 Kun Li
Kun Li Jiang Long1†
Jiang Long1† Wei Deng
Wei Deng Bochao Cheng
Bochao Cheng Jiaojian Wang
Jiaojian Wang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 09 November 2022
Sec. Psychopharmacology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.1040443
This article is part of the Research Topic The Pros and Cons of Psychotropic Drug-Induced Changes in Periphery and Central Nervous System: Elucidating Structural and Molecular Mechanisms View all 8 articles
Background: Chronic mental diseases such as obsessive-compulsive disorder (OCD) are associated with a high disability rate. Some patients still do not improve their symptoms even with adequate cognitive-behavioral therapy and drug treatment. In the treatment of OCD, electroconvulsive therapy (ECT) is not considered a neuromodulation modality with sufficient evidence.
Objective: This retrospective study aimed to determine the efficacy and associated risk factors of ECT in OCD patients.
Materials and methods: The study included 21 OCD patients who underwent ECT at a high-volume center in China between January 2009 and December 2020. The demographics and clinical characteristics of the patients were assessed using descriptive statistics. Based on Clinical Global Impressions–Improvement scale, patients were categorized into response and non-response groups. Clinical and demographic characteristics of two groups of patients were compared.
Results: An analysis of 21 patients was conducted. In total, 12 patients (57.1%) responded to ECT, 11 patients (52.4%) reported side effects, and an average of 7 ECT sessions were administered. In terms of demographic, there was no statistically significant difference between the two groups. It is noteworthy that the non-response group reported more depression and schizophrenia related disorders comorbidities than the response group (χ2 = 6.252, P = 0.041).
Conclusion: The effectiveness of ECT in treating OCD is limited, especially in patients with refractory symptoms. Comorbidity with other mental disorders may affect the efficacy of ECT.
It is a chronic and disabling mental illness called obsessive-compulsive disorder (OCD). Obsessions and compulsions are the most prominent symptoms. In the general population, lifetime prevalence is 2.3%, and 12-month prevalence is 1.2% (1). Further, OCD prevalence in China is 1.63% over a 12-month period, with significant economic and social burden (2). Compared to the general population, all-cause mortality is twice as high, and comorbid other psychiatric disorders can further increase the risk (3). Estimates suggest that up to 90% of individuals with OCD have a comorbid psychiatric disorder (4, 5).
Cognitive-behavioral therapy and serotonin reuptake inhibitors (SRIs) are recommended as first-line treatments for OCD by various treatment guidelines and expert consensus (6–8). It is estimated that about 40–60% of people with OCD do not achieve satisfactory results in spite of the availability of a variety of treatment options (9). It may be due to intolerable side effects of the drug, unsatisfactory efficacy, poor compliance, treatment resistance, and comorbidity (10–13). A neurosurgical technique known as deep brain stimulation by FDA approved can be used to treat refractory OCD (14). However, its cost, availability, and intrusiveness have severely limited its use. It is therefore urgent to find alternative treatment strategies.
Electroconvulsive therapy (ECT) is a technique used to treat mental illnesses by applying electrical current through the brain. There is ample clinical evidence that ECT is mainly used in major depressive disorder (MDD), bipolar disorder, schizophrenia (15–18). However, Current guidelines do not include ECT as an alternative treatment for refractory OCD (6). The primary cause is an absence of sufficient evidence-based data (11, 19). Recent years have seen an increase in interest in ECT as a treatment for OCD. A systematic review included 265 patients and found reported a response rate of 60.4% (20). However, there were mainly case reports, no RCT test, and a small number of observational studies. As a result, clinical evidence regarding the use of ECT in OCD needs to be provided.
As a result, this retrospective study aimed to investigate ECT’s response rate among OCD patients and examine features associated with the response of OCD to ECT.
This study included patients who received ECT therapy at West China Hospital of Sichuan University between January 2009 and December 2020. The OCD patients were included if they met the criteria outlined in the International Classification of Diseases, Tenth Revision (ICD-10) for the diagnosis. We analyzed only the first ECT series of patients who received more than one treatment series. Consequently, 21 OCD patients were included in the study.
In accordance with the Declaration of Helsinki, it was approved by the Ethics Committee on Biomedical Research of West China Hospital of Sichuan University. Informed consent was not required for this study since it was exempt from institutional review.
The ECT was performed with Thymatron System IV (SOMATICS, LLC). As part of our study, we collected data on ECT treatments, including the number of treatments and electrode placement. Whether or not ECT was required and the ECT protocol was determined by the clinical psychiatrist according to the patient’s condition. The diagnosis, treatment options, and risks and benefits of ECT were explained to patients and their legal guardians and informed consent was obtained prior to the start of ECT.
Typically, ECT administration was performed 3 times per week (on alternate days). The electrodes were positioned bilaterally in the temporal region. Under the supervision of an anesthesiologist and psychiatrist, propofol and succinylcholine were given separately for anesthetic and muscle relaxant.
Demographic information was collected, including age, gender, and education level. In this study, we collected clinical factors, such as the age at which OCD onset occurred, the course of illness, comorbidities, and treatment histories. Furthermore, we examined ECT-related characteristics, such as the number of ECT sessions and the reasons for administering ECT.
We evaluated the charts independently by two authors (KL and JL) to determine their response to ECT. There was a consensus reached by reviewing disagreements with the experts (WD). Improvement of OCD were assessed using the Clinical Global Impressions-Improvement scale (CGI-I). On the CGI-I, a response was defined as a score of 1 (very much improved) or 2 (much improved). Patients or psychiatrists will record all side effects reported spontaneously or observed. Records and CGI-side effects scales were used to assess side effects.
All statistical analyses were conducted using SPSS (IBM SPSS, version 25, Chicago, IL, USA). We performed descriptive statistical analyses on all variables, including demographic characteristics, clinical factors, and ECT-related characteristics. Descriptive statistics involves computing means, standard deviations, and frequencies for continuous and categorical variables. Comparisons between groups were made with independent samples t-tests or Mann–Whitney U test for continuous variables. For categorical variables, we used the Chi-square test or Fisher’s exact test. The significance of the results was defined as P values < 0.05.
Twenty-one OCD patients receiving ECT were included in the study. Table 1 provides information about the demographics and clinical characteristics of the 21 participants. The average age was 27.14, the standard deviation was 10.41, the median age was 23, the minimum age was 16, the maximum age was 52. As for education levels, 95.2% of the respondents graduated from middle school or above. There are 11 (52.4%) males and 10 (47.6%) females. Concerning the clinical factors, the mean Course of illness was 82.00 ± 73.10 years, and the age of OCD onset was 20.82 ± 8.07 years. As far as comorbid conditions are concerned, 7 patients (33.3%) had comorbid MDD, 2 patients (9.5%) comorbid schizophrenia related disorders, and 12 (57.1%) had no comorbid condition at the time of admission. Of 21 patients, ECT was prescribed for severe OCD symptoms or major depression with suicidality in 4 (19.0%); treatment resistance in 9 (42.9%); catatonia symptoms in 1 (4.8%); psychosis, or agitation in 3 (14.3%). Seventeen (71.4%) patients were treated with adequate dose and time of SRIs. The OCD patients in this category are also called refractory OCD patients. There was a total of 21 ECT sessions, with an average (SD) of 7.00 (2.15) sessions per patient. After the ECT treatment course, the overall response rate was 57.1%. Side effects included headaches and amnesia in 5 patients (23.8%) respectively, while 11 patients (52.4%) did not report any side effects (see Table 1).
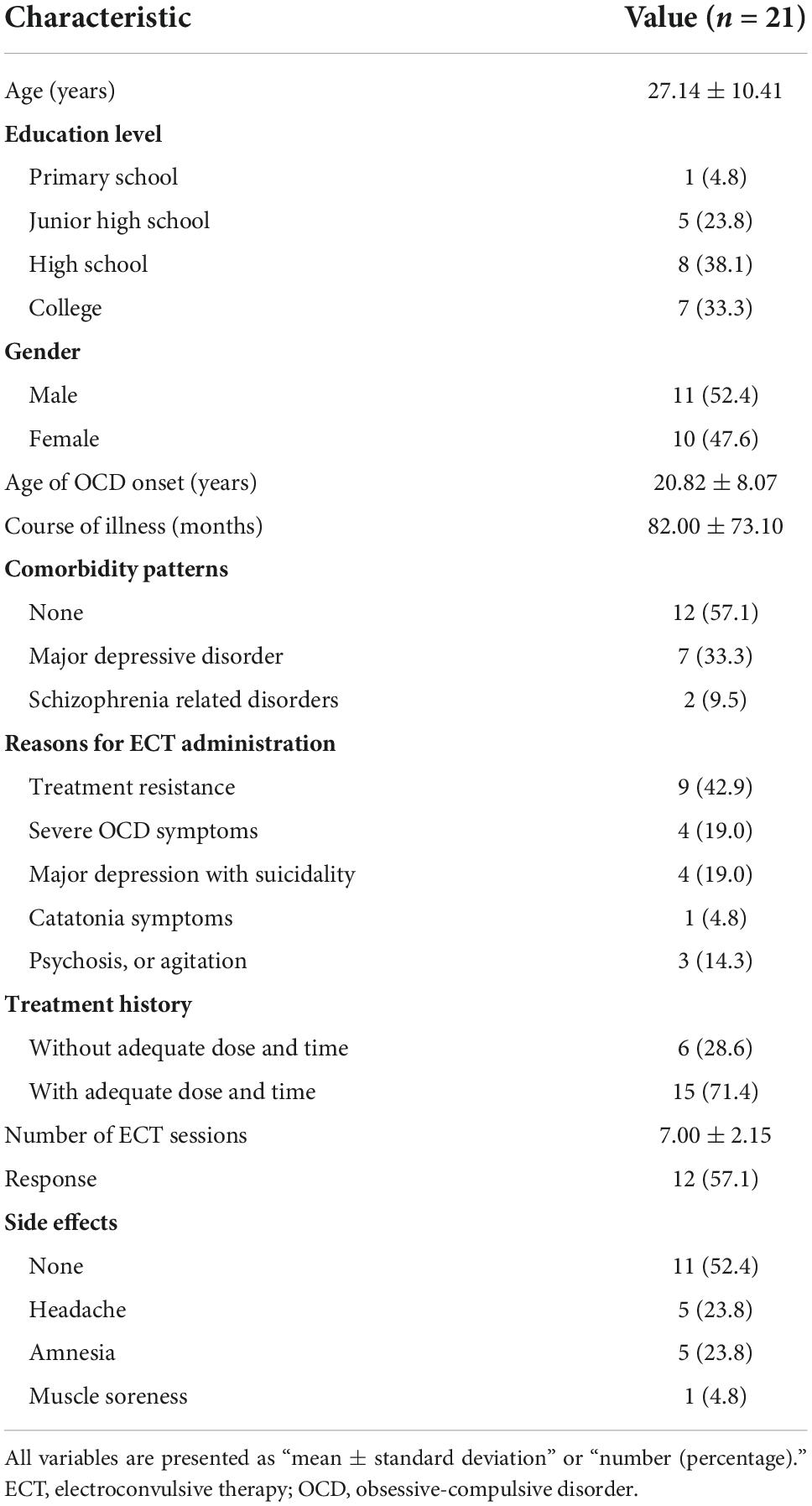
Table 1. Clinical and demographic characteristics.
As shown in Table 2, the demographics and clinical characteristics of the responders and non-responders are compared. There were no significant differences in the demographic and clinical characteristics of the two groups of patients enrolled. In terms of comorbidities, the p value for comparison between the two groups was 0.041 (χ2 = 6.252). In addition, we separately compared the effects of comorbid MDD group with comorbid schizophrenia related disorders group and found no statistically significant difference between the two groups (χ2 = 0.735, P = 1). The comorbidity rate was higher in the non-response group (77.8%) than in the response group (16.7%).
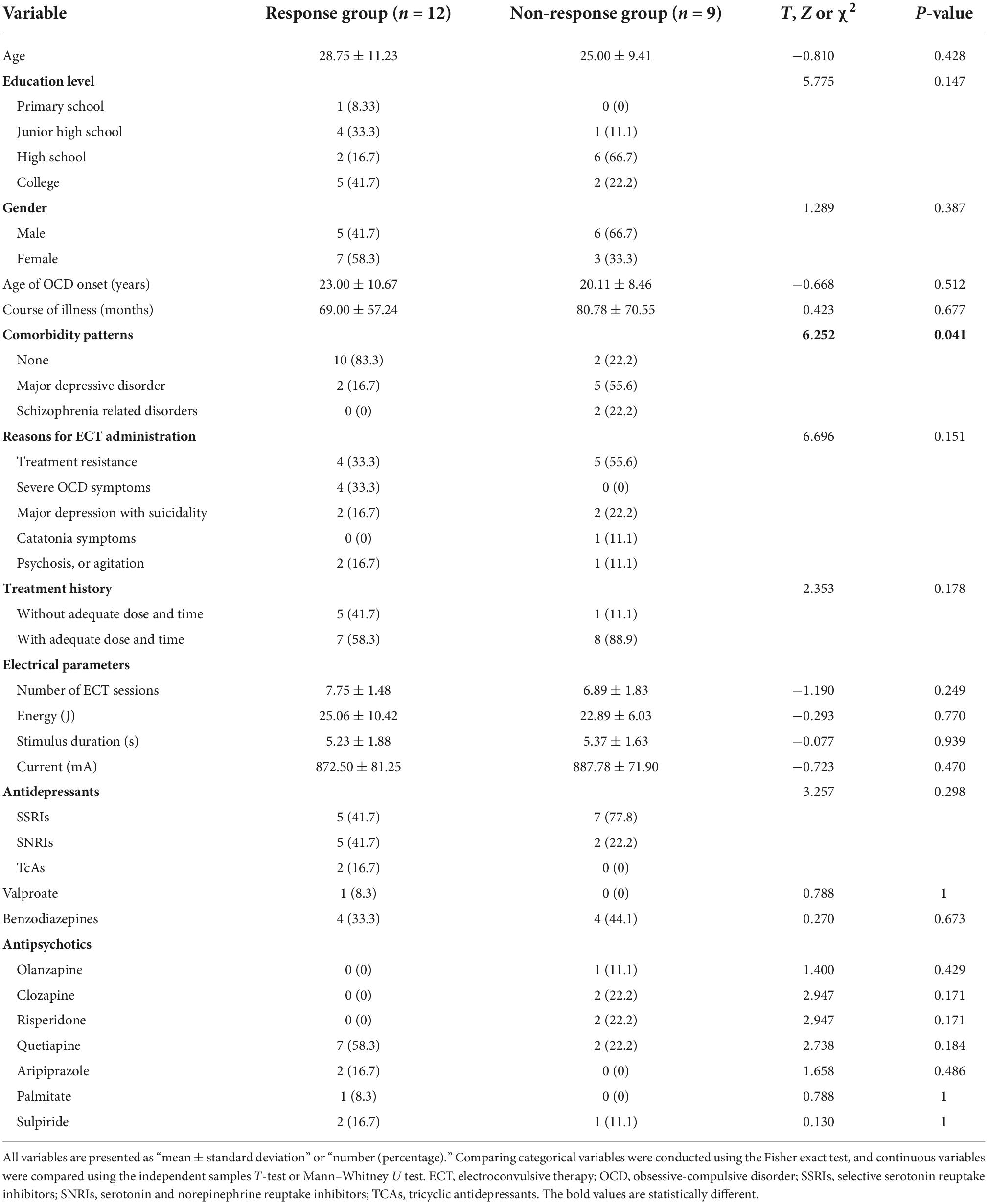
Table 2. Comparison of clinical characteristics between response and non-response groups.
To our knowledge, this is the first cohort of Chinese OCD patients treated with ECT. In this study, the effectiveness of ECT treatment of OCD and the occurrence of side effects were examined and predictors of efficacy were identified. In the total sample, at least 57.1% of patients reported positive responses to ECT. The OCD is frequently comorbid with MDD or schizophrenia-related disorders, with a 33.3 and 9.5% comorbidity rate, respectively. The effectiveness of ECT may be reduced if it is comorbid with other mental disorders, which is notable.
While this study suggests ECT has 57.1% response rate for OCD, patients are highly heterogeneous. The results of this study were similar to previous observational studies in which ECT significantly improved symptoms of OCD in most patients (21). It might be associated with an increase in paroxetine binding sites in the frontal cortex caused by ECT (22). Furthermore, previous studies have demonstrated that the therapeutic effects of ECT may have been partly related to brain-derived neurotrophic factor (23) and neuro metabolites (13). There were 21 patients with OCD, and 15 (71.4%) had received adequate dose and time of SRIs. The remaining 6 patients (28%), however, did not receive adequate treatment before ECT and were not classified as OCD patients with refractory symptoms. A systematic review included only 265 patients, with a response rate of 60.4%, but only 52.7% of these patients had been treated with SRIs and 16.9% had received a full dose (20). In clinical practice, ECT may be prematurely administered to some patients. Furthermore, 8 of the non-responders (88.9%) and 7 of the responders (58.3%) had refractory OCD. Due to this, ECT has a certain effect on OCD patients, but it has a less significant effect on refractory patients. The use of ECT has also been associated with significant improvements in refractory OCD in many cases (24–31). A small prospective study also found that ECT had an anti-obsessional effect (32). So, in patients with refractory OCD, ECT remains recommended.
It is interesting to note that 13 (61.9%) patients who received ECT had refractory or severe symptoms, but other patients required ECT for comorbidities of other severe psychiatric symptoms that needed to be addressed. It is noteworthy that patients with OCD who have comorbid MDD or schizophrenia-related disorders were less effective than those without. The results of this study are consistent with previous studies (20). The obsessive-compulsive symptoms changed independently of depressive symptoms (21, 33). The neural circuits of OCD with depression comorbidity differ from those of other depressed patients, according to some studies (34). OCD is markedly different from depression in that it is insensitive to norepinephrine reuptake inhibitors (35). There may be no link between serotonergic function and ECT’s antidepressant properties (36), but it is important to ECT’s anti-obsessive-compulsive effects. The ECT, although effective in depression, seems to affect the hypothalamus, insula (37), and hippocampus (38, 39), but in OCD, it affects the cortico-striato-thalamo-cortical circuits (40–45). The mechanism of action of ECT in treating OCD may be related to the inhibition in the prefrontal cortex (46). Therefore, treating obsessive-compulsive symptoms may be affected by the complex neurologic mechanisms involved in OCD comorbidities. Another factor influencing the efficacy of ECT for OCD comorbid depression may be the therapeutic target. A single stimulation target does not provide an optimal plan for individualized treatment, especially for the complex brain network disorders of OCD (43, 47). Future research needs to combine multiple approaches to achieve precise stimulation, such as neuronavigation (48).
Moreover, ECT has been found to be effective in treating both obsessive-compulsive symptoms and depression symptoms (13, 21, 27, 49, 50). It is necessary to conduct studies with larger samples in order to confirm this conclusion. Even in the presence of comorbidities, ECT is still recommended for patients with refractory OCD because of the invasiveness and cost of neurosurgery.
It is also important to note that there are some limitations to this research. Due to the retrospective nature of this study, we were unable to control for various confounding variables. The future will demand large-scale, high-quality randomized controlled studies to fulfill clinical practice requirements. Secondly, statistical power was limited by the small sample, which may explain some of the non-significant findings. Moreover, we lack quantifiable metrics for comorbid symptoms, such as catatonic symptoms (51–53). As the study population was heterogeneous, future research will need to focus specifically on patients who are refractory to treatment for OCD.
As a result of this study, we can conclude that ECT for OCD has limited efficacy, especially in refractory patients. There is a possibility that comorbid MDD or schizophrenia related disorders could adversely affect ECT. Therefore, this study needs to be further verified by a randomized controlled trial involving a large sample size.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee on Biomedical Research of West China Hospital of Sichuan University. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
KL: conceptualization, formal analysis, data curation, and writing – original draft. JL: formal analysis and data curation. BC: data curation, investigation, and methodology. JW: data curation, project administration, supervision, and writing – review and editing. WD: conceptualization, data curation, project administration, supervision, and writing – review and editing. All authors contributed to the article and approved the submitted version.
This work was supported by the Special R&D project for Scientific and Technological support of Biomedicine and Health Industry in Hangzhou (Nos. 2021WJCY194 and 2021WJCY067); the Clinical medical expert team introduction project in Suzhou (No. SZYJTD201715); the Key Research and Development of Sichuan Science and Technology Program (No. 2022YFS0178); and the Key Project for Hangzhou Medical Disciplines.
Our thanks go out to all patients who took part in this study as well as the staff at the West China Hospital’s Information Center for assisting with data retrieval and extraction.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the national comorbidity survey replication. Mol Psychiatry. (2010) 15:53–63. doi: 10.1038/mp.2008.94
2. Huang Y, Wang Y, Wang H, Liu Z, Yu X, Yan J, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. (2019) 6:211–24. doi: 10.1016/s2215-0366(18)30511-x
3. Meier SM, Mattheisen M, Mors O, Schendel DE, Mortensen PB, Plessen KJ. Mortality among persons with obsessive-compulsive disorder in Denmark. JAMA Psychiatry. (2016) 73:268–74. doi: 10.1001/jamapsychiatry.2015.3105
4. Ma X, Li R. Case report: effect of electroconvulsive therapy on obsessive-compulsive disorder comorbid with body dysmorphic disorder. Front Psychiatry. (2021) 12:706506. doi: 10.3389/fpsyt.2021.706506
5. LaSalle VH, Cromer KR, Nelson KN, Kazuba D, Justement L, Murphy DL. Diagnostic interview assessed neuropsychiatric disorder comorbidity in 334 individuals with obsessive-compulsive disorder. Depress Anxiety. (2004) 19:163–73. doi: 10.1002/da.20009
6. Koran LM, Hanna GL, Hollander E, Nestadt G, Simpson HB. Practice guideline for the treatment of patients with obsessive-compulsive disorder. Am J Psychiatry. (2007) 164:5–53.
7. Stein DJ, Koen N, Fineberg N, Fontenelle LF, Matsunaga H, Osser D, et al. A 2012 evidence-based algorithm for the pharmacotherapy for obsessive-compulsive disorder. Curr Psychiatry Rep. (2012) 14:211–9. doi: 10.1007/s11920-012-0268-9
8. Beaulieu AM, Tabasky E, Osser DN. The psychopharmacology algorithm project at the harvard south shore program: an algorithm for adults with obsessive-compulsive disorder. Psychiatry Res. (2019) 281:112583. doi: 10.1016/j.psychres.2019.112583
9. Pallanti S, Quercioli L. Treatment-refractory obsessive-compulsive disorder: methodological issues, operational definitions and therapeutic lines. Prog Neuropsychopharmacol Biol Psychiatry. (2006) 30:400–12. doi: 10.1016/j.pnpbp.2005.11.028
10. Simpson HB, Huppert JD, Petkova E, Foa EB, Liebowitz MR. Response Versus Remission in Obsessive-Compulsive Disorder. J Clin Psychiatry. (2006) 67:269–76. doi: 10.4088/jcp.v67n0214
11. Rapinesi C, Kotzalidis GD, Ferracuti S, Sani G, Girardi P, Del Casale A. Brain stimulation in obsessive-compulsive disorder (OCD): a systematic review. Curr Neuropharmacol. (2019) 17:787–807. doi: 10.2174/1570159x17666190409142555
12. Rozenman M, Piacentini J, O’Neill J, Bergman RL, Chang S, Peris TS. Improvement in anxiety and depression symptoms following cognitive behavior therapy for pediatric obsessive compulsive disorder. Psychiatry Res. (2019) 276:115–23. doi: 10.1016/j.psychres.2019.04.021
13. Liu D, Liang R, Bai S, Lan B, Liu G, Wang D, et al. Effect of modified electroconvulsive therapy on neuro metabolites and magnetic resonance spectroscopy imaging signals in patients with refractory obsessive-compulsive disorder. J Affect Disord. (2022) 296:616–21. doi: 10.1016/j.jad.2021.10.005
14. Miterko LN, Lin T, Zhou J, van der Heijden ME, Beckinghausen J, White JJ, et al. Neuromodulation of the cerebellum rescues movement in a mouse model of ataxia. Nat Commun. (2021) 12:1295. doi: 10.1038/s41467-021-21417-8
15. Kellner CH, Obbels J, Sienaert P. When to Consider Electroconvulsive Therapy (Ect). Acta Psychiatr Scand. (2020) 141:304–15. doi: 10.1111/acps.13134
16. Liang CS, Chung CH, Ho PS, Tsai CK, Chien WC. Superior anti-suicidal effects of electroconvulsive therapy in unipolar disorder and bipolar depression. Bipolar Disord. (2018) 20:539–46. doi: 10.1111/bdi.12589
17. Li X, Meng H, Fu Y, Du L, Qiu H, Qiu T, et al. The impact of whole brain global functional connectivity density following MECT in major depression: a follow-up study. Front Psychiatry. (2019) 10:7. doi: 10.3389/fpsyt.2019.00007
18. Hu Q, Huang H, Jiang Y, Jiao X, Zhou J, Tang Y, et al. Temporoparietal connectivity within default mode network associates with clinical improvements in schizophrenia following modified electroconvulsive therapy. Frontiers Psychiatry. (2021) 12:768279. doi: 10.3389/fpsyt.2021.768279
19. Acevedo N, Bosanac P, Pikoos T, Rossell S, Castle D. Therapeutic neurostimulation in obsessive-compulsive and related disorders: a systematic review. Brain Sci. (2021) 11:948. doi: 10.3390/brainsci11070948
20. Fontenelle LF, Coutinho ES, Lins-Martins NM, Fitzgerald PB, Fujiwara H, Yücel M. Electroconvulsive therapy for obsessive-compulsive disorder: a systematic review. J Clin Psychiatry. (2015) 76:949–57. doi: 10.4088/JCP.14r09129
21. Maletzky B, McFarland B, Burt A. Refractory obsessive compulsive disorder and ECT. Convuls Ther. (1994) 10:34–42.
22. Hayakawa H, Okamoto Y, Shimizu M, Nishida A, Motohashi N, Yamawaki S. Single or repeated treatment with electroconvulsive shock increases number of serotonin uptake binding sites in the frontal cortex. Neuropsychobiology. (1995) 31:1–5. doi: 10.1159/000119164
23. Li J, Zhang X, Jiang J, Zhang B, Tang Y, Zhang T, et al. Comparison of electroconvulsive therapy and magnetic seizure therapy in schizophrenia: structural changes/neuroplasticity. Psychiatry Res. (2022) 312:114523. doi: 10.1016/j.psychres.2022.114523
24. Mellman LA, Gorman JM. Successful treatment of obsessive-compulsive disorder with ECT. Am J Psychiatry. (1984) 141:596–7. doi: 10.1176/ajp.141.4.596
25. D’Urso G, Mantovani A, Barbarulo AM, Labruna L, Muscettola G. Brain-behavior relationship in a case of successful ECT for drug refractory catatonic OCD. J ECT. (2012) 28:190–3. doi: 10.1097/YCT.0b013e3182542649
26. Raveendranathan D, Srinivasaraju R, Ratheesh A, Math SB, Reddy YC. Treatment-refractory ocd responding to maintenance electroconvulsive therapy. J Neuropsychiatry Clin Neurosci. (2012) 24:E16–7. doi: 10.1176/appi.neuropsych.11060124
27. Liu X, Cui H, Wei Q, Wang Y, Wang K, Wang C, et al. Electroconvulsive therapy on severe obsessive-compulsive disorder comorbid depressive symptoms. Psychiatry Invest. (2014) 11:210–3. doi: 10.4306/pi.2014.11.2.210
28. Manhas RS, Mushtaq R, Tarfarosh SF, Shoib S, Dar MM, Hussain A, et al. An interventional study on the clinical usefulness and outcomes of electroconvulsive therapy in medication-resistant mental disorders. Cureus. (2016) 8:e832. doi: 10.7759/cureus.832
29. Agrawal A, Das S, Thirthalli J. When obsessive compulsive disorder responds only to electroconvulsive therapy: a rare case for maintenance electroconvulsive therapy?. J Neurosci Rural Pract. (2018) 9:450–1. doi: 10.4103/jnrp.jnrp_12_18
30. Saðlam T, Aksoy Poyraz C, Poyraz B, Tosun M. Successful use of electroconvulsive therapy in a patient with anorexia nervosa and severe acute-onset obsessive-compulsive disorder. Int J Eat Disord. (2018) 51:1026–8. doi: 10.1002/eat.22923
31. Martins-Correia J, Rodrigues-Silva N, Nunes S. Electroconvulsive therapy in refractory obsessive-compulsive disorder: a case report. J ECT. (2021) 37:e17–9. doi: 10.1097/yct.0000000000000731
32. Khanna S, Gangadhar BN, Sinha V, Rajendra PN, Channabasavanna SM. Electroconvulsive therapy in obsessive-compulsive disorder. Convuls Ther. (1988) 4:314–20.
33. Lins-Martins NM, Yücel M, Tovar-Moll F, Rodrigues EC, Fontenelle LF. Electroconvulsive therapy in obsessive-compulsive disorder: a chart review and evaluation of its potential therapeutic effects. J Neuropsychiatry Clin Neurosci. (2015) 27:65–8. doi: 10.1176/appi.neuropsych.13080184
34. Fontenelle LF, Harrison BJ, Pujol J, Davey CG, Fornito A, Bora E, et al. Brain functional connectivity during induced sadness in patients with obsessive-compulsive disorder. J Psychiatry Neurosci. (2012) 37:231–40. doi: 10.1503/jpn.110074
35. Hoehn-Saric R, Ninan P, Black DW, Stahl S, Greist JH, Lydiard B, et al. Multicenter double-blind comparison of sertraline and desipramine for concurrent obsessive-compulsive and major depressive disorders. Arch Gen Psychiatry. (2000) 57:76–82. doi: 10.1001/archpsyc.57.1.76
36. Goto S, Terao T, Hoaki N, Wang Y, Tsuchiyama K, Araki Y, et al. Is serotonergic function associated with the antidepressant effects of modified-electroconvulsive therapy?. J Affect Disord. (2012) 136:1062–6. doi: 10.1016/j.jad.2011.11.020
37. Xu J, Wang J, Bai T, Zhang X, Li T, Hu Q, et al. Electroconvulsive therapy induces cortical morphological alterations in major depressive disorder revealed with surface-based morphometry analysis. Int J Neural Syst. (2019) 29:1950005. doi: 10.1142/s0129065719500059
38. Bolwig TG. How does electroconvulsive therapy work? theories on its mechanism. Can J Psychiatry. (2011) 56:13–8. doi: 10.1177/070674371105600104
39. Bai T, Wei Q, Xie W, Wang A, Wang J, Ji GJ, et al. Hippocampal-subregion functional alterations associated with antidepressant effects and cognitive impairments of electroconvulsive therapy. Psychol Med. (2019) 49:1357–64. doi: 10.1017/s0033291718002684
40. Tang W, Zhu Q, Gong X, Zhu C, Wang Y, Chen S. Cortico-striato-thalamo-cortical circuit abnormalities in obsessive-compulsive disorder: a voxel-based morphometric and FMRI study of the whole brain. Behav Brain Res. (2016) 313:17–22. doi: 10.1016/j.bbr.2016.07.004
41. Chen Y, Meng Z, Zhang Z, Zhu Y, Gao R, Cao X, et al. The right thalamic glutamate level correlates with functional connectivity with right dorsal anterior cingulate cortex/middle occipital gyrus in unmedicated obsessive-compulsive disorder: a Combined fMRI and (1)H-MRS study. Aust N Z J Psychiatry. (2019) 53:207–18. doi: 10.1177/0004867418806370
42. Hou JM, Zhao M, Zhang W, Song LH, Wu WJ, Wang J, et al. Resting-state functional connectivity abnormalities in patients with obsessive-compulsive disorder and their healthy first-degree relatives. J Psychiatry Neurosci. (2014) 39:304–11. doi: 10.1503/jpn.130220
43. Li K, Zhang H, Yang Y, Zhu J, Wang B, Shi Y, et al. Abnormal functional network of the thalamic subregions in adult patients with obsessive-compulsive disorder. Behav Brain Res. (2019) 371:111982. doi: 10.1016/j.bbr.2019.111982
44. Yan H, Shan X, Li H, Liu F, Guo W. Abnormal spontaneous neural activity as a potential predictor of early treatment response in patients with obsessive-compulsive disorder. J Affect Disord. (2022) 309:27–36. doi: 10.1016/j.jad.2022.04.125
45. Chen Y, Ou Y, Lv D, Yang R, Li S, Jia C, et al. Altered network homogeneity of the default-mode network in drug-naive obsessive-compulsive disorder. Prog Neuropsychopharmacol Biol Psychiatry. (2019) 93:77–83. doi: 10.1016/j.pnpbp.2019.03.008
46. Nobler MS, Oquendo MA, Kegeles LS, Malone KM, Campbell CC, Sackeim HA, et al. Decreased Regional Brain Metabolism after Ect. Am J Psychiatry. (2001) 158:305–8. doi: 10.1176/appi.ajp.158.2.305
47. Northoff G, Hirjak D, Wolf RC, Magioncalda P, Martino M. All roads lead to the motor cortex: psychomotor mechanisms and their biochemical modulation in psychiatric disorders. Mol Psychiatry. (2021) 26:92–102. doi: 10.1038/s41380-020-0814-5
48. Zhang Z, Zhang H, Xie CM, Zhang M, Shi Y, Song R, et al. Task-related functional magnetic resonance imaging-based neuronavigation for the treatment of depression by individualized repetitive transcranial magnetic stimulation of the visual cortex. Sci China Life Sci. (2021) 64:96–106. doi: 10.1007/s11427-020-1730-5
49. Casey DA, Davis MH. Obsessive-compulsive disorder responsive to electroconvulsive therapy in an elderly woman. South Med J. (1994) 87:862–4. doi: 10.1097/00007611-199408000-00027
50. Chiu CH, Yang WC, Lin CH. Electroconvulsive therapy in treatment-resistant obsessive-compulsive disorder comorbid with major depressive disorder: a series of 3 cases. J ECT. (2020) 36:e34–5. doi: 10.1097/yct.0000000000000660
51. Hirjak D, Thomann PA, Northoff G, Kubera KM, Wolf RC. [German version of the northoff catatonia rating scale (NCRS-dv) : a validated instrument for measuring catatonic symptoms]. Der Nervenarzt. (2017) 88:787–96. doi: 10.1007/s00115-016-0136-7
52. Northoff G, Koch A, Wenke J, Eckert J, Böker H, Pflug B, et al. Catatonia as a psychomotor syndrome: a rating scale and extrapyramidal motor symptoms. Move Disord. (1999) 14:404–16. doi: 10.1002/1531-8257(199905)14:33.0.co;2-5
Keywords: obsessive-compulsive disorder, electroconvulsive therapy, efficacy, comorbidity, refractory
Citation: Li K, Long J, Deng W, Cheng B and Wang J (2022) Electroconvulsive therapy for obsessive-compulsive disorder: A retrospective study. Front. Psychiatry 13:1040443. doi: 10.3389/fpsyt.2022.1040443
Received: 09 September 2022; Accepted: 21 October 2022;
Published: 09 November 2022.
Edited by:
Wenbin Guo, Central South University, ChinaReviewed by:
Georg Northoff, University of Ottawa, CanadaCopyright © 2022 Li, Long, Deng, Cheng and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wei Deng, ZGVuZ3dAemp1LmVkdS5jbg==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.