 Elzbieta Krajewska-Kułak1
Elzbieta Krajewska-Kułak1 Agnieszka Kułak-Bejda2*
Agnieszka Kułak-Bejda2* Wojciech Kułak3Grzegorz Bejda4
Wojciech Kułak3Grzegorz Bejda4 Cecylia Łukaszuk1
Cecylia Łukaszuk1 Napoleon Waszkiewicz2
Napoleon Waszkiewicz2 Mateusz Cybulski1
Mateusz Cybulski1 Andrzej Guzowski1
Andrzej Guzowski1 Joanna Fiłon1
Joanna Fiłon1 Paulina Aniśko5
Paulina Aniśko5 Magda Popławska6
Magda Popławska6- 1Department of Integrated Medical Care, Medical University of Białystok, Białystok, Poland
- 2Department of Psychiatry, Medical University of Białystok, Białystok, Poland
- 3Department of Pediatric Rehabilitation and Center of Early Support for Handicapped Children “Give a Chance”, Medical University of Białystok, Białystok, Poland
- 4The School of Medical Science in Białystok, Białystok, Poland
- 5Doctoral School, Medical University of Białystok, Białystok, Poland
- 6Students' Scientific Society, Department of Integrated Medical Care, Medical University of Białystok, Białystok, Poland
Introduction: People recently or currently in forced quarantine or isolation at home have shown high levels of depression and symptoms of generalized anxiety.
Aim of the Study: To assess the impact of the COVID-19 pandemic on certain aspects of people's day-to-day functioning.
Materials and Methods: The study involved using an online diagnostic survey including a proprietary questionnaire, the DASS 21, and the Liebowitz Social Anxiety Scale.
Results: Information about the pandemic in Poland and around the world was systematically obtained by 48.8 and 27.4% of respondents, respectively (N = 1,312). Whereas, 75.6% of respondents declared having knowledge about the number of infected people in Poland, only 28.7% declared having such knowledge about infections worldwide. Most often, respondents had obtained information online (65.9%). According to 45.7% of respondents, infection with COVID-19 is a major threat, and not enough has been done to reduce its spread in Poland (66.7%) or worldwide (56.1%). Respondents considered social distancing (68.3%), quarantining people arriving from abroad (63.4%), and wearing protective masks and/or gloves (60.4%) to be the most effective actions for combatting the pandemic. Most often, in compulsory quarantines, respondents surfed the Internet (48.8%) and experienced a lack of energy or fatigue (40.2%) and anxiety (54.9%). The severity of anxiety (mean = 4.6 points), stress (7.5 points), and depression (7.3 points) were within normal ranges, and the respondents could generally be included in the group showing mildly severe social phobia (57.9 points).
Conclusions: Most respondents considered infection with COVID-19 to be a major threat and feared another quarantine. During quarantine, respondents most often experienced fatigue, a lack of energy, nervousness, anxiety, anger, and sadness. Despite demonstrating anxiety, stress, and depression with severity in the normal range, respondents showed no statistically significant correlation between severity and age, gender, place of residence, or level of education. Although they also showed mildly severe social phobia, only gender, not age, place of residence, or level of education, showed a statistically significant correlation with its severity.
Introduction
Contemporary recommendations for forced isolation during epidemics follow the centuries-old tradition of protecting people from serious infectious diseases (1). Today, however, awareness of the dire consequences of isolating large numbers of people in quarantine means that such measures are taken only in the most serious of situations. Isolation due to epidemics indeed presents several challenges, including a diminished sense of control that can promote a sense of fear, largely because quarantine and social isolation restrict people's mobility, social interaction, and range of daily activities.
During the current pandemic, to limit the spread of COVID-19 infection worldwide, quarantine strategies have been introduced the world over, including short- and mid-term blockades, curfews, the cancellation of planned social events, the restriction of social gatherings and sport activities, the introduction of travel bans, and airspace and border closures (1–4). However, because most societies have never experienced such restrictions, people have associated the introduction of quarantines with the restriction of freedoms and imprisonment and even treated them as a form of punishment and condemnation. After all, social isolation is a form of quarantine with a recommendation not only to stay at home but also to avoid social contact outside the home, which implies separation from family, friends, and wider social networks, as well as disengagement from social activities (5–7).
Literature on people in quarantine conducted before the COVID-19 pandemic is rather sparse and most often concerns the SARS-CoV-1, MERS, Ebola, and influenza epidemics (8). In response, research on the scale and severity of emotional distress, including symptoms of depression and anxiety, in various countries remains necessary, especially to identify groups at a clinically severe risk of those symptoms. Indeed, staying in forced quarantine or home isolation is associated with several stressors that risk emotional problems, including severe symptoms of depression and/or generalized anxiety, insomnia, burnout syndrome (BOS), and post-traumatic stress disorders (PTSD) (9–14). In addition, people recently or currently in forced quarantine or isolation at home have shown relatively high levels of depression and symptoms of generalized anxiety, as well as a significantly higher severity of suicidal ideation and/or thoughts of self-harm than people not in quarantine (9). Beyond that, Logie and Turan (15) have shown that people diagnosed with COVID-19 may also experience rejection and stigmatization, which may most severely affect individuals who face discrimination daily (e.g., people of low socioeconomic status, refugees, immigrants, and minorities).
According to Chirico et al. (16), lockdown measures effectively curbing COVID-19 related new infections and deaths and overburden on the healthcare system. However, these measures are difficult to be maintained for a long time for economic reasons. This has an important implication because COVID-19 may exacerbate social inequities. Indeed, countries, where economic inequity is prevalent may be disadvantaged in the fight against the COVID-19 pandemic because the lockdown measures are unsustainable for a longer time.
Brooks et al. (9) have confirmed that people in quarantine or isolation at home may also sense a serious threat to their health and life, as well as worry that they may infect other people. Quarantine and isolation at home may also be associated with boredom, frustration due to the lack of personal freedom, and a sense of separation from the rest of the world, including loved ones. In addition, people in quarantine depend on the help of others to meet their basic needs, even in acquiring food, and awareness of such dependence can generate strong negative emotions that may increase if appropriate support from others is not received (9). Moreover, similarly to Logie and Turan (15), Brooks et al. (9) emphasized that people in quarantine or isolation may experience stigmatization and rejection from their immediate social environments, further intensifying their negative emotions.
In the study reported here, we decided to assess how the COVID-19 pandemic has influenced certain aspects of people's day-to-day functioning.
Materials and Methods
All respondents were Poles. Inclusion criteria: age over 18 years, staying at forced 14 days quarantine amid the COVID-19 pandemic. Exclusion criteria: age below 18 years, no staying at forced 14 days quarantine amid the COVID-19 pandemic.
The study group comprised (N = 1,312) people, including 88.4% women and 11.6% men. The respondents' age ranged from 19 to 79 years; the mean age was 57.3 ± 19.1 years. Eighty-four percent of the respondents lived in the city, and 16% in the countryside. Forty-seven percent of the respondents had higher education, secondary - 37.2%, bachelor's - 6.7, and 8.5% during their studies, and 0.6% of people had primary education.
The study used a diagnostic survey using an Internet platform over 26 days (from January 3, 2021, to June 28, 2021). The questionnaire was anonymous. All data obtained during the study will be generalized and used in a scientific study. Participation in the study was voluntary. Entering the survey was tantamount to agreeing to fill in the survey. Respondents had the right to resign at any time, regardless of the survey stage.
The questionnaire consisted of an in-house questionnaire, the Depression Anxiety and stress scale (DASS-21), and The Leibowitz Social Anxiety Scale—LSAS.
The Bioethics Committee approved the study of the Medical University of Bialystok-APK.002.33.2021.
Lovibond and Lovibond developed the used version of the Depression Anxiety and stress scale (DASS-21) scale in 1995 (16–18);1 it consisted of 21 items into three groups of 7 articles each: depression, anxiety, and stress. The tool applies to the last seven days. The respondents assessed individual items on a scale from 0 to 3 points, where 0- never, 1 - sometimes, 2 - often, and 3 - always / almost always. In case of depression - normal this 0–9 point, mild this 10–13 point, moderate this 14–20 point, severe this 21–27, extremely severe this 28+. In case of anxiety - normal this 0–7 point, mild this 8–9 point, moderate this 10–14 point, severe this 15–19, extremely severe this 20+. In case of stress - normal this 0–14 point, mild this 15–18 point, moderate this 19–25 point, severe this 26–33, extremely severe this 34+.
The Leibowitz Social Anxiety Scale (LSAS) allowed assessing the severity of social phobia symptoms and their impact on everyday functioning (19). The respondent must read the descriptions of all the situations presented in the table. Each case answers two questions: “how much anxiety or fear do I experience in this situation” and “how much am I willing to avoid such a situation.” For fear/drug questions - 0 is none, 1 - mild, 2 - moderate, 3 - strong; in the case of avoiding situations - 0 - never, 1- sometimes, 2- often, and 3- always (16). The scoring scale: 0–29 No social anxiety; 30–49 Mild social anxiety; 50–64 Moderate social anxiety; 65–79 Marked social anxiety; 80–94 Severe social anxiety; >95 Very severe social anxiety.
Statistical Analysis
All statistical analysis was performed with Statistica PL 13.0. Results are presented as mean values ± SD. Non-parametric Wilcoxon test was applied to compare differences. Spearman's analysis was used to measure the dependence age, sex, place residence, education, and the severity of depression, stress, and anxiety symptoms in the DASS 21 scale. The critical level for all tests of significance was p < 0.05.
Results
Information on the COVID-19 pandemic in Poland was systematically interested in 48.8% of respondents. In turn, 27.4% of respondents were systematically interested in information about the world's coronavirus pandemic.
Almost 76% of respondents declared knowing the number of infected people in Poland, only 28.7% declared having such knowledge about infections worldwide. Most often, respondents had obtained information online (65.9%).
According to 45.7% of respondents, infection with COVID-19 is a major threat, and not enough has been done to reduce its spread in Poland (66.7%) or worldwide (56.1%).
Fifty percent of respondents reported the probability of infection with the COVID-19.
Almost 67% of Poland respondents reported that not enough had been done to protect the country against the coronavirus epidemic. Nearly 20% of respondents expressed the opposite opinion. Respondents considered social distancing (68.3%), quarantining people arriving from abroad (63.4%), and wearing protective masks and/or gloves (60.4%) to be the most effective actions for combatting the pandemic.
Almost a half (48.8%) of respondents preferred Internet surfing (42.7%), mobilizing and trying to do everything to protect themselves from infection, watching movies (39.6%), or reading (33.5%). Table 1 presents other indications.
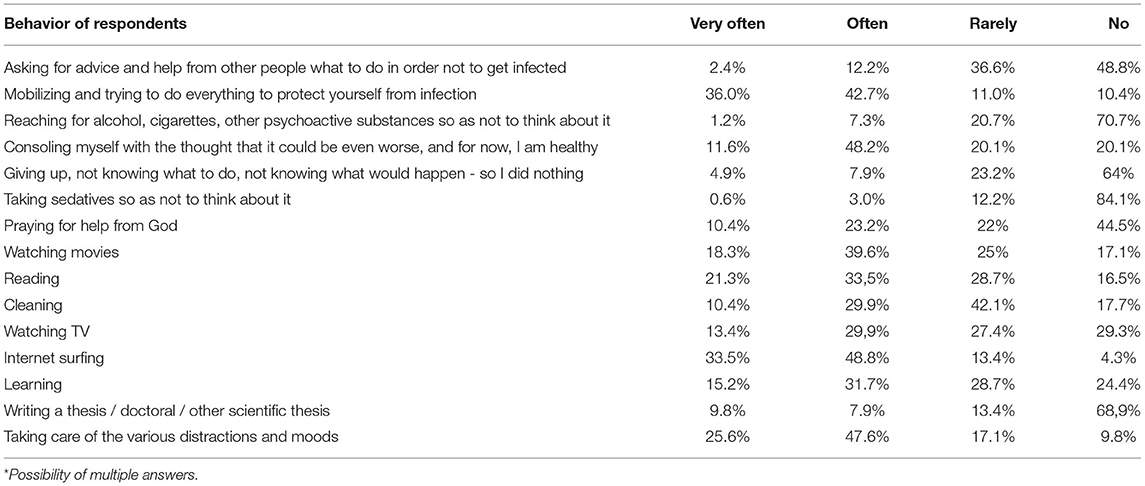
Table 1. Methods of the behavior of respondents in a situation of forced quarantine*.
The respondents declared that they most often spent between 8 and 12 h in front of the TV. The respondents often felt fatigue (40.2%), nervousness (39.6%), depression (37.2%), irritability (37.2%), or difficulty sleeping (32.9%). Details are presented in Table 2.
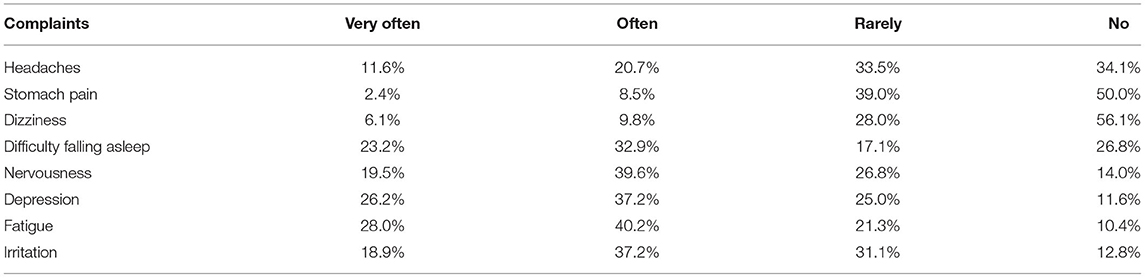
Table 2. Complaints occurring in respondents during their stay in forced quarantine.
The quarantine evoked the following various emotions in the respondents: anxiety (54.9%), exhaustion (46.3%), anger (39.6%), and sadness (38.4%).
The severity of anxiety (mean = 4.6 points), stress (7.5 points), and depression (7.3 points) was within normal ranges, and the respondents could generally be included in the group showing mildly severe social phobia (57.9 points). The detailed results are presented in Table 3.
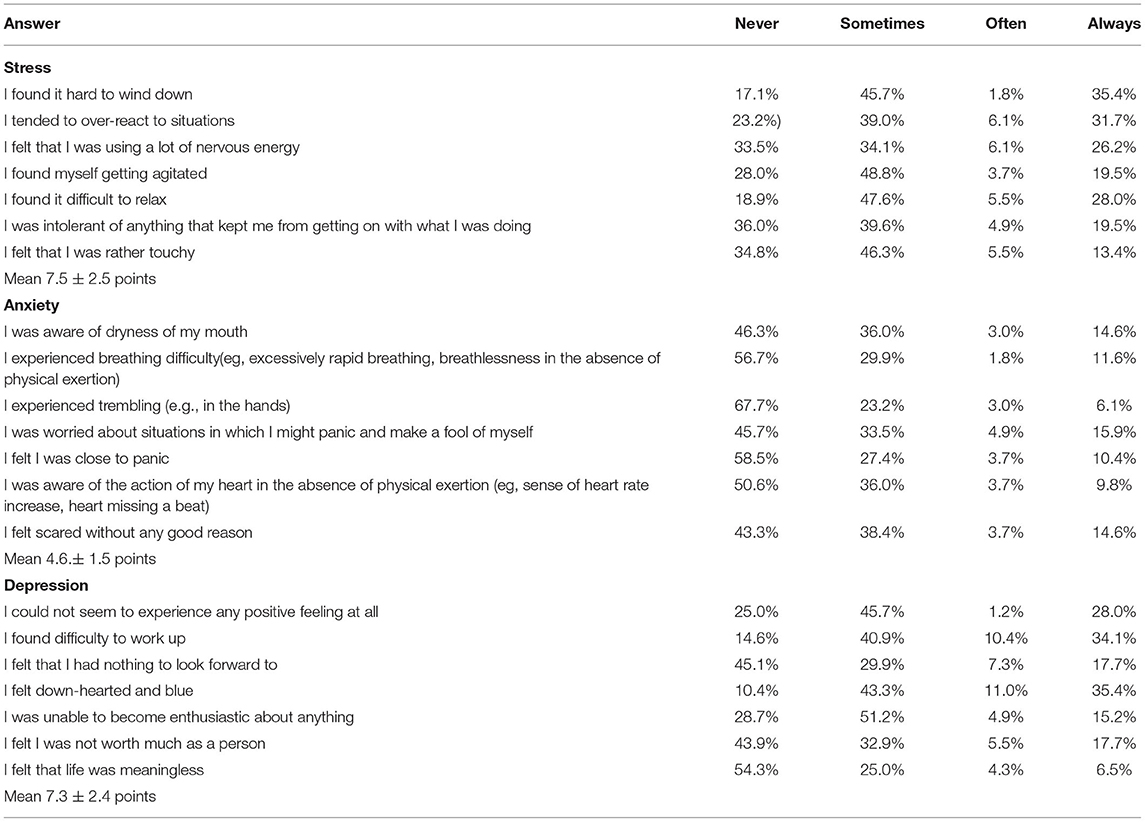
Table 3. Assessment of the respondents with the DASS 21 test.
No significant relationship between age, sex, place of residence, and education and the severity of depression, stress, and anxiety symptoms in the DASS 21 test was found.
Almost half (45.1%) of the respondents had no social phobia on the LSAS scale. Mild social phobia had 16.5% of respondents, moderate phobia – 17.1%, severe social phobia – 9.9%, and very severe – 11.4% of respondents. The results are presented in Table 4.
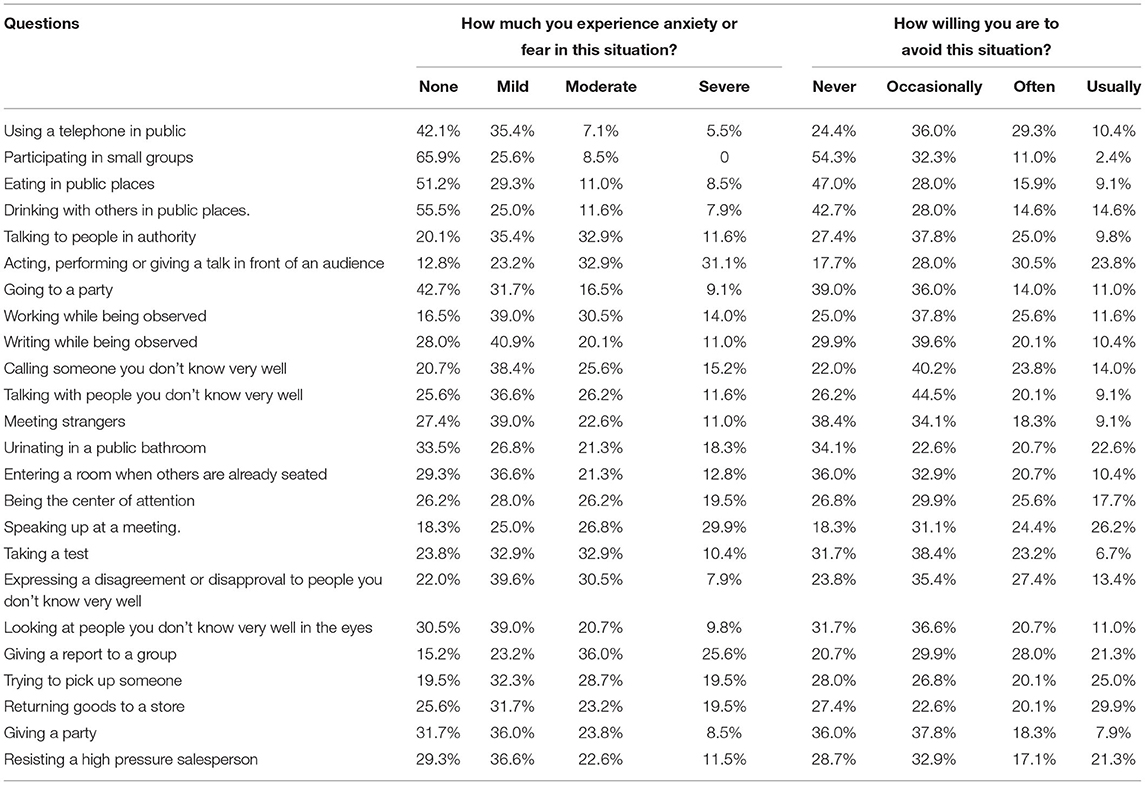
Table 4. Assessment of social anxiety in respondents using the Leibowitz scale.
No significant relationship between the severity of social phobia and age, place of residence, and education was found. The only positive correlation between the severity of social phobia and gender (R = 0.16904; p = 0.0304) was found.
Discussion
Due to the COVID-19 pandemic, sudden and severe restrictions influenced many people's mental health in the world. The quarantined people had to deal with stressful living conditions without prior preparation (20, 21). Each crisis or disaster pandemic carries a high risk of diminished wellbeing and individuals and societies as a whole (5, 22–24).
Hamer et Baran (22) conducted a study four times in 2020 (in March, April, at the turn of May and June, and in December) the CAWI (Computer-Assisted Web Interview) on a sample of 1,098 people aged 18 and over. They demonstrated a relatively high level of nervousness at the beginning of the pandemic in April. At the turn of May and June, a significant decrease was the lowest compared to the remaining months, then increased again to the level from April in December.
In a study from China (24), most respondents spent 20–24 h a day (84.7%) at home. In a study by Huang and Zhao (21), in a group of 603 randomly selected respondents, 264 people spent more than 3 h each day tracking information about the virus and the epidemic.
Information about the pandemic in Poland and around the world was systematically obtained by 48.8 and 27.4% of respondents, respectively (N = 328). The respondents most often obtained information about the pandemic from the Internet (65.9%) and television (22%).
The COVID-19 pandemic is a potent stressor affecting the functioning of many countries and aggravates social stress (9).
According to 40.9% of respondents, COVID-19 is a grave threat to Poles' lives in the present study. The probability of developing the coronavirus was most often determined by fifty percent of the respondents.
In the literature (25–34) quarantine may reveal mental health problems in people who did not before. Symptoms of post-traumatic stress and emotional exhaustion are also described.
The scientific publications show that in about 33% of people in isolation, their mental wellbeing worsened, and the severity of these symptoms was individual.
The pandemic clinical picture's most typical and common feature is an acute stress disorder. According to Heitzman (34), it is a prolonged anxiety reaction and the inability to break away from trauma's constant experience.
In a study from India, 12.5% of respondents reported sleep problems and, 37.8% had thoughts related to the possibility of COVID-19 infection. Furthermore, over 80% of respondents felt the need for mental support from the health care system (3).
The respondents reported mainly fatigue, nervousness, depression, and irritability in the current study.
Our results are similar to Pierce et al. (35) in the United Kingdom. The prevalence of clinically significant mental distress levels in the population increased from 18.9% in 2018–2019 to 27.3% in April 2020, 1 month after the UK economy closed. The increases were most significant among people aged 18–34, women living with young preschool children, and working before the epidemic.
In China, the impact of quarantine on the mental state, level of anxiety, depression, and stress during the initial stage of the COVID-19 outbreak in a group of 1,210 people was assessed by Wang et al. (36). More than half (53.8%) of respondents rated the psychological impact of the COVID-19 pandemic on wellbeing as moderate or severe; 16.5% of respondents had severe depression, and 28.8% had severe anxiety symptoms. Women and students had higher levels of stress, anxiety, and depression. Lower levels of stress, anxiety, and depression positively correlated with accurate health information about the COVID-19 epidemic.
In a large study group of 52,730 respondents from 36 provinces of China, Qiu et al. (37) evaluated the impact of stress amid COVID-19. Moderate stress was found in 29% of respondents, while 5% had severe stress intensity. Women had more severe stress than men. Furthermore, the subjects aged 18–30 and over 60 and higher education levels had greater stress intensity.
Another Chinese study of 600 general population during national quarantine (25) demonstrated that women had 3.01 times higher risk of anxiety than men. Respondents over 40 years of age had a lower risk of anxiety than people under 40. The risk of depression depended on the level of education.
Similar findings were reported (29) in a 603 randomly selected respondents study. Generalized anxiety had 34% of participants, and depressive disorders - in 18.1%-were more often observed respondents 35 years of age.
In an online survey from India, Roy et al. (3) assessed the level of anxiety and level of knowledge about the course of COVID-19 using. More than 80% of surveyed had a high level of anxiety. On the other hand, most of the respondents had a moderate level of knowledge about COVID-19 and a high level of knowledge about prevention.
In the current study, the severity of anxiety, stress, and depression was within normal ranges, and the respondents could be included in the group showing mildly severe social phobia (57.9 points). In addition, most respondents considered quarantine of people coming from abroad (63.4%), and cancellation of all mass events (59.1%) as the most effective actions in the fight against the spread of the coronavirus in Poland. Also, the respondents indicated keeping a safe distance between people in public space (68.3%), protective masks and gloves when leaving the house (60.4%), frequent washing of hands with soap (59.8%), the use of special disinfectants (57.3%) and avoiding public transport (43.3%).
In the present study, very common ways of behaving in a situation of forced quarantine were surfing the Internet (48.8%), mobilizing and trying to do everything to protect yourself from infection (42.7%), watching movies (39.6%), or reading (33.5%).
Heitzman (34) noted that people who test positive for the coronavirus, who are sick or quarantined, and their families would develop acute stress disorder symptoms (308.3, DSM-5) of the nature of distress.
In some countries, expert guidance was published at the pandemic's start. For example, the Korean Neuropsychiatric Association has published guidelines based on the assumption that quarantine induced by the COVID-19 epidemic may cause severe psychological effects in acute stress disorder, depression, post-traumatic stress disorder (PTSD), insomnia, irritability, and emotional exhaustion. The guidelines mention groups that are particularly vulnerable to the psychological consequences of quarantine. Experts include parents caring for children, young children, people quarantined after contact with COVID-19, doctors dealing with infected patients (38).
A study from Brazil (20), on 1,468 volunteers via an online survey, demonstrated that people who had to work outside live with an older adult have at least one common comorbid disease experienced more significant psychological discomfort and distress during the pandemic. Conversely, children's presence protected the subjects from depression.
It is impossible to compare the data to the norms as there are no standards for measuring quarantine response. Therefore, there is a need to understand the role of behavioral and psychosocial factors in predicting mental health in people in confinement and social isolation. Heitzman (34) notes that not everyone confronted with the pandemic will reveal post-traumatic psychiatric symptoms and will need psychological help and support from others. In the available works on the topics mentioned above, it was emphasized:
• the need for special care for vulnerable groups when planning preventive psychological interventions during the COVID-19 epidemic (37)
• the need to raise awareness of the psychological consequences of this COVID-19 pandemic and to intensify preventive measures to avoid long-term consequences (3)
• the need to support groups such as young people, the elderly, women, and migrants through the healthcare system, improving telemedicine and interventions during quarantine to prevent long-term consequences in the form of mental disorders (36)
• the need to identify the weakest people who may need the most help from health care systems, which seems particularly important as the human resources of psychologists or psychiatrists are limited and should be wisely (based on reliable parameters) used to fight the consequences of the COVID-19 pandemic (20)
• the need for the state to maintain access to assistance in the event of domestic violence, but also to prioritize the availability of childcare (36)
• that obtaining and relying on reliable information about an epidemic may reduce the intensity of the anxiety response, which is expected in the situation (38)
• when planning prophylaxis and interventions, one of at least six groups should be considered—healthcare professionals, people who have direct contact with patients, patients who refuse treatment, and people susceptible to infection (39).
It is well known that women were more likely to suffer from psychological stress than men. Females are more than twice as likely as males to be afflicted by mood disorders (40). This sex disparity indicates a potential role for gonadal hormones in the etiology of anxiety and depressive disorders. Women often experience anxiety, and depression during times of hormonal flux, such as puberty, menopause, perimenstrual and post-partum periods (41). According to Bucciarelli et al. (42), study gender represents a potential modifying factor in cardiovascular disease and depression and COVID-19 short- and long-term outcomes, particularly in cases involving long-term COVID complications. Results from emerging studies indicate that the COVID-19 pandemic affected male and female populations differently. Women seem to experience less severe short-term complications but suffer worse long-term COVID complications, including depression, reduced physical activity, and deteriorating lifestyle habits, all of which may impact cardiovascular risk. Mass-quarantine, self-quarantine, and isolation are associated with depression, anger, and chronic stress. The stressor factors suggested included longer quarantine duration, frustration, boredom, inadequate supplies, inadequate information, financial loss, and stigma (43).
Our current study has some potential limitations. First, the study group was too small to generalize the results to the entire population of people in Poland. Secondly, there was an overrepresentation of women in the studied subgroups. Hence the results should be verified in an equally numerous group of men. Nevertheless, despite these limitations, this study's results may provide a starting point for further research into the problems arising from quarantine.
Conclusions
1. Most respondents considered infection with COVID-19 to be a significant threat and feared another quarantine.
2. During quarantine, respondents most often experienced fatigue, a lack of energy, nervousness, anxiety, anger, and sadness.
3. Respondents demonstrated anxiety, stress, and depression severity in the normal range.
4. Respondents showed mildly severe social phobia.
5. Due to their frequent occurrence of anxiety disorders and depression, it is worth educating people on recognizing them to seek professional help in time (a psychologist, psychotherapist, or psychiatrist). It is important to disseminate the most important advice and tips of mental health experts during a pandemic among the public. TV and social media channels that fuel a spiral of anxiety and stress should be limited. Information should be sought from reliable sources. We have to try as much as possible to keep the current, personal way of spending time and the rhythm of the day. Do not give up on favorite activities and interests.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Bioethics Committee of the Medical University of Białystok-APK.002.33.2021. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
EK-K and AK-B designed the study and wrote the protocol. EK-K, AK-B, WK, GB, CŁ, NW, MC, AG, JF, PA, and MP data collection. WK undertook the statistical analysis. EK-K, AK-B, and GB wrote the first draft of the manuscript. All authors contributed to and have approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^Available online at: https://www.healthfocuspsychology.com.au/tools/dass-21/ (cited 29.12.2021).
References
1. Hossain MdM, Sultana A, Purohit N. Mental health outcomes of quarantine and isolation for infection prevention: a systematic umbrella review of the global evidence. Epidemiol Health. (2020) 42:e2020038. doi: 10.4178/epih.e2020038
2. Brooke J, Jackson D. Older people and COVID-19: isolation, risk and ageism. J Clin Nurs. (2020) 29:2044–6. doi: 10.1111/jocn.15274
3. Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr. (2020) 51:102083. doi: 10.1016/j.ajp.2020.102083
4. WHO. Considerations for Quarantine of Individuals in the Context of Containment for Coronavirus Disease (COVID-19): Interim Guidance, 19 March 2020 (WHO/2019-nCoV/IHR_Quarantine/2020.2). Geneva: World Health Organization (2020).
5. Norton PJ. Depression anxiety and stress scales (DASS): psychometric analysis across for racial groups. Anxiety Stress Coping. (2007) 20:253–65. doi: 10.1080/10615800701309279
6. Tanskanen J, Anttila T. A prospective study of social isolation, loneliness, and mortality in Finland. Am J Public Health. (2016) 106:2042–8. doi: 10.2105/AJPH.2016.303431
7. Valtorta N, Hanratty B. Loneliness, isolation and the health of older adults: do we need a new research agenda? J R Soc Med. (2012) 105:518–22. doi: 10.1258/jrsm.2012.120128
8. Sokół-Szawłowska M. Wpływ kwarantanny na zdrowie psychiczne podczas pandemii COVID-19 Psychiatry. (2021) 18:57–62. doi: 10.5603/PSYCH.a2020.0046
9. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
10. Ptacek R, Ptackova H, Martin A, Stefano GB. Psychiatric manifestations of COVID-19 and their social significance. Med Sci Monit. (2020) 26:e930340. doi: 10.12659/MSM.930340
11. Cénat JM, Blais-Rochette C, Kokou-Kpolou CK, Noorishad PG, Mukunzi JN, McIntee SE, et al. Prevalence of symptoms of depression, anxiety, insomnia, post-traumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. (2021) 295:113599. doi: 10.1016/j.psychres.2020.113599
12. Magnavita N, Chirico F, Garbarino S, Bragazzi NL, Santacroce E, Zaffina S. SARS/MERS/SARS-CoV-2 outbreaks and burnout syndrome among healthcare workers. An umbrella systematic review. Int J Environ Res Public Health. (2021) 18:4361. doi: 10.3390/ijerph18084361
13. Chirico F, Nucera G. An Italian experience of spirituality from the coronavirus pandemic. J Relig Health. (2020) 59:2193–5. doi: 10.1007/s10943-020-01036-1
14. Chirico F, Ferrari G, Nucera G, Szarpak L, Crescenzo P, Ilesanmi O. Prevalence of anxiety, depression, burnout syndrome, and mental health disorders among healthcare workers during the COVID-19 pandemic: A rapid umbrella review of systematic reviews. J Health Soc Sci. (2021) 6:209–20. doi: 10.19204/2021/prvl7
15. Logie CH, Turan JM. How do we balance tensions between COVID-19 public health responses and stigma mitigation? Learning from HIV research. AIDS Behav. (2020) 24:2003–6. doi: 10.1007/s10461-020-02856-8
16. Chirico F, Sacco A, Nucera G, Ferrari G, Vinci MR, Zaffina S, et al. Lockdown measures and COVID-19 related deaths during the first and second COVID-19 waves in Italy: a descriptive study. J Health Soc Sci. (2021) 6:379–90. doi: 10.19204/2021/lckd1
17. Lovibond PF, Lovibond SH. The structure negative emotional states: comparison of the depression anxiety stress scales (DASS) with Beck depression and anxiety inventories. Behav Res Ther. (1995) 33:335–43. doi: 10.1016/0005-7967(94)00075-U
18. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety & Stress Scales. 2nd ed. Sydney: Psychology Foundation (1995).
19. Liebowitz MR. Social Phobia. Mod Probl Pharmacopsychiatry. (1987) 22:141–73. doi: 10.1159/000414022
20. Rubin GJ, Wessely S. The psychological effects of quarantining a city. BMJ. (2020) 368:m313. doi: 10.1136/bmj.m313
21. Bonanno GA, Brewin C, Kaniast K, Greca A. Weighing the costs of disaster: consequences, risks, and resilience in individuals, families, and communities. PSPI. (2010) 11:1–49. doi: 10.1177/1529100610387086
22. Hamer K, Baran M, Marchlewska M, Kaniasty K. The influence of COVID19 pandemic on emotions, attitudes and behaviors of Poles - project, Wyd. SWPS. (2021). Available online at: https://iwahlab.com/news/iwahlab-in-a-project-the-influence-of-covid19-pandemic-on-emotions-attitudes-and-behaviors-of-poles (accessed December 29, 2021).
23. Van Bavel J, Baicker K, Boggio P, Capraro V, Cichocka A, Cikara M, et al. Using social and behavioural science to support COVID-19 pandemic response. Nat Hum Behav. (2020) 4:460–71. doi: 10.1038/s41562-020-0884-z
24. Wang Y, Di Yu, Ye J, Wei W. Study on the public psychological states and its related factors during the outbreak of coronavirus disease 2019 (COVID-19) in some regions of China. Psychol Health Med. (2020) 26:13–22. doi: 10.1080/13548506.2020.1746817
25. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. (2020) 288:112954. doi: 10.1016/j.psychres.2020.112954
26. Bai Y, Lin CC, Lin CY, Chen JY, Chue CM, et al. Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatr Serv. (2004) 55:1055–7. doi: 10.1176/appi.ps.55.9.1055
27. Cava MA, Fay KE, Beanlands HJ, McCay EA, Wignall R. The experience of quarantine for individuals affected by SARS in Toronto. Public Health Nurs. (2005) 22:398–406. doi: 10.1111/j.0737-1209.2005.220504.x
28. Desclaux A, Badji D, Ndione AG, Sow K. Accepted monitoring or endured quarantine? Ebola contacts' perceptions in Senegal. Soc Sci Med. (2017) 178:38–45. doi: 10.1016/j.socscimed.2017.02.009
29. Hawryluck L, Gold WL, Robinson S, Pogorski S, Galea S, Styra R, et al. SARS control and Psychological effects of quarantine, Toronto, Canada. Emerg Infect Dis. (2004) 10:1206–12. doi: 10.3201/eid1007.030703
30. Jeong H, Yim HW, Song Y-J, Ki M, Min JA, Cho J, et al. Mental health status of people isolated due to Middle East respiratory syndrome. Epidemiol Health. (2016) 38:e2016048 doi: 10.4178/epih.e2016048
31. Reynolds D, Garay J, Deamond SL, Moran MK, Gold W, Styra R. Understanding, compliance and psychological impact of the SARS quarantine experience. Epidemiol Infect. (2008) 136:997–1007. doi: 10.1017/S0950268807009156
32. Taylor MR, Agho KE, Stevens GJ, Raphael B. Factors influencing psychological distress during a disease epidemic: data from Australia's first outbreak of equine influenza. BMC Public Health. (2008) 8:347. doi: 10.1186/1471-2458-8-347
33. Wu P, Fang Y, Guan Z, Fan B, Kong J, Yao Z, et al. The psychological impact of the SARS epidemic on hospital employees in China: exposure, risk perception, and altruistic acceptance of risk. Can J Psychiatry. (2009) 54:302–11. doi: 10.1177/070674370905400504
34. Heitzman J. Wpływ pandemii COVID-19 na zdrowie psychiczne. Psychiatr Pol. (2020) 54:187–98. doi: 10.12740/PP/120373
35. Pierce M, Hope H, Ford T, Hatch S, Hotopf M, John A, et al. Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population. Lancet Psychiatry. (2020) 7:883–92. doi: 10.1016/S2215-0366(20)30308-4
36. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. doi: 10.3390/ijerph17051729
37. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y, et al. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatr. (2020) 33:e100213. doi: 10.1136/gpsych-2020-100213
38. Jung SJ, Jun JY. Mental health and psychological intervention amid COVID-19 outbreak: perspectives from South Korea. Yonsei Med J. (2020) 61:271–272. doi: 10.3349/ymj.2020.61.4.271
39. Dong Lu, Bouey J. Public mental health crisis during COVID-19 pandemic, China. Emerg Infect Dis. (2020) 26:1616–1618. doi: 10.3201/eid2607.200407
40. Bekker MH, van Mens-Verhulst J. Anxiety disorders: sex differences in prevalence, degree, and background, but gender-neutral treatment. Gend Med. (2007) 4 (Suppl. B):S178–93. doi: 10.1016/S1550-8579(07)80057-X
41. Douma SL, Husband C, O'Donnell ME, Barwin BN, Woodend AK. Estrogen-related mood disorders: reproductive life cycle factors. ANS Adv Nurs Sci. (2005) 28:364–75. doi: 10.1097/00012272-200510000-00008
42. Bucciarelli V, Nasi M, Bianco F, Seferovic J, Ivkovic V, Gallina S, et al. Depression pandemic and cardiovascular risk in the COVID-19 era and long COVID syndrome: gender makes a difference. Trends Cardiovasc Med. (2022) 32:12–7. doi: 10.1016/j.tcm.2021.09.009
Keywords: pandemic, COVID-19, quarantine, anxiety, stress, depression
Citation: Krajewska-Kułak E, Kułak-Bejda A, Kułak W, Bejda G, Łukaszuk C, Waszkiewicz N, Cybulski M, Guzowski A, Fiłon J, Aniśko P and Popławska M (2022) Well-Being at Home During Forced Quarantine Amid the COVID-19 Pandemic. Front. Psychiatry 13:846122. doi: 10.3389/fpsyt.2022.846122
Received: 30 December 2021; Accepted: 10 February 2022;
Published: 08 March 2022.
Edited by:
Xenia Gonda, Semmelweis University, HungaryReviewed by:
Francesco Chirico, Catholic University of the Sacred Heart, ItalyAnna Vittoria Mattioli, University of Modena and Reggio Emilia, Italy
Copyright © 2022 Krajewska-Kułak, Kułak-Bejda, Kułak, Bejda, Łukaszuk, Waszkiewicz, Cybulski, Guzowski, Fiłon, Aniśko and Popławska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Agnieszka Kułak-Bejda, YWduaWVzemthLmt1bGFrLmJlamRhQGdtYWlsLmNvbQ==