
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 13 January 2023
Sec. Schizophrenia
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.1071079
 Yan Yang1
Yan Yang1 Di Kong1Qiwen Li1
Di Kong1Qiwen Li1 Wei Chen1Guocheng Zhao1Xi Tan1Xincheng Huang1Zipeng Zhang1Can Feng1Min Xu1Ying Wan1Mi Yang1,2,3*
Wei Chen1Guocheng Zhao1Xi Tan1Xincheng Huang1Zipeng Zhang1Can Feng1Min Xu1Ying Wan1Mi Yang1,2,3*Background: Hospital-acquired pneumonia (HAP) has a significant and detrimental impact on schizophrenia patients. Non-antipsychotic medicines and modified electroconvulsive therapy (MECT) are frequently used in conjunction with antipsychotics to treat schizophrenia. Whether non-antipsychotic medicines or MECT are risk factors for HAP in schizophrenia treated with antipsychotics is still unknown.
Methods: Patients with schizophrenia who were admitted to the Fourth People's Hospital of Chengdu between January 2015 and April 2022 were included in this retrospective cohort study. Individuals with HAP were 1:1 matched to individuals without HAP (non-HAP) using propensity score matching (PSM). The risk factors for HAP were analyzed by comparing the two groups.
Results: A total of 7,085 schizophrenia patients were included in this study, with a mean age of 39.77 ± 14.45 years. 193 patients developed HAP on an average of 22.26 ± 21.68 days after admission with an incidence of 2.73%. After 1:1 PSM, 192 patients from each group (HAP and non-HAP) were included. The HAP group had significantly more patients with MECT and taking benzodiazepines, antidepressants, mood stabilizers, and anti-parkinsonians both before and after PSM by Bonferroni correction (P < 0.001). Multivariate logistic regression analysis showed that, combined with antipsychotics, non-antipsychotic medicines including benzodiazepines (OR = 3.13, 95%CI = 1.95-5.03, P < 0.001), mood stabilizers (OR =3.33, 95%CI =1.79–6.20, P < 0.001) and MECT (OR =2.58, 95%CI =1.49–4.46, P = 0.001) were associated with a significantly increased incidence of HAP.
Conclusion: The incidence of HAP in schizophrenia patients in our cohort was 2.73%. MECT and non-antipsychotic medicines, including benzodiazepines and mood stabilizers were risk factors for HAP in schizophrenia patients treated with antipsychotics.
Schizophrenia is a severe mental disorder with various symptom domains, including positive, negative, and cognitive symptoms, and it remains one of the most challenging disorders to treat (1). Antipsychotic medication is the primary pharmacological treatment used, but clinicians often find it necessary to use it in conjunction with non-antipsychotic medicines or modified electroconvulsive therapy (MECT) (1–3). Several non-antipsychotic medicines are commonly used. Antidepressants are used to improve negative symptoms, and mood stabilizers are used to incapacitate mood instability. In addition, benzodiazepines are used for comorbid anxiety or distress, and anti-Parkinsonians are used in patients with parkinsonism as a side effect of antipsychotic therapy (4–8). In addition, MECT is currently considered an effective treatment option to treat schizophrenia, especially in patients with drug resistance, aggression, catatonia, severe depression, or suicidal behavior (9).
During the COVID-19 pandemic, pneumonia in schizophrenia patients has received increased attention (10, 11). People with schizophrenia are prone to develop hospital-acquired pneumonia (HAP), which refers to new pneumonia occurring more than 48 h after admission in nonincubated patients (12–14). Han et al. (13) found that the incidence of HAP was 1.80% in patients with schizophrenia-spectrum disorder. Moreover, Yang et al. (14) reported that 7.8% of middle-aged and elderly schizophrenia had HAP. HAP can increase the cost of treatment, lengthen the duration of hospital stays, and cause a significant increase in morbidity and mortality (12). Some risk factors for HAP have been reported, such as aging, obesity, alcoholism, smoking, underlying diseases, aspiration, malnutrition, being bedridden for a long time, and the medical environment (15). In recent studies, the use of first-generation antipsychotics or second-generation antipsychotics has been identified as a risk factor for HAP (14, 16). However, the correlation between non-antipsychotic medicines or MECT and HAP in patients with schizophrenia under antipsychotic treatment remains unclear.
A recent review has reported that psychotropic drugs, including antipsychotic and non-antipsychotic drugs, are associated with an increased risk of pneumonia in the elderly (17). MECT is a medical procedure that induces seizures to treat mental disease and the main adverse reactions are cognitive dysfunction, headache, nausea, vomiting, mild anxiety, and fever. Some of these adverse reactions may increase the incidence of pneumonia (18). Furthermore, in our past clinical observation, we found that some patients with schizophrenia might be susceptible to HAP after MECT treatment in our hospital. Although both non-antipsychotics and MECT are common treatment strategies, few studies have examined the impact of these factors on HAP occurrence. Therefore, in this study, we carried out a retrospective cohort study to investigate whether non-antipsychotic medicines or MECT are risk factors for HAP in schizophrenia patients who are routinely receiving antipsychotics.
This retrospective cohort study was performed at the Fourth People's Hospital of Chengdu, a large-scale psychiatric hospital in southwest China. Patients with schizophrenia aged 14–75 years were enrolled in the study from January 2015 to April 2022, and all schizophrenics were in closed wards. The diagnosis of schizophrenia was consistent with ICD-10. The exclusion criterion included patients with infectious diseases at admission, a short stay (<3 days) in the hospital, and incomplete laboratory results and treatments. Included patients were divided into the HAP group and non-HAP group according to whether they had developed HAP. The diagnosis of HAP required all of the following conditions: fever, respiratory decline, new lung infiltrates on chest imaging, and a productive cough (12). This study was designed retrospectively. Written informed consent was waived, and the study was approved by the Institutional Review Committee of the Fourth People's Hospital of Chengdu.
All data were collected from the electronic medical record information system of our hospital. The following data were collected: age, sex, diabetes status, hypertension status, length of hospital stay, routine blood tests and serum biochemical examinations at admission, medications, and whether they had MECT or HAP. After data extraction, PSM analysis was performed with a caliper of 0.02 using State software (version 15.0, State Corporation, College Station, TX) by a 1:1 nearest neighbor matching method. The covariates included sex, age, diabetes, hypertension, direct bilirubin, indirect bilirubin, total bilirubin, uric acid, total cholesterol, high-density lipoprotein, low-density lipoprotein, triglycerides, red blood cell count, hemoglobin, white blood cell count, monocyte count, lymphocyte count, basophil count, eosinophil count, and platelet count.
In this study, continuous variables were summarized as means ± standard deviations, and categorical variables were summarized as frequencies or percentages (%). To compare the differences between the HAP and the non-HAP groups, the Student's t-test and chi-square test were performed both before and after PSM. A chi-square test was performed to analyze the differences in medication use and MECT between the HAP and non-HAP groups. The Bonferroni method was used to adjust the level of α for pairwise comparison (α = 0.05/26 = 0.0019). Logistic regression analysis was used to examine the impact of medications and MECT on HAP incidence, and an odds ratio (OR) was calculated with a 95% confidence interval (CI). Statistical analysis was performed using SPSS version 25.0 for Windows (SPSS Inc, Chicago, IL, USA), and P <0.05 was used as the cutoff for statistical significance.
A total of 19,392 inpatients with schizophrenia were screened and 7,085 participants were included (Figure 1). Among all patients, the median age was 39.77 ± 14.45 years and 3,119 (45.2%) were male. All patients were treated with antipsychotics. The patients were then divided into the HAP group (n = 193) and the non-HAP group (n = 6,892), and the incidence of HAP was 2.73%. The median time to HAP occurrence was 22.26±21.68 days after admission.
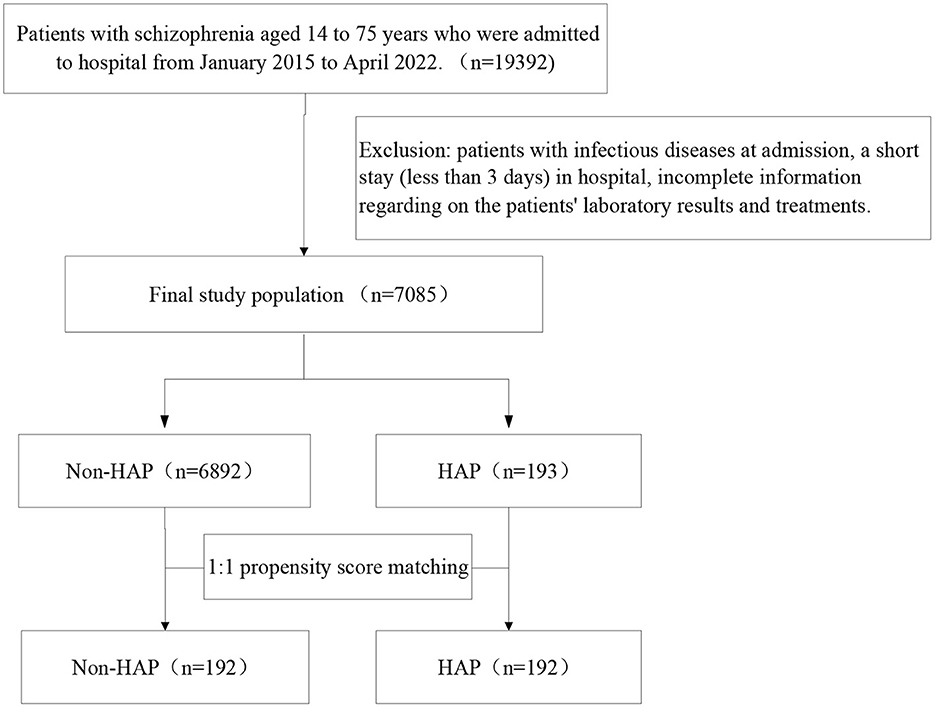
Figure 1. The study design flow chart.
Personal characteristics of the HAP group and non-HAP group before and after PSM are summarized in Table 1. Before PSM, the gender breakdowns of the HAP group and the non-HAP group were different (χ2=11.24, P = 0.001), and the age of the HAP group was higher than that of the non-HAP group (t = −3.32, P = 0.001). More people in the HAP group had diabetes (χ2=70.00, P<0.001) and hypertension (χ2= 56.16, P < 0.001). There were also statistically significant differences between the two groups in lab results, including blood direct bilirubin, total cholesterol, monocyte count, lymphocyte count, white blood cell count, basophil count, eosinophil count, red blood cell count, and platelet count at admission (P < 0.05) (Table 1). Monocyte count and lymphocyte count were also statistically significant differences between the two groups after Bonferroni correction (P < 0.001). After 1:1 PSM, the matched HAP (n = 192) and non-HAP groups (n = 192) were generated. The baseline characteristics were well-balanced, and there were no statistically significant differences between the two groups in age, sex, diabetes, hypertension, routine blood tests, or serum biochemical examinations at admission.
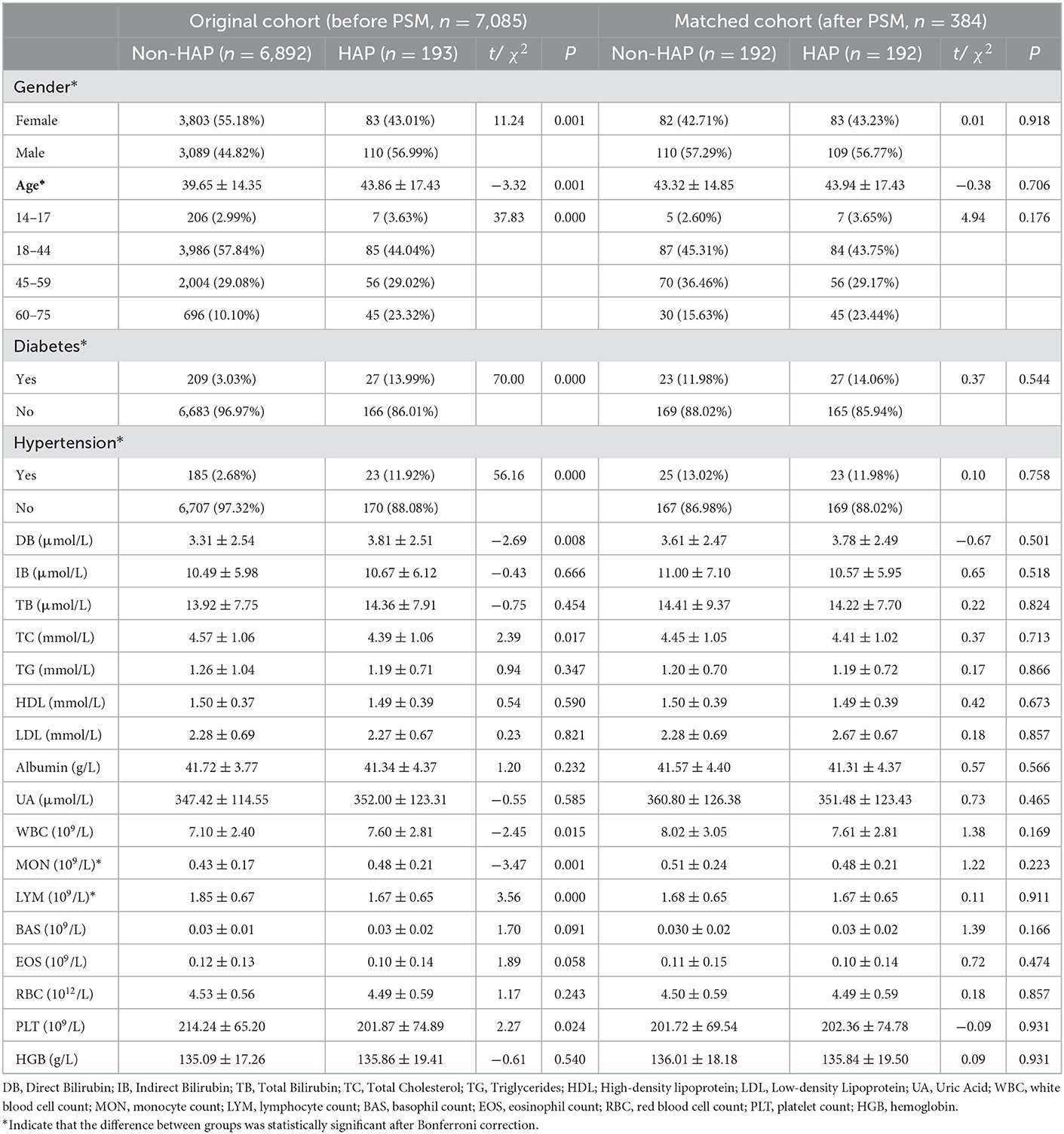
Table 1. Personal characteristics of patients with schizophrenia with and without HAP (before and after PSM).
After Bonferroni correction, The HAP group had significantly more patients taking benzodiazepines, antidepressants, mood stabilizers, and anti-parkinsonians both before and after PSM (P < 0.001) (Table 2). The multivariate logistic regression analysis revealed that except for antidepressants (OR = 3.01, 95%CI = 1.22–7.44, P = 0.017) and antiparkinsonians (OR =1.97, 95%CI = 1.22–3.17, P = 0.005), non-antipsychotic medicines including benzodiazepines (OR = 3.13, 95%CI = 1.95–5.03, P < 0.001), mood stabilizers (OR = 3.33, 95%CI = 1.79–6.20, P < 0.001) were significantly associated with an increased incidence of HAP in patients with schizophrenia treated with antipsychotics (P < 0.001) (Table 3).
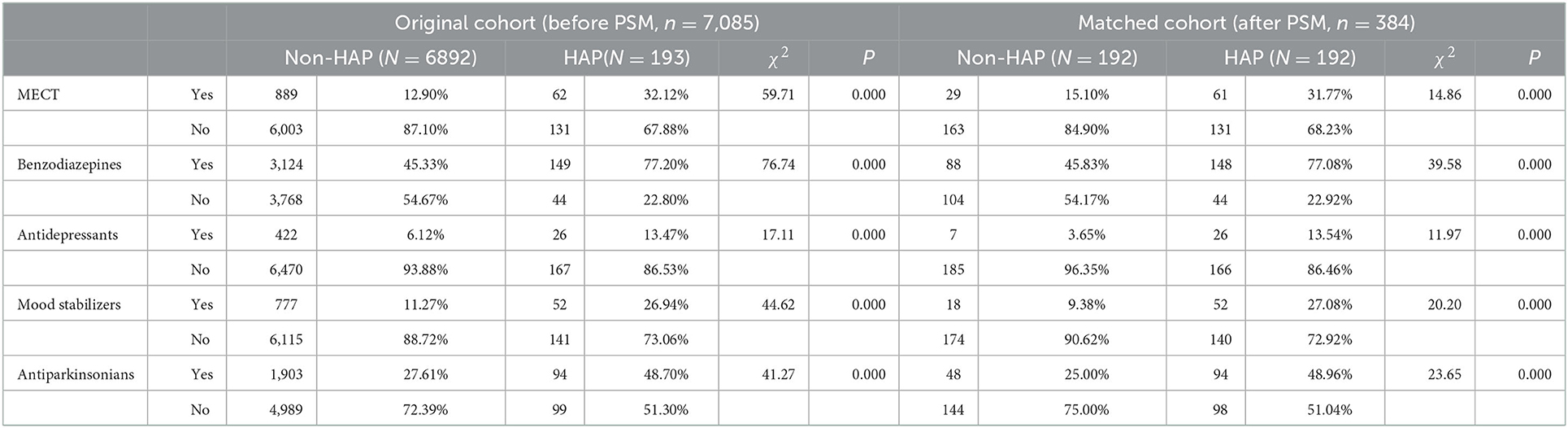
Table 2. Association of non-antipsychotic medicines and MECT with HAP in patients with schizophrenia treated with antipsychotics.
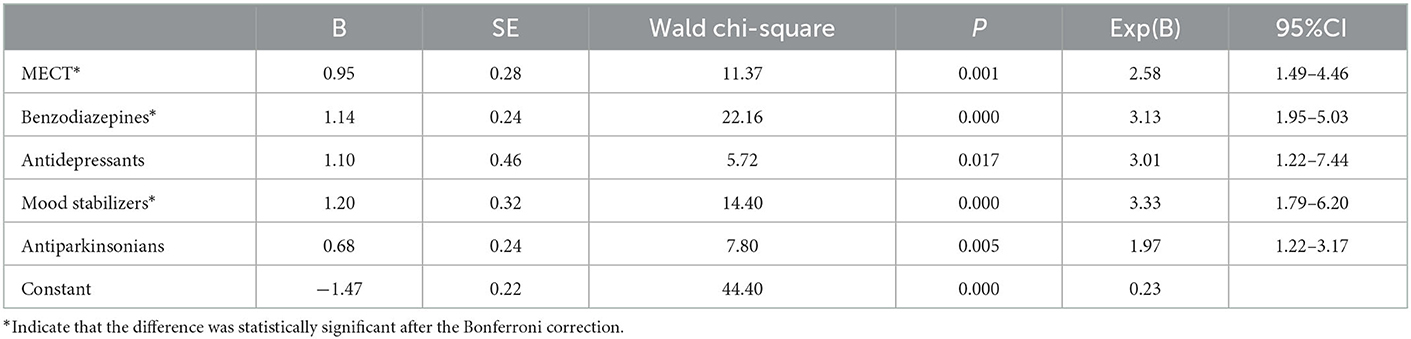
Table 3. Multivariate logistic regression analysis of risk factors for HAP in patients with schizophrenia treated with antipsychotics.
Before PSM, of the 193 patients with HAP, 62 patients (32.12%) were treated with MECT. The HAP group had significantly more patients who underwent MECT than the non-HAP group after PSM (χ2= 14.86, P < 0.001). From the multivariate logistic regression analysis, receiving MECT was significantly correlated with HAP (OR = 2.58, 95%CI = 1.49–4.46, P = 0.001).
Antipsychotic monotherapy is a recommended treatment for schizophrenia by the American Psychiatric Association Practice Guideline, but the combination of antipsychotics with non-antipsychotics or MECT is common in practice (19–22). Studies that have focused on pneumonia or HAP in patients with schizophrenia have only focused on the effects of antipsychotics (16, 23–25). However, the combination of other psychiatric drugs or treatment methods also needs to be considered. To our knowledge, this is the first study to examine the incidence of HAP in patients with schizophrenia in a specialized psychiatric hospital and to investigate whether non-antipsychotic medicines or MECT are risk factors for HAP in patients with schizophrenia treated with antipsychotics. This retrospective cohort study found a 2.73% of HAP for hospitalized patients with schizophrenia, which was higher than the overall incidence of 1.6% for nonventilator hospital-acquired pneumonia in the United States (26). After the Bonferroni correction, we found the HAP group had significantly more patients with MECT and taking benzodiazepines, antidepressants, mood stabilizers, and anti-parkinsonians both before and after PSM (P < 0.001). Multivariate logistic regression analysis showed that MECT and non-antipsychotic medicines only benzodiazepines and mood stabilizers were independent risk factors for HAP in patients with schizophrenia treated with antipsychotics.
It has been reported that benzodiazepines are effective drugs for anxiety, agitation, and insomnia (27). An antipsychotic-benzodiazepine combination treatment regimen is often necessary to control exacerbations of symptoms in the acute phase or severe psychotic relapses in patients with schizophrenia (5). Dublin et al. (28) and Iqbal et al. (29) suggested that benzodiazepines were not correlated with an increased risk of pneumonia. However, studies in recent years have had different results. Cheng et al. (30) reported a dose-dependent relationship between benzodiazepines and pneumonia in patients with schizophrenia and Taipale et al. (31) found that the use of benzodiazepine by patients with Alzheimer's disease was associated with an increased risk of pneumonia. A recent systematic review also reported that benzodiazepines and benzodiazepine-related drugs were associated with an increased pneumonia risk (32). Similar to recent reports, we found that benzodiazepine use increased the incidence of HAP in patients with schizophrenia treated with antipsychotics.
Adding a mood stabilizer is an option to reduce aggression or stabilize mood in patients with schizophrenia treated with antipsychotics (5). In this study, we found that the incidence of HAP was significantly higher in patients with schizophrenia who took mood stabilizers. Several studies have had similar results to ours. Taipale H et al. (33) found that mood stabilizers, including phenytoin, carbamazepine, valproic acid, and pregabalin, were associated with an increased risk of pneumonia. Han et al. (13) suggested that patients with mental disorders who received mood stabilizers had a higher likelihood of suffering HAP. Yang et al. (34) showed that patients treated with clozapine plus valproic acid (RR = 4.80, P < 0.001) and olanzapine plus carbamazepine (RR = 11.88, P < 0.01) had the highest risk of pneumonia.
Depressive symptoms are common in patients with schizophrenia, with an estimated incidence of about 25% (35). The addition of antidepressants to the treatment regimen of patients treated with antipsychotics is recommended to treat persistent symptoms, including depressive symptoms, negative symptoms, and other psychotic manifestations (5). Over the past decade, there have been conflicting reports regarding the relationship between the use of antidepressants and pneumonia. In 2007, Hennessy et al. (36) found that antidepressant use in elderly patients did not increase their risk of hospitalization for pneumonia or aspiration pneumonia. However, in 2018, Vozoris et al. (37) found that elderly patients using selective serotonin reuptake inhibitors/serotonin-noradrenaline reuptake inhibitors (SSRI/SNRI) had significantly higher rates of hospitalization for chronic obstructive pulmonary disease and pneumonia. In 2022, Kuo et al. (38) reported that the use of certain antidepressants of different classes was associated with pneumonia. We found that the HAP group had significantly more patients taking antidepressants, but multivariate logistic regression analysis showed no statistical difference. The differences between these findings as mentioned above may be a result of the different types or doses of antidepressants.
Among adults diagnosed with schizophrenia, 44% of anti-parkinsonian drugs were prescribed because of symptoms caused by antipsychotic treatment (20). Dies et al. (39) observed that patients treated with pramipexole had an increased rate of pneumonia (RR = 2.5,95%CI: 0.9–7.0) compared to placebo. In contrast, Ernst et al. (40) found that pramipexole did not increase the risk of pneumonia. We found that the HAP group had significantly more patients taking anti-parkinsonians, but multivariate logistic regression analysis showed no statistical difference. Since the use of anti-parkinsonians was related to the type and dose of antipsychotic drugs, more research is needed to investigate the interaction between antipsychotics and anti-parkinsonians on the occurrence of HAP.
Electroconvulsive therapy (ECT) has been used in psychiatry for more than 80 years (41). Traditional ECT involves passing an electrical current through the brain to cause a generalized seizure, but in modified ECT (MECT), anesthetics and muscle relaxants are applied before the treatment to alleviate side effects (42, 43). Although the therapeutic mechanism of MECT has not yet been fully elucidated, MECT is an effective and safe therapy for patients with schizophrenia if operating procedures are strictly followed. To our knowledge, this is the first report that MECT may increase the risk of HAP, with significantly higher rates of patients receiving MECT in the HAP group than in the non-HAP group after PSM (31.77 vs. 15.10%).
Drug-induced salivation, sedation, and anticholinergic effects may be responsible for HAP in patients with schizophrenia, which are the most common adverse effects of antipsychotics, antidepressants, benzodiazepines, mood stabilizers, and anti-parkinsonians (44). The mechanism may be mediated by several receptor mechanisms. Antipsychotics bind to dopaminergic, muscarinic 1 (M1), and histaminergic 1 (H1) receptors, resulting in sedation, anticholinergic effects, extrapyramidal symptoms, and hypersalivation. These symptoms may lead to dysphagia, aspiration, and pneumonia (45). In addition, antidepressants typically block the muscarinic (acetylcholine), histaminic (H1), dopaminergic (D2), alpha-1 adrenergic, and possibly serotonergic (5-HT2A) receptors, leading to salivation, sedation, and anticholinergic effects (46). Benzodiazepines act on the γ-aminobutyric acid (GABAA) receptors, and the most common adverse reaction is sedation, possibly leading to an increased risk of aspiration pneumonia (47). Mood stabilizers, especially antiepileptics, have been reported to have a sedative effect in elderly patients, which may increase the risk of aspiration and pneumonia (48, 49). Anti-parkinsonians such as trihexyphenidyl are commonly used in the treatment of Parkinsonian syndrome and for extrapyramidal reactions in schizophrenia, which have anticholinergic effects and can lead to malignant hyperthermia, both of which may increase the risk of HAP (48, 50).
The effects of MECT and medications on the immune system may also contribute to HAP in patients with schizophrenia. Serum cytokine concentration is closely associated with infections. High levels of interleukin (IL)-6 and IL-10 have been associated with poor prognosis in community-acquired pneumonia (51–53). A systematic review found that concentrations of tumor necrosis factor (TNF)-α, IL-1β, and IL-6 were elevated after a single session of MECT (54). Another meta-analysis revealed that MECT induced an increase in IL-6 levels and a potential decrease in TNF-α levels (55). Guloksuz et al. (56) suggested that repetitive MECT may downregulate immune activation, which may be associated with pneumonia. Psychotropic drugs have also been found to have both direct and indirect effects on the immune system that could lead to an increased risk of pneumonia (17, 57). Benzodiazepines have been reported to potentially increase pneumonia susceptibility as they have been found to activate certain GABA receptors on immune cells in mice (58).
It should be noted that catatonia is a typical condition of patients with schizophrenia who primarily required MECT and benzodiazepines treatment. Catatonia itself is a confounding factor in assessing whether MECT or benzodiazepines are risk factors, as they tend to induce aspiration pneumonia (59).
This study has several certain limitations. First, because this study is a retrospective study, no data were available such as body mass index, smoking, alcohol use, and hospital environment, which may be related to the risk of infection. Second, some potential confounding factors, such as physical complications, concomitant physical medications, and the severity of schizophrenia symptoms (e.g., catatonia) were missing from our analysis. Third, we did not analyze specific antipsychotics and dosages while studying the effects of MECT and non-antipsychotic medicines on HAP. Although exposure to both first-generation antipsychotics and second-generation antipsychotics is associated with an increased risk of pneumonia, clozapine is considered to be the most relevant. Therefore, the dose and type of antipsychotics should be taken into account in future research. Fourth, we provide evidence to support a causal relationship between MECT, non-antipsychotic medicines, and HAP, but the specific drug and mechanisms are still unclear. Finally, this is a single-center study, and a prospective multicenter study with a larger sample size is necessary to further validate our results.
In this study, we found a HAP incidence of 2.73% in patients with schizophrenia. MECT and non-antipsychotic medicines including benzodiazepines and mood stabilizers were independent risk factors for HAP in patients with schizophrenia treated with antipsychotics.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Institutional Review Committee of the Fourth People's Hospital of Chengdu. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
YY and MY contributed to the conception and design of the study, performed the statistical analysis, and acquired the funding. DK, WC, XT, XH, and MX organized the database. YY wrote the first draft of the manuscript. QL, MY, ZZ, CF, and YW wrote sections of the manuscript. YY, GZ, and MY reviewed the manuscript. All authors contributed to the manuscript revision, read, and approved the submitted version.
This research was funded by the National Natural Science Foundation of China (62073058), Chengdu Science and Technology Bureau (2022-YF05-01867-SN), and Chengdu Municipal Health Commission (2021057, 2022406).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hasan A, Falkai P, Wobrock T, Lieberman J, Glenthøj B, Gattaz WF, et al. World federation of societies of biological psychiatry (WFSBP) guidelines for biological treatment of schizophrenia - a short version for primary care. Int J Psychiatry Clin Pract. (2017) 21:82–90. doi: 10.1080/13651501.2017.1291839
2. Remington G, Addington D, Honer W, Ismail Z, Raedler T, Teedan M. Guidelines for the pharmacotherapy of schizophrenia in adults. Can J Psychiatry. (2017) 62:604–16. doi: 10.1177/0706743717720448
3. Grover S, Sahoo S, Rabha A, Koirala R, ECT. in schizophrenia: a review of the evidence. Acta Neuropsychiatr. (2019) 31:115–27. doi: 10.1017/neu.2018.32
4. Lähteenvuo M, Tiihonen J. Antipsychotic polypharmacy for the management of schizophrenia: evidence and recommendations. Drugs. (2021) 81:1273–84. doi: 10.1007/s40265-021-01556-4
5. Baandrup L. Polypharmacy in schizophrenia. Basic Clin Pharmacol Toxicol. (2020) 126:183–92. doi: 10.1111/bcpt.13384
6. Dold M, Li C, Gillies D, Leucht S. Benzodiazepine augmentation of antipsychotic drugs in schizophrenia: a meta-analysis and Cochrane review of randomized controlled trials. Eur Neuropsychopharmacol. (2013) 23:1023–33. doi: 10.1016/j.euroneuro.2013.03.001
7. Helfer B, Samara MT, Huhn M, Klupp E, Leucht C, Zhu Y, et al. Efficacy and safety of antidepressants added to antipsychotics for schizophrenia: a systematic review and meta-analysis. Am J Psychiatry. (2016) 173:876–86. doi: 10.1176/appi.ajp.2016.15081035
8. Hosák L, Libiger J. Antiepileptic drugs in schizophrenia: a review. Eur Psychiatry. (2002) 17:371–8. doi: 10.1016/s0924-9338(02)00696-x
9. Pompili M, Lester D, Dominici G, Longo L, Marconi G, Forte A, et al. Indications for electroconvulsive treatment in schizophrenia: a systematic review. Schizophr Res. (2013) 146:1–9. doi: 10.1016/j.schres.2013.02.005
10. Tzur Bitan D, Krieger I, Kridin K, Komaantscher D, Scheinman Y, Weinstein O, et al. COVID-19 prevalence and mortality among schizophrenia patients: a large-scale retrospective cohort study. Schizophr Bull. (2021) 47:1211–7. doi: 10.1093/schbul/sbab012
11. Nemani K, Li C, Olfson M, Blessing EM, Razavian N, Chen J, et al. Association of psychiatric disorders with mortality among patients with COVID-19. JAMA Psychiatry. (2021) 78:380–6. doi: 10.1001/jamapsychiatry.2020.4442
12. Modi AR, Kovacs CS. Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Cleve Clin J Med. (2020) 87:633–9. doi: 10.3949/ccjm.87a.19117
13. Han J, Lv Z, Shen M, Wan Q, Xiao L, Wang G. Risk factors for hospital-acquired pneumonia among inpatients with mental disorders in a large mental health center within a tertiary general hospital. Am J Infect Control. (2022) S0196-6553(22)00501-6. doi: 10.1016/j.ajic.2022.06.014
14. Yang M, Li Q, Wang C, Li L, Xu M, Yan F, et al. Influencing factors of hospital-acquired pneumonia infection in the middle-aged and elderly patients with schizophrenia. Front Psychiatry. (2021)12:746791. doi: 10.3389/fpsyt.2021.746791
15. Vignari M. Non-ventilator health care-associated pneumonia (NV-HAP): NV-HAP risk factors. Am J Infect Control. (2020) 48:A10-A13. doi: 10.1016/j.ajic.2020.03.010
16. Kuo KM, Talley PC, Huang CH, Cheng LC. Predicting hospital-acquired pneumonia among schizophrenic patients: a machine learning approach. BMC Med Inform Decis Mak. (2019) 19:42. doi: 10.1186/s12911-019-0792-1
17. Rajamaki B, Hartikainen S, Tolppanen AM. Psychotropic drug-associated pneumonia in older adults. Drugs Aging. (2020) 37:241–61. doi: 10.1007/s40266-020-00754-1
18. Tirmizi O, Raza A, Trevino K. et al. Electroconvulsive therapy: how modern techniques improve patient outcomes: refinements have decreased memory loss, other adverse effects while retaining efficacy: refinements have decreased memory loss, other adverse effects while retaining efficacy. Curr Psychiatr. (2012) 11:24–46.
19. Keepers GA, Fochtmann LJ, Anzia JM, Benjamin S, Lyness J, Mijtabai R, et al. The American psychiatric association practice guideline for the treatment of patients with schizophrenia. Am J Psychiatry. (2020) 177:868–72. doi: 10.1176/appi.ajp.2020.177901
20. Patrichi B, Tăpoi C, Rogojină RS, Badreage I, Dumitrache A, Itu A, et al. Antipsychotic polypharmacy in adult patients diagnosed with schizophrenia: a retrospective study. Exp Ther Med. (2021) 22:1225. doi: 10.3892/etm.2021.10659
21. Correll CU, Rubio JM, Inczedy-Farkas G, Birnbaum ML, Kane JM, Leucht S. Efficacy of 42 pharmacologic cotreatment strategies added to antipsychotic monotherapy in schizophrenia: systematic overview and quality appraisal of the meta-analytic evidence. JAMA Psychiatry. (2017) 74:675–84. doi: 10.1001/jamapsychiatry.2017.0624
22. Anozie IG, James BO, Omoaregba JO. Antipsychotic prescription and polypharmacy among outpatients with schizophrenia in a Nigerian hospital. Niger Postgrad Med J. (2020) 27:30–6. doi: 10.4103/npmj.npmj_93_19
23. Dzahini O, Singh N, Taylor D, Haddad PM. Antipsychotic drug use and pneumonia: Systematic review and meta-analysis. J Psychopharmacol. (2018) 32:1167–81. doi: 10.1177/0269881118795333
24. Kuo CJ, Yang SY, Liao YT, Liao YT, Chen WJ, Lee WC, et al. Second-generation antipsychotic medications and risk of pneumonia in schizophrenia. Schizophr Bull. (2013) 39:648–57. doi: 10.1093/schbul/sbr202
25. Milano VR, Kayhart BM, Morgan RJ, DeSimone DC, Mara K, Leung J. Second-generation antipsychotics and pneumonia-related hospitalizations. Prim Care Companion CNS Disord. (2020) 22:20m02594. doi: 10.4088/PCC.20m02594
26. Giuliano KK, Baker D, Quinn B. The epidemiology of nonventilator hospital-acquired pneumonia in the United States. Am J Infect Control. (2018) 46:322–7. doi: 10.1016/j.ajic.2017.09.005
27. Dold M, Li C, Tardy M, Khorsand V, Gillies D, Leucht S. Benzodiazepines for schizophrenia. Cochrane Database Syst Rev. (2012) 11:CD006391. doi: 10.1002/14651858.CD006391.pub2
28. Dublin S, Walker RL, Jackson ML, Nelson JC, Weiss NS, Von Korff M, et al. Use of opioids or benzodiazepines and risk of pneumonia in older adults: a population-based case-control study. J Am Geriatr Soc. (2011) 59:1899–907. doi: 10.1111/j.1532-5415.2011.03586.x
29. Iqbal U, Syed-Abdul S, Nguyen PA, Jian WS Li YC. The impact of benzodiazepines on occurrence of pneumonia and mortality from pneumonia: a nested case-control and survival analysis in a population-based cohort. Thorax. (2013) 68:591–2. doi: 10.1136/thoraxjnl-2013-203211
30. Cheng S-Y, Chen W-Y, Liu H-C, Yang T-W, Pan C-H, Yang S-Y, et al. Benzodiazepines and risk of pneumonia in schizophrenia: a nationwide case-control study. Psychopharmacology (Berl). (2018) 235:3329–38. doi: 10.1007/s00213-018-5039-9
31. Taipale H, Tolppanen A-M, Koponen M, Tanskanen A, Lavikainen P, Sund R, et al. Risk of pneumonia associated with incident benzodiazepine use among community-dwelling adults with Alzheimer disease. CMAJ. (2017) 189:E519–29. doi: 10.1503/cmaj.160126
32. Sun GQ, Zhang L, Zhang LN, Wu Z, Hu DF. Benzodiazepines or related drugs and risk of pneumonia: A systematic review and meta-analysis. Int J Geriatr Psychiatry. (2019) 34:513–21. doi: 10.1002/gps.5048
33. Taipale H, Lampela P, Koponen M, Tanskanen A, Tiihonen J, Hartikainen S, et al. Antiepileptic drug use is associated with an increased risk of pneumonia among community-dwelling persons with alzheimer's disease-matched cohort study. J Alzheimers Dis. (2019) 68:127–36. doi: 10.3233/JAD-180912
34. Yang S-Y, Liao Y-T, Liu H-C, Chen WJ, Chen C-C, Kuo C-J. Antipsychotic drugs, mood stabilizers, and risk of pneumonia in bipolar disorder: a nationwide case-control study. J Clin Psychiatry. (2013) 74:e79–86. doi: 10.4088/JCP.12m07938
35. Mao YM, Zhang MD. Augmentation with antidepressants in schizophrenia treatment: benefit or risk. Neuropsychiatr Dis Treat. (2015).11:701–13. doi: 10.2147/NDT.S62266
36. Hennessy S, Bilker WB, Leonard CE, Chittams J, Palumbo CM, Karlawish JH, et al. Observed association between antidepressant use and pneumonia risk was confounded by comorbidity measures. J Clin Epidemiol. (2007) 60:911–8. doi: 10.1016/j.jclinepi.2006.11.022
37. Vozoris NT, Wang X, Austin PC, Stephenson AL, O'Donnell DE, Gershon AS, et al. Serotonergic antidepressant use and morbidity and mortality among older adults with COPD. Eur Respir J. (2018) 52:1800475. doi: 10.1183/13993003.00475-2018
38. Kuo W-Y, Huang K-H, Kuan Y-H, Chang Y-C, Tsai T-H, Lee C-Y. Antidepressants usage and risk of pneumonia among elderly patients with the parkinson's disease: a population-based case-control study. Front Med (Lausanne). (2022) 9:740182. doi: 10.3389/fmed.2022.740182
39. Dies I, Hoffmann H, Albrecht S. Periodic safety update report sifrol no.12. 2009U09-001-01; Section 7.1.3; 2009 (Personal communication, Dr. Bartels, Boehringer Ingelheim).
40. Ernst P, Renoux C, Dell'Aniello S. Pramipexole use and the risk of pneumonia. BMC Neurol. (2012) 12:113. doi: 10.1186/1471-2377-12-113
41. Gazdag G, Ungvari GS. Electroconvulsive therapy: 80 years old and still going strong. World J Psychiatry. (2019) 9(1):1-6. doi: 10.5498/wjp.v9.i1.1
42. Lava-Parmele S, Lava C, Parmele JB. The historical struggles of modified electroconvulsive therapy: how anesthesia came to the rescue. J Anesth Hist. (2021) 7:17–25. doi: 10.1016/j.janh.2021.03.001
43. ARDIS JA, WYLLIE AM. The routine use of muscular relaxants prior to electrical convulsive therapy. J Ment Sci. (1953) 99:148–53. doi: 10.1192/bjp.99.414.148
44. Chatterjee S, Carnahan RM, Chen H, Holmes HM, Johnson ML, Aparasu RR. Anticholinergic medication use and risk of pneumonia in elderly adults: a nested case-control study. J Am Geriatr Soc. (2016) 64:394–400. doi: 10.1111/jgs.13932
45. Cicala G, Barbieri MA, Spina E, Leon J. A comprehensive review of swallowing difficulties and dysphagia associated with antipsychotics in adults. Expert Rev Clin Pharmacol. (2019) 12:219–34. doi: 10.1080/17512433.2019.1577134
46. Khawam EA, Laurencic G, Malone DA Jr. Side effects of antidepressants: an overview. Cleve Clin J Med. (2006) 73:351–61. doi: 10.3949/ccjm.73.4.351
47. Juergens SM. Problems with benzodiazepines in elderly patients. Mayo Clin Proc. (1993) 68:818–20. doi: 10.1016/s0025-6196(12)60643-0
48. Loeb M, McGeer A, McArthur M, Walter S, Simor AE. Risk factors for pneumonia and other lower respiratory tract infections in elderly residents of long-term care facilities. Arch Intern Med. (1999) 159:2058–64. doi: 10.1001/archinte.159.17.2058
49. Eddy CM, Rickards HE, Cavanna AE. The cognitive impact of antiepileptic drugs. Ther Adv Neurol Disord. (2011) 4:385–407. doi: 10.1177/1756285611417920
50. Zhao J, Xu G, Feng C, Chen Y, Kang Y, Liu F, et al. Trihexyphenidyl induced malignant hyperthermia in a patient with Parkinson's disease complicated with pneumonia: A case report. Medicine (Baltimore). (2020) 99:e20129. doi: 10.1097/MD.0000000000020129
51. Broman N, Rantasärkkä K, Feuth T, Valtonen M, Waris M, Hohenthal U, et al. IL-6 and other biomarkers as predictors of severity in COVID-19. Ann Med. (2021) 53:410–2. doi: 10.1080/07853890.2020.1840621
52. de Brito RdCM, Lucena-Silva N, Torres LC, Luna CF, Correia Jd, da Silva GAP. The balance between the serum levels of IL-6 and IL-10 cytokines discriminates mild and severe acute pneumonia. BMC Pulm Med. (2016) 16:170. doi: 10.1186/s12890-016-0324-z
53. Martínez R, Menéndez R, Reyes S, Polverino E, Cillóniz C, Martínez A, et al. Factors associated with inflammatory cytokine patterns in community-acquired pneumonia. Eur Respir J. (2011) 37:393–9. doi: 10.1183/09031936.00040710
54. Yrondi A, Sporer M, Péran P, Schmitt L, Arbus C, Sauvaget A. Electroconvulsive therapy, depression, the immune system and inflammation: a systematic review. Brain Stimul. (2018) 11:29–51. doi: 10.1016/j.brs.2017.10.013
55. Gay F, Romeo B, Martelli C, Benyamina A, Hamdani N. Cytokines changes associated with electroconvulsive therapy in patients with treatment-resistant depression: a Meta-analysis. Psychiatry Res. (2021) 297:113735. doi: 10.1016/j.psychres.2021.113735
56. Guloksuz S, Rutten BP, Arts B, van Os J, Kenis G. The immune system and electroconvulsive therapy for depression. J ECT. (2014) 30:132–7. doi: 10.1097/YCT.0000000000000127
57. Pollmächer T, Haack M, Schuld A, Kraus T, Hinze-Selch D. Effects of antipsychotic drugs on cytokine networks. J Psychiatr Res. (2000) 34:369–82. doi: 10.1016/s0022-3956(00)00032-7
58. Sanders RD, Godlee A, Fujimori T, Goulding J, Xin G, Salek-Ardakani S, et al. Benzodiazepine augmented γ-amino-butyric acid signaling increases mortality from pneumonia in mice. Crit Care Med. (2013) 41:1627–36. doi: 10.1097/CCM.0b013e31827c0c8d
Keywords: schizophrenia, hospital-acquired pneumonia, modified electroconvulsive therapy, benzodiazepines, mood stabilizers
Citation: Yang Y, Kong D, Li Q, Chen W, Zhao G, Tan X, Huang X, Zhang Z, Feng C, Xu M, Wan Y and Yang M (2023) Non-antipsychotic medicines and modified electroconvulsive therapy are risk factors for hospital-acquired pneumonia in schizophrenia patients. Front. Psychiatry 13:1071079. doi: 10.3389/fpsyt.2022.1071079
Received: 20 October 2022; Accepted: 28 December 2022;
Published: 13 January 2023.
Edited by:
Sarah Tosato, University of Verona, ItalyReviewed by:
Takashi Tsuboi, Kyorin University, JapanCopyright © 2023 Yang, Kong, Li, Chen, Zhao, Tan, Huang, Zhang, Feng, Xu, Wan and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mi Yang,  NTY1MTM2MTcwQHFxLmNvbQ==
NTY1MTM2MTcwQHFxLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.