 Basem Gohar
Basem Gohar Behdin Nowrouzi-Kia
Behdin Nowrouzi-Kia- 1Department of Population Medicine, The University of Guelph, Guelph, ON, Canada
- 2Centre for Research in Occupational Safety & Health, Laurentian University, Sudbury, ON, Canada
- 3Department of Occupational Therapy and Occupational Science, The University of Toronto, Toronto, ON, Canada
Objective: The purpose of this qualitative study was to understand the stressors and coping strategies of medical laboratory technologists (MLTs) and assistants (MLAs) working during the COVID-19 pandemic in Ontario, Canada.
Methods: In this descriptive qualitative study, we held two focus groups with MLTs and MLA who were working during the COVID-19 pandemic. The focus group sessions were transcribed verbatim followed by thematic analysis to develop codes and themes.
Findings: A total of 13 participants across Ontario were involved in our study, which included one MLT (n = 7) group and one MLA (n = 6) MLA. Overall, the stressors and coping methods identified between both focus groups were consistent. Our results revealed four main themes: (1) COVID-19 contributing to the notable and existing staff shortage; (2) the pandemic reinforced that medical laboratory employees are forgotten within the healthcare system; (3) a poor work environment exacerbated by the pandemic; and (4) a resilient and passionate group. Rich descriptions explained the underlying issues related to the themes.
Conclusions: MLTs and MLAs are critical members of the healthcare team and provide vital patient care services. This study explored their experiences working during the pandemic and offers timely recommendations to mitigate against occupational stressors.
Introduction
The coronavirus disease (COVID-19) has undoubtedly affected healthcare workers' mental health and wellbeing (1). Despite the remarkable effort in containing the virus through physical distancing, restrictions, and vaccinations, various strands of the virus continue mutating, increasing the number of COVID-19 cases and hospital admissions. As a result, the impact of the virus continues to impact frontline healthcare staff like physicians and nurses who have been working longer and harder. Unsurprisingly, the added demand has been impacting their psychosocial wellbeing. Consequently, there have been reports of higher burnout rates, increased sickness absenteeism, and intention to leave the profession (2–4).
We thank our doctors and nurses for their dedication and care as we combat this virus with immense sincerity. Nevertheless, notably, one group of healthcare workers appears to have been forgotten during this pandemic: our medical laboratory technologists (MLTs) and assistants (MLTAs). These workers provide vital services in disease prevention (5). MLTs and MLAs collect and analyze various specimens for diagnostic and treatment purposes. In addition, they play an integral role in COVID-19 virus testing and analysis. In 2021, Ontario medical laboratory personnel managed to collect and analyze 13,262,409 COVID-19 tests, reaching as high as 76,000 tests in a single day (6). Naturally, the demand for medical laboratory services has significantly increased due to the pandemic (7).
Our literature review identified some studies addressing the physical safety aspect of the profession (8, 9). However, despite their essential role in the healthcare system, very little is known about their stressors and experiences during the pandemic. The limited research about their stressors pre-pandemic is equally concerning, suggesting that compared to other healthcare workers, MLTs, and MLAs are vastly understudied. From a provincial perspective, data suggests a shortage in medical laboratory employees before the pandemic (7), which could adversely affect their wellbeing. Recognizing their essential role in healthcare, especially during the pandemic, it is critical to learn about their current stressors and identify stress management strategies. This is of utmost importance since the limited research among MLTs and MLAs point to adverse outcomes such as errors, sickness absenteeism, job dissatisfaction, and intention to leave the profession when work demands are increased (5, 10, 11). These outcomes could have adverse and costly consequences to the general public, as every healthcare system relies heavily on accurate and speedy laboratory results for diagnostics and treatment. Accordingly, the purpose of this qualitative study was to understand the stressors of MLTs and MLAs working during the COVID-19 pandemic in Ontario, Canada.
Methods
In this descriptive qualitative study, we held focus groups with MLTs and MLAs from Ontario, Canada. We obtained ethics approval from the University of Toronto's Research Ethics Board (REB#00039635). In partnership with the Medical Laboratory Professionals' Association of Ontario, they assisted us with the recruitment of this study. Specifically, they advertised our study through their newsletters and electronic correspondence. Interested participants contacted the authors directly, to which we obtained informed consent in writing and virtually prior to the focus group. Eligible participants were either MLTs or MLAs in Ontario working during the pandemic. MLTs are regulated healthcare providers in Ontario, governed by the College of Medical Laboratory Technologists of Ontario. MLAs include professionals known as phlebotomists, technicians, or assistants. They often assist MLTs in specimen collection for analysis.
Based on the number of interested participants, we held one focus group with MLTs and another with MLAs. It should be noted that MLTs and MLAs have seen a significant increase in work demand due to the pandemic, which could explain the challenges in recruiting participants to form additional focus groups. However, Guest et al. (12) argued that focus groups, as small as two, could reach saturation, capturing up to 80% of themes, including the most prevalent themes.
For health and feasibility reasons, we facilitated the focus groups virtually in June 2021, securely using Microsoft Teams, which were audio-recorded. Two researchers (BG and BNK) were present in each focus group. One author (BG) served as the moderator in both focus groups. Each focus group was ~75 min long. Following the participant introductions, which included information on the participant's region and work setting, we used a semi-structured interviewing process, asking open-ended questions with follow-ups as deemed appropriate (Appendix A). Given the scarcity of information from the literature, we asked about the general stressors in the job then followed up with questions related to pandemic-related stressors. Finally, we asked them how they reduced stress while working during the pandemic. Each participant was assigned a code to ensure confidentiality and accuracy during transcription. The audio recording was later transcribed verbatim into text. The researcher (BG) reviewed the transcripts while listening to the audio recording to improve credibility. This method was also helpful for the data analysis, as it allowed the researcher to be further familiarized with the content (13).
We applied Braun and Clarke's six steps of thematic analysis to develop codes and themes (13). We used Quirkos qualitative data analysis software to code our data (14). Both researchers (BG and BNK) inductively coded the data. Specifically, each researcher read each transcript and coded textual data based on important notes related to the research questions, including similarities and distinctions from each group (13). Based on these patterns, initial codes were produced, and the transcript was reread through, ensuring coding accuracy. Horizontal and vertical relationships were analyzed in forming and clustering codes by which related content was joined to form themes. The codes and themes developed by each researcher were then iteratively reviewed and consolidated accordingly to produce the final themes and subthemes. Both researchers met after coding the data to discuss the codes and themes. The researchers worked on finalizing the themes and subthemes and discussed any discrepancies until a decision had been reached. Additionally, we applied the Consolidated Criteria for Reporting Qualitative Research (COREQ) to ensure the quality of our work (15) (Appendix B).
Findings
A total of 13 participants were involved in our study. The MLT focus group had seven participants. These included five who identified as women and two who identified as men. The MLA focus group contained six participants who identified as women. Participants were from across Ontario, including northeastern, eastern, southwestern, and central Ontario, including rural and urban regions. There was also diversity in the occupational setting, which included hospitals, private laboratories, and medical health clinics. Please see Table 1 for demographic information.
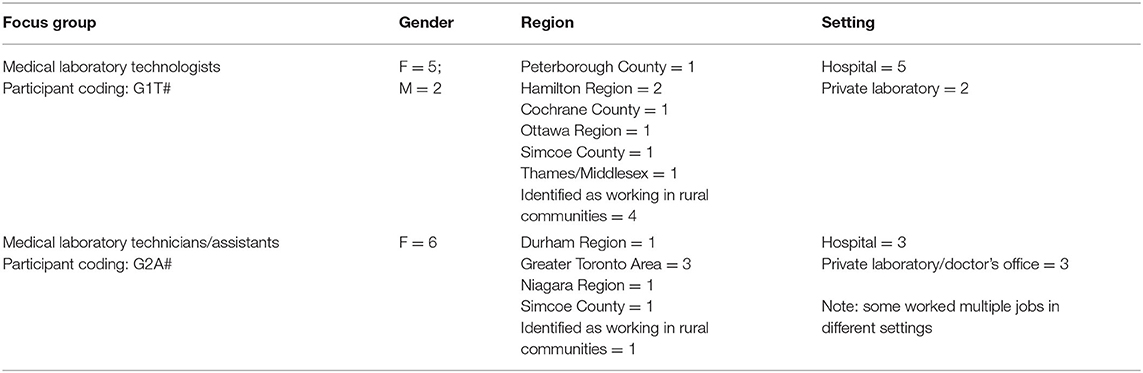
Table 1. Characteristics of participants involved in focus groups.
Overall, both focus groups' stressors and coping methods were reasonably consistent. We identified four primary themes based on our questions and the discussions held in the focus groups, which include (1) COVID-19 contributing to the notable and existing staff shortage; (2) the pandemic reinforced that medical laboratory employees are forgotten within the healthcare system; (3) a poor work environment, exacerbated by the pandemic; and (4) a resilient and passionate group (Table 2). These are discussed in detail in subsequent sections. Each theme contains a table delineating subthemes and selected excerpts.
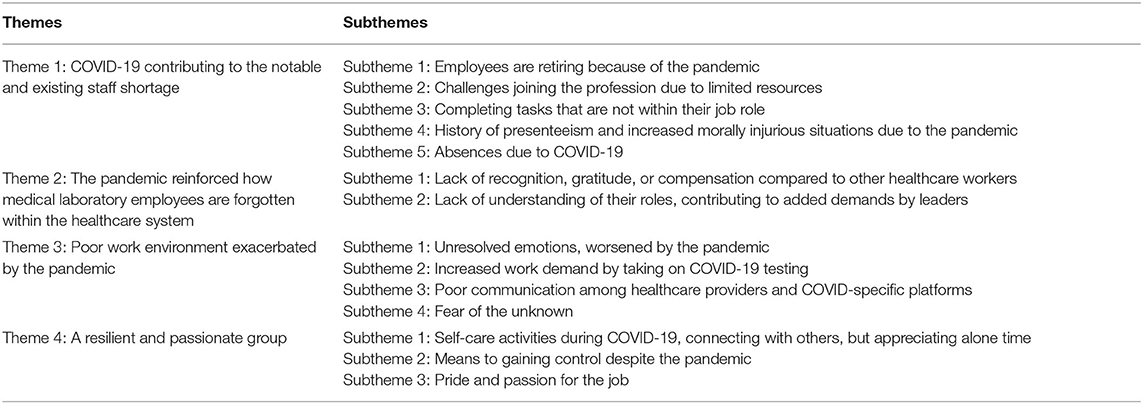
Table 2. Themes and subthemes emerged from focus groups via thematic analysis.
Theme 1: COVID-19 Contributing to the Notable and Existing Staff Shortage
Staff shortage was identified as a significant contributor to the stress of MLTs and MLAs. Participants reported that staff shortage had been an issue before the pandemic due to high turnover rates (Table 3). However, the negative impact of staff shortage became more profound due to the pandemic. Reportedly, a large proportion of the medical laboratory population is eligible for retirement. As a result, more employees are retiring sooner because of the increased work demand resulting from the pandemic, contributing further to the staff shortage. Additionally, there are few programs and seats within those programs available in Ontario that provide medical laboratory training. Furthermore, there are no “bridging” programs for MLAs who wish to become MLTs. Finally, the ability to complete clinical placements has been more challenging because of the pandemic.
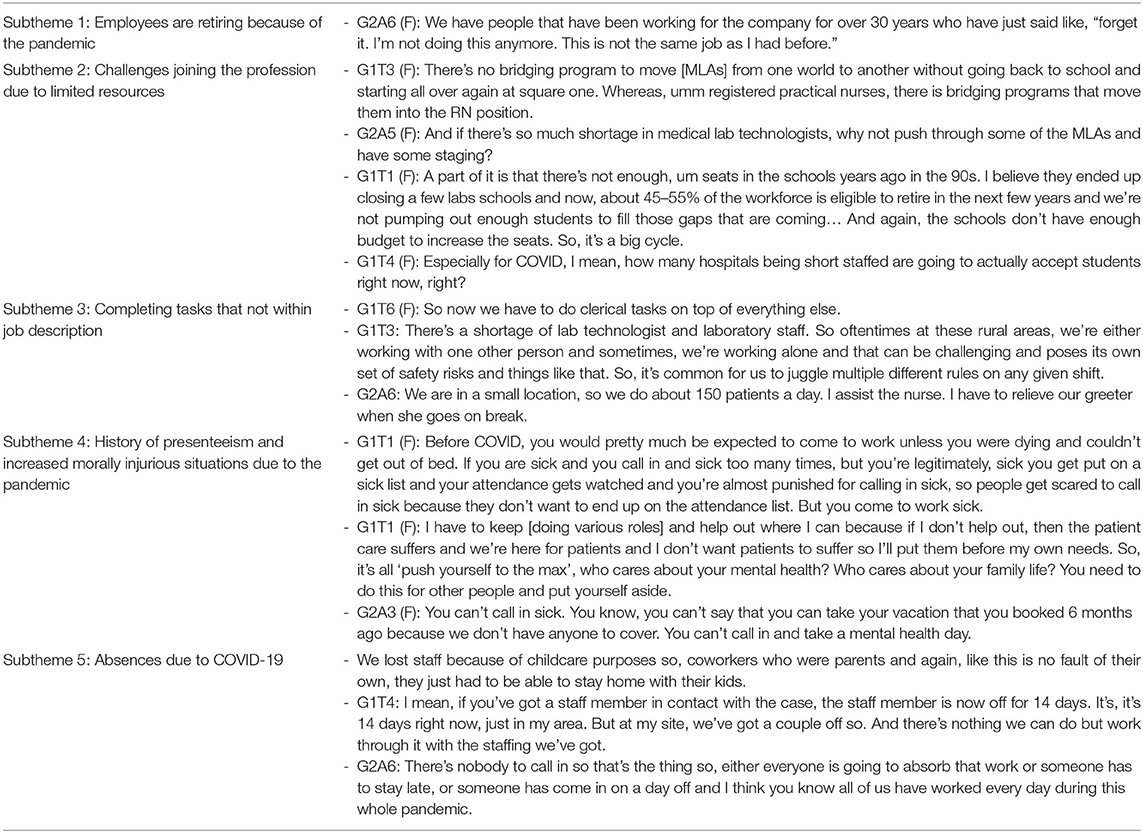
Table 3. Theme 1: COVID-19 Contributing to the notable and existing staff shortage.
Given the general shortage in healthcare, particularly in MLTs and MLAs, participants noted that they have been completing several tasks that are not a part of their job description. Some of these tasks include clerical and screening tasks that absorb a significant amount of time from their assigned duties. Juggling several tasks was particularly an area of concern in less populated regions, including rural areas.
Leaving the profession due to issues around childcare because of the pandemic was seen as a stressor contributing to the staff shortage. Additionally, our findings revealed that long absence rates increased because of contracting the virus, causing more staffing disruptions. It is important to note that some participants explained that presenteeism was a significant concern before the pandemic due to the guilt of leaving the team short-staffed. Presenteeism also occurred before the pandemic due to expectations from management, partly due to staff shortage.
Staff shortage was also linked to experiencing poorer mental health, particularly experiencing morally injurious situations. Specifically, MLTs and MLAs find it challenging to take time off due to the increased demands and limited resources. Instead, they feel obligated to work in these fast-paced conditions not to compromise patient care.
Theme 2: The Pandemic Reinforced That Medical Laboratory Employees Are Forgotten Within the Healthcare System
Our findings suggest that the medical laboratory environment's “behind-the-scenes” nature has led to unique stressors (Table 4). Expressly, participants indicated that they are often forgotten in relation to other healthcare providers. As an example, participants reported that, despite the added demands due to the pandemic, they did not receive expressions of gratitude from the healthcare sector, the public, or the government. Participants also felt forgotten from a financial perspective, where they did not receive “COVID” pay as other essential workers in Ontario. Added stress was incurred when the government indirectly condemned MLTs and MLAs through the media for not producing enough COVID tests. Some participants noted that this “attack” was a clear indication of the lack of understanding from the government about the work of the MLT and MLA population and the increased demands from the pandemic.
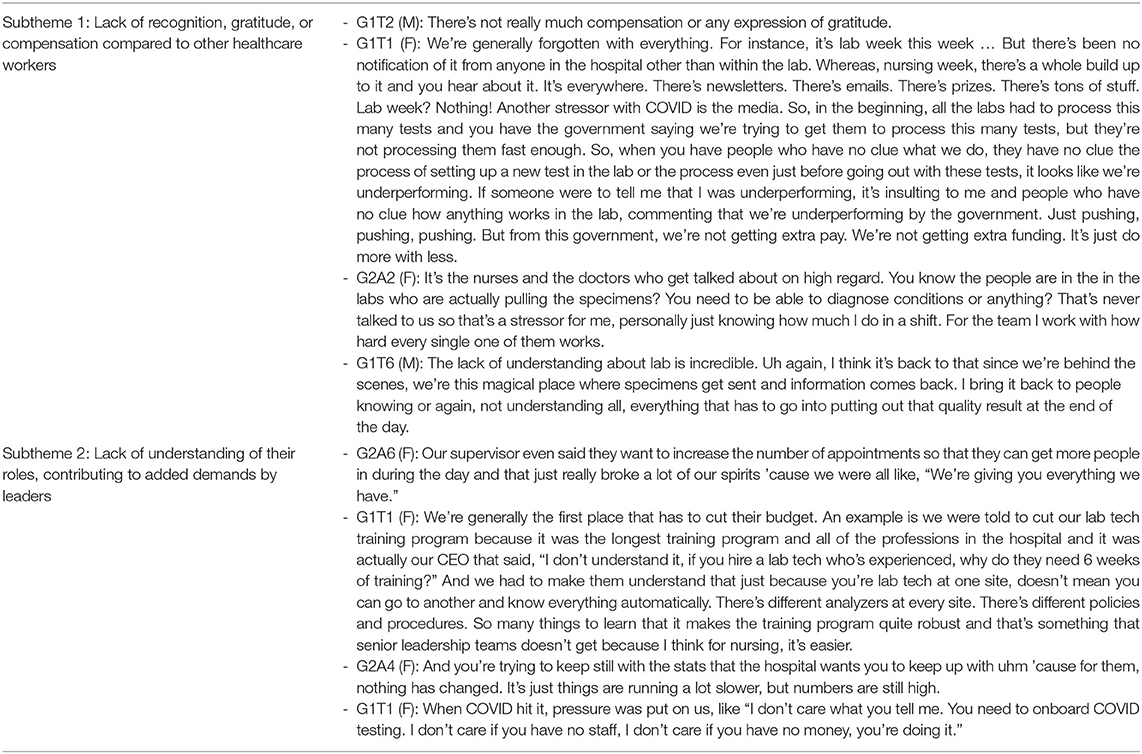
Table 4. Theme 2: The pandemic reinforced that medical laboratory employees are forgotten within the healthcare system.
Some participants explained that this lack of understanding extends beyond the government. They noted this lack of understanding from the general public and even other healthcare providers. Participants explained that MLTs could be forgotten because they are non-patient-facing. They also explained that the general public is unaware of patient-facing MLAs like phlebotomists. MLA participants explained that they are often mistaken for a nurse.
Participants expressed that the added demands from management could also result from the limited or unwillingness to understand their roles. They noted that despite the limited resources and staff shortage, expectations from management, whether it be in a hospital or a private clinic, have increased significantly. The pandemic is partly a reason for these high expectations, as MLTs and MLAs are required to complete their regular duties and collect and analyze COVID-19 tests.
Theme 3: A Poor Work Environment, Exacerbated by the Pandemic
Our results highlighted various factors within the work environment that contributed to the stress of MLTs and MLAs in general and within the context of the pandemic (Table 5). First, there is an emotional component of the job that does not appear to be addressed. Specifically, participants noted that given their role in analyzing specimens, they are the first to know of certain diseases like cancer. While many might not be patient-facing, they indicated that this is a stressful part of their job. For patient-facing MLAs, they reported that they are typically the first line of healthcare staff a patient visits once they receive diagnoses. Unsurprisingly, these workers deal with the patients' distress and poor mental health. Additionally, given the provincial restrictions to curb the spread of COVID-19, patient-facing MLAs noted that they typically work with patients who have been isolated. They listen to their challenges and support them as needed.
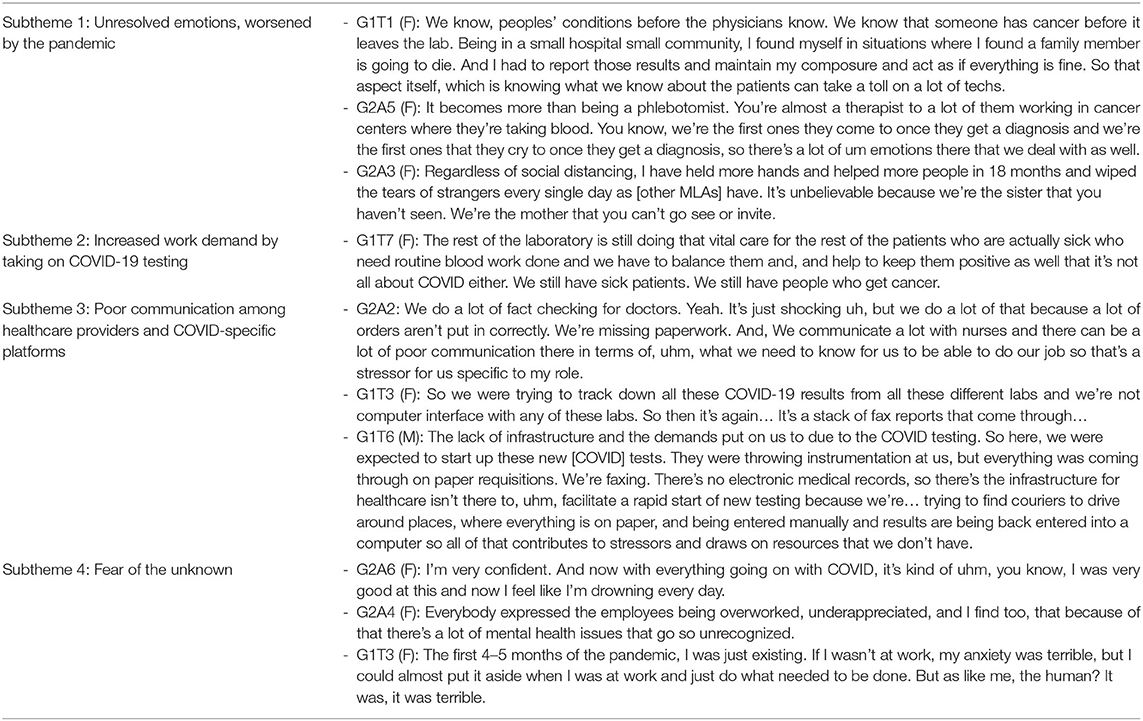
Table 5. Theme 3: Poor work environment, exacerbated by the pandemic.
Participants expressed that the workload has increased significantly because of the pandemic. Specifically, in addition to their highly demanding work, MLTs and MLAs were tasked with collecting and analyzing COVID tests, which reportedly has been a stressful experience. This is due to the need to learn new analyzers rapidly and, at the same time, maintain the same pace in terms of collecting and analyzing other specimens that are not related to the pandemic.
Based on the discussions from the focus groups, it appears that the pandemic has contributed to communication issues affecting the work environment. These communication issues exist between medical laboratory employees and other healthcare providers. For instance, MLAs noted that specific tests are sometimes not ordered correctly from the requesting physician or nurse, leading to patient frustration, and added work to the medical laboratory teams.
Communication issues also resulted from not having the right resources (e.g., computer programs) to interact with other necessary departments for COVID-19 testing. Specifically, medical laboratory staff were tasked with completing tasks inefficiently but were expected to complete them quickly. Additionally, they had to learn new instruments for COVID-19 testing, compounding the stress level.
With all the demands in conjunction with the limited resources, participants noted that their mental health has been poorer due to the pandemic. Like other professions, participants explained the “unknown” factor that came with the pandemic along with the restrictions; their mental health deteriorated considerably.
Theme 4: Resilient and Passionate Group
Despite the considerable challenges, including poorer mental health, MLTs and MLAs presented as passionate and resilient employees (Table 6). Specifically, they offered several coping methods to help them deal with their stressors at work. Exercising was a common coping mechanism among the participants. Similarly, was visiting nature and being outside was also a popular method. Whether from family, friends, colleagues, or management, social support was also noted as a helpful strategy. However, participants emphasized that “alone time” was equally important. They explained that because of their increased demand, need to support others, and the emotional component of their job, being alone was a therapeutic method to recuperate. In addition, seeking mental health support and positive self-talk were also used by some participants.
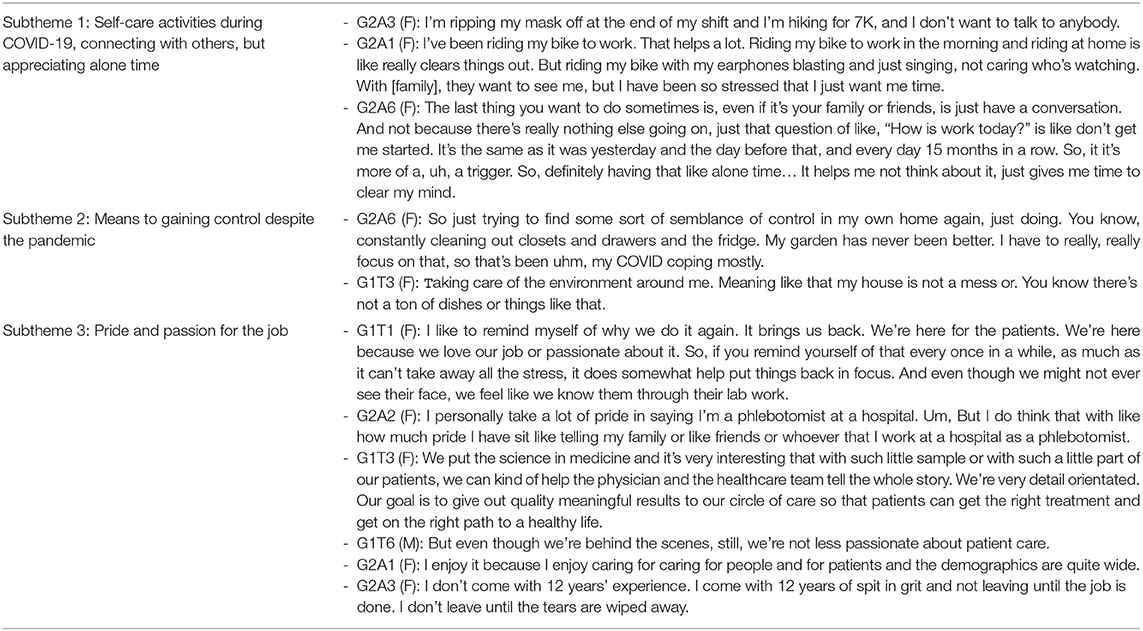
Table 6. Theme 4: A resilient and passionate group.
Gaining control was viewed as a COVID-specific coping method. Specifically, participants noted that due to the perceived lack of control from work or because of the imposed restrictions, they strived to gain control in other forms by organizing, cleaning, or focusing on projects like gardening. Some participants indicated that this was a helpful way to improve their mental health and compensate for other areas in their life where control is unmanageable.
Finally, the passion that the MLTs and MLAs have for their profession was viewed as a subtheme related to their resilience. This subtheme emerged organically from their discussions, highlighting that, despite their lack of recognition and the increased demands along with limited resources, they reported a great sense of pride in doing their job, highlighting their high regard for patient-centered care.
Discussion
This qualitative study revealed general stressors of MLTs and MLAs in Ontario, Canada, and within the context of the pandemic. It also helped us learn about their passion for their work and coping strategies. Our findings revealed substantial stressors evident before the pandemic but have exacerbated since. Due to the notable staff shortage, the behind-the-scenes nature of the job, and challenging working conditions, medical laboratory employees have been experiencing unique and significant stress levels.
Staff shortage is a known yet challenging issue within the healthcare sector (16–18). For instance, a qualitative study revealed that staff shortage was an underlying factor in sickness absenteeism among nurses and healthcare aides (18). As a result of staff shortage, nursing employees often work longer hours with increased demands, which increases their risk of going on sick leave due to physical and mental health reasons. This cyclical paradigm in the healthcare sector is consistent with our study's findings. However, three main factors are making the medical laboratory profession particularly vulnerable.
First, there are few programs and seats available for students interested in enrolling in the medical laboratory field in Ontario. At the same time, there is an increase in employees retiring or leaving the profession due to the stress of the pandemic. Second, there seems to be a missed opportunity for MLAs interested in becoming MLTs. Therefore, opportunities for professional growth in the province are scant, which likely contributes to the disinterest in entering the field at an MLA or MLT capacity. As one participant compared, there are opportunities for career development in the nursing field through bridging programs such as transitioning from a registered practical nurse to a registered nurse. Similar options do not exist in Ontario for the medical laboratory population. A third factor contributing to the staff shortage in the medical laboratory field is the sense of feeling forgotten due to the behind-the-scenes nature of the profession, which is one of the main themes that emerged from this undertaking. As participants noted, MLTs are typically non-patient-facing employees, and MLAs who are patient-facing are mistaken for other positions like nurses. This lack of recognition from the healthcare sector and the government likely contributes to the staff shortage as the public seems vastly unaware of this population. Notably, with limited research in this population, we suspect this lack of recognition is not unique to Ontario but rather a global issue.
In Ontario, MLTs and MLAs were not included in what the government identified as “pandemic pay” (19) to support frontline staff experiencing severe challenges and elevated risk during the COVID-19 pandemic. Their exclusion further exacerbated their frustrations regarding lack of appreciation in the work environment. Like all healthcare workers, MLTs and MLAs are compassionate providers who care about their patients and felt the lack of recognition by the government in acknowledging their contribution as frontline staff providing patient care during the pandemic. The COVID-19 pandemic has significant and widespread influences across all practice areas for medical laboratory professionals. Perturbations in workflow, increases in job demands and occupational stressors have inversely impacted job satisfaction, health, wellbeing, and overall functioning in delivering optimal patient care, thus compromising patient safety.
Pressures from the pandemic exposed the vulnerability of the healthcare system. Before the pandemic, MLTs and MLAs were expected to report to work even if they felt ill, a concept known as presenteeism (20). MLTs and MLAs reported similar issues to healthcare staff like nurses in which they are attending work, feeling concerned about job security (e.g., being sick and still reporting to work), exaggerated levels of attendance that results in illness, occupational stress, work productivity (21), and disability (20). Furthermore, presenteeism has been reported to exacerbate medical conditions (22), damage the quality of working life (23), impact functioning (24), and lead to impressions of ineffectiveness at work due to reduced productivity (25). The relationship between presenteeism and occupational stress may follow a certain dynamic (26). Specifically, pressures placed on relatively scarce health human resources (e.g., recruitment challenges, restricted funding) lead to increased job stress and higher rates of sickness absence. When more MLTs and MLAs are off work, occupational stress increases further, job duties will compound and be viewed as inflexible by workers, and further reductions in service delivery will appear as intolerable by management. The severe consequences for the delivery of health services if MLTs and MLAs are absent lead to elevated thresholds for taking sick leave and result in higher presenteeism levels (26). Strategies are warranted to address sickness absences through evidence-based recommendations that examine their impact on MLTs and MLAs' mental health and work performance.
An added concern for this population is the occurrence of morally injurious events. Morally injurious situations occur when individuals must make decisions that conflict with their values. Specifically, it is the dissonance occurring between what “should” be done and what “could” (or could not) be done (27, 28). This research area remains relatively scant in the extant literature for healthcare workers. However, given the impact of the pandemic on healthcare workers, it has been gaining more traction (29). For medical laboratory employees, facing morally injurious situations occurs primarily due to the guilt of taking time off, recognizing the impact it could have on the remainder of the team, and also the impact it could have on patient care. It also occurs with MLAs working with vulnerable populations who have been unable to seek face-to-face support from their loved ones due to the imposed restrictions to reduce the risk of contagion. To this end, we recommend further research in moral injury in healthcare workers, including occupational groups such as MLTs and MLAs.
Notwithstanding the presented challenges and the lack of recognition, our study revealed that medical laboratory professionals are passionate and patient-centered individuals who presented with positive coping strategies. Despite these positive traits, many are retiring or are leaving the profession, causing a more significant gap in the staff shortage crisis. Thus, moving forward, we recommend that workplaces espouse a culture where MLTs and MLAs feel supported and respected for their contributions to patient care, including the delivery of services. Their roles should be described to the broader healthcare sector, including their work demands, staff shortage, and the emotional aspect of their job to allow for better communication and prioritization of patient needs. While it might be challenging to execute, we recommend more media attention, capturing the work that goes into COVID testing and other specimen analyses to help inform the government and the general public. We also recommend that policymakers and senior managers take a proactive approach. Specifically, they should work collaboratively with MLT and MLA groups to learn about their roles in more detail, allowing for reasonable working demands and realistic expectations.
One main limitation to this study was recruiting enough participants from both groups to form additional focus groups. However, as previously noted, these employees have been facing added pressures, which could have affected recruitment. However, to our surprise, the themes that emerged from both groups were very consistent. Thus, readers should conceptualize these findings at a broader level to understand the challenges faced within the medical laboratory population. Future studies should investigate these groups independently to understand their needs better during the pandemic and beyond.
Conclusions
MLTs and MLAs are the “conveyer belt” of the healthcare system, as they are involved in the analysis of specimens for diagnostic purposes, yet their contributions are largely unnoticed. While staff shortage and attrition are common issues in the healthcare field, disruptions in medical laboratory services would likely cause significant disruptions to the overall healthcare system. Our study identified key themes that highlight critical knowledge gaps about occupational stressors that are only being raised due partly to the COVID-19 pandemic. Future research studies should explore MLTs and MLAs' lived experiences in their work environment. We believe such an approach will strengthen recruitment and retention capacities for both groups and provide evidence-based information to strengthen government funding to increase MLT enrolment at Ontario Colleges to train the next generation of medical laboratory professionals.
Data Availability Statement
As this is a qualitative study, releasing the raw data (i.e., transcripts) poses the risk of identifying participants. Thus, due to ethical restrictions, this data is not available. Questions should be directed to: YmVoZGluLm5vd3JvdXppLmtpYUB1dG9yb250by5jYQ==.
Ethics Statement
The studies involving human participants were reviewed and approved by University of Toronto Research Ethics Board. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
Both authors substantially contributed to the conception of the work, the interpretation of the data, substantially contributed to the drafting and revising of the work, agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy and integrity of any part of the work are appropriately investigated and resolved, and approved the final version to be published.
Funding
The Medical Laboratory Professionals' Association of Ontario funded the Article Processing Charge of this study.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.854507/full#supplementary-material
References
1. Gaind Ks. Mental Health and Healthcare in Canada during the COVID-19 epidemic: a social perspective. World Social Psychiatry. (2020) 2:20. doi: 10.4103/WSP.WSP_45_20
2. Labrague LJ, Santos JAA. Fear of COVID-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J Nurs Manag. (2021) 29:13168. doi: 10.1111/jonm.13168
3. Nowrouzi-Kia B, Sithamparanathan G, Nadesar N, Gohar B, Ott M. Factors associated with work performance and mental health of healthcare workers during pandemics: a systematic review and meta-analysis. J Public Health. (2021) 2021:fdab173. doi: 10.1093/pubmed/fdab173
4. Said RM, El-Shafei DA. Occupational stress, job satisfaction, and intent to leave: nurses working on front lines during COVID-19 pandemic in Zagazig City, Egypt. Environ Sci Pollut Res. (2021) 28:8791–801. doi: 10.1007/s11356-020-11235-8
5. Abdollahi A, Saffar H, Saffar H. Types and frequency of errors during different phases of testing at a clinical medical laboratory of a teaching hospital in Tehran, Iran. N Am J Med Sci. (2014) 6:224. doi: 10.4103/1947-2714.132941
6. COVID-19 Provincial Daignostic Network Operations Centre,. Testing Volumes Results. Government of Ontario (2022). Available online at: https://covid-19.ontario.ca/data/testing-volumes-and-results#testingData (accessed February 16, 2022).
7. Tran J. Research Initiative: Clinical Placement Shortage of Medical Laboratory Technologists. Toronto, ON (2021). Available online at: https://www.mlpao.org/_files/ugd/054d07_14a4d4931ee740419253ab401a3752ef.pdf (accessed February 16, 2022).
8. Maulik S, Iqbal R, De A, Chandra AM. Evaluation of the working posture and prevalence of musculoskeletal symptoms among medical laboratory technicians. J Back Musculoskel Rehabil. (2014) 27:453–61. doi: 10.3233/BMR-140466
9. El-Helaly M, Balkhy HH, Vallenius L. Carpal tunnel syndrome among laboratory technicians in relation to personal and ergonomic factors at work. J Occup Health. (2017) 59:513–20. doi: 10.1539/joh.16-0279-OA
10. Blau G, Ward-Cook K, Edgar LK. Testing for the impact of correlates on medical technologists' intent to leave their jobs. J Allied Health. (2006) 35:94–100.
11. Alrawahi S, Sellgren SF, Alwahaibi N, Altouby S, Brommels M. Factors affecting job satisfaction among medical laboratory technologists in University Hospital, Oman: an exploratory study. Int J Health Plann Manag. (2019) 34:2689. doi: 10.1002/hpm.2689
12. Guest G, Namey E, McKenna K. How many focus groups are enough? Building an evidence base for nonprobability sample sizes field. Methods. (2017) 29:3–22. doi: 10.1177/1525822X16639015
13. Braun V, Clarke V. Using thematic analysis in psychology. Qualitat Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
15. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. (2007) 19:349–57. doi: 10.1093/intqhc/mzm042
16. Hassmiller SB, Cozine M. Addressing the nurse shortage to improve the quality of patient care. Health Aff. (2006) 25:268–74. doi: 10.1377/hlthaff.25.1.268
17. Gohar B, Larivière M, Nowrouzi-Kia B. Sickness absence in healthcare workers during the COVID-19 pandemic. Occup Med. (2020). 70:kqaa093. doi: 10.1093/occmed/kqaa093
18. Gohar B, Larivière M, Lightfoot N, Wenghofer E, Larivière C, Nowrouzi-Kia B. Understanding sickness absence in nurses and personal support workers: Insights from frontline staff and key informants in Northeastern Ontario. Work. (2020) 66:203222. doi: 10.3233/WOR-203222
19. Government of Ontario. Archived - COVID-19: Temporary Pandemic Pay. Toronto, ON: Government of Ontario (2021). Available online at: https://www.ontario.ca/page/covid-19-temporary-pandemic-pay (accessed February 16, 2022).
20. Johns G. Presenteeism in the workplace: a review and research agenda. J Organ Behav. (2010) 31:519–42. doi: 10.1002/job.630
21. Fiorini LA, Houdmont J, Griffiths A. Nurses' perceived work performance and health during presenteeism: cross-sectional associations with personal and organisational factors. J Nurs Manag. (2020) 2020:13065. doi: 10.1111/jonm.13065
22. Callen BL, Lindley LC, Niederhauser VP. Health risk factors associated with presenteeism in the workplace. J Occup Environ Med. (2013) 55:1312–7. doi: 10.1097/JOM.0b013e3182a200f4
23. Whysall Z, Bowden J, Hewitt M. Sickness presenteeism: measurement and management challenges. Ergonomics. (2018). 61:341–54. doi: 10.1080/00140139.2017.1365949
24. Landry M, Miller C. Presenteeism: are we hurting the patients we are trying to help? J Gen Intern Med. (2010) 25:1142–3. doi: 10.1007/s11606-010-1487-6
25. Kinman G. Sickness presenteeism at work: prevalence, costs and management. Br Med Bull. (2019) 129:69–78. doi: 10.1093/bmb/ldy043
26. Elstad JI, Vabø M. Job stress, sickness absence and sickness presenteeism in Nordic elderly care. Scand J Public Health. (2008) 36:467–74. doi: 10.1177/1403494808089557
27. Cartolovni A, Stolt M, Scott PA, Suhonen R. Moral injury in healthcare professionals: a scoping review and discussion. Nurs Ethics. (2021) 28:590–602. doi: 10.1177/0969733020966776
28. Dean W, Talbot S, Dean A. Reframing clinician distress: moral injury not burnout. Fed Pract. (2019) 36:400–2.
Keywords: medical laboratory professionals, COVID-19, mental health, Ontario, Canada, qualitative
Citation: Gohar B and Nowrouzi-Kia B (2022) The Forgotten (Invisible) Healthcare Heroes: Experiences of Canadian Medical Laboratory Employees Working During the Pandemic. Front. Psychiatry 13:854507. doi: 10.3389/fpsyt.2022.854507
Received: 14 January 2022; Accepted: 18 February 2022;
Published: 16 March 2022.
Edited by:
Sebastian von Peter, Brandenburg Medical School Theodor Fontane, GermanyReviewed by:
Valentin Ritschl, Medical University of Vienna, AustriaAmin Yazdani, Conestoga College, Canada
Copyright © 2022 Gohar and Nowrouzi-Kia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Behdin Nowrouzi-Kia, YmVoZGluLm5vd3JvdXppLmtpYUB1dG9yb250by5jYQ==