 Yali Yi
Yali Yi Yuanyan Hu
Yuanyan Hu Mengxin Cui3
Mengxin Cui3 Jibing Wang
Jibing Wang- 1School of Mathematics and Statistics, Southwest University, Chongqing, China
- 2School of Mathematics and Statistics, Yulin Normal University, Yulin, China
- 3Qingdao Mental Health Center, Qingdao University, Qingdao, China
- 4Department of Sports, Northwestern Polytechnical University, Xi’an, China
- 5International College of Football, Tongji University, Shanghai, China
Virtual reality (VR) interventions are increasingly being used in rehabilitating and treating patients with neurological disorders. This study aimed to explore the effects of VR exercise interventions for patients with Alzheimer’s disease (AD). A systematic review of the published literature on randomized controlled trials of VR technology applied to patients with AD was conducted using the preferred reporting entry for systematic reviews and Meta-analysis guidelines. Descriptive analyses were performed to assess the quality of the studies in terms of the characteristics of the included studies, samples, diagnoses, types of VR technologies, subjective and objective levels of immersion, and quality of studies. Eight studies were included, including a pooled sample of 362 patients with AD. A systematic review showed that most studies focused on patients with AD’s cognitive and physical functions. The main finding was that VR interventions could help improve cognitive and physical balance in patients with AD. However, future studies should emphasize design and use well-accepted assessment tools to validate the effects of VR interventions further.
Introduction
Alzheimer’s disease (AD) is a progressive brain disease and is currently one of the most common causes of dementia worldwide (1). The incidence of AD increases after age 65 and is more common in women (2, 3). Numerous risk factors influence the development of AD, including age, gender, education, socioeconomic status, smoking, alcohol consumption, obesity, physical activity, hypertension, diabetes, hypercholesterolemia, head trauma, sleep disorders, and depression (4). Currently, Food and Drug Administration-approved AD therapies provide symptom relief benefits for some individuals but neither prevent nor improve the disease (5). Once clinicians make a clinical diagnosis of AD in older adults, adults often want to know what they can do to slow cognitive decline with non-pharmacologic treatments (6). Additionally, people also want to know what they can do to delay the onset or reduce their risk of developing AD (7).
Virtual reality (VR) technology has been widely used in rehabilitating older adults with medical conditions to enhance their ability to perform activities of daily living in the last years (8, 9). VR technology has also been reported to be used for people with mild cognitive impairment (MCI) (10), people at high risk of cognitive decline (11); memory rehabilitation patients with noncommunicable diseases (NCDs) (12); patients with NCDs due to traumatic brain injury (13), stroke patients (14, 15), and patients with severe NCDs due to AD (16, 17). VR is an emerging technology which creates a three-dimensional environments digitally, allows people to interact, provides sensory input, and tracks change (18). Several commercial VR gaming systems, such as Dance Revise, Microsoft Xbox Kinect, Nintendo Switch, and Wii Sports provide simulated and realistic exercise experiences (19). Real-time feedback, movement reflection, and rewards in a three-dimensional (3D) world for older patients are provided to encourage motivation to adhere to exercise and willingness to continue exercising (20).
Virtual reality exercise training has become a popular method of treating individuals with mental illness. VR environments add additional spatial features to enhance the cognitive benefits of exercise. Several studies have also shown that VR may improve psychological functioning in patients with cognitive impairment (21, 22). In the treatment of depressive symptoms, older adults facing visual and auditory stimuli in VR may experience an increase in energy, enjoyment of exercise, tranquility, and a decrease in negative feelings. Also, VR exercise supports older adults’ decision-making, emotional regulation, and interaction skills to promote psychological, emotional, and social benefits (23, 24).
Virtual reality technology is an innovative approach to rehabilitation that minimizes the adverse effects of NCDs on individuals, families, and society and has been used in healthcare and rehabilitation (25–28). Current research findings on VA technology being used to improve cognitive function are inconsistent (29). The effects of VR technology on cognitive function in MCI patients were summarized by Wu et al. (10) but they did not offer sufficient data. A scoping review on VR therapies’ impact on people with MCI or dementia was unable to clarify how VR affects people with MCI (30). Several recent original studies of VR interventions in cognitive function recently supplemented the field with new evidence (31–34). Another typical intervention population for VR cognitive training includes people with MCI (9, 35). However, current evidence is less reported on interventions for individuals with AD, and a comprehensive understanding of the effects of VR motor interventions on individuals with AD is needed (36). That is, the overall description of the use of VR in AD disease rehabilitation remains uncertain (21). This review study aims to analyze experimental studies of VR and synthesize its effects on intervention outcomes in AD patients, including cognitive function, daily activities, and physical functioning.
Methods
Data sources and search strategies
A systematic review was conducted using different combinations of keywords (“virtual reality,” “video games,” “interactive games,” and “VR”) and (“Alzheimer,” “Alzheimer’s disease,” and “AD”) with these terms in the databases Web of Science and PubMed/MEDLINE from inception to December 2021. Two reviewers and the corresponding author collaborated to develop the search strategy, and the two reviewers independently completed the search and cross-validated it. Endnote X7 software was used for literature management.
Study selection
The inclusion criteria for the study literature were (1) VR interventions for adults with AD; (2) Measurement of cognitive indicators or physical function indicators pre- and post-VR interventions; (3) Interventions that included the use of an immersive or non-immersive VR technology targeting cognitive or physical function in patients with AD; (4) A controlled experimental study, and (5) Studies are provided in English. We excluded studies based on the following characteristics: (1) Case studies; (2) Feasibility studies; (3) non-AD patient-focused studies; (4) Study protocols and reviews; (5) Expert letters, editorials, notes, and book chapters; and (6) Conference abstracts and papers.
Data extraction
First, titles and abstracts were screened using eligibility criteria by two independent reviewers. Studies that met the criteria for inclusion or were uncertain were kept for full-text scanning. Disagreements on unclear studies were resolved in consultation with the corresponding authors. Second, two independent reviewers assembled the following details from each study: publication details (including author, year, and title), study design (objectives, methods, and setting), participants (including sample size, mean age, and gender), VR intervention (including name of VR, technical details, subjective and objective immersion levels, number and frequency of VR workouts, duration of each VR workout, and total mean duration of VR), outcome measures, results, user acceptance, adverse effects, and summary of intervention effects.
Levels of virtual reality immersion
The term “immersion” refers to a method for describing how much human participants’ senses may be fooled into believing something is genuine by computer displays. Generally, the level of the immersion technology is evaluated using five criteria: (1) Inclusiveness indicates the extent to which physical reality is rejected; (2) Extensiveness indicates the range of sensory modalities to which it is adapted; (3) Surrounding shows how wide-ranging this VA is as opposed to being restricted to a narrow field; (4) Vivid conveys fidelity, the resolution, and a range of energies (e.g., visual and color resolution) of the simulation within a given channel. The degree of vividness is related to the richness of the display, the content of the information, the resolution, and the quality. These aspects of immersion are related to the display of information; and (5) Matching requires a match between the participant’s proprioceptive feedback about body movement and the information generated on display (37, 38).
Quality assessment
Two reviewers (YY and MC) independently assessed the quality of the inclusion literature using the PEDro scale (38). The scale consists of 11 items, with the first item not scored and a maximum score of 10. Studies scoring ≥6 was considered high quality, while those scoring below six were considered low quality (39). Two reviewers resolved disagreements in scoring in consultation with the corresponding authors (YH and JL).
Statistical analysis
The literature was critically analyzed based on (1) study characteristics, sample, type of VR technology, and intervention duration and frequency; (2) VR immersion level; and (3) quality assessment of the study and risk of bias. The applicability of the meta-analysis was considered concerning the available information.
Results
Study selection
Eight of the 2,023 studies were included in the systematic review, and the total sample of AD patients participating in these studies was 362 (Figure 1). A meta-analysis is not feasible considering the variability of the study results.
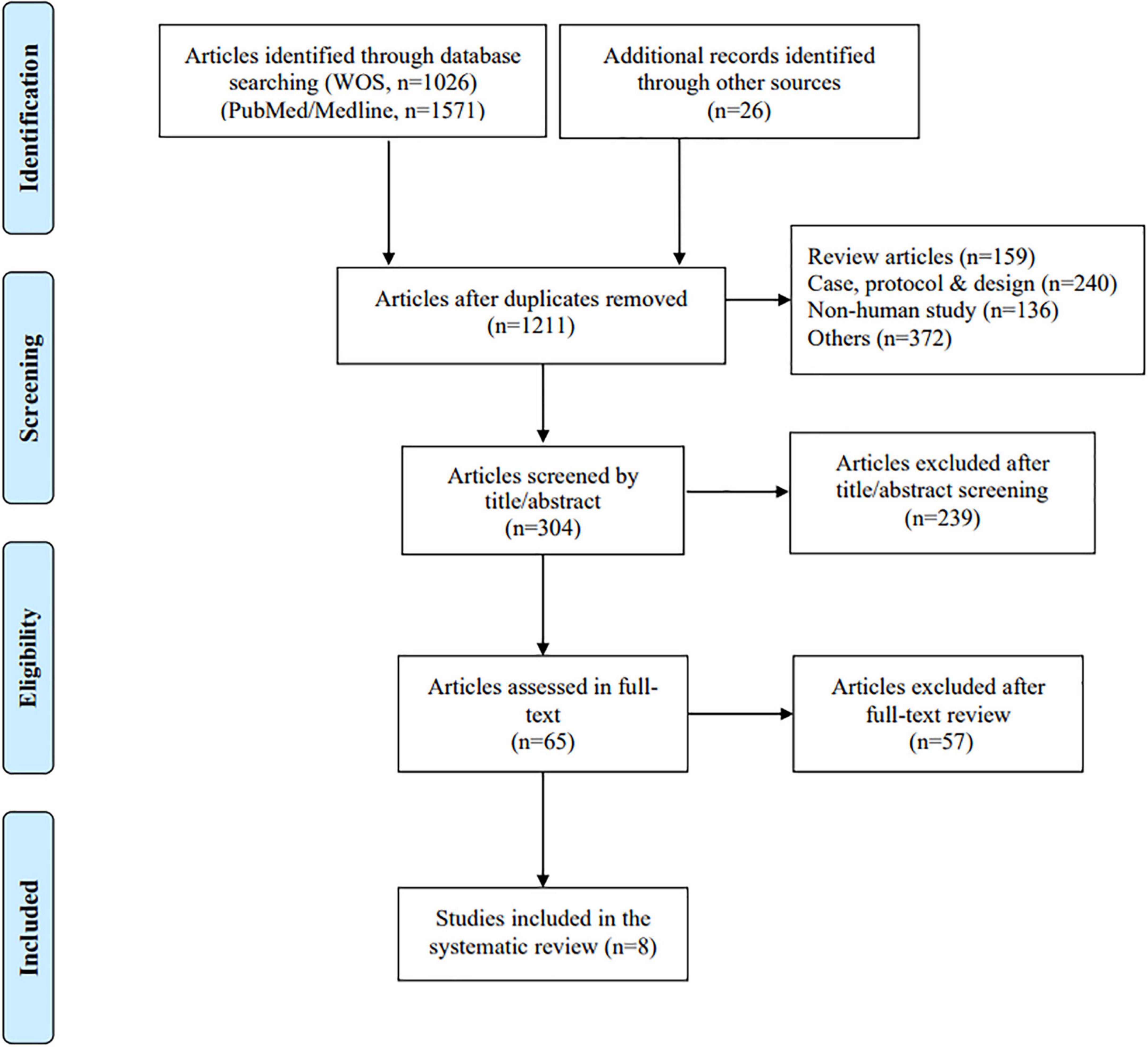
Figure 1. PRISMA flowchart of included and excluded studies.
Study characteristics
Table 1 lists each study sample’s characteristics, study design, intervention type, measurement outcomes, and intervention effects. The study sample was 59.1% female, and the experimental design was a non-randomized controlled trial in only one study (29). The type of exercise intervention was a combination of VR and cognitive or motor exercise; the outcome measures were mainly cognitive, memory, and executive function, with some studies involving physical function. All included studies showed positive changes, with AD patients showing improvements or enhancements in cognitive function, executive function, memory, and body balance. Overall, the different VR interventions showed positive outcomes or feasibility of implementing the intervention.
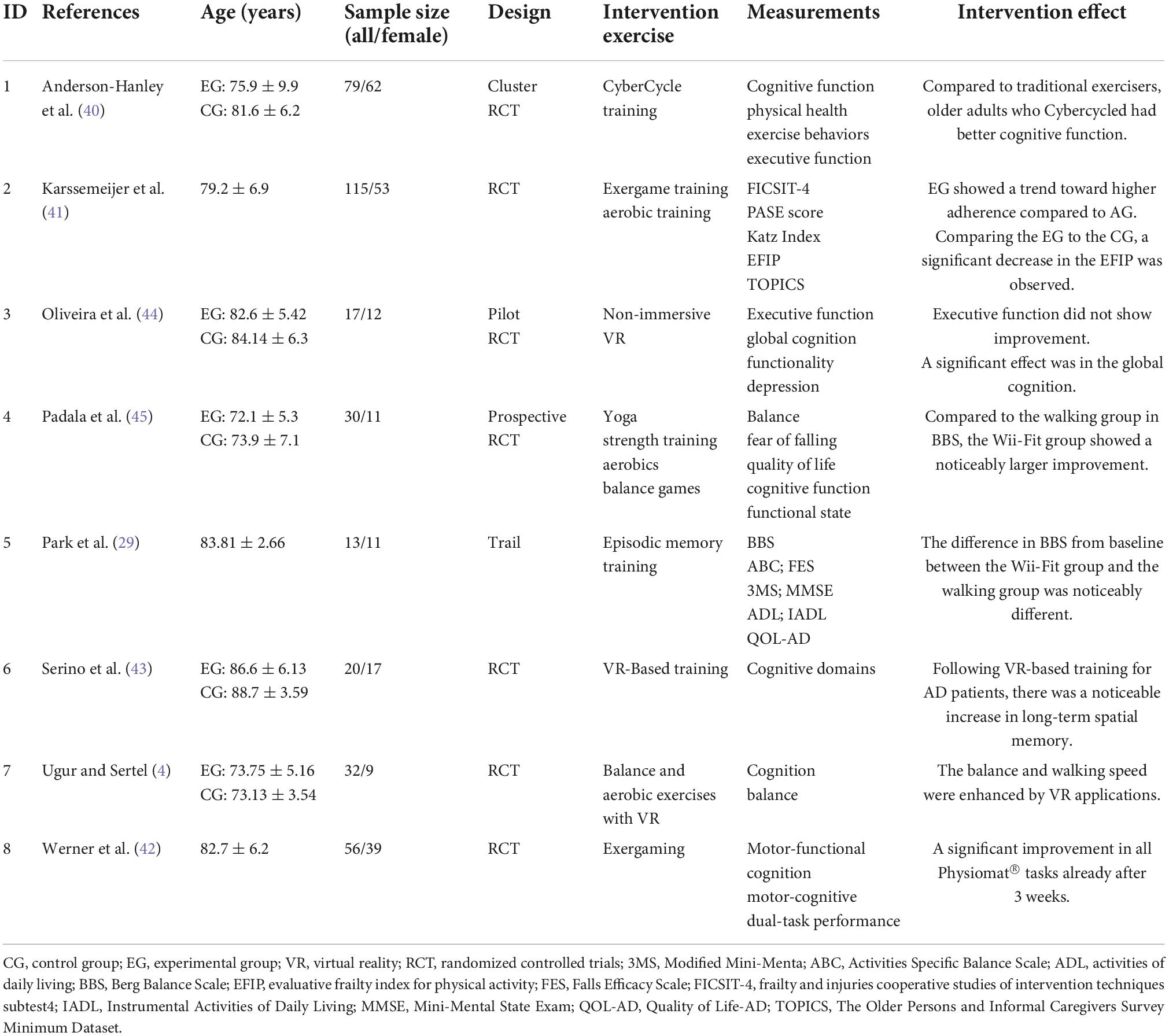
Table 1. Characteristics of the inclusion studies.
Virtual reality technology and levels of immersion
Table 2 shows the titles of the different VR applications, VR immersion levels, VR usage settings, VR user experiences, and their adverse feedback reported in studies. Regarding the description of VR immersion levels, as provided by the studies, 50% of the technologies were described as semi-immersive (4, 40–42), 25% as immersive (29, 43), and 25% as non-immersive (44, 45). The mean duration of a single intervention was 30 min (SD = 12.8, range = 10–50) in the eight studies; the mean number of interventions was 23 (SD = 13.2, range = 10–40); and the mean duration of total intervention activities was 758 min (SD = 628.7, range = 200–1,800). Interestingly, no adverse events were reported in 62.5% of the included studies (4, 29, 43, 44). Of the adverse events reported, one study had four adverse events, but they were not considered relevant to the study (41); another study reported in detail four participants dropping out midway through the intervention due to severe medical time and seven participants dropping out after the intervention due to lack of motivation (n = 4), the injury falls (n = 2), and death (n = 1) (42). One additional study provided 13 adverse events in an attachment, including motor impairment, nausea and disorientation, neck pain, and dizziness (39).
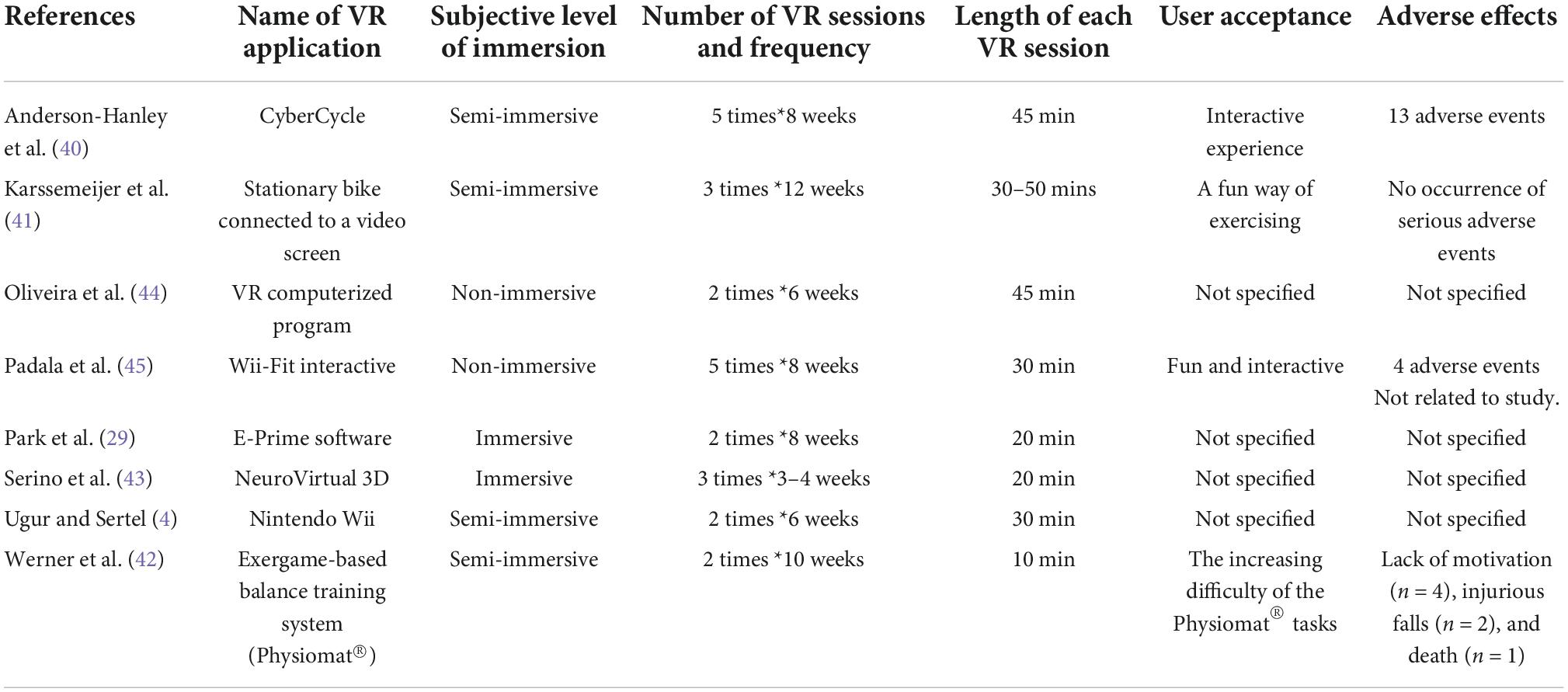
Table 2. Virtual reality (VR) levels of immersion, characteristics of the VR programs, and user experience.
Table 3 shows the objective level of immersion based on the FIVE criteria developed by Slater et al. (37). Many studies (62.5%) met the criteria for moderate immersion (40, 42–45), with the remainder being 12.5% high immersion (4), 12.5% low immersion experiences (41), and 12.5% information unavailable for immersion (29).
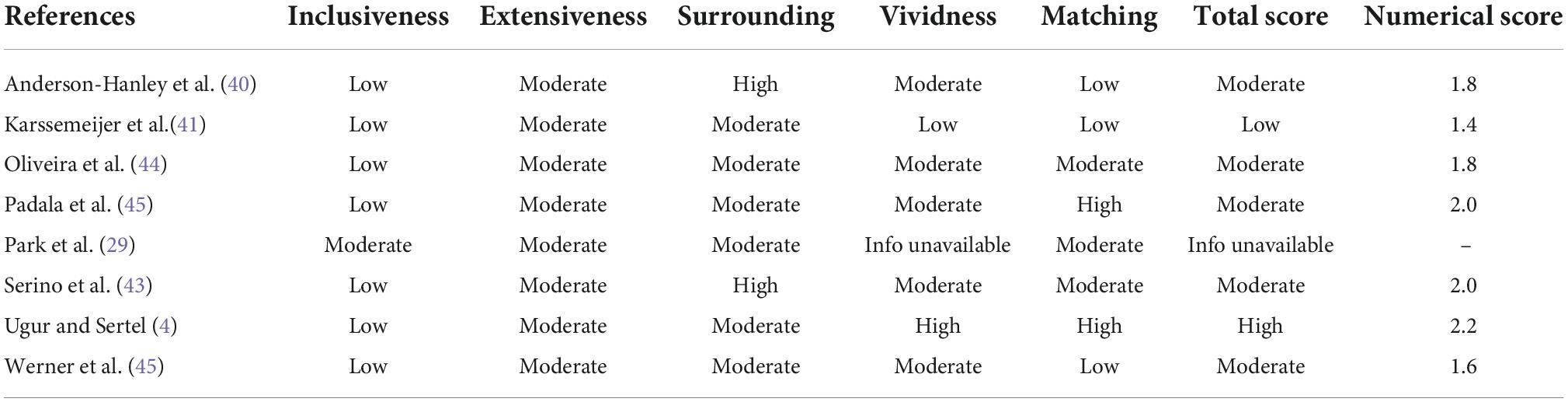
Table 3. Immersion levels of virtual reality (VR) technologies.
Quality assessment
The PEDro scale was used to assess the methodological quality of the eight studies included in the systematic review. The PEDro score was below six in only one study (43) and ≥6 in the other seven studies, indicating good quality of the included studies. However, we also discovered fewer studies in the PEDro quality evaluation on participant and therapist blinding. Only three studies blindfolded the participants, and only one research blinded the therapists. Details of the raw records are shown in Table 4.
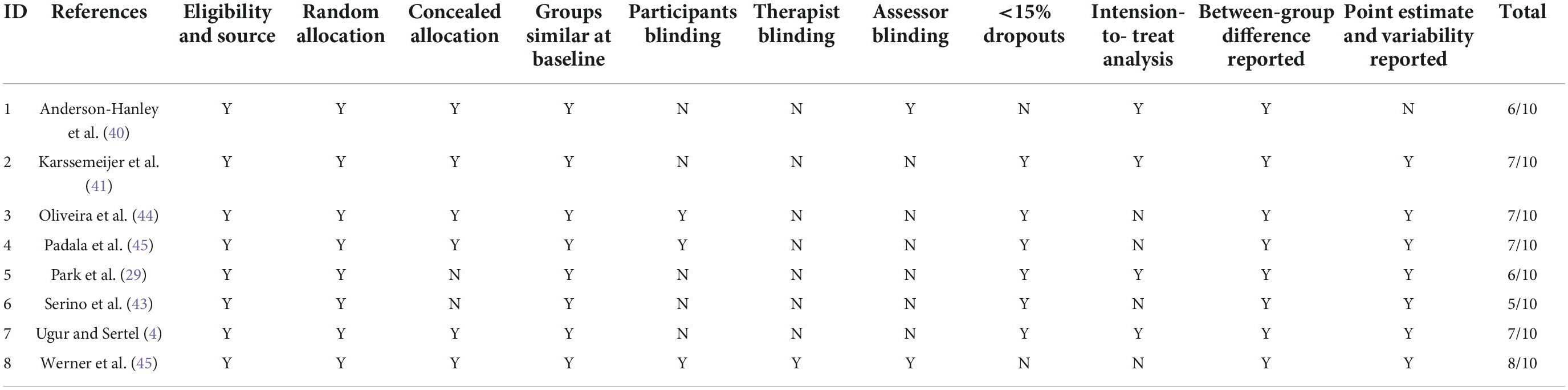
Table 4. Studies quality assessment.
Discussion
The present study aimed to investigate the impact of VA on the effectiveness of interventions for patients with AD. Descriptive analyses were conducted to assess the quality of the study characteristics, study sample, diagnosis, type of VA technology, level of subjective and objective immersion, and quality assessment of eight studies with a total sample of 362 AD patients. Our two independent evaluators extracted information separately and simultaneously to improve the accuracy of the screening process for inclusion in the studies.
The main finding was that VR interventions for patients with AD showed improvements in cognition, memory, executive function, and body balance at various levels. VR applied to interventions for patients with AD had significant effects. This systematic review’s findings supports the use of VR therapies for cognitive rehabilitation and physical function enhancement.
The subjective level of immersion reported for most VR technologies was described as semi-immersive. The average number of VR exercises was 23, with each lasting approximately 30 min, 2–3 times per week. Thus, the frequency and effectiveness of VR interventions appear to be acceptable as part of an innovative initiative. Most studies did not report adverse events. The adverse events addressed in some of the studies were also not caused by the studies. Only in one study were two falls and one death reported in detail at the end of the participant’s intervention (41). Thus, future use of VR interventions for patients with AD will need to be monitored for adverse effects, but these effects do not constitute a reason to exclude the use of VR.
Most studies met the objective criteria for moderate immersion. It is common knowledge that greater levels of immersion may improve the user experience and significantly impact the sensation of presence. However, in VR applications for AD patients, promoting a high level of immersion that corresponds to the experience of feeling “present” in the real world is critical to the patient’s response to the intervention. In the available literature, we cannot yet determine whether fully immersive VR technologies are better than moderate or low immersion VR technologies (46–48).
Although the overall quality of the study was good, adverse effects must be kept ensuring that study participants are blinded to the interventions they receive. This will ensure that evidence is presented favorably in the analyses that lead to the main findings (49).
Conclusion
We systematically reviewed the literature on the use of VR technology for rehabilitating cognition and its physical function in patients with AD. VR interventions help improve cognition, memory, executive function, and physical balance. VR interventions for the rehabilitation of AD patients are an innovative approach. Despite the possibility that this systematic review does not lend itself to a meta-analysis, the findings indicate that VR therapies are useful and can potentially improve patients with AD’s physical function and cognitive rehabilitation.
Based on the findings of this review, we recommend the following for future research. (1) Studies focus on the experimental design of VR interventions, especially the design of randomized controlled trials blinded to the method. (2) Compare different levels of immersion, explore the differences between full immersion and moderate and low immersion, and develop optimal immersion application strategies. (3) Systematically assess user perceptions and adverse effects. (4) Use widely used outcome metrics to evaluate cross-cultural effectiveness. (5) Use well-promoted VR programs to promote comparability of intervention effects.
Data availability statement
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
YY and MC: data collection. YY, YH, and CW: data analysis, conception, and design. YY, YH, and JW: research design, writing the manuscript, and revision. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the Humanities and Social Sciences Project of the Ministry of Education of China (No.20XJC880002).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fereshetian S, Agranat JS, Siegel N, Ness S, Stein TD, Subramanian ML. Protein and imaging biomarkers in the eye for early detection of Alzheimer’s disease. J Alzheimers Dis Rep. (2021) 1:375–87. doi: 10.3233/ADR-210283
2. Niu H, Álvarez-Álvarez I, Guillén-Grima F, Aguinaga-Ontoso I. Prevalencia e incidencia de la enfermedad de Alzheimer en Europa: metaanálisis. Neurología. (2017) 8:523–32. doi: 10.1016/j.nrl.2016.02.016
3. Wilson RS, Segawa E, Boyle PA, Anagnos SE, Hizel LP, Bennett DA. The natural history of cognitive decline in Alzheimer’s disease. Psychol Aging. (2012) 4:1008. doi: 10.1037/a0029857
4. Uğur F, Sertel M. The effect of virtual reality applications on balance and gait speed in individuals with Alzheimer dementia: a pilot study. Top Geriatr Rehabil. (2020) 4:221–9. doi: 10.1097/TGR.0000000000000285
5. Gilbert JA, Blaser MJ, Caporaso JG, Jansson JK, Lynch SV, Knight R. Current understanding of the human microbiome. Nat Med. (2018) 4:392–400. doi: 10.1038/nm.4517
6. Chang J, Zhu W, Zhang J, Yong L, Yang M, Wang J, et al. The effect of Chinese square dance exercise on cognitive function in older women with mild cognitive impairment: the mediating effect of mood status and quality of life. Front Psychiatry. (2021) 12:711079. doi: 10.3389/fpsyt.2021.711079
7. Yong L, Liu L, Ding T, Yang G, Su H, Wang J, et al. Evidence of effect of aerobic exercise on cognitive intervention in older adults with mild cognitive impairment. Front Psychiatry. (2021) 12:713671. doi: 10.3389/fpsyt.2021.713671
8. Montana JI, Tuena C, Serino S, Cipresso P, Riva G. Neurorehabilitation of spatial memory using virtual environments: a systematic review. J Clin Med. (2019) 10:1516. doi: 10.3390/jcm8101516
9. Zhong D, Chen L, Feng Y, Song R, Huang L, Liu J, et al. Effects of virtual reality cognitive training in individuals with mild cognitive impairment: a systematic review and meta-analysis. Int J Geriatr Psychiatry. (2021) 12:1829–47. doi: 10.1002/gps.5603
10. Wu J, Ma Y, Ren Z. Rehabilitative effects of virtual reality technology for mild cognitive impairment: a systematic review with meta-analysis. Front Psychol. (2020) 11:1811. doi: 10.3389/fpsyg.2020.01811
11. Coyle H, Traynor V, Solowij N. Computerized and virtual reality cognitive training for individuals at high risk of cognitive decline: systematic review of the literature. Am J Geriatr Psychiatry. (2015) 4:335–59. doi: 10.1016/j.jagp.2014.04.009
13. Eliav R, Rand D, Schwartz Y, Blumenfeld B, Stark-Inbar A, Maoz S, et al. “Training with adaptive body-controlled virtual reality following acquired brain injury for improving executive functions,” in Proceedings of the Brain injury. Conference: 12th World Congress on Brain Injury of the International Brain Injury Association, United states. (Vol. 31), (New Orleans, LA: Brain Trauma Foundation) (2017). p. 857–8.
14. Laver K, George S, Thomas S, Deutsch JE, Crotty M. Virtual reality for stroke rehabilitation: an abridged version of a Cochrane review. Eur J Phys Rehabil Med. (2015) 4:497–506.
15. Laver KE, Lange B, George S, Deutsch JE, Saposnik G, Crotty M. Virtual reality for stroke rehabilitation. Cochrane Database Syst Rev. (2017) 11:CD008349. doi: 10.1002/14651858.CD008349
16. García-Betances RI, Arredondo Waldmeyer MT, Fico G, Cabrera-Umpiérrez MF. A succinct overview of virtual reality technology use in Alzheimer’s disease. Front Aging Neurosci. (2015) 7:80. doi: 10.3389/fnagi.2015.00080
17. Grundy J, Mouzakis K, Vasa R, Cain A, Curumsing M, Abdelrazek M, et al. Supporting diverse challenges of ageing with digital enhanced living solutions. Stud Health Technol Inform. (2018) 246:75–90.
18. Roosink M, Robitaille N, Jackson PL, Bouyer LJ, Mercier C. Interactive virtual feedback improves gait motor imagery after spinal cord injury: an exploratory study. Restor Neurol Neurosci. (2016) 2:227–35. doi: 10.3233/RNN-150563
19. Yen HY, Chiu HL. Virtual reality exergames for improving older adults’ cognition and depression: a systematic review and meta-analysis of randomized control trials. J Am Med Direct Assoc. (2021) 5:995–1002. doi: 10.1016/j.jamda.2021.03.009
20. Chao YY, Scherer YK, Montgomery CA. Effects of using Nintendo Wii™ exergames in older adults: a review of the literature. J Aging Health. (2015) 3:379–402. doi: 10.1177/0898264314551171
21. Moreno A, Wall KJ, Thangavelu K, Craven L, Ward E, Dissanayaka NN. A systematic review of the use of virtual reality and its effects on cognition in individuals with neurocognitive disorders. Alzheimers Dement. (2019) 5:834–50. doi: 10.1016/j.trci.2019.09.016
22. Cherniack EP. Not just fun and games: applications of virtual reality in the identification and rehabilitation of cognitive disorders of the elderly. Disabil Rehabil. (2011) 4:283–9. doi: 10.3109/17483107.2010.542570
23. Kim O, Pang Y, Kim JH. The effectiveness of virtual reality for people with mild cognitive impairment or dementia: a meta-analysis. BMC Psychiatry. (2019) 1:219. doi: 10.1186/s12888-019-2180-x
24. Liao YY, Tseng HY, Lin YJ, Wang CJ, Hsu WC. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur J Phys Rehabil Med. (2020) 1:47–57. doi: 10.23736/S1973-9087.19.05899-4
25. Joseph PA, Mazaux JM, Sorita E. Virtual reality for cognitive rehabilitation: from new use of computers to better knowledge of brain black box? Int J Disabil Hum Dev. (2014) 3:319–25. doi: 10.1515/ijdhd-2014-0322
26. Pareto L, Sharkey PM, Merrick JG. Using virtual reality technologies to support everyday rehabilitation. J Pain Manag. (2016) 3:197–8.
27. Pugnetti L, Mendozzi L, Motta A, Cattaneo A, Barbieri E, Brancotti A. Evaluation and retraining of adults’ cognitive impairments: which role for virtual reality technology? Comput Biol Med. (1995) 2:213–27.
28. Spiegel BM. Virtual medicine: how virtual reality is easing pain, calming nerves and improving health. Med J Aust. (2018) 6:245–7. doi: 10.5694/mja17.00540
29. Park JH, Liao Y, Kim DR, Song S, Lim JH, Park H, et al. Feasibility and tolerability of a culture-based virtual reality (VR) training program in patients with mild cognitive impairment: a randomized controlled pilot study. Int J Environ Res Public Health. (2020) 9:3030. doi: 10.3390/ijerph17093030
30. Lasaponara S, Marson F, Doricchi F, Cavallo M. A scoping review of cognitive training in neurodegenerative diseases via computerized and virtual reality tools: what we know so far. Brain Sci. (2021) 5:528. doi: 10.3390/brainsci11050528
31. Kim DR, Song S, Kim GM, Chang JH, Tak YJ, Huh U, et al. Effects of ICT-based multicomponent program on body composition and cognitive function in older adults: a randomized controlled clinical study. Clin Interv Aging. (2021) 16:1161–71. doi: 10.2147/CIA.S306894
32. Lamargue D, Koubiyr I, Deloire M, Saubusse A, Charre-Morin J, Moroso A, et al. Effect of cognitive rehabilitation on neuropsychological and semiecological testing and on daily cognitive functioning in multiple sclerosis: the REACTIV randomized controlled study. J Neurol Sci. (2020) 415:116929. doi: 10.1016/j.jns.2020.116929
33. Gates NJ, Rutjes AW, Di Nisio M, Karim S, Chong LY, March E, et al. Computerised cognitive training for maintaining cognitive function in cognitively healthy people in late life. Cochrane Database Syst Rev. (2019) 3:CD012277. doi: 10.1002/14651858.CD012277
34. Park JS, Jung YJ, Lee G. Virtual reality-based cognitive–motor rehabilitation in older adults with mild cognitive impairment: a randomized controlled study on motivation and cognitive function. Healthcare. (2020) 3:335. doi: 10.3390/healthcare8030335
35. Tuena C, Mancuso V, Stramba-Badiale C, Pedroli E, Stramba-Badiale M, Riva G, et al. Egocentric and allocentric spatial memory in mild cognitive impairment with real-world and virtual navigation tasks: a systematic review. J Alzheimers Dis. (2021) 1:95–116. doi: 10.3233/JAD-201017
36. Sakaki K, Nouchi R, Matsuzaki Y, Saito T, Dinet J, Kawashima R. Benefits of VR physical exercise on cognition in older adults with and without mild cognitive decline: a systematic review of randomized controlled trials. Healthcare. (2021) 7:883. doi: 10.3390/healthcare9070883
37. Slater M, Wilbur S. A framework for immersive virtual environments (FIVE): speculations on the role of presence in virtual environments. Presence. (1997) 6:603–16. doi: 10.1162/pres.1997.6.6.603
38. Miller HL, Bugnariu NL. Level of immersion in virtual environments impacts the ability to assess and teach social skills in autism spectrum disorder. Cyberpsychol Behav Soc Netw. (2016) 4:246–56. doi: 10.1089/cyber.2014.0682
39. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. (2003) 8:713–21. doi: 10.1093/ptj/83.8.713
40. Anderson-Hanley C, Arciero PJ, Brickman AM, Nimon JP, Okuma N, Westen SC, et al. Exergaming and older adult cognition: a cluster randomized clinical trial. Am J Prevent Med. (2012) 2:109–19. doi: 10.1016/j.amepre.2011.10.016
41. Karssemeijer EG, Bossers WJ, Aaronson JA, Sanders LM, Kessels RP, Rikkert MG. Exergaming as a physical exercise strategy reduces frailty in people with dementia: a randomized controlled trial. J Am Med Direct Assoc. (2019) 12:1502–8. doi: 10.1016/j.jamda.2019.06.026
42. Werner C, Rosner R, Wiloth S, Lemke NC, Bauer JM, Hauer K. Time course of changes in motor-cognitive exergame performances during task-specific training in patients with dementia: identification and predictors of early training response. J Neuroeng Rehabil. (2018) 15:100. doi: 10.1186/s12984-018-0433-4
43. Serino S, Pedroli E, Tuena C, De Leo G, Stramba-Badiale M, Goulene K, et al. A novel virtual reality-based training protocol for the enhancement of the “mental frame syncing” in individuals with Alzheimer’s disease: a development-of-concept trial. Front Aging Neurosci. (2017) 9:240. doi: 10.3389/fnagi.2017.00240
44. Oliveira J, Gamito P, Souto T, Conde R, Ferreira M, Corotnean T, et al. Virtual reality-based cognitive stimulation on people with mild to moderate dementia due to Alzheimer’s disease: a pilot randomized controlled trial. Int J Environ Res Public Health. (2021) 10:5290. doi: 10.3390/ijerph18105290
45. Padala KP, Padala PR, Lensing SY, Dennis RA, Bopp MM, Roberson PK, et al. Home-based exercise program improves balance and fear of falling in community-dwelling older adults with mild Alzheimer’s disease: a pilot study. J Alzheimers Dis. (2017) 2:565–74. doi: 10.3233/JAD-170120
46. Jia LF, Du YF, Chu L, Zhang Z, Li F, Lyu D, et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health. (2020) 12:E661–71. doi: 10.1016/S2468-2667(20)30185-7
47. Chang J, Chen Y, Liu C, Yong L, Yang M, Zhu W, et al. Effect of square dance exercise on older women with mild mental disorders. Front Psychiatry. (2021) 12:699778. doi: 10.3389/fpsyt.2021.699778
48. Liu W, Zhang J, Wang Y, Li J, Chang J, Jia Q. Effect of physical exercise on cognitive function of alzheimer’s disease patients: a systematic review and meta-analysis of randomized controlled trial. Front Psychiatry. (2022) 13:927128. doi: 10.3389/fpsyt.2022.927128
Keywords: virtual reality, Alzheimer’s disease, systematic review, exercise, internation
Citation: Yi Y, Hu Y, Cui M, Wang C and Wang J (2022) Effect of virtual reality exercise on interventions for patients with Alzheimer’s disease: A systematic review. Front. Psychiatry 13:1062162. doi: 10.3389/fpsyt.2022.1062162
Received: 05 October 2022; Accepted: 24 October 2022;
Published: 09 November 2022.
Edited by:
Zezhi Li, Guangzhou Medical University, ChinaReviewed by:
Junfeng Li, Shandong Institute of Business and Technology, ChinaWenbing Zhu, Chongqing Normal University, China
Copyright © 2022 Yi, Hu, Cui, Wang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuanyan Hu, NTgzOTA4NTczQHFxLmNvbQ==; Cheng Wang, d2NoLXdhbmdAMTI2LmNvbQ==; Jibing Wang, YmVud2FuZ2tpbmdAMTI2LmNvbQ==