 Yanhua Chen1,2†
Yanhua Chen1,2† Peicheng Wang2†
Peicheng Wang2† Lina Zhao3
Lina Zhao3 Yanrong He1
Yanrong He1 Nuoya Chen4
Nuoya Chen4 Huanzhong Liu5,6
Huanzhong Liu5,6 Yuanli Liu7Tingfang Liu3
Yuanli Liu7Tingfang Liu3 Yi-lang Tang8,9
Yi-lang Tang8,9 Feng Jiang10,11*
Feng Jiang10,11* Jiming Zhu1,12*
Jiming Zhu1,12*- 1Vanke School of Public Health, Tsinghua University, Beijing, China
- 2School of Medicine, Tsinghua University, Beijing, China
- 3Institute for Hospital Management, Tsinghua University, Beijing, China
- 4Health Related Activity Recognition System Based on IoT Project, University of Macerata, Macerata, Italy
- 5Department of Psychiatry, Chaohu Hospital of Anhui Medical University, Hefei, China
- 6Anhui Psychiatric Center, Anhui Medical University, Hefei, China
- 7School of Health Policy and Management, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, China
- 8Mental Health Service Line, Atlanta VA Medical Center, Decatur, GA, United States
- 9Addiction Psychiatry Fellowship Program, Department of Psychiatry and Behavioral Sciences, Emory University, Atlanta, GA, United States
- 10School of International and Public Affairs, Shanghai Jiao Tong University, Shanghai, China
- 11Institute of Healthy Yangtze River Delta, Shanghai Jiao Tong University, Shanghai, China
- 12Institute for Healthy China, Tsinghua University, Beijing, China
Background: Workplace violence (WPV) in healthcare has received much attention worldwide. However, scarce data are available on its impact on turnover intention among psychiatrists, and the possible mechanisms between WPV and turnover intention have not been explored in China.
Methods: A cross-sectional survey was conducted among psychiatrists in 41 tertiary psychiatric hospitals from 29 provinces and autonomous regions in China. A stress-strain-outcome (SSO) model was adopted to examine the effects of WPV on mental health and turnover intention. The association and mediation by burnout and stress were examined by multivariate logistic regression (MLR) and generalized structure equation modeling (GSEM).
Results: We invited 6,986 psychiatrists to participate, and 4,520 completed the survey (64.7% response rate). The prevalence of verbal and physical violence against psychiatrist in China was 78.0 and 30.7%, respectively. MLR analysis showed that psychiatrists who experienced verbal violence (OR = 1.15, 95% CI = 1.10–1.21) and physical violence (OR = 1.15, 95% CI = 1.07–1.24) were more likely to report turnover intention. GSEM analysis showed that burnout (β = 4.00, p < 0.001) and stress (β = 1.15, p < 0.001) mediated the association between verbal violence and turnover intention; similarly, burnout (β = 4.92, p < 0.001) and stress (β = 1.80, p < 0.001) also mediated the association between physical violence and turnover intention.
Conclusions: Experience of WPV is a significant contributor to turnover intention among psychiatrists. Mental health status, such as burnout and stress level significantly mediated the association. Policy makers and hospital administrators need to be aware of this association. Action is needed to promote mental health among the psychiatrists to improve morale and workforce sustainability.
Introduction
Although some progress has been made in recent years, including the improved quality of training programs (1), the psychiatric workforce is still in severe shortage (2) and unevenly distributed in China. Maintaining workforce sustainability and reducing attrition are vital ways to slow down the shortage of mental health workforce (3). To reduce turnover rate for psychiatrists, it is important to identify the upstream drivers of turnover intention of psychiatrists, and then to inform strategies in recruitment and retention.
In recent decades, workplace violence (WPV) against healthcare workers has drawn attention and become a serious public health issue globally (4, 5). Workplace violence can be defined as “incidents where staff are abused, threatened or assaulted in circumstances related to their work, involving an explicit or implicit challenge to their safety, wellbeing or health” (6). According to the World Health Organization (WHO), health workers are subject to high risk of violence, with 8%-38% of health workers suffering from physical violence at some point in their careers, and even more are threatened by or exposed to verbal aggression (7). It has been found that healthcare workers in the psychiatric settings are approximately three times higher of encountering violence (8, 9) when compared to other medical specialties. Patients' violent behavior, especially physical aggression and verbal violence in psychiatric settings, was of great concern for researchers (10–12) and has become increasingly common in China (13, 14).
WPV can physically and psychologically harm healthcare workers and affect the workforce stability (15). A growing body of research literature suggests that WPV is a key risk factor associated with turnover intention. For instance, a study from an emergency department in Korea showed that WPV increased nurses' intention to leave the hospital (16). A study among physicians in China found that WPV was significantly associated with turnover intention (17). Another survey with physicians in Finland also showed that WPV led to increased turnover intention (18).
The stressor–strain–outcome (SSO) model specified a process between stressors and the outcome with a mediating role played by strain (19, 20). In the SSO model, stressors are environmental stimulus that individuals experience, strains are individuals' personal emotions, and outcomes are behavioral responses to stressors (21). According to the SSO model, strain plays an essential role in the associations between workplace violence and turnover intention. Other related research reaches the consensus that stress and exhaustion are viewed as transactional processes between individual environment stimulus and response behaviors (22, 23). A meta-analytic review proposed that, the negative effects of WPV on affects and attitudes would have indirect consequences on behavioral outcomes (24). Many researchers further examined mental health as a mediator in the association of WPV with turnover intention. Recently, burnout and stress were considered as key mediators and have been examined (25–27). Nonetheless, few of the existing studies systematically explored the relationship between WPV and turnover intention among psychiatrists, and none have examined the mechanism embedded in the stressor-to-outcome process.
With a widely recognized shortage of mental health care workers (28), preventing brain drain has become one of workable solutions to psychiatrists shortage both in short-and long-term. Understanding the impacts of WPV on turnover intention is crucial for preventing more psychiatrists from quitting their job. This is of even more significance in China as a high rate of WPV in healthcare setting has been reported (14). Our study, based on the SSO model, would reveal the transactional process among WPV, mental health and turnover intention in order to provide insight for prevention interventions (22). Based on the SSO model, our research examined the transactional process from WPV to turnover intention by focusing on the following: (1) identifying upstream drivers of turnover intention among psychiatrists; (2) examining the association between verbal and physical violence and turnover intention among psychiatrists; (3) exploring the mediating roles of burnout and stress in the process. The study aimed to understand the mechanism behind turnover intention and shed light on policymaking, in order to maintain human resource sustainability in psychiatric settings.
Methods
Participants and Procedures
Data were retrieved from 2019 National Hospital Performance Evaluation Survey, which approached 41 tertiary psychiatric hospitals in 29 provinces across China. Only two provinces, namely Gansu and Tibet, were not covered by the survey as there were no tertiary psychiatric hospitals there. All the psychiatrists (n = 6,986) from the 41 hospitals were invited to participate in this survey and 4,520 (64.7%) completed the questionnaire. The survey was conducted anonymously and voluntarily through WeChat, an online social media application widely used in China. An electronic informed consent form was obtained from each participant before they began answering questions. Each WeChat account was allowed to submit the questionnaire once only. Socio-demographic data, self-reported experience of workplace violence, turnover intention and mental health status were collected. The research protocol was approved by the Ethics Committee of Chaohu Hospital of Anhui Medical University (No. 201903-kyxm-02).
Measures
Burnout
Burnout was measured with the Chinese version of the Maslach Burnout Inventory-Human Service Survey (MBI-HSS). The MBI-HSS has been used in many studies including in Chinese samples (29). It has 22 items and measures burnout from three dimensions: emotional exhaustion (EE, 9 items), depersonalization (DP, 5 items) and reduced personal accomplishment (PA, 8 items). A seven-point scale ranging from 0 (“never experienced such a feeling”) to 6 (“experience such feelings every day”) was used to measure how much respondents agree or disagree with a particular statement. In this study, higher scores (ranging from 0 to 84) in emotional exhaustion and depersonalization subscales indicate higher degree of burnout (30, 31), and the Cronbach alpha coefficient for reliability testing was 0.926.
Stress
Stress was measured by the Depression Anxiety Stress Scale (DASS, 21 items). DASS-21 was a quantitative measure that examines three domains: depression, anxiety, and stress. Seven items scored from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time) were calculated within each domain. The scale has been used as a screening tool for different populations with various culture background (32) as well as for Chinese samples (33). Based on the scale, the stress score in this study ranged from 0 to 21. The DASS-21 serves as a short version of the DASS (42 items). The final score of each scale was multiplied by two (ranging from 0 to 42), making the scores comparable with the normal DASS scores (34, 35). The Cronbach alpha reliability coefficients (α = 0.956; depression α =0.912; anxiety α = 0.877; and stress α =0.889) for DASS subscales indicates the reliability of our sample for further statistical analysis.
Workplace Violence
Participants were asked to answer two questions concerning the verbal and physical violence they experienced in the workplace. The first question is “How many times, in the past 12 months, did you find yourself in a situation of verbal aggression (e.g., expressions of abuse, slandering, contempt, insulting or humiliating without physical contact) by patients?” The second question is “How many times, in the past 12 months, did you find yourself in a situation of physical aggression by patients (e.g., pushing, hitting, inflicting physical harm on persons or violence with weapons)?” Answer score: 1 = never/almost never, 2 = <12 times/year, 3 = once a month, 4 = 2–3 times/month, 5 = once a week, 6 = 2–5 times/week, 7 = almost every day. Higher scores indicates a higher level of experienced violence (3, 36).
Turnover Intention
Psychiatrists' turnover intention was evaluated by a single-item question asking “Have you ever thought of quitting your job in the past month?” and the response included “yes” and “no.”
Demographic Factors
In this study we included socio-demographic and occupational characteristics data such as, age, gender (male or female), education level (associate degree or lower, college degree, or master's degree or higher), working years (<5, 5–9,10–19 or ≥20 years old), monthly net income (<5,001, 5,001–8,000, 8,001–12,000, or more than 12,000, in CNY), working hours per week (<41, 41–48, 49–54, ≥55), and self-rated health status (unsatisfied, somewhat satisfied, or satisfied).
Data Analysis
The multivariable logistic regression (MLR) model was used to examine the role played by demographic factors, stress, burnout and WPV in causing widespread turnover intention. To assess the mediating roles played by burnout and stress on the relationship between WPV and turnover intention, generalized structural equation models (GSEM) were constructed for verbal and physical violence by specifying a binomial distribution of outcome variabls, and then a logit link was used to estimate the odds ratios (ORs) and corresponding 95% confidence intervals (CI). Harman's single factor test was performed to address common method bias issue. Mediation analysis was supplementarily used to test indirect effects in our model. Root mean squared error of approximation (RMSEA) and standardized root mean squared residual (SRMR) were assessed for the GSEM model's fit. Given that the DASS-21 is a widely used comprehensive assessment scale for mental health disorders, DASS-Depression and DASS-Anxiety were used for robustness check to verify our findings. All analyses were done with STATA (version 16) and Mplus 7.0. Two-tailed tests with P-value < 0.05 were considered statistically significant.
Results
Participants' Characteristics
The sociodemographic characteristics and the basic profiles of 4,520 psychiatrists are shown in Table 1. The mean age of the participants was 38.5 (SD = 8.6); 41.9% were male, and 97.3% had a college degree (including a medical degree) or above. The median income was 7,000 RMBs (~ $1,082), with only 36.7% of them earned more than 8,000 RMBs (~$1,236). The mean working hours per week was 53.0 h (SD = 16.2), and 37.0% of the participants worked more than 55 h per week. Overall, the rate of turnover intention was 31.9% in this sample.
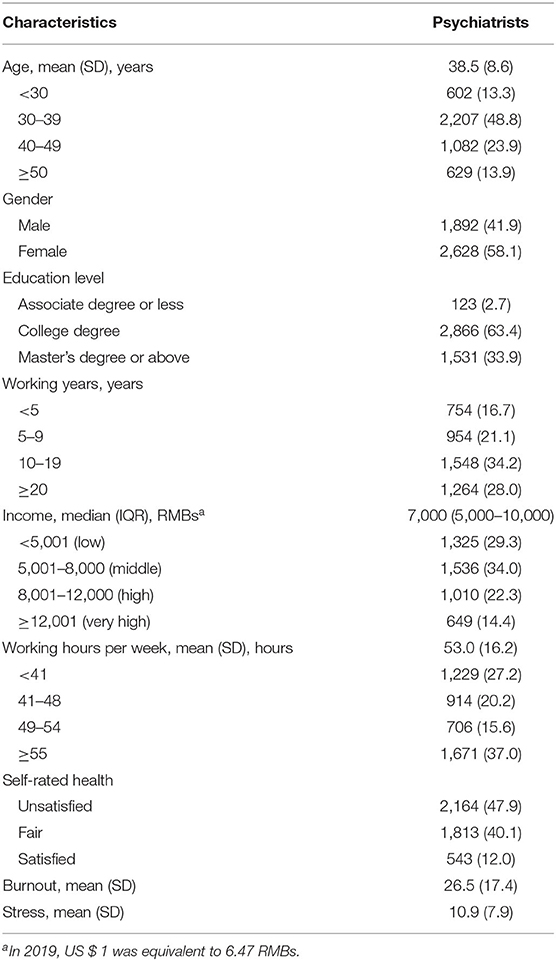
Table 1. Characteristics of the participants (n = 4,520).
Prevalence of Workplace Violence
As Table 2 shows, when compared with physical violence (30.7%), a greater proportion of psychiatrists in China experienced verbal violence (78.0%). Specifically, verbal violence was more common in males (80.1%), among people in their 40s (81.3%), with a master's degree or above (80.5%), in the highest income category (82.4%), or among those who worked 49–54 h per week (84.3%). Physical violence was most common in males (35.5%), among those in their 30s (32.4%), with a college degree (32.2%), in the middle-income category (33.3%), or among those who worked 49–54 h per week (36.1%).
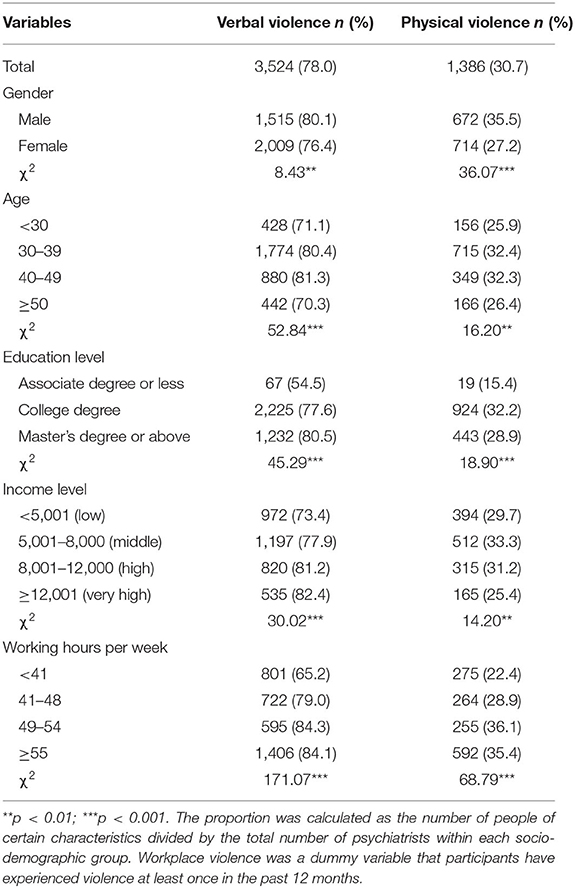
Table 2. The prevalence of exposure to workplace violence among psychiatrists.
Factors Associated With Turnover Intention
Table 3 presents the results of the MLR model. Male, working for 10-19 years, working more than 48 h per week were factors that are more likely to be related with turnover intention. Participants with higher monthly income and more satisfied self-reported health status were less likely to have turnover intention. Model 2–5 suggested the association between verbal violence, physical violence, burnout, and stress with turnover intention after controlling for all the covariates. Exposure to verbal violence (OR = 1.15, 95% CI = 1.10–1.21) and physical violence (OR = 1.15, 95% CI = 1.07–1.24) were significantly associated with turnover intention. In addition, burnout (OR = 1.05, 95% CI = 1.04–1.05) and stress (OR = 1.07, 95% CI = 1.076–1.08) would significantly increase the odds of psychiatrists' turnover intention. As the direct effect of WPV was insignificant, we further conducted the moderation analysis (see Supplementary Table 1). The results showed that WPV had no significant moderating effect on the association between mental health and turnover intention. We also examined the association between two subscales of DASS (depression and anxiety) and turnover intention as robustness test (see Supplementary Table 2).
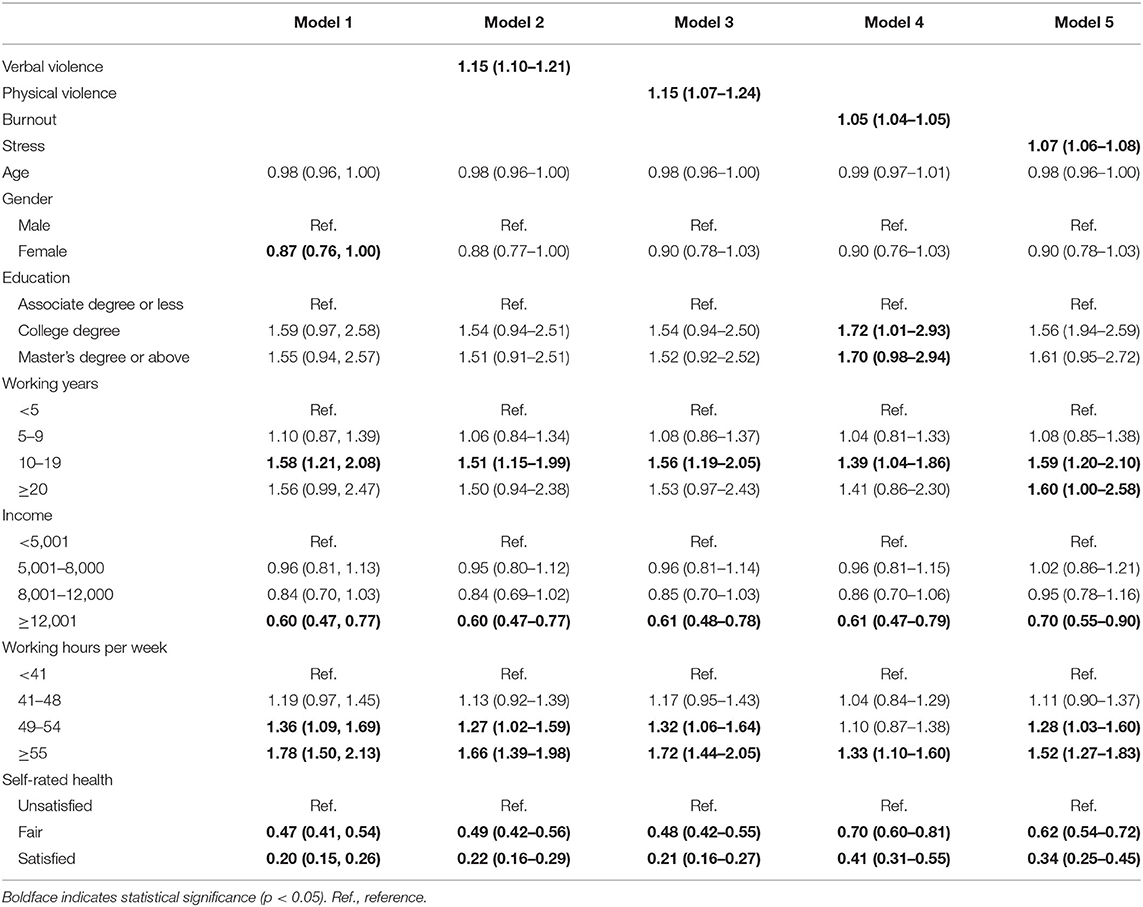
Table 3. Logistics regression analyses for factors associated with turnover intention.
Mediating Effects of Burnout and Stress
In Figure 1A, the GSEM results demonstrated that verbal violence predicted burnout (β = 4.00, P < 0.001) and stress (β = 1.15, P < 0.001) directly and positively, but verbal violence had no significantly direct effects on turnover intention (OR = 1.02, 95% CI = 0.97, 1.07). Figure 1B showed that physical violence also had a direct and significant predictive effect on burnout (β = 4.92, P < 0.001) and stress (β = 1.80, P < 0.001); meanwhile, physical violence had no significantly indirect effects on turnover intention (OR = 1.00, 95% CI = 0.92, 1.08). In both models, burnout (OR = 1.04, 95% CI = 1.04, 1.05) and stress (OR = 1.02, 95% CI = 1.01, 1.04) were significant predictors of turnover intention. The results of robustness check for depression and anxiety were showed in Supplementary Figures 1, 2.
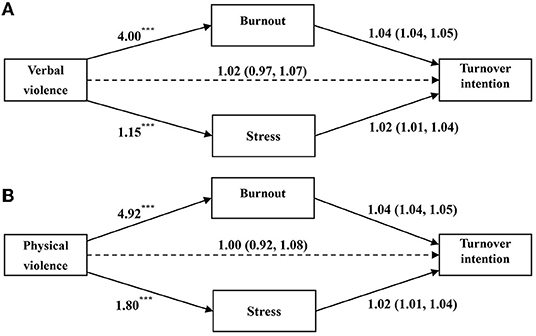
Figure 1. Mediation effects of mental health between WPV and turnover intention. (A) illustrates the path coefficients of the relationship between verbal violence and turnover intention; (B) of the relationship between physical violence and turnover intention. Regression coefficients are shown for the path from WPV to burnout and stress, *p < 0.05; **p < 0.01; ***p < 0.001. ORs and corresponding 95% CI (in parentheses) are shown for the path between mental health and turnover intention, which is measured as a binary variable. Both models adjusted for age, gender, education, working years, income, working hours per week, self-rated health.
The mediation analysis was used to test the significance of mediating effects of burnout and stress. The 95% confidence intervals for burnout and stress did not contain 0, indicating that the mediating effects were significant. The results in Table 4 suggest that the mediating effects of verbal violence (OR = 0.20, 95% CI = 0.17–0.22) and physical violence (OR = 0.25, 95% CI = 0.22–0.29) over turnover intention were statistically significant. The mediating effect of “Verbal violence → Burnout → Turnover intention” was 0.17 (95% CI = 0.14–0. 19); and the effect of “Physical violence → Stress → Turnover intention” was 0.03 (95% CI = 0.01–0.04). The mediating effect of “Physical violence → Burnout → Turnover intention” was 0.21 (95% CI = 0.17–0.24); and the effect of “Physical violence → Stress → Turnover intention” was 0.06 (95% CI = 0.02–0.06). Indirect effects of depression and anxiety were tested (see Supplementary Table 3). In addition, under the linear assumption, RMSEA and SRMR were assessed with a large sample size used in this study (37–39). The test model fit both conducted in GSEM model A (RMSEA = 0.066 and SRMR = 0.082) and GSEM model B (RMSEA = 0.064 and SRMR = 0.081), indicating an adequate model fit for our GSEM models.
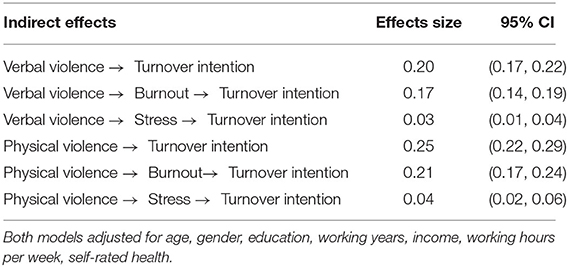
Table 4. Mediation analysis of indirect effects of burnout and stress.
Discussion
With a large national sample of psychiatrists from 41 tertiary psychiatric hospitals in China, we found that psychiatrists experienced higher rates of verbal violence (78.0%) and physical violence (30.7%) when compared to the overall rates of verbal violence (48.52%) and physical violence (5.84%) in 144 Chinese public hospitals (40). Some possible reasons may explain the high rates. In psychiatric settings, patients with unstable mental status may be stressed and are more likely to express anger toward those who care for them. In addition, due to the increasing demand of mental health services in China, psychiatrists are facing an inflow of patients suffering from mental illness, which would increase their workload. Hospitalizations in psychiatric settings maybe for days, weeks, or longer, and this ongoing care relationship may also increase the incidence of WPV (41–43). The prevalence of WPV vary across socio-economic groups. This finding is consistent with our other study (44), where we found that WPV undermines workforce stability and got inspired to further explore the mechanisms between WPV and turnover intention. In this study, we examined the associations between workplace violence and turnover intention, and the mediating effects of mental health on the associations, contributing to the existing literature on WPV, mental health and turnover intention among physicians. Our findings suggest the existence of a psychologically transactional process (as strains) between WPV (as individual environment stimulus factors) and turnover intention (as response behaviors) among psychiatrists.
We found a high rate (31.9%) of psychiatrists reporting they would leave their job. The percentage was also much higher than the turnover intention of nurses (20.0%) and pharmacists (17.8%) in psychiatric settings (1, 45). Consistent with previous studies (46–48) in several countries, psychiatrists with higher salary and satisfaction with their health conditions are more likely to stay in their current job; male doctors with longer work history and working hours are more likely to have turnover intention. These findings may help policymakers and hospital administrator to take more targeted measures (e.g., health promotion, lower hours of work or higher level of salary) to retain employees and boost their wellbeing. In addition, consistent with previous studies, healthcare workers who reported burnout and stress were more likely to have turnover intentions (49–51). This finding suggests that reducing burnout and stress among psychiatrists may be effective in preventing their turnover intention.
We found that psychiatrists with greater exposure to WPV were more likely to have turnover intention. This is consistent with previous studies in which workplace violence was found to be associated with higher turnover intention among physicians (52, 53). As the experience of verbal violence and physical violence were positively associated with leave intention, it was not surprising that such “negative experience” could contribute to the increasing turnover intention. Concordant with previous studies where physical and verbal violence are found to have significant impact on burnout among Chinese physicians (40), our findings suggest that WPV, including both verbal violence and physical violence, is associated with burnout and stress. A study in Israel also suggests that verbal and physical violence were significantly associated with stress among mental health nurses (10).
Moreover, the mediation analysis in this study showed that the relationship between WPV and turnover intention was mediated by mental health. This result supports the mediating effect of mental health (including occupational stress and burnout) reported in association between patient violence and turnover intention among nurses (25). Our findings were also partly in line with the observation during COVID-19 in China that the effect of workplace violence on turnover intention was partially mediated by mental health (i.e., stress) (27). Although exposure to WPV might lead to mental health problems, our analysis indicates that mental health is a meaningful knob to reduce the negative impact of WPV on turnover intention in this population.
Strategies are needed to reduce and prevent the incidence of WPV (54, 55). Adequate training, education and support should be provided for healthcare workers (56). Improving communication skills of healthcare workers would also be helpful in reducing patient-physician misunderstandings (57). Legislation against WPV in healthcare facilities can be established in order to protect vulnerable healthcare workers (9). Governments could declare a crackdown on assault on doctors and on violence in hospitals (14). Our findings additionally suggest that hospital administrators should take measures to promote the mental health and wellbeing of psychiatrists after the exposure to WPV. This indicates that, besides providing sufficient support, helping psychiatrists deal with mental health in the face of WPV might be equally important to reduce their turnover intention (58). Just as researchers advocated, hospital management should consider the effects of workplace violence on workers' mental health and their subsequent intention to leave (59). The de-escalation of incidents would be an effective way to decrease the likelihood of a violent outcome (60). For example, the hospital management policy should conduct stress reduction intervention program to mitigate mental health burden (10). Hospitals can also provide specialized and confidential trauma-informed mental health services (61) and provide timely psychological interventions (such as establishing professional pressure relief workshops), and arrange psychologists for physicians who have experienced workplace violence (58).
The study has a few limitations. First, the data was collected in a self-reported manner, which might have cognitive bias. Second, the data sets were cross-sectional with no causal relationship can be inferred. Third, psychological violence and sexual harassment and other implicit violence were not included in our survey. While we discussed the mediation effects of burnout and stress, more potential mediators (e.g., job performance, professional identity, and job security) between WPV and turnover intention could be further explored. Fourth, as STATA does not provide GSEM model fit information, we assessed RMSEA and SRMR with a large sample size under the linear assumption instead. Finally, the study focused primarily on violence from patients and their families and did not evaluate violence from staff members, which could have similar, if not more, effects on individuals who were exposed to it.
Conclusion
It is alarming that nearly one third of psychiatrists in China have reported an intention to leave their current position. We have also found that WPV, including verbal and physical violence, are significant predictors of turnover intention, while mental health has significant mediating effects on turnover intention. Our findings suggest, while measures to decrease WPV are important, policy makers and hospital administrators need to be aware of the mediating role of mental health on psychiatrists. It may be helpful and cost-effective to promote mental health among the psychiatrists to improve their morale and workforce sustainability.
Data Availability Statement
Data are available from the corresponding authors upon reasonable request.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of Chaohu Hospital of Anhui Medical University (No. 201903-kyxm-02). The Ethics Committee waived the requirement of written informed consent for participation.
Author Contributions
FJ, HL, TL, and YL collected the data set. The original idea for the research was developed by YC, PW, and JZ. PW, YC, and LZ conducted the statistical analyses. YC, PW, LZ, and JZ drafted the paper. YH, NC, YT, and JZ were involved with manuscript preparation and revisions. All authors approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.855584/full#supplementary-material
References
1. Jiang F, Zhou H, Rakofsky J, Hu L, Liu T, Wu S, et al. Intention to leave and associated factors among psychiatric nurses in China: a nationwide cross-sectional study. Int J Nurs Stud. (2019) 94:159–65. doi: 10.1016/j.ijnurstu.2019.03.013
2. Huang Y, Wang Y, Wang H, Liu Z, Yu X, Yan J, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. (2019) 6:211–24. doi: 10.1016/S2215-0366(18)30511-X
3. Aguglia A, Belvederi Murri M, Conigliaro C, Cipriani N, Vaggi M, Di Salvo G, et al. Workplace violence and burnout among mental health workers. Psychiatr Serv. (2020) 71:284–8. doi: 10.1176/appi.ps.201900161
4. ILO I, WHO P. Joint Programme on Workplace Violence in the Health Sector. Workplace Violence in the Health Sector Country Case Study–Questionnaire. Geneva (2003), 14.
5. Kobayashi Y, Oe M, Ishida T, Matsuoka M, Chiba H, Uchimura N. Workplace violence and its effects on burnout and secondary traumatic stress among mental healthcare nurses in Japan. Int J Environ Res Public Health. (2020) 17:2747. doi: 10.3390/ijerph17082747
6. WHO. Framework Guidelines for Addressing Workplace Violence in the Health Sector. World Health Organization (2002). Available online at: https://www.who.int/violence_injury_prevention/violence/interpersonal/en/WVguidelinesEN.pdf (accessed April 01, 2022).
7. WHO. Preventing Violence Against Health Workers. WHO (2021). Available online at: https://apps.who.int/iris/bitstream/handle/10665/42617/9221134466.pdf?sequence=1&isAllowed=y (accessed December 12, 2021).
8. Knoll Iv JL. Violence risk assessment for mental health professionals. In: Wiley Encyclopedia of Forensic Science. Chichester: John Wiley & Sons, Ltd (2009). doi: 10.1002/9780470061589.fsa639
9. Phillips JP. Workplace violence against health care workers in the United States. N Engl J Med. (2016) 374:1661–9. doi: 10.1056/NEJMra1501998
10. Itzhaki M, Bluvstein I, Peles Bortz A, Kostistky H, Bar Noy D, Filshtinsky V, et al. Mental health nurse's exposure to workplace violence leads to job stress, which leads to reduced professional quality of life. Front Psychiatry. (2018) 9:59. doi: 10.3389/fpsyt.2018.00059
11. Rolin SA, Lawrence RE, Dixon LB, Appelbaum PS. Violence in psychiatric settings: demographic and clinical characteristics of patients who were targets of aggression. J Nerv Ment Dis. (2021) 209:307–10. doi: 10.1097/NMD.0000000000001311
12. Xie X-M, Zhao Y-J, An F-R, Zhang Q-E, Yu H-Y, Yuan Z, et al. Workplace violence and its association with quality of life among mental health professionals in China during the COVID-19 pandemic. J Psychiatr Res. (2021) 135:289–93. doi: 10.1016/j.jpsychires.2021.01.023
13. Hesketh T, Wu D, Mao L, Ma N. Violence against doctors in China. Bmj. (2012) 345:e5730. doi: 10.1136/bmj.e5730
14. Lu L, Dong M, Wang S-B, Zhang L, Ng CH, Ungvari GS, et al. Prevalence of workplace violence against health-care professionals in China: a comprehensive meta-analysis of observational surveys. Trauma Violence Abuse. (2020) 21:498–509. doi: 10.1177/1524838018774429
15. Wang N, Wu D, Sun C, Li L, Zhou X. Workplace violence in County hospitals in eastern China: risk factors and hospital attitudes. J Interpers Violence. (2021) 36:4916–26. doi: 10.1177/0886260518792242
16. Jeong IY, Kim JS. The relationship between intention to leave the hospital and coping methods of emergency nurses after workplace violence. J Clin Nurs. (2018) 27:1692–701. doi: 10.1111/jocn.14228
17. Duan X, Ni X, Shi L, Zhang L, Ye Y, Mu H, et al. The impact of workplace violence on job satisfaction, job burnout, and turnover intention: the mediating role of social support. Health Qual Life Outcomes. (2019) 17:1–10. doi: 10.1186/s12955-019-1164-3
18. Heponiemi T, Kouvonen A, Virtanen M, Vänskä J, Elovainio M. The prospective effects of workplace violence on physicians' job satisfaction and turnover intentions: the buffering effect of job control. BMC Health Serv Res. (2014) 14:19. doi: 10.1186/1472-6963-14-19
19. Koeske GF, Koeske RD. A preliminary test of a stress-strain-outcome model for reconceptualizing the burnout phenomenon. J Soc Serv Res. (1993) 17:107–35. doi: 10.1300/J079v17n03_06
20. Um M-Y, Harrison DF. Role stressors, burnout, mediators, and job satisfaction: a stress-strain-outcome model and an empirical test. Soc Work Res. (1998) 22:100–15. doi: 10.1093/swr/22.2.100
21. Shahzad F, Du J, Khan I, Fateh A, Shahbaz M, Abbas A, et al. Perceived Threat of COVID-19 Contagion and Frontline Paramedics' Agonistic Behaviour: Employing a Stressor–Strain–Outcome Perspective. Int J Environ Res Public Health. (2020) 17:5102. doi: 10.3390/ijerph17145102
22. Lazarus RS. Theory-based stress measurement. Psychol Inq. (1990) 1:3–13. doi: 10.1207/s15327965pli0101_1
23. Cao X, Masood A, Luqman A, Ali A. Excessive use of mobile social networking sites and poor academic performance: antecedents and consequences from stressor-strain-outcome perspective. Comput Hum Behav. (2018) 85:163–74. doi: 10.1016/j.chb.2018.03.023
24. Nielsen MB, Einarsen S. Outcomes of exposure to workplace bullying: a meta-analytic review. Work Stress. (2012) 26:309–32. doi: 10.1080/02678373.2012.734709
25. Laeeque SH, Bilal A, Babar S, Khan Z, Ul Rahman S. How patient-perpetrated workplace violence leads to turnover intention among nurses: the mediating mechanism of occupational stress and burnout. J Aggress Maltreat Trauma. (2018) 27:96–118. doi: 10.1080/10926771.2017.1410751
26. Liu W, Zhao S, Shi L, Zhang Z, Liu X, Li L, et al. Workplace violence, job satisfaction, burnout, perceived organisational support and their effects on turnover intention among Chinese nurses in tertiary hospitals: a cross-sectional study. BMJ Open. (2018) 8:e019525. doi: 10.1136/bmjopen-2017-019525
27. Yang Y, Wang P, Kelifa MO, Wang B, Liu M, Lu L, et al. (2021). How workplace violence correlates turnover intention among Chinese health care workers in COVID-19 context: the mediating role of perceived social support and mental health. J Nurs Manag. doi: 10.1111/jonm.13325
28. Bruckner TA, Scheffler RM, Shen G, Yoon J, Chisholm D, Morris J, et al. The mental health workforce gap in low-and middle-income countries: a needs-based approach. Bull World Health Organ. (2011) 89:184–94. doi: 10.2471/BLT.10.082784
29. Lee H-F, Yen M, Fetzer S, Chien TW. Predictors of burnout among nurses in Taiwan. Community Ment Health J. (2015) 51:733–7. doi: 10.1007/s10597-014-9818-4
30. Durham ME, Bush PW, Ball AM. Evidence of burnout in health-system pharmacists. Am J Health Syst Pharm. (2018) 75:S93–100. doi: 10.2146/ajhp170818
31. Mészáros V, Ádám S, Szabó M, Szigeti R, Urbán R. The bifactor model of the maslach burnout inventory–human services survey (MBI-HSS)—an alternative measurement model of burnout. Stress Health. (2014) 30:82–8. doi: 10.1002/smi.2481
32. Tran TD, Tran T, Fisher J. Validation of the depression anxiety stress scales (DASS) 21 as a screening instrument for depression and anxiety in a rural community-based cohort of northern Vietnamese women. BMC Psychiatry. (2013) 13:24. doi: 10.1186/1471-244X-13-24
33. Yue A, Gao J, Yang M, Swinnen L, Medina A, Rozelle S. Caregiver depression and early child development: a mixed-methods study from rural China. Front Psychol. (2018) 9:2500. doi: 10.3389/fpsyg.2018.02500
34. Park SH, Song YJC, Demetriou EA, Pepper KL, Thomas EE, Hickie IB, et al. Validation of the 21-item depression, anxiety, and stress scales (DASS-21) in individuals with autism spectrum disorder. Psychiatry Res. (2020) 291:113300. doi: 10.1016/j.psychres.2020.113300
35. Olds T, Burton NW, Sprod J, Maher C, Ferrar K, Brown WJ, et al. One day you'll wake up and won't have to go to work: the impact of changes in time use on mental health following retirement. PLoS ONE. (2018) 13:e0199605. doi: 10.1371/journal.pone.0199605
36. Jankovic M, Sijtsema J, Reitz A, Masthoff E, Bogaerts S. Workplace violence, post-traumatic stress disorder symptoms, and personality. Pers Individ Dif. (2021) 168:110410. doi: 10.1016/j.paid.2020.110410
37. Wang Z, Buu A, Lohrmann DK, Shih PC, Lin H-C. The role of family conflict in mediating impulsivity to early substance exposure among preteens. Addict Behav. (2021) 115:106779. doi: 10.1016/j.addbeh.2020.106779
38. Dadi AF, Mwanri L, Woodman RJ, Azale T, Miller ER. Causal mechanisms of postnatal depression among women in Gondar town, Ethiopia: application of a stress-process model with generalized structural equation modeling. Reprod Health. (2020) 17:1–15. doi: 10.1186/s12978-020-00912-z
39. Clouston SA, Manganello JA, Richards M. A life course approach to health literacy: the role of gender, educational attainment and lifetime cognitive capability. Age Ageing. (2017) 46:493–9. doi: 10.1093/ageing/afw229
40. Wu Y, Jiang F, Ma J, Tang Y-L, Wang M, Liu Y. Experience of medical disputes, medical disturbances, verbal and physical violence, and burnout among physicians in China. Front Psychol. (2021) 11:556517. doi: 10.3389/fpsyg.2020.556517
41. Hilton NZ, Addison S, Ham EC, Rodrigues N, Seto MC. Workplace violence and risk factors for PTSD among psychiatric nurses: systematic review and directions for future research and practice. J Psychiatr Ment Health Nurs. (2022) 29:186–203. doi: 10.1111/jpm.12781
42. Basfr W, Hamdan A, Al-Habib S. Workplace violence against nurses in psychiatric hospital settings: perspectives from Saudi Arabia. Sultan Qaboos Univ Med J. (2019) 19:e19. doi: 10.18295/squmj.2019.19.01.005
43. Lu L, Lok K-I, Zhang L, Hu A, Ungvari GS, Bressington DT, et al. Prevalence of verbal and physical workplace violence against nurses in psychiatric hospitals in China. Arch Psychiatr Nurs. (2019) 33:68–72. doi: 10.1016/j.apnu.2019.07.002
44. Han X, Jiang F, Shen L, Liu Y, Liu T, Liu H, et al. Workplace violence, workforce stability, and well-being in China's psychiatric hospitals. Am J Prev Med. (2021) 62:e265–73. doi: 10.1016/j.amepre.2021.09.013
45. Fan S, Liu T, Jiang F, Liu Y. Analysis of the intention to leave pharmacists and related factors in 41 psychiatrichospitals in China. Chinese Hospitals. (2021) 25:26–9. doi: 10.19660/j.issn.1671-0592.2021.2.09
46. Abd-Ellatif EE, Anwar MM, Aljifri AA, El Dalatony MM. Fear of COVID-19 and its impact on job satisfaction and turnover intention among Egyptian physicians. Saf Health Work. (2021) 12:490–5. doi: 10.1016/j.shaw.2021.07.007
47. Oh S, Kim H. Turnover intention and its related factors of employed doctors in Korea. Int J Environ Res Public Health. (2019) 16:2509. doi: 10.3390/ijerph16142509
48. Zaheer S, Ginsburg L, Wong HJ, Thomson K, Bain L, Wulffhart Z. Turnover intention of hospital staff in Ontario, Canada: exploring the role of frontline supervisors, teamwork, and mindful organizing. Hum Resour Health. (2019) 17:1–9. doi: 10.1186/s12960-019-0404-2
49. Leiter MP, Maslach C. Nurse turnover: the mediating role of burnout. J Nurs Manag. (2009) 17:331–9. doi: 10.1111/j.1365-2834.2009.01004.x
50. Kelly LA, Gee PM, Butler RJ. Impact of nurse burnout on organizational and position turnover. Nurs Outlook. (2021) 69:96–102. doi: 10.1016/j.outlook.2020.06.008
51. Liu J, Zhu B, Wu J, Mao Y. Job satisfaction, work stress, and turnover intentions among rural health workers: a cross-sectional study in 11 western provinces of China. BMC Fam Pract. (2019) 20:9. doi: 10.1186/s12875-019-0904-0
52. Eneroth M, Gustafsson Sendén M, Schenck Gustafsson K, Wall M, Fridner A. Threats or violence from patients was associated with turnover intention among foreign-born GPs–a comparison of four workplace factors associated with attitudes of wanting to quit one's job as a GP. Scand J Prim Health Care. (2017) 35:208–13. doi: 10.1080/02813432.2017.1333319
53. Gan Y, Gong Y, Chen Y, Cao S, Li L, Zhou Y, et al. Turnover intention and related factors among general practitioners in Hubei, China: a cross-sectional study. BMC Fam Pract. (2018) 19:74. doi: 10.1186/s12875-018-0752-3
54. Morphet J, Griffiths D, Beattie J, Reyes DV, Innes K. Prevention and management of occupational violence and aggression in healthcare: a scoping review. Collegian. (2018) 25:621–32. doi: 10.1016/j.colegn.2018.04.003
55. Nøland ST, Taipale H, Mahmood JI, Tyssen R. Analysis of career stage, gender, and personality and workplace violence in a 20-year nationwide cohort of physicians in Norway. JAMA Netw Open. (2021) 4:e2114749. doi: 10.1001/jamanetworkopen.2021.14749
56. Jackson D, Clare J, Mannix J. Who would want to be a nurse? Violence in the workplace–a factor in recruitment and retention. J Nurs Manag. (2002) 10:13–20. doi: 10.1046/j.0966-0429.2001.00262.x
57. Magnavita N. Violence prevention in a small-scale psychiatric unit: program planning and evaluation. Int J Occup Environ Health. (2011) 17:336–44. doi: 10.1179/oeh.2011.17.4.336
58. Shi L, Li G, Hao J, Wang W, Chen W, Liu S, et al. Psychological depletion in physicians and nurses exposed to workplace violence: a cross-sectional study using propensity score analysis. Int J Nurs Stud. (2020) 103:103493. doi: 10.1016/j.ijnurstu.2019.103493
59. Pariona-Cabrera P, Cavanagh J, Bartram T. Workplace violence against nurses in health care and the role of human resource management: a systematic review of the literature. J Adv Nurs. (2020) 76:1581–93. doi: 10.1111/jan.14352
60. Hader R. Workplace violence survey 2008: unsettling findings. Nurs Manage. (2008) 39:13–9. doi: 10.1097/01.NUMA.0000326561.54414.58
Keywords: workplace violence, turnover intention, mental health, psychiatrists, China
Citation: Chen Y, Wang P, Zhao L, He Y, Chen N, Liu H, Liu Y, Liu T, Tang Y-l, Jiang F and Zhu J (2022) Workplace Violence and Turnover Intention Among Psychiatrists in a National Sample in China: The Mediating Effects of Mental Health. Front. Psychiatry 13:855584. doi: 10.3389/fpsyt.2022.855584
Received: 15 January 2022; Accepted: 13 May 2022;
Published: 15 June 2022.
Edited by:
Yanhui Liao, Zhejiang University School of Medicine, ChinaReviewed by:
Jianfei Xie, Central South University, ChinaCatalina Sau Man Ng, The Education University of Hong Kong, Hong Kong SAR, China
Xuebing Su, Hong Kong Polytechnic University, Hong Kong SAR, China
Copyright © 2022 Chen, Wang, Zhao, He, Chen, Liu, Liu, Liu, Tang, Jiang and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiming Zhu, amltaW5nemh1QHRzaW5naHVhLmVkdS5jbg==; Feng Jiang, ZmVuZ2ppYW5nQHNqdHUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship