
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 22 July 2022
Sec. Psychopharmacology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.830301
This article is part of the Research Topic Therapeutic Use of Ketamine in Psychiatric Disorders View all 12 articles
 Marco Aurélio Cigognini*
Marco Aurélio Cigognini* Alia Garrudo GuiradoDenise van de MeeneMônica Andréia SchneiderMônica Sarah SalomonVinicius Santana de AlexandriaJuliana Pisseta AdrianoAna Maria ThalerFernando dos Santos Fernandes
Alia Garrudo GuiradoDenise van de MeeneMônica Andréia SchneiderMônica Sarah SalomonVinicius Santana de AlexandriaJuliana Pisseta AdrianoAna Maria ThalerFernando dos Santos Fernandes Adriana CarneiroRicardo Alberto Moreno
Adriana CarneiroRicardo Alberto MorenoObjective: Ketamine, an N-methyl D-aspartate (NMDA) receptor antagonist, can promote rapid action in the management of individuals with treatment-resistant depression (TRD) at sub-anesthetic doses. However, few studies have investigated the long-term use of ketamine administered intravenously (IV) and intranasally (IN). We report the design and rationale of a therapeutic trial for assessing the efficacy, safety, and tolerability of repeated-dose intramuscular (IM) ketamine vs. active treatment (escitalopram and aripiprazole) in TRD patients.
Methods: A comparative, parallel-group, randomized double-blind trial assessing the efficacy, safety, and tolerability of acute (4 weeks) and maintenance (24 weeks) use of IM ketamine (0.75 mg/kg) vs. active control (escitalopram 15 mg and aripiprazole 5 mg) in individuals with moderate-severe intensity TRD (no psychotic symptoms) with or without suicide risk will be conducted. Patients with TRD (18–40 years) will be randomized and blinded to receive ketamine IM or active treatment at a 1:1 ratio for 4 weeks (active treatment) and 24 weeks (maintenance treatment). Subjects will be assessed using clinical scales, monitored for vital signs (VS) after application of injectable medication, and undergo neuropsychological tests. The primary outcome will be changed on the Montgomery-Åsberg Depression Rating Scale (MADRS) during the course of the trial. The study is in running.
Results: This study can potentially yield evidence on the use of IM ketamine in the treatment of depressive disorders as an ultra-rapid low-cost therapy associated with less patient discomfort and reduced use of medical resources, and can elucidate long-term effects on different outcomes, such as neuropsychological aspects.
Conclusions: The trial can help promote the introduction of a novel accessible approach for the treatment of complex disease (TRD) and also allow refinement of its long-term use.
Clinical trial registration: https://clinicaltrials.gov/ct2/show/NCT04234776, identifier: NCT04234776.
In 2015, an estimated 300 million people had depression (4.4% of the world's population) (1). Depression is a common recurrent serious mental disorder associated with morbimortality and a burden of 50 million years lived with disability (YLD), constituting the mental disease with the highest global disability (2, 3). The economic impact of depression on productivity ran into billions of dollars (presenteeism and absenteeism) in terms of Gross National Product (GDP) (4). The disease is the largest contributor to suicide (some 800,000 deaths/year), a figure which is probably underestimated (5, 6).
Depressive disorders are heterogeneous diseases categorized by international systems of disease classification and whose treatment approaches are well-defined (7–10). However, only 1/3 of patients experience symptom remission after the first intervention (11, 12). Therapeutic goals have changed over time, and include symptoms remission, recovery of function, improvement in quality of life, and cognitive remission, as well as new antidepressants called “atypical”, have been developed in recent decades, such as duloxetine, agomelatine, vortioxetine, among others, in an attempt to optimize therapeutic results (13–15).
A number of definitions of treatment-resistant depression (TRD) exist, but there is a consensus on non-response after the use of 2 or more antidepressants of different classes (with adjustment of adherence, dose, and duration of use) (16, 17). Since the introduction of the concept in 1974, numerous studies have investigated treatment strategies adopting different definitions of the meaning of the illness (18). Treatment-resistant depression accounts for 12–20% of depressed patients and ~20% of TRD cases are staged as chronic, with various unfavorable clinical outcomes and both social and economic impacts (19–21).
Although numerous TRD treatment strategies exist, many interventions have limited efficacy, undesirable side effects and are high cost or inaccessible, besides presenting other barriers to implementation (22, 23). A new effective, less invasive treatment could significantly relieve the suffering and anguish of patients and their families compared to complex interventions for TRD, for example, neurostimulation treatments (24).
The clinical effects of ketamine involve anesthetic, analgesic, antidepressant, and anti-inflammatory actions (25). The drug is derived from phencyclidine and was developed in the 1960s (26). It has two enantiomers: S-ketamine and R-ketamine, with the racemic preparation containing concentrations of 1:1 (27). The drug undergoes hepatic biotransformation by the liver into different metabolites, norketamine being the most important, a product of demethylation by the P450 cytochrome that is excreted by the kidneys (28). Readily distributed by the tissues, including the brain, ketamine is very lipid soluble and exhibits plasma protein binding (12%) with a half-life of around 10 min (29). Ketamine is an N-methyl D-aspartate (NMDA) receptor antagonist with additional weaker actions on sigma receptors, as well as noradrenalin, serotonin, and dopamine transporters among others (30, 31). A signaling cascade may play a role in the regulation, and synaptic plasticity of the mammalian target of rapamycin (mTOR), and in mediating the rapid effects of ketamine (32). Effective, rapid antidepressant effects via non-conventional mechanisms represent one of the most important breakthroughs in the field of psychiatry over the last 50 years (33, 34).
Berman et al. carried out the first clinical trial using intravenous (IV) ketamine at a dose of 0.5 mg/kg in a small sample, observing a meaningful reduction on the Hamilton Depression Scale (HAM-D) after 3 days (35). Subsequently, a growing number of methodologically-refined studies (involving single IV applications) were conducted (36–39). A systematic review of 22 studies [randomized clinical trials (RCTs) and non-RCTs] involving 629 participants investigating the role of ketamine [IV 0.5 mg/kg for unipolar depression (UD) and bipolar depression (BD)] found a rapid effect in most of the studies reviewed, observing greatest magnitude of effect in RCTs at 210–230 min post-application (40). In another systematic review, McGirr et al. investigated the efficacy of ketamine (IV 0.5 mg/kg) in the treatment of depressive episodes of 73 individuals in parallel arms and 110 in cross-over designs (34 participants with BD and 149 with UD), where the primary outcome was clinical remission of symptoms at 24 h, 3 and 7 days vs. placebo: results at 24 h [Odds Ratio (OR) of 7.06 and number needed to treat (NNT) of 5], at 3 days (OR of 3.86 and NNT of 6) and, at 7 days (OR of 4 and NNT of 6) (41).
The strategy of repeated ketamine infusions has been explored over the past decade (24). Six 12-day infusions [10 patients (non-medicated)] with DRT who previously responded to 1 dose (MADRS ≥ 50%) had a mean (SD) reduction in scores after the last infusion of 85% (12%) (42). S-ketamine IV was administered to 6 depressed patients (6 infusions over 4 weeks) to investigate clinical efficacy (HAMD-21: after 120 min of application) obtaining scores from the first to the last measurement in 5 subjects of 19 → 11, 19 → 10, 35 → 25, 22 → 1, and 21 → 2 (43). Subjects with RDT (n = 24) undergoing up to 6 ketamine infusions (IV, 0.5 mg/kg, 3 times a week, 12 days) had a response rate of 70.8% with a mean decrease in score MADRS 2 h after the first infusion (18.9 ± 6.6; p < 0.001); sustained during applications (44). A multi-center, double-blind, randomized, placebo-controlled trial of ketamine (IV 0.5 mg/kg) 2 and 3 times weekly confirmed the efficacy of the 2 regimens, with mean change on the MADRS (baseline to day 15, vs. placebo groups [ketamine twice weekly: −18.4 (SD = 12.0); placebo: −5.7 (SD = 10.2); p < 0.001; ketamine 3 times weekly: −17.7 (SD = 7.3); placebo: −3.1 (SD = 5.7); p < 0.001] (45).
The safety of ketamine has been confirmed for some decades, with anesthetic doses of 4–5 mg/kg intramuscularly (IM) proving effective [93–100% of children (1,022 pediatric cases)] for airways, emesis, or agitation (46). In a small number of patients, the drug can temporarily affect heart rate, and blood pressure and promote myocardial ischemia, although these risks can be attenuated by the use of sub-anesthetic doses and careful patient selection (27, 41, 44, 47). Dissociative states, a common side effect of the drug, are transient (lasting ~40 min, 2 h after use) and are not associated with persistent psychosis or mood swings (48). Of 158 patients given ketamine, 21 (13.3%) withdrew from the study, compared to 10 (7.4%) out of the 135 patients receiving control interventions (OR 1.95, 95%CI 0.86–4.42, z = 1.59, p = 0.11) (39). Claims that NMDA receptor blocking can cause “brain damage” and that ketamine affects the urinary retract remain the subject of controversy (49). The most common (≥20%) adverse events following the use of the drug include, headache, anxiety, dissociation, nausea, dizziness, and drowsiness on days of the administration, with these effects dissipating within 2 h, while more serious side effects leading to hospitalization or suicide attempts are rare (40, 50, 51). Anti-depressant effects of ketamine are short-lived (days or weeks), although longer-term benefits can be maintained by use of repeat doses, warranting further studies on the prolonged effects of the drug (44, 52). Intranasal (IN) esketamine was approved for use in 2019 by both the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) (53). Other administration routes have also been investigated: IN, subcutaneous (SC), and oral (54–56).
With 93% bioavailability, the plasma concentration of IM ketamine is linear (mg/kg) (57, 58). A woman with depression and metastatic ovarian cancer experienced rapid remission (MADRS < 7) 1 h after receiving the first injection (1 mg/kg IM ketamine) (59). The same dosing repeated over 10 months (1× per week) kept MADRS scores low over the period (60). In 2 cases of bipolar depression with suicide risk, 4 applications of IM ketamine (0.75 mg) every 2 days, there was a reduction of 75.5%-83.3%-85.7% (case 1) and 71.4%-77.2%-60.8% (case 2) in the BDI, BAI, and BSI, respectively (61). Twenty-seven subjects in 3 parallel groups (9 subjects each) had ketamine administered IM and IV (G1 = 0.5 mg/kg IV, G = 0.5 mg/kg IM, and G3 = 0.25 mg/kg IM) with the HAM-D reduced by 58.86, 60.29, and 57.36%, respectively (62). IM ketamine has a recently similar response as potent ECT in 6–9 sessions for 3 weeks (HAM-D and BDI-suicide ideation) (63).
The anti-depressant efficacy of IM ketamine can offer several advantages: less cost (IN esketamine), less discomfort, ease of administration, and reduced reliance on the care team and resources than IV ketamine. The safety and tolerability of this route can provide greater accessibility and represent an adjunct in the treatment of depression and management of suicide risk. Although, the studies currently available on the IM route for ketamine are scarce and have methodological shortcomings: incipient samples, open studies, administration of few doses, subjective outcomes, no comparison with active substances, varying doses, case studies, etc. (59–64).
A comparative, parallel-group, randomized, double-blind trial is to be conducted involving an anti-depressant intervention. The experimental group (EG) will use the experimental substance [ketamine IM 0.75 mg/kg, oral placebo (morning), and oral placebo (evening)], while the control group (CG) will use an active treatment administered orally [escitalopram 15 mg (morning), aripiprazole 5 mg (evening) and placebo IM]. The study will be carried out by the Institute of Psychiatry of the University of São Paulo Medical School (HCFMUSP), in conjunction with the Center for Mind Health Studies (NUPE) in the Vale do Itajaí, Santa Catarina state, Brazil. The study is called the KETAMIM project and is Registered Under No. NCT04234776 on the www.ClinicalTrials.gov platform. The study phases and methodological aspects comply with the recommendations of the CONSORT (Consolidated Standard of Reporting Trials) statement and with Good Clinical Practice guidelines (GCP) (65, 66). The study is in running.
The study shall entail 5 phases: (1) Dissemination (P0): patients referred by health professionals, dissemination in the press or online media; (2) Pre-treatment (PI): ~2 weeks for the baseline assessment of candidates for study entry; (3) Therapeutic trial (PII): 4 weeks for ketamine use 3 times weekly and of daily oral medications, as well as placebos for both groups, characterizing acute treatment of the disease; (4) Maintenance (PIII): 24 weeks for weekly ketamine use and maintenance of standard treatment and respective placebos; (5) Post-treatment (PIV): 4 weeks for assessing patients after use of ketamine, maintenance oral medication or placebo.
A total of 88 patients with TRD (≥2 failed trials using anti-depressants, plus ECT as an alternative or otherwise) of moderate-severe intensity [according to criteria of Diagnostic and Statistical Manual of Mental Disorders (DSM-5)], and the diagnosis confirmed by the Portuguese version of the clinical interview of the DSM-IV, will be recruited (67). Patients will be block randomized using a computer-generated list into one of the two interventions (1:1 ratio), EG or CG (68). A nurse blinded to the allocation will administer ketamine or saline IM, placebo orally, or the active treatment, respectively.
The following individuals will be eligible for study inclusion: Subjects residing in Itajaí valley (Santa Catarina state, Brazil); adults (age 18–40 years) with a primary diagnosis of TRD based on clinical evaluation and confirmed by the SCID-IV [research version (TRD defined as failure of 2–5 clinical trials with anti-depressants including ECT)]; moderate-severe intensity disease [clinical criteria and/or score ≥14 on the Hamilton Depression Rating Scale (17-item HAM-D)]; with no psychotic symptoms; not presenting an imminent risk of suicide (as indicated by clinical evaluation and HAM-D) and/or murder; with anxiety disorders (secondary); with compensated clinical comorbidities and; literate and able to understand the tasks requested (69). Patients and/or legal guardians must be aware of the nature of the study and give consent by signing the Free and Informed Consent form. All patients will undergo a physical and neurological examination, laboratory tests, and an electrocardiogram (ECG) to ascertain their comorbid clinical and/or uncompensated conditions. The following individuals will be excluded from the study: Subjects exhibiting imminent risk of suicide, presenting bipolar spectrum disorders or other diagnosed psychiatric conditions (primary); psychoactive substance dependence within the last year; intellectual deficit; allergy to ketamine; and glaucoma. Fertile women must be in use of a clinically acceptable method of birth control [oral contraceptive and/or condom (only unfollowed topic in GCP)]. In the event of clinical doubt regarding pregnancy, a test for beta-human chorionic gonadotropin (βHCG) hormone will be ordered. Patients who become pregnant during the study period will be excluded and referred for obstetric care. The medication wash-out period required before visit 0 will be 1 week for antipsychotics, antidepressants [except fluoxetine (4 weeks)], and for mood stabilizers. No other medications with psychiatric action will be allowed during the study, except for Lorazepam and Zolpidem for patients in the use of a benzodiazepine or hypnotic agent.
The principal hypothesis of this study is that ketamine IM provides similar efficacy to active treatment in patients with TRD due to a comparison between the experimental intervention (ketamine IM) vs. active treatment (escitalopram and aripiprazole). Other objectives of the study include confirming the safety and tolerability of the use of ketamine IM during acute and maintenance treatment.
The study will assess (given in Table 1):
1) Sociodemographic variables: gender, marital status, ethnicity, number of children, income, education, and employment.
2) Clinical characteristics over the life course: clinical and psychiatric comorbidities, smoking, family history of mood disorders, prior pharmacological treatment and ECT, number of mood episodes, previous psychiatric admissions, suicide attempts, currently receiving psychotherapy, and history of sexual, or physical abuse.
3) Clinical history: visits to the emergency room, attempted suicides, or psychiatric hospitalizations.
4) The Montgomery-Åsberg Depression Rating Scale (MADRS) (70, 71): will be applied as a primary outcome measure 3× per week for the first month (PII), 1× per week for 6 months (PIII), and 1× per week (PIV) for 1 month.
5) The Hamilton Rating Scale for Depression (HAM-D) (72, 73): will be applied once in PI to assess symptom severity and again 3× per week for 1 month (PII), 1× per week for 6 months (PIII), and 1× per week (PIV) for 1 month.
6) Vital signs (VS): pulse oximetry, heart monitoring, breathing rate, heart rate, and blood pressure will be checked continuously using non-invasive methods. VS to be monitored 3× per week for the 1st month (PII) and 1× week (PIII) for 2 h continuously after completion of each application.
7) Global Clinical Impression (GCI) scale: this will be applied 3× a week for 1 month (PII), 1× week for 6 months (PIII), and 1× week (PIV) to assess disease severity, global improvement of the condition and hence, treatment efficacy (74).
8) Depression Thoughts Scale (DTS): the DTS will be applied at visit one (V-1), V11, and V-39 to assess for thought distortions (75, 76).
9) Clinician-Administered Dissociative States Scale (CADSS): this will provide a measure of the dissociative effects of ketamine and will be applied 3× per week for the 1st month (PII), and 1× per week for 6 months (PIII), ~1 h after application of injections (77).
10) Young's Mania Rating Scale (YMRS): this scale will be employed in this study to assess manic switching as an adverse effect of the medications and applied 3× week for the 1st month (PII) and 1× week for 6 months (PIII), ~1 h after application of injections (78).
11) Brief Psychiatric Rating Scale (BPRS): Sub-item 12 of the scale will be used for detecting the presence of psychotic symptoms arising after application of ketamine, applied 3× week for 1 month (PII) and 1× week (PIII), ~1 h after application of injections (79).
12) Udvalg Kliniske Undersoegelser Side Effect Rating Scale (UKU-SERS): this will be used to determine the presence of side effects of the medications used and will be applied 3× week for the 1st month (PII) and 1× week (PIII) thereafter, around 1 h after application of injections (79).
13) World Health Organization Quality of Life, brief version (WHOQOL-Bref): this scale will be applied at V-1, V-11, and V-35 (80).
14) Sheehan Disability Scale (SDS): this scale will be applied at V-1, V-11, and V-35 (81).
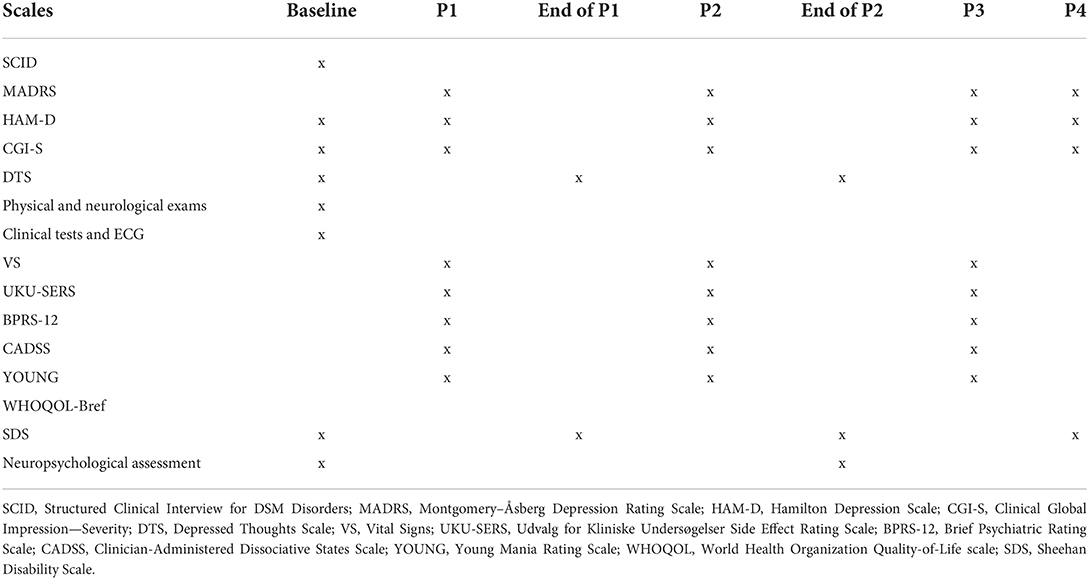
Table 1. Outcome measurements over time.
Randomization will be based on a computer-generated scheme, balanced by the use of randomly permutated blocks and stratified by the statistician of the Institute of Psychiatry of the FMUSP to receive ketamine IM or active treatment at a 1:1 ratio (82).
Two groups will be formed: a study group and an active control group. The study group will receive dextroketamine chloralhydrate IM (0.75 mg/kg) plus 2 placebo tablets orally, one in the morning and the other at night. The active control group will receive saline solution IM plus one of the alternative therapies for TRD: escitalopram 15 mg (morning) or aripiprazole 5 mg (night) (10). Injections will be applied alternately to gluteal muscles in the external upper quadrants. For 4 weeks (1 month), applications will be applied on Mondays, Wednesdays, and Fridays (giving a total of 12 interventions). For the ensuing 6 months, applications will be weekly (giving a total of 24 interventions). For 4 weeks (1 month), participants will continue to receive the tablets (active treatment or placebo) and be monitored. Safety parameters: vital signs will be monitored continuously by the researchers for 2 h post-application: fingertip pulse oximetry, heart rate, breathing rate, blood pressure, and electrocardiography. Abnormal blood pressure will be defined as low <90/60 mmHg and high >140/90 mmHg. Abnormal heart rate will be defined as <60 or >100 bpm. Abnormal breathing rate will be defined as <10 cycles/min or >20 cycles/min. Low oxygen saturation will be defined as levels <95%. Collateral symptoms such as nausea and vomiting will be managed using ondansetron 8 mg sublingually (SL). Individuals presenting episodes of anxiety, hallucinations, or intense dissociative effects will be given clonazepam SL 0.25 mg. An emergency team will be deployed in the event of serious acute events such as heart arrhythmia or prolonged hypertension. Patients will be placed under observation in a quiet comfortable environment and will be cleared to leave after 2 h, accompanied by a competent adult.
The researchers performing the clinical monitoring and application of the outcomes will be blinded, and the study participants will also be blinded. A nurse, not involved in data collection, will distribute the medications and apply the injections according to the randomization process.
The sample size was calculated based on a similarly designed RCT (45). Assuming a statistical power of 90% with a clinically significant minimum effect of 0.5 (Cohen's d) and alpha 5%, a total of 88 subjects will be needed (44 in the EG and 44 in the CG). Given this is a long-duration study, a drop-out rate of 10–20% was estimated.
All analyzes will be performed using the Statistical Package for the Social Sciences-SPSS® (82). Specific and sociodemographic variables will be expressed generally and between intervention groups in relative and absolute frequencies, means, medians, standard deviation, and 95% confidence interval. Continuous variables will be evaluated by the T-student or U-Mann Whitney-test according to their distribution and the qualitative ones by the X2-test. The distribution of variables will be evaluated using the Shapiro Wilk. The global significance level adopted is 0.05. To determine the effects of intervention throughout the study (main outcome and other scales), repeated measures ANOVA (two-way) will be applied, considering the temporal effect of visits (v-0 to v-final) and the intervention effect (EG × CG). In identifying the significant interaction effect, one-way repeated measures ANOVA test or its non-parametric alternative (Friedmann test) will be performed to verify that the effect is independent of treatment. Contingency tables and X2-tests will be applied to compare responders and non-responders in the intervention groups. Analysis using intent-to-treat (ITT) will be employed to assess the results (83). Vital signs will be assessed using two repeated measures ANOVA (two-way). First, considering the effect of the intervention immediately (3 evaluations at each visit) and the second, evaluating the effect of the intervention on VS over time (acute and maintenance treatment).
Neuropsychological tests will be applied at P0 and upon conclusion of PIII: to evaluate changes resulting from treatments:
(1) Digit span (subtest of Wechsler Intelligence Scale): measures attention span capacity and working memory; (2) Wisconsin Card Sorting Test-64: evaluate mental flexibility and ability to form abstract concepts in rapidly changing situations; (3) Stroop Color-Word Test (84): analyzes the maintenance of inhibitory control, from the suppression of the usual response in favor of an unusual response; (4) Wechsler Abbreviated Scale of Intelligence (WASI): the IQ is obtained from the sum of the gross results of the subtests converted to results weighted according to the individual's age (85); (5) Verbal Fluency Test: measures the ability to spontaneously produce words under semantic restriction and mind control (86); (6) Rey's Complex Figure: analyzes the visual-constructive ability, the ability to plan and problem-solving strategies (87) and; (7) Trail-Making Test: The purpose of this test is to assess alternate attention.
Subjects who meet one or more of the criteria outlined below will be withdrawn from the study:
1) Intolerance to medications;
2) Abnormal results on lab tests;
3) Serious adverse event;
4) The above-mentioned items will be assessed individually by the team according to medical criteria. Prolonged arterial hypertension, serious allergies, abnormal heart rate, or worsening of pre-existing diseases, among others, will be checked. Manic switching, imminent risk of suicide, attempted suicide, severe psychotic symptoms, aggressiveness, etc. will constitute grounds for study withdrawal.
5) Relapse or lack of response in Phases II or III. Lack of response will be defined as reduction or maintenance of scores on the index scale of ≤25%, whereas relapse will be the attainment of scores <50% in individuals who had achieved remission or response during the study.
6) Two consecutive visits missed;
7) Withdrawal of consent for the study.
Patients who discontinue the study shall be given guidance to continue outpatient psychiatric treatment.
We describe a protocol for an RCT to assess the efficacy, safety, and tolerability of ketamine vs. active treatment in the acute and maintenance stages of TRD. This study represents the first such trial with this design to date. A total of 12 applications of ketamine IM (0.75 mg/kg) will be administered in the active phase and 24 in the maintenance phase to volunteers randomized into the EG. The sample size for the study was determined by drawing on a similar study found in the literature. The objectives of the planned study, besides the primary outcome of improving symptoms (as measured by the MADRS), is to assess the safety (VS) and tolerability of ketamine at sub-anesthetic doses and side effects, such as the development of depressive thoughts, functioning, quality of life, and neuropsychological effects, in addition to evaluating treatment efficacy in the acute and maintenance phases. The anti-depressant effects of ketamine appear to be dose-dependent and over the last 20 years have been studied using “sub-anesthetic” doses (0.5–1 mg/kg) for the treatment of depression (51). For this trial, it was decided to use ketamine at a dose that lies in the middle of this range (0.75 mg/kg), together with an administration route (IM) that provides similar bioavailability as IV, the most studied route to date. Studies comparing the different routes for ketamine in depression remain incipient (58). Although TRD is an amalgam of modern psychiatry, the impact of the disease and its myriad symptoms remain a major public health problem (19, 20). The issues involved in the efficacy and safety of ketamine IM include the wide use and accessibility of this low-cost substance, known to medicine for decades, yet lacking a clear prescription in current guidelines. The rapid anti-depressant and anti-suicidal action of the drug, together with its glutamatergic neurotransmitter regulation, has led to the recognition of ketamine as a new paradigm in modern psychiatry (34). Patients with compensated clinical comorbidities are to be included in the sample, conferring greater external validity to the findings. The study described must be interpreted according to its limitations regarding generalization of results: sample size, criteria for eligibility (exclusion of individuals with other decompensated psychiatric and clinical comorbidities). Difficulties blinding to ketamine given its dissociative effects, despite the various measures taken to safeguard this bias, may constitute a further limitation.
The study will investigate the efficacy, safety, and tolerability of the use of ketamine IM in the treatment of TRD via a double-blind, parallel-group randomized, placebo-controlled trial. Clinical information, monitoring to control vital signs and standardized scales will help further understanding of the relationship of the disease with ketamine use. Future studies investigating the potential benefits of repeated ketamine infusions, non-parenteral administration alternatives, the safety of long-term use, reduced potential for abuse, and alternatives with fewer systemic effects can contribute to the management of TRD, a chronic and complex disease.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Research Ethics Committee of the University of São Paulo (Permit No. 2.530.851). The patients/participants provided their written informed consent to participate in this study.
Study conception and design: MC, FF, AC, and RM. Drafting of the manuscript: MC and RM. Statistic review: AG. Study execution: MC, DM, MAS, MSS, VA, JA, and AT. All authors contributed to the article and approved the submitted version.
This work was supported by Research Support Fund (Institute and Department of Psychiatry).
The authors extend thanks to the CLAVE Institute for granting the use of their infrastructure to carry out this study: rooms for consultations and procedures.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. Geneva: World Health Organization (2017).
2. Kessler RC, Bromet EJ. The epidemiology of depression across cultures. Annu Rev Public Health. (2013) 34:119–38. doi: 10.1146/annurev-publhealth-031912-114409
3. GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. (2016) 388:1545–602. doi: 10.1016/S0140-6736(16)31678-6
4. Evans-Lacko S, Knapp M. Global patterns of workplace productivity for people with depression: absenteeism and presenteeism costs across eight diverse countries. Soc Psychiatry Psychiatr Epidemiol. (2016) 51:1525–37. doi: 10.1007/s00127-016-1278-4
5. World Health Organization. Preventing Suicide: A Global Imperative. Geneva: World Health Organization (2014).
6. Rihmer Z, Gonda X. Pharmacological prevention of suicide in patients with major mood disorders. Neurosci Biobehav Rev. (2013) 37:2398–403. doi: 10.1016/j.neubiorev.2012.09.009
7. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders-5. Washington, DC: American Psychiatric Association (2013).
8. World Health Organization. International Classification of Diseases, 11th Revision (ICD-11). Geneva: World Health Organization (2018).
9. Millan MJ, Goodwin GM, Meyer-Lindenberg A, Ove Ögren S. Learning from the past and looking to the future: emerging perspectives for improving the treatment of psychiatric disorders. Eur Neuropsychopharmacol. (2015) 25:599–656. doi: 10.1016/j.euroneuro.2015.01.016
10. Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, Bhat V, Blier P, et al. Canadian network for mood and anxiety treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 3. Pharmacol Treat Can J Psychiatry. (2016) 61:540–60. doi: 10.1177/0706743716659417
11. Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. (2006) 163:1905–17. doi: 10.1176/ajp.2006.163.11.1905
12. Rush AJ, Trivedi MH, Stewart JW, Nierenberg AA, Fava M, Kurian BT, et al. Combining medications to enhance depression outcomes (CO-MED): acute and long-term outcomes of a single-blind randomized study. Am J Psychiatry. (2011) 168:689–701. doi: 10.1176/appi.ajp.2011.10111645
13. McIntyre RS. Using measurement strategies to identify and monitor residual symptoms. J Clin Psychiatry. (2013) 74:14–8. doi: 10.4088/JCP.12084su1c.03
14. Pompili M, Serafini G, Innamorati M, Venturini P, Fusar-Poli P, Sher L, et al. Agomelatine, a novel intriguing antidepressant option enhancing neuroplasticity: a critical review. World J Biol Psychiatry. (2013) 14:412–31. doi: 10.3109/15622975.2013.765593
15. Girardi P, Pompili M, Innamorati M, Mancini M, Serafini G, Mazzarini L, et al. Duloxetine in acute major depression: review of comparisons to placebo and standard antidepressants using dissimilar methods. Hum Psychopharmacol. (2009) 24:177–90. doi: 10.1002/hup.1005
16. Berlim MT, Turecki G. Definition, assessment, and staging of treatment-resistant refractory major depression: a review of current concepts and methods. Can J Psychiatry. (2007) 52:46–54. doi: 10.1177/070674370705200108
17. Bennabi D, Aouizerate B, El-Hage W, Doumy O, Moliere F, Courtet P, et al. Risk factors for treatment resistance in unipolar depression: a systematic review. J Affect Disord. (2015) 171:137–41. doi: 10.1016/j.jad.2014.09.020
18. Ruhé HG, van Rooijen G, Spijker J, Peeters FP, Schene AH. Staging methods for treatment resistant depression. A systematic review. J Affect Disord. (2012) 137:35–45. doi: 10.1016/j.jad.2011.02.020
19. McIntyre RS, Filteau MJ, Martin L, Patry S, Carvalho A, Cha DS, et al. Treatment-resistant depression: definitions, review of the evidence, and algorithmic approach. J Affect Disord. (2014) 156:1–7. doi: 10.1016/j.jad.2013.10.043
20. Mrazek DA, Hornberger JC, Altar CA, Degtiar I. A review of the clinical, economic, and societal burden of treatment-resistant depression: 1996-2013. Psychiatr Serv. (2014) 65:977–87. doi: 10.1176/appi.ps.201300059
21. Lepine BA, Moreno RA, Campos RN, Couttolenc BF. Treatment-resistant depression increases health costs and resource utilization. Braz J Psychiatry. (2012) 34:379–88. doi: 10.1016/j.rbp.2012.05.009
23. Philip NS, Carpenter LL, Tyrka AR, Price LH. Pharmacologic approaches to treatment resistant depression: a re-examination for the modern era. Expert Opin Pharmacother. (2010) 11:709–22. doi: 10.1517/14656561003614781
24. Szymkowicz SM, Finnegan N, Dale RM. A 12-month naturalistic observation of three patients receiving repeat intravenous ketamine infusions for their treatment-resistant depression. J Affect Disord. (2013) 147:416–20. doi: 10.1016/j.jad.2012.10.015
25. Zanos P, Moaddel R, Morris PJ, Riggs LM, Highland JN, Georgiou P, et al. Ketamine and ketamine metabolite pharmacology: insights into therapeutic mechanisms. Pharmacol Rev. (2018) 70:621–60. doi: 10.1124/pr.117.015198
26. Hillhouse TM, Porter JH. A brief history of the development of antidepressant drugs: from monoamines to glutamate. Exp Clin Psychopharmacol. (2015) 23:1–21. doi: 10.1037/a0038550
27. Reich DL, Silvay G. Ketamine: an update on the first twenty-five years of clinical experience. Can J Anaesth. (1989) 36:186–97. doi: 10.1007/BF03011442
28. Zarate CA Jr, Brutsche N, Laje G, Luckenbaugh DA, Venkata SL, Ramamoorthy A, et al. Relationship of ketamine's plasma metabolites with response, diagnosis, and side effects in major depression. Biol Psychiatry. (2012) 72:331–8. doi: 10.1016/j.biopsych.2012.03.004
29. Haas DA, Harper DG. Ketamine: a review of its pharmacologic properties and use in ambulatory anesthesia. Anesth Prog. (1992) 39:61–8.
30. Andrade C. Ketamine for depression, 3: does chirality matter? J Clin Psychiatry. (2017) 78:e674–7. doi: 10.4088/JCP.17f11681
31. Stahl SM. Mechanism of action of ketamine. CNS Spectr. (2013) 18:171–4. doi: 10.1017/S109285291300045X
32. Dwyer JM, Duman RS. Activation of mammalian target of rapamycin and synaptogenesis: role in the actions of rapid-acting antidepressants. Biol Psychiatry. (2013) 73:1189–98. doi: 10.1016/j.biopsych.2012.11.011
33. Li N, Liu RJ, Dwyer JM, Banasr M, Lee B, Son H, et al. Glutamate N-methyl-D-aspartate receptor antagonists rapidly reverse behavioral and synaptic deficits caused by chronic stress exposure. Biol Psychiatry. (2011) 69:754–61. doi: 10.1016/j.biopsych.2010.12.015
34. Zarate C, Duman RS, Liu G, Sartori S, Quiroz J, Murck H. New paradigms for treatment-resistant depression. Ann N Y Acad Sci. (2013) 1292:21–31. doi: 10.1111/nyas.12223
35. Berman RM, Cappiello A, Anand A, Oren DA, Heninger GR, Charney DS, et al. Antidepressant effects of ketamine in depressed patients. Biol Psychiatry. (2000) 47:351–4. doi: 10.1016/S0006-3223(99)00230-9
36. Diazgranados N, Ibrahim L, Brutsche NE, Newberg A, Kronstein P, Khalife S, et al. A randomized add-on trial of an N-methyl-D-aspartate antagonist in treatment-resistant bipolar depression. Arch Gen Psychiatry. (2010) 67:793–802. doi: 10.1001/archgenpsychiatry.2010.90
37. Zarate CA Jr., Brutsche NE, Ibrahim L, Franco-Chaves J, Diazgranados N, Cravchik A, et al. Replication of ketamine's antidepressant efficacy in bipolar depression: a randomized controlled add-on trial. Biol Psychiatry. (2012) 71:939–46. doi: 10.1016/j.biopsych.2011.12.010
38. Sos P, Klirova M, Novak T, Kohutova B, Horacek J, Palenicek T. Relationship of ketamine's antidepressant and psychotomimetic effects in unipolar depression. Neuro Endocrinol Lett. (2013) 34:287–93.
39. Murrough JW, Iosifescu DV, Chang LC, Al Jurdi RK, Green CE, Perez AM, et al. Antidepressant efficacy of ketamine in treatment-resistant major depression: a two-site randomized controlled trial. Am J Psychiatry. (2013) 170:1134–42. doi: 10.1176/appi.ajp.2013.13030392
40. Caddy C, Giaroli G, White TP, Shergill SS, Tracy DK. Ketamine as the prototype glutamatergic antidepressant: pharmacodynamic actions, and a systematic review and meta-analysis of efficacy. Ther Adv Psychopharmacol. (2014) 4:75–99. doi: 10.1177/2045125313507739
41. McGirr A, Berlim MT, Bond DJ, Fleck MP, Yatham LN, Lam RW, et al. systematic review and meta-analysis of randomized, double-blind, placebo-controlled trials of ketamine in the rapid treatment of major depressive episodes. Psychol Med. (2015) 45:693–704. doi: 10.1017/S0033291714001603
42. aan het Rot M, Collins KA, Murrough JW, Perez AM, Reich DL, Charney DS, et al. Safety and efficacy of repeated-dose intravenous ketamine for treatment-resistant depression. Biol Psychiatry. (2010) 15:139–45. doi: 10.1016/j.biopsych.2009.08.038
43. Segmiller F, Rüther T, Linhardt A, Padberg F, Berger M, Pogarell O, et al. Repeated S-ketamine infusions in therapy resistant depression: a case series. J Clin Pharmacol. (2013) 53:996–8. doi: 10.1002/jcph.122
44. Shiroma PR, Johns B, Kuskowski M, Wels J, Thuras P, Albott CS, et al. Augmentation of response and remission to serial intravenous subanesthetic ketamine in treatment resistant depression. J Affect Disord. (2014) 155:123–9. doi: 10.1016/j.jad.2013.10.036
45. Singh JB, Fedgchin M, Daly EJ, De Boer P, Cooper K, Lim P, et al. A double-blind, randomized, placebo-controlled, dose-frequency study of intravenous ketamine in patients with treatment-resistant depression. Am J Psychiatry. (2016) 173:816–26. doi: 10.1176/appi.ajp.2016.16010037
46. Green SM, Hummel CB, Wittlake WA, Rothrock SG, Hopkins GA, Garrett W. What is the optimal dose of intramuscular ketamine for pediatric sedation? Acad Emerg Med. (1999) 6:21–6. doi: 10.1111/j.1553-2712.1999.tb00089.x
47. Jin JF, Zhu LL, Chen M, Xu HM, Wang HF, Feng XQ, et al. The optimal choice of medication administration route regarding intravenous, intramuscular, and subcutaneous injection. Patient Prefer Adherence. (2015) 9:923–42. doi: 10.2147/PPA.S87271
48. Luckenbaugh DA, Niciu MJ, Ionescu DF, Nolan NM, Richards EM, Brutsche NE, et al. Do the dissociative side effects of ketamine mediate its antidepressant effects? J Affect Disord. (2014) 159:56–61. doi: 10.1016/j.jad.2014.02.017
49. Rasmussen KG. Has psychiatry tamed the “ketamine tiger?” Considerations on its use for depression and anxiety. Prog Neuropsychopharmacol Biol Psychiatry. (2016) 64:218–24. doi: 10.1016/j.pnpbp.2015.01.002
50. Daly EJ, Singh JB, Fedgchin M, Cooper K, Lim P, Shelton RC, et al. Efficacy and safety of intranasal esketamine adjunctive to oral antidepressant therapy in treatment-resistant depression: a randomized clinical trial. JAMA Psychiatry. (2018) 75:139–48. doi: 10.1001/jamapsychiatry.2017.3739
51. Memon RI, Naveed S, Faquih AE, Fida A, Abbas N, Chaudhary AMD, et al. Effectiveness and safety of ketamine for unipolar depression: a systematic review. Psychiatr Q. (2020) 91:1147–92. doi: 10.1007/s11126-020-09830-6
52. Murrough JW, Perez AM, Pillemer S, Stern J, Parides MK, aan het Rot M, et al. Rapid and longer-term antidepressant effects of repeated ketamine infusions in treatment-resistant major depression. Biol Psychiatry. (2013) 74:250–6. doi: 10.1016/j.biopsych.2012.06.022
53. McIntyre RS, Rosenblat JD, Nemeroff CB, Sanacora G, Murrough JW, Berk M, et al. Synthesizing the evidence for ketamine and esketamine in treatment-resistant depression: an international expert opinion on the available evidence and implementation. Am J Psychiatry. (2021) 178:383–99. doi: 10.1176/appi.ajp.2020.20081251
54. Lapidus KA, Levitch CF, Perez AM, Brallier JW, Parides MK, Soleimani L, et al. A randomized controlled trial of intranasal ketamine in major depressive disorder. Biol Psychiatry. (2014) 76:970–6. doi: 10.1016/j.biopsych.2014.03.026
55. Arabzadeh S, Hakkikazazi E, Shahmansouri N, Tafakhori A, Ghajar A, Jafarinia M, et al. Does oral administration of ketamine accelerate response to treatment in major depressive disorder? Results of a double-blind controlled trial. J Affect Disord. (2018) 235:236–41. doi: 10.1016/j.jad.2018.02.056
56. Cavenaghi VB, da Costa LP, Lacerda ALT, Hirata ES, Miguel EC, Fraguas R. Subcutaneous ketamine in depression: a systematic review. Front Psychiatry. (2021) 12:513068. doi: 10.3389/fpsyt.2021.513068
57. Grant IS, Nimmo WS, Clements JA. Pharmacokinetics and analgesic effects of im and oral ketamine. Br J Anaesth. (1981) 53:805–10. doi: 10.1093/bja/53.8.805
58. Loo CK, Gálvez V, O'Keefe E, Mitchell PB, Hadzi-Pavlovic D, Leyden J, et al. Placebo-controlled pilot trial testing dose titration and intravenous, intramuscular and subcutaneous routes for ketamine in depression. Acta Psychiatr Scand. (2016) 134:48–56. doi: 10.1111/acps.12572
59. Zanicotti CG, Perez D, Glue P. Mood and pain responses to repeat dose intramuscular ketamine in a depressed patient with advanced cancer. J Palliat Med. (2012) 15:400–3. doi: 10.1089/jpm.2011.0314
60. Grott Zanicotti C, Perez D, Glue P. Case report: long-term mood response to repeat dose intramuscular ketamine in a depressed patient with advanced cancer. J Palliat Med. (2013) 16:719–20. doi: 10.1089/jpm.2013.0057
61. Cigognini MA, Moreno RA. Intramuscular ketamine in depression, suicidal thoughts and anxiety: a report on two case. Eur Psychiatry. (2017) 41:S420. doi: 10.1016/j.eurpsy.2017.01.378
62. Chilukuri H, Reddy NP, Pathapati RM, Manu AN, Jollu S, Shaik AB. Acute antidepressant effects of intramuscular versus intravenous ketamine. Indian J Psychol Med. (2014) 36:71–6. doi: 10.4103/0253-7176.127258
63. Kheirabadi D, Kheirabadi GR, Mirlohi Z, Tarrahi MJ, Norbaksh A. Comparison of Rapid antidepressant and antisuicidal effects of intramuscular ketamine, oral ketamine, and electroconvulsive therapy in patients with major depressive disorder: a pilot study. J Clin Psychopharmacol. (2020) 40:588–93. doi: 10.1097/JCP.0000000000001289
64. Harihar H, Dasari P, Srinivas JS. Intramuscular ketamine in acute depression: a report on two cases. Indian J Psychiatry. (2013) 55:186–8. doi: 10.4103/0019-5545.111461
65. Moher D, Schulz KF, Altman DG. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomized trials. Lancet. (2001) 357:1191–4. doi: 10.1016/S0140-6736(00)04337-3
66. European Medicines Agency. Guideline for Good Clinical Practice E6(R2). London: European Medicines Agency (2018). p. 1–68.
67. Del-Ben CM, Vilela JAA, Crippa JADS, et al. Confiabilidade da Entrevista Clínica Estruturada para o DSM-IV: versão clínica traduzida para o português. Braz J Psychiatry. (2001) 23:156–9. doi: 10.1590/S1516-44462001000300008
68. Schulz KF, Grimes DA. Allocation concealment in randomized trials: defending against deciphering. Lancet (2002); 359: 614–618. doi: 10.1016/S0140-6736(02)07750-4
69. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. (1960) 23:56–62. doi: 10.1136/jnnp.23.1.56
70. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. (1979) 134:382–9. doi: 10.1192/bjp.134.4.382
71. Fernandes F, Carneiro A, Campos RN. Soeiro-de-Souza MG, Barros VB, Moreno RA. SIGMA-VB: validity and reliability of the Brazilian Portuguese version of the Montgomery-Åsberg Depression Rating Scale using the Structured Interview Guide for the MADRS. Braz J Psychiatry. (2019) 41:297–302. doi: 10.1590/1516-4446-2018-0105
72. Freire MA, de Figueiredo VLM, Gomide A, et al. Hamilton Scale: a study of the psychometric characteristics in a sample from Southern Brazil. J Bras Psiquiatr. (2014) 63:281–9. doi: 10.1590/0047-2085000000036
73. Carneiro AM, Fernandes F, Moreno RA. Hamilton depression rating scale and montgomery-asberg depression rating scale in depressed and bipolar I patients: psychometric properties in a Brazilian sample. Health Qual Life Outcomes. (2015) 13:1–8. doi: 10.1186/s12955-015-0235-3
74. Busner J. Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry. (2007) 4:28–37.
75. Carneiro AM, e Baptista MN. Desenvolvimento e propriedades psicométricas da Escala de Pensamentos Depressivos – EPD. Revista Brasileira de Terapias Cognitivas. (2012) 8:74–84. doi: 10.5935/1808-5687.20120012
76. Carneiro AM, Baptista MN, Moreno RA. Depression thoughts scale: association with depression rating scales. J Depress Anxiety. (2014) 3:1–6.
77. Bremner JD, Krystal JH, Putnam FW, Southwick SM, Marmar C, Charney DS, et al. Measurement of dissociative states with the Clinician-Administered Dissociative States Scale (CADSS). J Trauma Stress. (1998) 11:125–36. doi: 10.1023/A:1024465317902
78. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
79. Overall JE, Gorham DR. The brief psychiatry rating scale. Psychol Rep. (1962) 10:799–812. doi: 10.2466/pr0.1962.10.3.799
80. Fleck MP, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Application of the Portuguese version of the abbreviated instrument of quality life WHOQOL-bref. Rev Saude Publica. (2000) 34:178–83. doi: 10.1590/S0034-89102000000200012
81. Sheehan DV, Harnett-Sheehan K, Raj BA. The measurement of disability. Int Clin Psychopharmacol. (1996) 11:89–95. doi: 10.1097/00004850-199606003-00015
83. Soares I, Carneiro AV. Intention-to-treat analysis in clinical trials: principles and practical importance. Rev Port Cardiol. (2002) 21:1191–8.
84. Regard M. Cognitive rigidity and flexibility: a neuropsychological study. A Compendium of neuropsychological tests. Oxford: Oxford University Press (1998).
85. Wechsler D. Wechsler Abbreviated Scale of Intelligence. New York, NY: Psychological Corporation (1999).
Keywords: ketamine, treatment-resistant depression, N-methyl-D-aspartate receptor antagonist, randomized clinical trial, intramuscular (IM)
Citation: Cigognini MA, Guirado AG, Meene D, Schneider MA, Salomon MS, Alexandria VS, Adriano JP, Thaler AM, Fernandes FS, Carneiro A and Moreno RA (2022) Intramuscular ketamine vs. escitalopram and aripiprazole in acute and maintenance treatment of patients with treatment-resistant depression: A randomized double-blind clinical trial. Front. Psychiatry 13:830301. doi: 10.3389/fpsyt.2022.830301
Received: 07 December 2021; Accepted: 04 July 2022;
Published: 22 July 2022.
Edited by:
Celia J. A. Morgan, University of Exeter, United KingdomReviewed by:
Gianluca Serafini, San Martino Hospital (IRCCS), ItalyCopyright © 2022 Cigognini, Guirado, Meene, Schneider, Salomon, Alexandria, Adriano, Thaler, Fernandes, Carneiro and Moreno. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marco Aurélio Cigognini, bWFyY28uY2lnb2duaW5pQHVzcC5icg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.