 Yiwei Gu
Yiwei Gu ChangJing Wu1
ChangJing Wu1 Feng Qin
Feng Qin Jiuhong Yuan
Jiuhong Yuan
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Psychiatry, 26 May 2022
Sec. Sleep Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.766639
This article is part of the Research TopicPrecision Medicine in Obstructive Sleep Apnea (OSA)View all 6 articles
Erectile dysfunction (ED) is a disease with a wide scope of etiologies. Obstructive sleep apnea (OSA) is considered one of the risk factors for ED and is less studied. A growing lot of evidence show an association between OSA and ED. This study provides an updated review of the relationship between ED and OSA and the possible physiological mechanisms of ED in patients with OSA based on the current evidence. In clinical interviews, patients with ED may benefit from a sleep evaluation. However, further clinical investigations and more basic research are needed to illustrate the relationship between ED and OSA.
Obstructive sleep apnea (OSA) is characterized by the repeated episodic collapse of the upper airway, leading to arousal from sleep and recurrent oxyhemoglobin desaturation (1). When OSA events occur, the oropharynx at the back of the throat collapses, causing wakefulness, decreased oxygen saturation, or both, which leads to sleep Fragmentation. An estimated 936 million individuals aged 30–69 years worldwide were found to have obstructive sleep apnea; 425 million adults aged 30–69 years have moderate to severe obstructive sleep apnea globally. The number of affected individuals was highest in China, followed by the USA, Brazil, and India (2). The prevalence of OSA in men increases with age, from 10% among those aged 30 to 49 to 17% among those aged 50 to 70, with approximately 24 million persons undiagnosed in the United States (3). OSA has several common sleep and daytime symptoms although the symptoms reported by patients may vary. During sleep, snoring is one of the most collective symptoms and is bothersome to others. The usual symptoms of OSA include inordinate daytime sleepiness or weariness, which reduces the quality of life. Despite acquiring the recommended 7 to 9 h of sleep, feeling unrefreshed is also common in patients with OSA. The severity of OSA is commonly classified according to the apnea-hypopnea index (AHI) value, which is defined as the number of apnea plus hypopnea episodes per hour of sleep. According to expert consensus, a normal AHI is <5 events per hour, 5 to 14.9 is considered mild OSA, 15 to 29.9 is considered moderate OSA, and at least 30 is considered severe OSA (4). A lack of consistency in the definitions of hypopnea influences the AHI value (5).
Erectile dysfunction (ED) has been described as the inability to obtain or maintain a sufficiently firm erection for satisfactory sexual intercourse (6). In the Massachusetts Male Aging Study, the prevalence of ED among men aged 40 to 70 was ~50%, and in the same age group, the prevalence of complete ED was 15% (7). The pooled prevalence of ED was 49.69% in mainland China and increased with age (8). ED is generally considered to be associated with natural aging, other diseases, medical treatment, or changes in emotional state (9).
Regardless of the origin, ED or OSA has a strong negative influence on health and quality of life. In the past, OSA was often overlooked when patients with ED sought treatments. However, the relationship between OSA and ED has been increasingly studied since Guilleminault et al. (10) first reported an underlying association between ED and OSA in 1977. Both disorders are known to be associated with a variety of systemic diseases (e.g., diabetes, hypertension, depression, and other psychological factors) (11). A number of scholars have evaluated the prevalence of ED in patients with OSA (12, 13), and possible mechanisms have been proposed, including an abnormal sympathetic nervous system, endothelial dysfunction, chronic intermittent hypoxia, sleep fragmentation, and/or rapid eye movement (REM) sleep disturbances (14). In this study, we summarized and updated current evidence for OSA and ED and the possible mechanisms underlying the development of ED in patients with OSA, which may help prioritize public health policies and fund public health initiatives and health care planning.
We conducted a thorough literature search based on computerized databases, including PubMed, EMBASE, and SCOPUS, for English-language studies on the association of ED with OSA and related mechanism studies without time restrictions and searched the references of the retrieved papers for additional relevant articles. After the first search, 329 articles were identified. Subsequently, 33 articles were included in this review. The characteristics of the included studies are presented in Tables 1, 2.
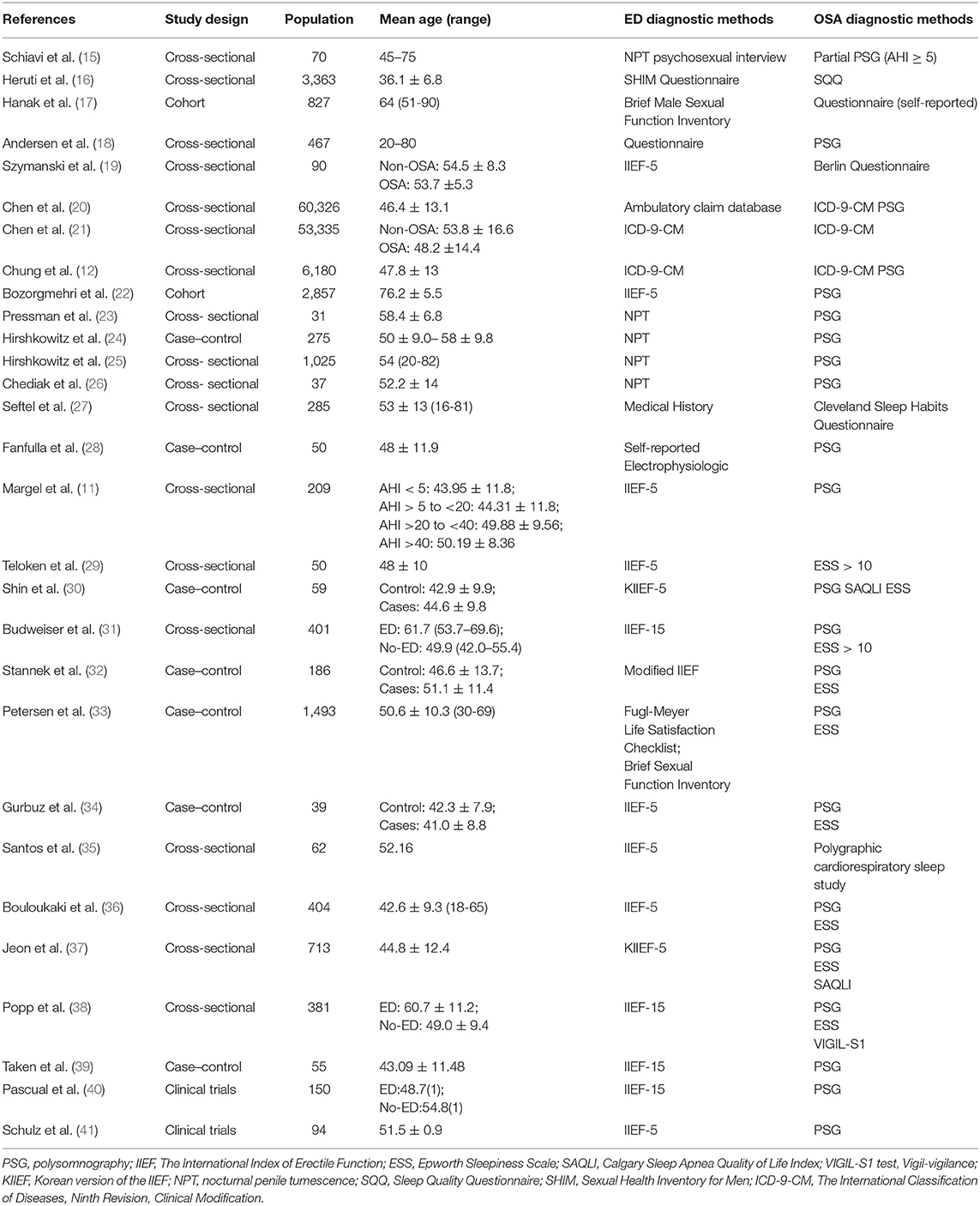
Table 1. The characteristics of the included clinical studies.
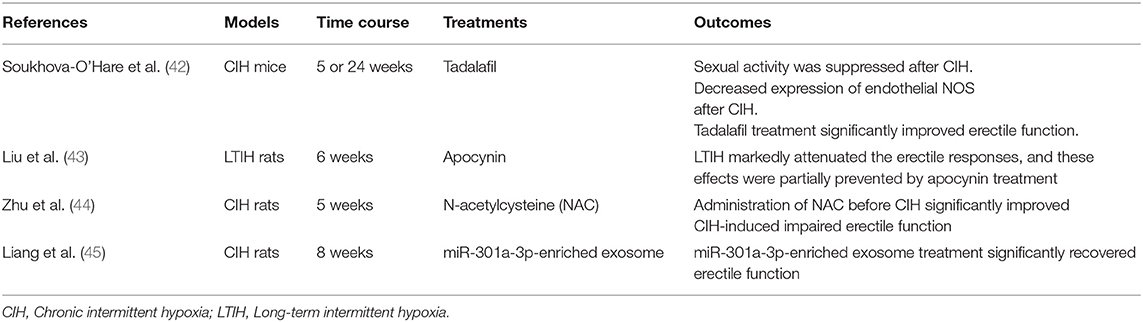
Table 2. The characteristics of the included basic science studies.
A total of nine studies (12, 15–22) evaluated the relationship between OSA and ED in the general population. Three studies (15, 17, 22) reported no statistically significant association between OSA and ED. Szymanski et al. (19) reported a higher prevalence of ED in patients with OSA with a history of myocardial infarction. The severity of OSA was found to be positively correlated with low sexual satisfaction (17). Chen et al. (20) reported an increasing ED incidence in the Chinese OSA population. Another study (21) showed that the incidence of ED was higher in patients with OSA after adjusting for relevant confounders for ED or OSA.
The frequency of OSA in patients with ED was investigated in five studies, with a range of 28–78.92% (23–27). Hirshkowitz et al. (24) found that hypertensive patients with ED had more severe OSA than patients without ED, and abnormal respiratory activity during sleep was found in both hypertensive and normotensive groups with erectile problems. One study (25) showed that the prevalence of OSA in 1,025 patients with ED was 43.8% with an AHI ≥ 5, 27.9% with an AHI ≥ 10, and 19.6% with an AHI ≥ 15, which increased dramatically with increased age in patients with ED. Seftel et al. (27) found that persistent waketime sleepiness or fatigue is not associated with ED.
A total of thirteen studies (11, 28–39) reported ED among sleep clinic populations. The incidence of ED in patients with OSA ranges from 40.9 to 80% (19, 28–31, 34–39). Fanfulla et al. (28) found an association between OSA severity and altered bulbocavernosus reflex. Conflicting results existed regarding the relationship between OSA severity and ED. Furthermore, three studies (11, 32, 36) reported that patients with more severe AHI showed ED with higher severity. Jeon et al. (37) suggested that both a low sleep apnea quality of life index and depressive symptoms were independent risk factors for ED in patients with OSA. Budweiser et al. (31) found that waketime sleepiness was not associated with ED. Popp et al. (38) investigated the association between ED and impaired vigilance performance among patients with OSA and found that the severity of erectile function was significantly associated with vigilance performance regardless of other known common risk factors for ED or OSA.
There are two studies of clinical trials evaluating the association between ED and OSA (40, 41). Pascual et al. (40) conducted a cross-sectional study assessing ED prevalence in patients with OSA and found that the prevalence of ED was 51% in patients with OSA. This study suggested the potential usefulness of ED screening in patients with OSA. In another study, 94 men with severe OSA were prospectively evaluated for the presence of ED. The result showed that 64 of the 94 patients were diagnosed to suffer from ED (41).
Some common shortcomings of quality assessment are evident among these observational studies: inadequate control selection, incomplete and short-term follow-up, and oversight of assessing confounding variables such as smoking, alcohol consumption, and testosterone levels. In addition, ED was diagnosed based on interviews or questionnaires (for instance, the international index of erectile function-5, IIEF-5) in most studies (46). The IIEF-5, which was developed in 1997, is a tool widely used to assess erectile function (6). However, questionnaire-based evaluations are very subjective and can be affected by educational level (47). Some specialized diagnostic tests, including the nocturnal penile tumescence and rigidity (NPTR) test and Doppler ultrasound, are also used to diagnose ED. The NPTR is generally used to distinguish psychogenic ED from organic ED (48). Hence, more prospective studies are needed to elucidate the relationship between ED and OSA.
Although a high prevalence of ED in the male population with OSA has been detected, no literature reports the precise mechanism for the development of ED in patients with OSA. Penile erection is a neurovascular event modulated by psychological factors and hormonal status. An erection develops after sexual stimulation, which is accompanied by an increase in intracellular cyclic guanosine monophosphate with neurotransmitters and relaxing factors from the cavernous nerve terminal and endothelial cells in the penis, resulting in a several-fold increase in the blood flow in the penis, and penile tunica albuginea occludes venous outflow (49). Therefore, any process that impairs either the neural or vascular pathways that contribute to erection can lead to ED. ED can be classified as psychogenic, organic (neurogenic, hormonal, arterial, cavernosal, or drug-induced), or mixed psychogenic and organic mechanisms. The risks of OSA and ED share some factors, including alcohol abuse, cigarette smoking, and obesity. Some mechanisms have been proposed for ED in OSA, including hormonal, vasculogenic, neurogenic, and psychogenic mechanisms.
The leading theory is that frequent hypoxic events during sleep are an independent risk factor associated with ED (31). A cascade of vascular and inflammatory events is activated by intermittent hypoxic events, including downregulation of circulating nitric oxide (NO) levels, vascular endothelial dysfunction, and the release of oxygen radicals. In the physiology of erection, NO is a crucial transmitter. A decrease in circulating NO levels may also contribute to diminishing nocturnal penile tumescence (50, 51). Endothelin is a potent vasoconstrictor that is stimulated and produced by disturbed endothelial cell regulation and hypoxia and can impair penile tumescence, thus contributing to ED in patients presenting OSA (52).
Neural mechanisms, including peripheral neuropathy and high sympathetic activities, have been considered potential causes of ED in patients with OSA (28, 53). The severity of peripheral nerve axon and myelin injury contributes to impaired erection (54). Fanfulla et al. (28) highlighted peripheral nerve involvement by evaluating the somatosensory evoked potentials of the pudendal nerve and the bulbocavernosus reflex in patients with OSA. Patients with OSA have been reported to have higher sympathetic activity during sleep, especially rapid eye movement sleep (55). The elevated level of circulating norepinephrine not only has an effect on erectile function but also leads to hypertension, which is a risk factor associated with penile arterial insufficiency (56).
Psychological mechanisms have also been proposed. Depression is a common comorbidity in men with ED (57) and may result in ED by reducing sexual desire and/or inhibiting parasympathetic nerve activities (58). Additionally, OSA can cause psychological changes and neural impairment (59). Peppard et al. (60) found a causal link between sleep-related breathing disorder (SRBD) and depression in their long-term investigation. Therefore, individuals with OSA may be at an increased risk of developing psychogenic or mixed psychogenic and organic ED.
Additionally, a hormonal effect of testosterone has been proposed as a potential mechanism for ED with OSA. Testosterone is the primary reproductive hormone in men and is secreted through the stimulation of luteinizing hormone and follicle-stimulating hormone. The hypothalamic-pituitary-testicular axis regulates the amount of testosterone synthesis (61–63). Many studies have found that the serum testosterone level of male patients with OSA is low, and the AHI and oxygen saturation index are negatively correlated with testosterone levels (64, 65). Additionally, low testosterone levels are often accompanied by decreased sleep-related erections, notably below 200 ng/dl (66). Gambineri et al. (67) found lower testosterone levels in obese patients with OSA than in obese control patients and a negative correlation between oxygen saturation and testosterone levels. On the other hand, testosterone plays a role in the pathogenesis of sleep apnea, and supplementation with testosterone may aggravate OSA (68). Also, aberrant reproductive hormone secretion may lead to infertility in male patients. A case-control population-based study found that OSA increases the risk of infertility in male patients, and the risk is associated with the OSA exposure time interval (69). Interestingly, sexual dysfunction occurs frequently in men of reproductive age, causing infertility in some instances where ED and premature ejaculation are common types of male sexual dysfunction, which have a prevalence of one in six infertile men (70). There may be a possible link between ED, OSA, and infertility in men, which needs further research to investigate. Recently, new studies showed that the penis may also be an organ with a circadian rhythm and that disruption of the sleep-wake cycle may impair erectile function (71). Sleep fragmentation may disrupt the diurnal rhythm of testosterone levels (72). Normal NPTR includes 3 to 6 periods with tumescence lasting for 10 to 15 min with a rigidity of at least 70% at the penile tip (73). Nocturnal penile tumescence (NPT) can regulate oxygen-required biological processes to protect the integrity of the corpora cavernosa (74). Although the exact regulatory mechanism of NPT is still unclear, some studies have shown that NPT may be related to neurovascular mechanisms and hormone regulation (75). A diminished or an absence of erections is thought to result from a decrease in REM sleep in patients with OSA (76). As the circadian clock has an effect on physiological functions in many tissues (77), Vignozzi et al. (78) proposed whether a penile clock exists. Nocturnal hypoxia effects should not be ignored when investigating potential pathogenic mechanisms underlying ED and OSA. A study demonstrated reciprocal regulation between hypoxia signaling and the circadian clock, where an intact circadian clock could protect heart cells (79). To date, no core circadian rhythm-related factors have been studied in the penis.
However, limited basic research exists regarding the pathophysiologic basis of ED with OSA. OSA is a multicomponent, heterogeneous disease that can lead to a variety of comorbidities. The intricacies of the disease reduce the possibility of patient investigation, particularly at the tissue level, which limits the understanding of the pathophysiology of ED in OSA and the development of specific treatment. Dr. Gozal's group demonstrated that chronic intermittent hypoxemia was associated with decreased libido and reduced expression of endothelial nitric oxide synthase (NOS; eNOS) in the penis in a murine model (42). They also found no changes in testosterone and neuronal NOS (nNOS) and inducible NOS (iNOS) immunoreactivity after intermittent hypoxia. In another study, Liu et al. (43) demonstrated that long-term intermittent hypoxia (LTIH) was associated with a marked influence on erectile function and was attributed to increased NADPH oxidase activity in a rat model of sleep apnea. The same group in 2015 demonstrated that endoplasmic reticulum stress-related cell apoptosis is involved with low levels of constitutive NOS and NO in rats (44). Recently, Liang et al. (45) showed that exosome treatment significantly improved erectile function in LTIH exposure-induced ED rats and corpus cavernous smooth muscle cells (CCSMCs) by inhibiting apoptosis and promoting autophagy, which were associated with the PTEN/hypoxia-inducible factor-1 alpha (HIF-1α) and Toll-like receptor 4 (TLR4) signaling pathways.
Erection, which is a physiological event involving psychological, neurological, endocrinological, and vascular systems, may be influenced by any reduction in this cooperation. Asking about sleep situations seems rational in clinical interviews for ED, and examinations for ED and gonadal suppression should also be recommended for patients who have severe OSA and should be reevaluated after OSA treatment.
Overall, the current evidence suggests that OSA may be a risk factor for ED, and basic research on the mechanisms of ED in OSA is limited. However, since only English-language studies were included in this review, we will broaden our search including different languages in the future. Further clinical trials with good designs and more pathophysiological mechanism studies are needed to elucidate the causes and find new definitive therapies.
YG and CW designed this study. YG, CW, and FQ took part in the data collection and analyzed the data. YG drafted the manuscript. JY revised the final manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the Natural Science Foundation of China (Nos. 81871147 and 82071639) and the Chengdu Science and Technology Program (2019-YFYF-00087-SN).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank American Journal Experts for their assistance with language editing.
1. Speed JS, Hyndman KA, Roth K, Heimlich JB, Kasztan M, Fox BM, et al. High dietary sodium causes dyssynchrony of the renal molecular clock in rats. Am J Physiol Ren Physiol. (2018) 314:F89–98. doi: 10.1152/ajprenal.00028.2017
2. Benjafield AV, Ayas NT, Eastwood PR, Heinzer R, Ip MSM, Morrell MJ, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. (2019) 7:687–98. doi: 10.1016/S2213-2600(19)30198-5
3. Young T, Palta M, Dempsey J, Peppard PE, Nieto FJ, Hla KM. Burden of sleep apnea: rationale, design, and major findings of the Wisconsin Sleep Cohort study. WMJ. (2009) 108:246–9.
4. Ruehland WR, Rochford PD, O'Donoghue FJ, Pierce RJ, Singh P, Thornton AT. The new AASM criteria for scoring hypopneas: impact on the apnea hypopnea index. Sleep. (2009) 32:150–7. doi: 10.1093/sleep/32.2.150
5. Ho V, Crainiceanu CM, Punjabi NM, Redline S, Gottlieb DJ. Calibration model for apnea-hypopnea indices: impact of alternative criteria for hypopneas. Sleep. (2015) 38:1887–92. doi: 10.5665/sleep.5234
6. Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology. (1997) 49:822–30. doi: 10.1016/S0090-4295(97)00238-0
7. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the massachusetts male aging study. J Urol. (1994) 151:54–61. doi: 10.1016/S0022-5347(17)34871-1
8. Wang W, Fan J, Huang G, Zhu X, Tian Y, Tan H, et al. Meta-analysis of prevalence of erectile dysfunction in mainland China: evidence based on epidemiological surveys. Sex Med. (2017) 5:e19–30. doi: 10.1016/j.esxm.2016.10.001
9. National Institutes of Health (NIH) Consensus Conference. NIH consensus conference. impotence. NIH consensus development panel on impotence. JAMA. (1993) 270:83–90. doi: 10.1001/jama.270.1.83
10. Guilleminault C, Eldridge FL, Tilkian A, Simmons FB, Dement WC. Sleep apnea syndrome due to upper airway obstruction. Arch Intern Med. (1977) 137:296–300. doi: 10.1001/archinte.137.3.296
11. Margel D, Cohen M, Livne PM, Pillar G. Severe, but not mild, obstructive sleep apnea syndrome is associated with erectile dysfunction. Urology. (2004) 63:545–9. doi: 10.1016/j.urology.2003.10.016
12. Chung SD, Hung SH, Lin HC, Tsai MC, Kao LT. Obstructive sleep apnea and urological comorbidities in males: a population-based study. Sleep Breath. (2016) 20:1203–8. doi: 10.1007/s11325-016-1336-x
13. Campos-Juanatey F, Fernandez-Barriales M, Gonzalez M, Portillo-Martin JA. Effects of obstructive sleep apnea and its treatment over the erectile function: a systematic review. Asian J Androl. (2017) 19:303–10. doi: 10.4103/1008-682X.170440
14. Hoyos CM, Melehan KL, Phillips CL, Grunstein RR, Liu PY. To ED or not to ED – is erectile dysfunction in obstructive sleep apnea related to endothelial dysfunction? Sleep Med Rev. (2015) 20:5–14. doi: 10.1016/j.smrv.2014.03.004
15. Schiavi RC, Mandeli J, Schreiner-Engel P, Chambers A. Aging, sleep disorders, and male sexual function. Biol Psychiatry. (1991) 30:15–24. doi: 10.1016/0006-3223(91)90066-U
16. Heruti R, Shochat T, Tekes-Manova D, Ashkenazi I, Justo D. Association between erectile dysfunction and sleep disorders measured by self-assessment questionnaires in adult men. J Sex Med. (2005) 2:543–50. doi: 10.1111/j.1743-6109.2005.00072.x
17. Hanak V, Jacobson DJ, McGree ME, Sauver JS, Lieber MM, Olson EJ, et al. Snoring as a risk factor for sexual dysfunction in community men. J Sex Med. (2008) 5:898–908. doi: 10.1111/j.1743-6109.2007.00706.x
18. Andersen ML, Santos-Silva R, Bittencourt LRA, Tufik S. Prevalence of erectile dysfunction complaints associated with sleep disturbances in São Paulo, Brazil: a population-based survey. Sleep Med. (2010) 11:1019–24. doi: 10.1016/j.sleep.2009.08.016
19. Szymanski FM, Filipiak KJ, Hrynkiewicz-Szymanska A, Grabowski M, Dabrowska-Kugacka A, Opolski G. The high risk of obstructive sleep apnea—an independent risk factor of erectile dysfunction in ST-segment elevation myocardial infarction patients. J Sex Med. (2011) 8:1434–8. doi: 10.1111/j.1743-6109.2010.02075.x
20. Chen CM, Tsai MJ, Wei PJ, Su YC, Yang CJ, Wu MN, et al. Erectile dysfunction in patients with sleep apnea–a nationwide population-based study. PLoS ONE. (2015) 10:e0132510. doi: 10.1371/journal.pone.0132510
21. Chen KF, Liang SJ, Lin CL, Liao WC, Kao CH. Sleep disorders increase risk of subsequent erectile dysfunction in individuals without sleep apnea: a nationwide population-base cohort study. Sleep Med. (2016) 17:64–8. doi: 10.1016/j.sleep.2015.05.018
22. Bozorgmehri S, Fink HA, Parimi N, Canales B, Ensrud KE, Ancoli-Israel S, et al. Association of sleep disordered breathing with erectile dysfunction in community dwelling older men. J Urol. (2017) 197:776–82. doi: 10.1016/j.juro.2016.09.089
23. Pressman MR, DiPhillipo MA, Kendrick JI, Conroy K, Fry JM. Problems in the interpretation of nocturnal penile tumescence studies: disruption of sleep by occult sleep disorders. J Urol. (1986) 136:595–8. doi: 10.1016/S0022-5347(17)44984-6
24. Hirshkowitz M, Karacan I, Gurakar A, Williams RL. Hypertension, erectile dysfunction, and occult sleep apnea. Sleep. (1989) 12:223–32. doi: 10.1093/sleep/12.3.223
25. Hirshkowitz M, Karacan I, Arcasoy MO, Acik G, Narter EM, Williams RL. Prevalence of sleep apnea in men with erectile dysfunction. Urology. (1990) 36:232–4. doi: 10.1016/0090-4295(90)80262-L
26. Chediak AD, Acevedo-Crespo JC, Seiden DJ, Kim HH, Kiel MH. Nightly variability in the indices of sleep-disordered breathing in men being evaluated for impotence with consecutive night polysomnograms. Sleep. (1996) 19:589–92. doi: 10.1093/sleep/19.7.589
27. Seftel AD, Strohl KP, Loye TL, Bayard D, Kress J, Netzer NC. Erectile dysfunction and symptoms of sleep disorders. Sleep. (2002) 25:643–7. doi: 10.1093/sleep/25.6.637
28. Fanfulla F, Malaguti S, Montagna T, Salvini S, Bruschi C, Crotti P, et al. Erectile dysfunction in men with obstructive sleep apnea: an early sign of nerve involvement. Sleep. (2000) 23:775–81. doi: 10.1093/sleep/23.6.1e
29. Teloken PE, Smith EB, Lodowsky C, Freedom T, Mulhall JP. Defining association between sleep apnea syndrome and erectile dysfunction. Urology. (2006) 67:1033–7. doi: 10.1016/j.urology.2005.11.040
30. Shin HW, Rha YC, Han DH, Chung S, Yoon IY, Rhee CS, et al. Erectile dysfunction and disease-specific quality of life in patients with obstructive sleep apnea. Int J Impot Res. (2008) 20:549–53. doi: 10.1038/ijir.2008.39
31. Budweiser S, Enderlein S, Jörres RA, Hitzl AP, Wieland WF, Pfeifer M, et al. Sleep apnea is an independent correlate of erectile and sexual dysfunction. J Sex Med. (2009) 6:3147–57. doi: 10.1111/j.1743-6109.2009.01372.x
32. Stannek T, Hürny C, Schoch OD, Bucher T, Münzer T. Factors affecting self-reported sexuality in men with obstructive sleep apnea syndrome. J Sex Med. (2009) 6:3415–24. doi: 10.1111/j.1743-6109.2009.01486.x
33. Petersen M, Kristensen E, Berg S, Midgren B. Sexual function in male patients with obstructive sleep apnoea. Clin Respir J. (2009) 4:186–91. doi: 10.1111/j.1752-699X.2009.00173.x
34. Gurbuz C, Kuzu Okur H, Demir S, Ordu S, Caskurlu T. Pure obstructive sleep apnea syndrome and erectile dysfunction. Balk Med J. (2011) 28:333–9. doi: 10.5152/balkanmedj.2011.011
35. Santos T, Drummond M, Botelho F. Erectile dysfunction in obstructive sleep apnea syndrome—prevalence and determinants. Rev Port Pneumol. (2012) 18:64–71. doi: 10.1016/j.rppnen.2012.01.002
36. Bouloukaki I, Papadimitriou V, Sofras F, Mermigkis C, Moniaki V, Siafakas NM, et al. Abnormal cytokine profile in patients with obstructive sleep apnea-hypopnea syndrome and erectile dysfunction. Mediat Inflamm. (2014) 2014:568951. doi: 10.1155/2014/568951
37. Jeon YJ, Yoon DW, Han DH, Won TB, Kim DY, Shin HW. Low quality of life and depressive symptoms as an independent risk factor for erectile dysfunction in patients with obstructive sleep apnea. J Sex Med. (2015) 12:2168–77. doi: 10.1111/jsm.13021
38. Popp R, Kleemann Y, Burger M, Pfeifer M, Arzt M, Budweiser S. Impaired vigilance is associated with erectile dysfunction in patients with sleep apnea. J Sex Med. (2015) 12:405–15. doi: 10.1111/jsm.12789
39. Taken K, Ekin S, Arisoy A, Günes M, Dönmez MI. Erectile dysfunction is a marker for obstructive sleep apnea. Aging Male. (2016) 19:102–5. doi: 10.3109/13685538.2015.1131259
40. Pascual M, de Batlle J, Barbé F, Castro-Grattoni AL, Auguet JM, Pascual L, et al. Erectile dysfunction in obstructive sleep apnea patients: a randomized trial on the effects of continuous positive airway pressure (CPAP). PLoS ONE. (2018) 13:e0201930. doi: 10.1371/journal.pone.0201930
41. Schulz R, Bischof F, Galetke W, Gall H, Heitmann J, Hetzenecker A, et al. CPAP therapy improves erectile function in patients with severe obstructive sleep apnea. Sleep Med. (2019) 53:189–94. doi: 10.1016/j.sleep.2018.03.018
42. Soukhova-O'Hare GK, Shah ZA, Lei Z, Nozdrachev AD, Rao CV, Gozal D. Erectile dysfunction in a murine model of sleep apnea. Am J Respir Crit Care Med. (2008) 178:644–50. doi: 10.1164/rccm.200801-190OC
43. Liu K, Liu XS, Xiao L, Shang J, Li MC, Xu YJ, et al. NADPH oxidase activation: a mechanism of erectile dysfunction in a rat model of sleep apnea. J Androl. (2012) 33:1186–98. doi: 10.2164/jandrol.112.016642
44. Zhu D, Deng Y, Pan Y, Wang Z, Yuan X, Guo X, et al. N-acetylcysteine ameliorates the erectile dysfunction caused by chronic intermittent hypoxia in rats: partly involvement of endoplasmic reticulum stress. Urology. (2015) 86:844. doi: 10.1016/j.urology.2015.07.013
45. Liang L, Zheng D, Lu C, Xi Q, Bao H, Li W, et al. Exosomes derived from miR-301a-3p-overexpressing adipose-derived mesenchymal stem cells reverse hypoxia-induced erectile dysfunction in rat models. Stem Cell Res Ther. (2021) 12:87. doi: 10.1186/s13287-021-02161-8
46. Ramanathan R, Mulhall J, Rao S, Leung R, Salamanca JIM, Mandhani A, et al. Predictive correlation between the international index of erectile function (IIEF) and sexual health inventory for men (SHIM): implications for calculating a derived SHIM for clinical use. J Sex Med. (2007) 4:1336–44. doi: 10.1111/j.1743-6109.2007.00576.x
47. Van Vo T, Hoang HD, Thanh Nguyen NP. Prevalence and associated factors of erectile dysfunction among married men in Vietnam. Front Public Health. (2017) 5:94. doi: 10.3389/fpubh.2017.00094
48. Qin F, Gao L, Qian S, Fu F, Yang Y, Yuan J. Advantages and limitations of sleep-related erection and rigidity monitoring: a review. Int J Impot Res. (2018) 30:192–201. doi: 10.1038/s41443-018-0032-8
49. Arruda-Olson AM, Olson LJ, Nehra A, Somers VK. Sleep apnea and cardiovascular disease. implications for understanding erectile dysfunction. Herz. (2003) 28:298–303. doi: 10.1007/s00059-003-2482-z
50. Ip MSM, Lam B, Chan LY, Zheng L, Tsang KWT, Fung PCW, et al. Circulating nitric oxide is suppressed in obstructive sleep apnea and is reversed by nasal continuous positive airway pressure. Am J Respir Crit Care Med. (2000) 162:2166–71. doi: 10.1164/ajrccm.162.6.2002126
51. Schulz R, Schmidt D, Blum A, Lopes-Ribeiro X, Lücke C, Mayer K, et al. Decreased plasma levels of nitric oxide derivatives in obstructive sleep apnoea: response to CPAP therapy. Thorax. (2000) 55:1046–51. doi: 10.1136/thorax.55.12.1046
52. Rakugi H, Tabuchi Y, Nakamaru M, Nagano M, Higashimori K, Mikami H, et al. Evidence for endothelin-1 release from resistance vessels of rats in response to hypoxia. Biochem Biophys Res Commun. (1990) 169:973–7. doi: 10.1016/0006-291X(90)91989-6
53. Ziegler MG, Milic M. Sympathetic nerves and hypertension in stress, sleep apnea, and caregiving. Curr Opin Nephrol Hypertens. (2017) 26:26–30. doi: 10.1097/MNH.0000000000000288
54. Mayer P, Dematteis M, Pépin JL, Wuyam B, Veale DAN, Vila A, et al. Peripheral neuropathy in sleep apnea. a tissue marker of the severity of nocturnal desaturation. Am J Respir Crit Care Med. (1999) 159:213–9. doi: 10.1164/ajrccm.159.1.9709051
55. Somers VK, Dyken ME, Clary MP, Abboud FM. Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Investig. (1995) 96:1897–904. doi: 10.1172/JCI118235
56. Ziegler MG, Nelesen R, Mills P, Ancoli-Israel S, Kennedy B, Dimsdale JE. Sleep apnea, norepinephrine-release rate, and daytime hypertension. Sleep. (1997) 20:224–31. doi: 10.1093/sleep/20.3.224
57. Seftel AD, Sun P, Swindle R. The prevalence of hypertension, hyperlipidemia, diabetes mellitus and depression in men with erectile dysfunction. J Urol. (2004) 171:2341–5. doi: 10.1097/01.ju.0000125198.32936.38
58. Lue TF. Erectile dysfunction. N Engl J Med. (2000) 342:1802–13. doi: 10.1056/NEJM200006153422407
59. Zias N, Bezwada V, Gilman S, Chroneou A. Obstructive sleep apnea and erectile dysfunction: still a neglected risk factor? Sleep Breath. (2009) 13:3–10. doi: 10.1007/s11325-008-0212-8
60. Peppard PE. Longitudinal association of sleep-related breathing disorder and depression. Arch Intern Med. (2006) 166:1709–15. doi: 10.1001/archinte.166.16.1709
61. Wittert G. The relationship between sleep disorders and testosterone. Curr Opin Endocrinol Diabetes Obes. (2014) 21:239–43. doi: 10.1097/MED.0000000000000069
62. Wittert G. The relationship between sleep disorders and testosterone in men. Asian J Androl. (2014) 16:262–5. doi: 10.4103/1008-682X.122586
63. Bercea RM, Mihaescu T, Cojocaru C, Bjorvatn B. Fatigue and serum testosterone in obstructive sleep apnea patients. Clin Respir J. (2015) 9:342–9. doi: 10.1111/crj.12150
64. Li Z, Tang T, Wu W, Gu L, Du J, Zhao T, et al. Efficacy of nasal continuous positive airway pressure on patients with OSA with erectile dysfunction and low sex hormone levels. Respir Med. (2016) 119:130–4. doi: 10.1016/j.rmed.2016.09.001
65. Zhang XB, Lin QC, Zeng HQ, Jiang XT, Chen B, Chen X. Erectile dysfunction and sexual hormone levels in men with obstructive sleep apnea: efficacy of continuous positive airway pressure. Arch Sex Behav. (2016) 45:235–40. doi: 10.1007/s10508-015-0593-2
66. Granata AR, Rochira V, Lerchl A, Marrama P, Carani C. Relationship between sleep-related erections and testosterone levels in men. J Androl. (1997) 18:522–7.
67. Gambineri A, Pelusi C, Pasquali R. Testosterone levels in obese male patients with obstructive sleep apnea syndrome: relation to oxygen desaturation, body weight, fat distribution and the metabolic parameters. J Endocrinol Investig. (2003) 26:493–8. doi: 10.1007/BF03345209
68. Schneider BK, Pickett CK, Zwillich CW, Weil JV, McDermott MT, Santen RJ, et al. Influence of testosterone on breathing during sleep. J Appl Physiol. (1986) 61:618–23. doi: 10.1152/jappl.1986.61.2.618
69. Jhuang YH, Chung CH, Wang ID, Peng CK, Meng E, Chien WC, et al. Association of obstructive sleep apnea with the risk of male infertility in Taiwan. JAMA Netw Open. (2021) 4:e2031846. doi: 10.1001/jamanetworkopen.2020.31846
70. Lotti F, Maggi M. Sexual dysfunction and male infertility. Nat Rev Urol. (2018) 15:287–307. doi: 10.1038/nrurol.2018.20
71. Rodriguez KM, Kohn TP, Kohn JR, Sigalos JT, Kirby EW, Pickett SM, et al. Shift work sleep disorder and night shift work significantly impair erectile function. J Sex Med. (2020) 17:1687–93. doi: 10.1016/j.jsxm.2020.06.009
72. Luboshitzky R, Aviv A, Hefetz A, Herer P, Shen-Orr Z, Lavie L, et al. Decreased pituitary-gonadal secretion in men with obstructive sleep apnea. J Clin Endocrinol Metab. (2002) 87:3394–8. doi: 10.1210/jcem.87.7.8663
73. Jannini EA, Granata AM, Hatzimouratidis K, Goldstein I. Controversies in sexual medicine: use and abuse of rigiscan in the diagnosis of erectile dysfunction. J Sex Med. (2009) 6:1820–9. doi: 10.1111/j.1743-6109.2009.01343.x
74. Moreland RB. Is there a role of hypoxemia in penile fibrosis: a viewpoint presented to the society for the study of impotence. Int J Impot Res. (1998) 10:113–20. doi: 10.1038/sj.ijir.3900328
75. Schmid DM, Hauri D, Schurch B. Nocturnal penile tumescence and rigidity (NPTR) findings in spinal cord injured men with erectile dysfunction. Int J Impot Res. (2004) 16:433–40. doi: 10.1038/sj.ijir.3901188
76. Ware JC, Hirshkowitz M. Characteristics of penile erections during sleep recorded from normal subjects. J Clin Neurophysiol. (1992) 9:78–87. doi: 10.1097/00004691-199201000-00009
77. Masri S, Sassone-Corsi P. The emerging link between cancer, metabolism, and circadian rhythms. Nat Med. (2018) 24:1795–803. doi: 10.1038/s41591-018-0271-8
78. Vignozzi L, Maggi M. Circadian rhythm and erectile function: is there a penile clock? Nat Rev Urol. (2020) 17:603–4. doi: 10.1038/s41585-020-00376-7
Keywords: prevalence, ED, obstructive sleep apnea (OSA), physiopathological mechanism, relationship
Citation: Gu Y, Wu C, Qin F and Yuan J (2022) Erectile Dysfunction and Obstructive Sleep Apnea: A Review. Front. Psychiatry 13:766639. doi: 10.3389/fpsyt.2022.766639
Received: 29 August 2021; Accepted: 25 April 2022;
Published: 26 May 2022.
Edited by:
Andrea De Vito, Santa Maria delle Croci Hospital, ItalyReviewed by:
Arturo Garay, Centro de Educación Médica e Investigaciones Clínicas Norberto Quirno (CEMIC), ArgentinaCopyright © 2022 Gu, Wu, Qin and Yuan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiuhong Yuan, aml1aG9uZ3l1YW4yMTA3QDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.