 Inge Jager1,2*
Inge Jager1,2* Nienke Vulink1
Nienke Vulink1 Arnoud van Loon1Marthe van der Pol1Arjan Schröder2Simone Slaghekke1
Arnoud van Loon1Marthe van der Pol1Arjan Schröder2Simone Slaghekke1 Damiaan Denys1
Damiaan Denys1- 1Department of Psychiatry, Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands
- 2GGZ inGeest, Amsterdam, Netherlands
Misophonia is a disorder in which patients suffer from anger or disgust when confronted with specific sounds such as those associated with eating or breathing, causing avoidance of cue related situations resulting in significant functional impairment. Functional magnetic resonance imaging studies suggest misophonia is associated with increased activity in the auditory cortex and salience network, which might reflect increased vigilance toward specific misophonia triggers. New treatments have been developed and investigated in the last years in which this vigilance plays an important role. This is a synopsis of the first group protocol for systemic Cognitive Behavioral Therapy (G-CBT) for misophonia. We discuss the model of CBT for misophonia, provide a detailed guide to the treatment illustrated with a case study, discuss advantages, limitations, and possible pitfalls by a qualitative evaluation of the protocol, and review evidence for the protocol.
Introduction
Misophonia is a term which has been used first in 2001 (1). It's characterization as a potential psychiatric condition was first discussed by the Denys group in 2013 (2). Research in the last two decades has been has focused primarily on its phenomenology. The diagnosis has not been added to psychiatric classification systems as DSM-V or ICD-11 yet. Misophonia is characterized by the symptoms described in Table 1, which are consistent with the symptoms observed in a group of 575 patients that allowed the revised diagnostic criteria for misophonia proposed by Jager et al. (3). Recently, a Delphi Process study (4) led to an agreement of experts on at least 80% of the consensus definition. This consensus definition corresponds highly to the Amsterdam UMC 2020 revised criteria.
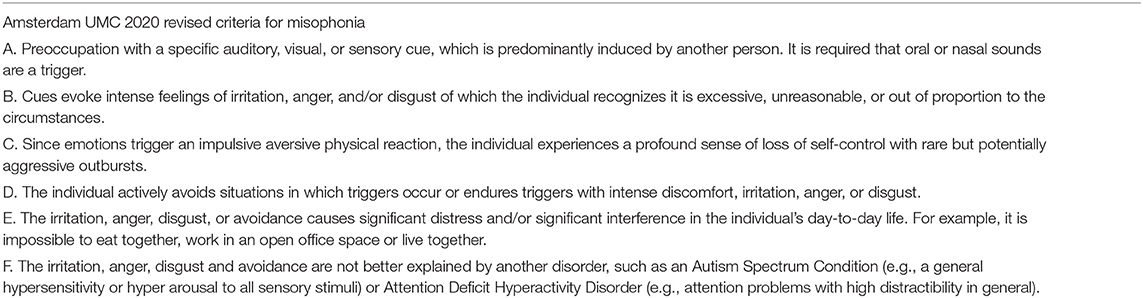
Table 1. Revised diagnostic criteria for misophonia (3).
Common triggers are: eating sounds (e.g., food chewing or swallowing) and nose—and breathing sounds (e.g., sniffing and heavy breathing). The intensity of the emotional response varies in different contexts and the level of stress in general. In the phenomenology of misophonia preoccupation with specific triggers is a main criterion (A). Two functional magnetic resonance imaging studies found evidence for this vigilance by showing increased activity in the auditory cortex and left amygdala in misophonia patients (5, 6). Misophonia effects quality of life; patients especially experience disabilities in family and social functioning (3, 7).
Prevalence and incidence still remain unclear, but first estimations of its prevalence suggest misophonia to be a common condition. In some reports prevalence is even estimated to be close to 20% of the population (8). In a sample of Chinese students, 6% was assessed to have misophonia (9) and in a sample of English students 12% reported moderate to severe misophonia symptoms (10). The origin of misophonia is a current topic of research. For now, we know at least a third of patients report a family history of misophonia (3, 11). Misophonia symptoms usually arise gradually in peri puberty, around the age of 13 (2, 3, 12).
Research on treatment for misophonia started in audiology with the altered intervention of tinnitus retraining therapy (TRT) (13). Currently, treatment studies exist mainly within the domain of mental health. Cognitive behavioral therapy has been investigated most often and has shown promising results in treating misophonia in single case studies (14–18).
In this article we present the first protocol for group- cognitive behavioral therapy (G-CBT) for misophonia with a systemic approach. This is a synopsis of the Dutch manual for group (G-)CBT for adults with misophonia developed by van Loon et al. (19), which contains a protocol for individual therapy and a protocol for youth (age 12–18 years) as well. The main aims of the misophonia protocol are to decrease misophonia symptoms, improve quality of life, and to provide a greater sense of personal control. The highlights of this protocol have been succinctly described in the methods section of the randomized controlled trial (20).
Even though the effect of individual CBT is still under investigation, the interventions of this manual can be applied in individual treatment as well. Because of the existing evidence for G-CBT and the significant impact of misophonia on interpersonal interactions, group therapy is very suitable for misophonia patients. In G-CBT patients find recognition among themselves and support for their symptoms. Also, in G-CBT patients have a unique chance to experience both being the victim, and offender. Knowledge of group dynamics is obviously needed to use this factor therapeutically.
The aim of the present study is to present a model for (G-)CBT for misophonia through the description of a single clinical case. This case study will serve as a running example throughout this article. We provide a detailed guide to the treatment by describing all interventions and providing timing and illustrations for the procedures. We review evidence for the protocol and will discuss advantages, limitations, and possible pitfalls by a qualitative evaluation. This article is intended as a practical guide, instead of a discussion of theoretical learning principles of CBT for misophonia.
Methods
Theoretical Background
Misophonia symptoms have been previously conceptualized within a cognitive-behavioral model (21–25). An extensive conceptualization within the CBT model is provided by Vollbehr and ten Broeke (2017) in the Dutch journal of cognitive and behavioral therapy, but we refer specifically to the model provided by Frank and McKay (26) and the psychological model in the recently published article of Cowan et al. (27).
Misophonia can be explained by coupling and subsequent memory consolidation of in themselves neutral stimuli (conditioned stimuli, CS) to an aversive emotional stimulus and the accompanying emotion (as a conditioned response, CR). For instance, if a child is annoyed by the sounds of his father eating, but is not allowed to leave the table and has to listen to these sounds, he or she may feel disgusted and afraid to lose control. The next meal this child will focus on the eating sounds of father again and the feelings of the last meal will come to mind. Gradually the stimulus will robustly and repeatedly evoke aversive thoughts or emotions. After this classical conditioning, principles of operant conditioning maintain and aggravate symptoms. For instance, if this child fears it cannot inhibit this intense emotional reaction to triggers it will avoid situations such as dining together, and therefore misses out on important social events. Figure 1 shows the CS-CR coupling and the avoidance and hyperfocus of the conditioned stimuli commonly seen in misophonia.

Figure 1. CBT conceptualization of misophonia.
Even though the etiology of misophonia still is unclear, the phenomenology is extensively investigated by our research group (2, 3). This research and the resulting revised diagnostic criteria for misophonia (Table 1) has been the basis of our treatment. All elements of the CBT conceptualization above can be found in the revised diagnostic criteria as well. In Figure 2, the revised diagnostic criteria on which the various interventions of the treatment manual intervene, are displayed.
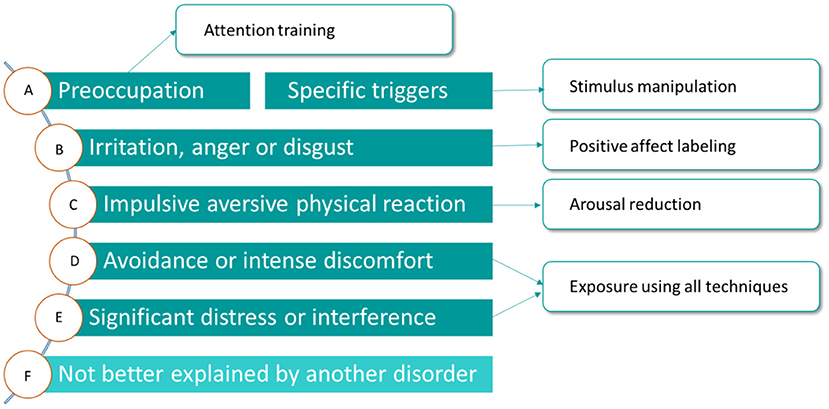
Figure 2. Amsterdam UMC revised criteria for misophonia and corresponding interventions.
The various CBT techniques intervene on different levels to maximize result. Stimulus manipulation and attention training intervene on the side of the conditioned stimulus. Arousal reduction intervenes on the conditioned response side and positive affect labeling intervenes on both the representation of the unconditioned stimulus and the conditioned response.
The used model for patients for characterizing misophonia in the protocol is the biopsychosocial model, presented in Figure 3.
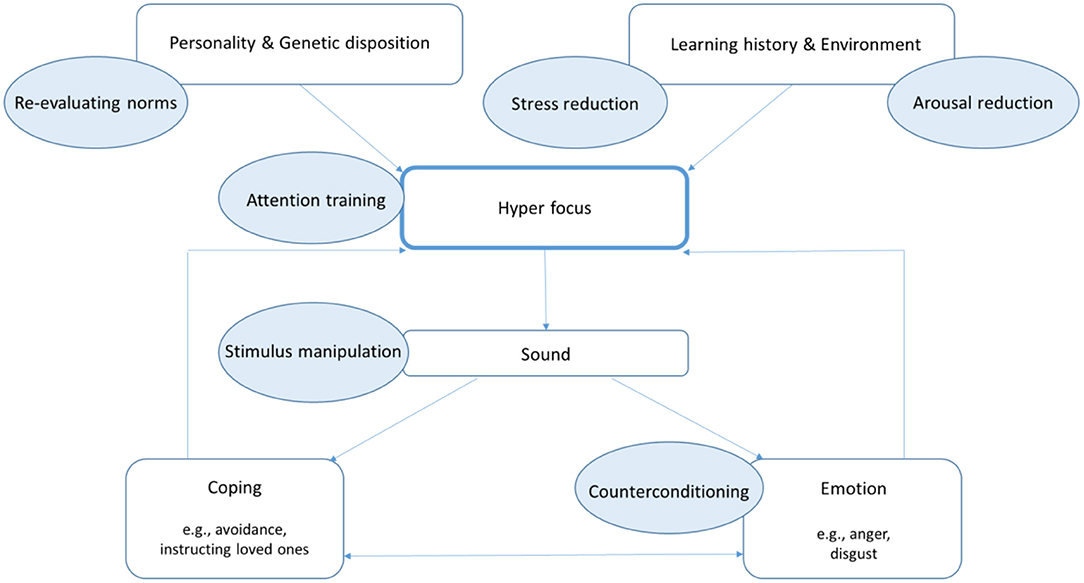
Figure 3. Biopsychosocial model of misophonia.
This model assumes that hyper focus, characterized by preoccupation with trigger sounds and a high arousal, has a central role in the maintenance or aggravation of misophonia symptoms. Almost all patients report a hyper focus (3, 28). This hyper focus implies that patients are trained to notice trigger sounds much sooner than others. And other triggers may be added if they also are attended to easily. For example, when the sound of a spouse chewing gum is the trigger for a misophonia patient, this patient will notice this sound made by the spouse before anyone else can notice this. But it is probable this patient will then notice a colleague eating gum, and may assess if this is just as disturbing. The hyper focus then will lead to a more generalized sensitization. Besides trigger sounds, non-auditory triggers (like seeing someone chewing gum) can then cause a strong aversive emotional reaction as well. A misophonic response to visual triggers is called “misokinesia.”
Since all misophonia patients report sounds as a trigger (3, 4), it is safe to say that sound is the primary trigger modality in the misophonia model.
Several factors can influence the development of a hyper focus. Specific personality traits can include clinical perfectionism which has been found in 66–97% of patients (3), and the setting of high norms, as a trait of obsessive-compulsive personality disorder are found in 26–52% (2, 3) of patients. These traits increase the chance of developing a hyper focus. Autism like traits have not been associated with misophonia symptoms, even though the prevalence of autism spectrum conditions as a comorbid disorder in misophonia is three-fold the prevalence as in the normal population (3). Last, many of the misophonia patients report a family history of misophonia.
Besides factors within the patients, external factors such as learning history and environment can also contribute in the development of a hyper focus. The learning history of a patient with misophonia is one in which specific sounds have been associated with negative experiences by the process of classical conditioning during life. Finally, environmental factors influence hyper focus more directly. When patients experience stress or are tired they experience more hyper focus than when they are in good condition.
To cope with the trigger sounds and provoked emotions, patients develop maladaptive strategies, such as avoiding trigger sounds (e.g., they work, travel, sleep or eat alone or use earplugs), using camouflaging sounds (e.g., an extractor or music), or compulsory instructing their social environment (e.g., forbid partner to eat crisps). These strategies implemented in turn have effect on the hyper focus as depicted by the return arrow in Figure 3. For instance, a strategy such as using headphones with music, may counterintuitively lead to increased vigilance over whether the sound is still present and even greater focus on the trigger sounds despite the overlaying music. This increases hyper focus.
Trigger sounds provoke strong emotions of irritation and anger, and in most cases disgust (2, 12). The intensity of the aggression is mostly very strong (3). Patients quite often report the urge to harm their close relatives, because of the (eating) sounds they produce. To avoid being overwhelmed and feeling powerless by these emotions, patients pay more attention to detect trigger sounds. This is depicted by the return arrow from emotion to hyper focus in Figure 3.
Case Conceptualization
As an illustration of the misophonia model we use the case conceptualization of an actual patient given the anonymized name of “Charlotte.” This patient meets all criteria proposed by the Amsterdam UMC in 2020. The revised Amsterdam Misophonia Scale [AMISOS-R; (29)] indicates she has severe to extreme misophonia (range 31–40). The labels in parentheses are links to the main elements of Figure 3.
Charlotte is a 37-year-old woman, who works as a lawyer and has a family with two children. Charlotte signed up for treatment, because she wants to avoid a divorce. She considers treatment as “her last straw to save her marriage.” Charlotte developed her symptoms at the age of 12, when she started puberty. She has always had high standards as a child (personality), but she started judging people who made more eating sounds and even disliked them. Now she considers people who make eating sounds as “people who have a defect” and refuses to interact with them. Her parents do not have misophonia, but she found out her father's mother had similar symptoms (genetic disposition). Charlotte grew up in a prosperous family as an only child. Her first and main trigger sound was the sound of food chewing her mother made. During her adolescence all joint meals were in a tense atmosphere, with her mother expressing she was hurt by the non-verbal aggression of Charlotte, and her father “trying to mediate between them.” Sometimes Charlotte was allowed to listen to a portable music player during dinners, but more often she was told by her father to stay at the table and control herself. This made her feel extremely powerless and she felt guilty for ruining dinner (learning history). During holidays, without her busy schedule of extracurricular activities, misophonia symptoms were less present. With lower stress and, as such, less sensitivity to misophonic triggers, she could enjoy her mother's company more (environment). Later in life she felt annoyed by nearby eating behaviors of students or colleagues, but misophonia symptoms were not disabling, because she could avoid her major triggers. When she visited her parents however, misophonia symptoms returned to levels that were present at puberty. The first 6 years of her relationship with her husband, she did not experience him as a misophonia trigger. But during the pregnancy of their firstborn child, she started to respond with disgust and aggression (emotion) to his eating sounds and breathing or snoring. She also had a strong reaction to the sounds of doors closing loudly, whispering, sniffing, “s” and “t” sounds, glasses being put on the table, ringing keys and the dishwasher during nighttime (trigger sound). She developed a strong focus on these sounds, which made it impossible to engage in social interaction or sleep during these sounds (hyper focus). Subsequently Charlotte avoided eating together with her family and started sleeping alone. She tried to correct her husband when he was eating, even though she realized he did not produce too much sound, and she picked many fights about his breathing sounds (coping).
Phases of the Protocol
The phased structure of this G-CBT protocol for misophonia is outlined below.
(A) Assessment and engagement phase
Firstly, patients in the group are invited to get acquainted with each other, possibly with the use of introductory games (i.e., ice-breakers). Within the first session, group therapy rules concerning presence, confidentiality, and between session tasks are explained and the focus is to create a safe context for patients to share personal experiences. Therapists give psychoeducation about misophonia, validate the patients' experiences, normalize symptoms such as internal rage and emphasize similarities between the patients in the group. The therapeutic attitude is first of all validating and supporting. However, we believe that the use of humor in the group sessions from the start is an important element with positive results. Humor creates a distance toward the symptoms and helps patients to revise their high norms. It provides room to be more flexible and try out new behavior.
The biopsychosocial model for understanding misophonia is explained and filled with patients' experiences. Patients are motivated to share their memories of the onset of the misophonia symptoms (to the best of their knowledge) and the effect of misophonia on their life and life choices. Experiences are shared when patients present their “mood boards” (a personal collage consisting of images, texts, and samples of objects in a composition), an in-between-session task, with current negative associations with triggers and their desired associations.
A pretreatment measurement for misophonia symptoms can be performed at the first session with the revised Amsterdam Misophonia Scale [AMISOS-R; (29)]. We advise adding a questionnaire for general psychopathology, such as the Symptom Checklist-90 (SCL-90) (30). Further, the Sheehan Disability Scale (SDS) (31), used for other psychiatric and general medical conditions, can be applied to misophonia to determine the effect of treatment.
In the first phase consequences of misophonia symptoms on work, social life, and family life are discussed, as well as the pros and cons of being open about the diagnosis to family, friends or colleagues. Patients are encouraged to invite their close relatives to actively participate in the treatment. In this phase close relatives are invited for a separate meeting without the patients to provide psychoeducation about misophonia and the treatment, to share experiences, to manage expectations (e.g., no symptom reduction should be expected before week four) and to motivate them to participate actively and support their close relatives.
Expectations of treatment of all patients are discussed and information is provided about scientific research, as well as clinical experiences with the misophonia group protocol. Patients must be willing to devote the time needed for weekly sessions, as well as to devote energy to out-of-session work (e.g., homework). Goals are set within the first two sessions. Once goals have been identified and prioritized, they are operationalized, which involves defining the goals and all the steps that it will take to achieve them in concrete, observable/measurable cognitive or behavioral terms (SMART). Finally, patients are invited to examine their tension and attention as a first step toward reduction of arousal and stress with the body scan procedure (32).
(B) Change strategy phase
Once the secure base of the group is formed and goals are formulated in a SMART manner, various interventions to change are applied. Each group session has a theme matching the main intervention with corresponding psychoeducation and exercises (e.g., Misophonia models, Perception and attention, Stress, Conditioning, and Norms). For misokinesia psycho-education about the function of for instance wobbling legs or playing with your hair (re-evaluating norms) or the simple instruction to stop watching (attention training), is often sufficient to reduce symptoms. Additionally, fantasy and humor can be used, such as imagining a ball on a wobbly leg (counterconditioning).
Patients learn to gain control over their (internal) reactions to misophonia triggers and practice new behavior and adaptive coping strategies. The interventions are described in detail below in the Section “Overview of the Protocol.” Since patients first need to practice the various techniques before they can apply them to misophonia trigger situations, actual change often only emerges after session four. The protocol should be adapted to the different severity levels; leave patients in control when you align which steps are feasible, but always start with mild triggers.
In this stage avoidance behavior is phased out, which means patients are gradually exposed to misophonia triggers situations. The inhibitory learning model (33) is used for exposure, which emphasizes new learning when confronted with previously avoided stimuli rather than merely the cessation of fear or aversive emotional responding (26). Our systemic approach of misophonia is evidenced by the role of close relatives in this protocol. Close relatives receive psychoeducation, share experiences amongst each other, give support with between-session-tasks and patients and family or friends practice the learned techniques together.
This phase ends with a session to practice all the learned techniques together with close relatives producing trigger sounds under supervision of the therapists.
(C) Consolidation phase
The aim of the final two sessions is to develop a plan of action for the maintenance of gains and for relapse prevention. Patients practice with their misophonia triggers and exercises are done in real-life situations (e.g., visiting a food court). A list of remaining safety and avoidance behavior is made and patients make a specific plans to reduce their maladaptive misophonia behavior. This phase involves collaboration of the system. Patients and their close relatives practice together at home. For example, a spouse is “allowed” to make trigger sounds for a limited period of time, while the patient applies attention training or counterconditioning. The time of practice is gradually extended conform inhibitory learning principles.
Treatment is evaluated by discussing the effect of the different interventions, providing feedback for the therapists and a final measure of the misophonia symptom questionnaire (AMISOS-R) and possibly of general psychopathology (SCL-90) or quality-of-life (SDS) questionnaires.
Overview of the Protocol
The protocol is designed for a closed group of maximum nine patients with seven weekly meetings and one follow-up meeting after 3 weeks. Therapy sessions last 180 min with a short break. The manual has specific instructions for each session (e.g., with a set time for each intervention and fully written exercises). CBT consists of four main components: stimulus manipulation, counterconditioning, arousal reduction, and task concentration exercises. In the most recent version two smaller elements are added: re-evaluating (eating) norms and stress reduction. Matching themes are, respectively, Perception, Conditioning, Stress, Attention, and Norms. In our center, the practical exercises, like task concentration exercises, are guided by psychomotor therapists in an exercise room, but this is not a necessity. Table 2 offers an overview of the sessions including themes, psychoeducation, in session work and homework assignments. The time of each procedure is provided in minutes. The time displayed at “Homework” refers to the explanation of the assignments. It should be noted there is a need for flexibility and the manual should be used as a guide.
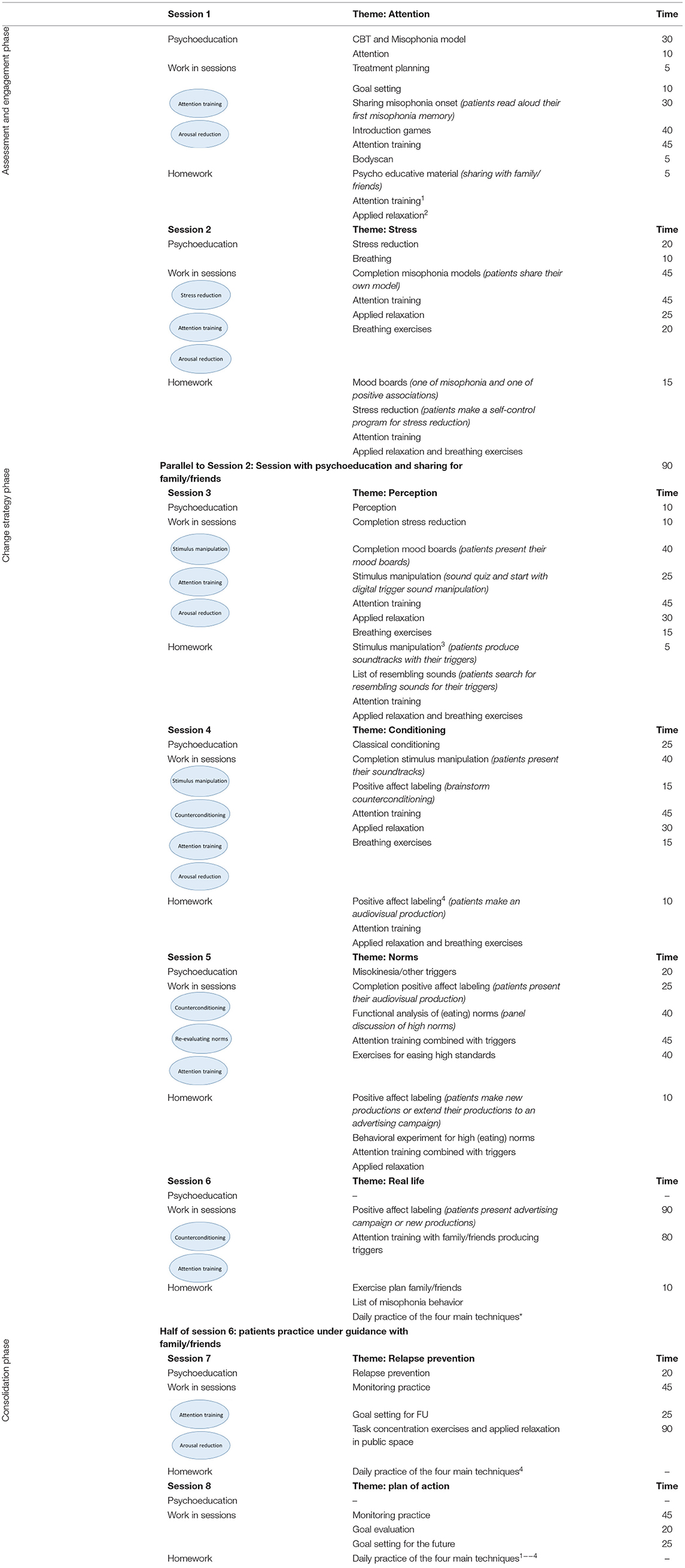
Table 2. Overview treatment protocol per session.
In the next section, we will discuss each intervention and illustrate the interventions with the clinical case vignette of Charlotte. All interventions are displayed within Figures 2, 3.
Stimulus Manipulation
In stimulus manipulation the ambiguity of sounds is used as stimulus control (thus intervening on the CS). The ambiguity of sounds confuses and/or produces humor. This property of sound is illustrated by a quiz in which patients have to guess different (trigger-) sounds. Patients learn other interpretations of their trigger sounds and manipulate their trigger sounds, by editing volume or speed or merging it in different sounds or music.
For example, the sound of sniffing resembles the sound of scratching a record much like a musical DJ would do, so Charlotte mixed her colleagues' sniffing sounds into a scratched music number. When she could not see the “sniffer” but hears a sniff, she learned to imagine it was paper ripping. See for an illustration of stimulus manipulation Supplementary Video 1.
Counter Conditioning
The intervention of counterconditioning is used to neutralize the negative affective-evaluation of misophonia triggers (hence intervening on the UCS/UCR). This intervention shows similarities with the procedure of COMET (34). Patients produce videos where powerful personal positive images (e.g., two favorite nieces with rain boots jumping up and down in a mud puddle) are combined with the aversive misophonia trigger (e.g., food chewing) emerging with their favorite music. These videos are part of a large “campaign” with images, slogans, messages on their phone, in their house and at work, to maximize the positive affect labeling. For stimulus manipulation and counterconditioning different digital editing programs for sounds and videos can be used, for instance the free audio editing software “Audacity.” Patients who are not digitally skilled or do not have access to these programs, are encouraged to ask their close relatives for help. During therapy the group members often help each other as well. And it is almost always possible to improvise with the use of mobile phones.
Charlotte produced a video of taped breathing sounds of her spouse and edited a personal diving video of her favorite holiday with the song “A beautiful day” from the band U2. She watched the video every day, but was also reminded and counter conditioned by coral next to her bed, a picture of her wearing a diving mask as background on her phone and a quote with positive self-verbalization (“Just breathe!”) with lipstick on her mirror. See for an illustration of counterconditioning Supplementary Videos 2, 3.
Arousal and Stress Reduction
Arousal reduction consists of breathing techniques, progressive muscle and passive relaxation, applied relaxation techniques and mindfulness techniques (35). Initially, patients learn to reduce arousal in a normal state, later they learn to relax in a state of arousal caused by misophonic triggers. Throughout the entire treatment arousal reduction is a part of the sessions. These techniques intervene on the CR.
Stress reduction is based on an intervention for symptom reduction from the burn-out protocol (36). Patients learn through self-control techniques [e.g., (37)] to recognize symptoms of stress and manage their stress levels by either taking relaxing measures or by reducing (work-)load. Mild stress levels require small measures and higher levels require more drastic measures. Patients are made aware of the, often precarious, balance between relaxation and stress and are, if necessary, invited to make more structural changes in their work-life balance.
Charlotte noticed by registering her levels of stress that her perceived average stress level was too high. Because of her perfectionism and high standards, she often worked late after putting her children to bed. This resulted in little time to relax. She discovered the impact of stress on her misophonia; dinners on Fridays following a busy week were more difficult than on Wednesdays, when she had the afternoon off. She was convinced she had to reduce stress and made a self-control program, with signals of increasing stress (such as tension headache) and increasing measures for more relaxation (for example taking a massage or bath) or less load (such as postponing a deadline), resulting in more spare time and lower stress levels.
Whereas, breathing sounds of her spouse were a trigger for Charlotte, she learned to relax by listening to her own breathing sounds with diaphragmatic breathing. She became very skilled in applied relaxation, as she practiced this during all her breaks at her work at the law firm.
Attention Training
With task concentration exercises patients learn to control their attention and to shift their focus from the misophonia triggers toward the task. This technique intervenes on the CS, similar to stimulus manipulation. Difficulty of exercises gradually increases, as in the CBT protocol for social anxiety (38). First patients learn to switch their attention in situations not related to misophonia to gain experience with controlling their focus. Then, when patients are more skilled, they practice being confronted with misophonia triggers in controlled situations. Finally, they apply the attention training in real-life misophonia situations.
Charlotte first used her love for classical music to control her attention. Switching between the different instruments was easy. She practiced with shifting focus from the environment (sounds of the clock, pen clicking, or the ventilation system) to the task, for example playing badminton. At home she practiced with shifting focus from her husbands' breathing sounds to a horror movie and from eating sounds of commuters on the train to a Sudoku puzzle.
Re-evaluating (Eating) Norms
This intervention consists of different exercises to challenge, unconscious, assumptions and norms about eating habits or other misophonia triggers, such as sniffing. Decisional balance exercises or discussions about norms are done. Patients debate about for example the proposition: “Making eating sounds is never allowed!” This technique intervenes on the UCS/UCR.
To experience the burden of high norms and (other people's) rules, a ball game “the game without rules” is introduced. Patients can introduce new game rules, by stopping the game and putting the rule to the vote. This often results in discussion and there's no room left for playing and having fun. Finally, patients are also challenged to break their own (eating) norms in a behavioral experiment, since these norms maintain the hyper focus on triggers.
Charlotte always avoided public transport, because she detested and judged commuters who were eating in the train. She was challenged to eat a bag of her favorite crisps on the train when she was hungry. Even though she felt like a criminal at first (which amused her), she could really enjoy the crisps and could therefore slightly imagine why commuters eat while traveling.
Results
Development and Effectivity of the Protocol
The original manual for G-CBT was the result of years of clinical practice. Between 2011 and 2021 over 1,200 patients referred from all parts of the Netherlands with misophonia were treated within our psychiatry department. Different CBT interventions, among which cognitive therapy, exposure, and imagery rescripting, were investigated, but did not show a positive effect on the symptoms. Years of trial and error finally resulted in a mix of CBT interventions who were fine-tuned for treating misophonia in the most effective way. This protocol has been most used in the treatment of misophonia patients in clinical practice so far.
This G-CBT manual has been used in two clinical trials by our research group where it has been efficacious in treating misophonia in Dutch adults (20, 39). The effectiveness of the first version of this protocol for group treatment has been examined with good results (39). Almost half of the 90 patients studied had over 30% symptom reduction (P < 0.001) and were clinically assessed as “much improved” or “very much improved” on the Clinical Global Impression-Improvement (CGI-I) (40).
The protocol, with the addition of stress reduction and re-evaluating (eating) norms, has also been studied in a randomized controlled trial (RCT) in 54 patients with positive effects which were preserved at 1-year follow-up (20). In comparison with a waiting list control group treatment was effective with much to very much clinical improvement in 37% of the studied patients (P < 0.001) and a very large standardized effect size (d = 1.97). In all completers, on average symptoms were reduced with 28% after treatment (P < 0.001) and 1 year after treatment symptoms were reduced with 24% (P < 0.001). Thirty seven percent of the completers did not meet diagnostic criteria for misophonia any more post-treatment.
Qualitative Evaluation of the Protocol
Treatment acceptability was quite high; 65% was (very) satisfied and 25% was neutral, and treatment was rated by patients with a mean of 6.7 out of 10 (20).
The extent to which the various techniques were used and the experienced effectivity of all techniques were systematically assessed in the RCT by qualitative questionnaires post treatment (n = 42). Results show two of the four main interventions are applied less and are evaluated negatively. The frequencies in which the various interventions are applied are shown in Figure 4. A remarkable 48.8% “rarely to never” applies stimulus manipulation and counterconditioning. The most applied interventions are relaxation training and attention training which are used “very often” or “always” by 34.9%. Only 4.7% (attention training) to 9.3% (relaxation training) reports to “rarely to never” use these interventions.
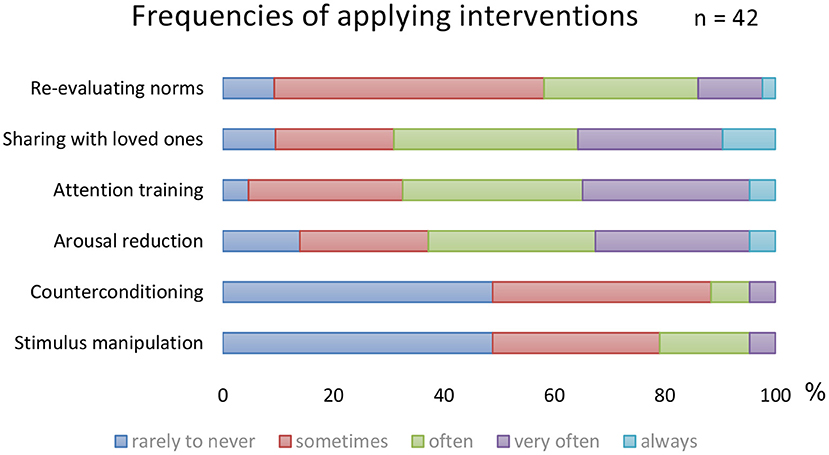
Figure 4. Frequencies of the CBT interventions.
In Figure 5, the results are displayed of the following question: “To what amount did the intervention contribute to your recovery?” Arousal (and stress) reduction and attention training are most highly valued. In additional comments 17 of 43 patients (40%) indicated the group element and peer support as substantially contributing to their recovery.
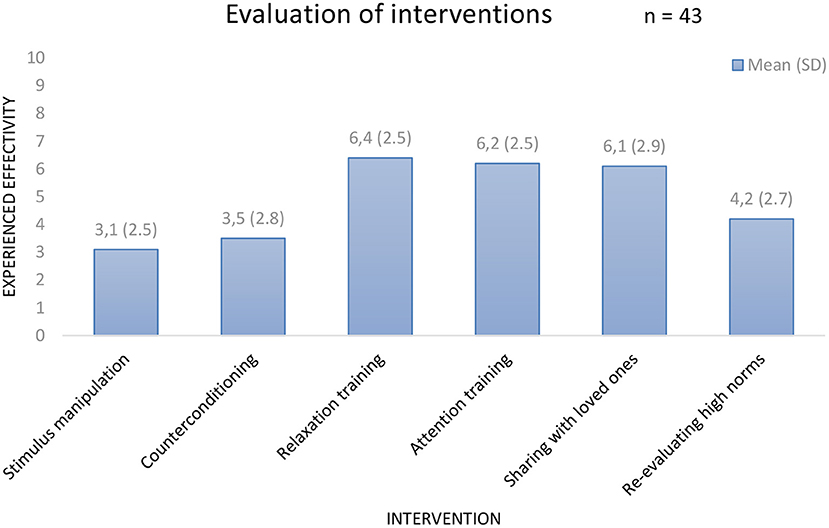
Figure 5. Evaluation of the CBT interventions.
Results Clinical Case Study
Results of the protocol are illustrated by the case study of Charlotte. Even though Charlotte was anxious at first to adopt new triggers from other patients, she did not. After treatment she experienced a large reduction in misophonia symptoms. Although she was still experiencing some symptoms, the relationship with her husband improved significantly. After treatment Charlotte was able to eat and sleep together again. She could make jokes with her husband about her misophonia (for example saying “Just breathe!,” when she got annoyed) and the tension at home decreased. She lost the hyper focus on most trigger sounds. The eating sounds of her mother remained a trigger for Charlotte, but she no longer avoided eating with her parents. She was able to cope in a functional manner when an emotional reaction was provoked. Charlotte stated she felt more relaxed and free in social interactions with other people.
At session 1, 4, 7, and 8 progress was monitored by two questionnaires; the AMISOS-R and SCL-90. Charlotte started treatment with severe to extreme misophonia (range 31–40) and at the end of treatment her symptoms were reduced to mild misophonia (range 11–20). Also, general psychopathology decreased from a very high level to a level above average (see Figure 6).
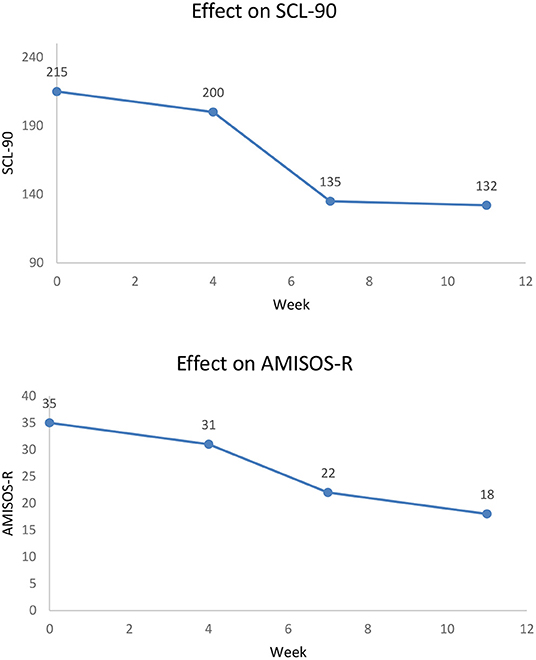
Figure 6. Symptoms Charlotte during G-CBT.
Discussion
This paper introduced the protocol for G-CBT for misophonia. The interventions are based on the revised diagnostic criteria (3). The G-CBT protocol includes various interventions: stimulus manipulation, counterconditioning, arousal and stress reduction, task concentration exercises, and re-evaluating (eating) norms. While the case study described in this paper responded to all interventions and was successfully treated by G-CBT, most patients benefit from various combinations of the interventions. More research to which elements of the treatment have most effect (on which type of patient) is needed, especially because of the lower evaluation and use of two of the main techniques. Different elements could be compared to each other or patient groups could be matched to specific interventions. For instance patients with disgust [64% according to (3)] might profit more from counterconditioning then patients without disgust. Since misophonia is an interpersonal problem with a large impact on all interactions, group therapy is very suitable. Close relatives are involved throughout the treatment, so patients are motivated to fight their misophonia together instead of fighting with each other or fighting internally.
The advantages of group treatment for misophonia consists of peer support, more opportunity to practice under guidance, more natural exposure and cost effectiveness. Compared to, for example, the case study of Muller et al. (18) with a duration of 24 sessions of 45 min of individual therapy (18 therapist-hours per patient) our treatment is brief with a duration of eight sessions of 180 min using less time per patient (6 therapist-hours per patient; in a group of eight patients with two therapists).
A first limitation of group treatment is the requirement of a number of misophonia patients. In our experience misophonia patients only admit themselves in large numbers to a center when this facility identifies itself as a misophonia treatment center. However, the described interventions can all be applied in individual treatment as well. A second limitation is the limited possibility to adjust to individual needs of patients. For example, if a patient has misophonia-related emotionally disturbing memories adding eye movement desensitization and reprocessing (EMDR) therapy as a trauma-focused approach may be considered (41). Such an additional intervention can more easily be integrated in individual therapy. A third limitation is possibly generalizability, since this protocol has been investigated in especially Dutch patient groups, with a relatively high percentage of females and Caucasians (20, 39).
The protocol has been used by one other research group so far; in a single case study by Roushani and Honarmand (42). Three patients were treated individually, but according to our protocol, with positive effect. Two of the three patients had a recovery percentage of 42–43% on anger. Further, the proposed treatment paradigm for misophonia by Frank and McKay (26) is largely based on the present protocol and includes (besides exposure using inhibitory learning): counter conditioning, stimulus manipulation and stress management in 12 sessions. Preliminary results of the 18 patients enrolled in their RCT have not been published yet. Hopefully this synopsis will contribute to the implementation of (G-)CBT in clinical trials for misophonia.
Conclusion
In this article we have presented our treatment protocol for systemic G-CBT for misophonia, which has been evaluated in two clinical trials and has been used in clinical practice for treating over 1,200 patients. Therefore, this protocol is the worldwide most used intervention for misophonia with the highest level of evidence. In this article we have also included a qualitative evaluation of the protocol.
This protocol is based on the revised diagnostic criteria for misophonia and classical and operant learning principles. All elements are described in detail and are illustrated with a case study. It is relatively easy to adjust the group protocol to an individual approach. Knowledge of the principles of CBT, as well as a phased approach should help to maximize results.
With this treatment manual, we hope to encourage other investigators for more clinical trials and to inspire clinicians working with misophonia patients to implement (G-)CBT.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
IJ: conceptualization, writing—original draft, writing—review, and editing. NV and DD: conceptualization, supervision, writing—review, and editing. AL, MP, and SS: conceptualization. AS: conceptualization and writing—review. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We are very grateful to all misophonia patients for their contribution in the development of this protocol. We also thank our colleagues from the misophonia treatment team.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.794343/full#supplementary-material
Supplementary Video 1. Example of stimulus manipulation: audio fragment DJ sniffing.
Supplementary Video 2. Example of counterconditioning: video fragment Baby sniffing.
Supplementary Video 3. Example of counterconditioning: video fragment Bird coughing.
References
1. Jastreboff MM, Jastreboff PJ. Components of decreased sound tolerance: hyperacusis, misophonia, phonophobia. ITHS News Lett. (2001) 2:1–5.
2. Schröder A, Vulink N, Denys D. Misophonia: diagnostic criteria for a new psychiatric disorder. PLoS ONE. (2013) 8:e54706. doi: 10.1371/journal.pone.0054706
3. Jager I, de Koning P, Bost T, Denys D, Vulink N. Misophonia: phenomenology, comorbidity and demographics in a large sample. PLoS ONE. (2020) 15:e0231390. doi: 10.1371/journal.pone.0231390
4. Swedo S, Baguley DM, Denys D, Dixon LJ, Erfanian M, Fioretti A, et al. A consensus definition of misophonia: using a delphi process to reach expert agreement. medRxiv [preprint]. (2021). doi: 10.1101/2021.04.05.21254951
5. Schröder A, van Wingen G, Eijsker N, San Giorgi R, Vulink NC, Turbyne C, et al. Misophonia is associated with altered brain activity in the auditory cortex and salience network. Sci Rep. (2019) 9:1–9. doi: 10.1038/s41598-019-44084-8
6. Schröder A, San Giorgi R, van Wingen G, Vulink N, Denys D. Impulsive aggression in misophonia: results from a functional magnetic resonance imaging study. Basic Clin Neurosci. (2019) 25:S307–8. doi: 10.1016/S0924-977X(15)30374-6
7. Cavanna AE, Seri S. Misophonia: current perspectives. Neuropsychiatr Dis Treat. (2015) 11:2117. doi: 10.2147/NDT.S81438
8. Wu MS, Lewin AB, Murphy TK, Storch EA. Misophonia: incidence, phenomenology, and clinical correlates in an undergraduate student sample. J Clin Psychol. (2014) 70:994–1007. doi: 10.1002/jclp.22098
9. Zhou X, Wu MS, Storch EA. Misophonia symptoms among Chinese university students: Incidence, associated impairment, and clinical correlates. J Obsess Compuls Relat Disord. (2017) 14:7–12. doi: 10.1016/j.jocrd.2017.05.001
10. Naylor J, Caimino C, Scutt P, Hoare DJ, Baguley DM. The prevalence and severity of misophonia in a UK undergraduate medical student population and validation of the amsterdam misophonia scale. Psychiatr Q. (2020) 92:609–19. doi: 10.1007/s11126-020-09825-3
11. Sanchez TG, da Silva FE. Familial misophonia or selective sound sensitivity syndrome: evidence for autosomal dominant inheritance?. Braz J Otorhinolaryngol. (2017) 84:553–9. doi: 10.1016/j.bjorl.2017.06.014
12. Rouw R, Erfanian M. A large-scale study of misophonia. J Clin Psychol. (2017) 74:453–79. doi: 10.1002/jclp.22500
13. Jastreboff PJ, Jastreboff MM. Treatments for decreased sound tolerance (hyperacusis and misophonia). In: Seminars in Hearing, Vol. 35. Thieme Medical Publishers (2014). p. 105–20. doi: 10.1055/s-0034-1372527
14. Bernstein RE, Angell KL, Dehle CM. A brief course of cognitive behavioural therapy for the treatment of misophonia: a case example. Cogn Behav Ther. (2013) 6:e10. doi: 10.1017/S1754470X13000172
15. McGuire JF, Wu MS, Storch EA. Cognitive-behavioral therapy for 2 youths with misophonia. J Clin Psychiatry. (2015) 76:573–4. doi: 10.4088/JCP.14cr09343
16. Reid AM, Guzick AG, Gernand A, Olsen B. Intensive cognitive-behavioral therapy for comorbid misophonic and obsessive-compulsive symptoms: A systematic case study. J Obsess Compuls Relat Disord. (2016) 10:1–9. doi: 10.1016/j.jocrd.2016.04.009
17. Altinoz AE, Unal NE, Altinoz ST. The effectiveness of cognitive behavioral psychotherapy in misophonia: a case report. J Clin Psychiatry. (2018) 21:414–7. doi: 10.5505/kpd.2018.18480
18. Muller D, Khemlani-Patel S, Neziroglu F. Cognitive-behavioral therapy for an adolescent female presenting with misophonia: a case example. Clin Case Stud. (2018) 17:249–58. doi: 10.1177/1534650118782650
19. Van Loon A, Van der Pol M, Slaghekke S, Van der Meer C, Schekman E, Nieuwendijk E, et al. Misofonie: Behandelprotocol in 8 Sessies [Misophonia: Treatment Protocol of 8 Sessions]. Amsterdam: Boom Publishers (2019).
20. Jager IJ, Vulink NC, Bergfeld IO, van Loon AJ, Denys DA. Cognitive behavioral therapy for misophonia: a randomized clinical trial. Depress Anxiety. (2020) 38:708–10. doi: 10.1002/da.23127
21. Schneider RL, Arch JJ. Letter to the editor: potential treatment targets for misophonia. Gen Hosp Psychiatry. (2015) 37:370–1. doi: 10.1016/j.genhosppsych.2015.03.020
22. Vrana SR. Lessons Learned From Other Conditions: Anxiety Disorders. Chicago, IL: Milken Institute Misophonia Research Retreat (2018).
23. Webber TA, Storch EA. Letter to the editor: toward a theoretical model of misophonia. Gen Hosp Psychiatry. (2015) 37:369–70. doi: 10.1016/j.genhosppsych.2015.03.019
24. Rabasco A, McKay D. Exposure therapy for misophonia: concepts and procedures. J Cogn Psychother. (2021) 35:156–66. doi: 10.1891/JCPSY-D-20-00042
25. Cecilione JL, Hitti SA, Vrana SR. Treating adolescent misophonia with cognitive behavioral therapy: considerations for including exposure. Clin Case Stud. (2021) 21:175–91. doi: 10.1177/15346501211045707
26. Frank B, McKay D. The suitability of an inhibitory learning approach in exposure when habituation fails: a clinical application to misophonia. Cogn Behav Pract. (2019) 26:130–42. doi: 10.1016/j.cbpra.2018.04.003
27. Cowan EN, Marks DR, Pinto A. Misophonia: a psychological model and proposed treatment. J Obsess Compuls Relat Disord. (2022) 32:100691. doi: 10.1016/j.jocrd.2021.100691
28. Edelstein M, Brang D, Rouw R, Ramachandran VS. Misophonia: physiological investigations and case descriptions. Front Hum Neurosci. (2013) 7:296. doi: 10.3389/fnhum.2013.00296
29. Schröder A, Spape M. Amsterdam Misophonia Scale - Revised (AMISOS-R) [Measurement Instrument]. Retrieved from: https://journals.plos.org/plosone/article/file?type=supplementaryandid=info(2014) (accessed October 13, 2021).
30. Derogatis LR, Lipman RS, Covi L. The SCL-90: an outpatient psychiatric rating scale-preliminary report. Psychopharmacol Bull. (1973) 9:13–8.
31. Sheehan DV. Sheehan disability scale. In: Handbook of Psychiatric Measures. Washington, DC: APA (1983) p. 100–2.
32. Davis M, Eshelman ER, McKay M. The Relaxation and Stress Reduction Workbook. Oakland: New Harbinger Publications (2008).
33. Craske MG, Treanor M, Conway CC, Zbozinek T, Vervliet B. Maximizing exposure therapy: an inhibitory learning approach. Behav Res Ther. (2014) 58:10–23. doi: 10.1016/j.brat.2014.04.006
34. Korrelboom K, Jong M, Huijbrechts I, Daansen P. Competitive memory training (COMET) for treating low self-esteem in patients with eating disorders: a randomized clinical trial. J Consult Clin Psychol. (2009) 77:974–80. doi: 10.1037/a0016742
35. Hayes SC, Hofmann SG, editors. Process-Based CBT: The Science and Core Clinical Competencies of Cognitive Behavioral Therapy. New Harbinger Publications.
36. van Dam A, Keijsers GPJ, Kriens S, Boelaars VAJM, Vossen CJC. Protocollaire behandeling van patiënten met somatisch-symptoom stoornis persisterend type met aanhoudende werkgerelateerde vermoeidheidsklachten (burn-out) - Protocolled treatment of patients with somatic symptom disorder persistent type with workrelated fatigue (burnout). In: Protocollaire Behandelingen Voor Volwassenen Met Psychische Klachten III - Protocolled Treatments for Patients With Psychological Complaints III. Keijsers G, van Minnen A, Verbraak M, Hoogduin C, Emmelkamp P, editors. Amsterdam: Uitgeverij Boom (2017). p. 63–147.
37. Mahoney MJ, Thoresen CE. Behavioral self-control: power to the person. Educ Res. (1972) 1:5–7. doi: 10.3102/0013189X001010005
38. Wild J, Clark DM. Experiential exercises and imagery rescripting in social anxiety disorder. In: Working With Emotion in Cognitive-Behavioral Therapy: Techniques for Clinical Practice. New York, NY: Guilford Press (2014). p. 216.
39. Schröder AE, Vulink NC, van Loon AJ, Denys DA. Cognitive behavioral therapy is effective in misophonia: an open trial. J Affect Disord. (2017) 217:289–94. doi: 10.1016/j.jad.2017.04.017
40. Guy WBRR. CGI, Clinical Global Impressions. ECDEU Assessment Manual for Psychopharmacology. Rockville: National Insitute of Mental Health (1976). p. 218–22. doi: 10.1037/e591322011-001
41. Jager I, Vulink N, de Roos C, Denys D. EMDR therapy for misophonia: a pilot study of case series. Eur J Psychotraumatol. (2021) 12:1968613. doi: 10.1080/20008198.2021.1968613
Keywords: misophonia, cognitive-behavioral therapy (CBT), protocol and guidelines, group treatment methods, psychotherapy
Citation: Jager I, Vulink N, van Loon A, van der Pol M, Schröder A, Slaghekke S and Denys D (2022) Synopsis and Qualitative Evaluation of a Treatment Protocol to Guide Systemic Group-Cognitive Behavioral Therapy for Misophonia. Front. Psychiatry 13:794343. doi: 10.3389/fpsyt.2022.794343
Received: 13 October 2021; Accepted: 08 June 2022;
Published: 28 June 2022.
Edited by:
Angela Fang, University of Washington, United StatesReviewed by:
Seth Davin Norrholm, Wayne State University, United StatesLydia Gimenez-Llort, Autonomous University of Barcelona, Spain
Copyright © 2022 Jager, Vulink, van Loon, van der Pol, Schröder, Slaghekke and Denys. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Inge Jager, aS5qLmphZ2VyQGFtc3RlcmRhbXVtYy5ubA==