 Katrin E. Giel1*†
Katrin E. Giel1*† Peter Martus2†
Peter Martus2† Gregor Paul3,4
Gregor Paul3,4 Jan Steffen Jürgensen5
Jan Steffen Jürgensen5 Bernd Löwe6
Bernd Löwe6 Lina Maria Serna Higuita2Annica F. Dörsam1
Lina Maria Serna Higuita2Annica F. Dörsam1 Felicitas Stuber1
Felicitas Stuber1 Stefan Ehehalt7
Stefan Ehehalt7 Stephan Zipfel1Florian Junne1,8
Stephan Zipfel1Florian Junne1,8- 1Department for Psychosomatic Medicine and Psychotherapy, Medical University Hospital Tuebingen, Tuebingen, Germany
- 2Institute for Medical Biometrics and Clinical Epidemiology, University Hospital Tuebingen, Tuebingen, Germany
- 3Department of Gastroenterology, Hepatology, Pneumology and Infectious Diseases, Klinikum Stuttgart, Stuttgart, Germany
- 4Department of Internal Medicine, Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany
- 5Klinikum Stuttgart, Stuttgart, Germany
- 6Department for Psychosomatic Medicine and Psychotherapy, University Hospital Hamburg Eppendorf, Hamburg, Germany
- 7Public Health Authority, Stuttgart, Germany
- 8Department for Psychosomatic Medicine and Psychotherapy, University Hospital Magdeburg, Magdeburg, Germany
The stress response to the COVID-19 pandemic might differ between early and later stages. Longitudinal data on the development of population mental health during COVID-19 pandemic is scarce. We have investigated mental health trajectories and predictors for change in a probability sample of the general population in Germany at the beginning and after 6 months of the pandemic. We conducted a longitudinal survey in a population-based probability sample of German adults. The current study analyzed data from a first assessment in May 2020 (T1; N = 1,412) and a second in November 2020 (T2; N = 743). Mental health was assessed in terms of anxiety and depression using the Patient Health Questionnaire-4 (PHQ-4). Mental health outcomes at T1 were compared with PHQ-4 norm data. Trajectories over time were investigated based on outcome classifications of PHQ-4 scores. Predictors of mental health outcomes and change were identified using multiple regression analysis. In spring 2020, participants showed significantly higher PHQ-4 scores as compared to the norm data, however, overall anxiety and depression remained low also 6 months later. 6.6% of respondents showed a mental health deterioration in autumn 2020, entering subclinical and clinical ranges, outweighing the proportion of people with improved outcomes. Sociodemographic variables associated with mental distress at T1 were mainly not predictive for change at T2. Even under prolonged pandemic-related stress, mental health remained mainly stable in the general population. Further development of the considerable subgroup experiencing deterioration of depression and anxiety should be monitored, in order to tailor prevention and intervention efforts.
Introduction
From a mental health perspective, the COVID-19 pandemic can be understood as a global stress induction. Large population groups live under recurrent lockdown situations and threat of a potential infection, experiencing a deprivation of resources and rewarding experiences while mostly having limited control and perspective regarding the situation. The course of the pandemic induces different stages and levels of stress which match well with seminal stress models (1, 2): While the first lockdown in spring 2020 might have induced acute stress, the ongoing pandemic might qualify as a chronic stressor. Hence, the pandemic provides us with novel insights into how individuals cope with stress and about who stays healthy and who is specifically vulnerable to adverse outcomes of chronic stress, including the development of mental symptoms and disorders. This knowledge is pivotal to inform government and health care decisions targeting mental health sequelae of the pandemic (3, 4). However, major methodological limitations of the evidence have been criticized, including a wide reliance on convenience samples (5–8) and a lack of longitudinal data (7, 9, 10). Two large representative surveys from the US (11) and UK (12) investigating pre-post-pandemic mental health outcomes found increased distress in the general population early after the COVID-19 outbreak. The few representative longitudinal studies draw a more differential picture: Data comparing multiple assessments during early stages of the pandemic indicate no changes in mental health outcomes (10, 13, 14), or even a decrease in depression and anxiety over the first 20 weeks of lockdown (15). The few representative studies analyzing individual mental health trajectories identify most people as resilient, while 7% to 11% of individuals reported mental health decline (9, 10, 16) vs. 9–12% experiencing improvements (10, 16). This pattern in mental health development over time has also been found in population-based surveys conducted in Germany (17, 18): Based on the same instrument as used in the present study to assess anxiety and depression, an initial increase in anxiety and depression was found in early stages of the pandemic, which was again reduced during the second wave of the pandemic (18), but overall higher scores of anxiety and depression were reported peri-pandemic as compared to pre-pandemic years (17). Consistently, a recent meta-analysis on lockdown effects on population mental health concludes that most individuals stay mentally healthy (8). Importantly, most of these data stem from the initial stage of the pandemic (8–15), a stage of adaption to an acute stressor (1) as well as stepwise withdrawal of lockdown measures (10). However, mental health might be affected differently along the different stages of the pandemic.
We contribute to the evidence on population mental health during the COVID-19 pandemic by presenting longitudinal data from two assessments within a period of 6 months from a probability sample survey in a German metropole region. We used the Patient Health Questionnaire-4 (PHQ-4) (19, 20) as validated self-report instrument to assess symptoms of depression and anxiety in spring 2020 (T1) and in autumn 2020 (T2). The second assessment point was chosen as in autumn 2020, this was the beginning of the second infection wave and also the second lockdown in Germany, and we hypothesized that these circumstances might impact population mental health. At T1, the 7-day incidence of COVID-19 infections was 5.7 / 100.000 inhabitants in Germany and 7.5 in Stuttgart; at T2, the 7-day incidence was 153.1 in Germany and 137.6 in Stuttgart.
We hypothesized that on average, we will find increased levels of anxiety and depression (a) at T1 as compared to representative norm data, and (b) at T2 as compared to T1 due to reapplied lockdown measures. We expected (c) a majority of the sample to be resilient to mental distress and a small group to show trajectories of impaired mental health and (d) that we will be able to identify sociodemographic predictors for increased distress at T1 and the change between T1 and T2. We tested female gender, younger age, lower education background, living alone and living with children as they have been previously identified as predictors for mental distress early in the pandemic (11, 12, 15, 18). Additionally, we looked at Body Mass Index (BMI) as exploratory variable as elevated BMI has been found to be associated with higher levels of anxiety and depression (21) and as BMI is a proxy of eating behavior which, in some individuals, can serve as an emotion regulation strategy under stressful conditions (22).
Methods
The present study is reported according to the STROBE statement (23).
Study design and recruitment
This survey is a subproject of a longitudinal serological investigation of undetected SARS-CoV-2 infection in the general population. Data was derived from a probability sample of the adult general population living in Stuttgart, Germany. Major confinement measures throughout the pandemic, including lockdowns, were in-place on a nationwide level in Germany, hence the situation of the population of Stuttgart is comparable with circumstances in other parts of the country.
Measures
Mental health was assessed in terms of core symptoms of anxiety and depression using the PHQ-4 (19, 20) which is a widely used screening tool comprised of two items assessing anxiety (GAD-2) and two items assessing depressive symptoms (PHQ-2). The PHQ-2 comprises the DSM-IV core criteria for depressive disorders which are assessed for the last 2 weeks (20), while the GAD-2 assesses the two core criteria for generalized anxiety disorder (20), which have been found to be also good screening approaches for panic, social anxiety and post-traumatic stress disorder (24). The PHQ-4 total score, a sum of PHQ-2 and GAD-2 scores, ranges from 0 to 12 with scores ≥ 6 ≤ 8 considered as yellow flag and scores ≥ 9 considered as red flag for the presence of anxiety and depression (20). The PHQ-4 is a very widely used brief screening tool for anxiety and depression with excellent psychometric qualities (20). We additionally assessed sociodemographic variables.
Procedure
Adult members of 4,400 households in Stuttgart were invited via postal letters to participate in the study. This initial sample was drawn based on data from the residents' registration office and was representative for the adult population living in Stuttgart. Only one single person was invited per household. The first assessment point took place in the second week of May 2020, which was toward the end of the first pandemic wave in Germany. Study participants were re-invited in the last week of November 2020, which was at the beginning of the second lockdown in Germany. Participants were offered to fill in either a paper or an online version of the survey with identical content. No further exclusion criteria applied.
Ethics statement
All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects were approved by the ethics committee of the Medical Faculty Tuebingen and the University Hospital Tuebingen (271/2020BO1). Written informed consent was obtained from all subjects.
Statistical analyses
Primary aim of the study was to investigate mental health trajectories assessed by the PHQ-4 in the general population at the beginning of the pandemic and after 6 months. Predictors for both, baseline and change after 6 months should be identified. For comparison, we used raw data from the PHQ-4 validation study (20). To address responder bias, relevant characteristics at baseline were compared between responders and non-responders using chi-squared test (full df or one df in case of ordinal variables) and t-tests (normally distributed data) or Mann-Whitney tests (non-normally distributed data). Normality was assessed by inspection of skewness and kurtosis (both had to be between −1 and +1).
PHQ-4 was analyzed quantitatively and according to a classification proposed by Löwe et al. (20) (see above). Like previously applied by other workgroups (10), we had a specific focus on individual trajectories between T1 and T2 and classified the study sample into participants who remained stable within the respective PHQ-4 band (below 6, ≥ 6 ≤ 8 and below 8), those who improved as they were moving to a lower band and those who deteriorated as they were moving to a higher band.
Change of PHQ-4 was assessed by t-tests for paired samples (continuous scale), and by sign tests (categorical scale). Associations between quantitative predictors and PHQ-4 at baseline were assessed by linear models (Pearson correlations, ANOVA, including Tukeys B for pairwise comparisons, Curve fit for inspection of quadratic terms, and multiple regression analysis). The same methods were used to assess associations with change of PHQ-4 scores. No imputation was performed and change over time was analyzed only for subjects who participated at T2. This was an exploratory study, thus the chosen level of significance (0.05 two-sided) is not strictly confirmatory and not adjusted for multiple testing. The analyses were carried out using SPSS release 26 (Armonk, NY: IBM Corp). For the Sankey plots, the package R (Vienna, Austria: R Foundation for Statistical Computing) was used.
Results
Sample characteristics
The baseline sample at T1 comprised 1,412 participants (32.1% response rate) with a mean age of 50.7 ± 18.7 years of which 48.1% were females. 18.3% were living alone, 21.3 % were living with one or more children (Table 1). 64.5 % were employed, and of those working, 51.6% were predominantly and 27% were completely working from home.
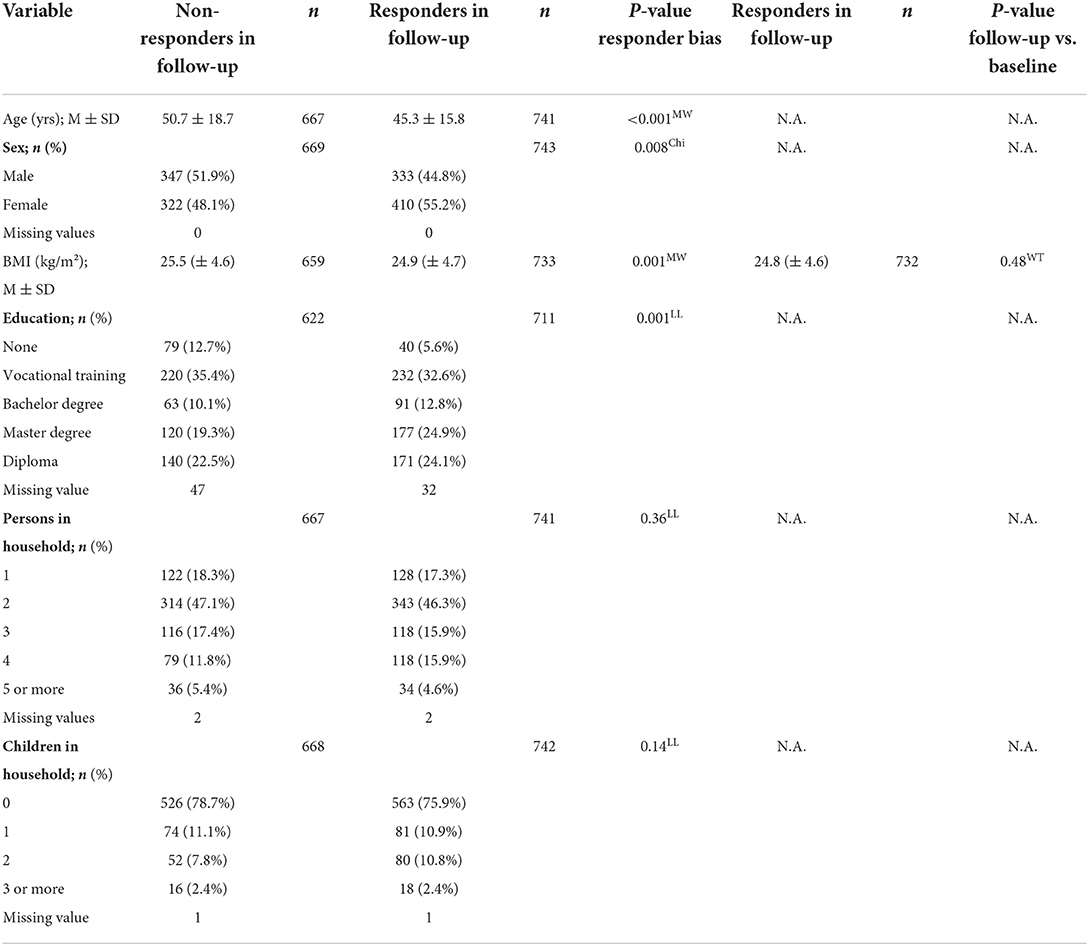
Table 1. Sociodemographic variables in survey responders vs. non-responders at follow-up.
At T2, 743 people (52.8%) participated in the survey. Responders were significantly younger, more often female and reported a lower BMI at baseline. None of the remaining characteristics were different between responders and non-responders (Table 1).
Mental health outcomes at baseline and their predictors
PHQ-4 scores at T1 were significantly higher in our sample as compared to the norm data (see Figure 1).
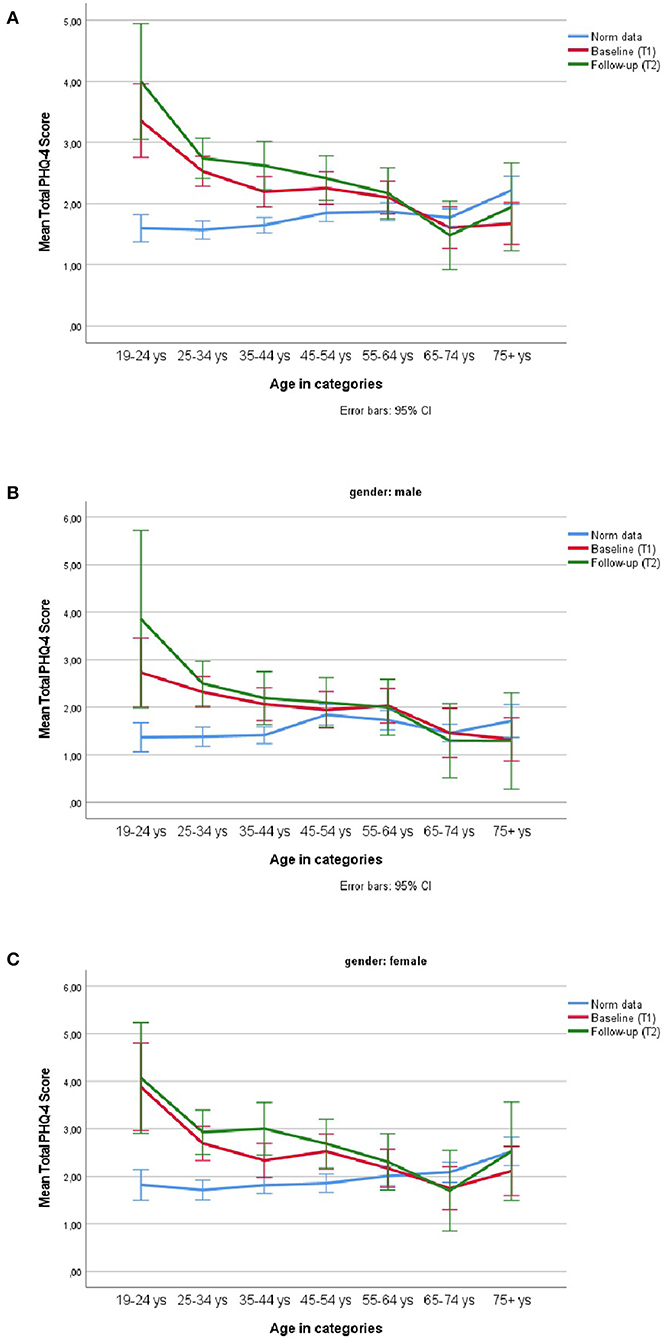
Figure 1. PHQ-4 mean scores at T1 and T2 in the survey population as compared to PHQ-4 normative data in different age groups in (A) the total sample, (B) in males, and (C) in females.
Higher PHQ-4 scores where observed for younger age (r = −0.158, P < 0.001), especially for participants between 19 and 24 years (Anova: F(6,1394) = 8.41, η2 = 0.036, Tukeys B P < 0.01,). Females were more affected than males [t(1,399) = −3.98, Cohen's d = 0.21, P < 0.001]. Figure 1 shows age and gender effects compared to PHQ-4 norm values in the German population. Participants with underweight (BMI < 18.5 kg/m2) and obesity (BMI > 30 kg/m2) were more affected than those with BMI between 18.5 and 30 kg/m2 [quadratic term, b = 0.104, t(1,382)= 3 .85, P < 0.001]. People with academic education were less affected than the remaining groups [b = −0.182, T(1,326) = −4.12, P < 0.001]. There was no effect for the number of children [b = 0.148, t(1,401) = 1.90, P = 0.058] and an unclear pattern for household size [ANOVA F(4,1,396) = 3.94, η2 = 0.01, P = 0.003, linear trend P = 0.093, quadratic P = 0.048]. In a multiple regression analysis, all predictors [r2 adjusted = 0.053, age, b = −0.022, t(1,300) =−6.17, p < 0.001; gender, b = 0.36, t(1,300) = 2.96, p = 0.003; BMI linear, b = 0.133, t(1,300) = 1.69, p = 0.092; BMI quadratic, b = 0.066, t(1,300) = 2.40, P = 0.017; education, b = −0.133, t(1,300) = −3.00, P = 0.003] were significant. Results were similar for the subscale PHQ-2 and less pronounced for the subscale GAD-2 (Supplementary material 1).
Longitudinal mental health trajectories
In the quantitative analysis, changes of the PHQ-4 score and the PHQ-2 subscale score were highly significant [cohen's d = 0.16 total, (subscale 0.18), (t(740) = 4.24, (4.99), P < 0.001 each] whereas the change in the GAD-2 subscale was less pronounced [cohen's d = 0.08, t(740) = 2.13, P = 0.03] (Table 2). Figure 2 shows that a vast majority of participants (87%) had stable PHQ-4 scores within the good mental health range. Significantly more participants (6.6%, n = 49) showed a deterioration of mental health at T2, as compared to those showing a mental health improvement (n = 49 vs. n = 21, 2.8%, P = 0.001, exact binomial test). Most of the deteriorations indicated migrating from good health into the “yellow flag” range and a small proportion moving in the “red flag” range.
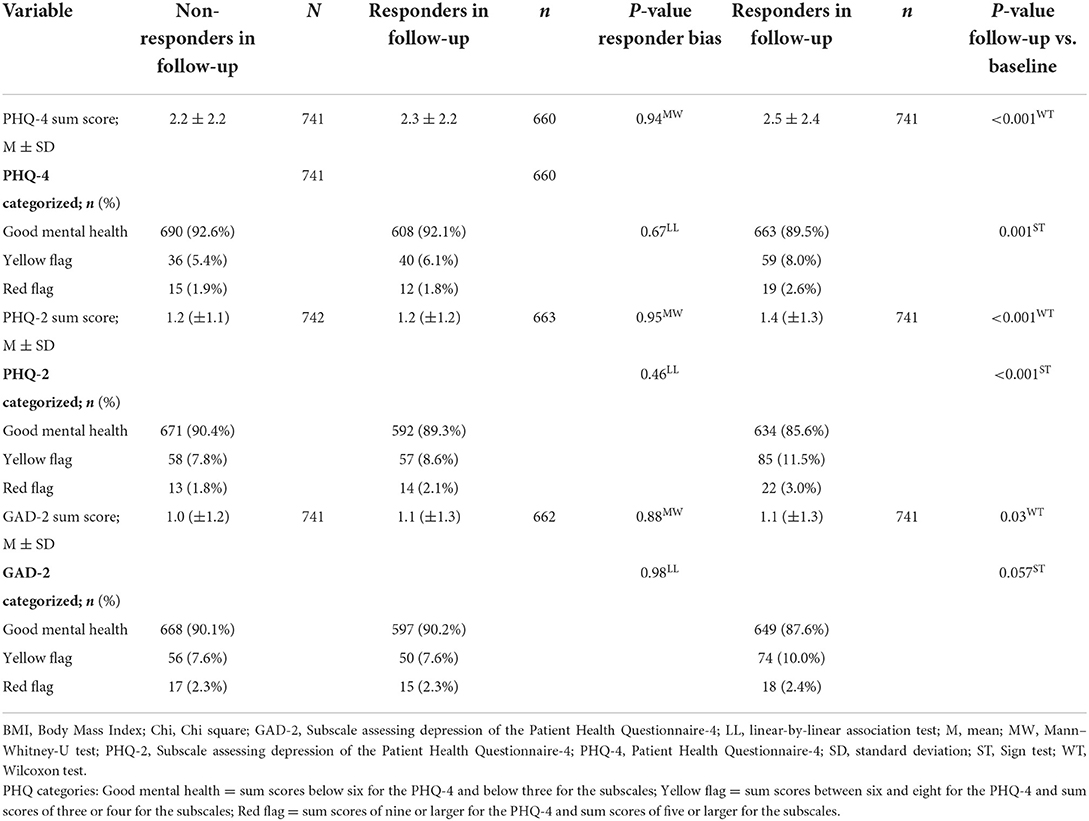
Table 2. Mental health outcomes in survey responders vs. non-responders at follow-up.
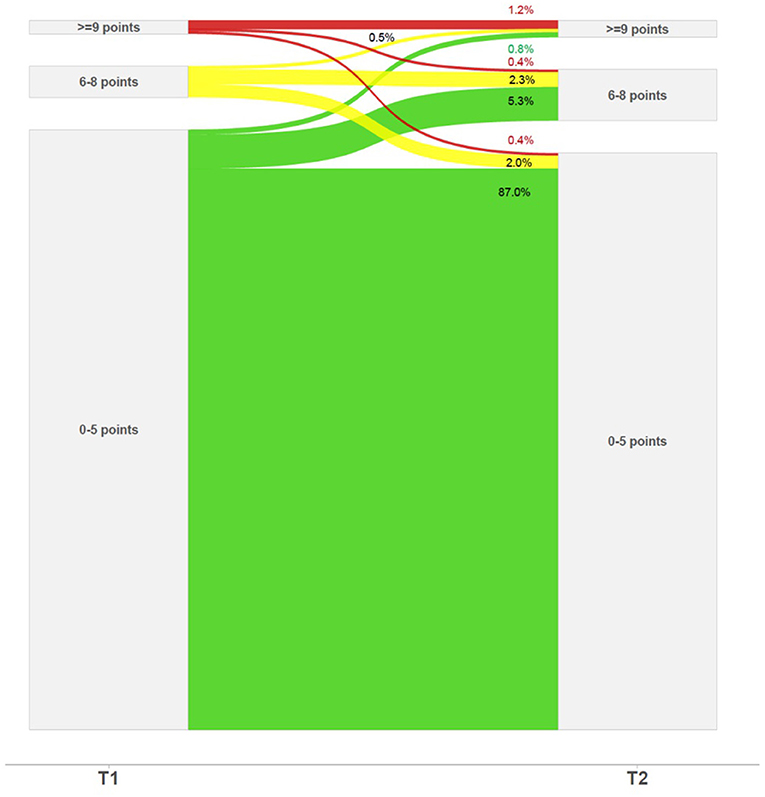
Figure 2. PHQ-4 mental health trajectories between T1 and T2.
Predictors of mental health changes after 6 months
In contrast to the cross-sectional baseline analysis, except for BMI, none of the predictors investigated were significantly associated with the change in PHQ-4 scores (continuous scale) during the observation period. There was a small significant effect (r =-0.087, P < 0.02) that participants with a higher BMI showed less deterioration as compared to people with lower BMI.
Discussion
The present longitudinal survey assessed depression and anxiety trajectories over 6 months of the COVID-19 pandemic in a large German population-based probability sample.
We replicated findings showing mental health impairments early in the pandemic (11, 12, 18), with females (18, 25), younger people (18) and people with lower education level being more affected (7). Moreover, we found people on both poles of the BMI spectrum to be more affected, while underweight/obesity might be associated with higher vulnerability toward stress and generally increased mental health burden (21). The BMI-related effects in our sample might partly also mirror current longitudinal trends indicating an increased incidence of eating disorder diagnoses over the first months of the pandemic (26). Regarding potential sex differences in mental health outcomes, it is important to consider several aspects: First of all, longitudinal representative trajectory data on mental health does not report sex differences (10, 15, 16), highlighting again the importance to differentiate between initial and ongoing reaction to the crisis. Secondly, sampling effects could influence data as especially in convenience samples, a significant larger group of participants is female (7). Third, population-based surveys are usually brief and cover the most common mental health outcomes, and while women might just be more likely to endorse symptoms of anxiety and depression, surveys potentially neglect symptoms that are more common experienced in males under stressful conditions (27). Finally, elevated rates of anxiety and depression in females early in the pandemic might partly reflect common gender roles rather than biological sex differences, for instance, women juggling employment and care work under lockdown conditions (27).
Our hypothesis of overall longitudinal deterioration in anxiety and depression 6 months later was supported. Yet, most people remained stable in the range of good mental health, and these individual trajectories support recent evaluations that the mental health of most participants remains stable despite pandemic-induced stress (8–10, 16). The trajectory data also matches with our theoretical argument related to assumptions of general stress models (1, 2): Initial increased mental health burden might mirror acute stress in the general population during the first lockdown in spring 2020. Over half a year, the majority of the population shows resilience toward the ongoing pandemic, however there is also a substantial group showing metal health deterioration under this now chronic stress situation. development of mental symptoms and disorders.
In contrast to trajectory data from UK covering earlier time intervals (10, 16), the group in our sample experiencing mental health deterioration was slightly smaller, still, there were clearly more people declining than improving in mental health, while these contrasting groups were nearly equal in the UK surveys (10, 16). Our data covers a comparably longer time interval, re-assessing the sample after reapplication of nationwide lockdown measures in Germany, and this might explain why we found less improvement regarding anxiety and depression. BMI was the only variable predicting mental health change over 6 months, though this effect was small and should be interpreted with caution. However, the evidence on who is vulnerable in the long run of the pandemic is still limited, and also a recent study investigating mental health trajectories concludes that most of the predictors for distress in early pandemic stages were less consistently associated with longitudinal mental health trajectories (10). There is preliminary evidence for pre-existing illness, socioeconomic status and ethnicity to predict long-term mental health deterioration during COVID-19 pandemic (16).
Germany is a high-income country, and, in light of this, it is important to consider that trajectories in population mental health may also be related to the national health and social care systems, as well as specific government responses to the crisis and available resources in the society. Indeed, Germany has taking several measures in order to mitigate the impact of the pandemic on people's live circumstance, for instance, financial reimbursement was widely implemented in Germany for individuals unable to work during lockdowns. In contrast, economic uncertainty throughout the pandemic might be more severe and might impact more strongly mental health outcomes in developing countries (28).
Strengths and limitations
In the present study, we report data on longitudinal mental health outcomes during COVID-19 pandemic from a population-based probability sample. As such, it overcomes some of the methodological weaknesses of online survey data (5) which currently forms most of the evidence based on mental health outcomes during the pandemic (7). Our survey participants were invited via mail to their postal address, which allows also people to participate who would have been digitally excluded. Our data covers an interval of 6 months, and we rely on a widely used instrument assessing anxiety and depression (20). The PHQ-4 is a brief screening instrument with excellent psychometric qualities (20), allowing for an ecological assessment of mental health outcomes, which is an advantage especially in large surveys. However, at the same time, we did not cover other aspects of mental health, for instance such as insomnia. Further limitations comprise that the study protocol was not pre-registered, we cannot compare to pre-pandemic data; our sample exclusively stems from an urban background, and the survey lacks information about variables which have previously been identified to influence mental health outcomes, such as ethnicity and income (15, 16), sense of coherence (29) or media use (30). The PHQ-4 norm data was published in 2010 which dates back several years from the implementation of the present study. In the course of time, the prevalence of anxious and depressive symptoms might have varied due to factors unrelated to the pandemic. We found a responder bias between T1 and T2 assessment, however, none of the respective variables was strongly associated with mental health change over time. It should be noted that at T1, the concept of predictors is weaker than in the longitudinal setting at T2.
Perspectives and future studies
Future research efforts are needed for an in-depth investigation of long-term trajectories of mental health throughout the pandemic and also post-pandemic (7). For instance, it will be insightful to analyze the development through winter and spring 2020/21 prolonged lockdown conditions in many countries, but also throughout winter 2022 which was characterized by altered strains and circumstances with a novel virus variant. Taking a longer-term perspective, it will be an important question if elevated mental health burden throughout the pandemic puts individuals at risk to develop clinical mental health conditions, and, on a population-level, if and when overall mental health status recovers to pre-pandemic levels. A further pivotal line of research focuses on predictors of both, mental health deterioration and mental resilience throughout the pandemic on a population level and in vulnerable subgroups (17, 31). Knowledge on such risk and protective factors will inform tailored prevention efforts and intervention strategies for future pandemic circumstances. Beyond, and taking a more global perspective, a stronger differentiation of how population mental health has been affected in countries with different government measures, socio-economic levels and health care systems is necessary in order to better understand which political and administrative interventions might be harmful and helpful.
Conclusions
Our longitudinal population-based study contributes to the literature on mental health outcomes during COVID-19 pandemic by reporting trajectory data beyond questionnaire mean scores. These data show that most individuals remain in a stable and healthy range regarding symptoms of anxiety and depression under prolonged pandemic-related stress. Our study indicates that vulnerability factors differ over the course of the pandemic: While most of those initially vulnerable to acute stress might quickly adapt (15), other groups vulnerable to long-term effects of stress evolve over time.
Importantly, a considerable subsample did experience a deterioration of depression and anxiety symptoms over 6 months. Research efforts on long-term peri- and post-pandemic trajectories of mental health are needed in order to tailor prevention efforts for future pandemic circumstances (4, 32) and to offer support to vulnerable individuals (4), including adapted dissemination strategies, digital and low-threshold interventions (33).
Data availability statement
Raw data related to the present study will be made available by the corresponding author upon reasonable request.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee at the Medical Faculty of the University Tübingen and the University Hospital Tübingen. The patients/participants provided their written informed consent to participate in this study.
Author contributions
KEG, GP, JSJ, SE, and FJ designed the study and implemented core study procedures. AD and FS contributed to preparation of the survey and supported survey conduction and data handling. PM is the responsible biostatistician. PM and LMSH conducted the data analysis and prepared the figures. BL provided data for parts of the data analysis. PM, KEG, SZ, and FJ interpreted the data. KEG drafted the manuscript. All authors critically revised it and approved the final manuscript.
Acknowledgments
We thank Ansgar Schmitz-Veltin for his support in drawing the sample as well as Ursula Krause and Oliver Wienand for support in conduction of the survey. We are grateful to Kristina Overkamp, Anne Herschbach, and Iris Armbruster for data entry.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.1000722/full#supplementary-material
References
1. Selye H. Forty years of stress research: principal remaining problems and misconceptions. Can Med Assoc J. (1976) 115:53–6.
2. Guidi J, Lucente M, Sonino N, Fava GA. Allostatic load and its impact on health: a systematic review. Psychother Psychosom. (2021) 90:11–27. doi: 10.1159/000510696
3. Pfefferbaum B, North CS. Mental health and the Covid-19 pandemic. N Engl J Med. (2020) 383:510–2. doi: 10.1056/NEJMp2008017
4. Rapado-Castro M, Arango C. Building up resilience in an uncertain world: mental health challenges in the aftermath of the first modern pandemic. Eur Arch Psychiatry Clin Neurosci. (2021) 271:1001–3. doi: 10.1007/s00406-021-01313-4
5. Nieto I, Navas JF, Vazquez C. The quality of research on mental health related to the COVID-19 pandemic: a note of caution after a systematic review. Brain Behav Immun Health. (2020) 7:100123. doi: 10.1016/j.bbih.2020.100123
6. Pierce M, McManus S, Jessop C, John A, Hotopf M, Ford T, et al. Says who? The significance of sampling in mental health surveys during COVID-19. Lancet Psychiatry. (2020) 7:567–8. doi: 10.1016/S2215-0366(20)30237-6
7. Kunzler AM, Rothke N, Gunthner L, Stoffers-Winterling J, Tuscher O, Coenen M, et al. Mental burden and its risk and protective factors during the early phase of the SARS-CoV-2 pandemic: systematic review and meta-analyses. Glob Health. (2021) 17:34. doi: 10.1186/s12992-021-00670-y
8. Prati G, Mancini AD. The psychological impact of COVID-19 pandemic lockdowns: a review and meta-analysis of longitudinal studies and natural experiments. Psychol Med. (2021) 51:201–11. doi: 10.1017/S0033291721000015
9. Ahrens KF, Neumann RJ, Kollmann B, Plichta MM, Lieb K, Tuscher O, et al. Differential impact of COVID-related lockdown on mental health in Germany. World Psychiatry. (2021) 20:140–1. doi: 10.1002/wps.20830
10. Shevlin M, Butter S, McBride O, Murphy J, Gibson-Miller J, Hartman TK, et al. Refuting the myth of a 'tsunami' of mental ill-health in populations affected by COVID-19: evidence that response to the pandemic is heterogenous, not homogeneous. Psychol Med. (2021). doi: 10.1017/S0033291721001665. [Epub ahead of print].
11. McGinty EE, Presskreischer R, Han H, Barry CL. Psychological distress and loneliness reported by US adults in 2018 and April 2020. JAMA. (2020) 324:93–4. doi: 10.1001/jama.2020.9740
12. Pierce M, Hope H, Ford T, Hatch S, Hotopf M, John A, et al. Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population. Lancet Psychiatry. (2020) 7:883–92. doi: 10.1016/S2215-0366(20)30308-4
13. McGinty EE, Presskreischer R, Anderson KE, Han H, Barry CL. Psychological distress and COVID-19-related stressors reported in a longitudinal cohort of US adults in April and July 2020. JAMA. (2020) 324:2555–7. doi: 10.1001/jama.2020.21231
14. Hyland P, Shevlin M, Murphy J, McBride O, Fox R, Bondjers K, et al. A longitudinal assessment of depression and anxiety in the Republic of Ireland before and during the COVID-19 pandemic. Psychiatry Res. (2021) 300:113905. doi: 10.1016/j.psychres.2021.113905
15. Fancourt D, Steptoe A, Bu F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: a longitudinal observational study. Lancet Psychiatry. (2021) 8:141–9. doi: 10.1016/S2215-0366(20)30482-X
16. Pierce M, McManus S, Hope H, Hotopf M, Ford T, Hatch SL, et al. Mental health responses to the COVID-19 pandemic: a latent class trajectory analysis using longitudinal UK data. Lancet Psychiatry. (2021) 8:610–9. doi: 10.2139/ssrn.3784647
17. Riepenhausen A, Veer IM, Wackerhagen C, Reppmann ZC, Kober G, Ayuso-Mateos JL, et al. Coping with COVID: risk and resilience factors for mental health in a German representative panel study. Psychol Med. (2022). doi: 10.1017/S0033291722000563. [Epub ahead of print].
18. Hettich N, Entringer TM, Kroeger H, Schmidt P, Tibubos AN, Braehler E, et al. Impact of the COVID-19 pandemic on depression, anxiety, loneliness, and satisfaction in the German general population: a longitudinal analysis. Soc Psychiatry Psychiatr Epidemiol. (2022). doi: 10.1007/s00127-022-02311-0. [Epub ahead of print].
19. Kroenke K, Spitzer RL, Williams JB, Lowe B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics. (2009) 50:613–21. doi: 10.1176/appi.psy.50.6.613
20. Lowe B, Wahl I, Rose M, Spitzer C, Glaesmer H, Wingenfeld K, et al. A 4-item measure of depression and anxiety: validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J Affect Disord. (2010) 122:86–95. doi: 10.1016/j.jad.2009.06.019
21. Herhaus B, Kersting A, Brahler E, Petrowski K. Depression, anxiety and health status across different BMI classes: a representative study in Germany. J Affect Disord. (2020) 276:45–52. doi: 10.1016/j.jad.2020.07.020
22. Guerrini Usubini A, Cattivelli R, Varallo G, Castelnuovo G, Molinari E, Giusti EM, et al. The relationship between psychological distress during the second wave lockdown of COVID-19 and Emotional eating in italian young adults: the mediating role of emotional dysregulation. J Pers Med. (2021) 11:569. doi: 10.3390/jpm11060569
23. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. (2008) 61:344–9. doi: 10.1016/j.jclinepi.2007.11.008
24. Kroenke K, Spitzer RL, Williams JB, Monahan PO, Lowe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. (2007) 146:317–25. doi: 10.7326/0003-4819-146-5-200703060-00004
25. Plomecka M, Gobbi S, Neckels R, Radzinski P, Skorko B, Lazzeri S, et al. Factors associated with psychological disturbances during the COVID-19 pandemic: multicountry online study. JMIR Ment Health. (2021) 8:e28736. doi: 10.2196/28736
26. Taquet M, Geddes JR, Luciano S, Harrison PJ. Incidence and outcomes of eating disorders during the COVID-19 pandemic. Br J Psychiatry. (2021) 220:1–3. doi: 10.1192/bjp.2021.105
27. Giel KE, Derntl B. The weaker sex? What we can learn from sex differences in population mental health during and beyond the COVID-19 pandemic. Eur Arch Psychiatry Clin Neurosci. (2021) 272:165–6. doi: 10.1007/s00406-021-01312-5
28. Duarte F, Jimenez-Molina A. A longitudinal nationwide study of psychological distress during the COVID-19 pandemic in Chile. Front Psychiatry. (2022) 13:744204. doi: 10.3389/fpsyt.2022.744204
29. Schafer SK, Sopp MR, Schanz CG, Staginnus M, Goritz AS, Michael T. Impact of COVID-19 on public mental health and the buffering effect of a sense of coherence. Psychother Psychosom. (2020) 89:386–92. doi: 10.1159/000510752
30. Bendau A, Petzold MB, Pyrkosch L, Mascarell Maricic L, Betzler F, Rogoll J, et al. Associations between COVID-19 related media consumption and symptoms of anxiety, depression and COVID-19 related fear in the general population in Germany. Eur Arch Psychiatry Clin Neurosci. (2021) 271:283–91. doi: 10.1007/s00406-020-01171-6
31. Veer IM, Riepenhausen A, Zerban M, Wackerhagen C, Puhlmann LMC, Engen H, et al. Psycho-social factors associated with mental resilience in the Corona lockdown. Transl Psychiatry. (2021) 11:67. doi: 10.1038/s41398-020-01150-4
32. Bu F, Steptoe A, Mak H, Fancourt D. Time use and mental health in UK adults during an 11-week COVID-19 lockdown: a panel analysis. British Journal of Psychiatry. (2021) 219:551–6. doi: 10.1192/bjp.2021.44
Keywords: anxiety, COVID-19, depression, mental health, pandemic, population
Citation: Giel KE, Martus P, Paul G, Jürgensen JS, Löwe B, Serna Higuita LM, Dörsam AF, Stuber F, Ehehalt S, Zipfel S and Junne F (2022) Longitudinal development of depression and anxiety during COVID-19 pandemic in Germany: Findings from a population-based probability sample survey. Front. Psychiatry 13:1000722. doi: 10.3389/fpsyt.2022.1000722
Received: 22 July 2022; Accepted: 27 September 2022;
Published: 24 October 2022.
Edited by:
Ravi Philip Rajkumar, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), IndiaReviewed by:
Álvaro Jiménez-Molina, Diego Portales University, ChileSameh Attia, Justus-Liebig University Giessen, Germany
Copyright © 2022 Giel, Martus, Paul, Jürgensen, Löwe, Serna Higuita, Dörsam, Stuber, Ehehalt, Zipfel and Junne. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katrin E. Giel, a2F0cmluLmdpZWxAbWVkLnVuaS10dWViaW5nZW4uZGU=
†These authors have contributed equally to this work and share first authorship