 Milica M. Borovcanin
Milica M. Borovcanin Katarina Vesic
Katarina Vesic Y. Hasan Balcioglu
Y. Hasan Balcioglu Nataša R. Mijailović
Nataša R. Mijailović
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Psychiatry , 19 October 2022
Sec. Molecular Psychiatry
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.1052710
This article is part of the Research Topic Neuropsychiatric Manifestations and Neuroimmune Correlates of COVID-19 View all articles
Although Coronavirus disease (COVID-19) infection is primarily associated with fever, respiratory symptoms, pneumonia, and acute respiratory distress syndrome, the virus causing this infection has shown signs of tropism in other tissues (1). Direct and indirect disturbances affecting the nervous system are well documented, but the exact mechanisms of brain pathology in COVID-19 infection are not fully elucidated (2, 3). Mounting evidence implicates that the novel coronavirus is both neurotropic and vasculotropic (4, 5). Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) has the potential to spread directly from the respiratory tract to the central nervous system (CNS) via retrograde axonal transport from peripheral nerves (6). In this pathway, nasal inoculation of SARS-CoV-2 led to direct infection of the olfactory epithelium, sensory and olfactory nerves, olfactory bulb and brain (7). An alternative pathway to the CNS is the hematogenous route (8) through which SARS-CoV-2-infected peripheral myeloid cells are transmigrated to organ systems (9). Multi-organ failure is a consequence of the spread of the virus to various organs via systemic circulation. Direct endothelial infection leading to disruption of the blood-brain barrier (BBB) or infiltration of immune cells carrying SARS-CoV-2 are presented as possible mechanisms of hematogenous dissemination of the virus (10–12). Angiotensin-Converting Enzyme-2 (ACE-2), a functional receptor of SARS-CoV-2, may facilitate direct invasion of cerebrovascular endothelial cells and neurons, leading to a pro-thrombotic state with occlusion of cerebral vessels, apoptosis, and neuronal cell death (13, 14).
At the onset of the pandemic COVID-19, the medical community made great efforts to establish appropriate treatment protocols and is still advancing in this area. There are a number of newly developed virostatic drugs (15), but another direction has been to use already known agents in these new circumstances. When the use of chloroquine was under discussion, we also discussed the possibility of using chlorpromazine in our previous paper (16). Until the beginning of the pandemic and even today, all psychotropic drugs have been cautiously used in individuals with different types of pulmonary obstruction (17). In light of the emerging fact that infection with COVID-19 is a multisystemic illness associated with various mental disorders, the appropriateness and justifiability of prescribing psychotropic drugs, particularly antidepressants, has been reconsidered. According to the current protocol, there are no precise recommendations for the use of antidepressants in the treatment of COVID-19 infections, especially considering their potential for causal use. In Serbia and Turkiye, only psychiatrists are licensed to prescribe antidepressants, and many consultations have been conducted in intensive care units, with unspoken pressure from colleagues who specialize in somatic treatment that antidepressants should be prescribed urgently to immediately resolve ongoing mental health problems.
We attempt to form our own opinion with clear boundaries, outlining why and when selective serotonin reuptake inhibitors (SSRI) such as fluoxetine, sertraline, fluvoxamine, paroxetine, citalopram, escitalopram, etc. can and should be prescribed in the treatment of COVID-19 infections. Our conclusions and recommendations are based on the recent extensive studies on the use of SSRIs in the treatment of COVID-19 and the known previous data on their mechanism of action, interactions, and prescription in an appropriate time and indication range. As their name implies, the predominant mechanism of action is selective serotonin reuptake inhibition, taking into account the monoaminergic hypothesis, while also expressing their effects on noradrenaline, dopamine, and other neurotransmitter systems. They are indicated and widely used in clinical practice for the treatment of depression (unipolar and bipolar), anxiety disorders, personality disorders, dementia, insomnia, addiction, neuropathic pain, cancer, and even psychosis, etc., and currently SSRI repurposing is very attractive, focusing on immunomodulatory, antiproliferative, and neuroprotective activity (18). Particular attention has been paid to the possible anti-inflammatory properties of SSRIs, which may be useful, although adverse effects have been warned for initial prescription and long-term use.
Most evidence suggests that aberrations in immune-inflammatory pathways contribute to the pathophysiology of depression (19). Leonard, in his review article (20), discusses whether sickness behavior is part of a continuum that develops into major depression or whether it is a separate process. Sickness behavior tends to be a short-term response to an acute inflammatory challenge, and when inflammation becomes chronic, mood symptoms predominate and may even worsen the outcome. Depression in COVID-19 infection could be due to viral infection or host immune response (21). Common underlying pathophysiological mechanisms of COVID-19 infection and depression could be the presence of ACE-2 receptors on the cell surface and cytokine secretion (22). More precisely, decreased ACE-2 action and increased production of mediators such as IL-6, TNF-α, and IFN-γ could contribute to depression.
Immune cells seem to have the potential for synthesis, transport, and storage of serotonin but are also responsive to serotonin impact (23). The results of meta-analysis of major depressive disorder studies showed that antidepressants in general and SSRIs and serotonin-norepinephrine reuptake inhibitors (SNRIs) in particular decreased plasma levels of several proinflammatory cytokines such as IL-6, IL-10, TNF-α, C-reactive protein, and C–C Motif Chemokine Ligand (24, 25). A recent meta-analysis revealed that respondents to antidepressants have lower IL-8 than non-responders (26). In analyzing the anti-inflammatory properties of antidepressants, SSRIs have been shown to more potently inhibit microglial production of TNF-α and nitric oxide (NO) via regulation of cyclic adenosine monophosphate (cAMP) signaling compared with SNRIs (27). Another possible mechanism of antidepressants is modulation of the NLRP3-inflammasome complex which has been demonstrated in THP-1 cells stimulated with ATP in vitro as well as in animal models of stress-induced depression or in depressed patients. Nine drugs, including paroxetine, fluoxetine, mirtazapine, mianserin, desvenlafaxine, venlafaxine, imipramine, amitriptyline, and agomelatine, induced a significant reduction in inflammasome activation by inhibiting IL-1β and IL-18 (28). Considering that many antidepressants have the ability to modulate immune reactions (25), it is likely that the beneficial effects of mental health medications, including SSRIs, on COVID-19 are partly based on their anti-inflammatory activity.
Tryptophan metabolism and kynurenines are related to inflammation and immunity (29), which are also simultaneously being explored as a possible pathway for antidepressant action (30). Analysis of the metabolome profile of patients infected with SARS-CoV-2 revealed the influence of tryptophan-nicotinamide pathway and cytosine on inflammatory signals and microbiota (31). Furthermore, serum analysis of COVID-19 patients showed altered tryptophan metabolism in the kynurenine pathway, which correlated with levels of IL-6 (32), thus implying that antidepressants might control destructive immune activity by balancing a disturbed tryptophan metabolism.
There are some recent suggestions for nonconventional mechanisms of action of SSRIs that may be of use in the treatment of COVID-19 infection. In preclinical models of inflammation and sepsis, the sigma-1 receptor (SIR-1) has been identified as an essential inhibitor of cytokine production (33), and it has been postulated that sigma receptors may be involved in the neuronal transmission of SARS-CoV-2 (34). Fluvoxamine, an SSRI antidepressant, has been shown to enhance a key cellular anti-inflammatory system by stimulating SIR-1 (35–37). Inhibition of the acid sphingomyelinase (ASM)/ceramide system plays an important role and may explain both the potential antiviral and anti-inflammatory effects of certain antidepressants in COVID-19 (38). ASM is an enzyme that converts sphingomyelin to phosphorylcholine and ceramide, and high concentrations of ceramide in the cell membrane are thought to disrupt membrane integrity, thereby facilitating viral entry (39, 40). The magnitude of in vitro inhibition of ASM by SSRIs varies across molecules (e.g., fluoxetine > paroxetine > fluvoxamine > other SSRIs) (41, 42), and appears to correlate with the magnitude of in vitro antiviral effect against SARS-CoV-2 (43, 44). Fluoxetine has been shown to inhibit SARS-CoV-2 entry into epithelial cells as well as SARS-CoV-2 replication (43, 45, 46). Moreover, decreased immunoglobulin E-mediated mast-cell degranulation and impaired endolysosomal viral trafficking are considered mechanisms limiting hyperinflammatory immune responses (47–49). The antiviral activity of SSRIs could also be reflected in targeting phospholipid production and melatonin levels (50).
The newest clinical experience in the treatment of COVID-19 has demonstrated the beneficial role of antidepressant use, particularly SSRIs, in somatic status and potential outcomes. More importantly, however, this benefit has been observed not only for mental functioning but also for the somatic state of these patients. In exploring the “anti-COVID-19” potential of antidepressants, SSRIs such as fluvoxamine and, to a lesser extent, fluoxetine have been shown to be the most important drugs with positive effects on overall disease outcome.
Application of fluvoxamine as an additional treatment for COVID-19 significantly reduced severe COVID-19 outcomes and effectively prevented clinical worsening and hospitalization (51, 52), and also reduced mortality in COVID-19-patients hospitalized in the intensive care unit (53). Furthermore, it predicted fewer hospitalizations and residual symptoms in SARS-CoV-2-positive adult home-isolated patients (54). In a recent study, fluvoxamine was examined at a low dose of 50 mg twice daily but did not prevent hypoxia, emergency department visits, hospitalization, or death (55).
The use of SSRIs, particularly fluoxetine, was associated with a lower relative risk of death compared with patients not on SSRIs (56). The protective effect of antidepressants in COVID-19 was mainly governed by SSRI, SNRI, and serotonin-2 antagonist reuptake inhibitors (57). Adult patients hospitalized with moderate or severe COVID-19 pneumonia that received fluoxetine along with anti-COVID-19 therapies had significantly decreased mortality (70%) compared to the non-fluoxetine group (58). Exposure to fluoxetine, venlafaxine, mirtazapine, and escitalopram was found to be significantly associated with a lower risk of intubation or death in COVID-19 patients (59).
On the other hand, no relevant influence of antidepressants on COVID-19 duration and severity was observed (60). The meta-analyses by Vai et al. (61) showed an increased risk of COVID-19 mortality in patients with psychotic and mood disorders, and those taking antipsychotics or anxiolytics represent a susceptible subgroup, whereas antidepressant use had no effect on mortality risk. No significant difference in mortality risk was observed between patients taking/non-taking SSRIs (62). The use of tricyclic and related antidepressants prior to COVID-19 diagnosis was not associated with the occurrence of severe COVID-19 clinical symptoms (63).
Patients with severe mental illness (e.g., schizophrenia spectrum disorder, bipolar disorder, unipolar depression) have been shown to be at increased risk for a more drastic COVID-19 course and resulting lethality (64–66). According to recent evidence, this risk may not be due to the psychiatric illness alone, but rather to the presence of somatic comorbidity, which significantly influences the development of COVID-19 morbidity and mortality, especially in the specific population of psychiatric patients (67, 68). On the basis of these data, we strongly recommend psychiatric examination and safety assessment before the application of SSRIs in COVID-19 patients, regardless of their mental illness history.
We must point out that it is necessary to continue treatment with antidepressants in patients with mental disorders, even if they have contracted SARS-CoV-2. There are no data indicating absolute contraindications in these cases. The inclusion of known SSRI antidepressants in the treatment protocols of COVID-19 requires more thorough consideration and precautions, as potential risks may arise. It is well known that these drugs can cause adverse side effects despite their good safety profile, even when used for the right indications. Expected somatic side effects such as nausea and abdominal discomfort, diarrhea and vomiting, headache, insomnia, drowsiness, and dry mouth may also occur (69).
Due to their potent anti-depressive effects, SSRIs can induce a manic switch or mixed episode or a long-term condition called rapid cycling in patients with undiagnosed bipolar affective disorder (70). On the other hand, ample evidence suggests that SARS-CoV-2, by its very nature, can also trigger the acute onset of mood disorders or psychotic symptoms (71), further complicating the prescription of SSRIs. After the first week of treatment with SSRI, clinical improvement was observed with an increased chance of a 50% reduction in Hamilton Depression Rating Scale scores at 1 week compared to placebo (72). Dionisie et al. (73) discuss that the clinical effect of SSRIs occurs after 2–4 weeks of treatment, suggesting that it is not only the increase in monoamine transmitters that is responsible for the improvement in depressive symptoms. All this points to the previous properties of SSRIs in inflammation, infection, and neuroprotection, and subsequently we need to be concerned about their effects on serotonergic transmission, especially in individuals without diagnosed depression.
In patients with COVID-19, the use of antidepressants may be particularly challenging since these medications may interact with medical treatments for COVID-19 and some of their adverse effects may worsen the course and outcome of the underlying medical condition. It is extremely important to consider the interactions of SSRIs with antiviral and other COVID-19 medications (74, 75) to determine how meaningful their repurposing is in fighting this infection. Because most COVID-19 patients are treated with low-molecular-weight heparin or novel peroral anticoagulants, it is very important to monitor hemorrhagic side effects. This is especially important when SSRIs are administered concomitantly, as SSRIs have been shown to affect platelet function (76).
Although the benefits of mental health medications, such as SSRIs in coronavirus infection have been documented to date, we have attempted to provide a balanced review of current knowledge and the risks associated with the unwarranted and imprudent clinical use of antidepressants in patients with COVID-19 infection. These drugs should certainly be applied with more caution and consideration. In addition, COVID-19 patients undergoing SSRI treatment should be closely monitored for possible adverse effects (all summarized in Figure 1).
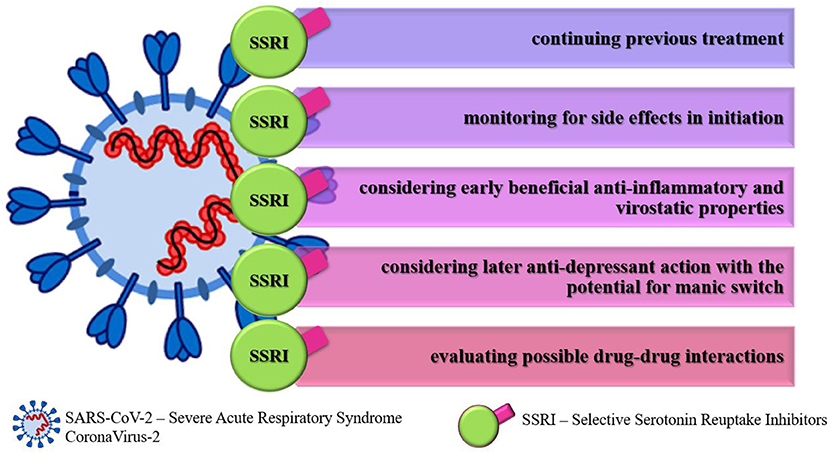
Figure 1. Recommendations for selective serotonin reuptake inhibitors usage in COVID-19 infection.
As the SARS-CoV-2 virus becomes more controllable, its pandemic importance is diminishing, necessitating a revision of therapeutic protocols. Currently, ongoing clinical trials are expected to exclude some drugs, while new drugs will improve the drug repository. We believe that further clinical studies will demonstrate determinately whether the use of these antidepressants in COVID-19 is efficient and clinically justified.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
We thank Bojana Mircetic for language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gupta A, Madhavan MV, Sehgal K, Nair N, Mahajan S, Sehrawat TS, et al. Extrapulmonary manifestations of COVID-19. Nat Med. (2020) 26:1017–32. doi: 10.1038/s41591-020-0968-3
2. Aghagoli G, Gallo Marin B, Katchur NJ, Chaves-Sell F, Asaad WF, Murphy SA. Neurological involvement in COVID-19 and potential mechanisms: a review. Neurocrit Care. (2021) 34:1062–71. doi: 10.1007/s12028-020-01049-4
3. Varatharaj A, Thomas N, Ellul MA, Davies NWS, Pollak TA, Tenorio EL, et al. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: a UK-wide surveillance study. Lancet Psychiatry. (2020) 7:875–82. doi: 10.2139/ssrn.3601761
4. Song W-J, Hui CKM, Hull JH, Birring SS, McGarvey L, Mazzone SB, et al. Confronting COVID-19-associated cough and the post-COVID syndrome: role of viral neurotropism, neuroinflammation, and neuroimmune responses. Lancet Respir Med. (2021) 9:533–44. doi: 10.1016/S2213-2600(21)00125-9
5. Baig AM. Neurological manifestations in COVID-19 caused by SARS-CoV-2. CNS Neurosci Ther. (2020) 26:499–501. doi: 10.1111/cns.13372
6. Desforges M, Le Coupanec A, Dubeau P, Bourgouin A, Lajoie L, Dubé M, et al. Human coronaviruses and other respiratory viruses: underestimated opportunistic pathogens of the central nervous system? Viruses. (2019) 12:14. doi: 10.3390/v12010014
7. Briguglio M, Bona A, Porta M. Dell'Osso B, Pregliasco FE, Banfi G. Disentangling the hypothesis of host dysosmia and SARS-CoV-2: the bait symptom that hides neglected neurophysiological routes. Front Physiol. (2020) 11:671. doi: 10.3389/fphys.2020.00671
8. Li J, Gao J, Xu Y, Zhou T, Jin Y, Lou J. Expression of severe acute respiratory syndrome coronavirus receptors, ACE2 and CD209L in different organ derived microvascular endothelial cells. Zhonghua Yi Xue Za Zhi. (2007) 87:833–7.
9. Yesilkaya UH, Balcioglu YH. Neuroimmune correlates of the nervous system involvement of COVID-19: a commentary. J Clin Neurosci. (2020) 78:449–50. doi: 10.1016/j.jocn.2020.05.056
10. Jacomy H, Fragoso G, Almazan G, Mushynski WE, Talbot PJ. Human coronavirus OC43 infection induces chronic encephalitis leading to disabilities in BALB/C mice. Virology. (2006) 349:335–46. doi: 10.1016/j.virol.2006.01.049
11. Sardu C, Gambardella J, Morelli MB, Wang X, Marfella R, Santulli G. Hypertension, thrombosis, kidney failure, and diabetes: is COVID-19 an endothelial disease? A comprehensive evaluation of clinical and basic evidence. J Clin Med. (2020) 9:1417. doi: 10.3390/jcm9051417
12. Yarlagadda A, Preston SL, Jeyadhas RP, Lang AE, Hammamieh R, Clayton AH. Blood-brain barrier: COVID-19, pandemics, and cytokine norms. Innov Clin Neurosci. (2021) 18:21–3.
13. Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. (2020) 181:271-280.e8. doi: 10.1016/j.cell.2020.02.052
14. Che Mohd Nassir CMN, Zolkefley MKI, Ramli MD, Norman HH, Abdul Hamid H, Mustapha M. Neuroinflammation and COVID-19 ischemic stroke recovery—evolving evidence for the mediating roles of the ACE2/angiotensin-(1–7)/mas receptor axis and NLRP3 inflammasome. Int J Mol Sci. (2022) 23:3085. doi: 10.3390/ijms23063085
15. Kumari M, Lu R-M, Li M-C, Huang J-L, Hsu F-F, Ko S-H, et al. A critical overview of current progress for COVID-19: development of vaccines, antiviral drugs, and therapeutic antibodies. J Biomed Sci. (2022) 29:68. doi: 10.1186/s12929-022-00852-9
16. Muric NN, Arsenijevic NN, Borovcanin MM. Chlorpromazine as a potential antipsychotic choice in COVID-19 treatment. Front Psychiatry. (2020) 11:612347. doi: 10.3389/fpsyt.2020.612347
17. Yohannes AM, Jin JW, Kunik ME. Benefit–risk assessment of psychotropic drugs in older patients with chronic obstructive pulmonary disease. Drugs Aging. (2022) 39:323–32. doi: 10.1007/s40266-022-00935-0
18. Nykamp MJ, Zorumski CF, Reiersen AM, Nicol GE, Cirrito J, Lenze EJ. Opportunities for drug repurposing of serotonin reuptake inhibitors: potential uses in inflammation, infection, cancer, neuroprotection, and Alzheimer's disease prevention. Pharmacopsychiatry. (2022) 55:24–9. doi: 10.1055/a-1686-9620
19. Miller AH, Raison CL. The role of inflammation in depression: from evolutionary imperative to modern treatment target. Nat Rev Immunol. (2016) 16:22–34. doi: 10.1038/nri.2015.5
20. Leonard BE. Inflammation and depression: a causal or coincidental link to the pathophysiology? Acta Neuropsychiatr. (2018) 30:1–16. doi: 10.1017/neu.2016.69
21. Troyer EA, Kohn JN, Hong S. Are we facing a crashing wave of neuropsychiatric sequelae of COVID-19? Neuropsychiatric symptoms and potential immunologic mechanisms. Brain Behav Immun. (2020) 87:34–9. doi: 10.1016/j.bbi.2020.04.027
22. da Silva Lopes L, Silva RO, de Sousa Lima G, de Araújo Costa AC, Barros DF, Silva-Néto RP. Is there a common pathophysiological mechanism between COVID-19 and depression? Acta Neurol Belg. (2021) 121:1117–22. doi: 10.1007/s13760-021-01748-5
23. Wu H, Denna TH, Storkersen JN, Gerriets VA. Beyond a neurotransmitter: the role of serotonin in inflammation and immunity. Pharmacol Res. (2019) 140:100–14. doi: 10.1016/j.phrs.2018.06.015
24. Hiles SA, Baker AL, de Malmanche T, Attia J. Interleukin-6, C-reactive protein and interleukin-10 after antidepressant treatment in people with depression: a meta-analysis. Psychol Med. (2012) 42:2015–26. doi: 10.1017/S0033291712000128
25. Alcocer-Gómez E, Casas-Barquero N, Williams MR, Romero-Guillena SL, Cañadas-Lozano D, Bullón P, et al. Antidepressants induce autophagy dependent-NLRP3-inflammasome inhibition in major depressive disorder. Pharmacol Res. (2017) 121:114–21. doi: 10.1016/j.phrs.2017.04.028
26. Köhler CA, Freitas TH, Stubbs B, Maes M, Solmi M, Veronese N, et al. Peripheral alterations in cytokine and chemokine levels after antidepressant drug treatment for major depressive disorder: systematic review and meta-analysis. Mol Neurobiol. (2017) 55:4195–206. doi: 10.1007/s12035-017-0632-1
27. Tynan RJ, Weidenhofer J, Hinwood M, Cairns MJ, Day TA, Walker FR. A comparative examination of the anti-inflammatory effects of SSRI and SNRI antidepressants on LPS stimulated microglia. Brain Behav Immun. (2012) 26:469–79. doi: 10.1016/j.bbi.2011.12.011
28. Liu JJ, Wei Y, Strawbridge R, Bao Y, Chang S, Shi L, et al. Peripheral cytokine levels and response to antidepressant treatment in depression: a systematic review and meta-analysis. Mol Psychiatry. (2020) 25:339–50. doi: 10.1038/s41380-019-0474-5
29. Dantzer R. Role of the kynurenine metabolism pathway in inflammation-induced depression-preclinical approaches HHS public access. Curr Top Behav Neurosci. (2017) 31:117–38. doi: 10.1007/7854_2016_6
30. Correia AS, Vale N. Tryptophan metabolism in depression: a narrative review with a focus on serotonin and kynurenine pathways. Int J Mol Sci. (2022) 23:8493. doi: 10.3390/ijms23158493
31. Blasco H, Bessy C, Plantier L, Lefevre A, Piver E, Bernard L, et al. The specific metabolome profiling of patients infected by SARS-CoV-2 supports the key role of tryptophan-nicotinamide pathway and cytosine metabolism. Sci Rep. (2020) 10:16824. doi: 10.1038/s41598-020-73966-5
32. Thomas T, Stefanoni D, Reisz JA, Nemkov T, Bertolone L, Francis RO, et al. COVID-19 infection alters kynurenine and fatty acid metabolism, correlating with IL-6 levels and renal status. JCI Insight. (2020) 5:140327. doi: 10.1172/jci.insight.140327
33. Rosen DA, Seki SM, Fernández-Castañeda A, Beiter RM, Eccles JD, Woodfolk JA, et al. Modulation of the sigma-1 receptor–IRE1 pathway is beneficial in preclinical models of inflammation and sepsis. Sci Transl Med. (2019) 11:5266. doi: 10.1126/scitranslmed.aau5266
34. Yesilkaya UH, Balcioglu YH, Sahin S. Reissuing the sigma receptors for SARS-CoV-2. J Clin Neurosci. (2020) 80:72–3. doi: 10.1016/j.jocn.2020.08.014
35. Hashimoto K. Repurposing of CNS drugs to treat COVID-19 infection: targeting the sigma-1 receptor. Eur Arch Psychiatry Clin Neurosci. (2021) 271:249–58. doi: 10.1007/s00406-020-01231-x
36. Narita N, Hashimoto K, Tomitaka S, Minabe Y. Interactions of selective serotonin reuptake inhibitors with subtypes of σ receptors in rat brain. Eur J Pharmacol. (1996) 307:117–9. doi: 10.1016/0014-2999(96)00254-3
37. Hashimoto K. Activation of sigma-1 receptor chaperone in the treatment of neuropsychiatric diseases and its clinical implication. J Pharmacol Sci. (2015) 127:6–9. doi: 10.1016/j.jphs.2014.11.010
38. Hoertel N, Sánchez-Rico M, Cougoule C, Gulbins E, Kornhuber J, Carpinteiro A, et al. Repurposing antidepressants inhibiting the sphingomyelinase acid/ceramide system against COVID-19: current evidence and potential mechanisms. Mol Psychiatry. (2021) 26:7098–9. doi: 10.1038/s41380-021-01254-3
39. Chung H-Y, Claus RA. Keep your friends close, but your enemies closer: role of acid sphingomyelinase during infection and host response. Front Med. (2021) 7:616500. doi: 10.3389/fmed.2020.616500
40. Abusukhun M, Winkler MS, Pöhlmann S, Moerer O, Meissner K, Tampe B, et al. Activation of sphingomyelinase-ceramide-pathway in COVID-19 purposes its inhibition for therapeutic strategies. Front Immunol. (2021) 12:784989. doi: 10.3389/fimmu.2021.784989
41. Kornhuber J, Tripal P, Reichel M, Mühle C, Rhein C, Muehlbacher M, et al. Functional inhibitors of acid sphingomyelinase (FIASMAs): a novel pharmacological group of drugs with broad clinical applications. Cell Physiol Biochem. (2010) 26:9–20. doi: 10.1159/000315101
42. Kornhuber J, Hoertel N, Gulbins E. The acid sphingomyelinase/ceramide system in COVID-19. Mol Psychiatry. (2022) 27:307–314. doi: 10.1038/s41380-021-01309-5
43. Schloer S, Brunotte L, Goretzko J, Mecate-Zambrano A, Korthals N, Gerke V, et al. Targeting the endolysosomal host-SARS-CoV-2 interface by clinically licensed functional inhibitors of acid sphingomyelinase (FIASMA) including the antidepressant fluoxetine. Emerg Microbes Infect. (2020) 9:2245–55. doi: 10.1080/22221751.2020.1829082
44. Hoertel N. Do the selective serotonin reuptake inhibitor antidepressants fluoxetine and fluvoxamine reduce mortality among patients with COVID-19? JAMA Netw Open. (2021) 4:e2136510. doi: 10.1001/jamanetworkopen.2021.36510
45. Carpinteiro A, Edwards MJ, Hoffmann M, Kochs G, Gripp B, Weigang S, et al. Pharmacological inhibition of acid sphingomyelinase prevents uptake of SARS-CoV-2 by epithelial cells. Cell Reports Med. (2020) 1:100142. doi: 10.1016/j.xcrm.2020.100142
46. Brunotte L, Zheng S, Mecate-Zambrano A, Tang J, Ludwig S, Rescher U, et al. Combination therapy with fluoxetine and the nucleoside analog GS-441524 exerts synergistic antiviral effects against different SARS-CoV-2 variants in vitro. Pharmaceutics. (2021) 13:1400. doi: 10.3390/pharmaceutics13091400
47. Zimniak M, Kirschner L, Hilpert H, Geiger N, Danov O, Oberwinkler H, et al. The serotonin reuptake inhibitor Fluoxetine inhibits SARS-CoV-2 in human lung tissue. Sci Rep. (2021) 11:5890. doi: 10.1038/s41598-021-85049-0
48. Hashimoto Y, Suzuki T, Hashimoto K. Old drug fluvoxamine, new hope for COVID-19. Eur Arch Psychiatry Clin Neurosci. (2022) 272:161–3. doi: 10.1007/s00406-021-01326-z
49. Sukhatme VP, Reiersen AM, Vayttaden SJ, Sukhatme VV. Fluvoxamine: a review of its mechanism of action and its role in COVID-19. Front Pharmacol. (2021) 12:652688. doi: 10.3389/fphar.2021.652688
50. Hashimoto Y, Suzuki T, Hashimoto K. Mechanisms of action of fluvoxamine for COVID-19: a historical review. Mol Psychiatry. (2022) 27:1898–907. doi: 10.1038/s41380-021-01432-3
51. Lenze EJ, Mattar C, Zorumski CF, Stevens A, Schweiger J, Nicol GE, et al. Fluvoxamine vs. placebo and clinical deterioration in outpatients with symptomatic COVID-19. JAMA. (2020) 324:2292. doi: 10.1001/jama.2020.22760
52. Reis G, dos Santos Moreira-Silva EA, Silva DCM, Thabane L, Milagres AC, Ferreira TS, et al. Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial. Lancet Glob Heal. (2022) 10:e42–51. doi: 10.1016/S2214-109X(21)00448-4
53. Calusic M, Marcec R, Luksa L, Jurkovic I, Kovac N, Mihaljevic S, et al. Safety and efficacy of fluvoxamine in COVID-19 ICU patients: an open label, prospective cohort trial with matched controls. Br J Clin Pharmacol. (2022) 88:2065–73. doi: 10.1111/bcp.15126
54. Seftel D, Boulware DR. Prospective cohort of fluvoxamine for early treatment of coronavirus disease 19. Open Forum Infect Dis. (2021) 8:50. doi: 10.1093/ofid/ofab050
55. Bramante CT, Huling JD, Tignanelli CJ, Buse JB, Liebovitz DM, Nicklas JM, et al. Randomized trial of metformin, ivermectin, and fluvoxamine for Covid-19. N Engl J Med. (2022) 387:599–610. doi: 10.1056/NEJMoa2201662
56. Oskotsky T, Marić I, Tang A, Oskotsky B, Wong RJ, Aghaeepour N, et al. Mortality risk among patients with COVID-19 prescribed selective serotonin reuptake inhibitor antidepressants. JAMA Netw Open. (2021) 4:e2133090. doi: 10.1001/jamanetworkopen.2021.33090
57. Clelland CL, Ramiah K, Steinberg L, Clelland JD. Analysis of the impact of antidepressants and other medications on COVID-19 infection risk in a chronic psychiatric in-patient cohort. BJPsych Open. (2022) 8:e6. doi: 10.1192/bjo.2021.1053
58. Németh ZK, Szucs A, Vitrai J, Juhász D, Németh JP, Holló A. Fluoxetine use is associated with improved survival of patients with COVID-19 pneumonia: a retrospective case-control study. Ideggyogy Sz. (2021) 74:389–96. doi: 10.18071/isz.74.0389
59. Hoertel N, Sánchez-Rico M, Vernet R, Beeker N, Jannot A-S, Neuraz A, et al. Association between antidepressant use and reduced risk of intubation or death in hospitalized patients with COVID-19: results from an observational study. Mol Psychiatry. (2021) 26:5199–5212. doi: 10.1038/s41380-021-01021-4
60. Bonnet U, Claus B, Schaefer M, Kuhn J, Nyhuis P, Scherbaum N, et al. Impact of psychiatric and related somatic medications on the duration and severity of COVID-19: a retrospective explorative multi-center study from the German metropolitan ruhr-area. Pharmacopsychiatry. (2022) 55:30–9. doi: 10.1055/a-1559-3904
61. Vai B, Mazza MG, Delli Colli C, Foiselle M, Allen B, Benedetti F, et al. Mental disorders and risk of COVID-19-related mortality, hospitalisation, and intensive care unit admission: a systematic review and meta-analysis. Lancet Psychiatry. (2021) 8:797–812. doi: 10.1016/S2215-0366(21)00232-7
62. Rauchman SH, Mendelson SG, Rauchman C, Kasselman LJ, Pinkhasov A, Reiss AB. Ongoing use of SSRIs does not alter outcome in hospitalized COVID-19 patients: a retrospective analysis. J Clin Med. (2021) 11:70. doi: 10.3390/jcm11010070
63. McKeigue PM, Kennedy S, Weir A, Bishop J, McGurnaghan SJ, McAllister D, et al. Relation of severe COVID-19 to polypharmacy and prescribing of psychotropic drugs: the REACT-SCOT case-control study. BMC Med. (2021) 19:51. doi: 10.1186/s12916-021-01907-8
64. Barcella CA, Polcwiartek C, Mohr GH, Hodges G, Søndergaard K, Niels Bang C, et al. Severe mental illness is associated with increased mortality and severe course of COVID-19. Acta Psychiatr Scand. (2021) 144:82–91. doi: 10.1111/acps.13309
65. Chen S, Fernandez-Egea E, Jones PB, Lewis JR, Cardinal RN. Longer-term mortality following SARS-CoV-2 infection in people with severe mental illness: retrospective case-matched study. BJPsych Open. (2021) 7:e201. doi: 10.1192/bjo.2021.1046
66. Toubasi AA, AbuAnzeh RB, Tawileh HBA, Aldebei RH, Alryalat SAS. A meta-analysis: the mortality and severity of COVID-19 among patients with mental disorders. Psychiatry Res. (2021) 299:113856. doi: 10.1016/j.psychres.2021.113856
67. Hoertel N, Sánchez-Rico M, Herrera-Morueco JJ, de la Muela P, Gulbins E, Kornhuber J, et al. Comorbid medical conditions are a key factor to understand the relationship between psychiatric disorders and COVID-19-related mortality: Results from 49,089 COVID-19 inpatients. Mol Psychiatry. (2022) 27:1278–1280. doi: 10.1038/s41380-021-01393-7
68. Sánchez-Rico M, Limosin F, Hoertel N. Is a diagnosis of schizophrenia spectrum disorder associated with increased mortality in patients with COVID-19? Am J Psychiatry. (2022) 179:71–3. doi: 10.1176/appi.ajp.2021.21020196
69. Ferguson JM. SSRI antidepressant medications:adverse effects and tolerability. Prim Care Companion J Clin Psychiatry. (2001) 03:22–7. doi: 10.4088/PCC.v03n0105
70. Baldessarini RJ, Faedda GL, Offidani E, Vázquez GH, Marangoni C, Serra G, et al. Antidepressant-associated mood-switching and transition from unipolar major depression to bipolar disorder: a review. J Affect Disord. (2013) 148:129–35. doi: 10.1016/j.jad.2012.10.033
71. Rogers JP, Chesney E, Oliver D, Pollak TA, McGuire P, Fusar-Poli P, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. (2020) 7:611–27. doi: 10.1016/S2215-0366(20)30203-0
72. Taylor MJ, Freemantle N, Geddes JR, Bhagwagar Z. Early onset of selective serotonin reuptake inhibitor antidepressant action. Arch Gen Psychiatry. (2006) 63:1217. doi: 10.1001/archpsyc.63.11.1217
73. Dionisie V, Filip GA, Manea MC, Manea M, Riga S. The anti-inflammatory role of SSRI and SNRI in the treatment of depression: a review of human and rodent research studies. Inflammopharmacology. (2021) 29:75–90. doi: 10.1007/s10787-020-00777-5
74. Gandhi Z, Mansuri Z, Bansod S. Potential interactions of remdesivir with pulmonary drugs: a Covid-19 perspective. SN Compr Clin Med. (2020) 2:1707–8. doi: 10.1007/s42399-020-00462-2
75. Kumar D, Trivedi N. Disease-drug and drug-drug interaction in COVID-19: risk and assessment. Biomed Pharmacother. (2021) 139:111642. doi: 10.1016/j.biopha.2021.111642
Keywords: SSRIs, COVID-19, antidepressants, inflammation, adverse effect
Citation: Borovcanin MM, Vesic K, Balcioglu YH and Mijailović NR (2022) Prescription of selective serotonin reuptake inhibitors in COVID-19 infection needs caution. Front. Psychiatry 13:1052710. doi: 10.3389/fpsyt.2022.1052710
Received: 24 September 2022; Accepted: 06 October 2022;
Published: 19 October 2022.
Edited by:
Michael Kluge, University Hospital Leipzig, GermanyReviewed by:
Kenji Hashimoto, Chiba University, JapanCopyright © 2022 Borovcanin, Vesic, Balcioglu and Mijailović. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Milica M. Borovcanin, bWlsaWNhYm9yb3ZjYW5pbkB5YWhvby5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.