 Otto Simonsson1,2†
Otto Simonsson1,2† José Carlos Bouso3,4,5*
José Carlos Bouso3,4,5* Florian Kurth6
Florian Kurth6 Dráulio B. Araújo7,8†
Dráulio B. Araújo7,8† Christian Gaser9,10Jordi Riba11
Christian Gaser9,10Jordi Riba11 Eileen Luders6,12,13
Eileen Luders6,12,13- 1Center for Psychiatry Research, Department of Clinical Neuroscience, Karolinska Institute, Stockholm, Sweden
- 2Department of Sociology, University of Oxford, Oxford, United Kingdom
- 3ICEERS–International Center for Ethnobotanical Education, Research and Services, Barcelona, Spain
- 4Medical Anthropology Research Center (MARC), Universitat Rovira i Virgili, Tarragona, Spain
- 5Department of Neurosciences and Behavior, Ribeirão Preto Medical School, University of São Paulo, Ribeirão Preto, Brazil
- 6School of Psychology, University of Auckland, Auckland, New Zealand
- 7Brain Institute, Federal University of Rio Grande do Norte, Natal, Brazil
- 8Onofre Lopes University Hospital, Federal University of Rio Grande do Norte, Natal, Brazil
- 9Department of Psychiatry and Psychotherapy, Jena University Hospital, Jena, Germany
- 10Department of Neurology, Jena University Hospital, Jena, Germany
- 11Centro de Investigación Biomédica en Red de Salud Mental, Madrid, Spain
- 12Department of Women’s and Children’s Health, Uppsala University, Uppsala, Sweden
- 13Laboratory of Neuro Imaging, School of Medicine, University of Southern California, Los Angeles, CA, United States
Background: Recent research suggests that ayahuasca and its alkaloid-containing ingredients may be helpful in the treatment and prevention of certain movement and neurodegenerative disorders. However, such research is still in its infancy and more studies in normative samples seem necessary to explore effects of ayahuasca on clinically relevant brain structures, such as the corpus callosum.
Aims: The purpose of the present study was to investigate links between ayahuasca use and callosal structure in a normative sample.
Methods: Using structural imaging data from 22 ayahuasca users and 22 matched controls we compared the thickness of the corpus callosum between both groups at 100 equidistant points across the entire midsagittal surface. In addition, we investigated point-wise correlations between callosal thickness and the number of past ayahuasca sessions.
Results: The corpus callosum was significantly thicker within the isthmus in the ayahuasca group than in the control group. There was also a significant positive correlation between callosal thickness and the number of past ayahuasca sessions within the rostral body, albeit none of these effects survived corrections for multiple comparisons. No region was significantly thicker in the control than in the ayahuasca group, and no callosal region was negatively linked to ayahuasca use, even at uncorrected significance thresholds.
Conclusion: This study provides preliminary evidence of links between ayahuasca use and the corpus callosum. However, future studies need to replicate these findings, preferably using larger sample sizes and ideally also utilizing longitudinal research designs, to draw any practical conclusion and offer implications for follow-up clinical research.
Introduction
Ayahuasca is a psychedelic botanical admixture that has been used for millennia by indigenous tribes in the Amazon basin. The most commonly known recipe for ayahuasca involves preparing a concoction of Banisteriopsis caapi and Psychotria viridis. The stem and bark of B. caapi contain the β-Carboline alkaloids harmaline, harmine, and tetrahydroharmine, while the leaves of P. viridis contain the psychoactive alkaloid N, N-Dimethyltryptamine (DMT), also known as DMT (1). If ingested orally, DMT becomes degraded by monoamine oxidase type A (MAO-A) in the gastrointestinal tract and therefore cannot reach the brain. However, when mixing B. caapi with P. viridis into an ayahuasca brew, reversible MAO-A inhibitors present in the β-Carboline alkaloids allows DMT to be delivered to the Central Nervous System (CNS), which produces potent psychoactive effects (2).
The evidence to date suggests that ayahuasca has a relatively good safety profile [(3); but also see (4, 5) for potential harmful effects]. While ayahuasca and its alkaloid-containing ingredients show promise in the treatment of mental health conditions (6–9), they might also aid in the treatment and prevention of movement and neurodegenerative disorders. For example, DMT binds and activates the sigma-1 receptor (10) as well as several serotonin receptors (11) which have been identified as potential therapeutic targets in certain movement and neurodegenerative disorders (12–15). Other research suggests that DMT and the alkaloids of B. caapi (harmine, tetrahydroharmine, harmaline) may stimulate adult neurogenesis (16–18) and reduce neuroinflammation (19). Ayahuasca might therefore become relevant for a variety of disorders, such as multiple sclerosis, amyotrophic lateral sclerosis, or Parkinson’s disease (19). While the etiology and disease progression varies across these types of disorders, many have been associated with aberrations of the corpus callosum (20–27), which is the largest interhemispheric fiber tract in the human brain (28).
Thus, the current study was designed to shed further light on the potential effects of ayahuasca use on the corpus callosum. More specifically, we conducted a secondary analysis [see (29) for the original study] comparing the midsagittal thickness of the corpus callosum between ayahuasca users and their matched controls at 100 equidistant points between the tip of the rostrum and the bottom of the splenium. In addition, we conducted point-wise correlation analyses to establish whether callosal thickness and the number of past ayahuasca sessions were significantly linked. We hypothesized thicker corpora callosa in ayahuasca users compared to matched controls as well as a positive correlation between callosal thickness and ayahuasca use. Since some research suggests that specific components of the ayahuasca brew may improve motor function [(30, 31); see also, (32)], we expected to find significant effects within the isthmus of the corpus callosum, which has been demonstrated to house motor fibers (33) and has been linked to certain movement and neurodegenerative disorders in previous research [(21, 34, 35); see also (36)].
Materials and methods
Sample
The study included 22 ayahuasca users from the Santo Daime church in Spain and 22 matched controls. The inclusion criteria for the ayahuasca group were: (1) frequent use of ayahuasca in the past 2 years; (2) no ayahuasca use or use of other types of drugs in the 2 weeks before the brain scan (verified by an urine toxicology test); (3) lifetime use of cannabis less than twenty times; (4) lifetime use of other drugs on ten occasions or less; and (5) no current or past history of psychiatric or neurological disorders [see (29) for a detailed overview of the full inclusion criteria]. The ayahuasca group and the control group were matched for sex (6 men and 16 women), age (ayahuasca group: mean = 40.9 years, SD = 12.6; control group: mean = 41.5 years, SD = 11.8), years of education (ayahuasca group: mean = 13.0 years, SD = 3.3; control group: 13.1 years, SD = 3.1), fluid intelligence as measured by the Wechsler Adult Intelligence Scale-III [(37); ayahuasca group: mean = 15.7, SD = 3.5; control group: 15.7, SD = 3.6], and verbal intelligence as measured by the Spanish version of the New Adult Reading Test [(38); ayahuasca group: mean = 25.9, SD = 3.5; control group: 25.0, SD = 3.7]. There were also no significant differences between the two groups with respect to employment status, marital status, tobacco use, and alcohol use. A more detailed explanation of the testing batteries and recruitment process can be found in Bouso et al. (29).
Image acquisition and processing
The structural brain images were acquired on a 3 Tesla scanner using a T1-weighted MPRAGE sequence (240 sagittal slices; matrix size = 256 × 256; voxel resolution = 1 mm × 1 mm × 1 mm; TR = 2300 ms; TE = 1 ms). The study was approval by the Ethics Committee at Hospital de Sant Pau (Barcelona, Spain). All participants provided written informed consent to participate in the study.
All brain images were preprocessed in SPM121 and the CAT12 toolbox (39) applying corrections for magnetic field inhomogeneities and spatial alignment, the latter using rigid-body transformations. Using the preprocessed images, the corpus callosum was manually outlined in each brain’s midsagittal section (40). The callosal traces were extracted and automatically processed in a number of successive steps (41–43). More specifically, the callosal outlines were separated into 100 nodes and re-sampled at regular intervals rendering the discrete points comprising the two boundaries spatially uniform. Then, a new midline curve was created by calculating the two-dimensional average from the 100 equidistant nodes representing the upper and the lower callosal boundaries. Finally, the distances between the 100 nodes of the upper as well as the lower callosal boundaries to the 100 nodes of the midline curve were calculated and later entered as the dependent variables in the statistical model. In addition, the total intracranial volume (TIV) was calculated by classifying images as gray matter (GM), white matter (WM), and cerebrospinal fluid (CSF) in native space and adding the volumes of these compartments (TIV = GM + WM + CSF) to be entered as a nuisance variable in the statistical model.
Statistical analyses
All statistical analyses were conducted in Matlab2 using a mass-univariate general linear model. The calculated point-wise callosal distances constituted the dependent variable, group the independent variable, and age as well as TIV the variables of no interest. In addition to the group comparison (ayahuasca group vs. control group), we conducted a correlation analysis within the ayahuasca group examining the link between callosal thickness and the number of past ayahuasca sessions. Again, age and TIV were considered variables of no interest. For both analysis streams–group comparison and correlation–given our a priori hypotheses, we applied one-tailed T-tests at p ≤ 0.05 and generated uncorrected significance maps (effect size maps, respectively) by projecting the p-values (d- and r-vales, respectively) onto the averaged callosal outline. In addition, corrections for multiple comparisons were applied using a Monte-Carlo simulation with 10,000 permutations (44, 45) to test if findings survived a correction for multiple comparisons.
Results
As shown in Figure 1, we detected significant group differences within the isthmus, where the corpus callosum was thicker in the ayahuasca group than in the control group. With respect to the significance maximum within this isthmus cluster, the mean (±SD) callosal thickness in the ayahuasca group was 5.47 (±0.71) mm and 4.78 (±1.01) mm in the control group (p = 0.006; d = 0.85). The ayahuasca group reported 123 past ayahuasca sessions on average (range: 30–352), and we observed a significant positive correlation between callosal thickness and the number of sessions within the rostral body (see Figure 2). With respect to the significance maximum within this rostral body cluster, the observed p-value was 0.026 and the correlation coefficient (r) was 0.45, which constitutes a medium effect size. None of these significant effects survived corrections for multiple comparisons. No region was significantly thicker in the control than in the ayahuasca group, and no callosal region was negatively linked to ayahuasca use, even without applying corrections for multiple comparisons.
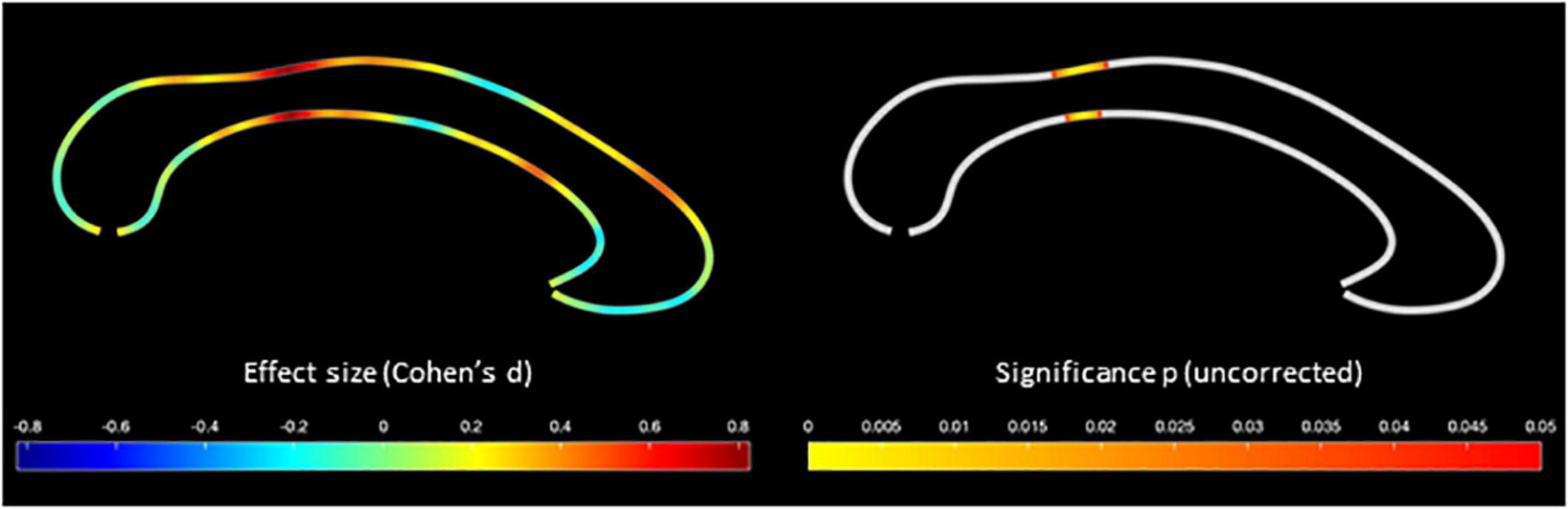
Figure 1. Greater callosal thickness in the ayahuasca group compared to the control group. The color bar encodes the effect size (Cohen’s d) on the left, and the uncorrected significance (p) on the right.
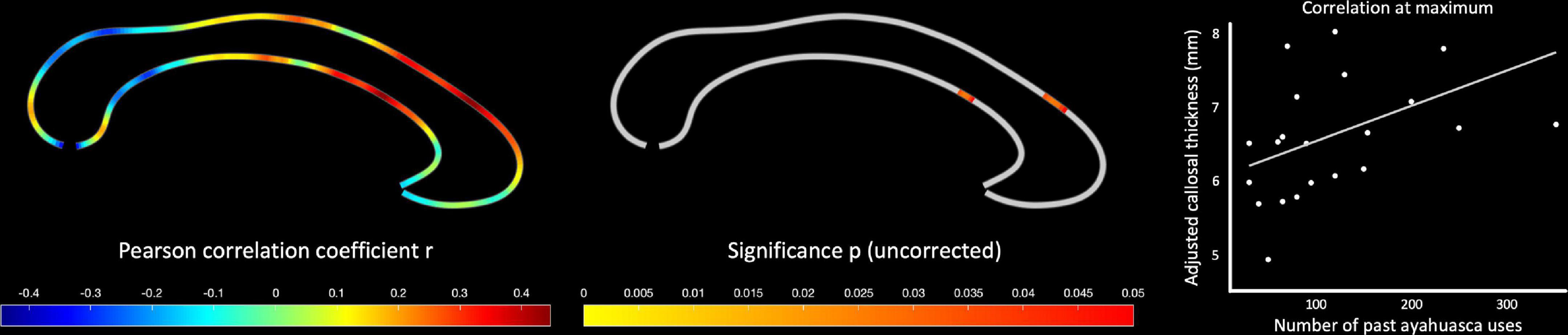
Figure 2. Positive correlations between callosal thickness and ayahuasca use. The color bar encodes the Pearson correlation coefficient (r) on the left, and the uncorrected significance (p) in the middle. The scatterplot on the right illustrates the association between the number of ayahuasca uses and callosal thickness at the maximum of the significance cluster, adjusted for age and total intracranial volume (TIV).
Discussion
This study investigated associations between long-term use of ayahuasca and the anatomy of the corpus callosum. The results showed that the isthmus of the corpus callosum was thicker in the ayahuasca group than in the control group, but there was also a positive correlation between callosal thickness and the number of past ayahuasca sessions within the rostral body. None of these findings survived a correction for multiple comparisons, however, and should therefore be interpreted with caution. Prior investigations comparing ayahuasca users with non-users have found group differences in neuropsychological functioning and neuroanatomy, albeit none in the corpus callosum (29, 46, 47). The preliminary and exploratory findings of this study therefore contribute to a growing body of research on the potential effects of ayahuasca on brain function and structure.
In terms of the location of the observed effects and their possible functional implications, both the isthmus and the rostral body of the corpus callosum have been linked to motor function (33, 48–51). With respect to the possible underlying mechanisms, previous research suggests that a thicker corpus callosum (i.e., as observed in the ayahuasca group) implies a higher number of axons, thicker axons, a greater degree of myelination, or possibly a combination of these (52). More axons might indicate greater anatomical interhemispheric connectivity, and thicker axons as well as a greater myelination are likely associated with higher signal conduction velocities [see (48, 53, 54)]. It is therefore possible that ayahuasca could have a modulating impact and possibly benefiting effect on symptoms linked to impaired motor function, such as those evident in many movement and neurodegenerative disorders (55–57).
Limitations and implications for future research
The current pilot study has several short-comings. First, given that the structural brain images were only acquired at one time point, causality of the reported effects cannot be resolved. It is possible, for instance, that brains of long-term ayahuasca users are inherently different from non-users. Second, participants were asked about the number of past ayahuasca sessions, but no information was provided on the (average) dose of ayahuasca on each occasion. The analyses that were conducted could therefore not account for potential dose-dependent effects. Third, none of the significant effects survived corrections for multiple comparisons. Caution should therefore be exercised when interpreting the results. Last but not least, the study was conducted in healthy participants and not in patients affected by movement and neurodegenerative disorders. All conclusions with respect to potential treatments should therefore be drawn with extreme caution and considered conjecture.
Future research is clearly necessary to replicate the current findings as well as to address the aforementioned limitations by using longitudinal research designs, by collecting information on motor and potentially other behavioral or cognitive information, and by additionally investigating dose-dependent effects. Once a solid basis has been established, normative research can be taken into patient populations.
Conclusion
The research on ayahuasca has primarily focused on mental health, but relatively little is known about the potential of ayahuasca and its alkaloid-containing ingredients in the treatment and prevention of movement and neurodegenerative disorders. Given that the corpus callosum has been implicated as a key structure in certain movement and neurodegenerative disorders, this study investigated links between ayahuasca use and the corpus callosum. The findings provide preliminary evidence of links between ayahuasca use and callosal structure, albeit a causality of the reported effects cannot be resolved given the cross-sectional design. Future studies, ideally longitudinal in nature, need to replicate the current findings in larger normative samples, which could be followed by clinical studies using actual patient populations.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee at Hospital de Sant Pau (Barcelona, Spain). The participants provided their written informed consent to participate in this study.
Author contributions
JB, JR, and DA designed the study and were responsible for data acquisition. FK, CG, and EL analyzed the data. OS wrote the manuscript, with input from EL, FK, JB, DA, and CG. All authors contributed to the article and approved the submitted version.
Funding
OS was supported by Osmond Foundation and Ekhaga Foundation. EL was supported by the Humboldt Foundation. This work was funded by grant 2006/074 from the “Plan Nacional SobreDrogas” (PNSD) of the Spanish Government.
Conflict of interest
OS is a co-founder of Eudelics AB. DA serves as a scientific and clinical advisor at Biomind Labs.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. Brito-da-Costa AM, Dias-da-Silva D, Gomes NG, Dinis-Oliveira RJ, Madureira-Carvalho Á. Toxicokinetics and toxicodynamics of Ayahuasca alkaloids N, N-Dimethyltryptamine (DMT), harmine, harmaline and tetrahydroharmine: clinical and forensic impact. Pharmaceuticals. (2020) 13:334. doi: 10.3390/ph13110334
2. Ruffell S, Netzband N, Bird C, Young AH, Juruena MF. The pharmacological interaction of compounds in ayahuasca: a systematic review. Braz J Psychiatry. (2020) 42:646–56. doi: 10.1590/1516-4446-2020-0884
3. Rossi GN, Dias ICDS, Baker G, Bouso Saiz JC, Dursun SM, Hallak JE, et al. Ayahuasca, a potentially rapid acting antidepressant: focus on safety and tolerability. Expert Opin Drug Saf. (2022) 21:789–801. doi: 10.1080/14740338.2022.2054988
4. Dos Santos RG. A critical evaluation of reports associating ayahuasca with life-threatening adverse reactions. J Psychoact Drugs. (2013) 45:179–88. doi: 10.1080/02791072.2013.785846
5. Martinotti G, Santacroce R, Pettorruso M, Montemitro C, Spano MC, Lorusso M, et al. Hallucinogen persisting perception disorder: etiology, clinical features, and therapeutic perspectives. Brain Sci. (2018) 8:47. doi: 10.3390/brainsci8030047
6. Palhano-Fontes F, Barreto D, Onias H, Andrade KC, Novaes MM, Pessoa JA, et al. Rapid antidepressant effects of the psychedelic ayahuasca in treatment-resistant depression: a randomized placebo-controlled trial. Psychol Med. (2019) 49:655–63.
7. Sanches RF, de Lima Osório F, Dos Santos RG, Macedo LR, Maia-de-Oliveira JP, Wichert-Ana L, et al. Antidepressant effects of a single dose of ayahuasca in patients with recurrent depression: a SPECT study. J Clin Psychopharmacol. (2016) 36:77–81. doi: 10.1097/JCP.0000000000000436
8. Zeifman RJ, Palhano-Fontes F, Hallak J, Arcoverde E, Maia-Oliveira JP, Araújo DB. The impact of ayahuasca on suicidality: results from a randomized controlled trial. Front Pharmacol. (2019) 10:1325. doi: 10.3389/fphar.2019.01325
9. Zeifman RJ, Singhal N, Dos Santos RG, Sanches RF, de Lima Osório F, Hallak JE, et al. Rapid and sustained decreases in suicidality following a single dose of ayahuasca among individuals with recurrent major depressive disorder: results from an open-label trial. Psychopharmacology. (2021) 238:453–9. doi: 10.1007/s00213-020-05692-9
10. Fontanilla D, Johannessen M, Hajipour AR, Cozzi NV, Jackson MB, Ruoho AE. The hallucinogen N, N-dimethyltryptamine (DMT) is an endogenous sigma-1 receptor regulator. Science. (2009) 323:934–7. doi: 10.1126/science.1166127
11. Barker SA. N, N-Dimethyltryptamine (DMT), an endogenous hallucinogen: past, present, and future research to determine its role and function. Front Neurosci. (2018) 12:536. doi: 10.3389/fnins.2018.00536
12. Herrando-Grabulosa M, Gaja-Capdevila N, Vela JM, Navarro X. Sigma 1 receptor as a therapeutic target for amyotrophic lateral sclerosis. Br J Pharmacol. (2021) 178:1336–52.
13. Lisak RP, Nedelkoska L, Benjamins JA. Sigma-1 receptor agonists as potential protective therapies in multiple sclerosis. J Neuroimmunol. (2020) 342:577188.
14. Nguyen L, Lucke-Wold BP, Mookerjee SA, Cavendish JZ, Robson MJ, Scandinaro AL, et al. Role of sigma-1 receptors in neurodegenerative diseases. J Pharmacol Sci. (2015) 127:17–29.
15. Vermeiren Y, Janssens J, Van Dam D, De Deyn PP. Serotonergic dysfunction in amyotrophic lateral sclerosis and Parkinson’s disease: similar mechanisms, dissimilar outcomes. Front Neurosci. (2018) 12:185. doi: 10.3389/fnins.2018.00185
16. Dakic V, de Moraes Maciel R, Drummond H, Nascimento JM, Trindade P, Rehen SK. Harmine stimulates proliferation of human neural progenitors. PeerJ. (2016) 4:e2727.
17. Morales-García JA, de la Fuente Revenga M, Alonso-Gil S, Rodríguez-Franco I, Feilding A, Perez-Castillo A, et al. The alkaloids of Banisteriopsis caapi, the plant source of the Amazonian hallucinogen Ayahuasca, stimulate adult neurogenesis in vitro. Sci Rep. (2017) 7:5309. doi: 10.1038/s41598-017-05407-9
18. Morales-Garcia JA, Calleja-Conde J, Lopez-Moreno JA, Alonso-Gil S, Sanz-SanCristobal M, Riba J, et al. N, N-dimethyltryptamine compound found in the hallucinogenic tea ayahuasca, regulates adult neurogenesis in vitro and in vivo. Transl Psychiatry. (2020) 10:331. doi: 10.1038/s41398-020-01011-0
19. da Silva MG, Daros GC, de Bitencourt RM. Anti-inflammatory activity of ayahuasca: therapeutical implications in neurological and psychiatric diseases. Behav Brain Res. (2021) 400:113003. doi: 10.1016/j.bbr.2020.113003
20. Amandola M, Sinha A, Amandola MJ, Leung HC. Longitudinal corpus callosum microstructural decline in early-stage Parkinson’s disease in association with akinetic-rigid symptom severity. npj Parkinsons Dis. (2022) 8:108. doi: 10.1038/s41531-022-00372-1
21. Di Paola Á, Luders E, Cherubini A, Sanchez-Castaneda C, Thompson PM, Toga AW, et al. Multimodal MRI analysis of the corpus callosum reveals white matter differences in presymptomatic and early Huntington’s disease. Cereb Cortex. (2012) 22:2858–66. doi: 10.1093/cercor/bhr360
22. Filippini N, Douaud G, Mackay CE, Knight S, Talbot K, Turner MR. Corpus callosum involvement is a consistent feature of amyotrophic lateral sclerosis. Neurology. (2010) 75:1645–52.
23. Frederiksen KS, Waldemar G. Corpus callosum in aging and neurodegenerative diseases. Neurodegener Dis Manag. (2012) 2:493–502.
24. Minnerop M, Luders E, Specht K, Ruhlmann J, Schneider-Gold C, Schröder R, et al. Grey and white matter loss along cerebral midline structures in myotonic dystrophy type 2. J Neurol. (2008) 255:1904–9. doi: 10.1007/s00415-008-0997-1
25. Minnerop M, Lüders E, Specht K, Ruhlmann J, Schimke N, Thompson PM, et al. Callosal tissue loss in multiple system atrophy—A one-year follow-up study. Mov Disord. (2010) 25:2613–20. doi: 10.1002/mds.23318
26. Ota M, Obata T, Akine Y, Ito H, Ikehira H, Asada T, et al. Age-related degeneration of corpus callosum measured with diffusion tensor imaging. Neuroimage. (2006) 31:1445–52.
27. Wang XD, Ren M, Zhu MW, Gao WP, Zhang J, Shen H, et al. Corpus callosum atrophy associated with the degree of cognitive decline in patients with Alzheimer’s dementia or mild cognitive impairment: a meta-analysis of the region of interest structural imaging studies. J Psychiatr Res. (2015) 63:10–9.
28. van der Knaap LJ, van der Ham IJ. How does the corpus callosum mediate interhemispheric transfer? A review. Behav Brain Res. (2011) 223:211–21.
29. Bouso JC, Palhano-Fontes F, Rodríguez-Fornells A, Ribeiro S, Sanches R, Crippa JAS. Long-term use of psychedelic drugs is associated with differences in brain structure and personality in humans. Eur Neuropsychopharmacol. (2015) 25:483–92.
30. Nardai S, László M, Szabó A, Alpár A, Hanics J, Zahola P, et al. N, N-dimethyltryptamine reduces infarct size and improves functional recovery following transient focal brain ischemia in rats. Exp Neurol. (2020) 327:113245. doi: 10.1016/j.expneurol.2020.113245
31. Serrano-Dueñas M, Cardozo-Pelaez F, Sánchez-Ramos JR. Effects of Banisteriopsis caapi extract on Parkinson’s disease. Sci Rev Alternat Med. (2001) 5:127–32.
32. Djamshidian A, Bernschneider-Reif S, Poewe W, Lees AJ. Banisteriopsis caapi, a forgotten potential therapy for Parkinson’s disease? Move Disord Clin Pract. (2016) 3:19–26. doi: 10.1002/mdc3.12242
33. Hofer S, Frahm J. Topography of the human corpus callosum revisited—comprehensive fiber tractography using diffusion tensor magnetic resonance imaging. Neuroimage. (2006) 32:989–94. doi: 10.1016/j.neuroimage.2006.05.044
34. Sugiyama M, Takao M, Hatsuta H, Funabe S, Ito S, Obi T, et al. Increased number of astrocytes and macrophages/microglial cells in the corpus callosum in amyotrophic lateral sclerosis. Neuropathology. (2013) 33:591–9. doi: 10.1111/neup.12027
35. Tu S, Wang C, Menke RA, Talbot K, Barnett M, Kiernan MC, et al. Regional callosal integrity and bilaterality of limb weakness in amyotrophic lateral sclerosis. Amyotroph Lateral Scler Frontotemporal Degener. (2020) 21:396–402. doi: 10.1080/21678421.2020.1733020
36. Ryberg C, Rostrup E, Paulson OB, Barkhof F, Scheltens P, Van Straaten ECW, et al. Corpus callosum atrophy as a predictor of age-related cognitive and motor impairment: a 3-year follow-up of the LADIS study cohort. J Neurol Sci. (2011) 307:100–5. doi: 10.1016/j.jns.2011.05.002
37. Wechsler D. Wechsler Adult Intelligence Scale-Revised (WAIS-R). New York, NY: Psychological Corporation (1981).
38. Nelson HE, O’Connell A. Dementia: the estimation of premorbid intelligence levels using the new adult reading test. Cortex. (1978) 14:234–44. doi: 10.1016/s0010-9452(78)80049-5
39. Gaser C, Dahnke R, Thompson PM, Kurth F, Luders E. CAT-a computational anatomy toolbox for the analysis of structural MRI data. bioRxiv. [Preprint]. (2022). doi: 10.1101/2022.06.11.495736
40. Luders E, Di Paola M, Tomaiuolo F, Thompson PM, Toga AW, Vicari S, et al. Callosal morphology in Williams syndrome: a new evaluation of shape and thickness. Neuroreport. (2007) 18:203.
41. Luders E, Thompson PM, Kurth F. Morphometry of the corpus callosum. In: G Spalletta, T Gili, F Piras editors. Brain Morphometry: Methods and Clinical Applications. New York, NY: Humana Press (2018). p. 131–42.
42. Luders E, Thompson PM, Narr KL, Zamanyan A, Chou YY, Gutman B, et al. The link between callosal thickness and intelligence in healthy children and adolescents. Neuroimage. (2011) 54:1823–30. doi: 10.1016/j.neuroimage.2010.09.083
43. Luders E, Toga AW, Thompson PM. Why size matters: differences in brain volume account for apparent sex differences in callosal anatomy: the sexual dimorphism of the corpus callosum. Neuroimage. (2014) 84:820–4. doi: 10.1016/j.neuroimage.2013.09.040
44. Nichols T, Holmes A. Non-parametric procedures. In: K Friston, J Ashburner, S Kiebel, TE Nichols, WD Penny editors. Statistical Parametric Mapping: The Analysis of Functional Brain Images. London: Elsevier (2007). p. 253–72.
45. Winkler AM, Ridgway GR, Webster MA, Smith SM, Nichols TE. Permutation inference for the general linear model. Neuroimage. (2014) 92:381–97.
46. Barbosa PCR, Strassman RJ, da Silveira DX, Areco K, Hoy R, Pommy J, et al. Psychological and neuropsychological assessment of regular hoasca users. Compr Psychiatry. (2016) 71:95–105. doi: 10.1016/j.comppsych.2016.09.003
47. Bouso JC, González D, Fondevila S, Cutchet M, Fernández X, Ribeiro Barbosa PC, et al. Personality, psychopathology, life attitudes and neuropsychological performance among ritual users of ayahuasca: a longitudinal study. PLoS One. (2012) 7:e42421. doi: 10.1371/journal.pone.0042421
48. Kurth F, Mayer EA, Toga AW, Thompson PM, Luders E. The right inhibition? Callosal correlates of hand performance in healthy children and adolescents callosal correlates of hand performance. Hum Brain Mapp. (2013) 34:2259–65. doi: 10.1002/hbm.22060
49. Meyer BU, Röricht S, Woiciechowsky C. Topography of fibers in the human corpus callosum mediating interhemispheric inhibition between the motor cortices. Ann Neurol. (1998) 43:360–9. doi: 10.1002/ana.410430314
50. Ryberg C, Rostrup E, Stegmann MB, Barkhof F, Scheltens P, van Straaten EC, et al. Clinical significance of corpus callosum atrophy in a mixed elderly population. Neurobiol Aging. (2007) 28:955–63. doi: 10.1016/j.neurobiolaging.2006.04.008
51. Zarei M, Johansen-Berg H, Smith S, Ciccarelli O, Thompson AJ, Matthews PM. Functional anatomy of interhemispheric cortical connections in the human brain. J Anat. (2006) 209:311–20.
52. Aboitiz F, Scheibel AB, Fisher RS, Zaidel E. Fiber composition of the human corpus callosum. Brain Res. (1992) 598:143–53.
53. Luders E, Narr KL, Bilder RM, Thompson PM, Szeszko PR, Hamilton L, et al. Positive correlations between corpus callosum thickness and intelligence. Neuroimage. (2007) 37:1457–64.
54. Luders E, Narr KL, Hamilton LS, Phillips OR, Thompson PM, Valle JS. Decreased callosal thickness in attention-deficit/hyperactivity disorder. Biol Psychiatry. (2009) 65:84–8.
55. Ahmed RM, Ke YD, Vucic S, Ittner LM, Seeley W, Hodges JR, et al. Physiological changes in neurodegeneration—mechanistic insights and clinical utility. Nat Rev Neurol. (2018) 14:259–71.
56. Hardiman O, Al-Chalabi A, Chio A, Corr EM, Logroscino G, Robberecht W, et al. Amyotrophic lateral sclerosis. Nat Rev Dis Primers. (2017) 3:17071.
Keywords: psychedelics, ayahuasca, neuro, brain, corpus callosum, isthmus
Citation: Simonsson O, Bouso JC, Kurth F, Araújo DB, Gaser C, Riba J and Luders E (2022) Preliminary evidence of links between ayahuasca use and the corpus callosum. Front. Psychiatry 13:1002455. doi: 10.3389/fpsyt.2022.1002455
Received: 25 July 2022; Accepted: 05 October 2022;
Published: 26 October 2022.
Edited by:
Domenico De Berardis, Mental Health Center (CSM) and Psychiatric Service of Diagnosis and Treatment (SPDC), ItalyReviewed by:
Mauro Pettorruso, University of Studies G. D’Annunzio Chieti and Pescara, ItalyJan Ramaekers, Maastricht University, Netherlands
Copyright © 2022 Simonsson, Bouso, Kurth, Araújo, Gaser, Riba and Luders. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Carlos Bouso, amNib3Vzb0BpY2VlcnMub3Jn
†ORCID: Otto Simonsson, orcid.org/0000-0003-4197-7566; Dráulio B. Araújo, orcid.org/0000-0002-6934-2485