 Suting Chen
Suting Chen Hang Hong2
Hang Hong2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 10 October 2022
Sec. Public Mental Health
Volume 13 - 2022 | https://doi.org/10.3389/fpsyt.2022.1004318
Background: Depressive symptoms were common among HIV/AIDS patients. Previous studies had shown that HIV-infected patients were twice as likely to be diagnosed with depression as the general population. However, only few studies have explored the prevalence and related factors of depressive symptoms among HIV/AIDS in China.
Materials and methods: A cross-sectional study was conducted to study the prevalence of depressive symptoms among HIV/AIDS from January to December 2021 through the database of HIV/AIDS antiretroviral therapy and psychological evaluation system in Ningbo, China. The Patient Health Questionnaire-2 (PHQ-2) was used to screen for depressive symptoms (PHQ-2 > 0), the Patient Health Questionnaire-9 (PHQ-9) was used to diagnose depressive symptoms, and multivariate Logistic regression model was carried on to evaluate the related factors.
Results: A total of 3,939 HIV/AIDS patients were enrolled, and the age of initiation of antiretroviral therapy was 37.15 (IQR = 28.41–48.73) years. Among them, 3,230 (82.00%) were male, 3,844 (97.59%) were Han nationality, 1,391 (35.49%) were unmarried, 1,665 (42.27%) were homosexual transmission, and 2,194 (55.70%) were HIV-infected patients. There were 265 patients (6.73%) with depressive symptoms, and the proportion of mild, moderate, moderate and severe depressive symptoms was 4.01% (158/3939), 1.65% (65/3939), 0.76% (30/3939), and 0.30% (12/3939), respectively. Multivariate analysis showed that married [odds ratio (OR) = 0.675, 95% CI = 0.501–0.908], divorced or widowed (OR = 0.571, 95% CI = 0.380–0.860), homosexual transmission (OR = 1.793, 95% CI = 1.349–2.396) were associated with depressive symptoms among HIV/AIDS.
Conclusion: The prevalence of depressive symptoms among HIV/AIDS patients was 6.73% in Ningbo, China. More attention should be paid to the psychological status of unmarried and homosexual HIV/AIDS patients in Ningbo and timely psychological intervention or treatment should be given to those patients with depressive symptoms.
The widespread application of antiretroviral therapy has greatly reduced the morbidity and mortality of HIV/AIDS patients, thus realizing the goals of HIV suppression and prolonging the life of patients (1, 2). The improvement of life quality among HIV/AIDS was accompanied by the onset of some psychiatric symptoms such as depression (3–5). It was estimated that depression alone may be one of the three leading causes of disease burden in low-income countries by 2030 (6, 7). Therefore, preventing the incidence of depression is extremely important among HIV/AIDS patients.
The incidence of depressive symptoms was higher among HIV-infected patients (8–11). Previous studies have shown that people living with HIV were twice as likely as the general population to be diagnosed with depression (10). Depression is a debilitating condition that adversely affects adherence to antiretroviral therapy and viral suppression among HIV/AIDS (12–15), thereby reducing the life quality of patients (16). It has been found that the 2-year mortality risk of those with depressive symptoms was 9.7%, higher than that of those without depressive symptoms among HIV-infected patients who inject drugs (17). Recent systematic reviews about the relationship between HIV and depressive symptoms showed that depressive symptoms were associated with gender, age, marital status, economic level, social support, HIV-1 RNA level, CD4 count, antiviral therapy, sexual transmission, opportunistic infections and social stigma among HIV/AIDS (18–22).
The prevalence and related factors of depressive symptoms among HIV/AIDS have been rarely studied in China; yet there is a need to investigate the related factors of depressive symptoms among HIV/AIDS. Therefore, in order to understand the depressive symptoms and related factors in HIV/AIDS patients, further improve the compliance of antiretroviral therapy and life quality of patients, this study conducted a cross-sectional study among HIV/AIDS patients who had been treated with antiretroviral therapy in Ningbo, China.
The HIV/AIDS patients in Ningbo before December 31, 2020 were selected. The inclusion and exclusion criteria were as follows. Inclusion criteria: (1) informed consent; (2) treatment status of HIV/AIDS was “new treatment,” “under treatment,” or “referral” and the card review mark was “final approval card”; (3) age ≥ 18 years; (4) psychological evaluation was conducted and the results were complete; (5) complete recent viral load information. Exclusion criteria: (1) informed consent was not obtained; (2) subjects of lost follow-up, death or long-term absence; (3) age < 18 years; (4) without psychological evaluation; (5) without recent viral load information.
Based on the database of HIV/AIDS antiretroviral therapy and the psychological evaluation network system of patients, the general demographic information, basic information of antiretroviral therapy and psychological evaluation information were collected from January to December 2021. The information includes: (1) general demographic information: gender, age, education, marital status, occupation, etc. (2) basic information of antiretroviral therapy: sexual transmission, WHO clinical stage, number of disease symptoms at baseline, positive date of HIV antibody test, start date of antiretroviral therapy, antiretroviral drugs, number of baseline CD4 + T lymphocytes (CD4 count for short), etc. (3) psychological evaluation information: The assessment of depressive symptoms was a two-stage screening. Follow-up doctors in Voluntary Counseling and Testing (VCT) outpatient initially provided antiretroviral therapy number, patients scanned the QR code of The Patient Health Questionnaire-2 (PHQ-2) (23) to screen for depressive symptoms. The Patient Health Questionnaire-9 (PHQ-9) (24) was used to diagnose depressive symptoms secondly if PHQ-2 scores higher than zero (Figure 1).
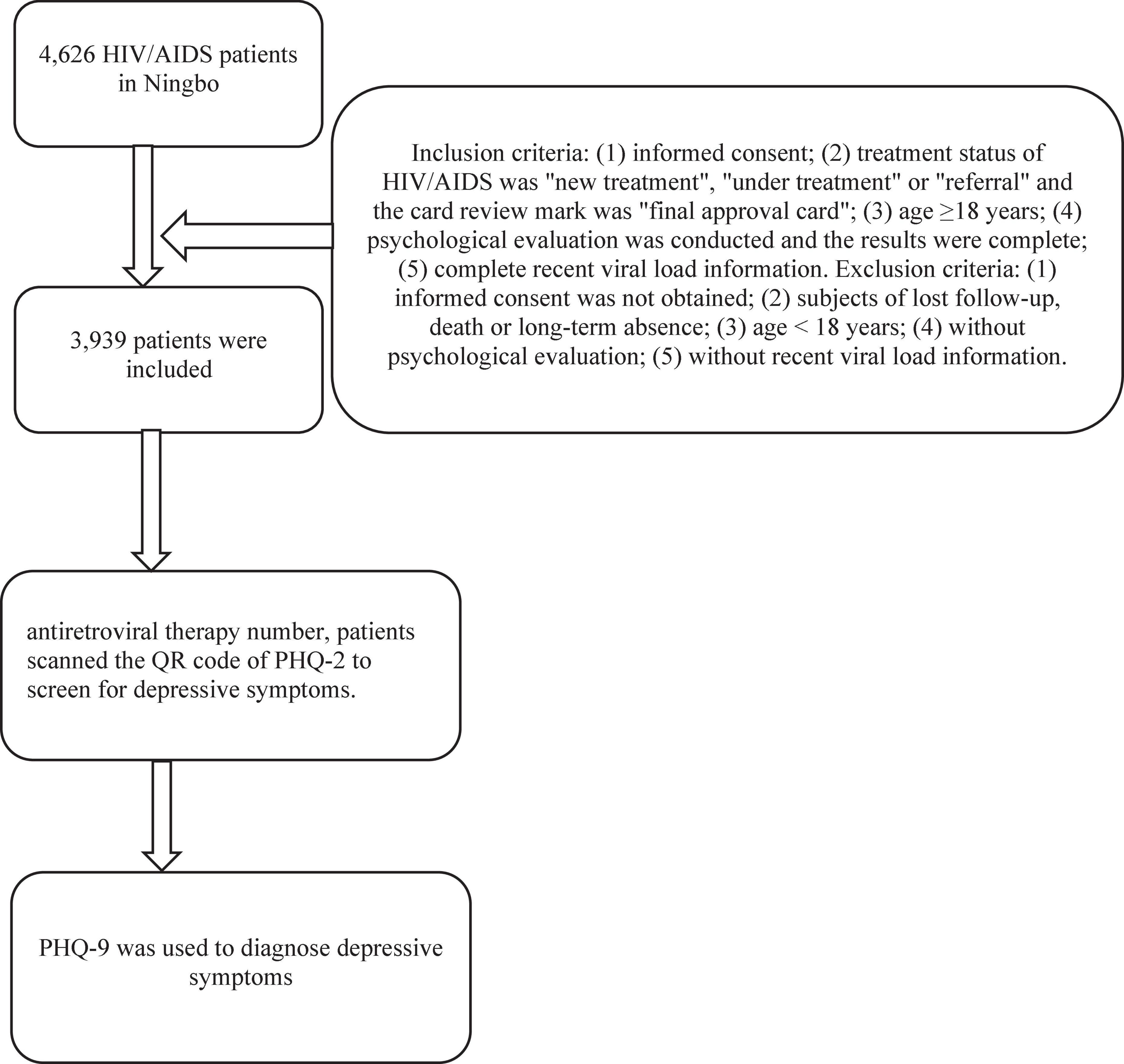
Figure 1. Flowchart for the data collection.
The PHQ-2 (23) scale consisted of two items and was rated from 0 (none at all) to 3 (almost daily). The contents include: (1) little interest or pleasure in doing things, (2) feeling down, depressed, or hopeless. There were nine items in the PHQ-9 (24) scale, and the score was 0 (not at all) to 3 (almost every day). These include: (1) little interest or pleasure in doing things, (2) feeling down, depressed, or hopeless, (3) trouble falling or staying asleep, or sleep too much, (4) feeling tired or having little energy, (5) poor appetite or overeating, (6) feeling bad about yourself-or that you are a failure or have let yourself or your family down, (7) trouble concentrating on things, such as reading the newspaper or watching television, (8) moving or speaking so slowly that other people could have noticed? Or the opposite-being so fidgety or restless that you have been moving around o lot more than usual, and (9) thoughts that you would be better off dead or hurting yourselves in some way.
The criteria for timely treatment was calculated by referring to the positive date of HIV antibody test and the start date of antiretroviral therapy, and the time interval between two dates ≤ 30 days was defined as timely treatment.
Participants with PHQ-9 scores higher than four was defined as patients with depressive symptoms in the second stage of psychological assessment (24). The PHQ-9 scale scores ranged from 5 to 9 as mild depressive symptoms, from 10 to 14 as moderate depressive symptoms, from 15 to 19 as moderate to severe depressive symptoms, and from 20 to 27 as severe depressive symptoms (24).
Statistical analysis was conducted using the Statistical Package for the Social Science (SPSS), version 26.0. Continuous data were expressed by geometric mean ± standard deviation, and differences between the depressive and non-depressive groups were examined by a completely randomized two-sample t-test or Wilcoxon rank-sum test. Categorical data were summarized by proportions, and differences between groups were examined by χ2 test. Multiple Logistic regression model (Forward: LR) was used to analyze the related factors of depressive symptoms, and P < 0.05 was considered statistically significant.
There were 4,626 HIV/AIDS patients in Ningbo before December 31, 2020, and 3,939 patients met the inclusion and exclusion criteria. Among 3,939 subjects, the initial age of antiretroviral therapy was 37.15 (IQR = 28.41–48.73) years. Of 3,939 participants, 3,230 were males (82.00%), 3,844 were Han nationality (97.59%), 1,391 were unmarried (35.49%), 1,367 had junior middle school education level (34.70%), 1,665 were homosexual transmission (42.27%). The time interval from HIV antibody positive to antiretroviral therapy ≤30 days accounted for 60.85%, and the primary treatment regimen was TDF + 3TC + EFV (56.79%) (TDF, tenofovir; 3TC, lamivudine; EFV, efavirenz). Among 3,939 HIV/AIDS patients, 2,194 were HIV infection (55.70%), and 1,745 were AIDS patients (44.30%). There were statistically significant differences between HIV infected patients and AIDS in terms of gender, age at which antiretroviral therapy started, education, marital status, occupation, household registration, WHO clinical stage, sexual transmission and initial treatment regime. Details see Table 1.
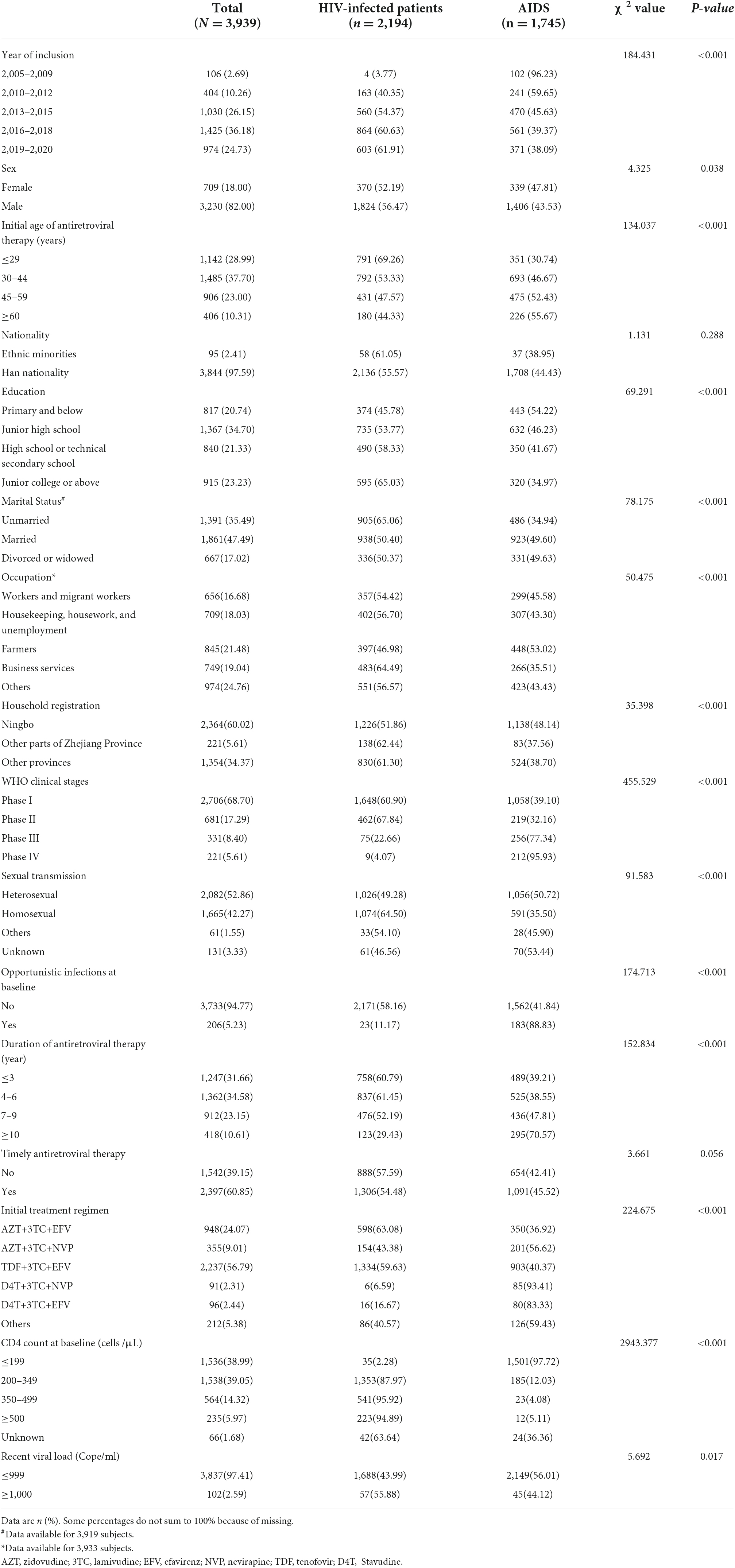
Table 1. Socio-demographic and related characteristics of participants.
Among 3,939 HIV/AIDS patients, WHO clinical stages were mainly in stage I (68.70%). There were 206 patients (5.23%) with opportunistic infections at baseline, mainly with recurrent severe bacterial infections (except pneumonia), pneumocystis pneumoniae pneumonia (PCP), and herpes zoster. The main clinical symptoms at baseline were fever (>37.5°C), skin lesions, and persistent diarrhea (adults > 1 month, children > 2 weeks). The proportion of baseline CD4 count < 200 cells/μL was 38.99%, and 200–349 cells/μL was 39.05%. There were 3,837 cases (97.41%) with the recent viral load <1,000 Cope/ml. HBsAg and anti-HCV were detected in 385 and 360 patients at baseline, respectively, of which 41 (10.65%) were HBsAg positive and 7 (1.94%) were anti-HCV positive. Details see Table 1.
Of 3,939 HIV/AIDS participants, 265 (6.73%) had depressive symptoms, 158 (4.01%) had mild depressive symptoms, 65 (1.65%) had moderate depressive symptoms, 30 (0.76%) had moderate to severe depressive symptoms, and 12 (0.30%) had severe depressive symptoms. The incidence rates of depressive symptoms were 6.93% (224/3,939) in males and 5.78% (41/3,939) in females, 7.34% (161/3,939) in HIV infected patients and 5.96% (104/3,939) in AIDS. As described in Table 2.
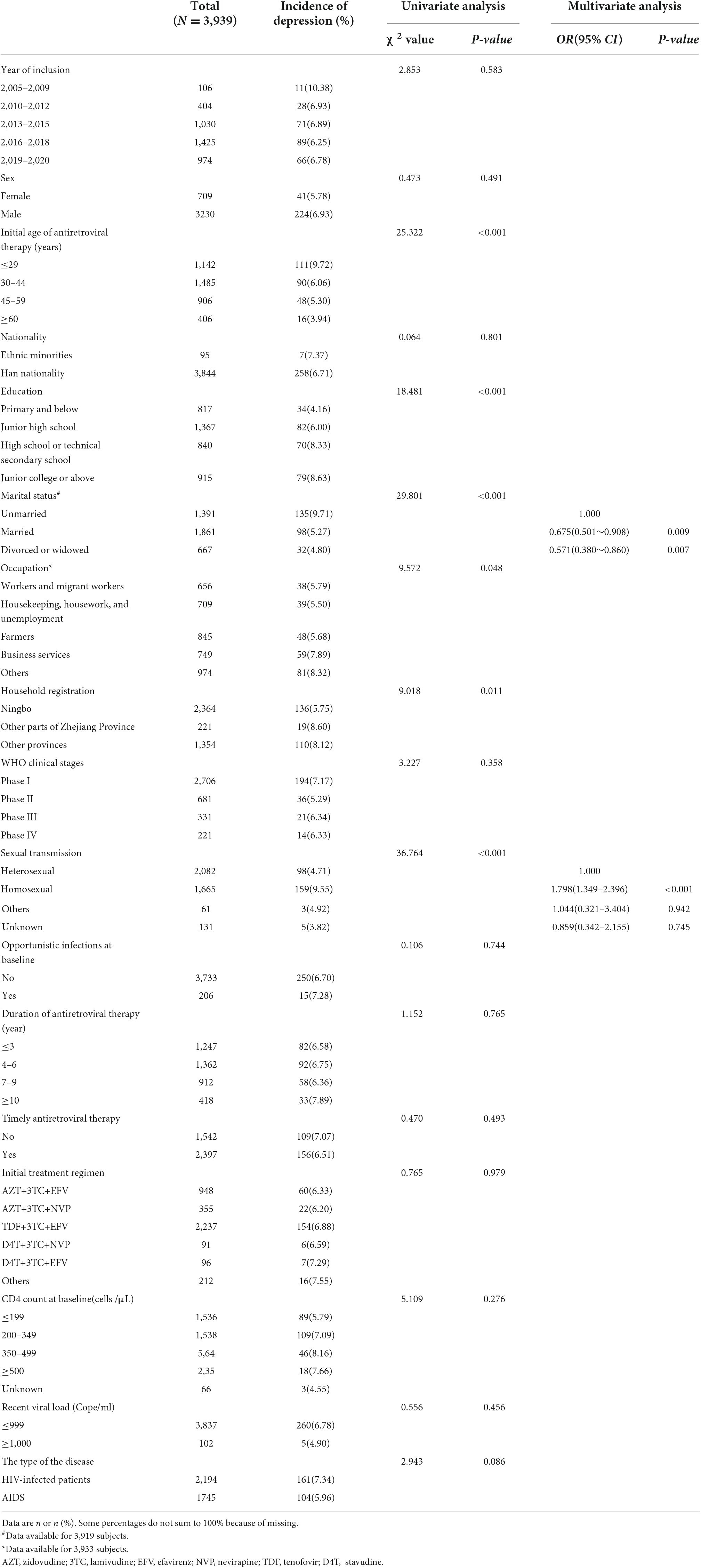
Table 2. Analysis on the related factors for depression among HIV/AIDS in Ningbo.
Univariate analysis showed that age, education, marital status, occupation, household registration and sexual transmission were related to depressive symptoms among HIV/AIDS. Multivariate Logistic regression model showed that unmarried status and homosexual transmission were significant risk factors for depressive symptoms among HIV/AIDS. Specifically, patients with married status and divorced or widowed status had about 0.675 times (95% CI = 0.501–0.908) and 0.571 times (95% CI = 0.380–0.860) greater risk for depressive symptoms compared to patients with unmarried status, the OR of depressive symptoms among HIV/AIDS with homosexual transmission was 1.793 (95% CI = 1.349–2.396) compared to those with heterosexual transmission. As shown in Table 2.
As a common depression screening method, both PHQ-2 scale and PHQ-9 scale had relatively good reliability and validity (23, 24). Previous studies had shown that the accuracy of combination with PHQ-2 and PHQ-9 for screening to detect major depression was more specific than using PHQ-2 alone (25), so the PHQ-2 was used as a pre-screening. In the present study, the PHQ-2 and PHQ-9 were combined to further improve the efficiency of diagnosis.
With the widespread application of antiretroviral therapy, more and more depressive symptoms occur in HIV/AIDS patients. Jiang et al. (26) found that the prevalence of depression was 18.33% among patients receiving antiretroviral therapy. The results of present study showed that the prevalence of depressive symptoms among HIV/AIDS in Ningbo was 6.73%, slightly lower than the prevalence of depressive symptoms among HIV infected patients reported in foreign cross-sectional study of 12,507 patients (8.7%) (27). Foreign studies have found that the prevalence of depressive symptoms in HIV-infected patients was approximately 20–79% (28–34), which was obviously higher than the results of this study. It could be due to differences in age, race, survey period and the tools used to define depressive symptoms. Among other HIV infected patients, the prevalence of moderate or higher depressive symptoms was over 10% (35–38), much higher than the result of present study of 2.72%.
In our study, the OR of having depressive symptoms among HIV/AIDS with married status and divorced or widowed status compared to those with unmarried status were 0.675 (95% CI = 0.501–0.908) and 0.571 (95% CI = 0.380–0.860), respectively. Unmarried HIV/AIDS patients were at greater risk of depressive symptoms, consistent with several previous studies (39–41).
The epidemics of HIV is stabilizing with the widespread use of antiretroviral therapy, HIV infection among men who have sex with men (MSM) continues to continue to increase in both developed and developing countries, with high rates of new infections especially among young MSM (42–44). In present study, participants with homosexual transmission were found to be a risk factor for depressive symptoms among HIV/AIDS compared to those with heterosexual transmission. Depressive symptoms were common among MSM with HIV infection (45, 46). It had also been reported that the incidence of depression or depressive symptoms among HIV-infected MSM in China was 43.9% (47). These results explain the conclusion of present manuscript in other perspectives. HIV-infected MSM faced further stigma and discrimination, as well as increased mental health challenges (48). Therefore, more attention should be paid to the psychological status of HIV/AIDS with homosexual transmission in Ningbo, and timely psychological intervention or treatment should be given to those patients with depressive symptoms.
The present study suffered from a few limitations. Firstly, depressive symptoms were determined by scale rather than clinical “gold standard,” and the results may be biased to some extent. In the future, it is necessary to further study the occur of depression among HIV/AIDS diagnosed by psychiatrists using a formal interview. Secondly, the cross-sectional research method cannot clear the causal relationship between the factors and depressive symptoms which needs to be further confirmed by prospective studies.
This study found that marital status and sexual transmission were significantly associated with the occur of depressive symptoms among HIV/AIDS. In particular, unmarried HIV/AIDS patients were at greater risk of depressive symptoms, and heterosexual transmission had protective effects against depressive symptoms among HIV/AIDS. Therefore, scholars should pay more attention to HIV/AIDS with these characteristics described above in the future research, and timely psychological intervention or treatment should be carried out.
The datasets presented in this article are not readily available because the data used for this study is available from the corresponding author upon request. Requests to access the datasets should be directed to MjI1MjM2OTE5OEBxcS5jb20=.
SC analyzed the data and wrote the draft of manuscript. HH contributed to the collection of data. HH and GX generated the idea and supervised the analysis. SC, HH, and GX revised the manuscript critically. All authors put their energies into the research and approved the final version of the manuscript.
This work was supported by grants from Zhejiang Medical and Health Technology Discipline (2021KY1017), Medical Key Discipline of Zhejiang Province (07–013), Medical and Health Brand Discipline of Ningbo (PPXK2018-10), and Zhejiang Natural Science Foundation Project (LQ20H260005).
We express our gratitude to the participants, primary clinicians and nurses who participated in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lwidiko A, Kibusi SM, Nyundo A, Mpondo BCT. Association between Hiv status and depressive symptoms among children and adolescents in the southern highlands zone, Tanzania: a case-control study. PLoS One. (2018) 13:e0193145. doi: 10.1371/journal.pone.0193145
2. Olson B, Vincent W, Meyer JP, Kershaw T, Sikkema KJ, Heckman TG, et al. Depressive symptoms, physical symptoms, and health-related quality of life among older adults with Hiv. Qual Life Res. (2019) 28:3313–22. doi: 10.1007/s11136-019-02271-0
3. van Luenen S, Garnefski N, Spinhoven P, Kraaij V. Guided internet-based intervention for people with Hiv and depressive symptoms: a randomised controlled trial in the Netherlands. Lancet HIV. (2018) 5:e488–97. doi: 10.1016/S2352-3018(18)30133-4
4. Asrat B, Schneider M, Ambaw F, Lund C. Effectiveness of psychological treatments for depressive symptoms among people living with Hiv/Aids in low- and middle-income countries: a systematic review and meta-analysis. J Affect Disord. (2020) 270:174–87. doi: 10.1016/j.jad.2020.03.068
5. Kohn JN, Loop MS, Kim-Chang JJ, Garvie PA, Sleasman JW, Fischer B, et al. Trajectories of depressive symptoms, neurocognitive function, and viral suppression with antiretroviral therapy among youth with Hiv over 36 months. J Acquir Immune Defic Syndr. (2021) 87:851–9. doi: 10.1097/QAI.0000000000002653
6. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. (2006) 3:e442. doi: 10.1371/journal.pmed.0030442
7. Nabunya P, Byansi W, Damulira C, Bahar OS, Jennings Mayo-Wilson L, Tozan Y, et al. Predictors of depressive symptoms and post traumatic stress disorder among women engaged in commercial sex work in Southern Uganda. Psychiatry Res. (2021) 298:113817. doi: 10.1016/j.psychres.2021.113817
8. Kanmogne GD, Qiu F, Ntone FE, Fonsah JY, Njamnshi DM, Kuate CT, et al. Depressive symptoms in Hiv-infected and seronegative control subjects in Cameroon: effect of age, education and gender. PLoS One. (2017) 12:e0171956. doi: 10.1371/journal.pone.0171956
9. De Francesco D, Winston A, Underwood J, Cresswell FV, Anderson J, Post FA, et al. Cognitive function, depressive symptoms and syphilis in Hiv-positive and Hiv-negative individuals. Int J STD AIDS. (2019) 30:440–6. doi: 10.1177/0956462418817612
10. Ciesla JA, Roberts JE. Meta-analysis of the relationship between Hiv infection and risk for depressive disorders. Am J Psychiatry. (2001) 158:725–30. doi: 10.1176/appi.ajp.158.5.725
11. Liu X, Wang H, Zhu Z, Zhang L, Cao J, Zhang L, et al. Exploring bridge symptoms in Hiv-positive people with comorbid depressive and anxiety disorders. BMC Psychiatry. (2022) 22:448. doi: 10.1186/s12888-022-04088-7
12. Bengtson AM, Pence BW, Moore R, Mimiaga MJ, Mathews WC, Heine A, et al. Relationship between ever reporting depressive symptoms and all-cause mortality in a cohort of Hiv-infected adults in routine care. AIDS. (2017) 31:1009–16. doi: 10.1097/QAD.0000000000001431
13. Ekat MH, Yotebieng M, Leroy V, Mpody C, Diafouka M, Loubaki G, et al. Association between depressive symptoms and adherence among adolescents living with Hiv in the Republic of Congo: a cross sectional study. Medicine (Baltimore). (2020) 99:e21606. doi: 10.1097/MD.0000000000021606
14. Damtie Y, Kefale B, Yalew M, Arefaynie M, Adane B, Edmealem A, et al. Depressive symptoms and associated factors among Hiv positive patients attending public health facilities of Dessie town: a cross-sectional study. PLoS One. (2021) 16:e0255824. doi: 10.1371/journal.pone.0255824
15. Mao Y, Qiao S, Li X, Zhao Q, Zhou Y, Shen Z. Depression, social support, and adherence to antiretroviral therapy among people living with Hiv in Guangxi, China: a longitudinal study. AIDS Educ Prev. (2019) 31:38–50. doi: 10.1521/aeap.2019.31.1.38
16. Ezeamama AE, Woolfork MN, Guwatudde D, Bagenda D, Manabe YC, Fawzi WW, et al. Depressive and anxiety symptoms predict sustained quality of life deficits in Hiv-positive Ugandan adults despite antiretroviral therapy: a prospective cohort study. Medicine (Baltimore). (2016) 95:e2525. doi: 10.1097/MD.0000000000002525
17. Levintow SN, Pence BW, Ha TV, Le Minh N, Sripaipan T, Latkin CA, et al. Depressive symptoms at Hiv testing and two-year all-cause mortality among men who inject drugs in Vietnam. AIDS Behav. (2019) 23:609–16. doi: 10.1007/s10461-018-2318-8
18. Arseniou S, Arvaniti A, Samakouri M. Hiv infection and depression. Psychiatry Clin Neurosci. (2014) 68:96–109. doi: 10.1111/pcn.12097
19. Fu H, Feng T, Wang T, Wu X, Cai Y, Yang T. Reported prevalence of depression or depressive symptoms among men who have sex with men in China, 2004–2018: a systematic review and meta-analysis. J Affect Disord. (2020) 277:192–203. doi: 10.1016/j.jad.2020.08.011
20. Zewudie BT, Geze S, Mesfin Y, Argaw M, Abebe H, Mekonnen Z, et al. A systematic review and meta-analysis on depression and associated factors among adult Hiv/Aids-positive patients attending art clinics of Ethiopia: 2021. Depress Res Treat. (2021) 2021:8545934. doi: 10.1155/2021/8545934
21. Nanni MG, Caruso R, Mitchell AJ, Meggiolaro E, Grassi L. Depression in Hiv infected patients: a review. Curr Psychiatry Rep. (2015) 17:530. doi: 10.1007/s11920-014-0530-4
22. Bernard C, Dabis F, de Rekeneire N. Prevalence and factors associated with depression in people living with Hiv in Sub-Saharan Africa: a systematic review and meta-analysis. PLoS One. (2017) 12:e0181960. doi: 10.1371/journal.pone.0181960
23. Kroenke K, Spitzer RL, Williams JB. The patient health questionnaire-2: validity of a two-item depression screener. Med Care. (2003) 41:1284–92. doi: 10.1097/01.MLR.0000093487.78664.3C
24. Kroenke K, Spitzer RL, Williams JB. The Phq-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
25. Levis B, Sun Y, He C, Wu Y, Krishnan A, Bhandari PM, et al. Accuracy of the Phq-2 alone and in combination with the Phq-9 for screening to detect major depression: systematic review and meta-analysis. JAMA. (2020) 323:2290–300. doi: 10.1001/jama.2020.6504
26. Jiang Y, Wang M, Wei XQ, He JM, Guo TS, Huang GQ, et al. [Prevalence of depression and related factors in 180 Hiv/Aids patients receiving highly active antiretroviral therapy]. Zhonghua Liu Xing Bing Xue Za Zhi. (2016) 37:638–42. doi: 10.3760/cma.j.issn.0254-6450.2016.05.010
27. Parcesepe AM, Remch M, Dzudie A, Ajeh R, Nash D, Anastos K, et al. Depressive symptoms, gender, disclosure, and Hiv care stage among people living with Hiv in Cameroon. AIDS Behav. (2022) 26:651–61. doi: 10.1007/s10461-021-03425-3
28. Rosenthal MA, Wanje G, Richardson BA, Shafi J, Wang L, Masese L, et al. A prospective study of depressive symptoms, condomless sex, and Hiv viral load in Hiv-positive female sex workers in Kenya. AIDS Behav. (2021) 25:3047–56. doi: 10.1007/s10461-021-03258-0
29. Bengtson AM, Pence BW, Powers KA, Weaver MA, Mimiaga MJ, Gaynes BN, et al. Trajectories of depressive symptoms among a population of Hiv-infected men and women in routine Hiv care in the United States. AIDS Behav. (2018) 22:3176–87. doi: 10.1007/s10461-018-2109-2
30. Javanbakht M, Shoptaw S, Ragsdale A, Brookmeyer R, Bolan R, Gorbach PM. Depressive symptoms and substance use: changes overtime among a cohort of Hiv-positive and Hiv-negative Msm. Drug Alcohol Depend. (2020) 207:107770. doi: 10.1016/j.drugalcdep.2019.107770
31. Al Madhani A, Al Harthi L, Balkhair A, Chan MF, Albusaidi BS, Al Sibani N, et al. Prevalence and correlates of depressive symptoms among people living with Hiv attending tertiary care hospitals in Oman. Pan Afr Med J. (2020) 37:90. doi: 10.11604/pamj.2020.37.90.23294
32. Abdisa E, Tolesa T, Abadiga M. Prevalence of depressive symptoms and its associated factors among people living with Hiv attending public hospitals of Nekemte town, Western Ethiopia, 2021. Behav Neurol. (2021) 2021:8854791. doi: 10.1155/2021/8854791
33. Aibibula W, Cox J, Hamelin AM, Moodie EEM, Anema A, Klein MB, et al. Association between depressive symptoms, Cd4 count and Hiv viral suppression among Hiv-Hcv co-infected people. AIDS Care. (2018) 30:643–9. doi: 10.1080/09540121.2018.1431385
34. Dal-Bo MJ, Manoel AL, Filho AO, Silva BQ, Cardoso YS, Cortez J, et al. Depressive symptoms and associated factors among people living with Hiv/Aids. J Int Assoc Provid AIDS Care. (2015) 14:136–40. doi: 10.1177/2325957413494829
35. Nyongesa MK, Mwangi P, Wanjala SW, Mutua AM, Newton C, Abubakar A. Prevalence and correlates of depressive symptoms among adults living with Hiv in rural Kilifi, Kenya. BMC Psychiatry. (2019) 19:333. doi: 10.1186/s12888-019-2339-5
36. Wang H, Zhang C, Ruan Y, Li X, Fennie K, Williams AB. Depressive symptoms and social support among people living with Hiv in Hunan, China. J Assoc Nurs AIDS Care. (2014) 25:568–76. doi: 10.1016/j.jana.2014.02.001
37. Bernard C, Font H, Diallo Z, Ahonon R, Tine JM, N’Guessan Abouo F, et al. Prevalence and factors associated with severe depressive symptoms in older West African people living with Hiv. BMC Psychiatry. (2020) 20:442. doi: 10.1186/s12888-020-02837-0
38. Zeziulin O, Mollan KR, Shook-Sa BE, Hanscom B, Lancaster KE, Dumchev K, et al. Depressive symptoms and use of Hiv care and medication-assisted treatment among people with Hiv who inject drugs. AIDS. (2021) 35:495–501. doi: 10.1097/QAD.0000000000002774
39. Levintow SN, Pence BW, Ha TV, Minh NL, Sripaipan T, Latkin CA, et al. Prevalence and predictors of depressive symptoms among Hiv-positive men who inject drugs in Vietnam. PLoS One. (2018) 13:e0191548. doi: 10.1371/journal.pone.0191548
40. Reta Y, Getachew R, Bahiru M, Kale B, Workie K, Gebreegziabhere Y. depressive symptoms and its associated factors among prisoners in Debre Berhan prison, Ethiopia. PLoS One. (2020) 15:e0220267. doi: 10.1371/journal.pone.0220267
41. Mekonen T, Belete H, Fekadu W. Depressive symptoms among people with Hiv/Aids in Northwest Ethiopia: comparative study. BMJ Open. (2021) 11:e048931. doi: 10.1136/bmjopen-2021-048931
42. Beyrer C, Sullivan P, Sanchez J, Baral SD, Collins C, Wirtz AL, et al. The increase in global Hiv Epidemics in Msm. AIDS. (2013) 27:2665–78. doi: 10.1097/01.aids.0000432449.30239.fe
43. Li Z, Hsieh E, Morano JP, Sheng Y. Exploring Hiv-related stigma among Hiv-infected men who have sex with men in Beijing, China: a correlation study. AIDS Care. (2016) 28:1394–401. doi: 10.1080/09540121.2016.1179713
44. Beyrer C, Baral SD, van Griensven F, Goodreau SM, Chariyalertsak S, Wirtz AL, et al. Global epidemiology of Hiv infection in men who have sex with men. Lancet. (2012) 380:367–77. doi: 10.1016/S0140-6736(12)60821-6
45. Li J, Mo PK, Kahler CW, Lau JT, Du M, Dai Y, et al. Prevalence and associated factors of depressive and anxiety symptoms among Hiv-infected men who have sex with men in China. AIDS Care. (2016) 28:465–70. doi: 10.1080/09540121.2015.1118430
46. Babowitch JD, Mitzel LD, Vanable PA, Sweeney SM. Depressive symptoms and condomless sex among men who have sex with men living with Hiv: a curvilinear association. Arch Sex Behav. (2018) 47:2035–40. doi: 10.1007/s10508-017-1105-3
47. Wang T, Fu H, Kaminga AC, Li Z, Guo G, Chen L, et al. Prevalence of depression or depressive symptoms among people living with Hiv/Aids in China: a systematic review and meta-analysis. BMC Psychiatry. (2018) 18:160. doi: 10.1186/s12888-018-1741-8
Keywords: HIV, antiretroviral therapy, depressive symptoms, prevalence, related factors
Citation: Chen S, Hong H and Xu G (2022) Prevalence and related factors of depressive symptoms among HIV/AIDS in Ningbo, China: A cross-sectional study. Front. Psychiatry 13:1004318. doi: 10.3389/fpsyt.2022.1004318
Received: 27 July 2022; Accepted: 22 September 2022;
Published: 10 October 2022.
Edited by:
Ashwani Kumar Mishra, All India Institute of Medical Sciences, IndiaReviewed by:
Henock Asfaw, Haramaya University, EthiopiaCopyright © 2022 Chen, Hong and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guozhang Xu, eHVnekBuYmNkYy5vcmcuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.