
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Psychiatry, 30 November 2022
Sec. Addictive Disorders
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.1031067
This article is part of the Research TopicNovel Treatment Approaches and Future Directions in Substance Use DisordersView all 21 articles
 Emily Karsinti1,2,3,4*
Emily Karsinti1,2,3,4* Florence Vorspan2,3,4,5
Florence Vorspan2,3,4,5 Norman Therribout1,2,3,4
Norman Therribout1,2,3,4 Romain Icick2,3,4,5
Romain Icick2,3,4,5 Vanessa Bloch2,3,4,5
Vanessa Bloch2,3,4,5 Maeva Fortias2,3,4Kristel Piani2
Maeva Fortias2,3,4Kristel Piani2 Lucia Romo1,6
Lucia Romo1,6Introduction: Stimulant use is an important health issue. In the US in 2018, 2.8% of males and 1.5% of females older than 18 had used cocaine in the preceding 12 months.
Objective: To intervene in a specific targeted group of Stimulant Use Disorder (SUD) patients according to CBT and relapse prevention theories, and to determine the program’s feasibility and attendance.
Method: Stimulant Use Disorder patients in addiction care were evaluated for addictive, psychological and psychiatric dimensions at baseline and conclusion in a 9-session CBT group program with several themes: define SUD, enhance motivation, involve close companions, cope with craving, decline a proposal, solve problems, invite expert patients, invest time and money, and review content.
Results: In total, 41 patients attended at least one session. They were mainly poly dependent, primarily cocaine users. Sixty percent of the population also suffered from another psychiatric comorbidity. Median attendance for participants was 7/9 sessions.
Conclusion: A specific targeted CBT group for stimulant dependent highly comorbid patients is feasible. These findings suggest that peers should be included in addiction care services.
Stimulant use is an important health issue. In the US in 2018, 2.8% of males and 1.5% of females older than 18 had used cocaine in the preceding 12 months (1), a number close to that in Europe in 2019, where 2.1% of 15 to 34 year olds had taken cocaine in the past 12 months, 1.4% amphetamines, and 1.9% MDMA (3,4-Methylenedioxymethamphetamine). In France these numbers are even higher (3.2, 0.6, and 1.3%, respectively) (2). The use of New Synthetic drugs, including cathinones and the non-stimulant synthetic cannabinoids is estimated at 1.1% among this same population in Europe. For the methamphetamine, some countries include it in their amphetamine use data and the prevalence rate seems to be highly variable, between 330 and 34,600 users at risk per country.
Stimulants use, including cocaine, has many consequences, including somatic (infarctus, pulmonary insufficiency, stroke…) (3, 4), psychiatric (a higher incidence of anxiety disorders or induced psychotic symptoms) (5, 6), and social consequences. Moreover, in the United States from 2010 to 2014, on average 7,500 of the 40,000 overdoses per year involved stimulants (cocaine or methamphetamine), and overdoses per year with these substances are rising (7).
Stimulant users attending care programs represent a specific population in many ways. Indeed, they are at high risk of experiencing delusional thinking (30% of cocaine-dependent patients) and unusual social or sexual behavior (65%) (5). They show a very strong association with childhood trauma. A previous study found that 62% of cocaine users had experienced such trauma (8). Furthermore, cocaine users are largely poly users. In another study they presented a median of three lifetime DSM IV dependence to other substances than cocaine (9). These substances were mostly “downers,” substances sharing sedative properties (alcohol, benzodiazepine, and cannabis), so patients are likely to use them to prevent coming-off effects.
In France, among stimulant users, cocaine users who entered treatment centers are mostly men (80%) and on average started cocaine at 24 years old and entered the center at 33 years old, meaning that there is a great delay between first use and treatment access (10). The management of stimulant users is characterized by several barriers to treatment. In substance abuse clinics, 34% quit the process within two months, and cocaine-related issues increased the risk of early drop-out (11). Of methamphetamine users, only 23% of outpatients remained in treatment after 180 days (12).
Moreover, significant neurocognitive impairment has been shown among cocaine users (13). A meta-analysis suggests that impulsivity is a core process underlying addictive disorders (14). A study comparing cocaine users to healthy controls found that cocaine users have elevated scores on trait impulsivity and have significantly poorer performance on inhibition and perseveration (15). Furthermore, dependent cocaine users display broad cognitive impairments in the domains of attention, working memory, declarative memory, and executive functions compared to recreational users or non-cocaine users (16).
Because there are no validated pharmacotherapies for stimulant treatment, psychotherapy seems to be an important part of the treatment. Cochrane Library published a meta-analysis in 2016 of 52 controlled randomized trials of psychotherapies for stimulant treatments, finding that all individual interventions diminished drop-out rates and enhanced abstinence (17). Another meta-analysis in 2018 of studies of cocaine and amphetamine users found that the combination of two different psychosocial interventions, contingency management and community reinforcement, was the most efficacious and accepted treatment in the short and long term (18). More recently, a systematic review published in 2020 states that no pharmaceutical intervention has proven its efficacy and the most promising psychological intervention was Contingency Management (CM). This therapy seems to have a short-term efficacy on abstinence. Moreover, the combination of CM and Cognitive Behavioral Therapy might be the most efficient therapy with a higher rate of abstinence, a lower drop out and probably more long-term effect. About CBT alone, the authors conclude that more research is needed to ensure its efficacy, particularly on abstinence (19).
The French High Health Authority recommends individual psychotherapy, such as Cognitive Behavioral Therapy (CBT), for cocaine dependence and states that groups could provide an interesting complement (20). They suggest a number of themes that could be discussed: Managing craving, enhancing motivation, gaining competences to resist solicitations, recognizing high-risk situations, generalizing strategies to face the desires to consume, and solving urgent problems that could pose the risk of using cocaine. Furthermore, Marlatt and Donovan suggest that Relapse Prevention for stimulant use should include an initial evaluation with common objectives, then a large part of the therapy should focus on cravings (trigger identification, exposition, refusal to use, alternative strategies, etc.) (21). Stimulant use can cause neuropsychological impairment that must be taken into account before engaging in any therapy, and it is preferable to postpone the relapse prevention program after a neurocognitive training to enhance the efficacy (22).
Because of the cost of the individual setting and the contribution of peer groups, there have been several studies of group therapies for stimulant users. The Matrix Program combines individual and group sessions (relapse prevention, 12-step, family, and social support groups) (23). Furthermore, Tzilos et al. developed a contingency model for cocaine users in methadone-maintained treatment. Among them, 26% never came to any session and 62% were non-completers (completers were defined as patients who came to at least six consecutive sessions with cocaine-negative urine samples) (24). A Spanish team developed a combined CBT and motivational open group 12-session program for cocaine users that demonstrated a very high retention rate (84%) (25). A study comparing CBT and Mindfulness Treatment (MT) open groups among drug users (alcohol and/or cocaine) showed high drop-out and similar drug reduction in both groups (26). In this study, the CBT program was implemented according to the National Institute for Drug Abuse guidelines (27). They suggest several topics to work with the patient: Coping with craving, shoring up motivation and commitment to stop, refusal skills/assertiveness, seemingly irrelevant decisions, coping plans, problem solving, case management, and HIV or other infectious risk reduction.
Several studies of cocaine treatment include avoidance and reinforcement components, but a large study illustrated the ineffectiveness of punitive approaches and highlighted the potential of improving goal-directed behavior and employing more desirable habits to replace drug-taking habits, such as CBT approaches (28). The third wave of CBT approaches, specifically Mindfulness Based Interventions, seems to have a significant effect on craving and substance misuse, so this approach could constitute a useful therapy for addiction treatment (29).
Therefore, the aim of this study was to intervene in a specific, targeted group for stimulant dependent patients. Few sessions were designed to take into consideration the impulsivity and lack of persistence of these patients in order to enhance attendance. The conceptual framework was CBT and relapse prevention theories. The secondary objective was to observe the feasibility, acceptability, and attendance in this group.
Participants were recruited from the clinical outpatient department of a university hospital in Paris (France). Potential participants were identified by their treating psychiatrist or psychologist. The inclusion criteria were: (1) regularly followed French-speaking patients, (2) met diagnostic criteria of Substance Use Disorder (SUD) according to the Diagnostic and Statistical Manual for Mental Disorder 5 (30) for any stimulants (cocaine, crack, amphetamines, methamphetamine, cathinones), (3) wanting to stop or diminish their consumption, and (4) without acute psychiatric symptoms preventing group participation such as current delusion, hallucinations, mood instability, or suicidal ideation. No psychiatric diagnosis was excluded. All participants joined the same therapy program as an add-on to their usual outpatient psychiatric and addiction medicine care.
The study was conducted according to the Declaration of Helsinki and the French legislation on biomedical research in human subjects (Loi Jardé 2014), as well as the ethical guidelines of our hospital for the analysis of data already collected during routine care (Authorization 2017–013 given on 19 January 2017 by the CNIL, the Commission Nationale Informatique et Liberté, or French National Board for Information Systems and Freedom). Verbal consent to participation and research application of the data was obtained from all participants after information. Furthermore, specific information and consent was obtained for relatives’ participation.
Eligible participants were invited to an initial visit to discuss participation and receive information about the group therapy program, rules, and assessments in the month before the session started.
Socio-demographic data was collected in a semi-directed interview with the therapist, as well as substance use histories (substance use disorders, age at onset, and routes of administration). Psychiatric diagnoses and actual psychotropic treatment were recorded from the medical record. Attendance was recorded as the number of sessions attended by each individual and participant subjective feed-back was recorded during the last session (no. 9).
Actual anxiety and depression were assessed using the HAD (Hospital Anxiety and Depression) screening questionnaire, a 14-item self-rated questionnaire that evaluates anxiety and depression during the past week (31). A Canadian study showed that this measure seems to have a good level of reliability with Cronbach alpha around 0.8 and confirm the two factors measure with anxiety and depression subscales. Their results were similar among the general population and multimorbidity patients (32).
Stimulant frequency and intensity of use were evaluated with the TLFB (TimeLine Followback) questionnaire. This tool is a calendar (initially developed for alcohol consumption) in which patients note when they use a drug and how much (33). The tool has proven its reliability using test-retest comparison for several substances. Also, the TLFB has demonstrated its validity, being highly correlated with the Addiction Severity Index and discrimination with high correlations with urine sample analysis (34).
Self-confidence was recorded with the BSCQ (Brief Situational Confidence Questionnaire) questionnaire, a state-dependent measure that assesses self-confidence to resist the urge to use a drug in several situations with 8 items in a Visual Analogic Scale (35). A study among incarcerated youth highlights a good test-rest stability (Pearson’s r around 0.60) and internal consistency (Cronbach’s alpha around 0.85) (36).
Craving was assessed using the OCCS questionnaire (Obsessive Compulsive Craving Scale), which is a 14-item questionnaire with a total score and two subscales: obsession and compulsion during the last 2 weeks (37). This same study shows a Cronbach’s alpha of 0.93. It also highlights a high correlation with the Visual Analog Scale (Pearson’s r = 0.641).
The motivation to change was evaluated with the URICA (University of Rhode Island Change Assessment), a 32-item self-rated questionnaire to evaluate change motivation on four subscales (pre-contemplation, contemplation, action, and maintenance), with a total score calculated by adding the scores for contemplation, action, and maintenance and subtracting the pre-contemplation score (38). Each subscale has good internal consistency with Cronbach’s alpha ranging from 0.81 to 0.88 (39).
This closed group consisted of nine sessions with two therapists, each of 1.5 h duration. The authors did design this group intervention according to classical Relapse Prevention themes (21, 40, 41). The synthetic themes of each session are presented in Table 1. Sessions included several themes such as: a common definition of TUS according to DSM 5 (30), introduction to motivational interviewing and Prochaska and Di Clemente’s theory (42); introduction to assertiveness principle (43), solving problem strategies (44) and relaxation (19, 45).
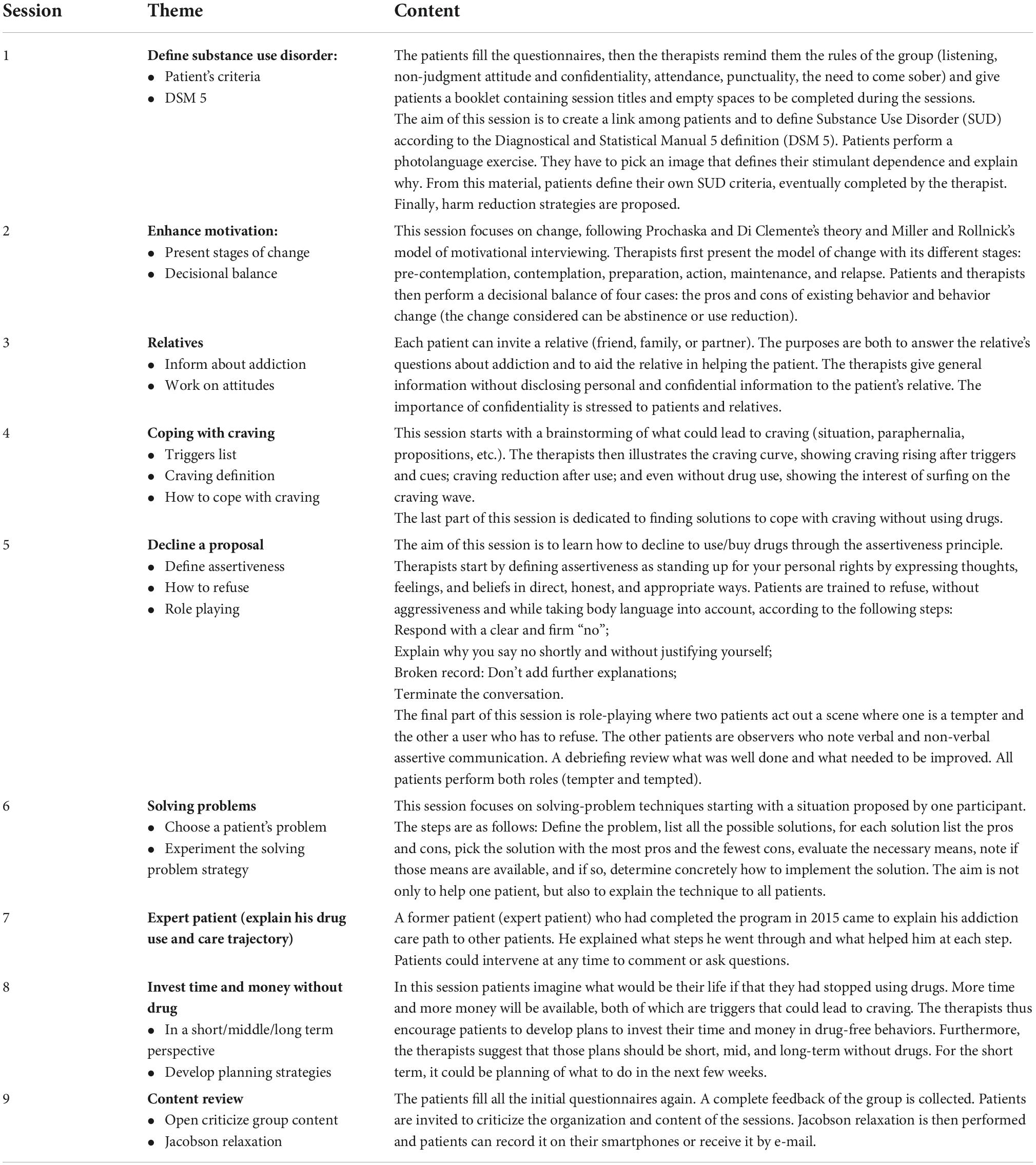
Table 1. Sessions and themes.
Variables are described using means (Standard Deviation) and percentages. When a patient did not answer all questionnaires, only available data was analyzed. This was also the case for drop outs. The distribution normality was checked. Comparison between pre and post intervention were tested using Khi2 and Repeated Measure Anova or Wilcoxon as appropriate, with a p < 0.05 threshold. The analysis were done using JASP 0.8.6.0 software.
The 41 patients who came to at least one session were recruited between June 2017 and November 2019. They were on average 43 years old; 73% were men, 26% did not have their own housing, 58% had a job, and 58% were single. Regarding stimulant use, patients preferentially used cocaine (65%) over other stimulants and preferred snorting cocaine (68% vs. injection or smoking). The mean age at onset of stimulant use was 28 years old (± 10 years). They had an average of 1.2 grams or 3 rocks per day of stimulant use.
Concerning other substances, 61% were currently dependent on tobacco, 62% on alcohol, 12% on cannabis, and 2% on opiates (among whom all were on agonist maintenance treatment).
Regarding their current psychiatric component (according to their medical records), 40% did not have any psychiatric comorbidity, 30% had mood disorder, 12.5% personality disorder, 10% anxiety disorder, and 2% schizophrenia. Twenty nine percent of the patients had no prescribed psychotropic treatment, 33% had antidepressants, 37% antipsychotics [including aripiprazole prescribed as anti-craving treatment (46)], 28% benzodiazepines, and 28% mood-stabilizer treatment.
Detailed results are presented in Table 2. The TLFB questionnaire showed that in the month before the group started, patients had a mean of 7 days of stimulant use. The median of the frequency of the number of days of abstinence was 76%. The OCCS craving mean total score was 18.9 (±7.4) in a range from 0 to 56, where a higher score indicates higher craving. The subscales were largely equivalent, with a mean obsessive score of 8.5 and a mean compulsive score of 10.4. The mean URICA score was 88 (±11.4) on a possible range of −16–112, where higher scores indicate greater motivation to change. The score can also be observed using stages. In this configuration, 25 patients had no equality between two stages and can be interpreted. We observe among those 25 patients that a half (52%) were in contemplation, 32% in action and 16% in maintenance; none was in pre-contemplation. The HAD anxiety mean score was 11.9 (±4.2) and the depression mean score was 7.9 (±4.7). Both scores highlight the presence of anxiety and depression symptoms (47). Furthermore, almost half of the population (N = 17), experiment depressive symptoms above the recommended screening cut off. Regarding anxiety screening, 90% of the participants experience symptoms above the cut off. The BSCQ self-confidence median was 350, the mean total score was 362 (±144) and the average score was 45.2 (±18.0), meaning that in the situations listed, patients felt that they were at a 45% risk of using the stimulant.

Table 2. Main assessment tools results.
Among completers (N = 17), the percentage of abstinence days prior to the inclusion was 85.3% (measured with the TLFB) with no statistical diminution between baseline and the end of the intervention. There was no significant change either for the following variables: OCCS total score (mean 18.82 ± 7.6), obsession score (mean 8.2 ± 3.6), compulsion score (mean 10.4 ± 4.5); the BSCQ total score (mean 427.1 ± 115.5) or mean score (mean 53.4 ± 14.4); the HAD depression score (mean 7.1 ± 4.2) or the Anxiety score (12.1 ± 4.5), see Table 3. Among patients attending the last session, they did not all answer all questionnaires proposed. Furthermore, some tools were added after the beginning of the intervention, so were not proposed for the first patients.
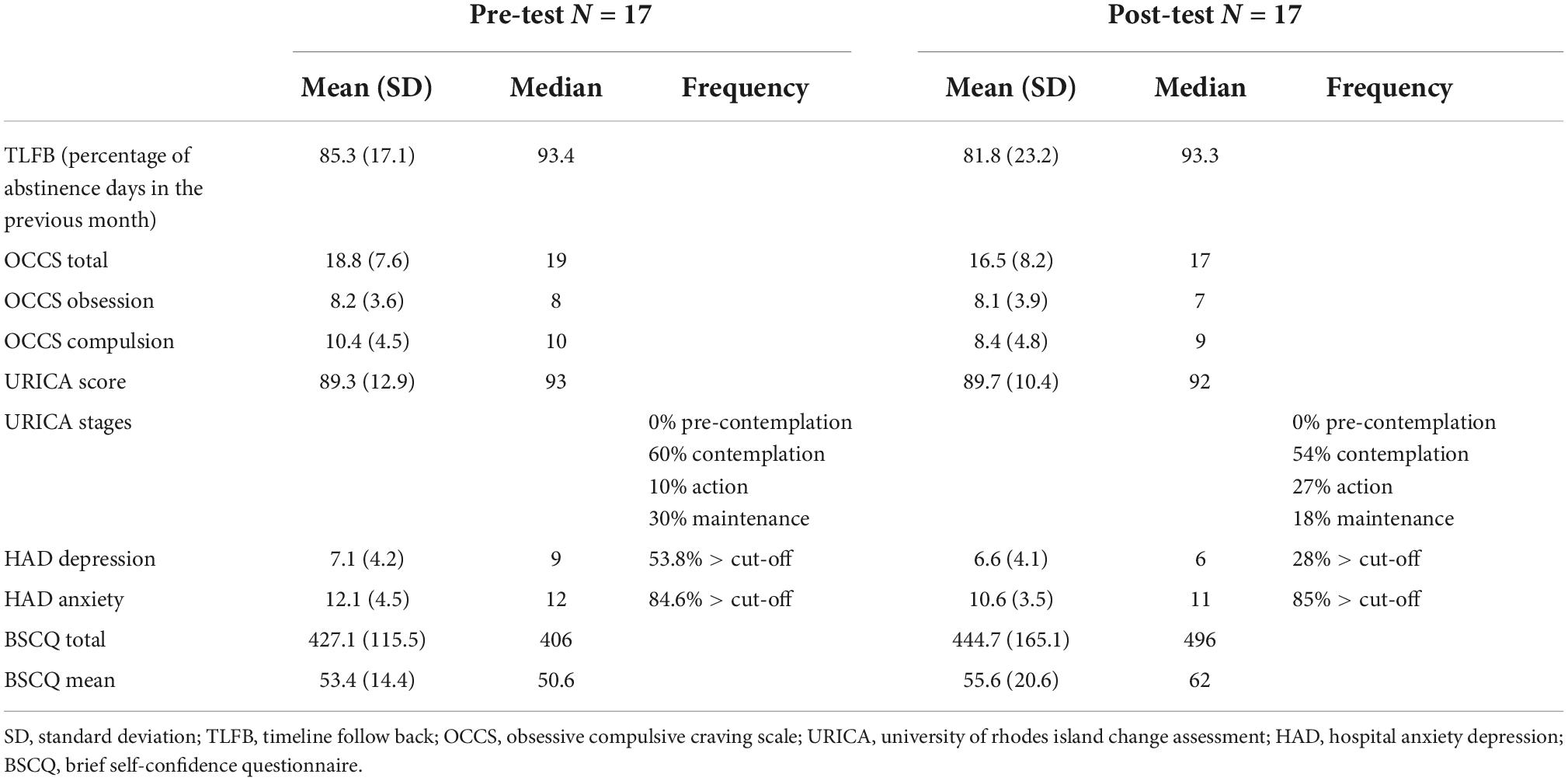
Table 3. Completers evaluation.
The average number of sessions attended by patients was 5.7 (±2.8) out of 9 sessions. The median was 7 and the mode was 8 sessions (see Figure 1). Figure 1 also highlight that 6 patients only attend one session and 5 went for all sessions. The TLFB did not significantly change between the beginning and the end of the intervention, the mean rate of abstinence days was 76% at the beginning and 82% at the end (see Table 2). Regarding the median, it was 87% at the beginning and at the end 60% of the population had scores higher than the initial median. Among the 41 patients who came to at least one session, 5 came to all sessions and 4/15 were abstinent at the end of the group, that is, 26% (among 15 patients) or 9% (among 41 patients). Among the 16 patients who attended the last session, on the URICA scale, 11 subjects described a specific stage. A half (54%) were in contemplation, 27% in action and 18% in maintenance. Those scores are very similar to those at the beginning of the intervention. About the HAD, among the 14 patients who completed the evaluation at the end of the group, 28% experience depressive symptoms above the cut off and 79% for anxiety. Those frequencies are lower than at the beginning of the intervention. Among pre-post evaluated patients (N = 13), a Khi2 was performed and depression rates above the cut-off significantly decrease (p = 0.026), this result is no longer significant for anxiety (p = 0.140).
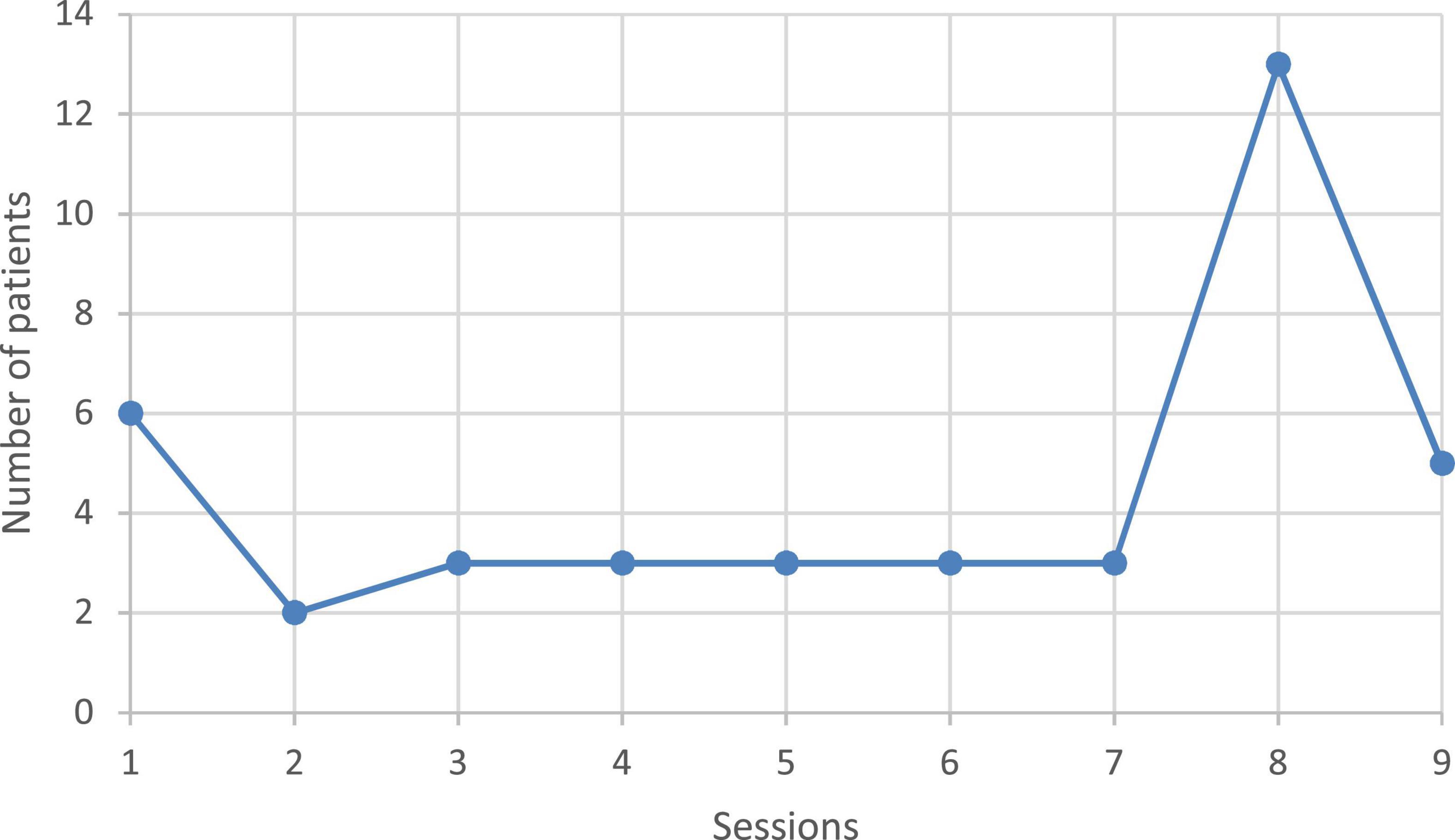
Figure 1. Attendance (number of sessions attended for each patient).
Concerning self-efficacy, at the end of the intervention, 69% of the patients had a score above the median of the beginning of the group, what could suggest that they improve their self-efficacy feeling during the intervention, even if the attrition rate was high.
On the craving scale, 59% of participants diminish their total score on the OCCS between the beginning and the end of the intervention. This rate was lower on the obsession scale (41%) and higher on the compulsion scale (65%).
Participants’ feedback was positive, as per the comments of patients attending the last session. For example, verbatim included that some patients learnt theoretical elements and appreciate to be with peers. On the other hand, patients often told us that sessions could raise stimulant craving by talking about drugs.
We designed a specific relapse prevention CBT group for outpatients with stimulant use disorder to address their specific need (poly dependence, induced delusions, alteration in social and sexual behavior, neurocognitive impairment, and childhood trauma).
It is noteworthy that patients who attended the group sessions had 76% abstinent days in the month before the first session, raising the question of whether patients who came to the group were already highly motivated or had already initiated a change, such that only “almost cured” patients would attend this highly demanding type of care.
The observed OCCS total score was correlated with the frequency and intensity of use, and as patients had numerous abstinent days, their scores tended to be intermediate between high and low craving (5).
The URICA score is high (mean = 88), indicating that the patients who could attend the sessions had a high motivation to change (48).
Attendance could be interpreted in different ways. Attendance could be seen as quite high, with a mode of 8 out of 9 sessions. Looked at another way, we also note that only 12% of patients went to all sessions. Furthermore, compared to previous studies, the attendance was good. One study (24) reported that 26% of patients never came to any session, whereas for ours the rate was 9.7%, but they had 62% non-completers (completers were defined as patients who came to at least 6 consecutive sessions with cocaine-negative urine samples), whereas in this study 58% came to at least 6 sessions. Another study (a CBT and motivational open group program of 12 sessions) among 19 patients, reported a high retention rate (84%), defined as attending 11/12 sessions (25). In comparison, in our study the retention rate was 44%, defined as attending eight to nine sessions, among patients who came to at least one session.
We did not observe a significant improvement in cocaine use or questionnaires’ scores, but patients already had low scores at the beginning of the program. However, 4 of the 15 patients were abstinent at the end of the program.
However, this study has some limitations. This study is an open study with no other group (control or other intervention). We thus might lack the power to demonstrate significant differences or patient improvement. Some of this lack of power could be due to the use of self-rated questionnaires only.
This group is hard to organize, in part because practitioners in our clinic did not easily refer patients to group therapies, and in part because it is difficult to constitute a homogenous group. However, patients attending the last session (who were asked to comment on the group) gave positive feedback about the help provided by the group, the organization, and session content.
In the future, we would like to raise the effectiveness of the program, explore the differences between the different stimulants, and change the tools to gain in sensibility.
There are several strengths of this study. A specific intervention was designed to respond to the specific needs of stimulant user patients in a prospective study with pre-post evaluations. The study was conducted among patients affected by a disorders associated with poor compliance, and a good feasibility and acceptability were demonstrated. Moreover, this article partially responds to a previous article with a real life application of a group therapy in an out-patient treatment setting (49).
To improve this study, it would be interesting to increase inclusions to demonstrate patient improvement. An a priori test (α = 0.05) for the difference between two means with matched pairs using the OCCS total score (one-tailed) suggests that the number needed to ensure sufficient statistical power is 67 patients, to whom both pre and post-evaluations would be applied. In order to confirm the efficacy, a comparison to another intervention, such as a computer-delivered program (50), is warranted.
Clinically, the content of the sessions could be enriched with mindfulness components and integrating psychoeducation on harm reduction on sexual behavior (51, 52).
This group intervention is feasible for patients suffering from stimulant use disorder and should be generalized in all care settings because the number of those patients is increasing in all care services without efficient pharmaceutical response.
This study presents a specific targeted CBT group program for severe poly dependent patients suffering from stimulant use disorder. Indeed, few interventions exist for this specific population. This group program proved feasible, even if most patients had difficulties attending all sessions.
Patients’ recruitment in this study should go on to verify the efficacy of this therapeutic intervention. Furthermore, it would be interesting to add a follow up session, as well as to keep in contact with patients and to assess them again after the intervention.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
EK and MF designed the group program. EK, KP, and NT included the participants and performed the intervention. LR and FV designed the research protocol. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Cano M, Oh S, Salas-Wright CP, Vaughn MG. Cocaine use and overdose mortality in the United States : evidence from two national data sources, 2002–2018. Drug Alcohol Depend. (2020) 214:108148. doi: 10.1016/j.drugalcdep.2020.108148
2. European Monitoring Centre for Drugs and Drug Addiction. European Drug Report 2021 : Trends and Developments. Lisbon: Publications Office (2021).
3. Keskin M, Hayıroğlu Mİ, Keskin Ü, Kaya A, Aydın BA, Börklü EB, et al. The most dangerous complication of intranasal cocaine abuse in a young man : cardiac arrest. Am J Emerg Med. (2016) 34:1731.e5–7. doi: 10.1016/j.ajem.2015.12.043
4. Wilson KC, Saukkonen JJ. Acute respiratory failure from abused substances. J Intens Care Med. (2004) 19:183-193. doi: 10.1177/0885066604263918
5. Vorspan F, Brousse G, Bloch V, Bellais L, Romo L, Guillem E, et al. Cocaine-induced psychotic symptoms in French cocaine addicts. Psychiatry Res. (2012) 200:1074-1076. doi: 10.1016/j.psychres.2012.04.008
6. Vorspan F, Mehtelli W, Dupuy G, Bloch V, Lépine J-P. Anxiety and substance use disorders : co-occurrence and clinical issues. Curr Psychiatry Rep. (2015) 17:4. doi: 10.1007/s11920-014-0544-y
7. Warner M, Trinidad JP, Bastian BA, Minino AM, Hedegaard H. Drugs most frequently involved in drug overdose deaths : United States, 2010-2014. Natl Vital Stat Rep. (2016) 65:1-15.
8. Karsinti E, Jarroir M, Zerdazi E-H, Bloch V, Dupuy G, Belforte B, et al. Childhood trauma are not associated with the intensity of transient cocaine induced psychotic symptoms. Psychiatry Res. (2015) 228:94-944. doi: 10.1016/j.psychres.2015.05.065
9. Karsinti E, Piani K, Zerdazi EH, Maskos U, Faure P, Romo L, et al. Relevance of treated cocaine users’ retrospective memory of first cocaine use. Psychiatry Res. (2018) 264:210-216. doi: 10.1016/j.psychres.2018.03.058
10. OEDT,. Rapport Européen sur les Drogues. Tendances et Évolutions 2017. (2017). Available online at: https://www.ofdt.fr/BDD/publications/docs/EDR2017.pdf (accessed August 8, 2022).
11. Calvo F, Carbonell X, Valero R, Costa J, Turró O, Giralt C, et al. [Early drop-outs and retentions in substance abuse outpatient clinics : a cross-sectional comparative study of factors that increase or decrease adherence]. Atencion Primaria. (2018) 50:477-485. doi: 10.1016/j.aprim.2017.06.006
12. Maglione M, Chao B, Anglin MD. Correlates of outpatient drug treatment drop-out among methamphetamine users. J Psychoactive Drugs. (2000) 32:221-228. doi: 10.1080/02791072.2000.10400232
13. Mahoney JJ, Kalechstein AD, De Marco AP, Newton TF, De La Garza R. The relationship between premorbid IQ and neurocognitive functioning in individuals with cocaine use disorders. Neuropsychology. (2017) 31:311-318. doi: 10.1037/neu0000344
14. Lee RSC, Hoppenbrouwers S, Franken I. A systematic meta-review of impulsivity and compulsivity in addictive behaviors. Neuropsychol Rev. (2019) 29:14-26. doi: 10.1007/s11065-019-09402-x
15. Fernández-Serrano MJ, Perales JC, Moreno-López L, Pérez-García M, Verdejo-García A. Neuropsychological profiling of impulsivity and compulsivity in cocaine dependent individuals. Psychopharmacology. (2012) 219:673-683. doi: 10.1007/s00213-011-2485-z
16. Vonmoos M, Hulka LM, Preller KH, Jenni D, Baumgartner MR, Stohler R, et al. Cognitive dysfunctions in recreational and dependent cocaine users : role of attention-deficit hyperactivity disorder, craving and early age at onset. Br J Psychiatry. (2013) 203:35-43. doi: 10.1192/bjp.bp.112.118091
17. Minozzi S, Saulle R, De Crescenzo F, Amato L. Psychosocial interventions for psychostimulant misuse. Cochrane Database Syst Rev. (2016) 9:CD011866. doi: 10.1002/14651858.CD011866.pub2
18. De Crescenzo F, Ciabattini M, D’Alò GL, De Giorgi R, Del Giovane C, Cassar C, et al. Comparative efficacy and acceptability of psychosocial interventions for individuals with cocaine and amphetamine addiction : a systematic review and network meta-analysis. PLoS Med. (2018) 15:e1002715. doi: 10.1371/journal.pmed.1002715
19. Ronsley C, Nolan S, Knight R, Hayashi K, Klimas J, Walley A, et al. Treatment of stimulant use disorder : a systematic review of reviews. PLoS One. (2020) 15:e0234809. doi: 10.1371/journal.pone.0234809
20. HAS. Recommandations de Bonne Pratique—Prise en charge des consommateurs de cocaïne. HAS: Saint-Denis (2010).
21. Marlatt GA, Donovan DM. Relapse Prevention : Maintenance Strategies in the Treatment of Addictive Behaviors. New York, NY: Guilford Press (2007).
22. Fagan CS, Carmody TJ, McClintock SM, Suris A, Nakamura A, Jeon-Slaughter H, et al. The effect of cognitive functioning on treatment attendance and adherence in comorbid bipolar disorder and cocaine dependence. J Subst Abuse Treatment. (2015) 49:15-20. doi: 10.1016/j.jsat.2014.06.008
23. Rawson RA, Shoptaw SJ, Obert JL, McCann MJ, Hasson AL, Marinelli-Casey PJ, et al. An intensive outpatient approach for cocaine abuse treatment : the matrix model. J Subst Abuse Treatment. (1995) 12:117-127. doi: 10.1016/0740-5472(94)00080-B
24. Tzilos GK, Rhodes GL, Ledgerwood DM, Greenwald MK. Predicting cocaine group treatment outcome in cocaine-abusing methadone patients. Exp Clin Psychopharmacol. (2009) 17:320-325. doi: 10.1037/a0016835
25. Sánchez L, Díaz-Morán S, Grau-López L, Moreno A, Eiroa-Orosa FJ, Roncero C, et al. [Ambulatory group treatment for cocaine dependent patients combining cognitive behavioral therapy and motivational interviewing]. Psicothema. (2011) 23:107-113.
26. Brewer JA, Sinha R, Chen JA, Michalsen RN, Babuscio TA, Nich C, et al. Mindfulness training and stress reactivity in substance abuse : results from a randomized, controlled stage I pilot study. Subst Abus. (2009) 30:306-317. doi: 10.1080/08897070903250241
27. Carroll KM. Therapy Manuals for Drug Abuse. Gaithersburg, MD: National Institute on Drug Abuse (1998).
28. Ersche KD, Gillan CM, Jones PS, Williams GB, Ward LHE, Luijten M, et al. Carrots and sticks fail to change behavior in cocaine addiction. Science. (2016) 352:1468-1471. doi: 10.1126/science.aaf3700
29. Garland EL, Howard MO. Mindfulness-based treatment of addiction : current state of the field and envisioning the next wave of research. Addict Sci Clin Pract. (2018) 13:14. doi: 10.1186/s13722-018-0115-3
30. American Psychiatric Association [APA], Crocq M-A, Guelfi J-D, Boyer P, Pull C-B, Pull M-C. DSM-5—Manuel Diagnostique et Statistique des Troubles Mentaux. 5th ed. Mason, IA: Elsevier (2015).
31. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361-370.
32. Roberge P, Doré I, Menear M, Chartrand E, Ciampi A, Duhoux A, et al. A psychometric evaluation of the French Canadian version of the hospital anxiety and depression scale in a large primary care population. J Affect Disord. (2013) 147:171-179. doi: 10.1016/j.jad.2012.10.029
33. Sobell LC, Sobell MB. Timeline follow-back. In: Litten RZ, Allen JP, editors. Measuring Alcohol Consumption. Totowa, NJ: Humana Press (1992). p. 41-72. doi: 10.1007/978-1-4612-0357-5_3
34. Fals-Stewart W, O’Farrell TJ, Freitas TT, McFarlin SK, Rutigliano P. The timeline followback reports of psychoactive substance use by drug-abusing patients : psychometric properties. J Consult Clin Psychol. (2000) 68:134-144. doi: 10.1037//0022-006x.68.1.134
35. Breslin FC, Sobell LC, Sobell MB, Agrawal S. A comparison of a brief and long version of the situational confidence questionnaire. Behav Res Ther. (2000) 38:1211-1220. doi: 10.1016/S0005-7967(99)00152-7
36. Delaney DJ, Bernstein MH, Harlow LL, Farrow M, Martin RA, Stein LAR. The brief situational confidence questionnaire for alcohol : a psychometric assessment with incarcerated youth. Psychol Assess. (2020) 32:254-264. doi: 10.1037/pas0000780
37. Vorspan F, Bellais L, Romo L, Bloch V, Neira R, Lépine J-P. The obsessive-compulsive cocaine scale (OCCS) : a pilot study of a new questionnaire for assessing cocaine craving. Am J Addict. (2012) 21:313-319. doi: 10.1111/j.1521-0391.2012.00248.x
38. McConnaughy EA, Prochaska JO, Velicer WF. Stages of change in psychotherapy : measurement and sample profiles. Psychotherapy. (1983) 20:368-375. doi: 10.1037/h0090198
39. Field CA, Adinoff B, Harris TR, Ball SA, Carroll KM. Construct, concurrent and predictive validity of the URICA : data from two multi-site clinical trials. Drug Alcohol Depend. (2009) 101:115-123. doi: 10.1016/j.drugalcdep.2008.12.003
40. Hendershot CS, Witkiewitz K, George WH, Marlatt GA. Relapse prevention for addictive behaviors. Subst Abus Treatment Prev Policy. (2011) 6:17. doi: 10.1186/1747-597X-6-17
41. Velasquez MM, Crouch C, Stephens NS, DiClemente CC. Group Treatment for Substance Abuse, Second Edition : A Stages-of-Change Therapy Manual. New York, NY: Guilford Publications (2015).
42. Prochaska JO, Diclemente CC. Toward a comprehensive model of change. In: Miller WR, Heather N, editors. Treating Addictive Behaviors. Berlin: Springer (1986). p. 3-27. doi: 10.1007/978-1-4613-2191-0_1
43. Fanget F, Rouchouse B. L’ affirmation de soi : Une Méthode de Thérapie. Paris: Éditions Odile Jacob (2007).
44. D’Zurilla TJ, Nezu AM. Problem-Solving Therapy : A Social Competence Approach to Clinical Intervention. Berlin: Springer (1999).
45. Jacobson E. The origins and development of progressive relaxation. J Behav Ther Exp Psychiatry. (1977) 8:119-123. doi: 10.1016/0005-7916(77)90031-3
46. Vorspan F, Bellais L, Keijzer L, Lépine J-P. An open-label study of aripiprazole in nonschizophrenic crack-dependent patients. J Clin Psychopharmacol. (2008) 28:570-572. doi: 10.1097/JCP.0b013e3181858311
47. Beekman E, Verhagen A. Clinimetrics : hospital anxiety and depression scale. J Physiother. (2018) 64:198. doi: 10.1016/j.jphys.2018.04.003
48. Bergly TH, Stallvik M, Nordahl HM, Hagen R. The predictive validity of the URICA in a sample of patients in substance use treatment. Addict Disord Their Treatment. (2014) 13:170. doi: 10.1097/ADT.0000000000000041
49. López G, Orchowski LM, Reddy MK, Nargiso J, Johnson JE. A review of research-supported group treatments for drug use disorders. Subst Abus Treatment Prev Policy. (2021) 16:51. doi: 10.1186/s13011-021-00371-0
50. Schaub MP, Castro RP, Wenger A, Baumgartner C, Stark L, Ebert DD, et al. Web-based self-help with and without chat counseling to reduce cocaine use in cocaine misusers : results of a three-arm randomized controlled trial. Internet Interv. (2019) 17:100251. doi: 10.1016/j.invent.2019.100251
51. Bowen S, Chawla N, Grow JC, Marlatt GA. Mindfulness-Based Relapse Prevention for Addictive Behaviors : A Clinician’s Guide. 2nd ed. New York, NY: The Guilford Press (2021).
Keywords: group therapy, substance use disorders, cocaine (PubChem CID: 11302220), Cognitive Behavioral Therapy (CBT), craving
Citation: Karsinti E, Vorspan F, Therribout N, Icick R, Bloch V, Fortias M, Piani K and Romo L (2022) A specific cognitive behavioral group therapy program for stimulant use disorder. Front. Psychiatry 13:1031067. doi: 10.3389/fpsyt.2022.1031067
Received: 29 August 2022; Accepted: 02 November 2022;
Published: 30 November 2022.
Edited by:
Marc Walter, University of Basel, SwitzerlandReviewed by:
Lavinia Flückiger, Health Department Basel, SwitzerlandCopyright © 2022 Karsinti, Vorspan, Therribout, Icick, Bloch, Fortias, Piani and Romo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emily Karsinti, ZW1pbHkua2Fyc2ludGlAYXBocC5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.