
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 26 October 2022
Sec. Psychopathology
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.1015616
This article is part of the Research Topic Situating Phenomenological Psychopathology: Subjective Experience Within the World View all 11 articles
 Line Lindhardt1*
Line Lindhardt1* Lars Siersbæk Nilsson2
Lars Siersbæk Nilsson2 Povl Munk-Jørgensen3
Povl Munk-Jørgensen3 Ole Steen Mortensen4,5
Ole Steen Mortensen4,5 Erik Simonsen6,7
Erik Simonsen6,7 Julie Nordgaard2,7
Julie Nordgaard2,7Background: Schizophrenia spectrum disorders typically emerge during adolescence or early adulthood. Often the symptomatology is vague initially, while a marked functional decline and social withdrawal can be seen. A group of young people with such social and functional impairments is the so-called “Not in Education, Employment or Training” (NEET), i.e., a youth population that is socially disconnected from education and work-life. Despite the NEET group’s disconnection from important parts of social life and a rising concern of an intersection with mental health problems, a psychopathological perspective on the problems experienced by this group remains underexplored.
Aim: To examine a NEET sample for psychopathology and if relevant allocate psychiatric diagnoses.
Methods: We performed an interview study comprising 40 participants from youth job-counseling services. All underwent a comprehensive psychiatric evaluation. Inclusion criteria were 18–29 years of age and a welfare benefit history of minimum 6 months.
Results: Diagnostic criteria of any mental disorder were fulfilled by 95% of the sample; half of whom were diagnosed with a schizophrenia spectrum disorder. The participants with schizophrenia spectrum disorders had lower global functioning, were more often in contact with the mental health services and had higher PANSS and Examination of Anomalous Self-Experiences (EASE) scores compared to those with non-schizophrenia spectrum disorders. The participants fulfilling the criteria for schizophrenia spectrum disorders had lower EASE and PANSS scores than usually reported in the literature, suggesting more “symptom-poor” presentations.
Conclusion: Psychiatric illness and particularly schizophrenia spectrum disorders affecting social interaction and the ability to take part in educational and work-life were grossly overrepresented in the NEET sample. Our findings suggest that pronounced social disconnection in youth in and of itself should lead to suspect the presence of a severe mental disorder.
Social disconnection in the general youth population results in marginalization for the individual, and has considerable economic consequences for society (1). Consequently, socially marginalized youth is a major public health concern with social policy interest (2, 3). The term “Not in Employment, Education or Training” (NEET) is an international consolidated indicator and among others used by Eurostat and the Organization for Economic Co-operation and Development to describe school-to-work transition difficulties in a vulnerable population of youth facing “social exclusion” (4–6). The concept of NEET has been adopted by researchers and governmental officials to define disconnection from education and work-life in the youth population (3, 7).
Obviously, there are societal differences such as dissimilar opportunities in education and work-life and social inequality which must be taken into account when looking at NEET from a global perspective (8, 9). Moreover, particular culture-bound forms of severe social withdrawal with underexplored relations to more well-defined mental disorders have been reported, cf. the Japanese phenomenon of hikikomori (10, 11).
Studies suggest, however, that mental health problems may be common denominators of the NEET population irrespectively of country and cultural setting and after controlling for possible confounding factors such as social disadvantage (7, 12–14). Unfortunately, not much is known about mental health problems in young, non-help-seeking NEET individuals.
It is primarily large surveys and health outcome data in population-based studies that have addressed the issue (13, 15–18). They have demonstrated significant associations with depressive symptoms, anxiety symptoms and substance use (13, 15, 18) and, that NEET status in young adults is associated with mental disorders in childhood and adolescence (7, 14, 19). A recent systematic review and meta-analysis by Gariépy et al. showed that the NEET status population had an odds ratio (OR) of 1.43 for having mood disorders, an OR of 1.55 for anxiety disorders and an OR of 1.72 for any mental disorder. However, the study pointed to the need for more knowledge about mental health and NEET status. Especially pertinent is the absence of studies addressing psychotic disorders in the NEET status population (20, 21). On the other hand it is well established that young adults experiencing a first-episode psychosis, are often disconnected from education and work when entering into contact with the mental health services (22–24).
Still, social disability tends to be overlooked or perhaps even outright neglected as a characteristic and important sign for schizophrenia spectrum disorders (25). This is especially relevant in symptom-poor schizophrenia in which a prominent decrease in social functioning is often among the first signs of evolving illness (26). In a 20-year longitudinal study comprising information from 485 patients Velthorst et al. found severe and persistent social impairment to be common in the schizophrenia spectrum disorder course (75%) (27).
Critics have pointed to initiatives in early detection of psychosis not taking the significance of social impairment or functional decline fully into account and as such young people with the NEET status are suggested to be a candidate group for early intervention and preventative strategies (28, 29). By thoroughly exploring psychopathology in a NEET population our understanding of the barriers for engaging in social and work life in such groups could be widened.
To investigate psychopathology outside the boundaries of the mental health system within a group of NEETs, and allocate a diagnosis if relevant. Additionally, to further examine the clinical characteristics of the NEETs.
The NEET population was recruited from municipality job-counseling centers within local government social services. In Denmark, young people not in work or education are entitled to financial support if they cannot support themselves. The organization of the assessment of rights to claim financial assistance, is governed by the municipalities and organized in job-counseling centers within the social services (30). Usually, a prerequisite for receiving such financial support is partaking in meetings in the job-counseling centers and non-participation customarily results in the loss of this entitlement (31). Thus, the vast majority of NEETs are in contact with the job-counseling centers.
The participants were recruited from three municipality job-counseling centers of the region Zealand of Denmark: Roskilde Municipality (89,000 inhabitants), Køge Municipality (60,000 inhabitants) and Stevns Municipality (22,000 inhabitants). The catchment areas of these municipalities are primarily rural or suburban.
The following inclusion criteria were applied:
1. Aged 18–29 years
2. Had received non-medical welfare benefits for at least 26 consecutive weeks before the invitation to the study
3. Fluently Danish-speaking
The age range corresponded to the organization in the Danish job-counseling centers, with some organizational differences between municipalities, with specific teams handling the 18–29 year-old young adults. In this study, NEET was defined as a duration of more than 26 consecutive weeks receiving educational benefits, thereby ruling out the possibility of a more transient state of disconnection. Eligibility for participation was independent of prior or current psychiatric treatment.
The participants were recruited by case workers in the three municipalities, who were asked to invite all young people in the job-counseling centers fulfilling the inclusion criteria. Collaboration with the caseworkers in the social services was established by in-person meetings with the teams of caseworkers handling the youth population seeking social assistance. If the invited candidates accepted, the first author LL contacted them by phone. The interviews were conducted either in a municipality facility or in the local outpatient mental health clinics, depending on the participant’s preference. All participated upon informed consent. The recruitment and inclusion of participants are presented in Figure 1.
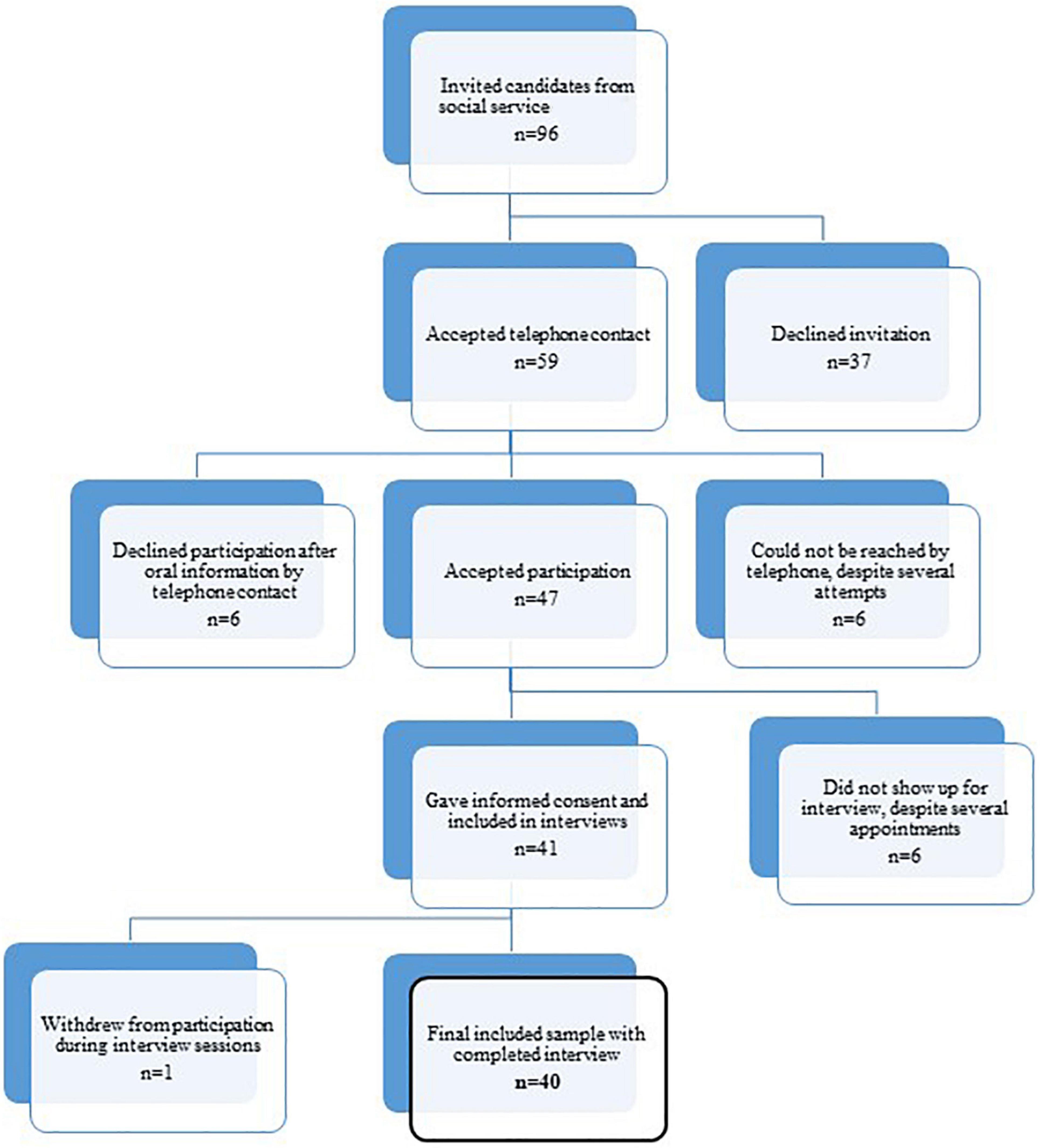
Figure 1. Flow of study participants.
The psychopathological and diagnostic interview included:
- Operational Criteria Checklist for Psychotic Illness and Affective Illness scale (OPCRIT) (32) [an extract of the Present State Examination (PSE)].
- Positive and Negative Syndrome Scale (PANSS) (33).
- Bonn Scale for the Assessment of Basic Symptoms (BSABS), the perceptual section (34).
- Assessment of the First Rank Symptom continua (35).
- Examination of Anomalous Self-Experiences (EASE) (36).
- Global Assessment of Functioning scale, the split version (GAF-S and GAF-F) (37, 38).
The composite of scales derived from former studies exploring schizophrenia spectrum psychopathology and differential diagnosis (39–43). The participants were also assessed with respect to life history, overall psychosocial functioning, educational and vocational history including periods of welfare benefit dependence, family history of mental disorders, and the history of contact with mental health professionals, mental illness evolution and history of somatic diseases and physical symptoms with consequences for overall functioning.
EASE, a symptom checklist consisting of 57 main items, was used to explore anomalous self-experiences (36). In accordance with previous publications, the EASE items were scored only present or absent, not including severity or frequency, and subtypes were collapsed into main items (41, 44).
The timeframe for the assessment of all the scales, other than PANSS and GAF, was lifetime. The timeframe of the PANSS was, as specified by its authors, “the previous week” but did not include descriptions by peers and surrounding professionals (33). The GAF was evaluated as current state at the time of evaluation (45). The interviews were split into several sessions if needed, depending on the participant’s capability. In such cases, the interview sessions were conducted with a short interval and within a maximum of a few weeks. The interviews were conducted between 1st April 2019 and 1st January 2021.
All interviews were either videotaped or audiotaped. The interviews were semi-structured, conversational, and phenomenologically orientated, encouraging faithful self-descriptions (39, 40). Items were only rated as present if the participants provided descriptions and examples that fitted a relevant item definition, i.e., an item was not rated as present based on a simple “yes” answer. All interviews were completed and there were no missing data.
The interviews were performed by the LL, an MD with several years of experience in clinical psychiatry, certified in the application of the EASE, and tested for interrater reliability for the EASE prior to the study with JN, a senior psychiatrist and researcher and certified EASE instructor (interrater reliability κ = 0.75). Further the interviewer LL is a PSE instructor at regular courses. Average duration of interviews was 4 h [range: 2 h and 45 min–7 h and 0 min].
Finally, all patients were allocated a “Best-Estimate Life-Time” ICD-10 diagnosis by LL. If any uncertainty about psychopathological phenomena or diagnosis occurred, JN or LSN, an experienced MD and certified EASE instructor, were consulted and extracts of interview recordings were evaluated jointly to reach consensus. Additionally, randomly selected videotaped interviews were jointly evaluated with respect to general psychopathology, EASE items, and overall consensus of best-estimate life-time diagnoses. In total, consensus ratings were performed in 26 (65%) of the included interviews. All items were rated conservatively i.e., if the presence of an item was considered doubtful, this item was consistently rated as absent.
If the participants reported any lifetime substance use, the diagnosis of schizophrenia, non-affective psychosis or schizotypal disorder was only made if the psychopathology could convincingly be related to periods in which the individuals had not used any substances for more than 6 months of abstinence or significant psychopathology present prior to onset of substance use.
We grouped the diagnoses according to the ICD-10 hierarchy with (1) schizophrenia and non-affective psychosis; (2) schizotypal disorder; (3) other mental disorders; (4) no mental disorder.
The study was evaluated by the National Committee on Health Research Ethics, journal no. 18-000080, and was concluded not to fall under the Health Research Act. The study was approved by the Danish Data Protection Agency, journal no. REG-064-2018.
If mental disorders requiring psychiatric treatment were identified during the interviews, the participants were referred to a relevant mental health service.
We dichotomized the diagnostic variables by merging the data into diagnostic groups of schizophrenia spectrum disorders, i.e., schizophrenia, non-affective psychosis and schizotypal disorder (43), and a group of other mental disorders. We tested for association between schizophrenia spectrum disorder and social functioning as measured by GAF-F, GAF-S, and total PANSS sum score applying t-test. The assumption of normal distribution was tested using Shapiro-Wilk test. The GAF-S and GAF-F scales were scored as continuous scales (37). For the variables GAF-F score and PANSS sum score the assumption of normal distribution was not fulfilled, and we therefore used the non-parametric Wilcoxon Signed Rank test to test for differences between groups.
We used ANOVA to compare EASE mean scores between the diagnostic groups (schizophrenia, schizotypal disorder, other mental disorder, and no mental disorder). We corrected for multiple testing by Scheffe’s test (46).
All analyses were conducted using SAS Enterprise Guide 7.1. Significance level was set to 0.05.
A total of 40 participants were included in the study with a mean age of 24 years, 53% male.
The typical participant had received non-medical welfare benefits for more than 1 year (mean 90 weeks, range [27.8–317.3]), had in at least one prior period received non-medical welfare benefits (n = 26, range [1–7 episodes]), and had an educational level of compulsory education or less (48%). In the majority of cases, there was a history of frequent disruptions to educational plans or vocational attachments (73%). In addition, the typical participant lived alone and was not in a relationship (55%), had parents that suffered from mental disorders or substance use problems (71%), and the participant had been in contact with mental health services in childhood or adolescence (42%). About one third had not completed final exams in compulsory school (30%). The sample had mean GAF-F 49.0 (IQR: 45.0–58.0).
We found that 38 (95%) participants fulfilled the criteria for a lifetime diagnosis of a mental disorder, and 21 (53%) were allocated a diagnosis of schizophrenia spectrum disorder. More specifically 10 participants fulfilled the diagnostic criteria for schizophrenia, 9 for schizotypal disorder, and 2 for unspecified non-affective psychosis. The distribution of disorders among the sample is presented in Figure 2.
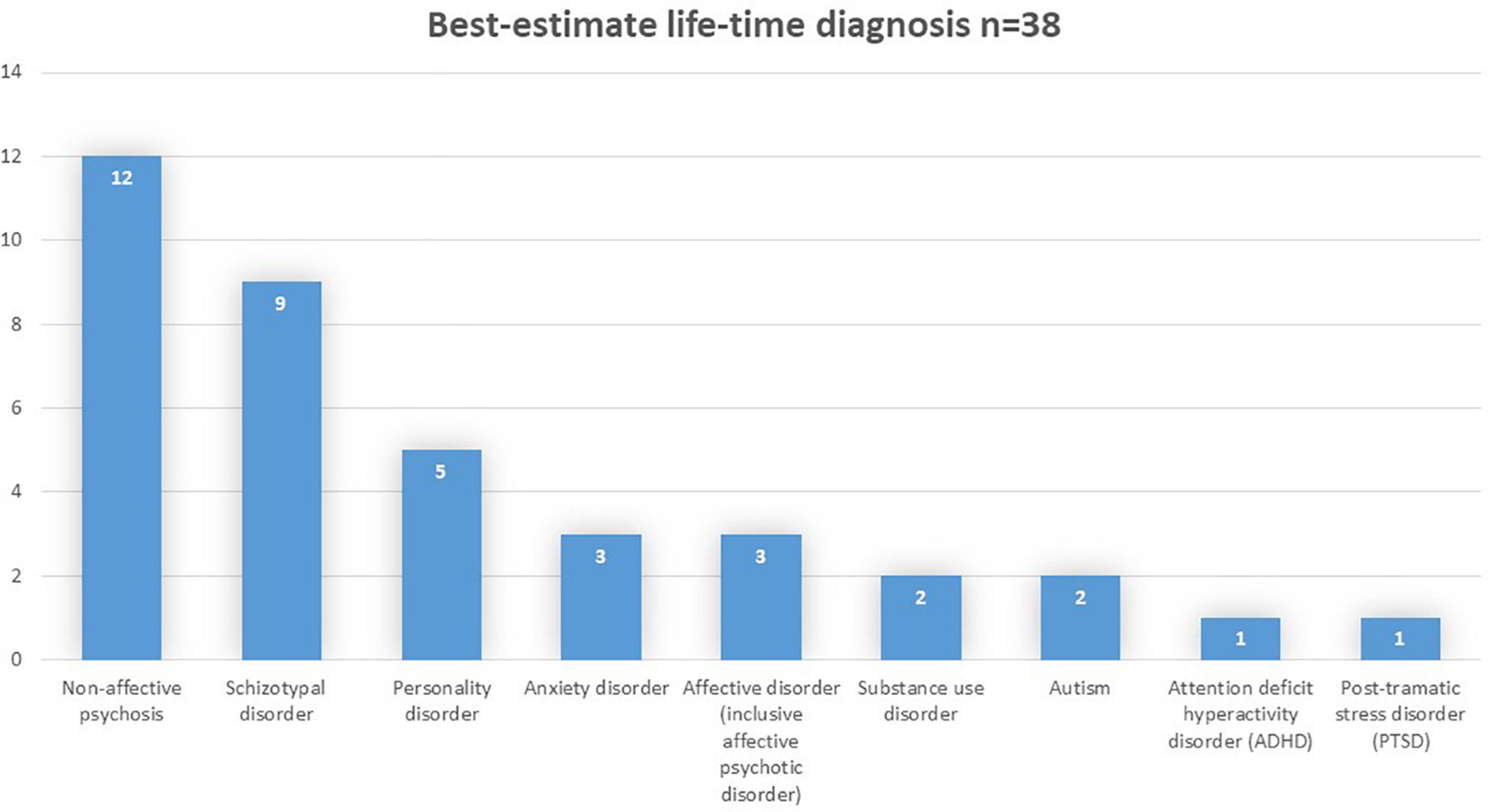
Figure 2. Distribution of mental disorders.
Only 2 participants did not meet the diagnostic criteria of any mental disorder. One of these was newly diagnosed with a chronic somatic disease that explained the reduced ability to engage in education and work. The other was during his school years suspected of having an attention deficit disorder, but the diagnostic outcome of the prior mental examination remained unclear. The interview revealed only vague symptomatology with social withdrawal as the most prominent finding, and no diagnosis of any mental disorder could be allocated in the present study.
For two participants, clear psychopathological phenomena were only present during periods with ongoing substance use, and they were therefore only assigned a diagnosis of substance use.
Among the 21 participants who were diagnosed with a schizophrenia spectrum disorder in the study 14 were already in contact with the psychiatric services: 5 of those were diagnosed with schizotypal disorder, 2 with schizophrenia and 7 with a non-schizophrenia spectrum disorder.
The participants who fulfilled the criteria for a schizophrenia spectrum disorder had mean EASE score of 11.8 (SD: 1.7). The EASE mean scores were significantly higher for participants with a diagnosis of schizophrenia, other non-affective psychoses or schizotypal disorder than for participants with other mental disorders and no mental disorders (Table 1). Correspondingly, participants with schizophrenia spectrum disorders scored lower than participants with other mental disorders on GAF-F [median: 48.0 (IQR 41.0–50.0) vs. 55.0 (IQR 49.0–69.0)] and GAF-S [mean 52.1 (SD 11.3) vs. 64.8 (SD 8.0)] and higher on PANSS [median 50.0 (IQR 40.0–57.0) vs. 34.0 (IQR 31.0–41.0)]. The median PANSS positive score was 11.0 (IQR 7.0), the median PANSS negative score was 11.0 (IQR 7.0) and the median PANSS general score was 25.0 (IQR 9.0) in the subgroup.

Table 1. Distribution among the study population of diagnoses allocated by assessment, previous lifetime clinical diagnoses, and EASE scores.
We here present two illustrative cases from the schizophrenia spectrum disorder group.
A 28-year-old female grew up in a family of four. She had social difficulties throughout childhood and adolescence; she had no friends and became anxious around other people. She had a hard time keeping up with the schoolwork and did not have any interests. She finished high school with low grades, partly because she had a depressed period after a break-up with a boyfriend. She dropped out of university after a few months. Later, she moved in with a friend and tried four times to start an education but dropped out repeatedly.
She was assessed in the mental health services under the diagnosis of social anxiety and started psychotherapy in group sessions but withdrew because she was unable to be in sessions with others.
For 3 years she had experienced the presence of a male person sitting on her shoulder, talking into her ear with criticizing statements about her and giving her commands that she felt obliged to obey. Still present, and reaching back as long as she could remember, she had felt the constant presence of yet another person and described herself as spiritually “open to anything.” She never felt that she had any real purpose or meaning in life and often questioned a lot of things seemingly without any special relevance to her: “Why do we have doors, is that really smart? Or who invented the door? Is the color of the door the same to me as it is to you?” Often, she would hear her name being shouted out loud. On a daily basis she experienced thinking about random experiences that seemed to be of no specific relevance to her, but nonetheless would play over and over again, even though she tried to get rid of them. Such thoughts would often play out like an inner picture or movie. She wondered if the world was real or “just a dream in some way,” and when standing on the railway station she might ponder if the people in the train would still exist, when she could no longer see them.
Auditory hallucinations and delusions had thus been present for more than 3 years. Currently, she experienced ongoing vague auditory hallucinations and negative symptoms. Additionally, she described Anwesenheit, a diminished sense of basic self, loss of common sense, social anxiety, primary self-reference, ambivalence, perceptual disturbances, mirror-phenomenon, hyperreflectivity, and solipsistic experiences. Her EASE score was 19, PANSS 37, GAF-S 50, and GAF-F 45. Best estimate lifetime diagnosis: Paranoid schizophrenia.
A 22-year-old male grew up with his mother, who suffered from periodic depression, and he only saw his father on rare occasions. In school, he had anger management issues, but later he became more withdrawn. He had social difficulties and ended up playing computer games and not attending school. He moved to live with his mother’s sister due to problems at home. At age 16–18, he was seen in a child and adolescent psychiatric outpatient clinic and was diagnosed with an attention deficit disorder. Medication helped somewhat on his concentration in school. He went to boarding school, where he had one close friend. He was seen twice in the psychiatric emergency department with suicidal thoughts during this period. He was enrolled in a vocational track in higher education but never showed up. The job-counseling center arranged a traineeship in a shop, which he attended for 4 months but with frequent absence—“then the whole thing went haywire.” He was diagnosed with depression at age 19 and 1 year later he was hospitalized after a suicidal attempt and diagnosed with acute stress reaction.
Social interactions scared him, as he feared to catch people’s attention. He described having many scary thoughts which he initially refused to elaborate on, but whose physical location he showed by placing his hand at the back of his head. After a break in the interview he described further that those “scary thoughts” placed in the back of his head included hearing an ongoing voice, which was not his own, talking to him and addressing his appearance in a devaluating way, always naming him in second person, for instance “you are a bad person.” The voice was described as being “just on repeat.” In addition, he described the voice as being out of his control which scared him. He was not able to reflect further on the experience and in the following just referred to it as “bad thoughts.”
He described auditory hallucinations for at least several months, perhaps longer. He did not describe symptoms of affective disorder, bur harbored pronounced negative symptoms. Additionally, he described spatialization of experience, hyperreflectivity, social anxiety, self-reference, and thought pressure, but had major difficulties verbalizing his psychopathological experiences. His EASE score was 5, PANSS 56, GAF-S 45, and GAF-F 41. Best estimate diagnosis: Non-organic Psychosis Not Otherwise Specified.
We examined a NEET population recruited from outside the mental health services for psychopathology and found that almost all participants qualified for a diagnosis of a mental disorder and that schizophrenia spectrum disorders were the most common. The 53% of the participants, who suffered from a schizophrenia spectrum diagnosis, had higher EASE mean scores and lower global functioning than the rest of the sample.
One third of the participants met the diagnostic criteria for an ICD-10 schizophrenia spectrum disorder but they were not in contact with the mental health services. More than half of the participants who fulfilled the diagnostic criteria of schizophrenia spectrum disorders were in contact with the mental health services but diagnosed with disorders outside this spectrum.
This could reflect that the subgroup meeting diagnostic criteria for schizophrenia spectrum disorders in our sample was less symptomatic than many other schizophrenia spectrum samples described in the literature. This is illustrated, e.g., by a low median PANSS total score of 50.0, which is on par with scores often reported at discharge from psychiatric admissions in schizophrenia spectrum cohorts (47, 48). The mean EASE score of 11.8, is lower than found in studies examining patient samples though one study reported a mean EASE score of 15.5. The most recent systematic review reported a total mean EASE score of 20.7 and 19.7 for schizophrenia and schizotypal disorder, respectively (49).
This low level of symptomatology could perhaps be explained by the illness being in an early phase at the time of the assessment in our study. This explanation is in line with the fact that a decline of social functioning often precedes the development of more obvious psychopathology in these disorders (26, 50). However, it is also well-established that a significant proportion of schizophrenia spectrum patients come across as relatively symptom-poor (51). Eugen Bleuler, who famously coined the concept of schizophrenia, explicitly noted that even manifestly ill patients may at a given time harbor—or at least be able to verbalize—rather few clear-cut symptoms. This, Bleuler noted, poses a significant diagnostic challenge, “because the attending physician cannot testify to the presence of mental disease, or because even if he has testified to it, the director of the mental hospital will occasionally release the patient as well or cured to the dismay of the desperate parents” (52) (p. 296). The existence of such symptom-poor schizophrenia spectrum patients, and the diagnostic conundrums they comprise, is addressed by several other classic psychopathological texts and clinical concepts (53–56). For example, Zilboorg described how such vaguely symptomatic patients, suffering from what he termed ambulatory schizophrenia “seldom reach the psychiatrist’s office for many reasons. First, they are considered by both the laity and the medical profession as merely weak people, “poor personalities,” “psychopathic personalities,” whatever these words may mean” (57) (p. 154).
Indeed, as noted by both Bleuler and Zilboorg, an ordinary clinical encounter with such a patient may reveal nothing particularly remarkable and raise no clear suspicion of a schizophrenia spectrum disorder. On the contrary it often takes an in-depth conversational interview that encourages the patient to reflect and elaborate on his experiences—and sometimes prolonged observation—to reach a valid diagnostic evaluation (39). This, however, is not just a time-consuming process, but also one that presupposes a great deal of clinical experience and sophisticated psychopathological knowledge on the part of the interviewer, all of which may be in short supply in contemporary clinical practice (58).
Importantly, self-disorders also play out in the intersubjective sphere. For example, many persons with self-disorders struggle with the experience of somehow being ontologically different that other people, or “not really human” (59) (p. 94) (i.e., diminished sense of basic self in the EASE). It seems to us that struggling with such experiences of profound dissimilarity might make it quite difficult to engage in social activities with others. Another example could be disturbances of the first-person perspective and hyper-reflection that in some cases lead to excessive forms of self-monitoring which operate alongside the person’s engagement with others thus impeding natural, effortless social interaction (60–62).
The population investigated in this study was not primarily help-seeking in the mental health services but was identified based on their claim of welfare benefits. In the Danish context, social caseworkers are the assessors of qualification for such claims and they are responsible for the evaluation of the young person’s current ability to participate in ordinary education or work. If there are coexisting difficulties, e.g., mental health problems, that hinder this process, the young person is entitled to a coordinated effort aimed at alleviating the problem at hand (30).
However, the complexity of this task seems undervalued. The severe mental health problems found among the NEET population demonstrate the difficulties that social caseworkers with no psychiatric training are faced with. As such they highlight the inherent problems in the physical and organizational separation of the social and mental health services that might, as pointed out in a BMJ editorial, result in insufficient attention being paid to the “double whammy” of NEET status and severe mental disorder (5, 63).
Our findings of a large proportion of schizophrenia spectrum disorders lend support to the guideline proposed by Meehl that a young individual’s gross underachievement seemingly unexplained by relevant factors should—in and of itself—lead the clinician to suspect a schizophrenia spectrum disorder (64). It should prompt a comprehensive differential-diagnostic evaluation as a first glance paucity of overt symptomatology does not rule out the presence of serious mental illness. As noted by Hoch: “A snake in the grass is not a “latent” snake nor a “larval” snake; it is a snake. And it is not concealed by the grass if one looks for it” (65) (p. 724).
This point seems of particular importance to the NEET population, which may be retained in an already disadvantaged position by ineffective psychiatric treatment and inaccurate evaluations in the job-counseling service, if psychotic disorders are not properly detected.
The principal strength of this study is the comprehensive phenomenological interviews performed by an experienced clinician and the consensus ratings of the psychopathological material. Further, the study was carried out with few exclusion criteria in the real-life setting of a job-counseling center thus enhancing external validity. The ratings were conservative and if it was doubtful if items were present, this item was consistently rated as absent.
The main limitation, on the other hand, is the small sample size. This is a feature of the study’s design with lengthy interviews but also reflects its setting and target group. The study did experience recruitment difficulties with inefficient invitation by the caseworkers among the eligible participants in addition to difficulties in establishing contact with those eligible participant who had accepted the invitation to join. Former studies have described similar difficulties when recruiting among the inactive youth population (66, 67).
It cannot be ruled out, that there was a selection bias built into the invitation procedure of the study, with the caseworkers perhaps being more prone to invite participants whom they believed to be in need of psychiatric assistance. However, the possible effect of such a bias is not univocal. It could be that those not invited were more difficult to reach with an even lower level of functioning and thus, assumingly, an even greater risk of severe mental health problems. Investigating the NEET youth population in a job-counseling center could itself have a built-in selection contributing to the findings of low levels of obvious symptomatology. One could suspect that an even more disadvantaged NEET population with more severe symptomatology might never reach the job-counseling center.
Including NEETs that were already known to have mental disorders in this study did affect the results i.e., a small part of the sample was already previously diagnosed with schizophrenia spectrum disorders. On the one hand, excluding the subjects that were previously diagnosed with mental disorders might have given a more accurate estimate of unrecognized mental disorders. But on the other hand, we found some of the schizophrenia spectrum disorders to be unrecognized among NEETs who had been misdiagnosed with disorders outside the spectrum. Another limitation was the inclusion criterion requiring participants to be fluently Danish speaking. However, this was considered a necessary means to ensuring meaningful participation in in-depth phenomenological interviews.
The psychiatric examination of a NEET youth sample in a job-counseling service setting revealed that 95% qualified for a diagnosis of any mental disorder. More than half of the sample was diagnosed with a schizophrenia spectrum disorder. The schizophrenia spectrum disorders among the studied sample had a symptom-poor presentation with low PANSS and EASE scores. These findings suggest that pronounced social disconnection in youth—in and of itself—should lead to the suspicion of a serious mental disorder.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Danish National Committee on Health Research Ethics, journal no. 18-000080/Danish Data Protection Agency, journal no. REG-064-2018. The patients/participants provided their written informed consent to participate in this study.
LL collected the data, performed the statistical analyses, and wrote the first draft of the manuscript. LL, LN, and JN performed the data management. JN and LN contributed to the writing of the manuscript. All authors participated in designing the study, contributed to the revision of the manuscript, which in its present version has been approved by all authors.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ralston K, Everington D, Feng ZQ, Dibben C. Economic inactivity, not in employment, education or training (NEET)and scarring: the importance of NEET as a marker of long-term disadvantage. Work Employ Soc. (2021) 36:59–79. doi: 10.1177/0950017020973882
2. Schultz-Nielsen ML. Den økonomiske Gevinst ved at Inkludere de Udsatte unge. København: Rockwool Fondens Forskningsenhed (2016)
3. Eurofound. NEETs—Young People not in Employment, Education or Training: Characteristics, Costs and Policy Responses in Europe. Luxembourg: Publications Office of the European Union (2012).
4. Serracant P. A brute indicator for a NEET case: genesis and evolution of a problematic concept and results from an alternative indicator. Soc Indicat Res. (2014) 117:401–19. doi: 10.1007/s11205-013-0352-5
5. OECD. Sick on the Job?: Myths and Realities about Mental Health and Work. Paris: Organisation for Economic Co-operation Development (2012).
6. Eurostat. Statistics on Young People Neither in Employment nor in Education or Training. (2020). Available online at: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Statistics_on_young_people_neither_in_employment_nor_in_education_or_training [accessed 10 July 2021].
7. Rodwell L, Romaniuk H, Nilsen W, Carlin JB, Lee KJ, Patton GC. Adolescent mental health and behavioural predictors of being NEET: a prospective study of young adults not in employment, education, or training. Psychol Med. (2018) 48:861–71. doi: 10.1017/S0033291717002434
8. Gutierrez-Garcia RA, Benjet C, Borges G, Mendez Rios E, Medina-Mora ME. NEET adolescents grown up: eight-year longitudinal follow-up of education, employment and mental health from adolescence to early adulthood in Mexico City. Eur Child Adolesc Psychiatry. (2017) 26:1459–69. doi: 10.1007/s00787-017-1004-0
9. Gutierrez-Garcia RA, Benjet C, Borges G, Mendez Rios E, Medina-Mora ME. Emerging adults not in education, employment or training (NEET): socio-demographic characteristics, mental health and reasons for being NEET. BMC Public Health. (2018) 18:1201. doi: 10.1186/s12889-018-6103-4
10. Uchida Y, Norasakkunkit V. The NEET and Hikikomori spectrum: assessing the risks and consequences of becoming culturally marginalized. Front Psychol. (2015) 6:1117. doi: 10.3389/fpsyg.2015.01117
11. Teo AR, Gaw AC. Hikikomori, a Japanese culture-bound syndrome of social withdrawal : a proposal for DSM-5. J Nerv Ment Dis. (2010) 198:444–9. doi: 10.1097/NMD.0b013e3181e086b1
12. Benjet C, Hernandez-Montoya D, Borges G, Mendez E, Medina-Mora ME, Aguilar-Gaxiola S. Youth who neither study nor work: mental health, education and employment. Salud Publica Mex. (2012) 54:410–7. doi: 10.1590/S0036-36342012000400011
13. Symonds J, Dietrich J, Chow A, Salmela-Aro K. Mental health improves after transition from comprehensive school to vocational education or employment in England: a national cohort study. Dev Psychol. (2016) 52:652–65. doi: 10.1037/a0040118
14. Power E, Clarke M, Kelleher I, Coughlan H, Lynch F, Connor D, et al. The association between economic inactivity and mental health among young people: a longitudinal study of young adults who are not in employment, education or training. Ir J Psychol Med. (2015) 32:155–60. doi: 10.1017/ipm.2014.85
15. Basta M, Karakonstantis S, Koutra K, Dafermos V, Papargiris A, Drakaki M, et al. NEET status among young Greeks: association with mental health and substance use. J Affect Disord. (2019) 253:210–7. doi: 10.1016/j.jad.2019.04.095
16. Berry C, Easterbrook MJ, Empson L, Fowler D. Structured activity and multiple group memberships as mechanisms of increased depression amongst young people not in employment, education or training. Early Interv Psychiatry. (2019) 13:1480–7. doi: 10.1111/eip.12798
17. Baggio S, Iglesias K, Deline S, Studer J, Henchoz Y, Mohler-Kuo M, et al. Not in Education, Employment, or Training status among young Swiss men. Longitudinal associations with mental health and substance use. J Adolesc Health. (2015) 56:238–43. doi: 10.1016/j.jadohealth.2014.09.006
18. Gariepy G, Iyer S. The mental health of young Canadians who are not working or in school. Can J Psychiatry. (2019) 64:338–44. doi: 10.1177/0706743718815899
19. Goldman-Mellor S, Caspi A, Arseneault L, Ambler A, Danese A, Fisher H, et al. Committed to work but vulnerable: self-perceptions and mental health in NEET 18-year olds from a contemporary British cohort. J Child Psychol Psychiatry. (2016) 57:196–203. doi: 10.1111/jcpp.12459
20. Gariépy G, Danna SM, Hawke L, Henderson J, Iyer SN. The mental health of young people who are not in education, employment, or training: a systematic review and meta-analysis. Soc Psychiatry Psychiatr Epidemiol. (2021) 57:1107–21. doi: 10.1007/s00127-021-02212-8
21. Lindhardt L, Storebø OJ, Bruun LS, Simonsen E, Mortensen OS. Psychosis among the disconnected youth: a systematic review. Cogent Psychol. (2022) 9:2056306. doi: 10.1080/23311908.2022.2056306
22. Addington J, Addington D. Patterns of premorbid functioning in first episode psychosis: relationship to 2-year outcome. Acta Psychiatr Scand. (2005) 112:40–6. doi: 10.1111/j.1600-0447.2005.00511.x
23. Stilo SA, Gayer-Anderson C, Beards S, Hubbard K, Onyejiaka A, Keraite A, et al. Further evidence of a cumulative effect of social disadvantage on risk of psychosis. Psychol Med. (2017) 47:913–24. doi: 10.1017/S0033291716002993
24. Marwaha S, Johnson S. Schizophrenia and employment - a review. Soc Psychiatry Psychiatr Epidemiol. (2004) 39:337–49. doi: 10.1007/s00127-004-0762-4
25. Häfner H, Löffler W, Maurer K, Hambrecht M, an der Heiden W. Depression, negative symptoms, social stagnation and social decline in the early course of schizophrenia. Acta Psychiatr Scand. (1999) 100:105–18. doi: 10.1111/j.1600-0447.1999.tb10831.x
26. Kvig EI, Brinchmann B, Moe C, Nilssen S, Larsen TK, Sorgaard K. “Lanthanic Presentation” in first-episode psychosis predicts long service delay: the challenge of detecting masked psychosis. Psychopathology. (2017) 50:282–9. doi: 10.1159/000478989
27. Velthorst E, Fett AJ, Reichenberg A, Perlman G, van Os J, Bromet EJ, et al. The 20-year longitudinal trajectories of social functioning in individuals with psychotic disorders. Am J Psychiatry. (2017) 174:1075–85. doi: 10.1176/appi.ajp.2016.15111419
28. Griffiths SL, Wood SJ, Birchwood M. Vulnerability to psychosocial disability in psychosis. Epidemiol Psychiatr Sci. (2019) 28:140–5. doi: 10.1017/S2045796018000495
29. Klosterkötter J, Schultze-Lutter F, Bechdolf A, Ruhrmann S. Prediction and prevention of schizophrenia: what has been achieved and where to go next? World Psychiatry. (2011) 10:165–74. doi: 10.1002/j.2051-5545.2011.tb00044.x
30. Retsinformation. Bekendtgørelse af lov om Aktiv Socialpolitik (act on active social policy). (2021). Available online at: https://www.retsinformation.dk/eli/lta/2021/241 [accessed February 12, 2021].
31. Reneflot A, Evensen M. Systematic literature review unemployment and psychological distress among young adults in the Nordic countries: a review of the literature. Int J Soc Welf. (2014) 23:3–15. doi: 10.1111/ijsw.12000
32. McGuffin P, Farmer A, Harvey I. A polydiagnostic application of operational criteria in studies of psychotic illness. Development and reliability of the OPCRIT system. Arch Gen Psychiatry. (1991) 48:764–70. doi: 10.1001/archpsyc.1991.01810320088015
33. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
34. Gross GHG, Klosterkötter J, Linz M. Bonner Skala für die Beurteilung von Basissymptomen. Berlin: Springer-Verlag (1987).
35. Koehler K. First rank symptoms of schizophrenia: questions concerning clinical boundaries. Br J Psychiatry. (1979) 134:236–48. doi: 10.1192/bjp.134.3.236
36. Parnas J, Moller P, Kircher T, Thalbitzer J, Jansson L, Handest P, et al. EASE: examination of anomalous self-experience. Psychopathology. (2005) 38:236–58. doi: 10.1159/000088441
37. Aas IH. Global Assessment of Functioning (GAF): properties and frontier of current knowledge. Ann Gen Psychiatry. (2010) 9:20. doi: 10.1186/1744-859X-9-20
38. Piersma HL, Boes JL. The GAF and psychiatric outcome: a descriptive report. Community Ment Health J. (1997) 33:35–41. doi: 10.1023/A:1022413110345
39. Nordgaard J, Revsbech R, Saebye D, Parnas J. Assessing the diagnostic validity of a structured psychiatric interview in a first-admission hospital sample. World Psychiatry. (2012) 11:181–5. doi: 10.1002/j.2051-5545.2012.tb00128.x
40. Nordgaard J, Sass LA, Parnas J. The psychiatric interview: validity, structure, and subjectivity. Eur Arch Psychiatry Clin Neurosci. (2013) 263:353–64. doi: 10.1007/s00406-012-0366-z
41. Nordgaard J, Nilsson LS, Sæbye D, Parnas J. Self-disorders in schizophrenia-spectrum disorders: a 5-year follow-up study. Eur Arch Psychiatry Clin Neurosci. (2018) 268:713–8. doi: 10.1007/s00406-017-0837-3
42. Nordgaard J, Henriksen MG, Berge J, Nilsson LS. First-rank symptoms and self-disorders in schizophrenia. Schizophr Res. (2019) 210:306–7. doi: 10.1016/j.schres.2019.06.027
43. Zandersen M, Parnas J. Exploring schizophrenia spectrum psychopathology in borderline personality disorder. Eur Arch Psychiatry Clin Neurosci. (2020) 270:969–78. doi: 10.1007/s00406-019-01039-4
44. Nordgaard J, Parnas J. Self-disorders and the schizophrenia spectrum: a study of 100 first hospital admissions. Schizophr Bull. (2014) 40:1300–7. doi: 10.1093/schbul/sbt239
45. American Psychiatric A, Frances A, First MB, Pincus HA. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV. IV ed. Washington, DC: American Psychiatric Association (1994).
46. Scheffé H. A “MIXED MODEL” FOR THE ANALYSIS OF VARIANCE. Ann. Math. Statist. (1956) 27:23–36. doi: 10.1214/aoms/1177728348
47. Schennach R, Riedel M, Obermeier M, Spellmann I, Musil R, Jäger M, et al. What are residual symptoms in schizophrenia spectrum disorder? Clinical description and 1-year persistence within a naturalistic trial. Eur Arch Psy Clin N. (2015) 265:107–16. doi: 10.1007/s00406-014-0528-2
48. Wang D, Gopal S, Baker S, Narayan VA. Trajectories and changes in individual items of positive and negative syndrome scale among schizophrenia patients prior to impending relapse. NPJ Schizophr. (2018) 4:10. doi: 10.1038/s41537-018-0056-6
49. Henriksen MG, Raballo A, Nordgaard J. Self-disorders and psychopathology: a systematic review. Lancet Psychiatry. (2021) 8:1001–12. doi: 10.1016/S2215-0366(21)00097-3
50. Owens DG, Miller P, Lawrie SM, Johnstone EC. Pathogenesis of schizophrenia: a psychopathological perspective. Br J Psychiatry. (2005) 186:386–93. doi: 10.1192/bjp.186.5.386
51. Nordgaard JJL. The Psychiatric Interview for Differential Diagnosis. I ed. Cham: Springer (2016).
53. Kahlbaum K, Berrios G, Kraam A. On heboidophrenia. Hist Psychiatry. (2002) 13:197–201. doi: 10.1177/0957154X0201305005
54. Hoch P, Polatin P. Pseudoneurotic forms of schizophrenia. Psychiatr Q. (1949) 23:248–76. doi: 10.1007/BF01563119
55. Diem O. The simple dementing form of dementia praecox. In: Cutting, J Shepherd M editors. The Clinical Roots of the Schizophrenia Concept: Translated from Die einfach demente Form der Dementia Praecox. (Vol. 37), Berlin: Archiv fur Psychiatrie und Nervenkrankheiten (1903). p. 81–7. doi: 10.1007/BF02227700
56. Blankenburg W. [Problems in latent schizophrenias]. Deutsche Medizinische Wochenschrift. (1968) 93:67–71. doi: 10.1055/s-0028-1105014
57. Zilboorg G. Ambulatory schizophrenia. Psychiatry. (1941) 4:149–55. doi: 10.1080/00332747.1941.11022329
58. Andreasen NC. DSM and the death of phenomenology in America: an example of unintended consequences. Schizophr Bull. (2007) 33:108–12. doi: 10.1093/schbul/sbl054
60. Salice A. The disrupted ‘we’: schizophrenia and collective intentionality. J Conscious Stud. (2015) 22:145–71.
61. Nilsson LS, Urfer Parnas A, Nordgaard J. Social life in the schizophrenia spectrum: a phenomenological study of five patients. Psychopathology. (2019) 52:232–9. doi: 10.1159/000501833
62. Salice A, Henriksen MG. Disturbances of shared intentionality in schizophrenia and Autism. Front Psychiatry. (2020) 11:570597. doi: 10.3389/fpsyt.2020.570597
63. Scott J, Fowler D, McGorry P, Birchwood M, Killackey E, Christensen H, et al. Adolescents and young adults who are not in employment, education, or training. BMJ. (2013) 347:f5270. doi: 10.1136/bmj.f5270
64. Meehl PE. Manual for Use with Checklist of Schizotypic Signs. Minnesota: Psychiatric Research Unit University of Minnesota Medical School Minneapolis (1964).
65. Hoch PH. Differential Diagnosis in Clinical Psychiatry: The Lectures of Paul H. Hoch: Science House (1972).
66. Reissner V, Rosien M, Jochheim K, Kuhnigk O, Dietrich H, Hollederer A, et al. Psychiatric disorders and health service utilization in unemployed youth. J Public Health. (2011) 19:13–20. doi: 10.1007/s10389-010-0387-x
Keywords: schizophrenia spectrum disorder, NEET, psychopathology, social disconnection, psychosis
Citation: Lindhardt L, Nilsson LS, Munk-Jørgensen P, Mortensen OS, Simonsen E and Nordgaard J (2022) Unrecognized schizophrenia spectrum and other mental disorders in youth disconnected from education and work-life. Front. Psychiatry 13:1015616. doi: 10.3389/fpsyt.2022.1015616
Received: 09 August 2022; Accepted: 30 September 2022;
Published: 26 October 2022.
Edited by:
Rosa Ritunnano, University of Birmingham, United KingdomReviewed by:
Jordan Sibeoni, Université de Paris, FranceCopyright © 2022 Lindhardt, Nilsson, Munk-Jørgensen, Mortensen, Simonsen and Nordgaard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Line Lindhardt, bGlubGlAcmVnaW9uc2phZWxsYW5kLmRr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.