
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychiatry, 16 August 2022
Sec. Social Psychiatry and Psychiatric Rehabilitation
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.807140
This article is part of the Research TopicInsights in Social Psychiatry and Psychiatric Rehabilitation: 2021View all 8 articles
 Christina Ziebart1,2*
Christina Ziebart1,2* Pavlos Bobos2,3,4
Pavlos Bobos2,3,4 Joy C. MacDermid1,2,5
Joy C. MacDermid1,2,5 Rochelle Furtado1,2
Rochelle Furtado1,2 Daniel J. Sobczak6Michele Doering6
Daniel J. Sobczak6Michele Doering6Background: Treatment of psychosis typically focuses on medication, but some of these medications can have unintended side effects, exercise has global health benefits, with minimal side effects. The purpose of this systematic review and meta-analysis is to investigate the effectiveness and safety of exercise and physical activity on psychotic symptoms, in people with psychosis when compared to usual care, in a hospital setting.
Methods: A systematic electronic search of the literature was performed in June 2022, in PubMed, Scopus, and PsychINFO with no date restrictions. We included randomized trials (RCTs) with patients with psychosis that received an exercise intervention within a hospital setting. The primary outcome of interest was Positive and Negative Symptom Severity Scale (PANSS) overall score. Secondary outcomes were adverse or serious adverse events.
Results: A total of 24 trials were included in this systematic review, with 9 included in the meta-analysis, including 1,426 participants. Aerobic had more pronounced effects when compared to usual care in PANSS positive (−0.23, 95% CI −0.53 to 0.07), negative (−0.38, 95% CI −0.65 to −0.10), general (−0.42, 95% CI −0.71 to −0.13) and overall scores (−0.25, 95% CI −0.52 to 0.03). Yoga when compared to usual care had no difference in PANSS subscale and overall scores. We found no difference on relapsing of psychiatric symptoms or somatic hospitalization when we compared aerobic or yoga to usual care (Risk Ratio, 1.12 95% CI 0.44–2.81).
Conclusion: Aerobic activity as an exercise modality in a hospital setting can be effective in decreasing negative and general psychosis symptom severity scores compared to usual care, however, it was uncertain if the effects were clinically important. More trials are needed to confirm the clinically benefit of aerobic exercise.
Systematic Review Registration: [https://www.crd.york.ac.uk/prospero/], identifier [CRD42021224997].
Psychosis can be part of a variety of conditions including, but not limited to, schizophrenia, schizoaffective disorder, bipolar disorder and major depressive disorder (1). Schizophrenia affects approximately 24 million people worldwide and is characterized by positive symptoms such as hallucinations and delusions, negative symptoms including alogia and avolition, and neurocognitive deficits including perception, memory, and attention (2, 3). Worse negative symptoms and cognitive decline are associated with poor functional outcomes (2, 3). Although antipsychotic medication can help to manage some of the symptoms, they may not be able to address all the symptoms, and the patient still may relapse, or the medication may not have a lasting effect (4).
Typically, medication can help to manage the positive symptoms (hallucinations, delusions, confused thoughts or disorganized speech, trouble concentrating, or movement disorders), but not the negative symptoms (having a lack of pleasure, not talking much or showing much emotion, withdrawal or struggling to keep up with daily activities like bathing) (5, 6). Antipsychotic medications can also have unintended side effects, for example, weight gain and metabolic syndrome (which is a cluster of health conditions that can increase the risk of heart attack, stroke, and diabetes) (5, 6). As part of the clinical practice guidelines for the treatment of patients with schizophrenia, an initial assessment should include a physical health assessment, among assessing substance use, trauma history, risk of suicide and aggressive behavior and patient’s goals and preferences for treatment (7).
The clinical practice guidelines recommend both pharmacotherapy and psychotherapy as intervention strategies to manage schizophrenia (7). The guidelines emphasize that the first episode of psychosis be treated in a coordinated specialty care program (7). The guidelines do not specify exercise, but other literature indicates a value to integrating exercise early in the treatment of psychosis.
Physical activity and exercise are one treatment strategy used to manage side effects such as weight gain and metabolic syndrome as well as the primary cognitive, negative, and positive symptoms associated with psychosis (5, 6). In a study by Damme et al. (8) the group with high risk for psychosis had significantly lower VO2max than the healthy controls (8), however, this relationship may be confounded by body mass index (BMI) (9). Recent systematic reviews have looked at the effect of exercise and physical activity as a treatment strategy for people with psychosis (10–13). Exercise was found to be superior to usual care when it comes to improving total symptom severity as assessed by the Positive And Negative Symptom Severity scale (PANSS), cardiorespiratory function, depression, aerobic capacity, quality of life, and psychosocial stressors (10–12).
Exercise and physical activity may be one strategy to improve function and address psychotic symptoms in individuals in hospitals; however, the American Psychiatric Association highlighted a need for more research on patient-centered outcomes which includes physical health, determine the optimal setting of care and the optimal approaches to recovery (14). Therefore, the purpose of this systematic review and meta-analysis was to investigate the effectiveness of exercise and physical activity on psychotic symptoms in people with psychosis in a hospital setting when compared to usual care.
We used the guidelines from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Cochrane collaboration guidelines for this systematic review and meta-analysis (15).
Studies were included in this review if the following criteria were met:
• Design: randomized controlled trial (RCT)
• Participants: Adults with psychosis in a hospital setting
• Intervention: Any form of exercise or physical activity
• Comparison: Usual care, other forms of exercise, self-directed care, treatment with another healthcare professional
• Outcomes: Psychosis symptom severity scores
Studies that were not written in English, were in a community setting or had no full text available were excluded from this systematic review explanation of excluded studies can be found in the Supplementary material. This review has been registered on PROSPERO: CRD42021224997.
A systematic electronic search of the literature was performed in November 2020, and updated in June 2022, in PubMed, Scopus, and PsychINFO with no date restrictions. The following key words were used to identify potentially relevant studies: “schizophrenia,” “bipolar,” “psychosis,” “exercise,” “exercise therapy,” “physical activity,” “randomized controlled trials,” “RCT.” In addition, we conducted a manual search of the reference lists of the included studies to identify any potential studies missed in the electronic search. The complete search strategy is summarized in Supplementary Figures 1–3.
The selection of individual studies involved three independent reviewers (CZ, RF, and PB) who performed the systematic electronic search of the databases. Two reviewers (CZ and PB) identified potentially relevant articles, removed duplicates, and then screened titles and abstracts. The full text of any study marked include or uncertain was obtained and the eligibility criteria were applied.
Three independent researchers (CZ, RF, and PB) extracted the data from the eligible included studies. Data extraction included: study, author, year, sample characteristics, intervention, comparison groups, PANSS score (overall as well as subscales) and adverse or serious adverse events.
Two independent review authors (CZ and PB) assessed the included RCTs for risk of bias (ROB). The ROB assessment was performed using the Cochrane Risk of Bias tool (16). The Cochrane ROB tool is based on 7 items, random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and other bias (16). The adequacy of each of the seven ROB domains was rated as “low,” “unclear,” or “high” risk according to criteria provided in the Cochrane Handbook for Systematic Reviews of Interventions (16). We summarized the assessment of ROB per study as Low ROB (if low ROB was judged for all the seven domains); as Unclear ROB (if unclear ROB was judged for one or more of the seven domains); and as High ROB (if high ROB was judged for one or more of the seven domains) (16).
The GRADE guidelines for systematic reviews were used to evaluate the quality of the psychosis symptom severity scores. The GRADE approach includes assessing ROB for study limitations, inconsistency, publication bias, imprecision, and indirectness (17–22) for the body of pooled trials. The rating of the quality of outcome across trials was carried out to summarize the extent of our confidence (high, moderate, low, or very low) that the estimates of the effect represent the truth (17–22).
We performed a random effects meta-analysis (Sidik-Jokman) of RCTs comparing exercise as a whole intervention or by different type of exercise (aerobic or yoga) to usual care in patients with psychosis on PANSS scores. We used STATA (Stata Statistical Software: Release 16, StataCorp LLC). We used the standardized mean difference (SMD) and reported 95% confidence intervals. We assessed small study effects with Harbord test (23) and we investigated the presence of publication bias with funnel plots (24). In the presence of publication bias we imputed the missing studies to account for publication bias in the meta-analysis. We compared the observed and the imputed studies by using the non-parametric “trim and fill” method. We used contour-enhanced funnel plot to assess if imputed studies fall in the region of statistical significance (25).
Our secondary outcome was to assess adverse events, safety outcomes were expressed as risk ratio. We quantified heterogeneity estimates of the between-study variance using the τ2 statistic (26). In the presence of substantial heterogeneity in the meta-analysis, we planned to perform separate univariate meta-regressions to quantify factors that may contribute to substantial heterogeneity. We prespecified the following factors: allocation concealment, year that the study was conducted and the time of follow-up.
The initial search generated 603 articles. After removal of duplicates, and title and abstract screening 87 articles remained for full-text review. Of these, 15 met the eligibility criteria. Screening of reference lists resulted in identifying an additional 8 articles to be included. Our updated search yielded an additional 45 articles to review, one of which met the eligibility criteria. A total of 24 studies included in this systematic review. The study selection flow chart is presented in Figure 1.
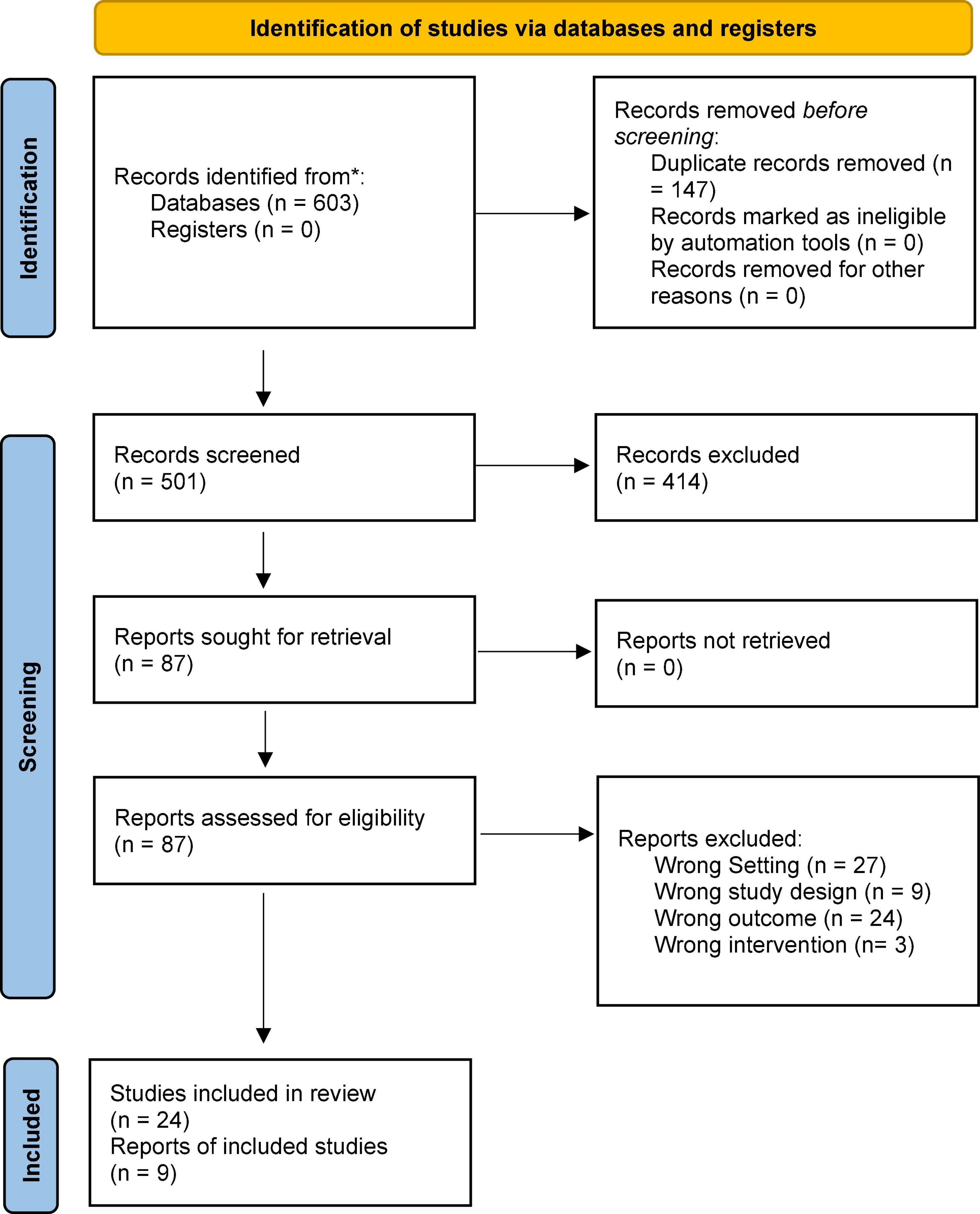
Figure 1. Flow chart of article screening and articles included in the review.
The 24 eligible RCTs were conducted between 2006 and 2022 and included 1,426 participants. The study ranged from 10 to 160 participants. All trials were conducted on adults over the age of 18. A summary of the study characteristics is presented in Table 1.
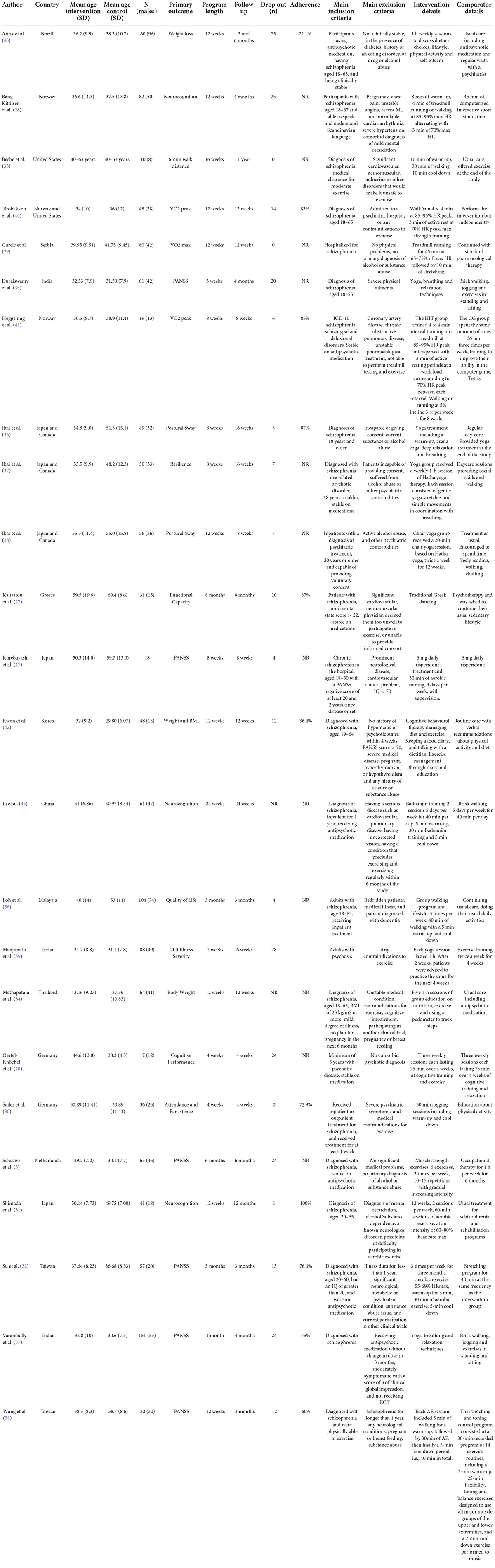
Table 1. Summary of study characteristics.
The studies included in this review were exercise and physical activity interventions, compared to usual care. There were a mix of exercise interventions including dancing (27), running (28–32), walking (33, 34), yoga (35–39), strength training (5), high intensity interval training (28, 40, 41), and lifestyle modifications, by increasing daily walking and mobility (42, 43). Some interventions included a combination of both strength and aerobic exercise training (44, 45).
The comparator groups were usual care or an active intervention. The usual care most commonly included antipsychotic medications and being followed by a psychiatrist. We found lack of reporting from majority of the included studies on which antipsychotic medication was prescribed. The information about the medication use that was available is described in Table 1. Active interventions in the comparator group included walking or stretching (28, 32, 35, 39, 45). Some of the comparator groups were related to education about physical activity (30) or spending time with an occupational therapist (5, 42). More information about the comparator characteristics is presented in Table 1.
Of the 90 articles that were deemed relevant for full text review, 24 were included in this systematic review and meta-analysis. The remaining articles were excluding for the following reasons:
- Wrong setting, was not in a hospital setting (n = 27)
- Wrong outcome, did not included PANSS as part of their outcome assessments (n = 24)
- Wrong study design, was not an RCT (n = 9)
- Wrong intervention, not exercise or physical activity (n = 3)
The reasons of the excluded studies are presented in Supplementary Web Appendix.
Blinding of the participants (performance bias) was rated as high in 18 out of 24 trials. Random sequence generation was rated as low risk of bias in 15 out of 24 trials. We found no indication of publication bias see funnel plot in Supplementary Web Appendix Figure 4, and Supplementary Tables 3, 4.
We found very low to moderate quality certainty for the pooled psychosis symptom severity scores (Table 2). Most of the studies were downgraded due to high risk of bias, from lack of blinding and incomplete outcome data.
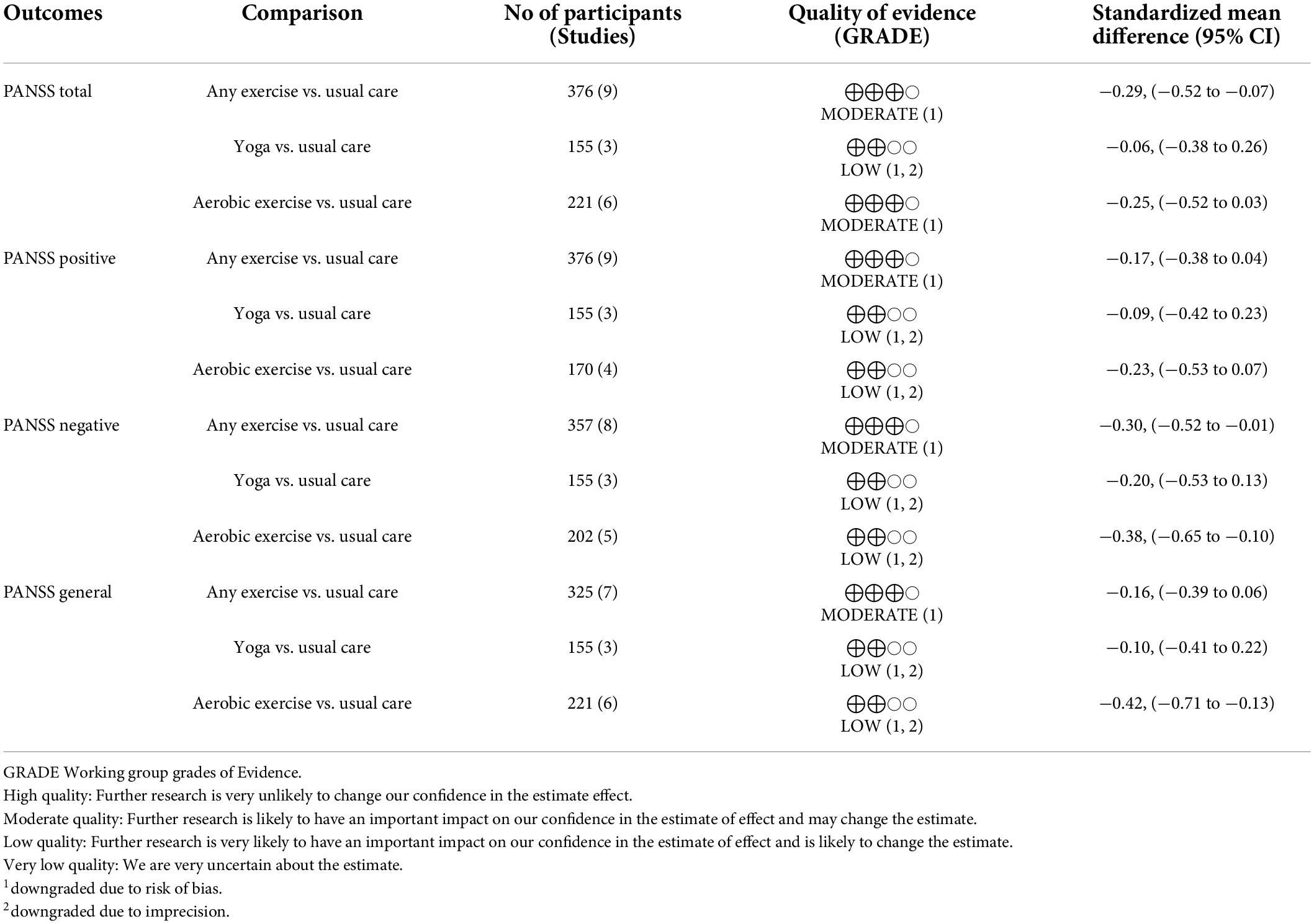
Table 2. Certainty of evidence per outcome.
A total of 1,426 participants were included in this review. The average age across all the studies was 39.5 years. There were 825 males included in the study, which was 58% of the participants. More information about the study demographics is included in Table 1.
Five of studies used the overall PANSS as the primary outcome (5, 32, 35, 46, 47), and two used the PANSS subscale as the primary outcome. Three of the studies assessed neurocognition as the primary outcome (28, 31, 45). Three of the studies assessed weight loss as a primary outcome (34, 42, 43). Four studies assessed performance through either the 6-min walk distance (33) or VO2 max/peak (29, 41, 44). A summary of the included articles’ primary outcomes is presented in Table 1.
The timeframe for most of the studies (9/24 studies) for the exercise intervention was 12 weeks [range (min-max) 3–34.4 weeks]. A summary of the program length and follow up time frames are presented in Table 1.
Drop out was not reported in two of the studies. Three of the studies had no participants drop out (29, 30, 46). One trial reported high attrition and had the highest number of participants to drop out (n = 75) across all trials which was 47% of the participants that were randomized (43).
Adherence was not well reported in the studies. Some studies required participants to maintain a certain adherence (e.g., 75 or 80% of sessions) or the participants were excluded from the study. A summary of all the studies that reported the rate of drop out and adherence is presented in Table 1.
Nine studies were included in the meta-analysis of the PANSS outcome. Figure 2 shows the between group differences of all the exercise modalities as whole intervention compared to usual care.
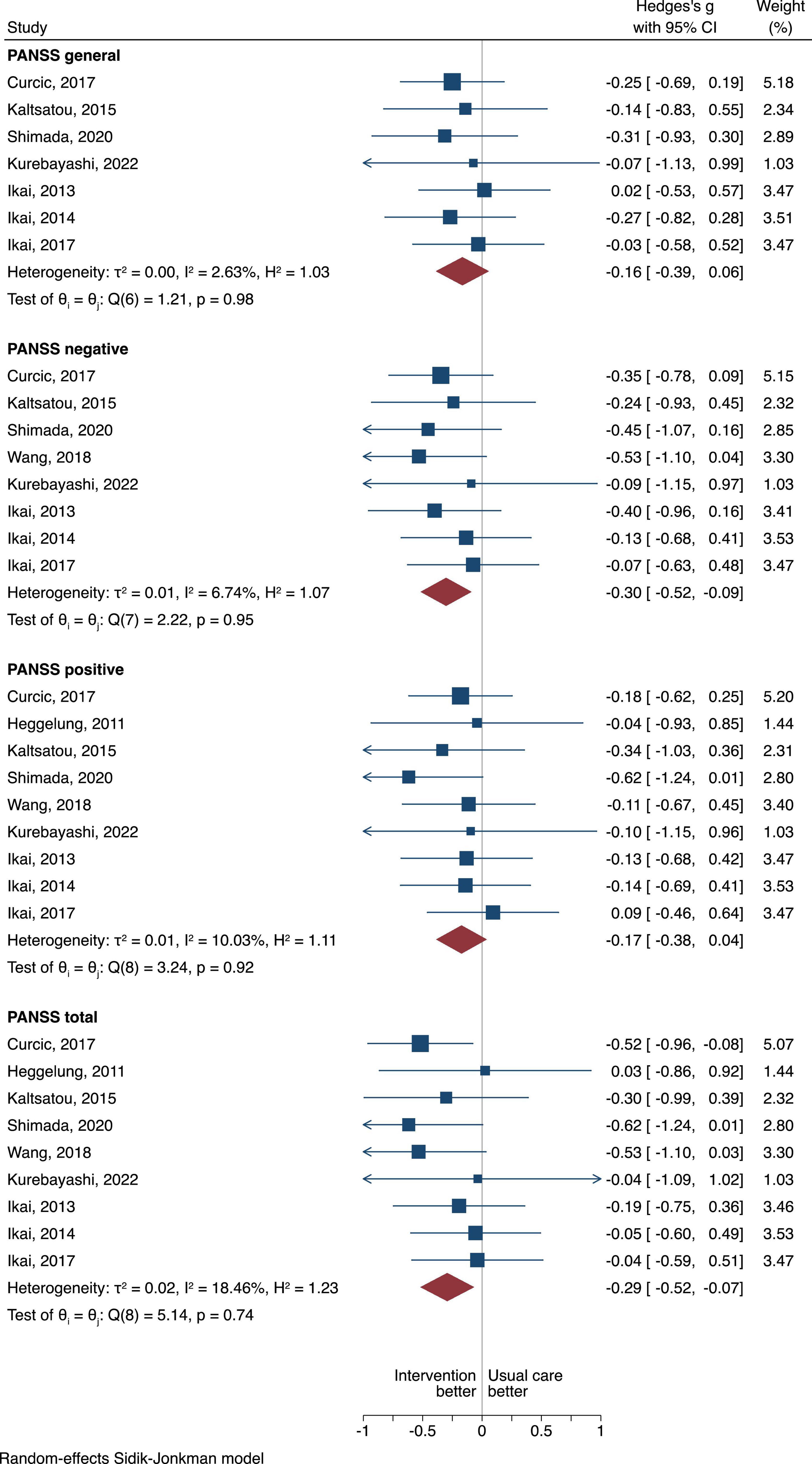
Figure 2. The between group difference of the exercise group compared to usual care is expressed as standardized mean difference (SMD). A negative difference means that the treatment resulted in a lower PANSS scores compared to the usual care, which is favorable.
Exercise as an intervention in hospital setting had more pronounced effects when compared to usual care in PANSS overall scores with a pooled SMD of −0.29, 95% CI = −0.52 to −0.07, τ2 = 0.02, n = 9, moderate certainty of evidence (Figure 2).
When looking at the negative PANSS scores, exercise compared to usual care displayed statistical superiority with a pooled SMD of −0.30, 95% CI = −0.52 to −0.09, τ2 = 0.01, n = 8, moderate certainty of evidence (Figure 2).
For the positive PANSS scores, although exercise was favored when compared to usual care the difference was not statistically different (SMD of −0.17, 95% CI = −0.38 to 0.04, τ2 = 0.01, n = 9), moderate certainty of evidence (Figure 2).
For the general PANSS scores, although exercise was favored when compared to usual care the difference was not statistically different (SMD of −0.16, 95% CI = −0.39 to 0.06, τ2 = 0, n = 7), moderate certainty of evidence (Figure 2).
To get a better understanding of which type of exercise affects psychotic symptoms, a comparison for the PANSS scores was made between aerobic and usual care, and yoga vs. usual care (Figures 3–6).
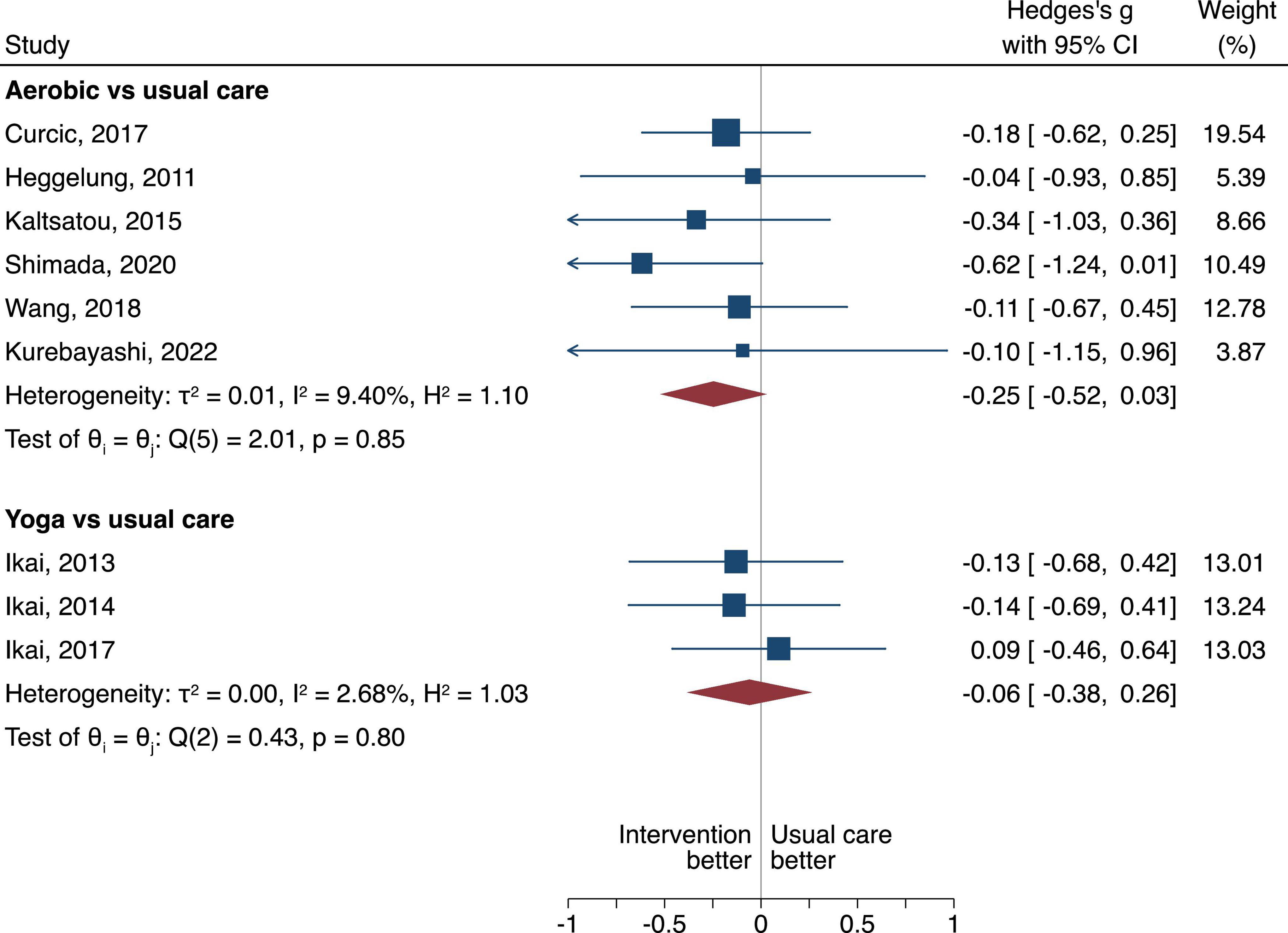
Figure 3. The between group difference of the aerobic or yoga compared to usual care is expressed as standardized mean difference (SMD). A negative difference means that the treatment resulted in a lower PANSS overall score compared to the usual care, which is favorable.
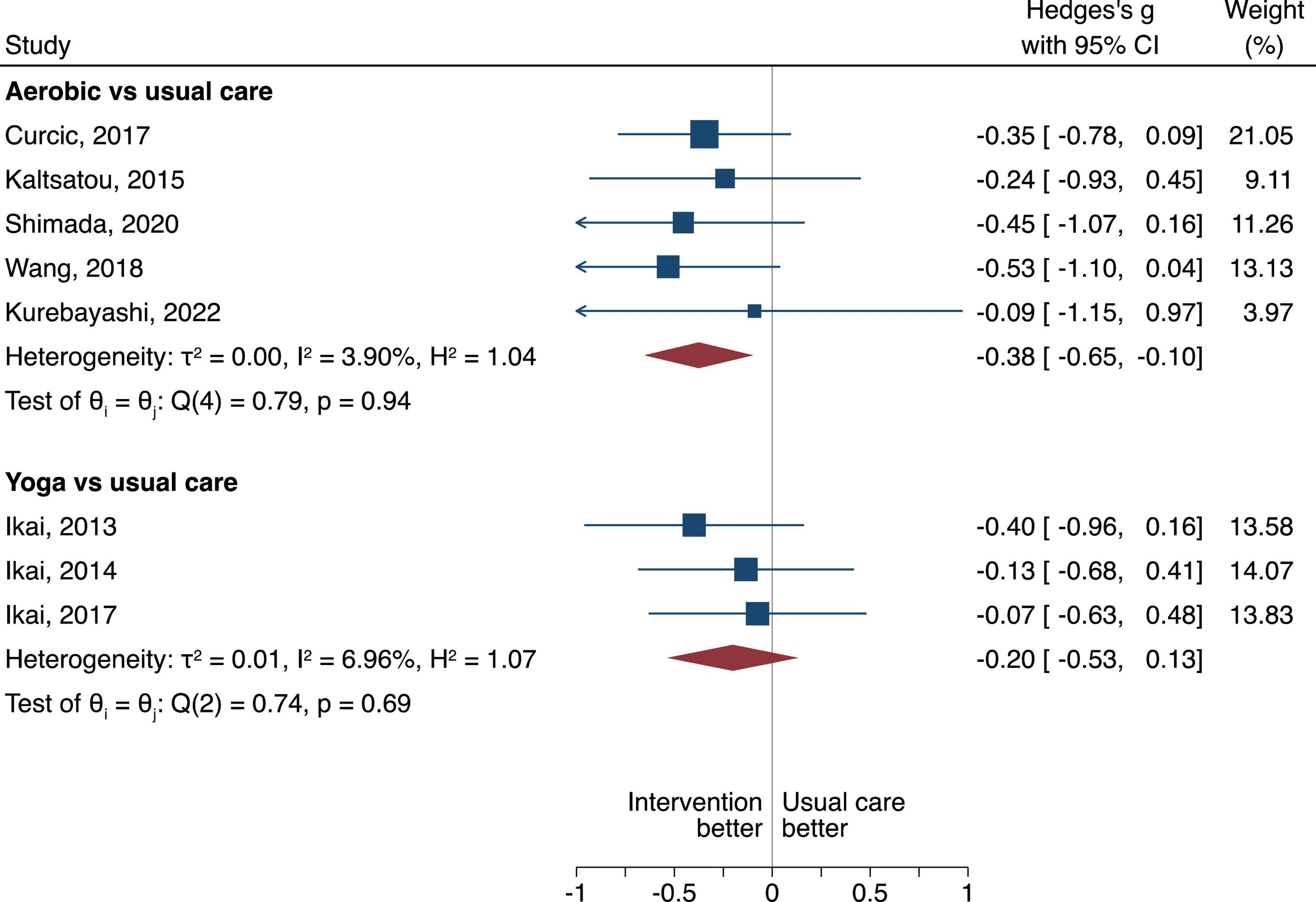
Figure 4. Negative PANSS scores in random-effects Sidik-Jonkman model. The between group difference of the aerobic or yoga compared to usual care is expressed as standardized mean difference (SMD). A negative difference means that the treatment resulted in a lower PANSS negative score compared to the usual care, which is favorable.
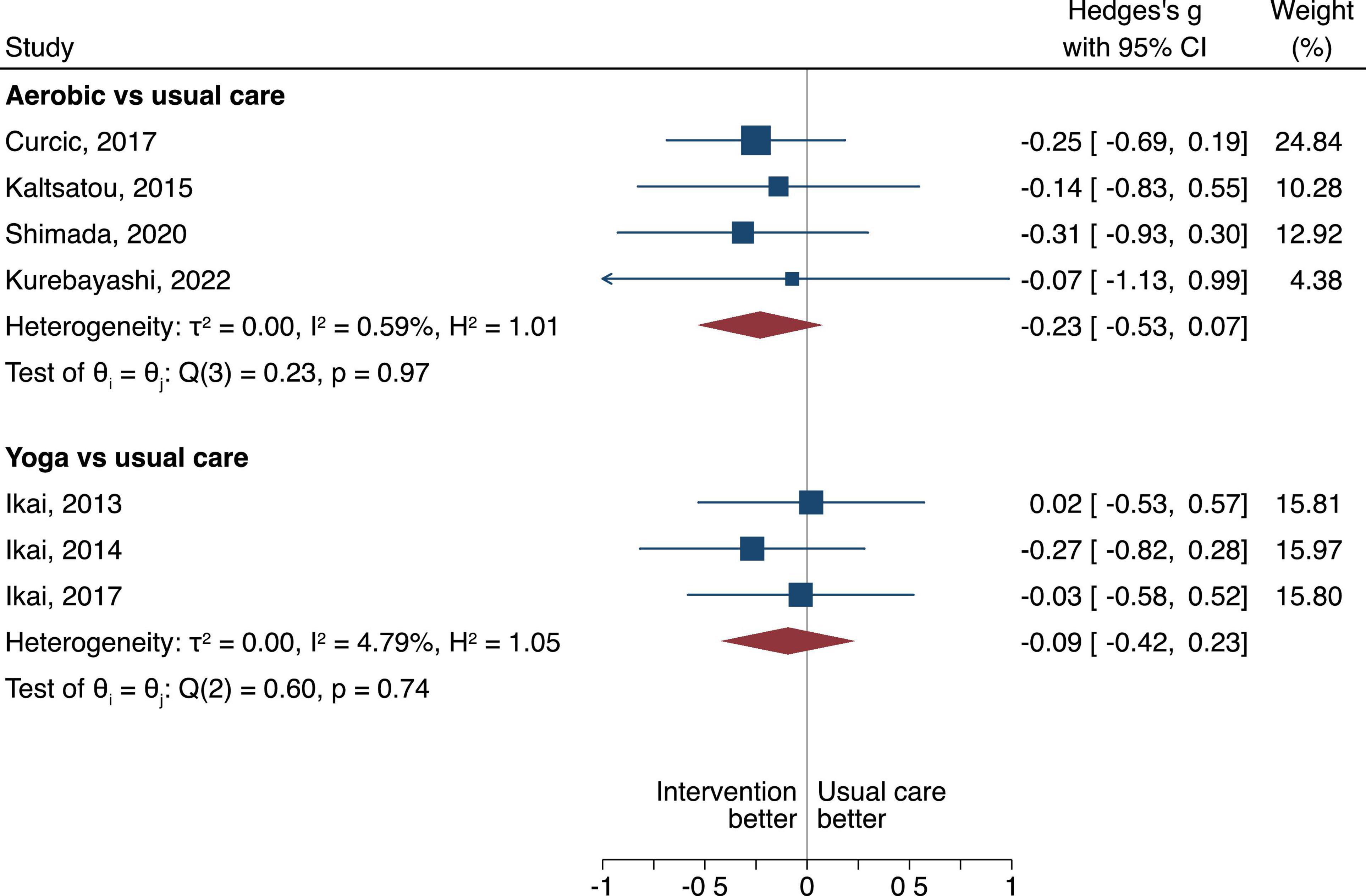
Figure 5. Positive PANSS scores in random-effects Sidik-Jonkman model. The between group difference of the aerobic or yoga compared to usual care is expressed as standardized mean difference (SMD). A negative difference means that the treatment resulted in a lower PANSS positive score compared to the usual care, which is favorable.
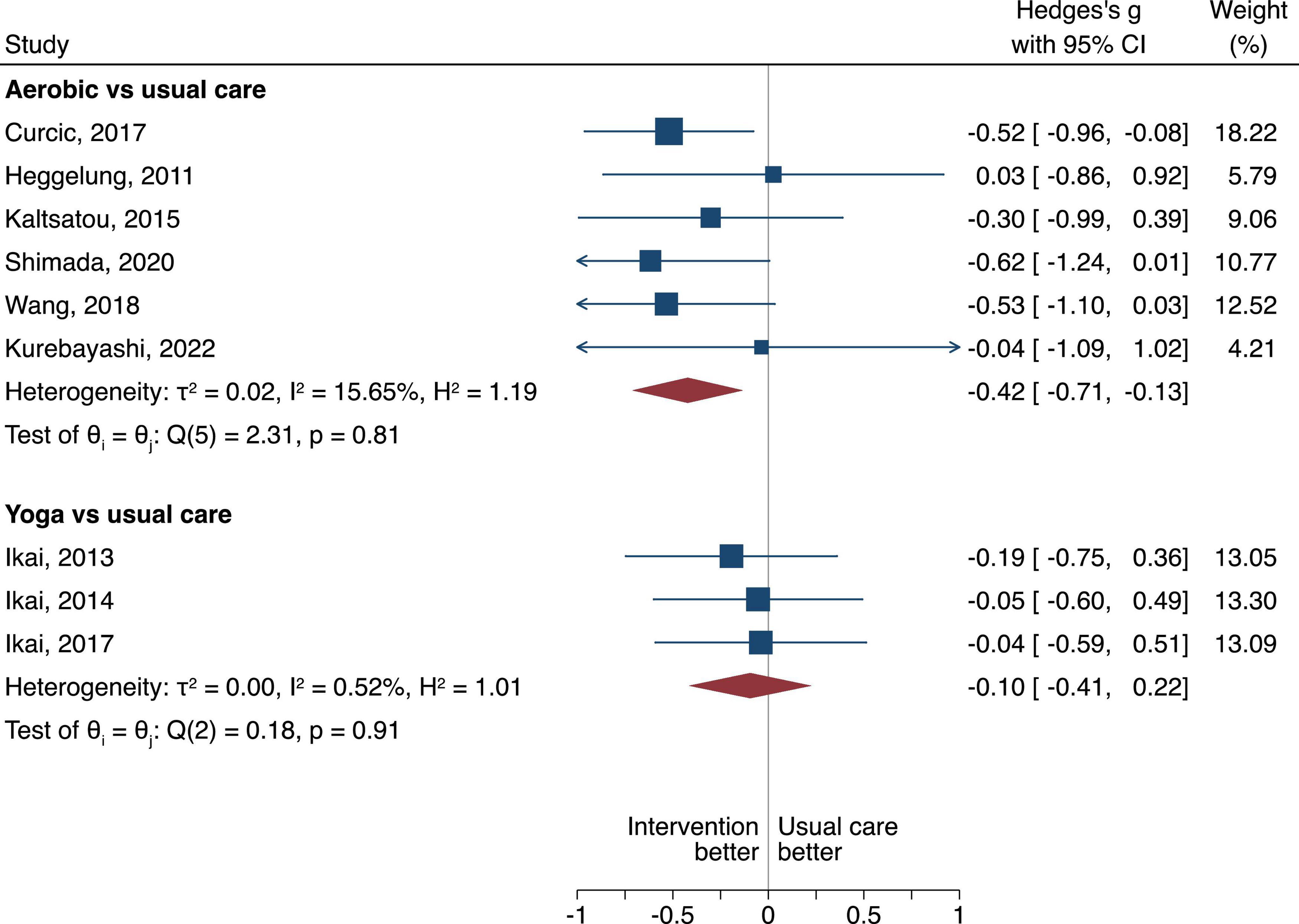
Figure 6. General PANSS scores in random-effects Sidik-Jonkman model. The between group difference of the aerobic or yoga compared to usual care is expressed as standardized mean difference (SMD). A negative difference means that the treatment resulted in a lower PANSS general score compared to the usual care, which is favorable.
Aerobic had more pronounced effects when compared to usual care, however, the difference was not statistically significant (SMD of −0.25, 95% CI = −0.52 to 0.03, τ2 = 0.01, n = 6, low certainty of evidence, Figure 3). Yoga had no difference when compared to usual care (SMD of −0.06, 95% CI = −0.38 to 0.26, τ2 = 0, n = 3, very low certainty of evidence, Figure 3).
When looking at the negative PANSS Score, aerobic when compared to usual care displayed statistical superiority with a pooled SMD of −0.38, 95% CI −0.65 to −0.10, τ2 = 0, n = 5, low certainty of evidence (Figure 4). Yoga when compared to usual care had no difference (SMD of −0.20, 95% CI = −0.53 to 0.13), τ2 = 0.01, very low certainty of evidence (Figure 4).
For the positive PANSS scores, we found no difference either for aerobic or yoga when compared to usual care (SMD of −0.23, 95% CI = −0.53 to 0.07, τ2 = 0, n = 4), very low certainty of evidence for the aerobic; and SMD of −0.09, 95% CI = −0.42 to 0.23, τ2 = 0, n = 3, very low certainty of evidence for the yoga intervention (Figure 5).
When looking at the general PANSS scores, aerobic when compared to usual care displayed statistical superiority with a pooled SMD of −0.42, 95% CI −0.71 to −0.13, τ2 = 0.02, n = 6, very low certainty of evidence (Figure 6). We found no difference when yoga compared to usual care (SMD of −0.10, 95% CI = −0.41 to 0.22), τ2 = 0, low certainty of evidence (Figure 6).
Adverse events were reported in 11 of the included studies (28, 30–32, 35, 37–39, 42–44). Most commonly the adverse event was a relapse of psychiatric symptoms, however, one study reported death, but the investigators reported that it was unrelated to the study protocols (44). One study reported on a somatic hospitalization (44). In our meta-analysis of serious adverse events, we found no difference on relapsing of psychiatric symptoms or somatic hospitalizations when we compared exercise to usual care with a pooled Risk Ratio (RR), 1.12 95% CI 0.44–2.81 (Figure 7).
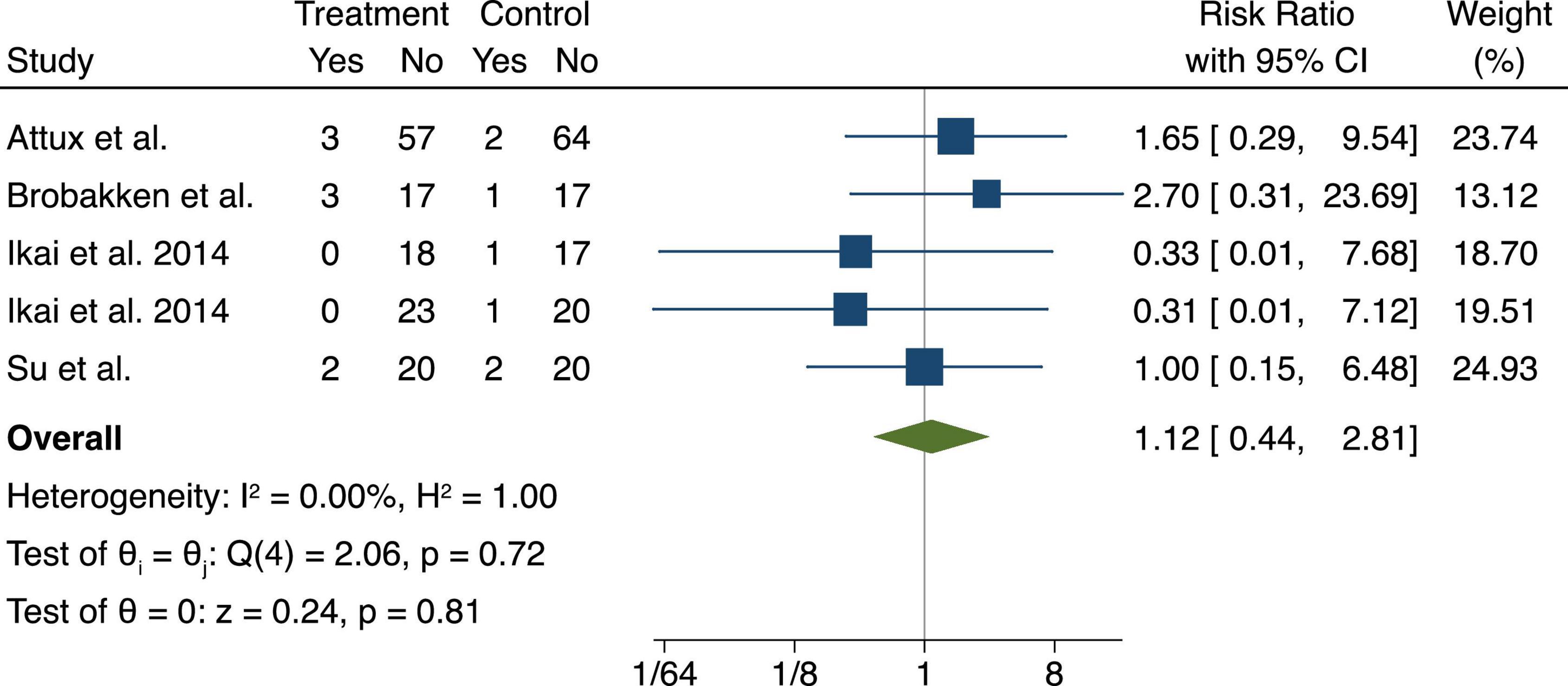
Figure 7. Serious adverse events (relapsing or hospitalization) displayed in a fixed-effects Mantel-Haenszel model. The between group difference of exercise modalities compared to usual care is expressed as Risk Ratio (RR). A risk ratio below 1 means that the exercise intervention had lower risk while above 1 indicates higher risk when compared to the usual care.
This systematic review and meta-analysis found a benefit to exercise training compared to usual care in schizophrenic adults in a hospital setting. Our meta-analysis showed more pronounced treatment effects in the PANSS overall score in the exercise intervention groups compared to the usual care. We further analyzed whether a certain type of exercise resulted in improvements in psychiatric symptoms. The ROB in the studies was mostly high, due to lack of blinding. ROB assessments for any study of exercise programs would have to be downgraded since it is impossible to blind the instructors or participants in exercise programs. The quality of the outcomes was low to moderate due to a high ROB, and imprecision. Larger sample sizes and more studies evaluating the effect of exercise in a hospital setting would need to confirm the effect of exercise for managing psychotic symptoms.
Several other systematic reviews and meta-analyses have been conducted on the effects of exercise for people with psychosis. A Cochrane review published in 2013 of 39 trials and 1,356 participants compared exercise with no treatment or control intervention for the primary outcome of depression (48). They found that there was a moderate clinical effect, and the results were statistically significant (48). In another Cochrane review looking at exercise therapy for schizophrenia, only three studies were included in this review but also found exercise significantly improved negative symptoms related to schizophrenia (49). A more recent meta-analysis of 17 RCT’s also found a benefit of exercise on negative symptoms for people with schizophrenia (50). Our study was unique in pooling all exercise as well as analyzing the effects of two different types of exercise (aerobic and yoga) compared to usual care on the effects of psychotic symptoms. We found improvements in psychotic symptoms in the intervention group compared to usual control, which is in agreement with the Cochrane reviews. We also found that aerobic exercise improved negative and general symptoms when compared to usual care, but yoga had no effect. One Cochrane review published in 2015 included 8 studies found that outcomes related to mental state, social functioning, and quality of life favored yoga compared to usual care (51). Our study could not confirm these findings because we did not evaluate these outcomes.
In another meta-analysis looking at mindful exercise compared to usual care, 7 studies were included and there was found to be a significant improvement in psychiatric symptoms and memory for the group that participated in the mindful exercise (52). Mindful exercise emphasizes deep, slow and relaxed breathing, and internal concentration to reduce stress by minimizing external stressors and improving mental focus (53). Although mindful exercise was not part of the interventions included in the current study, there could be an indirect effect of aerobic exercise and yoga on mindfulness, further supporting the benefits of exercise for people with psychosis.
This meta-analysis provided unique insight into the benefits of exercise in people with schizophrenia in a hospital setting. The study by Curcic et al. (29), showed the greatest effect in the meta-analysis (29). The intervention was a treadmill running program for 45 min at 65–75% of max HR, and the control group continued with standard care. In Curcic et al. (29), standard of care was pharmacotherapy (29). It is known that exercise at a higher intensity can help with symptoms like depression and anxiety, which may also contribute to the positive and negative symptoms experienced in people with schizophrenia (29). However, not all the running exercise studies included in this systematic review showed statistically or clinically significant improvements in the PANSS score compared to the control. This is likely because in some of the studies the control group was active control, and in one case the control group received the same intervention just without supervision (44).
One challenge to implementing an exercise program in a hospital setting is having access to personnel and resources. A study intervention allows for better implementation of an exercise program, because study personnel can run the program. Within the hospital setting, and outside of a research intervention, the program will rely on utilizing staff that are currently available. It is most feasible to rely on occupational and physical therapists to deliver exercise interventions. In the studies assessed in this review, one study intervention used occupational therapists to help with delivery (5), while none of the studies discussed the use of a physical therapist. Physical therapists are trained to provide exercise therapy safely and effectively. Recognizing the benefits that exercise has on psychiatric symptoms, exercise should be considered an essential part of treatment, and physical and occupational therapists should be used to administer the programs.
It is unclear how well received these programs were by the participants, as many studies did not report on adherence. However, in the studies that did report adherence the adherence ranged quite a bit with the lowest reported adherence as 36% adherence (42) and the highest reported adherence as 87% (36). In the study by Kwon et al. (42) with 36% adherence, participants had to attended 80% of the exercise sessions (42). The study by Ikai et al. (36) attribute their higher adherence to a flexible exercise schedule, and not requiring the participants to engage in exercise on their own (36). Based on these numbers it is not completely clear how well an exercise intervention is implemented into a hospital setting, but there seems to be some promising results, that even with a low adherence there may be benefit to psychiatric symptoms.
There were some adverse events reported, with 5 studies reporting serious adverse events, but suggested it was unrelated to the study protocol. For many of the studies contraindications to exercise was an exclusion criterion. That being said, due to increased movement, there is an increased risk of falling (54). It would be beneficial for all patients to undergo an exercise readiness screening, to assess balance, strength, and endurance prior to beginning the exercise program. As well, the exercise program should be modified for the individual, to provide maximal benefits and reduce the risk of exercise-related injuries. Most participants had to be stable on their medications to be eligible to participate in the study. However, it’s feasible to think there may be a risk to other participants or the instructor. It would be advised to follow hospital protocols to reduce the risk of behavior related adverse events. As well, relapse was another adverse event reported by five of the studies. It is not uncommon for patients with psychiatric symptoms to relapse, and it’s possible that with more exercise symptoms can be better managed and there may be less relapse events.
Finally, there were some notable gaps in the literature reducing the generalizability of these results. All the participants were between the ages of 18 and 65. Unfortunately this restricts the generalizability to older adults. Future studies should evaluate whether exercise interventions are feasible in older adults within a hospital setting. It may be that the mental illness is further progressed, and their mobility is further declined requiring a different approach than adults. There is also likely a fear of older adults with psychotic symptoms and likely other comorbidities like dementia participating in exercise interventions. However, there is evidence to suggest that exercise can help manage the behavioral and psychological symptoms of dementia (55). Trialing an exercise program in a hospital setting may be safer with extra personnel available.
Overall, this study demonstrated both strengths and limitations. The strength of this study was that we were able to conduct a meta-analysis in 9 trials, with the exercise intervention as whole and as two different exercise forms including yoga, and aerobic with no or very low statistical heterogeneity. The study effects and the overall effects of the meta-analysis demonstrated that the exercise intervention had a more pronounced effect, but the clinical benefit was uncertain. We also assessed the risk of bias to provide insight into the internal validity of the included studies. Although we believe we conducted a thorough literature search, where three databases, gray literature and reference lists were used, it’s possible some trials may have been missed. Also, the results in this study demonstrate a low to moderate certainty, and need to be interpreted with caution, until more studies can corroborate our findings. Pharmacotherapy was used as part of the treatment which can have a strong effect on mood, psychotic symptoms as well as physiological side effects which could make the clinical benefits and effectiveness of the intervention less pronounced, suggesting a potentially greater effect of exercise than is seen in our meta-analysis.
Aerobic intervention seems to be effective in reducing negative and general symptoms in patients with schizophrenia. However, we are uncertain if the effects of aerobic interventions were clinically important. We found no benefit of yoga when compared to standard of care. Additionally, the safety of exercise interventions needs to be monitored as less than half of the included trials reported adverse events. We found no increased risk on symptom relapsing or rehospitalizations for exercise interventions. Additional studies need to be conducted to corroborate these findings.
The original contributions presented in this study are included in this article/Supplementary material, further inquiries can be directed to the corresponding author.
CZ, DS, and MD contributed to the idea of the study. CZ, PB, and RF identified the articles and extracted the data. CZ, JM, and PB contributed to the analysis of the study. All authors contributed to the writing and editing of the manuscript.
CZ and PB were supported by the CIHR doctoral award. PB was supported by the Arthritis Society Postdoctoral Fellowship training award. JM was supported by a Canada Research Chair in Musculoskeletal Health Outcomes and Knowledge Translation and the Dr. James Roth Chair in Musculoskeletal Measurement and Knowledge Translation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.807140/full#supplementary-material
1. Conus P, Cotton S, Schimmelmann BG, McGorry PD, Lambert M. The first-episode psychosis outcome study: premorbid and baseline characteristics of an epidemiological cohort of 661 first-episode psychosis patients. Early Intervent Psychiatry. (2007) 1:191–200. doi: 10.1111/j.1751-7893.2007.00026.x
2. Peralta V, Cuesta MJ. Psychometric properties of the positive and negative syndrome scale (PANSS) in schizophrenia. Psychiatry Res. (1994) 53:31–40. doi: 10.1016/0165-1781(94)90093-0
3. Karow A, Moritz S, Lambert M, Schoder S, Krausz M. PANSS syndromes and quality of life in schizophrenia. Psychopathology. (2005) 38:320–6. doi: 10.1159/000088921
4. Schimmelmann BG, Conus P, Edwards J, McGorry PD, Lambert M. Diagnostic stability 18 months after treatment initiation for first-episode psychosis. J Clin Psychiatry. (2005) 66:1239. doi: 10.4088/JCP.v66n1006
5. Scheewe TW, Backx FJ, Takken T, Jörg F, Van Strater AC, Kroes A, et al. Exercise therapy improves mental and physical health in schizophrenia: a randomised controlled trial. Acta Psychiatr Scand. (2013) 127:464–73. doi: 10.1111/acps.12029
6. Vancampfort D, Rosenbaum S, Probst M, Soundy A, Mitchell AJ, De Hert M, et al. Promotion of cardiorespiratory fitness in schizophrenia: a clinical overview and meta−analysis. Acta Psychiatr Scand. (2015) 132:131–43. doi: 10.1111/acps.12407
7. American Psychiatric Association The American Psychiatric Association Practice Guideline for the Treatment of Patients with Schizophrenia. Washington, DC: American Psychiatric Pub (2020). doi: 10.1176/appi.books.9780890424841
8. Damme KS, Sloan RP, Bartels MN, Ozsan A, Ospina LH, Kimhy D, et al. Psychosis risk individuals show poor fitness and discrepancies with objective and subjective measures. Sci Rep. (2021) 11:1–10. doi: 10.1038/s41598-021-89301-5
9. Papiol S, Schmitt A, Maurus I, Rossner MJ, Schulze TG, Falkai P. Association between physical activity and schizophrenia: results of a 2-sample Mendelian randomization analysis. JAMA Psychiatry (2021) 78:441–4. doi: 10.1001/jamapsychiatry.2020.3946
10. Korman N, Armour M, Chapman J, Rosenbaum S, Kisely S, Suetani S, et al. High Intensity Interval training (HIIT) for people with severe mental illness: a systematic review & meta-analysis of intervention studies–considering diverse approaches for mental and physical recovery. Psychiatry Res. (2020) 284:112601. doi: 10.1016/j.psychres.2019.112601
11. Rosenbaum S, Tiedemann A, Sherrington C, Curtis J, Ward PB. Physical activity interventions for people with mental illness: a systematic review and meta-analysis. J Clin Psychiatry. (2014) 75:964–74. doi: 10.4088/JCP.13r08765
12. Dauwan M, Begemann MJ, Heringa SM, Sommer IE. Exercise improves clinical symptoms, quality of life, global functioning, and depression in schizophrenia: a systematic review and meta-analysis. Schizophr Bull. (2016) 42:588–99. doi: 10.1093/schbul/sbv164
13. Firth J, Cotter J, Elliott R, French P, Yung AR. A systematic review and meta-analysis of exercise interventions in schizophrenia patients. Psychol Med. (2015) 45:1343–61. doi: 10.1017/S0033291714003110
14. American Psychiatric Association. Areas for Further Research in Individuals With Schizophrenia: The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia. Washington, DC: American Psychiatric Association (2022).
15. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Rev Esp Cardiol. (2021) 74:790–9.
16. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Bmj. (2011) 343:d5928. doi: 10.1136/bmj.d5928
17. Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. (2011) 64:383–94. doi: 10.1016/j.jclinepi.2010.04.026
18. Guyatt GH, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, et al. GRADE guidelines 6. Rating the quality of evidence—imprecision. J Clin Epidemiol. (2011) 64:1283–93. doi: 10.1016/j.jclinepi.2011.01.012
19. Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 8. Rating the quality of evidence—indirectness. J Clin Epidemiol. (2011) 64:1303–10. doi: 10.1016/j.jclinepi.2011.04.014
20. Guyatt GH, Oxman AD, Montori V, Vist G, Kunz R, Brozek J, et al. GRADE guidelines: 5. Rating the quality of evidence—publication bias. J Clin Epidemiol. (2011) 64:1277–82. doi: 10.1016/j.jclinepi.2011.01.011
21. Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello P, et al. GRADE guidelines: 4. Rating the quality of evidence—study limitations (risk of bias). J Clin Epidemiol. (2011) 64:407–15. doi: 10.1016/j.jclinepi.2010.07.017
22. Mustafa RA, Santesso N, Brozek J, Akl EA, Walter SD, Norman G, et al. The GRADE approach is reproducible in assessing the quality of evidence of quantitative evidence syntheses. J Clin Epidemiol. (2013) 66:736–42. doi: 10.1016/j.jclinepi.2013.02.004
23. Harbord RM, Harris RJ, Sterne JA. Updated tests for small-study effects in meta-analyses. Stata J. (2009) 9:197–210. doi: 10.1177/1536867X0900900202
24. Sterne JA, Gavaghan D, Egger M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol. (2000) 53:1119–29. doi: 10.1016/S0895-4356(00)00242-0
25. Sterne JA, Egger M. Regression methods to detect publication and other bias in meta-analysis. In: Rothstein HR, Sutton AJ, Borenstein M editors. Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments. Hoboken, NJ: John Wiley & Sons, Inc (2005). p. 99–110. doi: 10.1002/0470870168.ch6
26. Deeks J, Higgins J, Altmann D. Incorporating heterogeneity into random-effects models. In: Higgins JPT, Green S editors. Cochrane Handbook for Systematic Reviews of Interventions. Hoboken, NJ: Wiley–Blackwell (2013).
27. Kaltsatou A, Kouidi E, Fountoulakis K, Sipka C, Theochari V, Kandylis D, et al. Effects of exercise training with traditional dancing on functional capacity and quality of life in patients with schizophrenia: a randomized controlled study. Clin Rehabil. (2015) 29:882–91. doi: 10.1177/0269215514564085
28. Bang-Kittilsen G, Egeland J, Holmen TL, Bigseth TT, Andersen E, Mordal J, et al. High-intensity interval training and active video gaming improve neurocognition in schizophrenia: a randomized controlled trial. Eur Arch Psychiatry Clin Neurosci. (2020) 271:339–53. doi: 10.1007/s00406-020-01200-4
29. Curcic D, Stojmenovic T, Djukic-Dejanovic S, Dikic N, Vesic-Vukasinovic M, Radivojevic N, et al. Positive impact of prescribed physical activity on symptoms of schizophrenia: randomized clinical trial. Psychiatria Danubina. (2017) 29:459–65. doi: 10.24869/psyd.2017.459
30. Sailer P, Wieber F, Pröpster K, Stoewer S, Nischk D, Volk F, et al. A brief intervention to improve exercising in patients with schizophrenia: a controlled pilot study with mental contrasting and implementation intentions (MCII). BMC Psychiatry. (2015) 15:211. doi: 10.1186/s12888-015-0513-y
31. Shimada T, Ito S, Makabe A, Yamanushi A, Takenaka A, Kawano K, et al. Aerobic exercise and cognitive functioning in schizophrenia: results of a 1-year follow-up from a randomized controlled trial. Psychiatry Res. (2020) 286:112854. doi: 10.1016/j.psychres.2020.112854
32. Su C-Y, Wang P-W, Lin Y-J, Tang T-C, Liu M-F, Chen M-D. The effects of aerobic exercise on cognition in schizophrenia: a 3-month follow-up study. Psychiatry Res. (2016) 244:394–402. doi: 10.1016/j.psychres.2016.08.011
33. Beebe LH, Tian L, Morris N, Goodwin A, Allen SS, Kuldau J. Effects of exercise on mental and physical health parameters of persons with schizophrenia. Issues Ment Health Nurs. (2005) 26:661–76. doi: 10.1080/01612840590959551
34. Methapatara W, Srisurapanont M. Pedometer walking plus motivational interviewing program for Thai schizophrenic patients with obesity or overweight: a 12−week, randomized, controlled trial. Psychiatry Clin Neurosci. (2011) 65:374–80. doi: 10.1111/j.1440-1819.2011.02225.x
35. Duraiswamy G, Thirthalli J, Nagendra H, Gangadhar B. Yoga therapy as an add−on treatment in the management of patients with schizophrenia–a randomized controlled trial. Acta Psychiatr Scand. (2007) 116:226–32. doi: 10.1111/j.1600-0447.2007.01032.x
36. Ikai S, Uchida H, Suzuki T, Tsunoda K, Mimura M, Fujii Y. Effects of yoga therapy on postural stability in patients with schizophrenia-spectrum disorders: a single-blind randomized controlled trial. J Psychiatr Res. (2013) 47:1744–50. doi: 10.1016/j.jpsychires.2013.07.017
37. Ikai S, Suzuki T, Uchida H, Saruta J, Tsukinoki K, Fujii Y, et al. Effects of weekly one-hour Hatha yoga therapy on resilience and stress levels in patients with schizophrenia-spectrum disorders: an eight-week randomized controlled trial. J Altern Complement Med. (2014) 20:823–30. doi: 10.1089/acm.2014.0205
38. Ikai S, Uchida H, Mizuno Y, Tani H, Nagaoka M, Tsunoda K, et al. Effects of chair yoga therapy on physical fitness in patients with psychiatric disorders: a 12-week single-blind randomized controlled trial. J Psychiatr Res. (2017) 94:194–201. doi: 10.1016/j.jpsychires.2017.07.015
39. Manjunath R, Varambally S, Thirthalli J, Basavaraddi I, Gangadhar B. Efficacy of yoga as an add-on treatment for in-patients with functional psychotic disorder. Indian J Psychiatry. (2013) 55(Suppl 3):S374. doi: 10.4103/0019-5545.116314
40. Oertel-Knöchel V, Mehler P, Thiel C, Steinbrecher K, Malchow B, Tesky V, et al. Effects of aerobic exercise on cognitive performance and individual psychopathology in depressive and schizophrenia patients. Eur Arch Psychiatry Clin Neurosci. (2014) 264:589–604. doi: 10.1007/s00406-014-0485-9
41. Heggelund J, Nilsberg GE, Hoff J, Morken G, Helgerud J. Effects of high aerobic intensity training in patients with schizophrenia—a controlled trial. Nordic J Psychiatry. (2011) 65:269–75. doi: 10.3109/08039488.2011.560278
42. Kwon JS, Choi JS, Bahk WM, Kim CY, Kim CH, Shin YC, et al. Weight management program for treatment-emergent weight gain in olanzapine-treated patients with schizophrenia or schizoaffective disorder: a 12-week randomized controlled clinical trial. J Clin Psychiatry. (2006) 67:547–53. doi: 10.4088/JCP.v67n0405
43. Attux C, Martini LC, Elkis H, Tamai S, Freirias A, Camargo MD, et al. A 6-month randomized controlled trial to test the efficacy of a lifestyle intervention for weight gain management in schizophrenia. BMC Psychiatry. (2013) 13:60. doi: 10.1186/1471-244X-13-60
44. Brobakken MF, Nygård M, Güzey IC, Morken G, Reitan SK, Heggelund J, et al. Aerobic interval training in standard treatment of out−patients with schizophrenia: a randomized controlled trial. Acta Psychiatr Scand. (2019) 140:498–507. doi: 10.1111/acps.13105
45. Li M, Fang J, Gao Y, Wu Y, Shen L, Yusubujiang Y, et al. Baduanjin mind-body exercise improves logical memory in long-term hospitalized patients with schizophrenia: a randomized controlled trial. Asian J Psychiatry. (2020) 51:102046. doi: 10.1016/j.ajp.2020.102046
46. Khonsari NM, Badrfam R, Mohammdi MR, Rastad H, Etemadi F, Vafaei Z, et al. Effect of aerobic exercise as adjunct therapy on the improvement of negative symptoms and cognitive impairment in patients with schizophrenia: a randomized, case-control clinical trial. J Psychosocial Nurs Ment Health Serv. (2022) 60:38–43. doi: 10.3928/02793695-20211014-03
47. Kurebayashi Y, Mori K, Otaki J. Effects of mild−intensity physical exercise on neurocognition in inpatients with schizophrenia: a pilot randomized controlled trial. Perspect Psychiatr Care. (2021) [Online ahead of print]. doi: 10.1111/ppc.12896
48. Cooney GM, Dwan K, Greig CA, Lawlor DA, Rimer J, Waugh FR, et al. Exercise for depression. Cochrane Database Syst Rev. (2013) 12:CD004366. doi: 10.1002/14651858.CD004366.pub6
49. Gorczynski P, Faulkner G. Exercise therapy for schizophrenia. Cochrane Database Syst Rev. (2010) 5:CD004412. doi: 10.1002/14651858.CD004412.pub2
50. Sabe M, Kaiser S, Sentissi O. Physical exercise for negative symptoms of schizophrenia: systematic review of randomized controlled trials and meta-analysis. General Hosp Psychiatry. (2020) 62:13–20. doi: 10.1016/j.genhosppsych.2019.11.002
51. Broderick J, Knowles A, Chadwick J, Vancampfort D. Yoga versus standard care for schizophrenia. Cochrane Database Syst Rev. (2015) 10:CD010554. doi: 10.1002/14651858.CD010554.pub2
52. Li J, Shen J, Wu G, Tan Y, Sun Y, Keller E, et al. Mindful exercise versus non-mindful exercise for schizophrenia: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Clin Pract. (2018) 32:17–24. doi: 10.1016/j.ctcp.2018.04.003
53. Bangalore NG, Varambally S. Yoga therapy for schizophrenia. Int J Yoga. (2012) 5:85. doi: 10.4103/0973-6131.98212
54. Zecevic AA, Salmoni AW, Speechley M, Vandervoort AA. Defining a fall and reasons for falling: comparisons among the views of seniors, health care providers, and the research literature. Gerontologist. (2006) 46:367–76. doi: 10.1093/geront/46.3.367
55. de Souto Barreto P, Demougeot L, Pillard F, Lapeyre-Mestre M, Rolland Y. Exercise training for managing behavioral and psychological symptoms in people with dementia: a systematic review and meta-analysis. Ageing Res Rev. (2015) 24:274–85. doi: 10.1016/j.arr.2015.09.001
56. Loh SY, Abdullah A, Bakar AK, Thambu M, Jaafar NR. Structured walking and chronic institutionalized schizophrenia inmates: a pilot RCT study on quality of life. Glob J Health Sci. (2016) 8:238–48. doi: 10.5539/gjhs.v8n1p238
57. Varambally S, Gangadhar BN, Thirthalli J, Jagannathan A, Kumar S, Venkatasubramanian G, et al. Therapeutic efficacy of add-on yogasana intervention in stabilized outpatient schizophrenia: Randomized controlled comparison with exercise and waitlist. Indian J Psychiatry. (2012) 54:227–32. doi: 10.4103/0019-5545.102414
Keywords: exercise, psychosis, physical activity, review—systematic, hospital
Citation: Ziebart C, Bobos P, MacDermid JC, Furtado R, Sobczak DJ and Doering M (2022) The efficacy and safety of exercise and physical activity on psychosis: A systematic review and meta-analysis. Front. Psychiatry 13:807140. doi: 10.3389/fpsyt.2022.807140
Received: 01 November 2021; Accepted: 28 June 2022;
Published: 16 August 2022.
Edited by:
Antonio Vita, University of Brescia, ItalyReviewed by:
Stefano Barlati, ASST Spedali Civili of Brescia, ItalyCopyright © 2022 Ziebart, Bobos, MacDermid, Furtado, Sobczak and Doering. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christina Ziebart, Y3ppZWJhcnRAdXdvLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.