13, 14, 19, 21–24). It has been noted that serious games combine three important aspects that contribute to the effectiveness of this approach: repetition, feedback, and motivation (8).
Previous experiences with serious games as “Road to awareness,” “The Trivia of Awareness,” “Escalation of Awareness,” “Trivia Psychotica,” “Reaction,” and “The Train” (21, 25–27), are clear examples of how a game can be a cognitive stimulation and rehabilitation tool, invigorating interventions, encouraging participation, providing information (psychoeducation) and working on social skills, problem solving, and deficit awareness.
For the design of “Trisquel” (22, 23, 28), the principles of neuropsychological rehabilitation have been taken into account. A neuropsychological assessment was performed, operational objectives were established, tasks were hierarchized and a continuous feedback system was provided. Besides that, different individualized strategies and techniques (restitution and compensation) (29) and others of group character (social skills) were combined and diverse theoretical reference models were taken into account.
The first “Trisquel” version began to be used in March 2008 and was completed in 2009 (Intellectual Property Registry VG 6-09) with a total of 590 theoretical-practical tests. Due to the good reception and evolution of the program, in 2014 a working group was created to carry out an extensive revision of the theoretical-practical contents of the entire program. Redundant, obsolete tests or those that did not provide information were eliminated, and the theoretical-practical contents of the program were expanded (28). To date, Trisquel has been used in over 12 centers in Spain and Portugal.
Although “Trisquel” has been tested in other populations with positive effects, the present work is the first one studying Trisquel effects on cognitive performance in SRD patients.
Materials and Methods
Design
Multicenter, longitudinal, prospective, randomized controlled study with pre and post neuropsychological measures.
Study Population
Participants were selected among those patients under treatment in assistance devices [day unit (UD) and therapeutic community (CT)] of the Galician Network of Care for Drug Addicts (A Coruña, Ferrol and Vigo, Spain) and of the Division for the Intervention of Addictive Behaviors and Dependencies (DICAD) of the Regional Health Administration-North of Portugal (Porto, Portugal). This project was conducted between the years 2018–2020.
Inclusion criteria were: (1) diagnosis of substance-related disorders and other addictions according to DSM-5, (2) having capacity to consent (competence), (3) reading the project information sheet and signing informed consent, (4) being of legal age, (5) being able to read and write.
Exclusion criteria were (1) illiteracy, (2) diagnosis of intellectual disability (IQ < 70), (3) moderate or severe neurological damage, (4) suffering from an acute psychiatric process, (5) inability to be evaluated, (6) having an abstinence of less than 15 days, (7) not having cognitive impairment according, the Montreal Cognitive Assessment (MOCA ≥ 26).
A total of 101 people were evaluated, all of them meeting the inclusion criteria and none of them meeting the exclusion criteria. The total 101 were invited to participate, although only 71 patients completed the study. 30 patients (29.70%) dropped out the treatment. From Trisquel group 9 patients (30%) abandoned (3 of them from CT and 6 UD). The reasons for leaving the unit were 17 dropouts, 10 expulsions (due to positive controls and disciplinary reasons) and 3 for health reasons.
Measuring Instruments
A questionnaire to collect sociodemographic data and tables shows a selected battery of neuropsychological tests (Tables 1, 2).
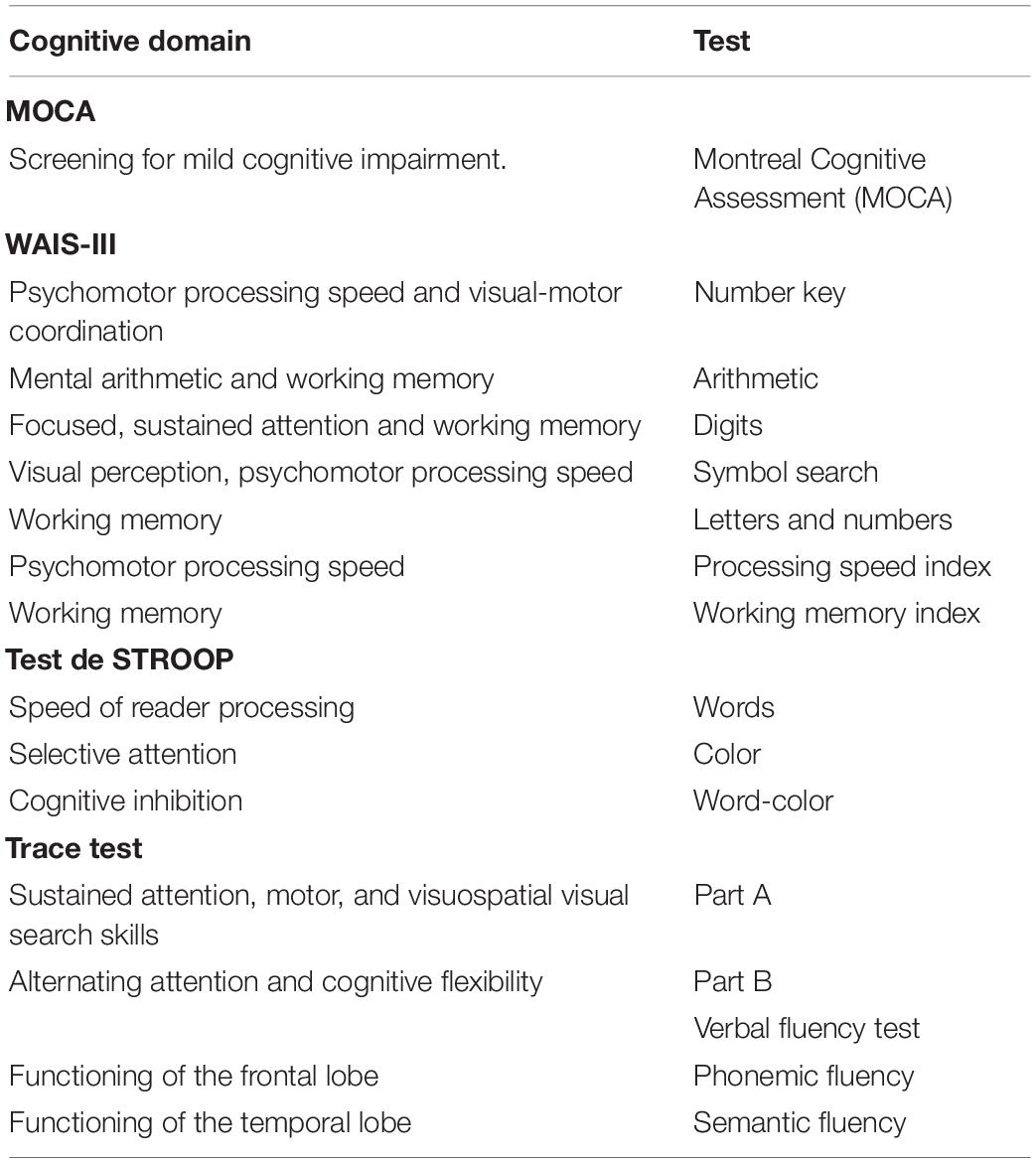
Table 1. Tests selected to build a battery of neurological tests and cognitive domains assessed.
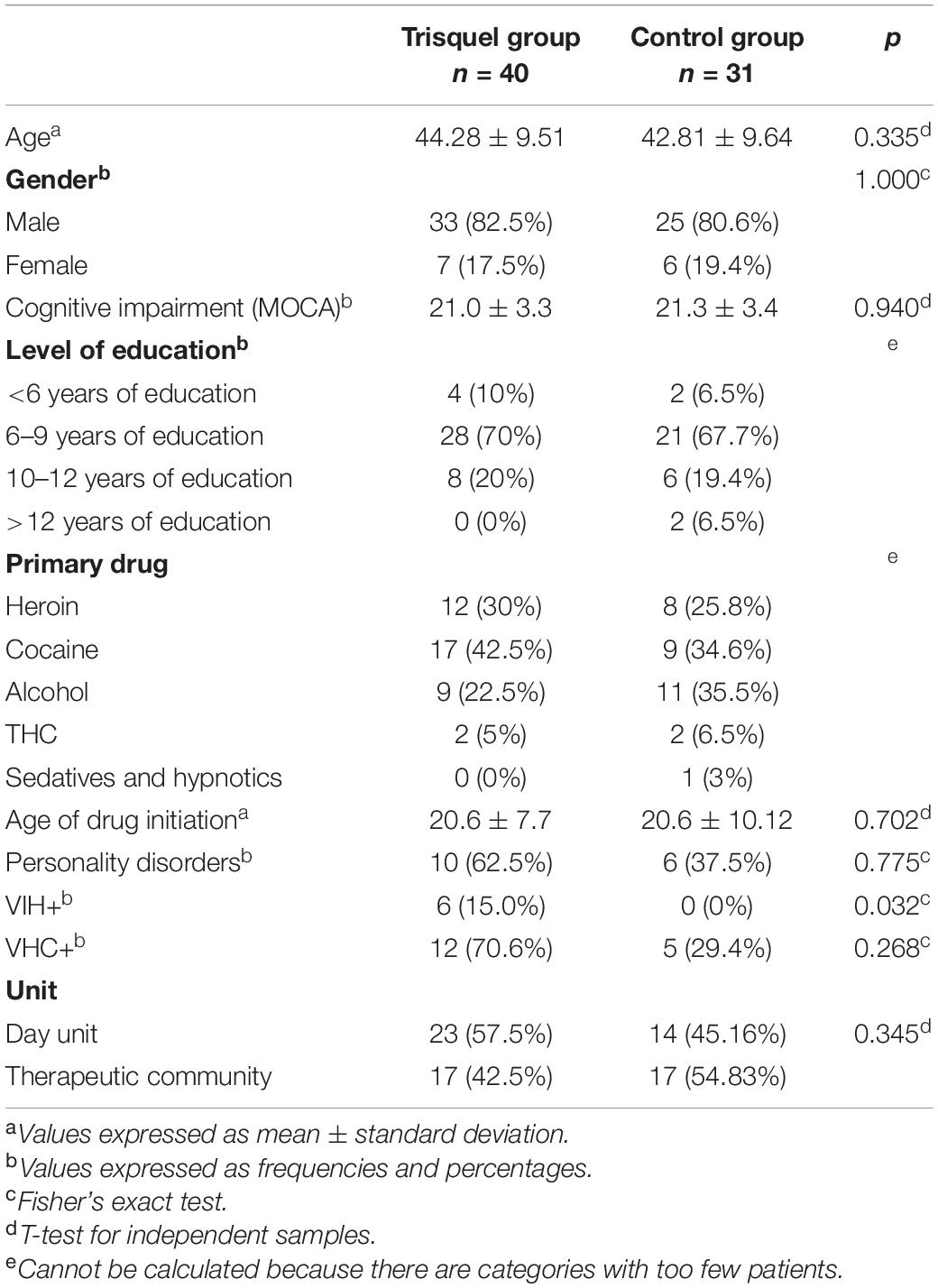
Table 2. Descriptive analysis of sociodemographic variables.
• Montreal Cognitive Assessment, MoCA (30): The Spanish version of the MoCA test (designed by Nasreddine) was used, with a maximum score of 30, being the cut-off points (suggested by the author), 25/26 for mild cognitive impairment and 17/18 for dementia. Normacog scales were applied (31).
• Scale for the Measurement of Adult and Adolescent Intelligence (WAIS III) (32): The number key and symbol search subtests were used to calculate the processing speed index. The letter-number, digit and arithmetic subtests allow to calculate the working memory index. The Spanish adaptation of the WAIS-III was used. Reliability coefficients (two halves) range between 0.77 and 0.96.
• STROOP test (33): It is an instrument that allows a very brief and simple evaluation reading processing speed, the ability to focus and redirect attention and the ability to resist interference. The reliability using the test-retest method is.89 for Stroop-P, 0.84 for Stroop-C and 0.73 for Stroop-PC. Neuronorm scales were used for young adult population in Spain (34).
• TMT Stroop Test (35): The test consists of two parts, A and B. Part A assesses sustained attention, processing speed, motor, and visuospatial visual search skills. Part B assesses alternating attention and cognitive flexibility. Reliability is between 0.86 and 0.94%. Neuronorma scales were used for young adult population in Spain (36).
• Verbal fluency tests (37): Phonemic Fluency test, a task of oral production of words before phonetic instructions, and the Semantic Fluency test (animals), a task of linguistic production that requires the implementation of the mechanisms of access to the lexicon. Neuronorm scales were used for the young adult population in Spain (38).
Procedure
The professionals who participated in the project received specific training on Trisquel’s methodology, dynamics and theoretical and practical contents prior to the start of the program. To avoid experimental biases and work overload in the centers, two psychologists were hired for the project to carry out the pre and post evaluations and the sessions with Trisquel in the respective centers.
All patients from the participating centers were filtered to meet the inclusion and exclusion criteria. On this filtered census, a simple random sampling technique was applied, until the estimated sample size was reached (between 6 and 14 patients per device). The individuals were then assigned to the experimental and control groups using a simple random sampling technique. All participants were provided a sociodemographic data collection questionnaire and a battery of neuropsychological tests before, and 1 week after the last intervention session. All tests were administered in two 30-min evaluation sessions under similar conditions.
Ethical Considerations and Personal Data Protection
This project was approved by the Autonomous Research Ethics Committee of Galicia (Registration Code: 2018/153). All patients were informed about the rehabilitation program before its start. Patients read and signed the informed consent, voluntarily accepted their participation in the study and did not receive any financial or other incentive. The processing, communication and transfer of data was performed in accordance with the provisions of the European Data Protection Regulation (EU Regulation 2016-679 of the European Parliament and of the Council of 27 April 2016).
Cognitive Rehabilitation
The experimental group was treated with Trisquel program and the control group received cognitive rehabilitation in the context of a biopsychosocial treatment, with a holistic and integrative approach, usually in the Treatment Facilities of the Drug Dependence Assistance Network of Galicia (Spain) and DICAD (Portugal). None of the two groups participated in any other rehabilitation program similar to the one proposed in this study. In order to carry out this work in the DICAD (Portugal), Trisquel has been translated and adapted to Portuguese language.
Program Description
Trisquel program combines psychoeducation and cognitive stimulation strategies. Following the theoretical framework of “serious games: the principles of neuropsychological rehabilitation were taken into account and different individual techniques were combined, such as restitution and compensation (29), and others of group character, such as social skills (19, 20). Likewise, different theoretical reference models were taken into account, such as the Therapeutic Milieu, learning from successes, the information processing model of Miller (39), the working memory model of Baddeley and Hitch (40), the model of retrieval processes of information from memory of Moscovitch (41) and the emotional processing model of Ekman (42).
Trsiquel program consists on a board, cards and thematic blocks of cards with 1,105 theoretical-practical tests. The theoretical-practical questions and cognitive tests are organized in thematic blocks and were elaborated according to the specific intervention needs of the population to be treated (relapse prevention, social skills, HIV prevention, mental health, health interventions, sexually transmitted diseases, etc.) and to the cognitive characteristics of the patients (degree of difficulty, level of cognitive impairment). During the sessions, the difficulty of the tasks is graded by the moderator (member of the therapeutic team) according to the previous results obtained by the participants in the working memory index of the WAIS-III (digits, arithmetic and letters-numbers) and in the MOCA cognitive screening test. Although “Trisquel” includes other additional thematic blocks, for the purpose of this study were used relapse prevention and HIV-AIDS, women, drug addiction, gender violence, social skills (communication pragmatics), executive functions (emotional expression and recognition, planning, inhibition, mention theory), manipulative cognitive tests (psychomotor skills, visoconstructive praxis, instrumental skills) and non-manipulative tests (processing speed, attention, phonemic and semantic fluency, verbal and visual memory, mental arithmetic, topographical orientation), health interventions (sleep hygiene, nutrition), and smoking (information, prevention and treatment) (Figure 1).

Figure 1. (A) Trisquel 2014 version, (B) box, professional’s manual and elements of the Trisquel 2014 game.
Dynamics of the game could be compared to that of the popular trivia game. The main differences lie in the figure of the moderator, the graduation and hierarchy of the difficulty of the cognitive tests, the establishment of game rules that encourage participation and the content of the tests themselves (psychoeducational interventions related to the treatment of patients and cognitive stimulation tasks). Trisquel is a competitive game in which, at the end of the session, there is a winning team and the game ends when a test of each colored square (Green, Orange, Blue, Yellow) is correctly performed and the central square (starting place) is reached again. Trisquel sessions involve a maximum of 6 or 7 patients divided into three groups. The cognitive tasks are performed individually and the group tasks can be agreed upon and answered by the members of the group. Each session is structured in terms of working on theoretical and practical aspects. The blocks of cards are ordered numerically (from simple to complex) and by topics to be covered. Most of the program’s theoretical-practical tests can be the subject of intervention by the professional, providing clarifications on some theoretical or practical concept, behavioral modifications of the maladaptive behaviors that arise in the role-playing or positive modeling of such behaviors. Since its creation in 2008, Trisquel has gone through several versions and design improvements during previous pilot study processes. For a more detailed description of the program and its characteristics (23, 28).
Trisquel Group
The experimental group consisted on the administration of Trisquel program for 3 months, through 24 sessions of ± 60 min duration, with a frequency of 2 sessions per week, in the context of a usual biopsychosocial treatment in the participating centers. The sessions were carried out in groups of a maximum of 6 or 7 patients (Figure 2).

Figure 2. Pictures of Trisquel sessions in different rehabilitation centers.
Control Group
This group carried out the routinely conventional therapeutic activities usually scheduled in each Care Center, consisting on Psychosocial Rehabilitation Support Programs (relapse prevention, occupational activities, and cognitive stimulation) implemented by a multidisciplinary team, with the same number of sessions (26), duration (± 60 min) and frequency (2 sessions per week) as the experimental group. The sessions were carried out in groups of a maximum of 6/7 patients. At the end of the study, all subjects in the control group were offered to perform the Trisquel program.
Data Analysis
A descriptive analysis of the data was performed. Frequencies and percentages were calculated for qualitative variables. For quantitative variables, means and deviations were calculated. The normality of the variables in each of the study groups was tested using the Shapiro-Wilks test. To identify differences between the two groups (Experimental and Control), the Mann-Whitney U-test or the t-test for independent samples were used. For the pre-post intervention comparison, the Wilcoxon test or the t-test for related samples were used. Cohen’s D was also calculated to quantify the effect size. The programs used were SPSS v.19 and G-power.
Results
Trisquel group consisted of 40 persons with a mean age of 44.28 years, of whom 33 (82.5%) were men and 7 (17.5%) women. Their mean MOCA cognitive impairment was 21.0 ± 3.3. Control group consisted of 31 persons with a mean age of 42.81 years of which 25 (80.6%) were men and 6 (19.4%) women. Their mean MOCA cognitive impairment was 21.3 ± 3.4. The descriptive analysis of the sociodemographic variables of each group is showed in Table 2. Statistically significant differences were found between groups in the variable’s Cannabis Addiction Diagnosis and HIV-associated organic pathology (Table 2).
Intergroup Differences
No statistically significant pre-intervention differences intergroup were found in relation to neuropsychological variables.
Intragroup Differences After the Intervention: Neuropsychological Assessment Module
In the cognitive performance of Trisquel group, statistically significant intragroup differences were found pre-post intervention in the subtests of number key (p = 0.001) with a moderate effect size (d = 0.763), symbol search (p = 0.001) with a moderate effect size (d = 0.598), arithmetic (p = 0.001) with a moderate effect size (d = 0.659), direct digits (p = 0.001) with a moderate effect size (d = 0.653), inverse digits (p = 0.025) with a small effect size (d = 0.385), total digits (p = 0.001) with a moderate effect size (d = 0.657), letters-numbers (p = 0.0001) with a large effect size (d = 0, 803) with WAIS-III, on the processing speed index (p = 0.001) with a moderate effect size (d = 0.598) and on the working memory index (p = 0.001) with a large effect size (d = 0.911) with WAIS-III, on the phonetic fluency subtest letter P (p = 0.001) with a moderate effect size (d = 0.756), phonetic fluency letter M (p = 0.004) with a small effect size (d = 0.488), phonetic fluency letter R (p = 0.002) with a small effect size (d = 0.575), in the word reading subtests (p = 0.007) with a small effect size (d = 0.372) and word-color of the STROOP test (p = 0.001) with a moderate effect size (d = 0.631).
In the cognitive performance of the control group, statistically significant intragroup differences were found pre-post intervention in the arithmetic (p = 0.003) with a small effect size (d = 0.488) and letter-number (p = 0.001) subtests with a moderate effect size (d = 0.652) and in the working memory index with WAIS-III (p = 0.002) with a moderate effect size (d = 0.572). Table 3 shows the mean scores and standard deviations of each group before and after treatment with respect to cognitive performance (Table 3).

Table 3. Intragroup comparison with respect to cognitive performance.
Discussion
The aim of this study was to analyze the effect of the board game intervention program “Trisquel” on cognitive performance in people with SRD. The former clinical experience with Trisquel of several professionals in different centers after 13 years of implementation was suggesting that Trisquel helps to reduce therapist-patient distances, facilitates group dynamics, stimulates cognitive functions, is a versatile and adaptable tool to the needs of each patient (level of impairment) and allows the development of motivation on the part of the patients. It was also observed that Trisquel favors the incentive to win, the challenge of reaching a goal and the sense of efficacy, the feedback of progress, the greater adhesion of the members of the same team.
Due to these preliminary observations and the interest aroused by the program in recent years, it was decided to initiate a process of evaluation of the effectiveness of this therapeutic game in different populations (mental health and addictions). This study shows that Trisquel leads to improvements in processing speed, attentional subprocesses and executive functions in patients with SRD diagnosis. Overall, the results of this work are congruent with other studies that support the use of serious games in the clinical approach of patients with different mental disorders and, more specifically, it provides evidence on the usefulness of an intervention program in board game format to induce improvements in cognitive-executive functioning in SRD patients.
In order to be able to discuss the results, an interpretation of the results was performed following a structure based on a process analysis (processing speed, attentional subprocesses and executive components). To perform this analysis, different theoretical reference models were taken into account such as the factorial structure of attention (43), the clinical model of attention and the factorial model of executive components (44). Table 4 shows a comparison of the cognitive performance of both groups, where Trisquel group obtained statistically significant improvements in most of the cognitive-executive processes evaluated in this study.
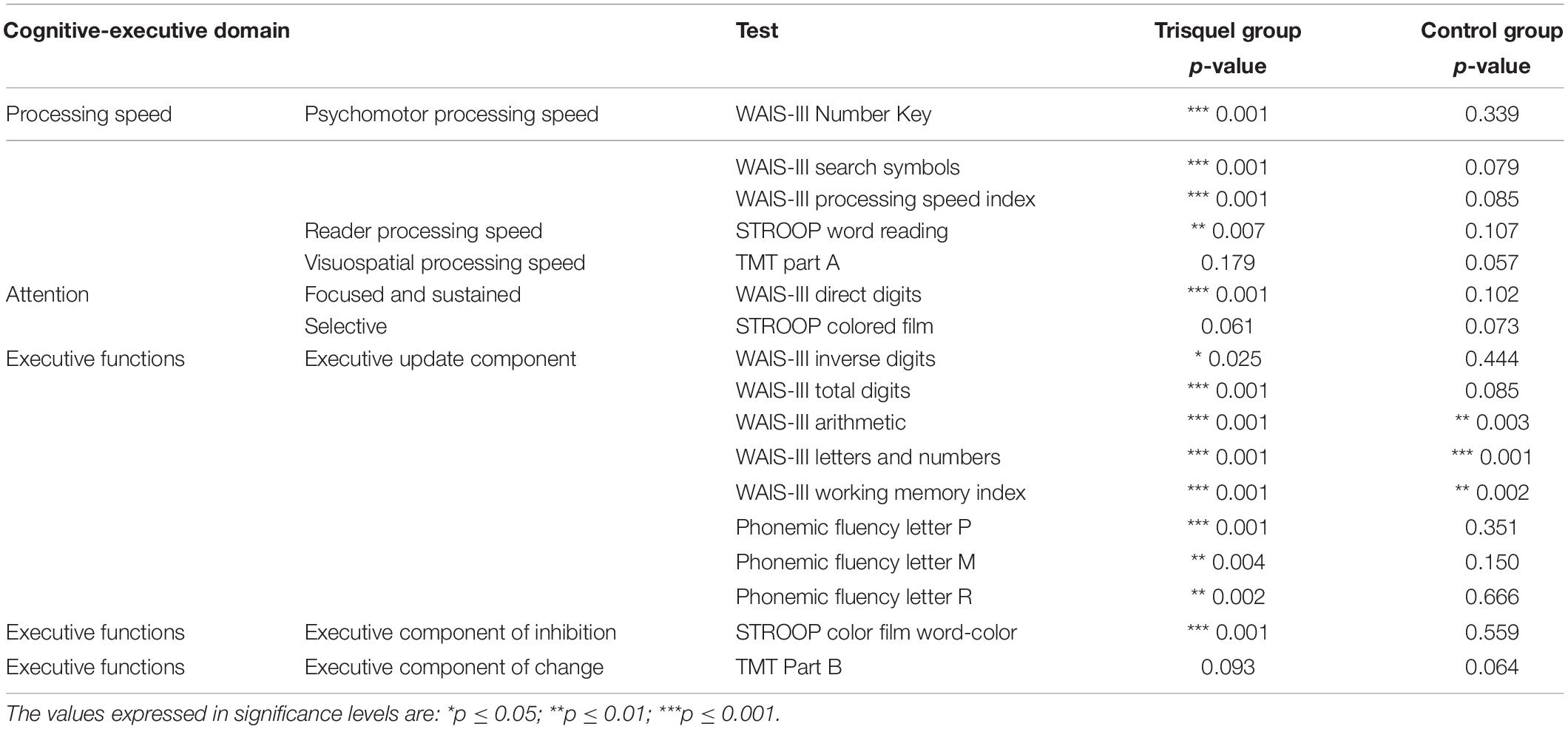
Table 4. Process-based intragroup comparison of cognitive performance.
According factorial structure of attention it is understood that processing speed reflects a basic property of the system where attention is implemented, and considers that it is a modulating factor of attentional performance (43). Trisquel group obtained statistically significant improvements in two of the three types of processing speed tasks evaluated (psychomotor and reading). These results are congruent with those obtained by other rehabilitation programs in which a significant improvement in processing speed is obtained after an intervention program (45, 46). A meta-analysis study on the evaluation of the efficacy of Goal Management Training concludes that intervention programs demonstrated efficacy in different populations by improving functioning in all cognitive-executive domains except processing speed (47, 48).
Regarding the attentional subprocesses performance, following the Clinical Model of Attention (one of the most referenced attention models in the literature), the results of the present study show that in Trisquel group statistically significant improvements were found in the subprocesses of focused and sustained attention, results in line with what has been found with other studies after the completion of a specialized rehabilitation program (45, 49). On the other hand, in control group no statistically significant improvements were found in any of the attentional subprocesses evaluated. These results may be consequence of the specific characteristics of Trisquel program (dynamic and motivating context, 266 cognitive-executive stimulation tasks, continuous reinforcement and feedback by the moderator, group dynamics, social exposure, etc.) or may be the result of the systematic repetition of a series of cognitive stimulation (restoration) exercises over a prolonged period of time. Overall, the results of this work are congruent with other studies that support the use of serious games in the clinical approach of patients with different mental disorders. Also, more specifically, this study provides evidence on the usefulness of an intervention program in board game format to induce improvements in cognitive-executive functioning in patients with SRD (13, 14, 19), in which it is consistently demonstrated that by challenging participants to think, explore and respond, they are motivated to learn new skills, knowledge, attitudes and behaviors, validating serious games as effective treatments of different psychiatric pathologies (21, 23, 24). Regarding executive functioning in the present study, and following one of the most referenced models of executive functioning in the literature (44), it was found that in the executive functioning of Trisquel group, statistically significant differences were found in the executive components of updating (working memory and phonemic fluency) and inhibition (cognitive).
In relation to the improvement of executive component of updating, the results of the present work are consistent with previous studies in which improvements in working memory are reported after the completion of a specialized rehabilitation program (2, 7, 11, 50, 51). Different studies show that the specific work of working memory is a facilitator of cognitive functions such as learning, verbal comprehension, thinking, reasoning or decision-making and a generator of an efficient buffering effect against attentional bias toward salient stimuli related to substance use (52, 53). Similar results to those obtained in the present study have been found in other populations with psychiatric pathologies (54, 55). Specifically, in a recent study assessing the efficacy of Trisquel in patients with a diagnosis of schizophrenia spectrum and other psychotic disorders, improvements in working memory were found after Trisquel program (23). Instead, other studies did not found benefits in specific working memory work, finding no effect on craving, substance use or attention bias (56). On the other hand, control group also obtained a statistically significant improvement in the executive updating component (working memory), indicative that biopsychosocial treatments with a holistic and integrative approach also generate changes in executive functioning, similar to those obtained with cognitive training programs. In this sense, this work may be one of the first studies that evaluates the efficacy of an intervention program in board game format compared to the holistic and integrative treatment model offered to patients with SRD in the care facilities (day unit, therapeutic community) of the Galician and Portuguese network of assistance to drug addicts.
In respect to the results obtained in the executive component of inhibition, Trisquel group obtained statistically significant improvements in the cognitive inhibition task (word-color) of the STROOP test, an executive component that allows us to stop an automated response and enables the inhibition of alternative learned behaviors as in this case represents the reading of words. These results are in line with other studies conducted with SRD patients, after the completion of a rehabilitation program such as Goal Management Training, one of the best validated interventions for executive dysfunction (47). Intervention program that has demonstrated its efficacy alone or in combination with other types of interventions such as mindfulness (11, 50). On the other hand, the control group obtained a worse performance in the cognitive inhibition task of the STROOP test.
Regarding the limitations of the present study, it can be said that the main one was not having studied the reasons for abandoning treatment, nor having correlated the different reasons for abandonment with the level of cognitive-executive deterioration of the patients studied. Another limitation was the absence of follow-up assessments. For this reason, no conclusions can be drawn as to whether the observed cognitive improvement contributed to maintaining abstinence in the following months, a fact found in other studies (57). In other studies it was found that the improvements observed at the end of cognitive training tend to be lost 6 months after the end of the intervention (45), an aspect that has not been assessed in this study either. Future efficacy studies should take these limitations into account.
Conclusion
The creation of Trisquel in 2008 was motivated by the clinical need to dynamize the therapeutic interventions offered to patients. In this study, the aims were to dynamize the psychoeducational group (relapse prevention, social skills, HIV-AIDS) and to include neurorehabilitative interventions. For this reason, a game format was chosen, which allows to generate a therapeutic context that facilitates learning (therapeutic milieu) and allows to work in vivo on aspects of group interaction (social skills, emotional expression and recognition).
The present study has important implications for research and clinical practice. It provides explicit information for the planning of future studies (sample selection, assessment protocol, procedure, process-based analysis of results), and evidence of its feasibility. It represents an example of how an intervention program in board game format can generate a motivating therapeutic context that induces improvements in cognitive-executive performance, health perception, perceived symptomatology. It can be considered a versatile and dynamic tool that each professional can adapt to their daily intervention needs. This work shows how an intervention program in board game format integrated in a bio-psycho-social treatment with a holistic and integrative approach, can improve the cognitive-executive performance of patients with cognitive impairment under treatment in care facilities for people with substance-related disorders.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of Vigo, Pontevedra, and Ourense Registration Code: 2018/153. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AP-B: conceptualization, methodology, writing—reviewing and editing, and supervision. EV-M: methodology and writing—original draft preparation. OG-M: methodology and investigation. PF-P, SR, ML-L, TV, MA, RG-T, AG-L, and VV-D: investigation. D-RA: writing—original draft preparation. ML-M, IV-F, GS-F, JC-M, AF, and SC: project administration. IC-M, FO-L, and JO: project administration, writing—original draft preparation, and supervision. TR-B: data curation and writing—original draft preparation. CS: data curation, supervision, writing–reviewing and editing, and funding acquisition. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by the Instituto de Salud Carlos III/FEDER (ISCIII) (grant no. PI20/00937), and Ministerio de Sanidad—Delegación del Gobierno para el Plan Nacional sobre Drogas (grant nos. 2020I054 and 2017I054), also by the GAIN (grant nos. IN607B 2018/17 and IN607B2021/12), and FCT, Fundação para a Ciência e Tecnologia (grant no. SFRH/BD/135623/2018).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank the professionals and patients of the Asociación Ciudadana de Lucha Contra la Droga (ACLAD) of La Coruña, Asociación Ferrolana de Drogodependencias de Ferrol (Asfedro), Asociación Ciudadana de Lucha Contra la Droga Alborada of Vigo, Unidad Asistencial de Drogodependencias CEDRO of Vigo, Comunidade terapéutica Ponte de Pedra of the ARS Norte IP, Porto and the Clínica de Outeiro in Porto, who made it possible to carry out the present study, for their collaboration. This is a short text to acknowledge the contributions of specific colleagues, institutions, or agencies that aided the efforts of the authors.
References
1. Barnhill JW American Psychiatric Association. Desk Reference to the Diagnostic Criteria from DSM-5. Virginia, VA: American Psychiatric Publishing (2013).
2. Verdejo-Garcia A. Cognitive training for substance use disorders: neuroscientific mechanisms. Neurosci Biobehav Rev. (2016) 68:270–81. doi: 10.1016/J.NEUBIOREV.2016.05.018
3. Garavan H, Stout JC. Neurocognitive insights into substance abuse. Trends Cogn Sci. (2005) 9:195–201. doi: 10.1016/J.TICS.2005.02.008
4. Vázquez-Justo E, Blanco AP, Vergara-Moragues E, Gestoso CG, Pérez-García M. Cognitive reserve during neuropsychological performance in HIV intravenous drug users. Appl Neuropsychol Adult. (2014) 21:288–96. doi: 10.1080/23279095.2013.813852
5. Fernández-Serrano MJ, Pérez-García M, Verdejo-García A. What are the specific vs. generalized effects of drugs of abuse on neuropsychological performance? Neurosci Biobehav Rev. (2011) 35:377–406. doi: 10.1016/J.NEUBIOREV.2010.04.008
6. Rojo-Mota G, Pedrero-Pérez EJ, de León JMRS, Llanero-Luque M, Puerta-García C. Neurocognitive screening in substance addicts: the montreal cognitive assessment. Rev Neurol. (2013) 56:129–36. doi: 10.33588/rn.5603.2012628
7. Bickel WK, Moody L, Quisenberry A. Computerized working-memory training as a candidate adjunctive treatment for addiction. Alcohol Res. (2014) 36:123–6.
8. Gamito P, Oliveira J, Lopes P, Brito R, Morais D, Silva D, et al. Executive functioning in alcoholics following an mHealth cognitive stimulation program: randomized controlled trial. J Med Internet Res. (2014) 16:e102. doi: 10.2196/JMIR.2923
9. Rezapour T, Hatami J, Farhoudian A, Sofuoglu M, Noroozi A, Daneshmand R, et al. NEuro COgnitive REhabilitation for disease of addiction (NECOREDA) program: from development to trial. Basic Clin Neurosci. (2015) 6:291–8.
10. Domínguez-Salas S, Díaz-Batanero C, Lozano-Rojas OM, Verdejo-García A. Impact of general cognition and executive function deficits on addiction treatment outcomes: systematic review and discussion of neurocognitive pathways. Neurosci Biobehav Rev. (2016) 71:772–801. doi: 10.1016/J.NEUBIOREV.2016.09.030
11. Valls-Serrano C, Caracuel A, Verdejo-Garcia A. Goal management training and mindfulness meditation improve executive functions and transfer to ecological tasks of daily life in polysubstance users enrolled in therapeutic community treatment. Drug Alcohol Depend. (2016) 165:9–14. doi: 10.1016/J.DRUGALCDEP.2016.04.040
12. Lau HM, Smit JH, Fleming TM, Riper H. Serious games for mental health: are they accessible, feasible, and effective? a systematic review and meta-analysis. Front psychiatry. (2017) 7:209. doi: 10.3389/FPSYT.2016.00209
13. Gauthier A, Kato PM, Bul KCM, Dunwell I, Walker-Clarke A, Lameras P. Board games for health: a systematic literature review and meta-analysis. Games Health J. (2019) 8:85–100. doi: 10.1089/g4h.2018.0017
14. Nakao M. Special series on ‘effects of board games on health education and promotion’ board games as a promising tool for health promotion: a review of recent literature. Biopsychosoc Med. (2019) 13:5. doi: 10.1186/S13030-019-0146-3
15. Estrada-Plana V, Esquerda M, Mangues R, March-Llanes J, Moya-Higueras JA. Pilot study of the efficacy of a cognitive training based on board games in children with attention-deficit/hyperactivity disorder: a randomized controlled trial. Games Health J. (2019) 8:265–74. doi: 10.1089/G4H.2018.0051
16. Estrada-Plana V, Montanera R, Ibarz-Estruga A, March-Llanes J, Vita-Barrull N, Guzmán N, et al. Cognitive training with modern board and card games in healthy older adults: two randomized controlled trials. Int J Geriatr Psychiatry. (2021) 36:839–50. doi: 10.1002/GPS.5484
17. Mayer I, Bekebrede G, Harteveld C, Warmelink H, Zhou Q, Van Ruijven T, et al. The research and evaluation of serious games: toward a comprehensive methodology. Br J Educ Technol. (2014) 45:502–27. doi: 10.1111/BJET.12067
18. Zagal JP, Rick J, Hsi I. Collaborative games: lessons learned from board games. Simul Gaming. (2016) 37:24–40. doi: 10.1177/1046878105282279
19. Akl EA, Kairouz VF, Sackett KM, Erdley WS, Mustafa RA, Fiander M, et al. Educational games for health professionals. Cochrane database Syst Rev. (2013) 2013:CD006411. doi: 10.1002/14651858.CD006411.PUB4
20. Castro-Sánchez E, Kyratsis Y, Iwami M, Rawson TM, Holmes AH. Serious electronic games as behavioural change interventions in healthcare-associated infections and infection prevention and control: a scoping review of the literature and future directions. Antimicrob Resist Infect Control. (2016) 5:34. doi: 10.1186/S13756-016-0137-0
21. Torres A, Mendez LP, Merino H, Moran EA. Improving social functioning in schizophrenia by playing the train game. Psychiatr Serv. (2002) 53:799–801. doi: 10.1176/APPI.PS.53.7.799
22. Blanco AP. Rehabilitation program for deficit awareness “the Trisquel”. J Psychol Clin Psychiatry. (2017) 7:00440. doi: 10.15406/jpcpy.2017.07.00440
23. Piñón-Blanco A, Vergara-Moragues E, Fernández-Martínez R, Gutiérrez-Martínez O, Álvarez-Couñago MC, Martínez-Reglero C, et al. Effectiveness of the “Trisquel” board game intervention program for patients with schizophrenia spectrum disorders. Actas Esp Psiquiatr. (2020) 48:209–19.
24. Vázquez-Campo M, Maroño Y, Lahera G, Mateos R, García-Caballero A. e-motional training§: pilot study on a novel online training program on social cognition for patients with schizophrenia. Schizophr Res Cogn. (2016) 4:10–7. doi: 10.1016/j.scog.2015.11.007
25. Chittum WR, Johnson K, Chittum JM, Guercio JM, Mcmorrow MJ. Road to awareness: an individualized training package for increasing knowledge and comprehension of personal deficits in persons with acquired brain injury. Brain Inj. (1996) 10:763–76. doi: 10.1080/026990596124034
26. Zhou J, Chittum R, Johnson K, Poppen R, Guercio J, McMorrow MJ. The Utilization of a Game Format to Increase Knowledge of Residuals Among People with Acquired Brain Injury. (1996). Available online at: https://journals.lww.com/headtraumarehab/abstract/1996/02000/the_utilization_of_a_game_format_to_increase.7.aspx (accessed on May 6, 2020).
27. Caballero-Coulon MC, Ferri-Campos J, Garcia-Blazquez MC, Chirivella-Garrido J, Renau-Hernandez O, Ferri-Salvador N, et al. [The ‘awareness climbing’: an educational board game for improving self-awareness following acquired brain injury]. Rev Neurol. (2007) 44:334–8. doi: 10.33588/rn.4406.2006190
29. Butfield E, Zangwill OL. Re-education in aphasia; a review of 70 cases. J Neurol Neurosurg Psychiatry. (1946) 9:75–9. doi: 10.1136/JNNP.9.2.75
30. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. (2005) 53:695–9. doi: 10.1111/J.1532-5415.2005.53221.X
31. Ojeda N, del Pino R, Ibarretxe-Bilbao N, Schretlen DJ, Peña J. Montreal cognitive assessment test: normalization and standardization for Spanish population. Rev Neurol. (2016) 63:488–96. doi: 10.33588/rn.6311.2016241
32. Wechsler D. Escala de Inteligencia de Wechsler Para Adultos-III [Wechsler Adult Intelligence Scale]. Manual de Aplicación y Corrección. 2nd, ed. Madrid: TEA Ediciones (2001).
33. Golden CJA. Group version of the stroop color and word test. J Pers Assess. (1975) 39:386–8. doi: 10.1207/s15327752jpa3904_10
34. Rognoni T, Casals-Coll M, Sánchez-Benavides G, Quintana M, Manero RM, Calvo L, et al. Spanish normative studies in young adults (NEURONORMA young adults project): norms for stroop color–word interference and tower of London-drexel university tests. Neurol. (2013) 28:73–80. doi: 10.1016/j.nrleng.2012.02.004
35. Reed JC, Reed HBC. ‘The halstead—reitan neuropsychological battery’. In: Goldstein G, Incagnoli TM editors. Contemporary Approaches to Neuropsychological Assessment. Critical Issues in Neuropsychology. Boston, MA: Springer (1997). p. 93–129.
36. Tamayo F, Casals-Coll M, Sánchez-Benavides G, Quintana M, Manero RM, Rognoni T, et al. [Spanish normative studies in a young adult population (NEURONORMA young adults Project): norms for the verbal span, visuospatial span, letter-number sequencing, trail making test and symbol digit modalities test]. Neurologia. (2012) 27:319–29. doi: 10.1016/J.NRL.2011.12.020
37. Benton AL, Hamsher KD, Sivan AB. Multilingual Aphasia Examination. Iowa, IA: AJA Associates (1989).
38. Casals-Coll M, Sánchez-Benavides G, Quintana M, Manero RM, Rognoni T, Calvo L, et al. Spanish normative studies in young adults (NEURONORMA young adults project): norms for verbal fluency tests. Neurol. (2013) 28:33–40. doi: 10.1016/j.nrleng.2012.02.003
39. Miller GA. The magical number seven, plus or minus two: some limits on our capacity for processing information. Psychol Rev. (1956) 63:81–97. doi: 10.1037/h0043158
40. Baddeley AD, Hitch G. Working memory. Psychol Learn Motiv. (1974) 8:47–89. doi: 10.1016/S0079-7421(08)60452-1
41. Moscovitch M. Memory and working with memory: evaluation of a component process model and comparisons with other models. In: DL Schacter, E Tulving editors. Memory Systems. (Vol. 224), Cambridge, MA: MIT Press (1994). p. 369-94.
42. Ekman P. Universals and cultural differences in facial expressions of emotion. In: J Cole editor. Nebraska Symposium on Motivation. (Vol. 19), Lincoln, NE: University of Nebraska Press (1972). p. 207.
43. Ríos Lago M, Periáñez JA, Muñoz-Céspedes JM. Attentional control and slowness of information processing after severe traumatic brain injury. Brain Inj. (2004) 18:257–72. doi: 10.1080/02699050310001617442
44. Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The unity and diversity of executive functions and their contributions to complex ‘Frontal Lobe’ tasks: a latent variable analysis. Cogn Psychol. (2000) 41:49–100. doi: 10.1006/COGP.1999.0734
45. Frías-Torres C, Moreno-España J, Ortega L, Barrio P, Gual A, Teixidor L. Remediation therapy in patients with alcohol use disorders and neurocognitive disorders: a pilot study. Adicciones. (2018) 30:93–100. doi: 10.20882/ADICCIONES.757
46. Goldstein G, Haas GL, Shemansky WJ, Barnett B, Salmon-Cox S. Rehabilitation during alcohol detoxication in comorbid neuropsychiatric patients. J Rehabil Res Dev. (2005) 42:225–34. doi: 10.1682/JRRD.2004.03.0040
47. Stamenova V, Levine B. Effectiveness of goal management training§in improving executive functions: a meta-analysis. Neuropsychol Rehabil. (2019) 29:1569–99. doi: 10.1080/09602011.2018.1438294
48. Lewis KE, Aujayeb A, Aaraj A Al, Henshall D, Gajewska-Knapik K, Javed H, et al. Convalescent plasma in patients admitted to hospital with COVID-19 (RECOVERY): a randomised controlled, open-label, platform trial. Lancet. (2021) 397:2049–59. doi: 10.1016/S0140-6736(21)00897-7
49. Fals-Stewart W, Lam WKK. Computer-assisted cognitive rehabilitation for the treatment of patients with substance use disorders: a randomized clinical trial. Exp Clin Psychopharmacol. (2010) 18:87–98. doi: 10.1037/A0018058
50. Alfonso JP, Caracuel A, Delgado-Pastor LC, Verdejo-García A. Combined Goal Management Training and Mindfulness meditation improve executive functions and decision-making performance in abstinent polysubstance abusers. Drug Alcohol Depend. (2011) 117:78–81. doi: 10.1016/J.DRUGALCDEP.2010.12.025
51. Rass O, Schacht RL, Buckheit K, Johnson MW, Strain EC, Mintzer MZ. A randomized controlled trial of the effects of working memory training in methadone maintenance patients. Drug Alcohol Depend. (2015) 156:38–46. doi: 10.1016/J.DRUGALCDEP.2015.08.012
52. Deldar Z, Ekhtiari H, Pouretemad HR, Khatibi A. Bias toward drug-related stimuli is affected by loading working memory in abstinent ex-methamphetamine users. Front psychiatry. (2019) 10:776.
53. Verdejo-Garcia A, Garcia-Fernandez G, Dom G. Cognition and addiction. Dialogues Clin Neurosci. (2019) 21:281–90. doi: 10.31887/DCNS.2019.21.3/GDOM
54. Hargreaves A, Dillon R, Anderson-Schmidt H, Corvin A, Fitzmaurice B, Castorina M, et al. Computerised working-memory focused cognitive remediation therapy for psychosis–a preliminary study. Schizophr Res. (2015) 169:135–40. doi: 10.1016/J.SCHRES.2015.09.004
55. Rodríguez-Blanco L, Lubrini G, Vidal-Mariño C, Ríos-Lago M. Eficacia de la rehabilitación cognitiva de la atención, funciones ejecutivas y memoria operativa en los trastornos psicóticos. Revisión sistemática. Actas Esp Psiquiatr. (2017) 45:167–78.
56. Wanmaker S, Leijdesdorff SMJ, Geraerts E, van de Wetering BJM, Renkema PJ, Franken IHA. The efficacy of a working memory training in substance use patients: a randomized double-blind placebo-controlled clinical trial. J Clin Exp Neuropsychol. (2018) 40:473–86. doi: 10.1080/13803395.2017.1372367
57. Rupp CI, Kemmler G, Kurz M, Hinterhuber H, Wolfgang Fleischhacker W. Cognitive remediation therapy during treatment for alcohol dependence. J Stud Alcohol Drugs. (2012) 73:625–34. doi: 10.15288/JSAD.2012.73.625
Keywords: substance-related disorders, cognitive impairment, neuropsychological rehabilitation, psychoeducation, Trisquel
Citation: Piñón-Blanco A, Vergara-Moragues E, Gutiérrez-Martínez O, Fernández-Palleiro P, Rodrigues S, Rodrigues-Amorím D, Lage-López MT, González-López A, Velasquez T, Amorim M, Lloves-Moratinos M, Viéitez-Fernández I, Sabio-Fernandez G, Graña-Torralba R, Vilar-Díaz V, Carrera-Machado I, Cancelo-Martinez J, Ferreira A, Cardoso S, Rivera-Baltanás T, Otero-Lamas F, Olivares JM and Spuch C (2022) Efficacy of the Therapeutic Game “Trisquel” in the Treatment of Patients With Substance-Related Disorders Randomized Clinical Study. Front. Psychiatry 13:864511. doi: 10.3389/fpsyt.2022.864511
Received: 28 January 2022; Accepted: 06 April 2022;
Published: 02 May 2022.
Edited by:
Yasser Khazaal, University of Lausanne, SwitzerlandReviewed by:
Micael Silva Sousa, University of Coimbra, PortugalAngelica Beatriz Ortiz De Gortari, University of Bergen, Norway
Copyright © 2022 Piñón-Blanco, Vergara-Moragues, Gutiérrez-Martínez, Fernández-Palleiro, Rodrigues, Rodrigues-Amorím, Lage-López, González-López, Velasquez, Amorim, Lloves-Moratinos, Viéitez-Fernández, Sabio-Fernandez, Graña-Torralba, Vilar-Díaz, Carrera-Machado, Cancelo-Martinez, Ferreira, Cardoso, Rivera-Baltanás, Otero-Lamas, Olivares and Spuch. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Manuel Olivares, am9zZS5tYW51ZWwub2xpdmFyZXMuZGllekBzZXJnYXMuZXM=; Carlos Spuch, Y3NwdWNoQHV2aWdvLmVz