 Long Zhai1†
Long Zhai1† Hua Zhang
Hua Zhang- 1Department of Occupational Health, Qingdao Municipal Center for Disease Control and Prevention, Qingdao Institute of Prevention Medicine, Qingdao, China
- 2Department of Third Supervisory Section, Shibei District Health Supervision Institute, Qingdao, China
- 3Department of Chronic Noncommunicable Diseases, Qingdao Municipal Center for Disease Control and Prevention, Qingdao Institute of Prevention Medicine, Qingdao, China
Results from longitudinal studies on involuntary retirement and depression remain controversial. PubMed, Web of Science, Embase, ScienceDirect, Wanfang, and VIP updated on 4 January 2022 were searched for eligible publications. Pooled relative risks (RRs) with 95% confidence interval (CI) were calculated using a random-effects model. Eight published articles with 14,604 participants for the effect of involuntary retirement on depression incidence and 26,822 participants for the relationship between depression and involuntary retirement were included. Compared with working, the pooled RR for depression was 1.31 (95% CI, 1.13–1.51; I2 = 37.7%) for the involuntary retirement overall. For involuntary retirement, the pooled RR was 1.70 (95% CI, 1.28–2.25; I2 = 84.2%). The associations between involuntary retirement and depression did not substantially change in sensitivity and subgroup analyses. No evidence of publication bias was found. This meta-analysis indicates that there might be mutual causal relationship between involuntary retirement and depression. More large longitudinal studies with different gender and income levels are needed.
Introduction
Depression is a prevalent chronic condition which often leads to increased morbidity and functional impairment; more than 264 million people are living with depression all around the world (1). Depression predisposes to medical illnesses and advances biological aging. Medical illnesses also increase the risk of late-life depression. The reciprocal relationships of depression with aging-related and disease-related processes have generated pathogenetic hypotheses (2).
Retirement is a major life transition in the second half of life with changes in daily schedules and social activities. Moving from a relatively busy and regular lifestyle to a relatively inactive one is a challenge, and the change of roles may be a trigger for some retirees to develop mental health problems (3).
Involuntary retirement was defined as being forced to retire before the regular retirement age due to business closure, layoff, family problems, or health problems (4). During the past couple of decades, studies did not reach a consensus on the relationship between involuntary retirement and depression (5–12). For the effect of involuntary retirement on depression incidence, a longitudinal cohort study reported that unemployed was not associated with the risk of depressive symptoms (10). However, another longitudinal study showed involuntary retirement increased the risk of depressive symptoms (9). Other longitudinal studies about the association between depression and involuntary retirement have also provided conflicting results. One nationally representative panel survey indicated that depression and depressive symptoms were significantly associated with retirement in late middle-aged U.S. workers (7). Whereas, a Chinese longitudinal study showed that depression had no effect on involuntary retirement (12).
Therefore, we conducted a meta-analysis of longitudinal studies to: (1) research the causal relationship between involuntary retirement and depression; (2) explore the potential between-study heterogeneity and (3) investigate the potential publication bias.
Methods
This systematic review was written according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (http://www.prisma-statement.org).
Literature Search and Selection
The English literatures of PubMed, Embase, ScienceDirect, and Web of Science and the Chinese literature of Wanfang, and VIP from their establishment to 4 January 2022 will be comprehensively and systematically searched. PubMed, Embase, ScienceDirect, and Web of Science were searched through the subject words and keywords retrieval method using the following keywords: “retirement” and “depression”. The Wanfang, and VIP were searched using the general Chinese translation of the above search terms (Table S1). Moreover, we reviewed the reference lists from retrieved articles to search for further relevant studies.
The eligibility criteria were mainly conducted in accordance with the PICOS (population, intervention/exposure, control, outcomes, and study design) principle limited to Chinese and English study.
The inclusion standards were shown below: (a) Population. Community participants; (b) Exposure. Employment status or depression state; (c) Comparators. Healthy adults (age ≥ 19) in normal working condition; (d) Outcomes. Depression or early retirement; (e) Study design. Longitudinal study.
The following exclusion criteria were utilized: (a) papers which were meta-analysis, reviews, animal experiments, case reports, conference abstracts, non-English/Chinese literature, mechanism researches or other diseases, or lacking the full text; (b) duplicate publication or incomplete data; (c) study provided insufficient information on multivariate-adjusted RRs/ORs of retirement and depression; (d) participants already taking antidepressants or having hospital treatment for depression.
Data Extraction and Quality Assessment
The following data were extracted from each study by two investigators: (1) name of the first author; (2) publication year; (3) study population; (4) origin of country; (5) follow-up years; (6) number of participants; (7) age range or mean age at baseline years; (8) gender; (9) measurement of employment status and depression; (10) RR/OR with 95% CI (adjusted by the most confounders in the original studies); (11) adjustment for confounders; (12) study quality. The study quality was assessed using the Newcastle-Ottawa quality assessment scale (http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp).
Statistical Analysis
We weighted the study-specific log relative risks by the inverse of their variance to calculate a summary estimate and its 95% CI. The DerSimonian and Laird random effects model was used to combine study-specific effect sizes (95% CIs), which considers both within-study and between-study variation (13). I2 of Higgins and Thompson was used to assess heterogeneity among studies (14) and I2 values of 0, 25, 50, and 75% represent no, low, moderate and high heterogeneity (13), respectively.
Univariate meta-regression analyses by study region, number of participants, and follow-up years were conducted to investigate the potential sources of heterogeneity. The leave-one-out sensitivity analysis (15) was carried out to evaluate the key studies that have a substantial impact on the between-study heterogeneity.
Publication bias was assessed with visual inspection of the funnel plots, Begg's rank correlation test (16), and Egger's linear regression test (17). We also conducted subgroup analyses by study region (Europe, America, and Asia), number of participants (≥4,000 and <4,000), and depression measurement (Center for Epidemiologic Studies Depression scale). All statistical analyses were conducted by Stata V.12.0 (Stata Corp, College Station, Texas, USA). A two tailed p < 0.05 was considered statistically significant.
Results
Literature Search and Study Characteristics
We identified 8,023 articles by our literature search, of which 5,100 were excluded after review of titles or abstracts (Figure 1). Two additional articles were found in reference lists of retrieved studies. We reviewed 150 possibly relevant articles in full text. One article included participant already taking antidepressants or having hospital treatment for depression, one article included men living with HIV, two articles using the same population, nine cross-sectional designed articles, and 129 articles without multivariate-adjusted RRs/ORs concerning the relation between involuntary retirement and depression were excluded. Thus, 10 longitudinal studies from eight articles (5–12) were included in the analysis (Table 1).
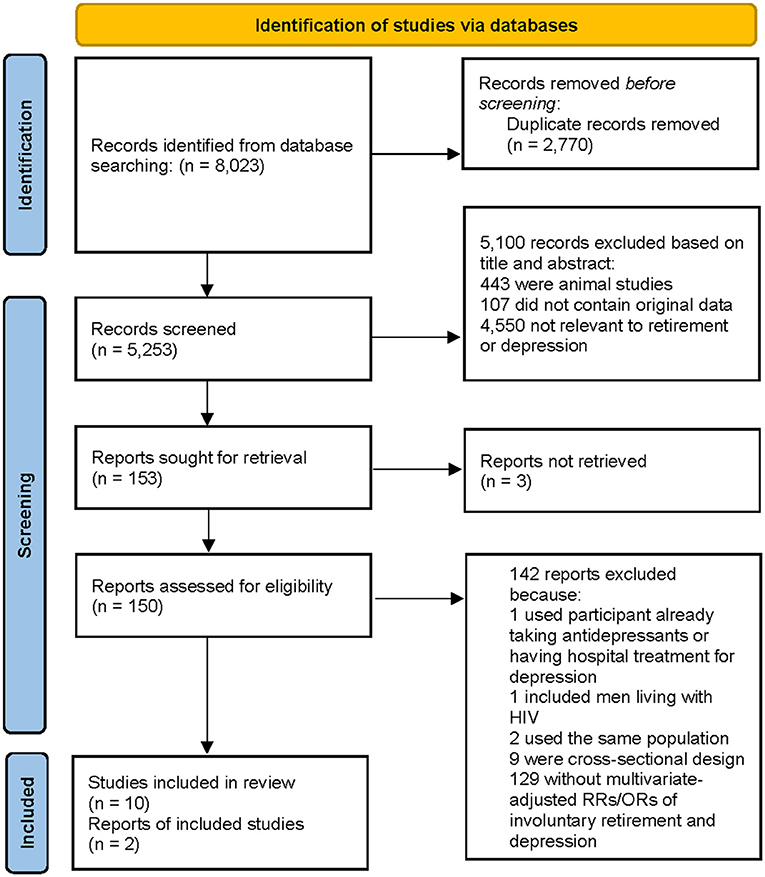
Figure 1. Flow of the literature.
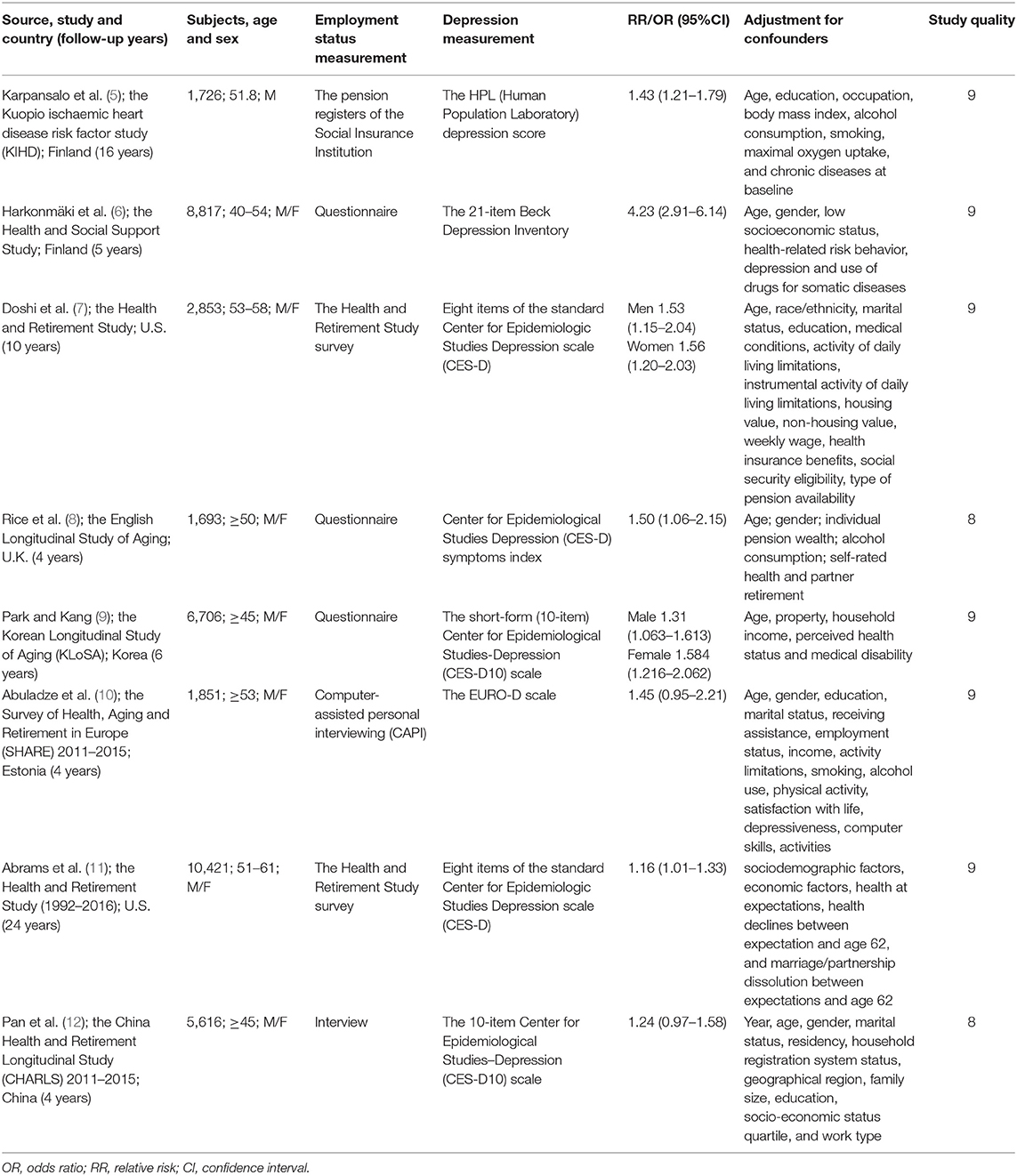
Table 1. Characteristics of longitudinal studies on involuntary retirement and depression.
All included studies had a longitudinal design. The duration of follow-up ranged from 4 to 24 years. Two studies (7, 9) included only women, three studies (5, 7, 9) included only men, and five studies (6, 8, 10–12) included men and women. With regard to the study region, four studies (5, 6, 8, 10) was conducted in Europe, three (7, 11) in America, and three (9, 12) in Asia. One study (5) measured employment status by record linkage, and other studies (6–12) used questionnaires. Seven studies (7–9, 11, 12) used Center for Epidemiologic Studies Depression scale to measure depressive symptoms, and the other three studies used EURO-D (10), Human Population Laboratory depression score (5), and Beck Depression Inventory (6), respectively. The major adjustment confounding factors included age, gender, education, race/ethnicity, and marital status. Quality assessment showed that the Newcastle-Ottawa score of each study was not <8, indicating that the methodological quality was generally good (Table S2).
Involuntary Retirement and Depression
Four longitudinal studies (9–11) involving 14,604 participants were included in the involuntary retirement and depression meta-analysis. Three studies (9, 11) showed a significant association between involuntary retirement and depression; while the other one study (10) indicated no relation between them. The pooled RR of overall data was 1.31 (95% CI, 1.13–1.51; P = 0) for the unexpectedly retired vs. employed, with low heterogeneity (I2 = 37.7 %, Pheterogeneity = 0.186) (Figure 2).
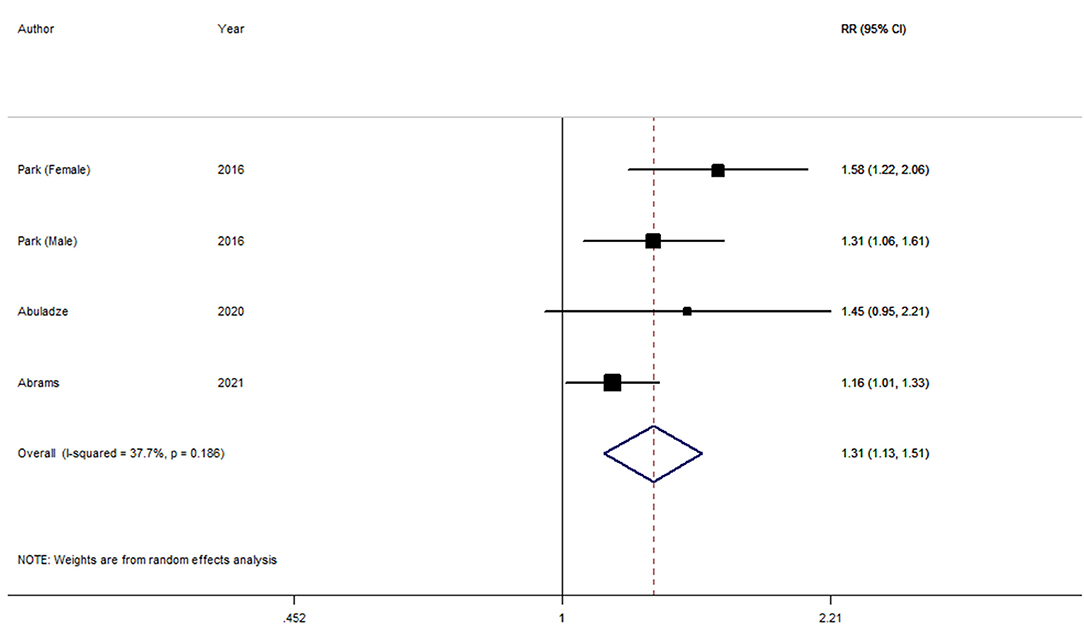
Figure 2. Forest plot for the pooled relative risk of depression.
Depression and Involuntary Retirement
Six longitudinal studies (5–8, 12) involving 26,822 participants were included in the depression and involuntary retirement meta-analysis. Five studies (5–8) showed a significant association between depression and involuntary retirement; while the other one study (12) indicated no relation between them. The overall result indicated that depression was significantly associated with involuntary retirement (RR, 1.70; 95% CI, 1.28–2.25; I2 = 84.2%, Pheterogeneity = 0) (Figure 3).
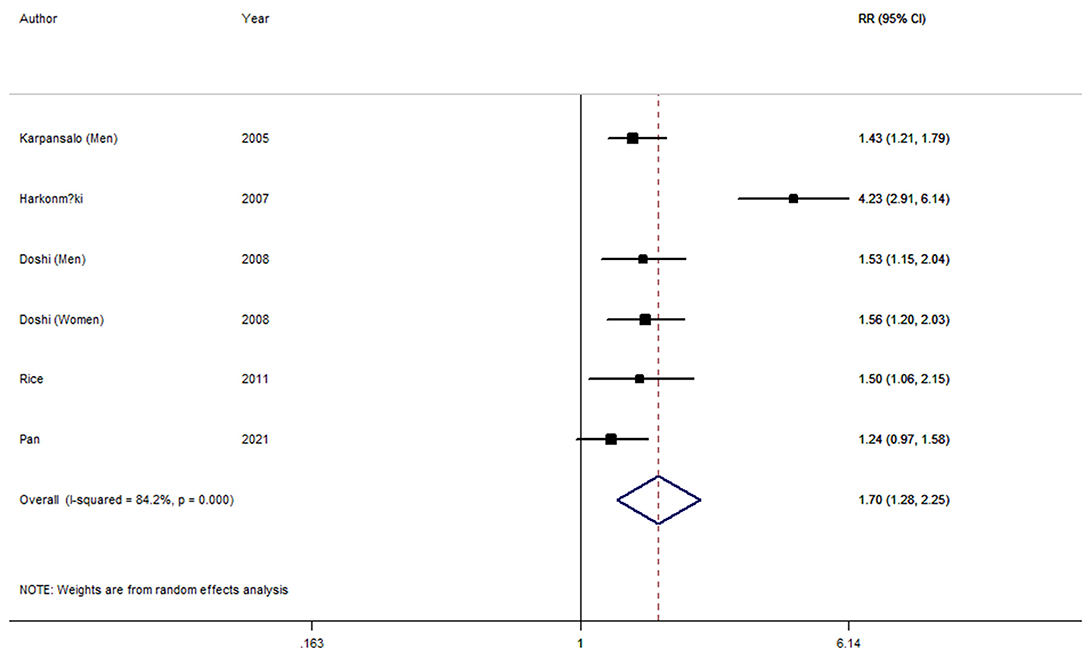
Figure 3. Forest plot for the pooled relative risk of involuntary retirement.
Meta-Regression and Subgroup Analyses
Low heterogeneity (I2 = 37.7 %, Pheterogeneity = 0.186) among all included studies was demonstrated for involuntary retirement and depression. P-values of univariate meta-regression analysis with the covariates of study region, number of participants and follow-up years were 0.212, 0.190, and 0.199, respectively.
As seen in Figure 3, high heterogeneity (I2 = 84.2%, Pheterogeneity = 0) was found for depression and involuntary retirement. P-values of univariate meta-regression analysis with the covariates of study region, number of participants and follow-up years were 0.949, 0.108, and 0.629, respectively.
Tables 2, 3 showed the results from subgroup analyses. The associations between involuntary retirement and depression did not differ substantially by study location and number of participants. For example, the pooled RRs for depression were consistent for studies conducted in Asia (RR, 1.42; 95% CI, 1.18–1.70). When we stratified studies by different number of participants, the pooled RRs of involuntary retirement were 1.45 (95% CI 1.22–1.72) for studies with subjects <4,000. For studies using Center for Epidemiologic Studies Depression scale to measure depressive symptoms, the pooled RRs were 1.30 (95% CI 1.10–1.54) for depression and 1.43 (95% CI 1.25–1.65) for involuntary retirement, respectively.
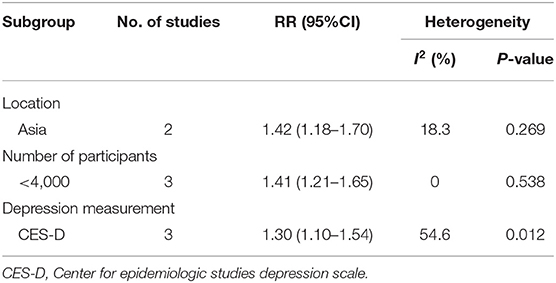
Table 2. Subgroup analyses of involuntary retirement and depression.
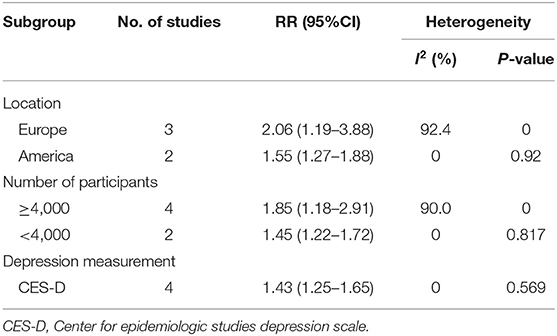
Table 3. Subgroup analyses of depression and involuntary retirement.
Sensitivity Analysis
One study (6) was found to be the key contributor to this high between-study heterogeneity for depression and early retirement by the leave-one-out sensitivity analysis. After further excluding this study, no heterogeneity (I2 = 0, Pheterogeneity = 0.732) was found, and the pooled RR was 1.43 (95% CI 1.28–1.60).
Publication Bias
The visual inspection of funnel plots (Figure 4 for depression and Figure 5 for involuntary retirement), Begg's rank correlation test (p = 0.308 for depression and p = 0.260 for involuntary retirement), and Egger's linear regression test (p = 0.180 for depression and p = 0.167 for involuntary retirement) showed no evidence of publication bias for the analysis between involuntary retirement and depression.
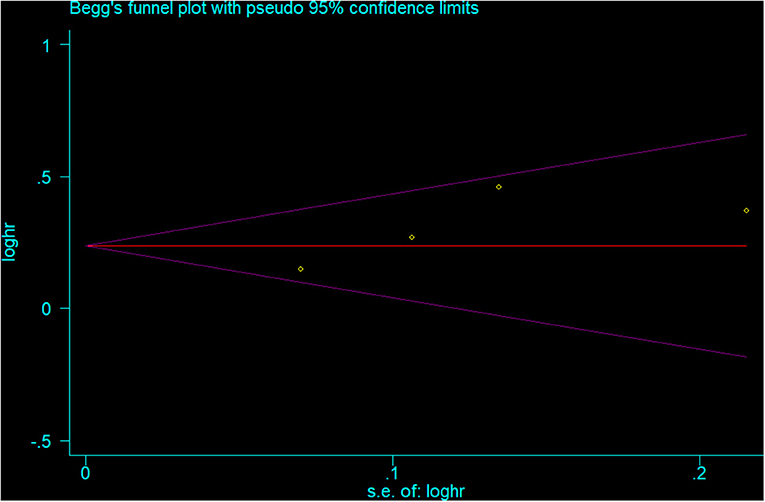
Figure 4. Funnel plot for the publication bias of depression analysis.
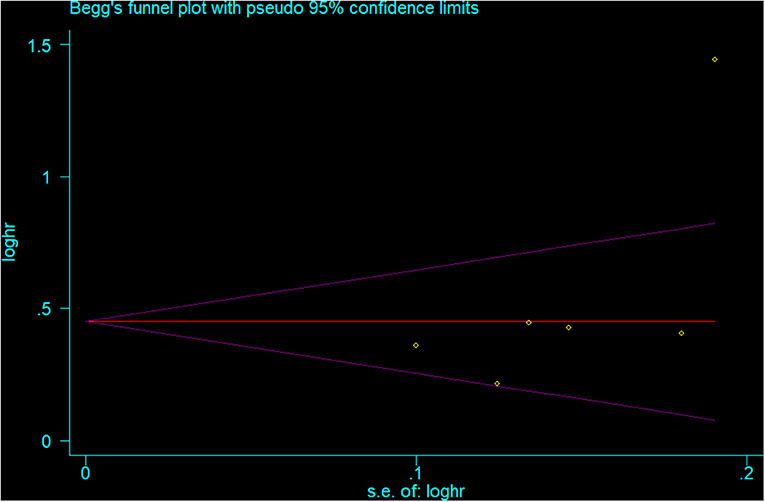
Figure 5. Funnel plot for the publication bias of involuntary retirement analysis.
Discussion
This study provides for the first time a meta-analysis of longitudinal-only studies examining the bidirectional association between involuntary retirement and depression. The meta-analysis of longitudinal studies including 14,604 participants for involuntary retirement and depression and 26,822 participants for depression and involuntary retirement identified that involuntary retirement was significantly associated with increased risk of depression and depression was an independent predictor of involuntary retirement in adults.
Recently, several studies researched the relation of retirement and depression (depressive symptoms scores). Findings from the present study were in agreement with a meta-analysis that used the standardized mean difference (d) as a measure of effect size and found involuntary retirement was associated with more depressive symptoms (d = 0.180, 95% CI 0.061–0.299) (18). Other reviews also found that people from developed Asian countries and lower socio-economic groups experienced a decline in mental health after retirement (19, 20).
The mechanisms underlying the association between involuntary retirement and depression are still not fully understood. One underlying explanation for our findings is that involuntary retirement may lead to changes in life patterns and social support, which has been important predictor of depression (21, 22). Otherwise, depression can also lead to involuntary retirement by affecting physical and social abilities (23, 24). Hence, retirees (depressed people) with disordered social intercourse and changed life routine are more likely to be depressed (retired). Further studies in understanding the underlying biological mechanisms linking involuntary retirement and depression are warranted.
Between-study heterogeneity occurs frequently in meta-analysis (13). In this study, low heterogeneity (Pheterogeneity = 0.186) was found in depression analysis, whereas high heterogeneity (Pheterogeneity = 0) was found in involuntary retirement analysis. Thus, we used meta-regression and the leave-one-out sensitivity analysis that aimed to explore the potentially important causes of the between-study heterogeneity. Univariate meta-regression showed that no abovementioned covariate was found to influence between-study heterogeneity. In our subgroup analyses by study region and number of participants, the between-study heterogeneity was decreased and the associations did not substantially change. One study (6) was found to be the key contributor to the high between-study heterogeneity of involuntary retirement analysis by the leave-one-out sensitivity analysis. When we excluded this study, there was no heterogeneity (I2 = 0%). After reducing the between-study heterogeneity, the results were found to be consistent with the one based on all studies, indicating that our results were stable and reliable.
A major strength of this study was the large number of participants included from longitudinal studies, allowing a much greater possibility of reasonable conclusions and investigating a potential causal relationship between involuntary retirement and depression. Second, all included studies had adjusted for potential confounders, increasing the credibility of the results. Third, the relationship between involuntary retirement and depression risk did not substantially change in sensitivity and subgroup analyses. Fourth, we found little evidence of publication bias in this meta-analysis, which indicated that our results were not affected by small-study effects.
Our results must be interpreted in light of the following limitations. First, although one study (10) considered satisfaction with life, and two studies (9) adjusted for disability, other psychological (personality traits and adaptability) and social (social networks and social activities) factors were not included, which may play a significant role in the presence or absence of depression in retirement age. Second, the limited information provided in the included studies precluded the possibility of subgroup analyses by different sex and income levels. Third, as only one study (5) used record linkage measures for employment status, the estimation of the true association between involuntary retirement and depression could be influenced by misclassification. Fourth, depression is considered a chronic, recurrent, remitting and continuous phenomenon. For included studies, the duration of follow-up had a wide range of 4–24 years; hence, the presence of previous depressive episodes could have an effect on the outcomes.
In summary, results from this meta-analysis indicate that there may be mutual causal relationship between involuntary retirement and depression in adults. More large studies with different gender and income levels are needed to identify the relation of involuntary retirement and depression in different groups of people and investigate the underlying biological mechanisms.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
LZ and HZ conceived the study, participated in its design, and coordination. LZ and JW carried out the literature searching, data extraction, and quality assessment. YL and HZ were involved in the interpretation of the data, drafting the manuscript, and revising it critically for important intellectual content. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.747334/full#supplementary-material
References
1. GBD Disease and Injury Incidence and Prevalence Collaborators. Collaborators. Global, regional, national incidence. prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1789–858. doi: 10.1016/S0140-6736(18)32279-7
2. Alexopoulos GS. Mechanisms and treatment of late-life depression. Transl Psychiatry. (2019) 9:188. doi: 10.1038/s41398-019-0514-6
3. Osborne JW. Psychological effects of the transition to retirement. Can J Couns Psychotherapy. (2011) 46:45–58.
4. Shultz KS, Morton KR, Weckerle JR. The influence of push and pull factors on voluntary and involuntary early retirees' retirement decision and adjustment. J Vocat Behav. (1998) 53:45–57. doi: 10.1006/jvbe.1997.1610
5. Karpansalo M, Kauhanen J, Lakka TA, Manninen P, Kaplan GA, Salonen JT. Depression and early retirement: prospective population based study in middle aged men. J Epidemiol Community Health. (2005) 59:70–4. doi: 10.1136/jech.2003.010702
6. Harkonmäki K, Korkeila K, Vahtera J, Kivimäki M, Suominen S, Sillanmäki L, et al. Childhood adversities as a predictor of disability retirement. J Epidemiol Community Health. (2007) 61:479–84. doi: 10.1136/jech.2006.052670
7. Doshi JA, Cen L, Polsky D. Depression and retirement in late middle-aged U.S. workers. Health Serv Res. (2008) 43:693–713. doi: 10.1111/j.1475-6773.2007.00782.x
8. Rice NE, Lang IA, Henley W, Melzer D. Common health predictors of early retirement: findings from the English Longitudinal Study of Ageing. Age Ageing. (2011) 40:54–61. doi: 10.1093/ageing/afq153
9. Park H, Kang MY. Effects of voluntary/involuntary retirement on their own and spouses' depressive symptoms. Compr Psychiatry. (2016) 66:1–8. doi: 10.1016/j.comppsych.2015.11.009
10. Abuladze L, Opikova G, Lang K. Factors associated with incidence of depressiveness among the middle-aged and older Estonian population. SAGE Open Med. (2020) 8:2050312120974167. doi: 10.1177/2050312120974167
11. Abrams LR, Clarke PJ, Mehta NK. Unmet expectations about work at age 62 and depressive symptoms. J Gerontol B Psychol Sci Soc Sci. (2021). doi: 10.1093/geronb/gbab113
12. Pan T, Mercer SW, Zhao Y, McPake B, Desloge A, Atun R, et al. The association between mental-physical multimorbidity and disability, work productivity, and social participation in China: a panel data analysis. BMC Public Health. (2021) 21:376. doi: 10.1186/s12889-021-10414-7
13. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
14. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
15. Patsopoulos NA, Evangelou E, Ioannidis JP. Sensitivity of between-study heterogeneity in meta-analysis: proposed metrics and empirical evaluation. Int J Epidemiol. (2008) 37:1148–57. doi: 10.1093/ije/dyn065
16. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. (1994) 50:1088–101. doi: 10.2307/2533446
17. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
18. Li W, Ye X, Zhu D, He P. The longitudinal association between retirement and depression: a systematic review and meta-analysis. Am J Epidemiol. (2021) 190:2220–30. doi: 10.1093/aje/kwab125
19. Mukku SSR, Harbishettar V, Sivakumar PT. Psychological morbidity after job retirement: a review. Asian J Psychiatr. (2018) 37:58–63. doi: 10.1016/j.ajp.2018.08.003
20. Schaap R, de Wind A, Coenen P, Proper K, Boot C. The effects of exit from work on health across different socioeconomic groups: a systematic literature review. Soc Sci Med. (2018) 198:36–45. doi: 10.1016/j.socscimed.2017.12.015
21. Myllyntausta S, Stenholm S. Sleep before and after retirement. Curr Sleep Med Rep. (2018) 4:278–83. doi: 10.1007/s40675-018-0132-5
22. Baranyi G, Sieber S, Cullati S, Pearce JR, Dibben CJL, Courvoisier DS. The longitudinal associations of perceived neighborhood disorder and lack of social cohesion with depression among adults aged 50 years or older: an individual-participant-data meta-analysis from 16 high-income countries. Am J Epidemiol. (2020) 189:343–53. doi: 10.1093/aje/kwz209
23. Broadhead WE, Blazer DG, George LK, Tse CK. Depression, disability days, and days lost from work in a prospective epidemiologic survey. JAMA. (1990) 264:2524–8. doi: 10.1001/jama.264.19.2524
Keywords: depressive symptom, epidemiology, meta-analysis, retirement, work
Citation: Zhai L, Wang J, Liu Y and Zhang H (2022) Involuntary Retirement and Depression Among Adults: A Systematic Review and Meta-Analysis of Longitudinal Studies. Front. Psychiatry 13:747334. doi: 10.3389/fpsyt.2022.747334
Received: 28 July 2021; Accepted: 14 January 2022;
Published: 04 February 2022.
Edited by:
Petra Maresova, University of Hradec Králové, CzechiaReviewed by:
Gabriela Cabett Cipolli, State University of Campinas, BrazilManuel Pabón-Carrasco, University of Seville, Spain
Ana Luisa Sosa Ortiz, Manuel Velasco Suárez Instituto Nacional de Neurología y Neurocirugía, Mexico
Copyright © 2022 Zhai, Wang, Liu and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hua Zhang, cWRjZGNzcUAxNjMuY29t
†These authors share first authorship