 Cui Yang
Cui Yang Xiaofeng Hou1†
Xiaofeng Hou1† Dongmei Wu
Dongmei Wu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry, 04 January 2023
Sec. Schizophrenia
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.1067260
Objective: This study aimed to understand frailty and its influencing factors in inpatients with Schizophrenia in Chengdu and to explore correlations between frailty and quality of life.
Methods: From May to July 2022, inpatients with Schizophrenia were surveyed using a general information questionnaire, frailty phenotype (FP) scoring, the Self-Rating Depression Scale (SDS), the Mini-Mental State Examination (MMSE), and the SZ Quality of Life Scale (SQLS). Multivariate logistic regression was conducted to assess factors influencing frailty and multivariate linear regression was conducted to assess the factors influencing quality of life.
Results: A total of 556 hospitalized patients with Schizophrenia were included and divided into three groups according to the degree of frailty, of which 153 cases (27.5%) were without frailty, 348 cases (62.6%) were in early frailty, and 55 cases (9.9%) were in frailty. Univariate analysis of age, history of falls during hospitalization, polypharmacy, compulsory treatment during hospitalization, self-reported health status, activity level, cognitive impairment, depressive symptoms, “psychology and society,” “motivation and energy” and “symptoms and side-effects” showed statistically significant differences between the groups. Multinomial logistic regression showed that age, BMI, self-reported health, activity, cognitive impairment, motivation and energy, and symptoms and side-effects were influencing factors for frailty in hospitalized patients with Schizophrenia. Correlation analysis shows that frailty score positively correlated with SQLS score.
Conclusion: We found that frailty was prevalent and that frailty was positively correlated with SQLS scores in inpatients with Schizophrenia. To effectively manage the frailty of hospitalized patients with Schizophrenia, medical staff should pay attention to its influencing factors and quality of life.
Schizophrenia (SZ) is a severe mental disorder of unknown etiology often with onset in early adulthood, recurrent relapses, a high disability rate, and a significant increase in the economic burden on families and society (1). Due to the chronic and reoccurring nature of the disease, the heavy burden of family care, and commonly insufficient community medical care, patients with SZ often require long-term hospitalization (2).
Frailty is defined as a decrease in the body’s multisystem reserve capacity that increases an individual’s susceptibility to small internal and external stimuli (3, 4). Frailty is usually assessed in older adults, and identifying frailty in adults under 60 may also be of value (5, 6). Some vulnerable groups with chronic diseases may be at risk of debilitation early in life (7–12). The accelerated aging hypothesis of SZ (13–17) states that physiological changes in patients with SZ tend to occur earlier than in the general population. Basic research (18–20) has shown that leukocyte telomere length, a new marker of cellular aging, is significantly shortened in patients with SZ, suggesting that they are more likely to age prematurely than the general population.
Quality of life is divided into the objective quality of life and subjective life satisfaction (20). Due to changes in medical models, the treatment goals and prognosis evaluation for SZ are no longer limited to the relief of clinical symptoms but also include comprehensive improvement of quality of life (21). Subjective quality of life in SZ is a subjective index for evaluating treatment effects, which can effectively reflect the current health status of the human body and the satisfaction with physical, psychological, social, and behavioral functions. This can guide policies and practices for patients with mental disorders (22).
Frailty increases the risk of adverse health outcomes (23), affects the employment outcomes of patients with SZ (24), increases the physical and psychological burden, and reduces the social quality of life. The relationship between frailty and quality of life is bidirectional (25), with poor quality of life leading to increased risk of frailty and frailty predisposing people to low quality of life, so understanding the relationship between frailty and quality of life is critical. Although studies in older age groups and patients with cancer have demonstrated a link between frailty and quality of life (26, 27), an extensive literature search found few studies on frailty in hospitalized patients with SZ and no evidence on the relationship between frailty and quality of life. Thus, the present study intended to explore the status of and factors contributing to frailty in inpatients with SZ and the correlation between frailty and quality of life.
From May to July 2022, we facilitated a sample of inpatients with SZ from four psychiatric hospitals in Chengdu. Inclusion criteria: hospitalized patients aged ≥ 18 years; diagnosis by attending psychiatrists meeting the diagnostic criteria for SZ in the 10th edition of the International Classification of Diseases (ICD-10) (28); Most of the treated psychiatric symptoms disappeared after hospitalization and stabilized during the investigation period, with a score of < 60 on the Positive and Negative Symptom Scale (PANSS) (29); No visual, hearing, or communication impairments (or these could be corrected). Exclusion criteria: comorbid intellectual disability, dementia, or other mental disorders; severe physical disease or brain organic disease; poor compliance, severe aggressive behavior, or suicidality. The Fourth People’s Hospital of Chengdu Ethics Committee approved this study.
There following five questionnaires were included: demographic data, the Fried frailty phenotype (FP) (3), the Mini-Mental State Examination (MMSE) (30), the Self-Rating Depression Scale (SDS) (31) and the SZ Quality of Life Scale (SQLS) (32). Researchers screened the participants who met the inclusion and exclusion criteria and distributed questionnaires, using unified guidelines to explain the research purpose and significance. The participants filled out the questionnaires independently, and the researchers collected them immediately and checked each item to ensure completeness. If the participants did not understand the content of any items, the researchers provided explanations according to the respective scale guide.
The FP (3) was used to screen the frailty of hospitalized patients with SZ. It includes five items: unexpected weight loss, fatigue, loss of grip strength, slowed pace, and reduced fitness. Frailty syndrome is defined as the presence of three or more items, fewer than three items is categorized as pre-frailty, and zero items means no frailty. The FP focuses on physical weakness of the body using objective and quantitative evaluation indicators and has a high predictive ability for weakened states. Tsai et al. (33) also used this to evaluate frailty in hospitalized patients with SZ in Taiwan. The present study measured grip strength using a Camry digital grip dynamometer (EH101; South El Monte, CA, USA). Patients were instructed to stand upright, with both feet separated and arms hanging naturally. Full-force grip strength was measured in one hand, and the maximum value of three measurements was recorded. Moreover, pace was measured with patients instructed to walk naturally for 4.5 m from a starting point, and the time was recorded with a stopwatch; the minimum value over three measurements was used.
The MMSE, developed by Folstein et al. (30) in 1975 and one of the most influential cognitive function screening tools, was used to assess the cognitive status of hospitalized patients with SZ. The MMSE consists of 30 items covering orientation, memory, attention and calculation, recall ability, and language ability. The scale is easy to operate and suitable for evaluating cognitive dysfunction in SZ (34). The scale has a maximum score of 30 points, with higher scores indicating better cognitive function; ≥ 27 points indicates normal cognitive function and < 27 indicates cognitive dysfunction.
The SDS, created by Zung et al. (31) was used to assess depressive symptoms. The scale consists of 20 items and reflects subjective feelings of patients by evaluating the frequency of depressive symptoms corresponding to each item. A 4-level rating was used: 1 point, for no or very low frequency, 2 points for low frequency, 3 points for a considerable frequency, and 4 points for high or continuous frequency; Ten items were scored in reverse. The total score of each item was the raw score, and this was multiplied by 1.25 and rounded up to the standard score. The SDS standard score ranges from 25 to 100 points. The higher the score, the more severe the depressive state, with good reliability and validity (35). Patients with an SDS standard score ≥ 50 were considered to have depressive symptoms.
The SQLS was used to evaluate inpatient quality of life. The scale was developed by British psychiatrist Greg Wilkingsony (32) in 1999 and includes three scales with a total of 30 items: psychosocial, motivation and energy, and symptoms and side-effects, using a 5-point scale (0 = “never”, 1 = “occasionally”, 2 = “sometimes”, 3 = “often”, 4 = “always”). Items 12, 13, 15 and 20 are reverse-scored. Each subscale is calculated as follows: psychosocial subscale = rough score of 15 items/(4 × 15) × 100; energy/motivation subscale = rough score of 7 items/(4 × 7) × 100; symptom/adverse response subscale = crude score of 8 items/(4 × 8) × 100. The total score for each subscale is 0 to 100, and the higher the score, the worse the subjective quality of life. Luo (36) introduced a translated Chinese version of the SQLS in 2002. The test-retest reliability of the Chinese version is 0.87, and Cronbach’s α is 0.70–0.92. It has good reliability and validity and is suitable for assessment of the quality of life in patients with SZ.
The socioeconomic and demographic factors selected were age group (18–44 years, 45–59 years, and 60 years or older); sex (male, female), education (primary school and below, junior school, high school, college and above); family monthly income (1000 Chinese yuan and less, 1,000–3,000 yuan, 3,001–5,000 yuan, 5,000 yuan and more); and frequency of family visits (none, 1 to 2 times/month, 3 times or more/month).
Factors used to assess patient health were age of onset (18 years below, 18–44 years, 45–59 years, and 60 years and older); disease duration (5 years below, 5–10 years, and10 years and above); smoking history (yes/no); history of falls during hospitalization (yes/no); family history of psychosis (yes/no); polypharmacy (yes/no); compulsory treatment during hospitalization (yes/no); activity levels (normal/low/inactive); self-reported health (good/fair/poor); and body mass index (BMI; calculated based on height and weight).
SPSS statistical software (v. 26.0; IBM Corp., Armonk, NY, USA) was used for data analysis. Count data are expressed as frequency and percentage, measurement data obeyed normal distribution and are expressed as the means and standard deviations. The Chi-squared test, Student’s t test and Analysis of Variance were used to compare groups. Logistic regression was used to analyze the influencing factors of frailty and Linear regression analysis was used to analyze the influencing factors of quality of life. Non-frail or frail was the dependent variable, and considering the interference factors, the univariate analysis of demographic data, age, sex, education, family monthly income, frequency of family visits, age of onset, smoking history, history of falls during hospitalization, family history of psychosis, polypharmacy, compulsory treatment during hospitalization, self-reported health, activity level, cognitive impairment, depressive symptoms, disease duration and SQLS scores with all variables were independent variables except for the dependent variable. SQLS scores was the dependent variable, and the inclusion method of independent variables was the same as that of frailty influencing factor analysis. The correlation between frailty and SQLS scores was analyzed. Spearman correlation analysis was used because the data did not follow a normal distribution. A p value < 0.05 was considered statistically significant.
A total of 570 hospitalized patients with SZ met the inclusion and exclusion criteria, and the number of completed questionnaires was 556 (97.5%). The sample had the following characteristics: most of the participants were male, patients were between 45 and 59 years old, and 31.1% had finished high school or technical secondary school education; 45.0% had a BMI of 18.5–23.9 kg/m2; 35.3% has a monthly household income 1,000–3,000 Chinese yuan; 44.6% had a frequency of family visits of 0 times/month; 85.3% had an age at first SZ diagnosis of 18–44 years old; 48.0% had a history of smoking; 22.8% had a history of falls during hospitalization; 18.9% had a family history of mental illness; 41.4% had polypharmacy; and 41.9% received compulsory treatment during hospitalization. The average SQLS score was 83.82 ± 40.30.
The characteristics of the participants based on different degrees of frailty are shown in Table 1. There were 153 cases (27.5%) of no frailty, 348 (62.6%) of pre-frailty, and 55 (9.9%) of frailty, and the mean frailty score of the 556 participants was 1.17 ± 1.00. As can be seen in Table 1, age, history of falls during hospitalization, polypharmacy, compulsory treatment during hospitalization, self-reported health status, activity level, cognitive impairment, depressive symptoms, “psychology and society,” “motivation and energy,” and “symptoms and side-effects” showed statistically significant differences among patients with different degrees of frailty (P < 0.05). The occurrence of frailty is shown in Table 2.
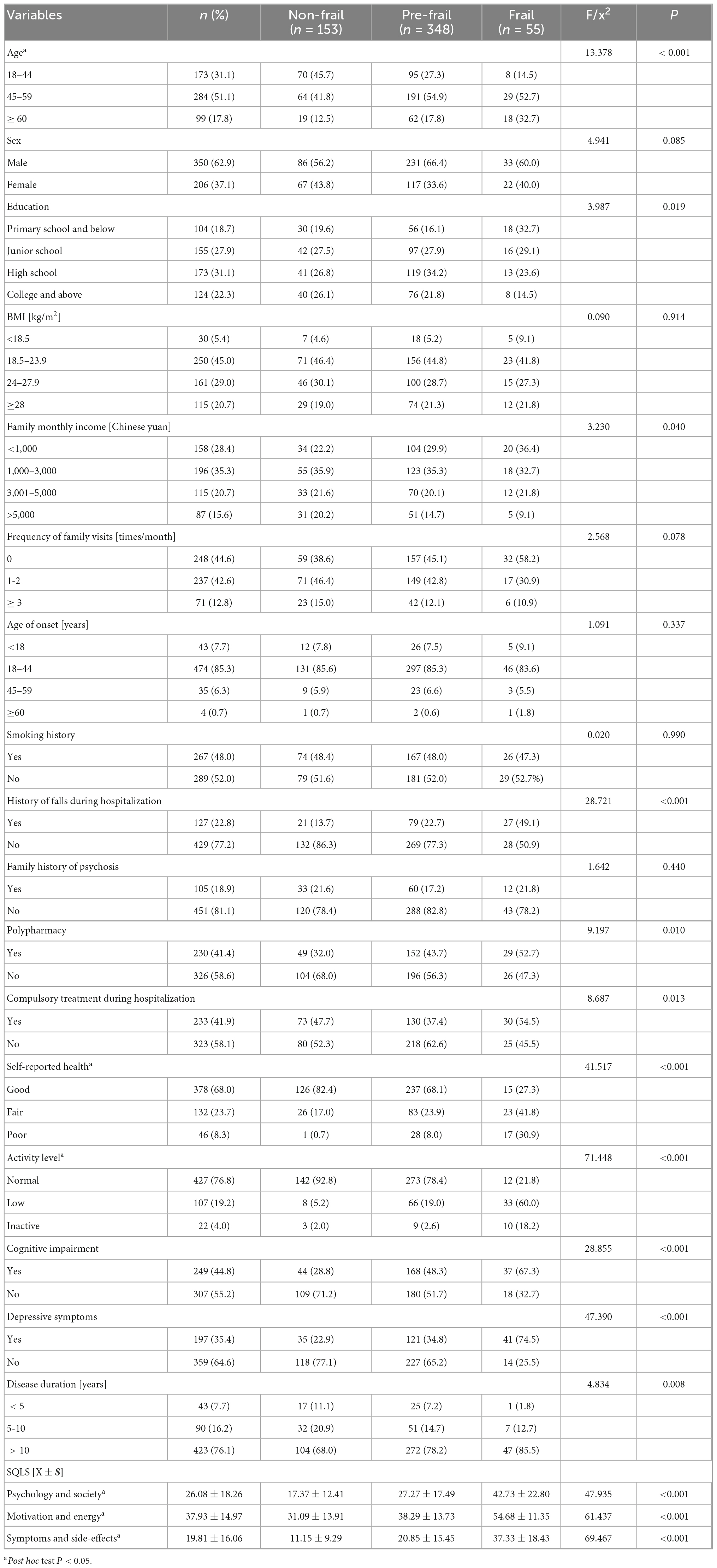
Table 1. Characteristics of the participants based on different frailty (n = 556).
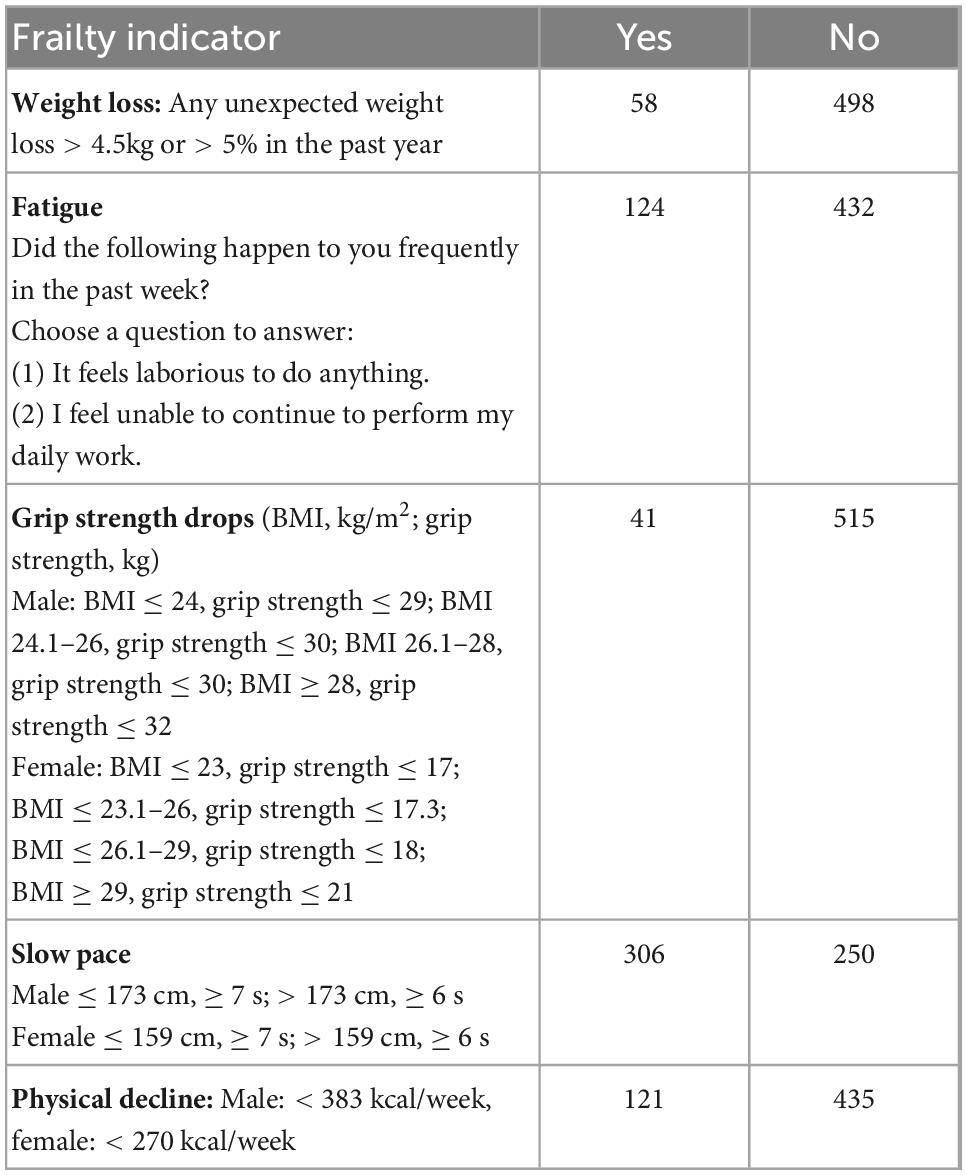
Table 2. The incidence of frailty in hospitalized patients with Schizophrenia (n = 556).
The characteristics of the participants based on SQLS are shown in Table 3. The mean SQLS score of the 556 participants was 83.82 ± 40.30. There were statistically significant differences among inpatients with SZ across the following variables: history of falls during hospitalization, family history of psychosis, polypharmacy, compulsory treatment during hospitalization, self-reported health, Cognitive impairment, Depressive symptoms, and frailty (P < 0.05).
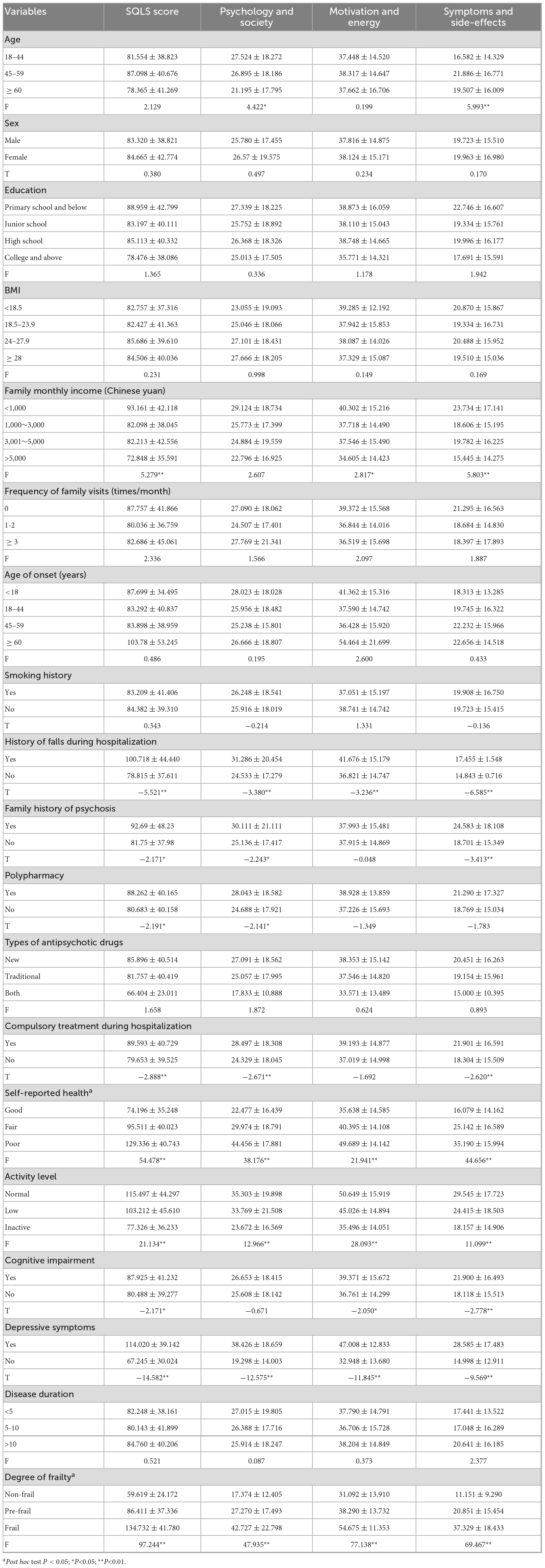
Table 3. Demographic characteristics of the participants and SQLS (n = 556).
The factors influencing frailty were analyzed. Different degrees of frailty were the dependent variable and remaining variables were used as independent variables. Multiple logistic regression analysis revealed that age, BMI, self-rated health status, activity level, cognitive impairment, “motivation and energy,” and “symptoms and side-effects” were associated with frailty. The results are shown in Table 4.
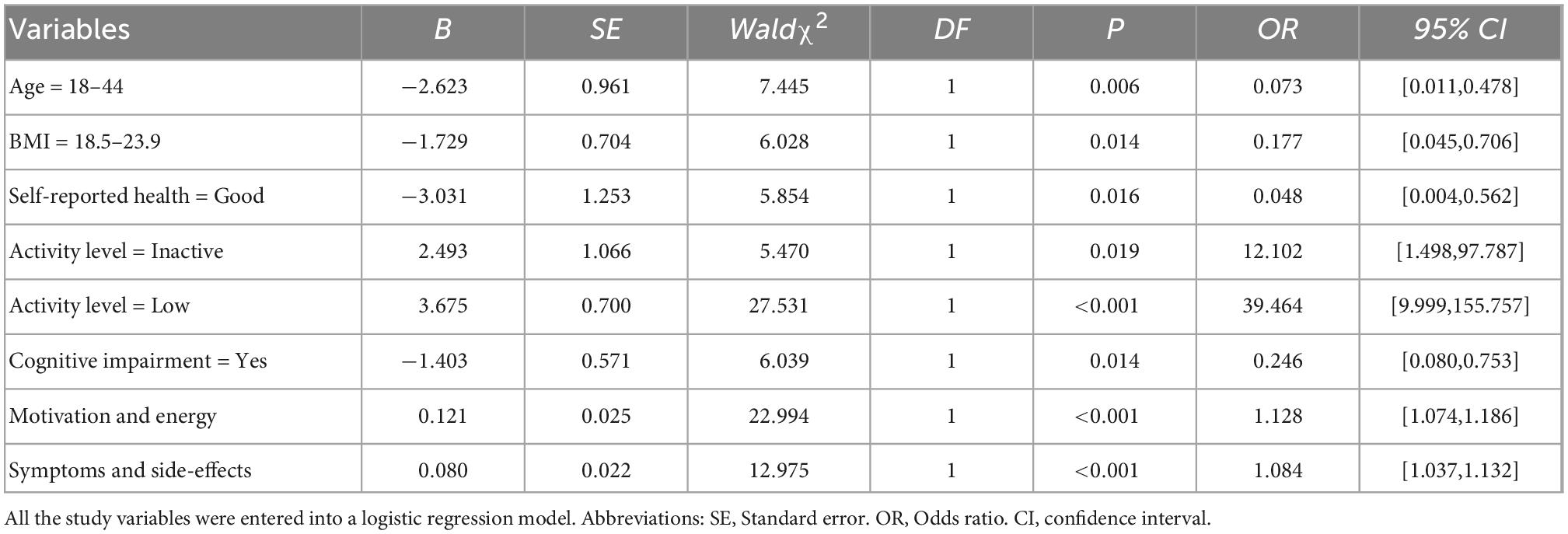
Table 4. Logistic regression analysis of factors related to frailty.
The influencing factors of quality of life were analyzed. The SQLS score was the dependent variable, and remaining variables were used as independent variables. Multiple linear regression analysis showed that age, sex, family monthly income, falls history during hospitalization, self-reported health, activity level, depressive symptoms, frailty were the main influencing factors related to quality of life for patients with SZ. The results are shown in Table 5.
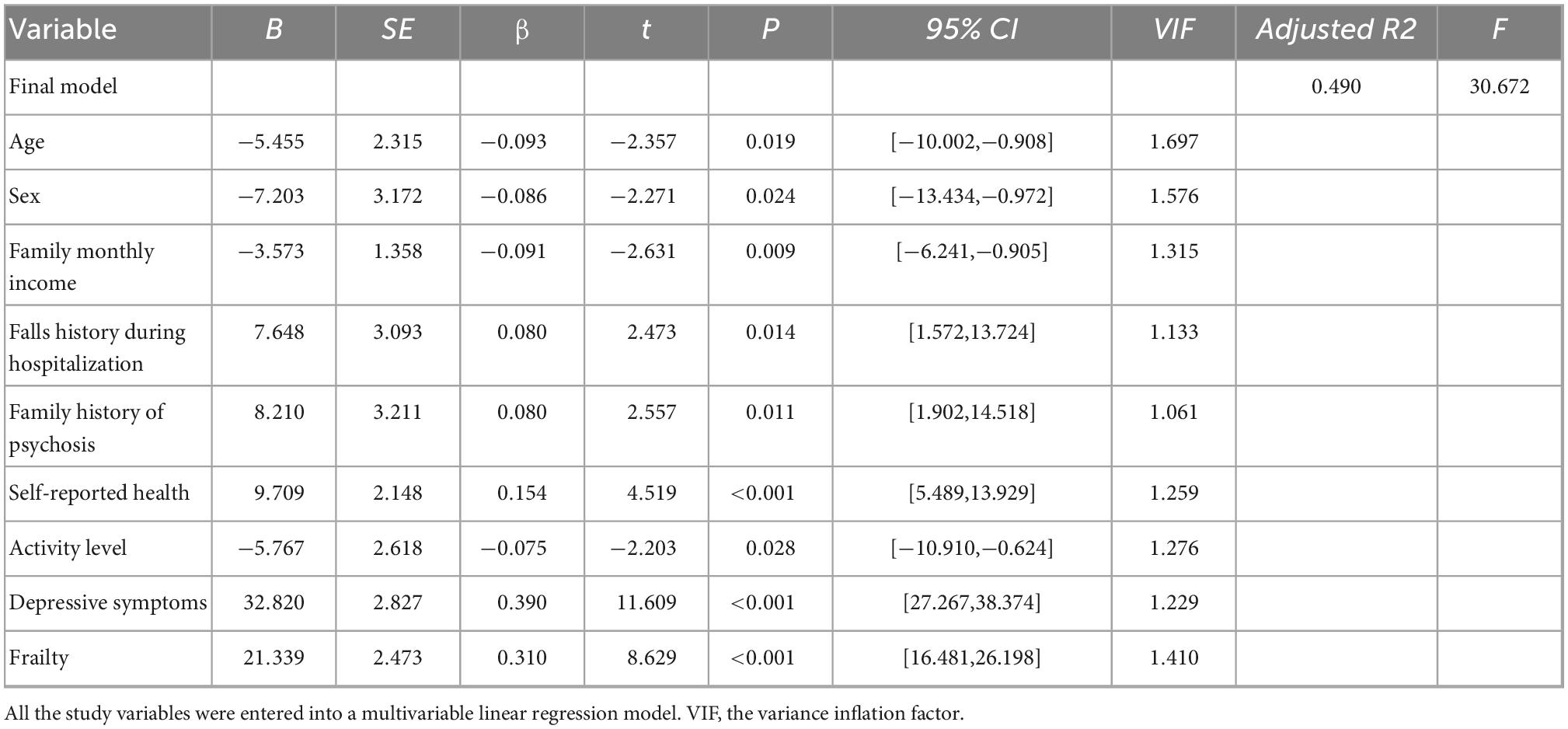
Table 5. Multivariable linear regression analysis of factors related to quality of life.
The frailty and SQLS scores did not follow a normal distribution, and Spearman’ s test was used to analyze the correlation between frailty and quality of life. The results of the correlation analysis showed that frailty was positively correlated with quality of life (R = 0.511, P < 0.001). The higher the frailty score is, the worse the quality of life.
The present study showed a frailty rate slightly lower than that of a study in Taiwan (10.2%) using the same criteria (33). Differences in frailty rates may be related to economic conditions and medical service levels. The survey areas of the present study are in new first-tier cities with relatively developed economies and suitable mental health treatment centers. These cities can provide vocational rehabilitation training with good treatment effects, such as agricultural therapy, garden therapy, and manual training.
Our study showed that age, BMI, motivation and energy, symptoms and side-effects, self-rated health status, activity level and cognitive impairment were the influencing factors related to frailty in inpatients with SZ. Age and BMI have been shown to be a risk factor for frailty (37, 38). “Motivation and energy” and “symptoms and side-effects” were associated with frailty in the present study, indicating that insufficient motivation and energy and severe symptoms and side-effects would increase the risk of frailty. The reason may be that the strong sedative effect causes a lack of subjective motivation and energy, which leads to laziness, limited activity, and frailty (39). Self-reported health is a widely used health criterion to predict and identify frailty (40, 41). The concept of frailty self-perception can explain the relationship between self-rated health status and frailty. Patients with a negative self-perception of frailty are more likely to develop frailty, and a positive self-perception of frailty can delay the development of frailty, and expressive symptoms and cognitive status can mediate the relationship between frailty self-perception and frailty (42). A large cross-sectional study in China (43) showed that poor self-rated health status was a risk factor for frailty in the elderly, similar to the results of the present study. A sedentary lifestyle is a significant risk factor for the progression and morbidity of frailty (44, 45). A study (46) with a large sample showed that the duration of sedentary periods could help judge the existence of frailty and predict the development of frailty. The present study showed that patients with low or moderate activity levels were more prone to frailty than those with higher activity levels, and this is similar to the study (47). Therefore, medical staff should observe the activity of hospitalized patients with SZ, help them formulate activity plans, and urge them to exercise to maintain a healthy lifestyle. Cognitive impairment may be an early marker of physical weakness (48). A cross-sectional study (49) showed that the incidence of frailty was higher in patients with dementia, and the risk of dementia in patients with frailty was also significantly higher. People with cognitive impairment and frailty had a six-fold higher risk of death and a 13-fold higher risk of functional disability than those with only frailty or cognitive impairment. The present study showed that cognitive impairment was a risk factor for frailty, and the risk of frailty in patients with cognitive impairment was significantly higher than their counterparts. This may be because cognitive impairment and frailty share common physiological mechanisms, such as genetic inheritance, chronic inflammation, malnutrition, mitochondrial dysfunction, oxidative stress, hypothalamic–pituitary–adrenal axis dysfunction, endocrine disorders, and energy metabolism imbalances (50). Therefore, it is of great significance to explore the relationship more deeply between cognitive impairment and frailty in patients with SZ and whether reducing or delaying frailty can improve cognition.
We also found that frailty were the influencing factor related to quality of life for patients with SZ. Previous studies have shown that frailty may lead to adverse health outcomes such as falls, fractures, and hospital admissions, increasing disease burden and reducing quality of life (33). Disability-adjusted life years (DALY) is one of the essential measures of disease burden. A large European study (51) showed that frailty was significantly associated with DALY, with frail individuals having significantly higher mean DALYs than non-frail individuals. Therefore, frailty may be related to quality of life. The relationship between frailty and quality of life has long been demonstrated in older populations (52, 53). The frailty phenotypes in the elderly are inversely related to the quality of life (54). The present study showed that frailty score was positively correlated with the SQLS score, indicating that the worse the frailty, the worse the quality of life. Furthermore, poor quality of life may increase frailty in turn (55). Therefore, we speculated that the relationship between frailty and quality of life may be reciprocal. Other studies have not reported a significant cross-sectional relationship between frailty and quality of life in hospitalized patients with SZ, so this relationship requires further research.
The present study has several limitations. First, this was a cross-sectional survey. Although it suggested the suspected risk factors for frailty, it did not consider the temporal and causal relationships between exposures and outcomes. We also could not track the health status in all patients, especially those with poor health statuses, such as those with cognitive impairment, depressive symptoms, a history of falls during hospitalization, polypharmacy, compulsory treatment during hospitalization, and self-reported poor health. These factors require further longitudinal studies. Second, the participants were not randomly selected, so the results cannot be generalized to all patients with SZ in psychiatric hospitals. Finally, we did not notice correlation between PANSS score and grade of frialty and daily equivalent dosage of antipsychotics was not examined.
We found that frailty was prevalent and the influencing factors were complex. Frailty syndrome was positively associated with quality of life in hospitalized patients with SZ. Psychiatric medical staff should pay attention to the quality of life of patients with frailty, screen for early identification of patients with pre-frailty, and formulate targeted prevention and intervention measures to improve quality of life further and delay the onset of frailty.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by The Fourth People’s Hospital of Chengdu Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
All authors contributed to conceiving, researching, and writing of this manuscript and approved the submitted version.
This work was supported by the Sichuan Science and Technology Program (grant no. 2018JY0306).
We thank all the participants in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Jauhar S, Johnstone M, McKenna P. Schizophrenia. Lancet. (2022) 399:473–86. doi: 10.1016/S0140-6736(21)01730-X
2. Han X, Jiang F, Needleman J, Guo M, Chen Y, Zhou H, et al. A sequence analysis of hospitalization patterns and service utilization in patients with major psychiatric disorders in China. BMC Psychiatry. (2021) 21:245. doi: 10.1186/s12888-021-03251-w
3. Fried L, Tangen C, Walston J, Newman A, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. (2001) 56:M146–56. doi: 10.1093/gerona/56.3.M146
4. Hoogendijk E, Afilalo J, Ensrud K, Kowal P, Onder G, Fried L. Frailty: implications for clinical practice and public health. Lancet. (2019) 394:1365–75. doi: 10.1016/S0140-6736(19)31786-6
5. Spiers G, Kunonga T, Hall A, Beyer F, Boulton E, Parker S, et al. Measuring frailty in younger populations: a rapid review of evidence. BMJ Open. (2021) 11:e47051. doi: 10.1136/bmjopen-2020-047051
6. Stolz E, Rásky É, Jagsch C. Frailty index predicts geriatric psychiatry inpatient mortality: a case-control study. Psychogeriatrics. (2020) 20:469–72. doi: 10.1111/psyg.12535
7. Önen N, Patel P, Baker J, Conley L, Brooks J, Bush T, et al. Frailty and pre-frailty in a contemporary cohort of HIV-infected adults. J Frailty Aging. (2014) 3:158–65. doi: 10.14283/jfa.2014.18
8. Onen N, Shacham E, Stamm K, Turner Overton E. Sexual behaviors and results of bacterial sexually transmitted infections testing among frail HIV-infected individuals. J Int Assoc Physicians AIDS Care. (2010) 9:30–3. doi: 10.1177/1545109709356946
9. Prince C, Noren Hooten N, Mode N, Zhang Y, Ejiogu N, Becker K, et al. Frailty in middle age is associated with frailty status and race-specific changes to the transcriptome. Aging. (2019) 11:5518–34. doi: 10.18632/aging.102135
10. Rochira V, Diazzi C, Santi D, Brigante G, Ansaloni A, Decaroli M, et al. Low testosterone is associated with poor health status in men with human immunodeficiency virus infection: a retrospective study. Andrology. (2015) 3:298–308. doi: 10.1111/andr.310
11. Vatanen A, Hou M, Huang T, Söder O, Jahnukainen T, Kurimo M, et al. Clinical and biological markers of premature aging after autologous SCT in childhood cancer. Bone Marrow Transplant. (2017) 52:600–5. doi: 10.1038/bmt.2016.334
12. Wilson C, Chemaitilly W, Jones K, Kaste S, Srivastava D, Ojha R, et al. Modifiable factors associated with aging phenotypes among adult survivors of childhood acute lymphoblastic leukemia. J Clin Oncol. (2016) 34:2509–15. doi: 10.1200/JCO.2015.64.9525
13. Kirkpatrick B, Messias E, Harvey P, Fernandez-Egea E, Bowie C. Is SZ a syndrome of accelerated aging? Schizophr Bull. (2008) 34:1024–32. doi: 10.1093/schbul/sbm140
14. Kirkpatrick B, Kennedy B. Accelerated aging in SZ and related disorders: future research. Schizophr Res. (2018) 196:4–8. doi: 10.1016/j.schres.2017.06.034
15. Jeste D, Wolkowitz O, Palmer B. Divergent trajectories of physical, cognitive, and psychosocial aging in SZ. Schizophr Bull. (2011) 37:451–5. doi: 10.1093/schbul/sbr026
16. Koutsouleris N, Davatzikos C, Borgwardt S, Gaser C, Bottlender R, Frodl T, et al. Accelerated brain aging in SZ and beyond: a neuroanatomical marker of psychiatric disorders. Schizophr Bull. (2014) 40:1140–53. doi: 10.1093/schbul/sbt142
17. Shivakumar V, Kalmady S, Venkatasubramanian G, Ravi V, Gangadhar B. Do SZ patients age early? Asian J Psychiatr. (2014) 10:3–9. doi: 10.1016/j.ajp.2014.02.007
18. Kota L, Purushottam M, Moily N, Jain S. Shortened telomere in unremitted SZ. Psychiatry Clin Neurosci. (2015) 69:292–7. doi: 10.1111/pcn.12260
19. Lindqvist D, Epel E, Mellon S, Penninx B, Révész D, Verhoeven J, et al. Psychiatric disorders and leukocyte telomere length: underlying mechanisms linking mental illness with cellular aging. Neurosci Biobehav Rev. (2015) 55:333–64. doi: 10.1016/j.neubiorev.2015.05.007
20. Lehman A. The well-being of chronic mental patients. Arch Gen Psychiatry. (1983) 40:369–73. doi: 10.1001/archpsyc.1983.01790040023003
21. Howes O, Murray RM. SZ: an integrated sociodevelopmental-cognitive model. Lancet. (2014) 383:1677–87. doi: 10.1016/S0140-6736(13)62036-X
22. Bullinger M, Kuhn J, Leopold K, Janetzky W, Wietfeld R. Lebensqualität als Zielkriterium in der Schizophrenietherapie. [Quality of life as a target criterion in SZ therapy]. Fortschr Neurol Psychiatr. (2019) 87:348–56. doi: 10.1055/a-0646-3951
23. Stubbs B, Gaughran F, Mitchell A, De Hert M, Farmer R, Soundy A, et al. SZ and the risk of fractures: a systematic review and comparative meta-analysis. Gen Hosp Psychiatry. (2015) 37:126–33. doi: 10.1016/j.genhosppsych.2015.01.004
24. Wang S, Wang J, Chang J, Wu B, Chern J, Wang T. Frailty affects employment outcomes in patients with SZ in noncompetitive employment: a 4-year longitudinal study. Schizophr Res. (2020) 222:375–81. doi: 10.1016/j.schres.2020.04.026
25. Su M, Yao N, Shang M, Shen Y, Qin T, Wang J, et al. Frailty and its association with health-related quality of life among older cancer patients: an evidence-based study from China. Health Qual Life Outcomes. (2022) 20:124. doi: 10.1186/s12955-022-02032-7
26. Veronese N, Noale M, Cella A, Custodero C, Smith L, Barbagelata M, et al. Multidimensional frailty and quality of life: data from the english longitudinal study of ageing. Qual Life Res. (2022) 31:2985–93. doi: 10.1007/s11136-022-03152-9
27. Hamaya T, Hatakeyama S, Momota M, Narita T, Iwamura H, Kojima Y, et al. Association between the baseline frailty and quality of life in patients with prostate cancer (FRAQ-PC study). Int J Clin Oncol. (2021) 26:199–206. doi: 10.1007/s10147-020-01798-4
28. World Health Organization [WHO]. The ICD-10 classification of mental and behavioural disorders: Diagnostic criteria for research. Genève, CH: World Health Organization (1993).
29. Kay S, Fiszbein A, Opler L. The positive and negative syndrome scale (PANSS) for SZ. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
30. Folstein M, Folstein S, McHugh P. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
31. Zung W, Richards C, Short M. Self-rating depression scale in an outpatient clinic. Further validation of the SDS. Arch Gen Psychiatry. (1965) 13:508–15. doi: 10.1001/archpsyc.1965.01730060026004
32. Wilkinson G, Hesdon B, Wild D, Cookson R, Farina C, Sharma V, et al. Self-report quality of life measure for people with SZ: the SQLS. Br J Psychiatry. (2000) 177:42–6. doi: 10.1192/bjp.177.1.42
33. Tsai M, Lee S, Chen H, Wu B. Association between frailty and its individual components with the risk of falls in patients with SZ spectrum disorders. Schizophr Res. (2018) 197:138–43. doi: 10.1016/j.schres.2018.01.023
34. Ong H, Subramaniam M, Abdin E, Wang P, Vaingankar J, Lee S, et al. Performance of mini-mental state examination (MMSE) in long-stay patients with SZ or schizoaffective disorders in a psychiatric institute. Psychiatry Res. (2016) 241:256–62. doi: 10.1016/j.psychres.2016.04.116
35. Thurber S, Snow M, Honts C. The zung self-rating depression scale: convergent validity and diagnostic discrimination. Assessment. (2002) 9:401–5. doi: 10.1177/1073191102238471
36. Luo H, Luo N, Wang Y. Reliability and validity of SZ quality of life scale. Chinese Mental Health J. (2003) 17:172–4.
37. Wang X, Hu J, Wu D. Risk factors for frailty in older adults. Medicine. (2022) 101:e30169. doi: 10.1097/MD.0000000000030169
38. Wang C, Fang X, Tang Z, Hua Y, Zhang Z, Gu X, et al. A frailty index based on routine laboratory data predicts increased risk of mortality in Chinese community-dwelling adults aged over 55 years: a five-year prospective study. BMC Geriatr. (2022) 22:679. doi: 10.1186/s12877-022-03374-z
39. Muhlack D, Hoppe L, Saum K, Haefeli W, Brenner H, Schöttker B. Investigation of a possible association of potentially inappropriate medication for older adults and frailty in a prospective cohort study from Germany. Age Ageing. (2019) 49:20–5. doi: 10.1093/ageing/afz127
40. Chu W, Ho H, Yeh C, Hsiao Y, Hsu P, Lee S, et al. Self-rated health trajectory and frailty among community-dwelling older adults: evidence from the taiwan longitudinal study on aging (TLSA). BMJ Open. (2021) 11:e49795. doi: 10.1136/bmjopen-2021-049795
41. Giri S, Mir N, Al-Obaidi M, Clark D, Kenzik K, McDonald A, et al. Use of single-item self-rated health measure to identify frailty and geriatric assessment-identified impairments among older adults with cancer. Oncologist. (2022) 27:e45–52. doi: 10.1093/oncolo/oyab020
42. Yuan K, Luo Y, Sun J, Chang H, Hu H, Zhao B. Depression and cognition mediate the effect of self-perceptions of aging over frailty among older adults living in the community in China. Front Psychol. (2022) 13:830667. doi: 10.3389/fpsyg.2022.830667
43. Liu W, Puts M, Jiang F, Zhou C, Tang S, Chen S. Physical frailty and its associated factors among elderly nursing home residents in China. BMC Geriatr. (2020) 20:294. doi: 10.1186/s12877-020-01695-5
44. Niederstrasse N, Rogers N, Bandelow S. Determinants of frailty development and progression using a multidimensional frailty index: evidence from the english longitudinal study of ageing. PLoS One. (2019) 14:e223799. doi: 10.1371/journal.pone.0223799
45. da Silva V, Tribess S, Meneguci J, Sasaki J, Garcia-Meneguci C, Carneiro J, et al. Association between frailty and the combination of physical activity level and sedentary behavior in older adults. BMC Public Health. (2019) 19:709. doi: 10.1186/s12889-019-7062-0
46. Virtuoso J, Roza L, Tribess S, Meneguci J, Mendes E, Pegorari M, et al. Time spent sitting is associated with changes in biomarkers of frailty in hospitalized older adults: a cross sectional study. Front Physiol. (2017) 8:505. doi: 10.3389/fphys.2017.00505
47. Fung T, Lee I, Struijk E, Rodriguez Artalejo F, Willett W, Lopez-Garcia E. Physical activity and risk of frailty in u.s. women age 60 and older. Med Sci Sports Exerc. (2022): [Epub ahead of print]. doi: 10.1249/MSS.0000000000003046
48. Raji M, Al Snih S, Ostir G, Markides K, Ottenbacher K. Cognitive status and future risk of frailty in older Mexican Americans. J Gerontol A Biol Sci Med Sci. (2010) 65:1228–34. doi: 10.1093/gerona/glq121
49. Wegelius A, Tuulio-Henriksson A, Pankakoski M, Haukka J, Lehto U, Paunio T, et al. An association between high birth weight and SZ in a Finnish SZ family study sample. Psychiatry Res. (2011) 190:181–6. doi: 10.1016/j.psychres.2011.05.035
50. Howrey B, Al Snih S, Middleton J, Ottenbacher K. Trajectories of frailty and cognitive decline among older Mexican Americans. J Gerontol A Biol Sci Med Sci. (2020) 75:1551–7. doi: 10.1093/gerona/glz295
51. O’Donovan M, Sezgin D, Liew A, O’Caoimh R. Burden of disease, disability-adjusted life years and frailty prevalence. QJM. (2019) 112:261–7. doi: 10.1093/qjmed/hcy291
52. Zhang X, Tan S, Franse C, Alhambra-Borrás T, Durá-Ferrandis E, Bilajac L, et al. Association between physical, psychological and social frailty and health-related quality of life among older people. Eur J Public Health. (2019) 29:936–42. doi: 10.1093/eurpub/ckz099
53. Siriwardhana D, Weerasinghe M, Rait G, Scholes S, Walters K. The association between frailty and quality of life among rural community-dwelling older adults in Kegalle district of Sri Lanka: a cross-sectional study. Qual Life Res. (2019) 28:2057–68. doi: 10.1007/s11136-019-02137-5
54. Vejux J, le Bruchec S, Bernat V, Beauvais C, Beauvais N, Berrut G. [Fragility and quality of life, the benefits of physical activity for the elderly]. French Geriatr Psychol Neuropsychiatr Vieil. (2021) 19:127–36. doi: 10.1684/pnv.2021.0924
Keywords: frailty, influencing factors, quality of life, correlation research, Schizophrenia
Citation: Yang C, Hou X, Ma X and Wu D (2023) Frailty among inpatients with Schizophrenia: Status, influencing factors, and their correlation with quality of life. Front. Psychiatry 13:1067260. doi: 10.3389/fpsyt.2022.1067260
Received: 11 October 2022; Accepted: 12 December 2022;
Published: 04 January 2023.
Edited by:
Wing Chung Chang, The University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Edwin Lee, The University of Hong Kong, Hong Kong SAR, ChinaCopyright © 2023 Yang, Hou, Ma and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dongmei Wu, ✉ d3Vkb25nbWVpXzIwMDFAMTYzLmNvbQ==; orcid.org/0000-0001-9830-0527
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.