 Yaqing Yuan
Yaqing Yuan Jianing Ding3†
Jianing Ding3† Yang Liu
Yang Liu Jingmin Liu
Jingmin Liu- 1Division of Sports Science and Physical Education, Tsinghua University, Beijing, China
- 2College of Sports and Health, Shandong Sport University, Jinan, Shandong, China
- 3Department of Physical Education, Fujian Agriculture and Forestry University, Fuzhou, Fujian, China
- 4Department of Health Management, Yongan Prison of Fujian Province, Yongan, Fujian, China
- 5Department of Physical Education, China Disabled Persons’ Federation, Beijing, China
- 6Beijing Tongzhou Nationalities Primary School, Beijing, China
- 7Department of Physical Education, Shandong Jianzhu University, Jinan, Shandong, China
Background: There is evidence that the after-school period plays an essential role in accumulating sedentary behavior (SB) among children and adolescents, as well as implementing potential interventions. However, relatively little is known regarding SB status of children and adolescents with intellectual disabilities (ID) during the after-school period. The purpose of this study was to investigate the total level and specific pattern of the after-school SB among children and adolescents with ID.
Methods: The after-school SB status among 325 children and adolescents with ID was evaluated by the parent-reported Children’s Leisure Activities Study Survey-Chinese edition questionnaire.
Results: Parents of children and adolescents with ID reported approximately 204 min/day of after-school SB. Specifically, the longest time of the after-school period was spent performing the screen-based SB (84 mins/d). This was followed by recreational SB and educational SB (50 and 30 mins/d, respectively). The children aged 6–12 years old engaged more time in recreational SB than adolescents aged 16–18 years old (p < 0.05) during the after-school period. Further, the data indicated that 37.5% of children and adolescents with ID achieved the guideline limitation of 2-h-maximum screen-based SB during the after-school hour.
Conclusion: Children and adolescents with ID spent a large portion of the after-school period in SB, particularly engaged in more time on after-school screen-based SB. Future efforts should focus on developing and implementing period-specific interventions designed to reduce after-school SB in the segment of this population.
Introduction
The review by Carson et al. showed that it was crucial and beneficial for children and adolescents to engage in moderate-to-vigorous physical activity (MVPA) for 60 min every day (1). However, research focusing on other health-related behavior for the remaining 23 h of the day has traditionally been scarce, although it is fast increasing. Sedentary behavior (SB) is one of the particular critical behaviors, which is defined as any waking behavior (e.g., in a seating, reclining, or lying down posture) with an energy expenditure ≤ 1.5 METs (metabolic equivalents) (2).
It has been demonstrated in numerous studies that SB is increasingly linked to all-cause mortality, overweight/obesity, type II diabetes, lower physical fitness, cardiovascular disease, and some cancers, independent of physical activity (PA) (3–5). Furthermore, the findings from Carson et al.’s review have also revealed that different types of SB (e.g., watching TV, using the computer, or doing homework) may have various impacts on health (1).
More recently, SB has been common among children and adolescents worldwide (6). Based on solid evidence from two national-level datasets in Canada and the United States, SB was found to account for a substantial proportion of waking times (50–60%) of the day in children and adolescents (7, 8). To reduce the adverse health impacts of SB, the World Health Organization (WHO) suggests that 5–17-year-old children and adolescents should limit screen-based SB to under 2 h per day (9). The 24-Hour Movement Guideline also recommends that children and adolescents minimize time spent in SB (10). These recommendations apply to most children and adolescents, including those peers with ID.
Prior studies have found that children and adolescents with ID spent more time sedentary than their counterparts without ID (11–13). Esposito et al. and Phillips et al. also pointed out that the high prevalences of obesity, poor fitness, and functional limitations experienced by children and adolescents with ID, possibly be related to their high levels of SB (11, 12). A high level of SB may, in turn, lead to a further increase in adverse health outcomes among children and adolescents with ID. Under such circumstances, children and adolescents with ID may not be able to avoid the negative health effect of long-term SB engagement, even though they could follow the MVPA recommendations. In addition, it is essential to note that in the general population, SB appears to increase from childhood to adulthood (6, 8). The existing data indicate that, from the life-cycle perspective, individuals with ID often experience premature aging issues (14). These early onset aging may affect the pattern of SB development throughout the lifespan of children and adolescents with ID. Thus, there is a great need for a more comprehensive and detailed look at the characteristics of SB among children and adolescents with ID.
A range of research has revealed that the specific time of the day that can potentially make a significant contribution to children and adolescents’ daily SB is the after-school period (15, 16). Children and adolescents are often not bound by school schedules during this period. They have more choices about their behavior than during the school day. However, to our knowledge, there was only one study that focused on the field of after-school SB among children with ID (17). Foley and McCubbin found that 7–12 year-old children with ID spent time on watching TV or on the computer was no different than their peers without ID, but it was encouraging that the majority of the children did not exceed the limitation of 2 h/d. It is worth noting that the study was published more than 10 years ago, and given the small sample size, it is uncertain whether its findings are still valid in terms of reflecting the after-school SB of children with ID today. In this context, our study was conducted to understand the overall level SB and detailed information on different types of SB during the after-school period among children and adolescents with ID aged 6–18 years through a relatively large sample sampling, as a step toward establishing and collecting baseline data to provide targeted period-specific strategies for health promotion in this population.
Materials and methods
Study design
A cross-sectional descriptive design assessed the after-school SB status among children and adolescents with ID by using parent-reported surveys. The survey was completed between September 13 and December 24, 2021. All parents involved in this study, as well as their children, were explicitly advised that participation was entirely voluntary. All the data were centrally analyzed anonymously. The study was conducted in accordance with the Declaration of Helsinki Principles, and approved by the ethics committee of the university.
Participants
A convenience sampling strategy focusing on the parents of children and adolescents with ID was utilized among special education schools in Shandong Province. The following were inclusion criteria for the parents: (1) their child came from day school; (2) their child was between the ages of 6 and 18; (3) their child could walk without any help; and (4) their child did not experience coexisting cerebral palsy, autism, and other sensory impairments. The ID level was categorized as profound [intelligence quotient (IQ) < 25], severe (IQ of 25–39), moderate (IQ of 40–54), and mild (IQ of 55–70) (18). Additionally, children and adolescents with ID were divided into three age subgroups, 6–12, 13–15, and 16–18 years old, which matched the Chinese school education system’s definition of the age range for the primary, junior middle, and junior high schools (19).
Procedures
Based on the most recent data, 33 special education schools primarily recruit children and adolescents with ID in Shandong Province of China (20). The school-keepers from 16 special education schools were contacted through the help of the China Disabled Persons’ Federation. Finally, 10 special education schools accepted the invitation and consented to participate in the study. Invitations containing the purpose and content of this study were sent out by headmasters to the legal guardians of children and adolescents with ID. In the meantime, the objective of the present study was explained briefly to children and adolescents with ID. Verbal permission was also obtained in their schools prior to data collection. Once the caregivers gave written informed consent, the teachers contacted them to come to school to complete the questionnaire. The parents were given step-by-step instructions by trained teachers and researchers through the parents’ meeting on how to complete the questionnaire. They were also given plenty of time for questions.
Sedentary behavior assessment
After-school SB of children and adolescents with ID was assessed using reliable items from the Children’s Leisure Activities Study Survey-Chinese edition (CLASS-C) questionnaire, which is widely used in China and has good reliability and validity (21). Li et al. also stressed that no statistically significant difference was observed in measurement between the CLASS-C questionnaire and accelerometry (21). In this study, prior to data collection, a pretest CLASS-C questionnaire was completed by a sample of 30 parents from one special education school in the Jinan City of Shandong Province. The pretest showed that the CLASS-C questionnaire possessed sound reliability (Cronbach’s a = 0.752). The CLASS-C questionnaire contained a list of twelve common after-school SB in addition to demographic information that consisted of gender, age, height, weight, and ID level. Based on the manifestation of behavior, these common after-school SB can be classified into four categories: screen-based SB (watch TV, play video/computer games, and surf the Internet), educational SB (do homework and read books), recreational SB (play with toys, listen to music, play musical instruments, play card games, and art activities) and social SB (chat while sitting stationary and make phone calls). In addition, as this study only focused on the after-school period, parents were requested to provide the amount of time their child spent on the specific after-school SB pattern from Monday to Friday (five consecutive days). After-school hours, in this study, were defined as the period between the end of school bell time and bedtime.
The parent-reported survey was chosen in the current study for the following three reasons. First, children and adolescents with ID may not completely understand the content of the questionnaire, and hard to finish the questionnaire independently. In documenting their child’s activities, Burdette et al. found that parents were able to give accurate estimates (22). Second, the questionnaire measurement could gather information about the type of SB–a capability not provided by device-based assessments, such as accelerometers. Further, large-scale epidemiological studies often consider questionnaires as a cost-effective alternative to accelerometers.
Statistical analyses
All data analyses were conducted on SPSS version 25.0 for Mac (SPSS Inc., Chicago, IL, USA). Descriptive statistics were calculated for all study variables (gender, age, weight status, and ID level). All variables were examined whether they were normally distributed by means of the Kolmogorov–Smirnov test. Due to the non-normal distribution of SB variables, the Mann–Whitney U test was utilized to compare the SB differences between gender and weight status. The Kruskal–Wallis test was applied to analyze differences in SB between age and ID level. For prevalence, estimates were calculated as the percentage of children and adolescents with ID who achieved the 2-h-maximum screen-based SB time limitation in the guideline. Differences in the prevalence of screen-based SB time limitation by gender, age, weight status, and ID level were tested using a binary logistic regression model. Prevalence estimates, odds ratio (OR), and corresponding 95% confidence interval (CI) were calculated from the logistic regression. P-values < 0.05 were considered statistically significant for all analyses.
Results
Demographic analysis
Data in relation to after-school SB from 325 children and adolescents with ID were provided from parents’ reports. A total of 220 (67.7%) children and adolescents with ID were boys, aged 12.4 ± 3.3, and 105 (32.3%) were girls, aged 12.7 ± 3.8. In addition, 104 (32.0%) of them were moderate ID, 167 (51.4%) were severe ID, and 54 (16.6%) were profound ID.
After-school sedentary behavior level among children and adolescents with intellectual disabilities
The daily time of total after-school SB and specific types of after-school SB among children and adolescents with ID are presented in Table 1. Children and adolescents with ID engaged in approximately 204 min of total after-school SB per day. In detail, they spent approximately 84 mins/d during the after-school period in the screen-based SB. Furthermore, after-school children and adolescents with ID performed about 50 mins/d of recreational SB and 30 mins/d of educational SB, respectively. Additionally, no significant differences were observed in total after-school SB or particular after-school SB for children and adolescents with ID by gender, weight status, and level of ID (p > 0.05). An exception, however, was seen during the after-school period where the youngest-aged (6–12 years old) group engaged more time in recreational SB than the oldest-aged (16–18 years old) group (p < 0.05).
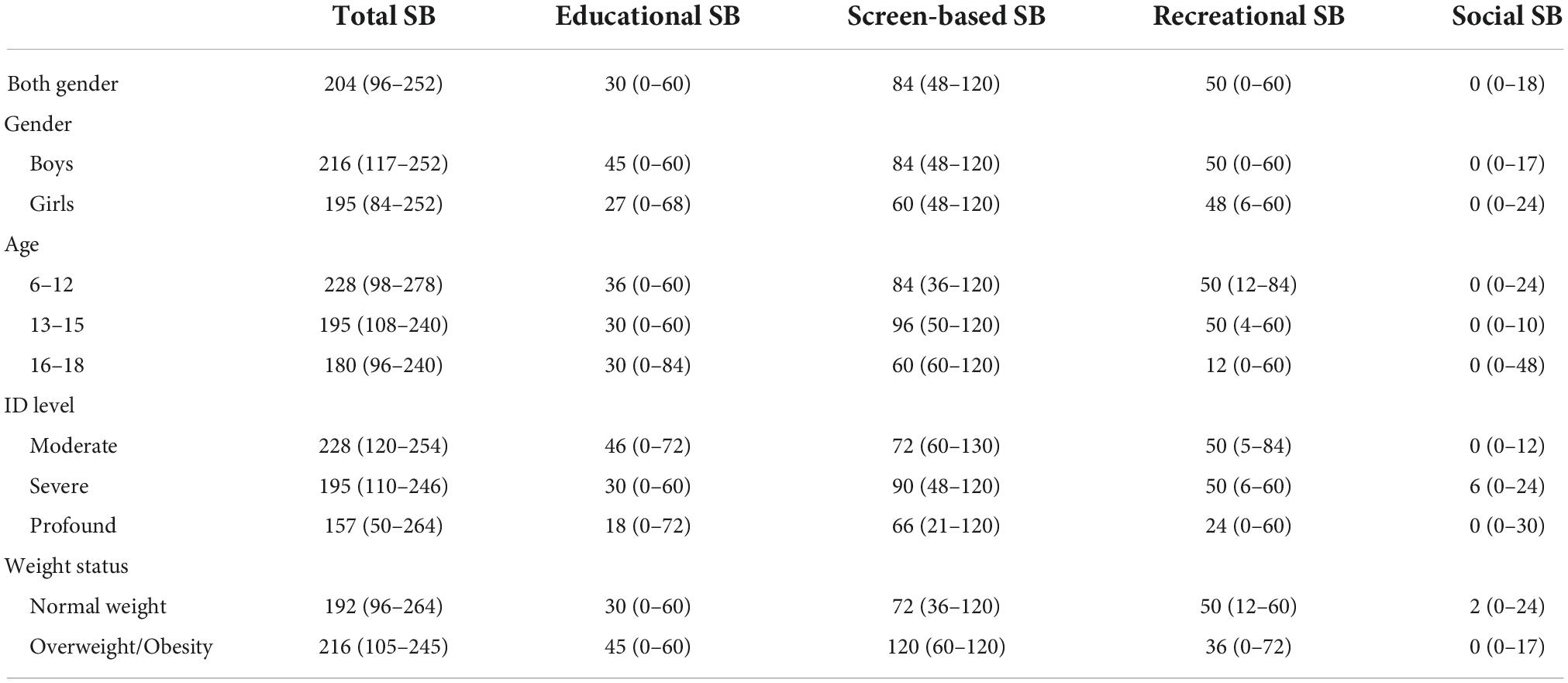
Table 1. Daily minutes of total after-school SB and specific types of after-school SB among children and adolescents with ID [M (P25–P75), min/days].
Table 2 displays the detailed prevalence estimates of screen-based SB during the after-school period by gender, age, weight status, and ID level of children and adolescents with ID. Overall, 37.5% of them achieved the 2-h-maximum screen-based SB time limited in the guideline during the after-school time. No statistically significant differences were found in the prevalence estimates of screen-based SB by gender, age, weight status, and ID level during the after-school period from the logistic regression model results (Table 3).
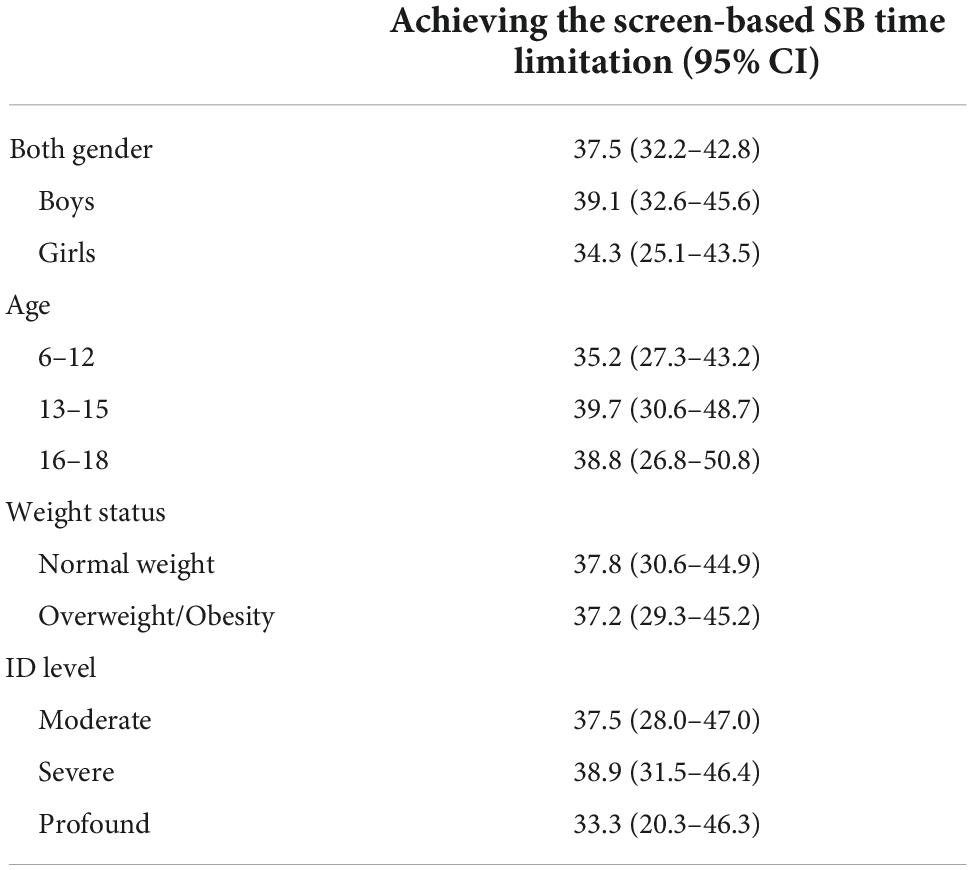
Table 2. Prevalence estimates of after-school screen-based SB time limitation among children and adolescents with ID by gender, age, weight status, and ID level.
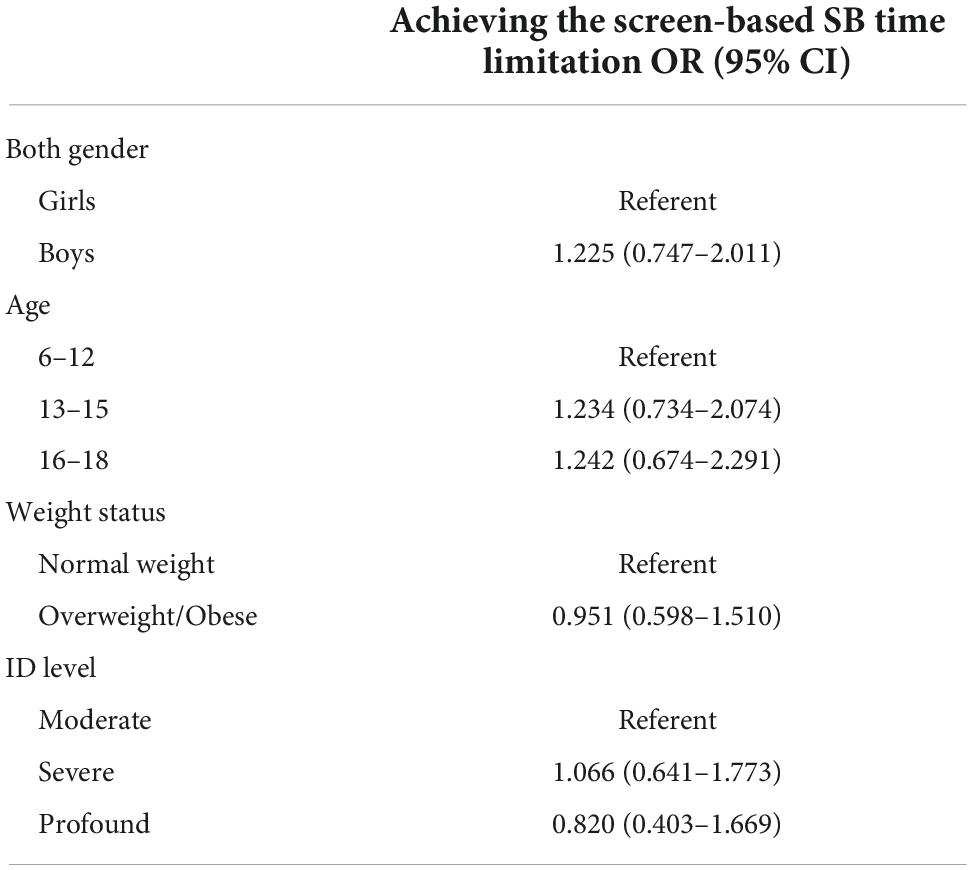
Table 3. Differences in prevalence of achieving the after-school screen-based SB time limitation among children and adolescents with ID by gender, age, weight status, and ID level.
Discussion
This study described the overall level and specific pattern of the after-school SB in children and adolescents with ID, derived from parent-reported data. Based on the daily routine of school days, we deduce that children and adolescents with ID leave school at 4:00 p.m. and sleep at 10:00 p.m. After removing approximately 1 h of time needed to get home and have dinner, there are approximately 5 h left during this period. The results of this study indicated that during the after-school time, present children and adolescents with ID had 204 mins/d of SB, which was equivalent to 3.4 h every day. Excessive after-school SB is a serious problem for children and adolescents with ID. It was evident that they spent approximately 70% of their after-school time in SB, which was relatively higher than the findings of Arundell et al.’s systematic review focused on after-school SB among typically developing (TD) children and adolescents (15). Arundell et al.’s study revealed that TD children spent between 41 and 51% of the after-school period sedentary, and TD adolescents engaged 57% of the after-school time in SB (15). The earlier reports of poor health conditions associated with SB in children and adolescents with ID may explain part of the higher level of their after-school SB (11, 12). However, it is hard to confidently conclude whether the after-school SB of children and adolescents with ID differs from TD peers due to the fact that difference in the after-school period definitions and the measurement tools between the present study and the systematic review study. Additionally, existing data focusing on the overall SB level appear conflicting in the literature. Foley et al., Whitt–Glover et al., and Pitchford et al. concluded that no significant difference was found in the overall SB between children and adolescents with ID and TD peers (17, 23, 24). In contrast, a study from Poland based on a large sample showed that children and adolescents with ID had significantly longer SB than their counterparts (25). The reasons for this may be related to the choice of SB measurement tools, the size and type of sample with ID, and the use of SB cut-off points between studies. Therefore, caution is needed when making comparisons across different studies.
A key finding of this study was that screen-based SB was the most common form of after-school SB for children and adolescents with ID. The results found that the amount of time spent on screen-based SB after school was approximately 84 mins/day, which made up 41.2% of the total after-school SB level. This finding is similar to that reported in a previous study by Foley et al. In Foley et al.’s study, children with ID spent the majority of their after-school time watching television and computers for a combined 82 ± 64 mins/d (17). The findings of Adelantado–Renau et al. (26) highlighted that screen-based SB was the most prevalent behavior for TD children and adolescents in their daily lives. According to the review study by Carson et al., prolonged screen-based SB time was linked with adverse health effects (1). In detail, higher screen time/frequency was associated with unfavorable body composition, lower fitness performance, lower self-esteem, and higher risk of clustered cardiometabolism (1). A gradient was also observed across the different health indicators, showing that less SB, particularly screen time, was related to better health (1). In addition to the screen-based SB, the present study found that the recreational and educational SB comprise 39.2% of the total after-school SB level. Of note, it is possible several of these particular SB occur concurrently during the after-school period. For example, some learning and leisure activities are screen-based devices, such as reading books on pads, doing homework on the computer, listening to music on phones, and drawing pictures on the laptop. Therefore, screen-based devices usage should be limited, except for essential learning or leisure activities during the after-school period. It is also recommended to choose non-screen learning and entertainment activities instead of screen-based learning and entertainment activities. Moreover, from the point of view of the type of after-school SB, although the time accumulation and energy expenditure of SB are similar between educational SB and recreational SB, there may be specificity in the determinants and biological effects of health consequences of positive and negative SB. It is therefore challenging to effectively distinguish between different particular SB pattern and their health benefits in future studies.
In the present study, one unanticipated finding was that children and adolescents with ID in the youngest-age group engaged in more recreational SB compared to those in the oldest-age group during the after-school period, which indicated that there might be different after-school SB patterns among children and adolescents with different age ranges. This result, therefore, needs to be interpreted with some caution because the sample size across age groups in this study was uneven, as well as investigating SB status only during the after-school period. In addition, it is clear that the evidence from the present stage of the study does not establish whether age is an influential factor in the SB of children and adolescents with ID. Esposito et al. highlighted that the time of SB per week for adolescents with ID usually increased with age (11). One study from Japan also noted that children with ID aged 11–12 years old engaged significantly more time in SB than those aged 7–8 years old (27). However, Foerste et al.’s study outlined that there was no correlation between SB and age in adolescents with ID (28). It is worthy to mention that the above-mentioned studies recruited samples with Down’s syndrome (DS). Phillips and Holland found that individuals with DS are significantly more sedentary than those with ID without DS. Furthermore, it has been noted that individuals with DS engaged in lower PA and fitness levels, leading to cardiac chronotropic incompetence, impaired autonomic function, low muscular strength, and muscle hypotonia compared to individuals with ID without DS (12). Therefore, more research is needed to provide an in-depth analysis of the relationship between age factors and SB level/specific SB pattern at different periods of the day (e.g., at school or after school) based on a clear sampling (e.g., recruitment of samples with ID without DS or samples with ID only) type.
Several theories have been applied to facilitate the investigation of behaviors and their correlates. The ecological model theory suggests that behavior is influenced by intrapersonal factors as well as social/cultural and physical/policy environment (29). In this study, personal, family, and environmental factors could contribute to excessive after-school SB among children and adolescents with ID. As far as personal factors are concerned, on the one hand, children and adolescents with ID may have skeletal development and motor development issues that limit their activities (30). On the other hand, because of their cognitive deficits, they have difficulty recognizing the adverse health effects of SB and planning/organizing their after-school activities. Furthermore, a lack of interest in sports activities and social difficulties may also be factors contributing to higher levels of after-school SB among children and adolescents with ID. Regarding family factors, Izquierdo–Gomez et al.’s pointed out that the mother’s education, work status, and socio-economic status were associated with total SB time and watching TV time among adolescents with DS (31). Additionally, overprotective or worried parents could restrict their children’s range of activities or deny them the opportunity to participate in sports activities, making them more anxious and vulnerable (30). Therefore, parents’ understanding of the harmful effects of SB and their behavioral habits may influence their children’s behavior. To reduce the after-school SB of children and adolescents with ID, parents’ awareness of the value of after-school sports activities should be raised, their role in the healthy development of their children should be clearly defined, and their role as role models should be fully explored. The environment in the community and the facilities at home can also impact the after-school SB of children and adolescents with ID. According to Izquierdo–Gomez et al.’s study, total SB levels were positively correlated with the number of bedrooms, the presence of a garden, and a walkable neighborhood (31), which give direction to the identification of factors relevant for family or community-based interventions. Hence, in summary, children and adolescents with ID may experience high levels of after-school SB because of a combination of individual, family, and environmental factors.
One situation that cannot be ignored is that children and adolescents with ID spend half of their waking hours at school on weekdays. Traditionally, the classroom environment has been related to children and adolescents with ID spending long periods of time sitting. Consequently, the after-school period represents a vital part of the day for them. In general, they are not restricted by school schedules after school, and they may have some choices between active and sedentary options during these discretionary periods of the day. Furthermore, after-school SB may also contribute to daily SB level and affect the health of children and adolescents with ID. Hence, the targeted period-specific interventions given may be effective. For example, outdoor plays may provide a feasible opportunity for children and adolescents with ID to take some exercise or participate in sports activities and subsequently reduce SB during the after-school period. Also, Robinson et al. offered after-school dance classes to TD children, which had been shown to successfully reduce their screen-based SB (32). These directed at after-school interventions may be adapted to children and adolescents with ID and have the potential to change their after-school SB status. Further, two previous studies took different approaches to intervene on SB status in children and adolescents with DS or ID at the community level and school level, respectively. Ulrich et al. conducted a 7-week bicycle intervention for children and adolescents with DS in the community setting, with the results indicating that children and adolescents with DS who learned to ride engaged significantly less time in SB compared to their peers in the control group (33). A study from Hong Kong, China examined the effectiveness of active video games intervention strategy on PA level, motor proficiency, and body composition. The result of the study showed that, compared to the control group, children with ID in the intervention group had a decrease in SB after a 12-week intervention (34). However, the long-term effectiveness of these interventions in reducing SB and whether they are also applicable to the period after school need to be further investigated.
There are some limitations to this study. First, data were collected from special education schools in the fall semester. Previous studies showed that children were found to be more sedentary in the winter than in the spring or summer (35, 36). Therefore, this surveillance data may only represent after-school SB at a specific period of the year and may not be generalizable throughout the entire school year due to the after-school SB may be associated with the seasonal variation. Second, the convenience sample used from northern China may not be representative of the entire children and adolescents with ID in China. Additionally, the unbalanced sample size of each ID severity may have some influence on the interpretation of the results of the present study. Thus, a more complete sampling strategy is necessary for future research. Third, due to the cross-sectional study’s design, no causal relationship can be established. Therefore, in order to clarify and understand the trend and patterns of change in after-school SB over time, this requires future prospective analysis in further large longitudinal studies focusing on investigating the prevalences, trajectories, and determining factors of the after-school SB. Finally, notwithstanding these limitations, this investigation provides invaluable information to understand the pattern and distribution of after-school SB among children and adolescents with ID.
Conclusion
Overall, the findings of this study highlighted that children and adolescents with ID spent a high level of SB during the after-school period. Among varieties of types of after-school SB, children and adolescents with ID particularly engaged in more time on after-school screen-based SB. A certain number of them exceeded the 2-h-maximum limit for screen-based SB time during the after-school period. Thus, it is necessary to implement period-specific strategies to reduce SB among the vulnerable population.
Data availability statement
The data are not publicly available due to privacy or ethical restrictions. Requests to access these datasets should be directed to YY, Y3J5c3RhbF8yNjdAMTYzLmNvbQ==.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethical Committee of Shandong Sport University, China. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
YL and JL contributed to conception and design of the study. CW and JD organized the database. SZ and YW performed the statistical analysis. YY and YL wrote the first draft of the manuscript. JD wrote sections of the manuscript. All authors contributed to manuscript revision and read and approved the submitted version.
Funding
This research was funded by the MOE (Ministry of Education in China) Project of Humanities and Social Sciences (No. 18YJC890026), Shandong Social Science Planning Project (Nos. 18CQXJ47 and 19CQXJ30), and Shandong Province Soft Sciences Research Plan Project (No. 2022RKY04009).
Acknowledgments
We would like to express our sincere appreciation to all special education schools from Shandong Province for their cooperation and contributions. We are also grateful to the parents and their children who participated in this study, and we wish them the best of luck.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Carson V, Hunter S, Kuzik N, Gray CE, Poitras VJ, Chaput JP, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Physiol Nutr Metab. (2016) 41:S240–65. doi: 10.1139/apnm-2015-0630
2. Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE, et al. Sedentary behavior research network (SBRN) - terminology consensus project process and outcome. Int J Behav Nutr Phys Act. (2017) 14:75. doi: 10.1186/s12966-017-0525-8
3. Tremblay MS, LeBlanc AG, Kho ME, Saunders TJ, Larouche R, Colley RC, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act. (2011) 8:98. doi: 10.1186/1479-5868-8-98
4. Gunnell KE, Flament MF, Buchholz A, Henderson KA, Obeid N, Schubert N, et al. Examining the bidirectional relationship between physical activity, screen time, and symptoms of anxiety and depression over time during adolescence. Prev Med. (2016) 88:147–52. doi: 10.1016/j.ypmed.2016.04.002
5. de Rezende LFM, Lopes MR, Rey-Lopez JP, Matsudo VKR, Luiz OD. Sedentary behavior and health outcomes: an overview of systematic reviews. PLoS One. (2014) 9:e105620. doi: 10.1371/journal.pone.0105620
6. Cooper AR, Goodman A, Page AS, Sherar LB, Esliger DW, van Sluijs EMF, et al. Objectively measured physical activity and sedentary time in youth: the international children’s accelerometry database (ICAD). Int J Behav Nutr Phys Act. (2015) 12:113. doi: 10.1186/s12966-015-0274-5
7. Colley RC, Garriguet D, Janssen I, Craig CL, Clarke J, Tremblay MS. Physical activity of Canadian children and youth: accelerometer results from the 2007 to 2009 Canadian health measures survey. Health Rep. (2011) 22:15–23.
8. Matthews CE, Chen KY, Freedson PS, Buchowski MS, Beech BM, Pate RR, et al. Amount of time spent in sedentary behaviors in the united states, 2003-2004. Am J Epidemiol. (2008) 167:875–81. doi: 10.1093/aje/kwm390
9. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World health organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
10. Tremblay MS, Rollo S, Saunders TJ. Sedentary behavior research network members support new Canadian 24-hour movement guideline recommendations. J Sport Health Sci. (2020) 9:479–81. doi: 10.1016/j.jshs.2020.09.012
11. Esposito PE, MacDonald M, Hornyak JE, Ulrich DA. Physical activity patterns of youth with down syndrome. Intellect Dev Disabil. (2012) 50:109–19. doi: 10.1352/1934-9556-50.2.109
12. Phillips AC, Holland AJ. Assessment of objectively measured physical activity levels in individuals with intellectual disabilities with and without down’s syndrome. PLoS One. (2011) 6:e28618. doi: 10.1371/journal.pone.0028618
13. Izquierdo–Gomez R, Martinez-Gomez D, Acha A, Veiga OL, Villagra A, Diaz-Cueto M, et al. Objective assessment of sedentary time and physical activity throughout the week in adolescents with Down syndrome. The UP&DOWN study. Res Dev Disabil. (2014) 35:482–9. doi: 10.1016/j.ridd.2013.11.026
14. McKenzie K, Ouellette-Kuntz H, Martin L. Applying a general measure of frailty to assess the aging related needs of adults with intellectual and developmental disabilities. J Policy Pract Intellect Disabil. (2017) 14:124–8. doi: 10.1111/jppi.12197
15. Arundell L, Fletcher E, Salmon J, Veitch J, Hinkley T. A systematic review of the prevalence of sedentary behavior during the after-school period among children aged 5-18 years. Int J Behav Nutr Phys Act. (2016) 13:93. doi: 10.1186/s12966-016-0419-1
16. Wickel EE, Issartel J, Belton S. Longitudinal change in active and sedentary behavior during the after-school hours. J Phys Act Health. (2013) 10:416–22. doi: 10.1123/jpah.10.3.416
17. Foley JT, McCubbin JA. An exploratory study of after-school sedentary behaviour in elementary school-age children with intellectual disability. J Intellect Dev Disabil. (2009) 34:3–9. doi: 10.1080/13668250802688314
18. China Disabled Persons’ Federation. Working Manual for the Second National Sampling Survey on Disabled. Beijing: China Disabled Persons’ Federation (2006).
19. Ministry of Education of the People’s Republic of China. Education law of the People’s Republic of China. (2018). Available online at: http://en.moe.gov.cn/Resources/Laws_and_Policies/201506/t20150626_191385.html (accessed September 14, 2018).
20. Shandong Provincial Education Department. The List of Special Education Schools. (2020). Available online at: http://edu.shandong.gov.cn/art/2020/6/1/art_107104_8156093.html (accessed June 1, 2020).
21. Li HY, Chen PJ, Zhuang J. Revision and reliability validity assessment of children’s leisure activities study survey. Chin J Sch Health. (2011) 32:268–70.
22. Burdette HL, Whitaker RC, Daniels SR. Parental report of outdoor playtime as a measure of physical activity in preschool-aged children. Arch Pediatr Adolesc Med. (2004) 158:353–7. doi: 10.1001/archpedi.158.4.353
23. Whitt–Glover MC, O’Neill KL, Stettler N. Physical activity patterns in children with and without down syndrome. Pediatr Rehabil. (2006) 9:158–64. doi: 10.1080/13638490500353202
24. Pitchford EA, Adkins C, Hasson RE, Hornyak JE, Ulrich DA. Association between physical activity and adiposity in adolescents with down syndrome. Med Sci Sports Exerc. (2018) 50:667–74. doi: 10.1249/MSS.0000000000001502
25. Wyszynska J, Podgorska-Bednarz J, Deren K, Mazur A. The relationship between physical activity and screen time with the risk of hypertension in children and adolescents with intellectual disability. Biomed Res Int. (2017) 2017:1940602. doi: 10.1155/2017/1940602
26. Adelantado–Renau M, Moliner-Urdiales D, Cavero-Redondo I, Beltran-Valls MR, Martínez-Vizcaíno V, Álvarez-Bueno C. Association between screen media use and academic performance among children and adolescents: a systematic review and meta-analysis. JAMA Pediatr. (2019) 173:1058–67. doi: 10.1001/jamapediatrics.2019.3176
27. Yamanaka E, Inayama T, Ohkawara K, Okazaki K, Kita I. The association between obesity and sedentary behavior or daily physical activity among children with down’s syndrome aged 7-12 years in Japan: a cross-sectional study. Heliyon. (2020) 6:e04861. doi: 10.1016/j.heliyon.2020.e04861
28. Foerste T, Sabin M, Reid S, Reddihough D. Understanding the causes of obesity in children with trisomy 21: hyperphagia vs physical inactivity. J Intellect Disabil Res. (2016) 60:856–64. doi: 10.1111/jir.12259
29. Bronfenbrenner U. Ecology of the family as a context for human development. Am Psychol. (1986) 52:513–31.
30. Liu Y, Yuan YQ, Wang MJ. Advance in physical activity of children and adolescents with intellectual disabilities. Chin J Rehabil Theory Pract. (2020) 26:197–203.
31. Izquierdo-Gomez R, Veiga OL, Sanz A, Fernhall B, Diaz-Cueto M, Villagra A, et al. Correlates of objectively measured physical activity in adolescents with down syndrome: the UP & DOWN Study. Nutr Hosp. (2015) 31:2606–17.
32. Robinson TN, Killen JD, Kraemer HC, Wilson DM, Matheson DM, Haskell WL, et al. Dance and reducing television viewing to prevent weight gain in African-American girls: the Stanford GEMS pilot study. Ethn Dis. (2003) 13:S65–77.
33. Ulrich DA, Burghardt AR, Lloyd M, Tiernan C, Hornyak JE. Physical activity benefits of learning to ride a two-wheel bicycle for children with down syndrome: a randomized trial. Phys Ther. (2011) 91:1463–77. doi: 10.2522/ptj.20110061
34. Lau PW, Wang G, Wang JJ. Effectiveness of active video game usage on body composition, physical activity level and motor proficiency in children with intellectual disability. J Appl Res Intellect Disabil. (2020) 33:1465–77. doi: 10.1111/jar.12774
35. Gracia-Marco L, Ortega FB, Ruiz JR, Williams CA, Hagstromer M, Manios Y, et al. Seasonal variation in physical activity and sedentary time in different European regions. The HELENA study. J Sports Sci. (2013) 31:1831–40. doi: 10.1080/02640414.2013.803595
36. Hjorth MF, Chaput JP, Michaelsen K, Astrup A, Tetens I, Sjodin A. Seasonal variation in objectively measured physical activity, sedentary time, cardio-respiratory fitness and sleep duration among 8-11 year-old Danish children: a repeated-measures study. BMC Public Health. (2013) 13:808. doi: 10.1186/1471-2458-13-808
Keywords: after-school, sedentary behavior, intellectual disabilities, children and adolescents, health promotion (HP)
Citation: Yuan YQ, Ding JN, Wang C, Zhang SH, Wang YP, Liu Y and Liu JM (2022) The after-school sedentary behavior status among children and adolescents with intellectual disabilities. Front. Psychiatry 13:1049180. doi: 10.3389/fpsyt.2022.1049180
Received: 20 September 2022; Accepted: 17 November 2022;
Published: 01 December 2022.
Edited by:
Huixuan Zhou, Beijing Sport University, ChinaReviewed by:
Shao Tianyi, Zhejiang Normal University, ChinaMa Liang, China Women’s University, China
Copyright © 2022 Yuan, Ding, Wang, Zhang, Wang, Liu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yang Liu, bGl1eWFuZzE5QHNkanp1LmVkdS5jbg==; Jingmin Liu, bGptX3RoQHRzaW5naHVhLmVkdS5jbg==
†These authors share first authorship